progress on taking forward the global strategy for - … on taking forward the global strategy for...
TRANSCRIPT

Progress on Taking Forward the Global Strategy for
Women’s and Children’s Health
– Bangladesh Country Case Study
Report commissioned by the Partnership for Maternal, Newborn & Child Health
(PMNCH) to inform the PMNCH 2012 report on commitments to the Global
Strategy for Women’s and Children’s Health
Final version
September 2012

1
Content
Chapter Title Page
Acronyms 2
1. Introduction 4
2. Situational analysis: Bangladesh 6
2.1 Overview 6
2.2 Development 6
2.3 Health context 7
2.4 RMNCH Indicators 7
2.5 Policy context 8
2.6 Institutional context 9
2.7 Timelines 11
3. Overview of commitments made 15
4. Key Findings 18
5. Conclusions 29
6. Summary of recommendations: 31
Annex 1: Research questions and methods 32
Annex 2: List of Key Informants 34
Annex 3: List of Commitments 36
Annex 4: Progress against the COIA’s 10 recommendations 41
Annex 5: Checklist for COIA Recommendations 44
Annex 6: Semi-structured Questionnaire (later modified) 45

2
Acronyms ANC Antenatal Care APR Annual Programme Review ARH Adolescent and Reproductive Health AusAID Australian Agency for International Development BDHS Bangladesh Demographic and Health Survey BEmOC Basic Emergency Obstetric Care BMMS Bangladesh Maternal Mortality Survey BNC Bangladesh Nursing Council BRAC Building Resources Across Communities
CAG Community Action Groups CEmONC Comprehensive Emergency Obstetric and Neonatal Care CIDA Canadian International Development Agency COIA Commission on Information and Accountability CSBA Community Skilled Birth Attendant CSO Civil Society Organization DFID Department for International Development (UK) DGFP Directorate General of Family Planning DGHS Directorate General of Health Services DHS Demographic and Health Survey DPF Direct Programme Funding DSF Demand Side Financing EKN Embassy of the Kingdom of the Netherlands EmOC Emergency Obstetric Care EPI Expanded Programme of Immunization FHA Family Welfare Assistant FMR Financial Management Reports FWA Female Welfare Assistant FWV Female Welfare Visitor GNI Gross National Income HA Health Assistant HDI Human Development Index HEU Health Economics Unit HIS Health Information System HMIS Health Management Information System HNPSP Health, Nutrition and Population Sector Programme HPNSDP Health Population and Nutrition Sector Development Programme ICDDR,B International Centre for Diarrhoeal Disease Research, Bangladesh ICT Information and Communication Technology IDA International Development Association iERG independent Expert Review Group IMCI Integrated Management of Childhood Illness INGO International Nongovernmental Organization
IPU Inter-Parliamentary Union
JATRI Journalism Training & Research Initiative
JICA Japanese International Cooperation Agency KFW Kreditanstalt fur Wiederaufbau (German Development Loan Corporation) M&E Monitoring and Evaluation

3
MCWC Mother and Child Welfare Centre MDG Millennium Development Goal MDTF Multi-Donor Trust Fund MICS Multiple Indicator Cluster Surveys MIS Management Information System MMR Maternal Mortality Rate MNH Maternal and Neonatal Health MoHFW Ministry of Health and Family Welfare MP Member of Parliament NGO Nongovernmental Organization NHA National Health Accounts NIPORT National Institute of Population Research and Training NMR Neonatal Mortality Rate OOP Out of Pocket (expenditure) PMNCH Partnership for Maternal, Newborn & Child Health PPH Postpartum Haemorrhage PRSP Poverty Reduction Strategy Paper RH Reproductive Health RMNCH Reproductive, Maternal, Newborn and Child Health SBA Skilled Birth Attendant Sida Swedish International Development Agency SWAp Sector Wide Approach TFR Total Fertility Rate UN United Nations UNESCO United Nations Educational, Scientific and Cultural Organization USAID United States Agency for International Development VAW Violence Against Women WB World Bank WHO World Health Organization WRA White Ribbon Alliance

4
1. Introduction The United Nations Secretary-General's Global Strategy for Women's and Children's Health, which was launched in September 2010, has generated more than 200 commitments from a range of stakeholders.1,2 Mobilization of new commitments and action to implement the Global Strategy is supported by the “Every Woman Every Child” effort. To support greater accountability, and to further the understanding of the Global Strategy commitments, PMNCH launched a report in September 2011 entitled “Analysing commitments to advance the Global Strategy for Women’s and Children’s Health: The PMNCH 2011 Report”.3 In 2012, PMNCH will produce a further report at the request of the independent Expert Review Group (iERG) following the recommendations of the Commission on Information and Accountability for Women’s and Children’s Health (COIA). To get a holistic perspective of how the commitments support national reproductive, maternal, newborn and child health (RMNCH) strategies and programmes, three country case studies have been carried out to inform the PMNCH 2012 Report:
Bangladesh and Burkina Faso by HLSP, and Uganda by World Vision International. The three case studies have followed the same scope and methods, as outlined below. The overall research question of the country case studies was as follows: Is the implementation of the commitments to the Global Strategy supporting country progress towards achieving MDGs 4 and 5 through aligning with national plans, addressing health and development gaps, and ensuring accountability for results and resources? To inform the overall research question, the analytical questions explored were:
a) How do commitments add value to national policies, investments and service
delivery (compared to the counter-factual of no commitments to the Global
Strategy)?
b) What are the contextual factors and mechanisms that influence, catalyse or
constrain the implementation of the commitments?
c) Through which mechanisms is accountability for commitments to the Global
Strategy, and their impact on results and resources for women’s and
children’s health, addressed?
d) What is the general knowledge of the Global Strategy and its goals, and how
does it fit with existing national or regional initiatives?
e) What innovative solutions are used to sustainably, and at scale, accelerate
improvement of women’s and children’s health?
Countries were selected based on the following main criteria: the country has made a commitment to the Global Strategy and is the focus of several commitments from other stakeholders; the country has a high burden of maternal and child mortality,
1 The Global Strategy and background papers are available at: http://www.un.org/sg/globalstrategy
2 For a full list of commitments, see: www.everywomaneverychild.org
3 The PMNCH 2011 Report and related documentation, included completed questionnaires, see:
http://www.who.int/pmnch/topics/part_publications/2011_pmnch_report/en/index.html

5
and unmet need for family planning; and regional balance between Africa, Asia and Latin America.4 Data to inform the case studies were collected through key informant interviews and review of data in the public domain. This report presents the case study findings for Bangladesh.
4 Haiti was selected, but was replaced by Burkina Faso due to security concerns.

6
2. Situational analysis: Bangladesh
2.1 Overview
The population of Bangladesh exceeds 142 million;5 77% live in rural areas. 31.5%
live in poverty, 35.2% in rural areas and 21.3% in urban areas. Overall, this
represented an 8.5% reduction (8.6% in rural areas and 7.1% in urban areas) from
2005 to 2010.6 The 2001 Census showed that 43% of the population is aged below
15 years. Progress has been made in improving Bangladesh’s Human Development
Index (HDI) which now places the country among the medium-ranking HDI countries.
The country has seen an improvement in economic well-being since 2005 with gross
national income (GNI) per capita rising from US$ 470 in 2005 to US$ 770 in 2011.7
2.2 Development
Major changes have taken place in education with Bangladesh achieving gender
parity in both primary and secondary education8 (2005-2008). The adult literacy rate
15 years and over is 51% (2005-2009) compared to 26% in 1985-1994.9 The
number of girls entering secondary education has increased and importantly, the
proportion of mothers with no education has halved since 2001 and the proportion
with secondary schooling has nearly doubled.10 The number of women in
employment increased from 22% to 33% in 2007 (Demographic Health Survey,
DHS). However, despite the fact that women have a voice in Bangladesh
particularly through women’s right groups and the representation of women in
parliament, domestic violence remains high with 40-50% of women experiencing
physical or sexual violence in marriage. This is seen across all wealth quintiles.11
Two-thirds of women marry before the legal age of 18; half are under 16 when they
marry. A third of girls aged 15-19 have already started childbearing. Implementing
the minimum age for marriage and reducing the rate of adolescent pregnancies are
key priorities of the Government, and included in its commitments to the Global
Strategy for Women’s and Children’s Health as stated in its new health sector plan.
By 2010 average nominal income had increased by 59% (58% rural/57% urban)
compared with 2005. This has direct implications for health. As an illustration,
mobile phone usage has been dramatic, increasing from 11% in 2005 to 63% in
2010, with over 56% of rural households using them (compared to 6% in 2005).12
This has led to improved communication with health facilities, text messaging to
pregnant women, registration for antenatal care, and prompt referral to, and use of
facility based care. A more recent additional benefit is the ability to transfer money
by mobile phone, which could relieve difficulties in accessing emergency health care.
5 5
th national census Bangladesh (2011)
6 Household income and expenditure survey. 2010. Bangladesh Bureau of statistics
7 World Bank data 2011 GNI per capita ( Atlas method US$)
8 www.unicef.org/education/bangladesh_35367.html and www.worldbank.org/mdgs/gender.html
9 EFA monitoring report. UNESCO. http://www.unesco.org/new/en/education
10 Bangladesh Maternal Mortality and Health care Survey 2010
11 Women’s Health in Bangladesh. National Institute for Population Research and Training
(NIPORT) with data from DHS 2007. 12
5th national census Bangladesh (2011) Bureau of Statistics

7
2.3 Health context
In 1991, the maternal mortality ratio (MMR) was 574 per 100 000 live births and the
under-5 mortality rate was 151 per 1000 live births. As with many other countries
attending the Millennium summit of 2000, Bangladesh has focused attention on
addressing the child and maternal health Millennium Development Goals (MDGs) 4
and 5. High level efforts on interventions such as the Integrated Management of
Childhood Diseases (IMCI) and a successful immunization programme (the
Expanded Programme of Immunization [EPI] coverage increased from 54% in 1991
to 87.2% in 2006) facilitated rapid progress on MDG 4 and has set Bangladesh firmly
on track to achieve the 2015 target. By 2006 the under-5 mortality had fallen to
62/1000 live births and infant mortality from 94 to 45 deaths per 1000 live births. In
recognition of this achievement, the Prime Minister received the United Nations
award for country progress against MDG4 in 2010. However neonatal mortality
remained a major contributor to under-5 mortality. By 2010, under-5 mortality had
fallen to 48 per 1000 live births. In 2001 the Bangladesh Maternal Mortality Survey
(BMMS) showed good progress on MDG 5 with the MMR at 322 per 100 000. Data
released in 2010 indicated this trend was continuing, with the MMR at 194 per
100 000 live births.
Other successes include the decline in the prevalence of malaria from 42
cases/100 000 in 2001 to 34 in 2005. In the same period the successful treatment of
tuberculosis saw an increase from 84% in 2002 to 91% in 2005.13 Bangladesh was
declared polio free in 2000. Several outbreaks of wild virus in subsequent years
have been met by a vigorous response by the Government.
2.4 RMNCH Indicators
In addition to those detailed in the previous section, the BMMS surveys 2001 and
2010 show positive trends for maternal health. Although between 2001 and 2010
there was a significant reduction in the rates of haemorrhage (35% reduction) and
eclampsia (50% reduction), these two remain the dominant direct causes of maternal
deaths. Abortion related deaths fell from 5% to around 1% of obstetric deaths. While
the overwhelming majority of births take place in the home (76% in 2010, according
to BMMS data), facility-based delivery over the period 2001 to 2010 has shown
increases: 2.7% to 11.3% in the private sector; 5.8% to 10% in the public sector; and
0.6% to 2.0% in the NGO sector. Skilled birth attendance at home deliveries
remains low (3.5% in 2001; 4.3% in 2010). The caesarean section rate increased
over the same period from 2.6 to 12.2% (mainly in the private sector). However,
among women who reported no complications, 9.4% had a caesarean section
performed suggesting these may have been done unnecessarily.
Progress in addressing the “Three Delays” (delay in seeking care, delay in transport
to a facility, delay in receiving appropriate care) has been significant. Care seeking
from a health facility for obstetric complications had increased from 16% to 29%
(2001 to 2010) and was reflected across all wealth quintiles. This is attributed to the
focus on improving community-based awareness and referral mechanisms.
However, there were cases where women had sought care at facilities that did not
13
National Health Policy update 2008
8
provide emergency obstetric care, leading to maternal deaths in some cases. More
rapid contact with health providers is also thought to be due to better communication
(greater use of mobile phone technology, improved roads, as well as improved
economic conditions). Although nearly all the indicators for utilization of health
services by the poorest quintile show improvement (and at a faster rate than those in
the wealthiest quintile), there remains a substantial absolute gap between rich and
poor.14
Between 2001 and 2010, the Total Fertility Rate fell 22% from 3.2 to 2.5.
Preliminary data from the DHS 2011 (not formally released) suggests this trend is
continuing. The BMMS 2001-2010 also shows a corresponding shift in high parity
births (4+) down from 30% to 19% which also reduces the overall risk of maternal
death.
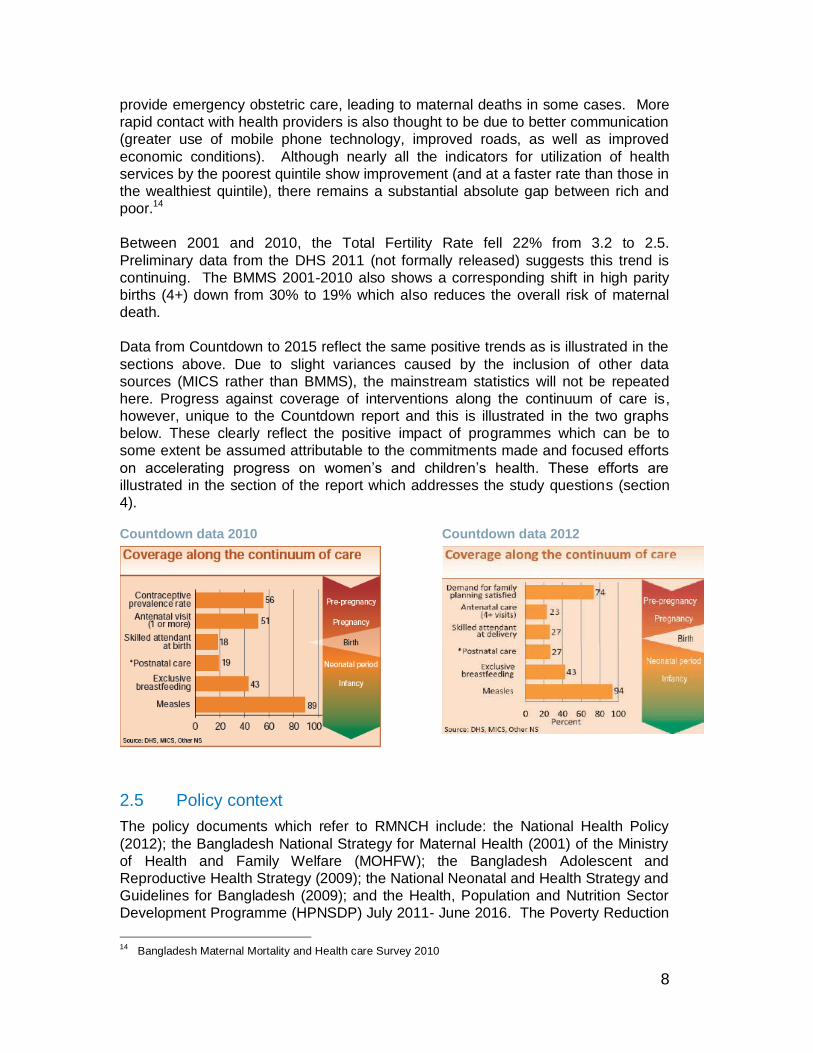
Data from Countdown to 2015 reflect the same positive trends as is illustrated in the
sections above. Due to slight variances caused by the inclusion of other data
sources (MICS rather than BMMS), the mainstream statistics will not be repeated
here. Progress against coverage of interventions along the continuum of care is,
however, unique to the Countdown report and this is illustrated in the two graphs
below. These clearly reflect the positive impact of programmes which can be to
some extent be assumed attributable to the commitments made and focused efforts
on accelerating progress on women’s and children’s health. These efforts are
illustrated in the section of the report which addresses the study questions (section
4).
Countdown data 2010 Countdown data 2012
2.5 Policy context
The policy documents which refer to RMNCH include: the National Health Policy
(2012); the Bangladesh National Strategy for Maternal Health (2001) of the Ministry
of Health and Family Welfare (MOHFW); the Bangladesh Adolescent and
Reproductive Health Strategy (2009); the National Neonatal and Health Strategy and
Guidelines for Bangladesh (2009); and the Health, Population and Nutrition Sector
Development Programme (HPNSDP) July 2011- June 2016. The Poverty Reduction
14
Bangladesh Maternal Mortality and Health care Survey 2010

9
Strategy Paper (PRSP) includes a specific goal to reduce the MMR by 75% and to
ensure access to reproductive health services for all by 2015, thereby addressing
the MDG 5 target.
The National Strategy for Maternal Health 2001 addresses Safe Motherhood in detail
with a focus on creating the conditions necessary for preventing maternal death and
disability. Its emphasis is on provision and utilization of quality antenatal care, safe
birth practices, postnatal care, and emergency obstetric care services. It does,
however, require updating as a detailed strategy document in order to support
HPNSDP. Despite several attempts, it still remains work in progress though the
BMMS data of 2010 and DHS data of 2011, once fully released, will be catalysts for
its amendment. The HPNSDP and its related Operational Plans (2011-2016),
although less detailed than the National Strategy for Maternal Health, do set out the
broad approach for implementation of the commitments made to the Global Strategy
in 2010.
2.6 Institutional context
i. Health systems
The health system in Bangladesh requires significant strengthening. Health system
strengthening is a major component of the new sector plan. Human resources,
leadership and governance are all areas of weakness. Issues of ensuring availability
of drugs at the health facilities, deployment of appropriately trained health
professionals and maintenance of health care facilities continue to be constraints to
service delivery.
There has been a significant effort to renovate and improve the conditions of public
health facilities since 2001 to increase the scope of RMNCH services offered. These
health facilities include: sub-district centres (3375); Upazila Health Centres (397);
district level hospitals (80); medical college hospitals (13); and postgraduate and
specialized hospitals (31).15 In 2001 just three Upazila Health Centres were offering
comprehensive emergency obstetric and newborn care. By 2010 the number had
increased to 132, and 1500 health and family welfare centres at sub-district level
were being upgraded by the Government.16 Despite these efforts, persistent
constrains (staff shortages etc) have led to more than half of health expenditure
taking place in the private sector which continues to flourish.17
The MOHFW has two main directorates: the Directorate General of Health Services
(DGHS) and the Directorate General of Family Planning (DGFP). This division has
led to difficulties in effectively managing health system issues (see next section).
ii. Service providers
15
Health Policy of Bangladesh 2012 16
Bangladesh Maternal Mortality and Health care Survey 2010 17
HPNSDP (2011-2016)

10
Public health care is provided through a number of institutions under these two directorates, as listed below.
Level DGHS institutions DGFP institutions
District District Hospital Mother and Child Welfare Centre (MCWC)
Sub-district (Upazila) Upazila Health Complex (UHC)
Union (a number of villages – several unions make up an Upazila )
Family Welfare Centre (FWC)
Village Community Clinic (CC)
In the Upazila Health Complexes, both DGHS and DGFP cadres work together. The
same is true in the case of Community Clinics, each staffed by a Health Assistant
(HAs) and Family Welfare Assistant (FWA). Difficulty arises at the district level where
EmONC is delivered. There is an acute shortage of anaesthetists and pairing them
with obstetricians or medical doctors for performing caesarean sections is an
ongoing constraint as anaesthetists may be based in an MCWC. Anaesthetists fall
under DGFP and obstetricians/doctors under DGHS. Difficulties arise in imposing
modes of working together from the central level and agreements, if reached, are
worked out locally.
Lack of human resources are considered a major constraint in heath service delivery
and lack of incentives have led to a large number of ghost workers (workers not
present in facilities, mainly medical doctors) in the public sector (the doctor to
population ratio is 1:4719 whilst the nurse to population ratio is 1:8226).18 FWAs
and HAs are undergoing training as Community Skilled Birth Attendants (C-SBA)
and operate in both the public and private (NGO) sectors. To meet health needs,
Bangladesh requires around 100 000 doctors, 215 000 nurses and 65 000 midwives.
Currently, however, there are fewer than 50 000 available doctors, fewer than
30 000 nurse-midwives (two years nursing and one year midwifery), and no more
than 200 formally trained stand-alone midwives. It is important to note that nurse-
midwives are not dedicated to midwifery but work in all areas, while facility-based
deliveries remain the domain of medical staff.
A Human Resource assessment is shortly to be commissioned by UNFPA. It is
anticipated that the results will highlight the main human resource bottlenecks.
iii. Donor landscape
There are around 15 major donors in Bangladesh. The majority of RMNCH activities
and their funding are currently captured in the HPNSDP which is implemented
through the sector-wide approach (SWAp). This funding modality is one in which
major donors, including DFID, AusAID, USAID, CIDA, Sida, KFW and EKN
(Embassy of the Kingdom of the Netherlands, have pooled their resources with the
International Development Association (IDA) into a multi-donor trust fund (MDTF).
These pooled funds are channelled through the Government of Bangladesh’s
Treasury system and are administered by the World Bank. Non-pooled funds are
18
Health Policy of Bangladesh 2012

11
given (principally by multilaterals e.g. United Nations agencies) as direct programme
funding (DPF) to the Government or to specific activities. One or two donors (JICA
and previously USAID)19 opt to contribute to DPF due to their specific reporting and
operational requirements.
The national budgets in Bangladesh comprise the revenue budget which is funded
entirely by the Government of Bangladesh, and the development budget, funded by
the Government and its development partners. The development budget, as the
name suggests, is spent on projects and programmes that are aimed at developing
various sectors of the economy, including social sectors (e.g. health and education).
For the implementation of the last sector-wide programme, 56% of the funds came
from the revenue budget, while 44% came from the development budget. Of the
total development budget to be disbursed through 38 operational plans, 38% was
contributed by Government of Bangladesh (US$ 912 million), while the remaining
62% came from the development partners (US$ 1488 million). The overall
contribution of the Government to the total health budget (revenue + development)
was US$ 3929 million (73%) and that of the development partners was US$ 1488
million (27%).20
iv. Key stakeholders
There are a wide range of stakeholders in Bangladesh including around 4000 NGOs.
Others include civil society organizations (CSOs) such as women activists and
community groups, academia and research institutes, and business and social
marketing groups. Annual mapping of maternal and newborn health (MNH) activities
funded by development partners helps to identify coverage gaps among principal
partners involved in MNCH. The mapping reports show geographic coverage of
MNCH projects, expansion plans, Upazilas providing comprehensive emergency
obstetric and neonatal care (CEmONC) services, the scope of interventions and the
total cost allocation.
2.7 Timelines
i. Global events
Key informants agreed that many of the RMNCH global events that were presented
to them in a list were seen to impact RMNCH in Bangladesh to various degrees.
However, it was unanimously stated by the majority of these respondents that the
four greatest catalysts to accelerating efforts on women’s and children’s health in
Bangladesh were those presented in the timeline below:
19
USAID has recently joined the MDTF and makes partial contributions to DPF. 20
World Bank's Project Appraisal Document for the Health Sector Development Program, May 2011.

12
ii. Key national milestones for RMNCH
It was less easy to gauge the impact of national events on RMNCH given the short
interview time and the fact that we were asking respondents to recall these events.
The first three mentioned in the timeline below are referred to in policy documents,
indicating they informed in part the policy or strategy:
2000 •Millennium Development Goals 4 and 5a
2010 •UN Joint Action Plan for accelerating progress on maternal and newborn Health (New
York, April 2010) Launched by UN Secretary General (precursor to the Global strategy)
2010 •65th General Assembly of the United Nations. MDG award to Bangladesh
2010
•Global Strategy for Women’s and Children’s Health (September 2010) Roadmap on how to enhance financing, strengthen policy and improve service delivery for vulnerable women and children “Every Woman Every Child” launched
2000
•Launch of ‘Women’s Right to Life and Health Initiative (WRLH)’ by Government of Bangladesh.
July 2008
•H4 Joint Statement for Accelerated Implementation of the Maternal and Newborn Continuum of Care
April 2010
•Joint Mission H4. To strengthen partnership for maternal, neonatal and reproductive health.
2010
•State visit to Bangladesh of WHO Director General, Dr Margaret Chan. Discussion of WHO support to health and micro credit initiatives
Nov 2011 •UN General Secretary, Ban Ki Moon, visits Bangladesh

13
iii. Key development milestones
The two graphs below illustrate MMR against growth in GNI and improvements in
education. Many factors come together to contribute to the decline in the MMR and
include others not shown here, such as improved communications and road
transport. Increased economic well-being, the achievement of universal primary
education and increased numbers of females in secondary education were reasons
given by various respondents for the decline in MMR. Increased female rates of
education were also seen to be a factor in declining fertility rates (see results
milestones below).
Decline in Maternal Mortality rate against growth in GNI
Decline in Maternal Mortality rate against education indicators
0
50
100
150
200
250
300
350
2000 2010
$-
$100.00
$200.00
$300.00
$400.00
$500.00
$600.00
GNI ($)
MMR
1994
2007
1991
2010
0%
10%
20%
30%
40%
50%
60%
70%
80%
1985 -1994 2005-2009
Adu
lt li
tera
cy (%
)
0
100
200
300
400
500
600
700
Adult Literacy
% of female householdpopulation attendingschool 11-15 yrs
MMR
14
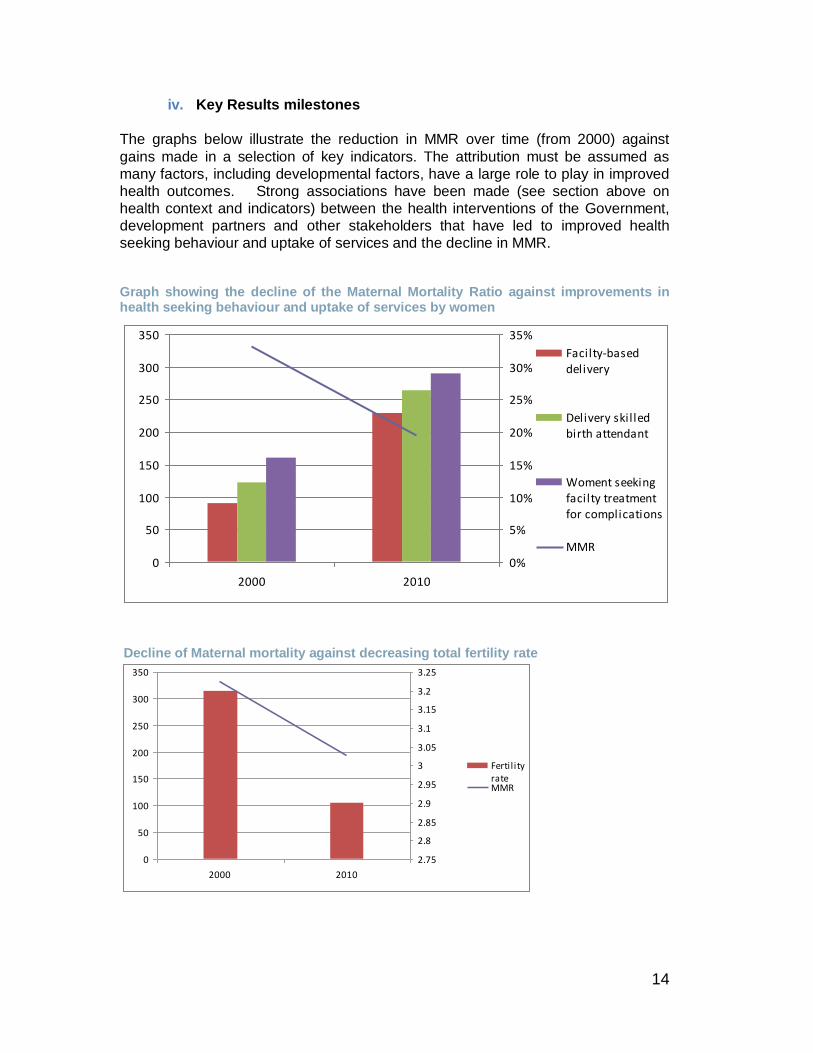
iv. Key Results milestones
The graphs below illustrate the reduction in MMR over time (from 2000) against
gains made in a selection of key indicators. The attribution must be assumed as
many factors, including developmental factors, have a large role to play in improved
health outcomes. Strong associations have been made (see section above on
health context and indicators) between the health interventions of the Government,
development partners and other stakeholders that have led to improved health
seeking behaviour and uptake of services and the decline in MMR.
Graph showing the decline of the Maternal Mortality Ratio against improvements in health seeking behaviour and uptake of services by women
Decline of Maternal mortality against decreasing total fertility rate
0
50
100
150
200
250
300
350
2000 2010
0%
5%
10%
15%
20%
25%
30%
35%
Facilty-baseddelivery
Delivery skil ledbirth attendant
Woment seekingfacilty treatmentfor complications
MMR
0
50
100
150
200
250
300
350
2000 2010
2.75
2.8
2.85
2.9
2.95
3
3.05
3.1
3.15
3.2
3.25
Fertil ityrate MMR

15
3. Overview of commitments made The combined commitments of the Government and non-governmental partners to
the Global Strategy in Bangladesh address a balance of needs across the continuum
of care. Donor commitments are well aligned with those of the Government, while at
policy and planning level there is significant harmonization in setting priorities and
ensuring gaps are addressed. Events in the run up to the launch of the Global Strategy provided a vehicle for intense dialogue between Government and development partners around the commitments to be made. The drive came from the Government but it sought technical input from development partners in the form of evidence-based knowledge sharing and strategic guidance in order to shape the commitments. The commitments were presented by the Prime Minister at the United Nations General Assembly in New York in 2010. Priority was given to the training of 3000 midwives in response to the body of evidence behind it. This work had already started in 2008 when the World Health Organization (WHO) developed a midwifery training policy position for the Government of Bangladesh. According to the United Nations Children’s Fund (UNFPA), there had been little real Government engagement in training of midwives until the Global Strategy was launched and the debate was revived. The evidence cited for the commitment made reference to the fact that skilled birth attendant at delivery has a significant impact on reducing the risk of maternal mortality. However this commitment was also informed by evidence of best practice, including that from the International Confederation of Midwives regarding length and structure of training. The number to be trained (3000 by the year 2015) was based on what was considered to be achievable in the timeframe. Notably, this number forms only a part of the midwifery workforce expansion planned for the longer term (beyond 2015). The projected target for the midwifery workforce post-2015 was reported to be based on evidence of required health worker numbers. The source of the evidence base was not clarified. However, WHO (2006) recommends 2.28 health workers/1000 population to deliver 80% coverage of essential basic service package21 and it was suggested that a similar WHO evidence base was used.
The high priority given to training of midwives is a good example of the process by
which a country led conception translated into a commitment, policy and
implementation (see box below).
21
Reassessing the relationship between Human resources for health, intervention coverage and health outcomes Niko Speybroeck, Yohannes Kinfu, Mario R. Dal Poz and David B. Evans Evidence and Information for Policy World Health Organization Geneva, March 2006

16
Box 1: Training midwives in order to provide safe delivery and refer complications
‘Midwives’ (as defined by the International Confederation of Midwives) are a new cadre of health
provider in Bangladesh. The need to increase the number of assistants who could provide a clean safe
delivery and refer complications had been identified by the Government of Bangladesh prior to the
launch of the Global Strategy, as a necessary means to reach the 77% of women delivering at home
especially in underserved areas. Attention to the value of skilled birth attendance was enhanced by
other events, such as the 2008 H4+ accelerated effort to improve MNH initiatives.
The immediate events that led up to the launch of the Global Strategy during which time commitments
were being formulated opened the route, by request of Government, for the consultation between itself,
donors and other stakeholders and provided technical exchange on best practice. This included
dialogue on the numbers of midwives required to provide RMNCH services. This moved the
commitment from a broader need for SBA to the specific need of a calculated number of midwives who
would both fill a human resource gap across 423 rural Upazila health facilities where 24 hour EmOC is
required, as well as providing supervision to the community-based SBAs.
Collaboration around this issue not only gave it priority as a commitment but ensured the policy and
planning process around its formulation was robust. The Government line director responsible for this
activity was interviewed and it is clear that he fully grasps the wider and complex systemic issues that
need to be addressed around training of midwives. Evidence from triangulation suggests that these
issues are being addressed through active planning processes. All key informants whose activities fall
within the HPNSDP were aware of this activity (information is shared at the respective task force
meetings for operational plans – for example, human resource and MNCH Decline in Maternal Mortality
rate against education indicators ) and those that train Community SBA’s were informed of this planned
commitment. H4+ partners (UNFPA leading with WHO technical input) are fully engaged with
Government and the Directorate of Nursing on this and a standard curriculum has been designed. The
number 3000 is also considered achievable as a commitment to the year 2015.
As these midwives are required immediately there will be two main streams. One will give an additional
six months midwifery training to update the existing health cadre of nurse midwife. These had two years
nursing and one year’s midwifery but they have not used the midwifery skill for delivery as in facilities it
remains the domain of medical doctors. The six months is considered adequate to update and add to
previously acquired skill. In July 2012 a direct entry course will start consisting of three years midwifery.
This does not require pre-entry health experience. As graduates will not emerge until 2015 the former
group will close the gap. Post 2015, the scale up will continue to approximately 20 000 midwives.
BRAC is planning to start a training course funded by DFID. This will use the same direct entry
curriculum but condensed into two years as the Afghan model. This is under discussion.
Midwifery training is already underway and 200 midwives of the 3000 targeted have completed their
training. The training of trainers is being addressed simultaneously and a meeting with two expatriate
midwives who are contracted by WHO to implement this activity, suggested that whilst ability is seen to
be very mixed, the commitment of tutors is high overall and response to training is positive in terms of
tutor interest and ability to grasp new concepts.

17
Although the commitments made by the business sector do align with the RMNCH
country plans and the key concept of the Global Strategy, some businesses may
have no direct relation with Government or development partners. However, there
are good lessons to be shared across the private sector, particularly addressing
human rights and equity issues. For example, Viyellatex Group Bangladesh
(garment industry) employs disabled workers; has set up special needs schooling for
physically disadvantaged children whose parents are in the workforce; provides
pregnant women in employment with two ultrasound scans in collaboration with a
private sector clinic; and provides child health checks for workers’ children (who are
referred onward if necessary). The Chairman believes that upholding these equity
rights promotes a sense of well-being among company employees and helps ensure
a more effective business. A second example is provided by Johnson & Johnson.
Johnson & Johnson (whilst not interviewed) supports the MaMoni project, a
government led project with multistakeholder buy-in that uses innovative mobile
phone technology to support health information systems for improved maternal and
neonatal health outcomes. Johnson & Johnson provides an example of a large-
scale public-private partnership engaging in the delivery of Global Strategy
commitments.

18
4. Key Findings It is clear that the implementation of commitments has supported country progress towards achieving MDGs 4 and 5 through aligning with national plans, addressing health and development gaps, and ensuring accountability for results and resources. In particular, many of the interventions built around commitments have a strong gender or human rights focus. Both Government and development partner respondents were aware of the strong relation between the increases in numbers of girls in secondary education and its positive impact on reducing MMR. A respondent at the World Bank referred to the existence of a multisectoral approach that includes education (conditional cash transfer), health, safety nets and nutrition.
The following sections, organized by specific research questions, describe how
effective this has been.
a. How do commitments add value to national policies, investments and service delivery (compared to the counter-factual of no commitments to the Global Strategy)?
Informants were asked about the added value of the Global Strategy and
commitments made, in terms of the counterfactual i.e. what may have been the
current situation regarding RMNCH policy and programming in country, had the
Global Strategy not existed?
Since the Millennium Summit in 2000, when the MDGs were agreed by world
leaders, and with the increased importance of MNCH on the global agenda during
the last decade, the Government of Bangladesh has given priority to MDGs 4 and 5
and increasing attention on how to strengthen its policy and strategy on MNCH in
order to achieve these goals.
Three key events were identified as being catalytic: the Millennium Summit in 2000;
the presentation of the United Nations award to Bangladesh on its progress on MDG
4 in 2010; and the Global Strategy launched in September 2010. The Global
Strategy was seen as catalytic in accelerating efforts to address MDG 5 and
neonatal health (intricately linked to health of the mother) in Bangladesh.
Subsequent commitments to the Global Strategy are clearly embedded in the
HPNSDP 2011-2016 and its supporting programme implementation plan and
operational plans. With its two focal areas being the improvement of health services
and strengthening health systems, this strategy “aims at improving priority health
services in order to accelerate the achievement of the health related MDGs by
capitalising on and scaling up the interventions undertaken under the HNPSP as well
as introducing new interventions”.22
The priority objectives of the HPNSDP are:
Increasing the number of skilled birth attendants through training of 3000
midwives;
22
Strategic Plan for Health, Population and Nutrition Sector Development Programme
(HPNSDP) 2011- 2016

19
Increasing facility-based 24 hour, seven day services for management for
maternal complications;
Emphasizing long-acting permanent methods and unmet needs of family
planning.
HPNSDP also includes interventions which are stated to ‘add value’ to the plan. Among the list of these and perhaps most relevant to the Global Strategy are:
Mainstreaming gender, equity and voice in core programmes such as MNCH and
nutrition;
Improving management information systems (MIS) with information and
communication technology (ICT) and establishing M&E systems;
Increasing coverage and quality of services by strengthening intersectoral
coordination private sector collaboration.
Against the backdrop of the accelerated efforts to achieve the MDGs key informants
found it difficult to say what is driving what vis-à-vis the Global Strategy and the
emerging emphasis on RMNCH at country level.
b. Have the efforts and activities of countries around MDGs 4 and 5 set the
scene for the Global Strategy or did the Global Strategy heavily influence
where many of these 49 Global Strategy priority countries sit today on
RMNCH?
The overall feeling among key informants for Bangladesh is ‘a bit of both’. Certainly
for some donors the Global Strategy works both ways – influencing donor policy as
well as ensuring that donors promote it at Government level.
However, the Global Strategy has unequivocally placed commitments at the core of
the country’s RMNCH policy and investments to which all stakeholders can be called
to account, and that in itself is a laudable achievement. Nowhere better is it
expressed than in the words of the Minister of Health in his foreword address on
HPNSDP where he states that this new strategic health plan :
“….reflects the direction and determination of the Government’s commitment
to serve the people with their needs in health, population and nutrition
services, as stated by the Honorable Prime Minister while addressing the 65th
General Assembly of the UN on progress in attaining the MDGs”
Respondents felt that the commitments “provide a pathway” and “enhance the
awareness of mutual responsibility towards fulfilling them”. This is less likely to have
happened in the absence of the Global Strategy. Investments follow the
commitments made for each donor group and the donors support Government
plans.
The MoHFW line directors interviewed were, without exception, all highly engaged
with the commitments to the Global Strategy and systems related issues e.g. the use
of information and communication technologies in national health information
systems (see comment below under Catalysts).

20
c. What are the contextual factors and mechanisms that influence, catalyse
or constrain the implementation of the commitments?
Mechanisms or factors that catalyse implementation of commitments tend to be
distinct whilst those that constrain the process are complex and interlinked.
Catalysts
The winning of the United Nations award by Bangladesh in 2010 for progress made
on MDG 4 (the award was made prior to the launch of the Global Strategy) acted as
a major catalyst to drive accelerated efforts towards addressing RMNCH gaps and
also providing an incentive for achieving MDG5. Of the global events listed, the
Millennium Summit in 2000 and the award at 65th General Assembly of the United
Nations resonated the most in country. The Global Strategy was seen as the event
which accelerated efforts further and keeps them at the forefront of attention. The
fact that country commitments were made at the highest level by the Prime Minister,
is seen to “drive the government machinery into action” (quote by Government key
informant and endorsed by others). Over this period there has also been an
increased acceptance of the value of and willingness of Government to collaborate
with the many NGOs delivering services and supporting service delivery, which
helps offset weaknesses in Government capacity. Likewise improved coordination
between Government and development partners through multiple channels
(donor/Government coordination meetings, task force groups for operational plans)
are forums in which programmatic gaps and weaknesses can be identified, as well
as information shared on successful innovation. The culture of Bangladesh was also
seen as a driver of innovation, allowing women to speak and give their contribution.
Women activists as an influencing force in community groups were cited as an
example of this.
Constraints
The overriding barriers to implementing commitments raised by key informants were:
(1) the highly centralized and politicized systems in which the bifurcation of
management and administration across the Directorate General of Health Services
(DGHS) and Directorate General Family Planning (DGFP) is seen to negatively
impact efficient implementation
(2) Slow release of funds (but not lack of them) on the part of Government, donors
and development partners alike, seen to be due to inefficiencies, bureaucracy and
over tight regulations. This is illustrated by the large amounts of unspent funds which
are detailed in the annual programme reviews for the health sector programme. For
example in the 2009 annual review, it was anticipated at the end of June 2009 that
about US$ 311 million would remain unspent to support HNPSP till June 2011.23
23
Bangladesh HNPSP Annual programme review, April-May 2009

21
(3) Lack of skilled staff and the unwillingness of medical staff to work in rural areas,
compounded by poor pay and service delivery constraints (e.g. lack of drugs in
public sector facilities), were bottlenecks referred to by many informants.
Human resources at every level of the health system fall either under the DGHS or
DGFP. The negative implications for the delivery of emergency services, such as
caesarean section with anaesthetists and obstetricians under different management
(DGHS and DGFP respectively), has been described earlier (above). The
constraints on effective working and low pay further cultivate the tendency for public
health service medical doctors to run parallel private practices. With their absence in
public facilities, usage of private practice also increases.
The human resource constraints are fully acknowledged in HPNSDP including issues of skills shortage and staff retention problems. In 2008-2009 the MOHFW started to prepare a comprehensive Reproductive Health Action Plan which addressed issues of promotion, transfers, in service training etc. Among other things this aimed to scale up training to increase levels of staff in various cadres and to provide incentives for those working in remote areas. However, the 2010 Aide Memoire for the Annual Programme Review suggested that, although some headway had been made in recruitment, the human resource information system and human resource strategy needed to be updated, and the lessons leant from pilot programmes involving incentives needed to be converted to action on the ground. UNFPA is currently commissioning an evaluation of Human Resources in Bangladesh which it anticipates will inform a new human resource strategy. Other documented and anecdotal evidence support the finding that many problems remain entrenched and are yet to be resolved.
Informants also highlighted other areas of the weak health system which they see as
having a major impact on the outcomes of programme activities namely – weak
governance, leadership or stewardship and management. Lack of capacity at
Government level has, however, been offset somewhat by their greater engagement
with NGOs whose programmes support capacity building. However, it does mean
that potential gains that could be made in service delivery, particularly in improving
quality and integration of care through commitments, are compromised by, and
possibly lost, due to unsupportive fragile health systems.
This in itself points to accountability issues. Annual reviews point to repeated
constraints but there is slow response to remedial action set out in action plans that
follow. This may also be the effect of a lack of common strategy. Though the health
plan sets out a clear set of objectives around a common goal and an unambiguous
strategic direction, the implementation details are absent. It is here at the strategic
level that harmonization is more fractured. Some respondents, although the
question was posed hypothetically by the reviewer, questioned whether this may in
part be due to the growing need of donors and stakeholders to show attribution of
results. JICA, as an example, sits outside the pooled fund for this reason.
d. Through which mechanisms is accountability for commitments to the
Global Strategy, and their impact on results and resources for women’s
and children’s health, addressed?

22
There is no separate or distinct accountability framework for commitments made to
the Global Strategy but as these commitments are embedded in country policy and
operational plans, they are accounted for through the SWAp evaluation mechanisms
in the form of Annual Programme Reviews (APR). These include the monitoring and
review of progress against indicators set in the strategy and its operational plans,
followed by a set of remedial actions in the form of recommendations and the
drawing up of action plans by which these recommendations are to be implemented.
There are however 32 operational plans which address each sub sector of the
Health Sector Programme, with seven distinct operational plans addressing
RMNCH. These seven operational plans have some natural overlap and are split
between two Government directorates. Weak collaboration between the two
directorates (attributed to the highly centralized and politicized system) combined
with the fragile health system, does lend itself to a slow and disjointed response on
remedial action plans.
Although 10 of the 11 core indicators for RMNCH recommended by the COIA are
already reflected in the evaluation framework of the Health Sector Strategy 2011-
2016, and are included in the DHS, the HDNSDP does identify an urgent need to
strengthen the monitoring capacities within the MOHFW and the directorates to
efficiently use the routine data for decision-making. It also states the need for “an
overall M&E strategy and work plan based on an assessment at all levels to guide
the improvement of the system especially the quality and capacity of the routine data
collection systems (development of registers, routine data collection forms, type and
frequency of reports) and to strengthen organizational capacity to conduct effective
M&E.”24
Not all funds are channelled through the SWAp. Multilaterals provide direct
programme funding to the Government or to specific activities. These activities must
be endorsed by Government and included in the operational plans. They are
therefore subject to the same processes of annual review against plans. Constraints
of this funding mechanism are that activities planned at district level with local
Government need to be endorsed by directorates at central level and included in
operational plans. This ‘delay’ caused by the re-routing through a central directorate,
whilst understandable, puts a severe constraint on responsive programming and
initiatives.
Disbursement of donor funds is based on quarterly Financial Management Reports
(FMRs), which include quarterly expenditures, and these are compared to the annual
budgets for the operational plans. The FMRs include revenue expenditure,
parallel/direct expenditure financed by non-pooling development partners thereby
ensuring a comprehensive picture covering all expenditures of the health sector25
(see annex 4, note on COIA recommendations).
One difficulty raised is that donors may face considerable additional workloads as
they ‘retrofit’ RMNCH programmes they are funding to align indicators for reporting
against COIA indicators which is a reporting requirement of their global office on
commitments made. An example is that a project may report on ‘Number of women
24
HPNSDP 2011 -2016 List of references 25
World Bank, Project Appraisal Document for HPNSDP, May 3, 2011

23
attending at least one antenatal care visit’, where in fact the COIA indicator is ‘four
ANC visits’.
A number of organizations make specific commitments to holding Government
accountable for results including, the H4+. The White Ribbon Alliance (WRA)
likewise has made its specific commitment to hold governments accountable to their
financial, policy and implementation commitments through 2015. WRA
commissioned an historical analysis study on “Allocation of Funds for Maternal
Health in Bangladesh”, published in January 2012 (Government allocations only).
This has been presented to the Government as an advocacy tool to hold
Government accountable for commitments made. WRA funded the Human Development Resource Centre in Dhaka to undertake a historical study to identify the allocation of the national budget to maternal health over the three years 2007-2009. The document is supplemented by a policy brief and has been used to hold the Government accountable for its commitments to the Global Strategy. The report holds important implications for funding requirements in order to achieve MDG 5. The study looked at financial allocation data available with the Budget Division, Ministry of Finance and Ministry of Planning. Findings estimated a total required allocation of US$ 88.1 million per year to address the unmet need for maternal health services to reach the MDG 5 target with improved quality of care, whilst to reach the ideal scenario with improved quality the estimate was US$ 117 million. The latter required a 4.69 times increase in the budget. Of the number of women to be covered by government maternal health services in 2009 (80% of the total), 3.2 million were served whilst the unmet need was 4.32 million. Over the three year period the revenue budget (government administrative costs) for maternal health was seen to be growing from 36% to 52%, whilst the development budget (programme costs) was reducing from 64% to 48%. The study also revealed that maternal health gets less priority in terms of public allocation and provision of services with the annual budget only 2.5% of the annual budget of the MoHFW.
e. What is the general knowledge of the Global Strategy and its goals, and
how does it fit with existing national or regional initiatives?
In Bangladesh there is no clear conflict between the goals of the Global Strategy and
existing national and regional initiatives. If anything it has been the next staging post
after the Millennium Summit that has drawn efforts together to ensure best practices
are upheld. Information gathered on this country study suggests that the greatest
impact of this is at the Government level. Line directors demonstrate a good
understanding of their own commitments and those interviewed have a clear vision
of how they will be taken forward.
Most key informants knew about the concept of the Global Strategy related to the
commitments made by their respective organizations but only a small minority
demonstrated any full understanding in terms of how the Global Strategy evolved,
the existence of the COIA, the 2011 progress report etc. The Global Strategy was,
according to one key informant, “commonly perceived as a UN strategy”, which may
make it more ‘remote’ to non-United Nations actors or those related to them.

24
Very few constituents were aware of the COIA recommendations made in 2011
including members of H4+. It was understood that dissemination is an ongoing
process through international workshops (one of which was mentioned by a United
Nations representative who will be attending). Another respondent had received
details of these specific COIA recommendations direct from their global office. Despite the lack of familiarity with COIA recommendations, five of these had already been recognized as important in the sector approach and had been partially or largely met (see Annex 4 for details). These five included: (1) 10 of the 11 key indicators recommended by the COIA for the purpose of monitoring progress towards the goals of the Global Strategy, nine of which were included in the DHS and results framework of the strategic health plan prior to 2010 and a tenth added in 2011 (see details in Annex 5). Much of this data is disaggregated for gender and other equity considerations. The missing indicator is that concerning antiretroviral prophylaxis among HIV positive pregnant women. It was not determined why though two respondents said this is still a highly sensitive issue. (2) In place of ‘country compacts’ recommended by COIA, existing agreements and contracts between country governments and all major development partners are held which require reporting on HPNSDP expenditures and programme related inputs. It is unlikely that those that do not share a formal relationship with Government concerning their commitments to the Global Strategy, i.e. businesses would welcome a country compact regarding reporting on them. They feel answerable to their own boards/shareholders. (3) National accountability mechanisms are in place in the form of annual programme reviews. (4) Transparency between stakeholders (donor, development partners, INGOs and CSO) is through various regular forum and task groups. However, this is to share project update and initiatives rather than progress against commitments to the Global Strategy. There is no formal way of reporting internationally. Organizations publish progress and results on their global websites but not specifically on commitments to the Global Strategy. (5) Vital events:
Bangladesh has come part way to establishing a system for registration of births and deaths (not yet robust). Its efforts towards establishing well-functioning health information systems that combine data from facilities, administrative sources and surveys will better enable the registration of vital events including causes of death by 2015, as recommended by the COIA.
Considerably more work needs to be done towards achieving other COIA
recommendations such as the Governments established capacity to regularly review
health spending (including spending on RMNCH) and to relate spending to
commitments, human rights, gender and other equity goals and results.
Others COIA indicators are not yet addressed or not fully understood (the latter
includes development partner’s agreement with OECD-DAC to improve the Creditor
Reporting System). Stakeholders remain to be fully briefed on the COIA
recommendations, only after which, further progress on these can be made.
f. What innovative solutions are used to sustainably, and at scale,
accelerate improvement of women’s and children’s health?
Bangladesh was seen by some informants as a country of innovation.
Communication technology is spreading rapidly and the use of mobile money

25
transfer has grown rapidly in the past six months. It is therefore not surprising that
some innovative practices have emerged from this base. While some of these
activities are in the process of being scaled up, others show very promising results
and are currently being reviewed or evaluated as to their envisioned potential for
scale up.
Management Information
As described above, the 2011-2016 sector plan states that the MOHFW’s current
M&E system is inadequate and the Monitoring and Evaluation Unit is not in a
position to function properly due to lack of resources and weak capacity. However,
Bangladesh has shown great progress in innovative planning to improve its health
information system. In September 2011 the country received the United Nations
“Digital Health for Digital Development” award for its outstanding contribution to
successfully using ICT for development of Health and Nutrition.
Some the elements of this include:
The planned use of a register of Family Welfare Assistants (FWAs) as a field-
based, robust data collection method by which FWAs record household
information. The forms are read and analysed by a central computerized software
system, already established at the MIS office. Once in full operation this is
expected to give detailed and rapidly obtained household level health data
results.
Telemedicine, which is functional in 10 union information and service centres
(owned by private providers who have a contract with Government of Bangladesh
to provide service – prescription print out etc). Telemedicine has been running in
one Upazila hospital since March 2010 for the referral and consultation of clinical
cases.
Ongoing work between the MoHFW and BRAC University, the Bureau of
Statistics and Ministry of Local Government on the measurement of vital events
through IT (MOVEIT). The latter are also working together with the Prime
Minister’s office on the harmonization of data.
Mobile phone messaging for improved maternal health outcomes MAMA Bangladesh – Aponjon:
This mobile messaging service (called Aponjon) for new mothers, pregnant women
and their families sends weekly messages timed to pregnancy stage/age of
newborn, on topics such as care during pregnancy, warning signs, breastfeeding
practices, nutrition, immunization reminders, connecting with local health services. It
includes a separate service for husbands, reinforcing messages sent to their wives.
Currently at the end of its pilot phase in 13 locations, the initiative has strong support
from the Prime Minister’s Office and the Ministry of Health, and is due to be
launched nationally in 2012. This is the first country project of the Mobile Alliance for
Maternal Action (MAMA), a public-private coalition founded by USAID and Johnson
& Johnson, and other supporting partners. MaMoni (Save the Children), Smiling Sun
Franchise Program (SSFP) and Infolady (D.Net) are outreach partners. BRAC is
also actively supporting the pilot through its community health workers. For
26
sustaining the initiative corporate sponsors are being mobilized through cash and in-
kind contributions including technical assistance, access to distribution and
promotional channels, technology inputs, and branding expertise. Johnson &
Johnson are responding to their commitment to the Global Strategy to “provide more
than 15 million expectant and new mothers in Bangladesh, and five other countries
with free mobile phone messages on prenatal health, reminders of clinic
appointments and calls from health mentors over the five-year program”.
Mobile phones for improving referral outcomes:
BRAC (DFID/AusAID funding) have introduced mobile phones for use by dedicated staff in each health facility of 10 districts. Through this system in-coming calls are received regarding the transfer of referrals from community health staff so that the facility can prepare for the emergency. In parallel with this BRAC has also created referral hubs where they have worked with local transport owners to establish patient pick up points, which facilitate transfers, thereby helping reduce the second delay. Community mobilization to address services providing the continuum of care
These projects are seen to have a significant role to play in better health seeking
behaviour and may account in part for the increase in facility deliveries from 9% to
23% from 2001-2010. They focus on community mobilization and formation of
community groups with engagement at facility level.
The MaMoni project, funded by USAID, is a partnership of several organizations
working with the Government of Bangladesh and is an integrated package of
services (maternal-newborn-family planning-nutrition package). Its activities
place community action groups (CAG) at the heart of the rural health services.
NGO workers liaise with front line health workers to raise awareness and identify
and address health issues with their own resources.
JICA works closely with Government through its partner NGO, CARE, to
strengthen government capacity building through district level coordination
mechanisms. This is conducted through monthly meetings for information sharing
across all facilities and engages local government at Union level. Contributions
are made from union budgets to support services, including community driven
initiatives. The project creates a strong interface between the community and
health facilities at Upazila level in order to promote accountability for results. Demand side financing – impact of voucher scheme on facility births and equity
The Government of Bangladesh has run a successful voucher scheme initiative for pregnant women which provides incentives for facility births – the Demand Side Financing (DSF) programme. DSF eligible women receive: three ANC check-ups; safe delivery care in a health facility or at home with a skilled birth attendant; emergency care for obstetric complications, including caesarean sections; one PNC check-up within six weeks of delivery; cash incentives to cover routine and emergency transport, some food and medicine costs for the family; and a small gifts box. The programme also provides incentives to health care providers to identify eligible women and provide maternal health services.

27
An evaluation found DFS to be strongly and significantly associated with higher rates
of skilled birth attendance (with the likelihood of skilled birth attendance more than
twice as high in intervention areas). The voucher scheme was also strongly and
significantly associated with higher rates of institutional deliveries and PNC visits,
and resulted in significantly higher likelihood of home deliveries being attended by a
qualified provider.26 Another study also evidenced much stronger demand-increasing
effects on the poor. Poor voucher recipients were 4.3 times more likely to deliver in a
health facility and two times more likely to use skilled health personnel at delivery
than the non-poor recipients. Contrary to the inverse equity hypothesis, the voucher
scheme reduced inequality even in the short run.27
United Nations initiative on identification of bottlenecks – Tanahashi model
Scaling up UNICEF supported the Government of Bangladesh in piloting a system of
evaluating bottlenecks on the availability and accessibility of care based on the
Tanahashi model (Marginal Budgeting for Bottlenecks – MBB). The results from
three districts were used for local level Government planning of services. Based on
the positive outcome, UNICEF are currently evaluating its impact on capacity
building at district level with the intent of scaling it up if the results are positive (as is
expected from anecdotal information).
Cost of violence against women (COVAW)
This innovative approach aims to tackle a gender issue and raise awareness of
domestic violence (including early marriage) in rural situations by demonstrating its
financial cost – which individuals and communities can relate to, and government
use for policy decisions. The initiative by CARE Bangladesh, funded by USAID,
targeted 40 000 participants in 24 communities, and estimated that an indicative
14 084.56 Tk, almost equivalent to 2.05% GDP, is spent at individual level annually
because of violence against women.
Advocating with Government to maintain momentum on commitments made
The White Ribbon Alliance (WRA) considers maternal health to have much broader
ramifications beyond health care, for example on human rights. A key focus is to
engage parliamentarians to ensure they know the reality for women in their
constituency, and can play a role in gaining commitments and deliver results.
Various media are used as means of strengthening social accountability. Recent
activities include:
Through WRA, Parliament member Mr Abul Hasan Mohammad Ali declared his
contribution to 52 community clinic renovations from local government funds to
ensure ANC, PNC and access of rural women and children at community clinics,
and pledged contributions to 21 Union health and family welfare centres in
26
Hatt, L. Et al (2010) Economic Evaluation of Demand-Side Financing (DSF) for Maternal Health in Bangladesh
[Draft]. Abt Associates Inc. The evaluation covered the 2007/09 period in 21 Upazilas, of which nine had universal
eligibility for vouchers (i.e. including the non-poor), and 12 had means-tested eligibility. 27
Ahmed, S., Khan, M. (2011) Is demand-side financing equity enhancing? Lessons from a maternal health voucher scheme in Bangladesh, Social Science & Medicine V 72, Issue 10, 1704-1710.

28
Khanshama and Chirirbandor sub-districts. He also advised government duty
bearers to accompany and cooperate with NGO service providers.28
WRA used a range of media (e.g. blogs, video, Twitter and Facebook) to report
from the 126th Inter-Parliamentary Union (IPU) Assembly in Kampala, Uganda,
on progress of a resolution on maternal and child health rights.29 Hon. Fazilatan
Nessa Indira MP and Hon. Saber Hossain Chowdhury MP, who joined over 600
parliamentarians at the IPU, appeared in a widely disseminated video interview
from IPU which was also relayed by global news media (The Huffington Post).
(March 2012)
The WRA collaborated with the Journalism Training & Research Initiative (JATRI)
in organising a workshop on “Public Sector Accountability for the fulfilment of
Maternal Health Commitments” at the 2012 JATRI conference. (April 2012)
Reducing maternal and neonatal mortality and morbidity, with emphasis on equity issues
The Accelerating Progress towards Maternal and Neonatal Mortality and Morbidity Reduction is a five-year project implemented by the Government, UNFPA, UNICEF and WHO in four districts. The purpose of the project (started in 2007) is to improve community MNH practices and the utilization of quality MNH services, particularly among the poor and the vulnerable. Early signs of impact included a 5% increase in the number of women with access to skilled professional help during delivery, and a 4% increase in the number of complicated deliveries that receive professional support.30 UNICEF reported that this project is to be scaled up in a total of 20 of the poorest districts.
28
February 2012. 29
“Access to Health as a Basic Right: The Role of Parliaments in Addressing Key Challenges to Securing the Health of Women and Children”. 30
Reported in: DFID in 2009-2010 (2011).

29
5. Conclusions The Global Strategy for Women’s and Children’s Health has been a factor in driving
and harmonizing policy by aligning around the commitments made to Bangladesh at
the 65th General Assembly of the United Nations in 2010. In has focused attention of
all stakeholders on the necessity to come together and drive the commitments in an
effort to accelerate progress to meeting MDGs 4 and 5. The leadership taken on this
by the Prime Minister has “mobilized the Government machinery” behind the
commitments and set out a clear pathway.
The greatest testimony to the value of the Global Strategy is that the commitments
are clearly set out in the new Government Policy and Strategic plans and their
associated operational plans. In the foreword to the Strategic Plan for Health,
Population and Nutrition Sector Development Programme (HPNSDP) 2011-2016,
the Health Minister sets out these commitments clearly. The Minister further states
that the plan:
“Reflects the direction and determination of the Government’s commitment to
serve the people with their needs in health, population and nutrition services, as
stated by the Honorable Prime Minister while addressing the 65 th General
Assembly of the UN on progress in attaining the MDGs”.
The information gained from this country study concludes that there was a clear
process in which commitments were formulated and finalized. This included
advocacy and awareness raising around evidence-based practice which guided
strategic direction and planning.
The development frameworks of government, bilateral and multilateral agencies
alike take account of commitments made. Donors considered how best to support
the country plan and reflected it in their own plans. Evidence gathered from
interviews with key informants during this country study suggests that, prior to the
launch of the Global Strategy, the visibility and support given by the Government on
its RMNCH plans and priorities was not high.
Since making the commitments this is reversed and progress is considered to be
rapid. A good example of this is the momentum behind midwifery training.
The constraints to implementing commitments are mainly systemic. These include:
weaknesses in health systems, principally human resource constraints; a lack of
government capacity compounded by weak stewardship, leadership and governance
within a highly centralized and politicized system. This is partly mitigated by the
increased value given by the Government to the role that NGOs can play in
supporting their programme. The slow release of funds both by Government as well
as donors and multilaterals thereby creating bottlenecks has further constrained
implementation.
Overall the accountability for commitments appears robust given that the mechanism
is a well-established part of the SWAp review process. The various levels of
coordination help ensure an aligned approach. The reviewer is left with the concern

30
that whilst harmonization at policy level is strong, this becomes somewhat
fragmented at strategic level. The updating of the Maternal Strategic Health Plan
may also help define a common, robust and detailed strategy for implementation of
commitments across the continuum of care.
The recommendations made by the Commission for Information and Accountability
are not well disseminated in the country but the reviewer understood that this is
continuing through a series of international workshops to which stakeholders are
invited. Some of these recommendations have, in conceptual terms, already been
implemented (see annex 4) as they are recognized as a necessary part of
implementation.
The Global Strategy for Women’s and Children’s Health is often only known by name
and not well understood in detail by country stakeholders. Knowledge is strongest
among Government and donors. However the ‘commitments’ are well understood by
all constituents and the responsibility in meeting them is felt by all.

31
6. Summary of recommendations:
The PMNCH 2011 report and the COIA document ‘Keeping Promises, Measuring Results’ (May 2011) should be circulated to donors and stakeholders who have cited Bangladesh as a key recipient for commitments made. This will strengthen the global, regional, and country knowledge on processes – providing a two way exchange on constraints and lesson learning.
COIA to engage with global offices of constituents on a regular basis (be these donor, INGO, private companies) to liaise with them and monitor the dissemination and receipt of information to and from global/regional and country offices regarding commitments to the Global Strategy. COIA and PMNCH can assist with gaps in information. This aims to reduce the stated country office ‘disconnect’ from regional/global level regarding Global Strategy commitments made.
Likewise PMNCH should make recommendations to stakeholders as to the alignment of indicators in existing projects where these may differ from those of the COIA. This is to mitigate the large amount of work generated by the need to report to global offices on these 11 core indicators.
Maximum efforts should be made to promote the Global Strategy and keep up the momentum. Bangladesh provides a good example of a country that is fully engaged in its commitments but it will be important to keep this in the headlines over the next five years.
It is relatively early to look at the outcomes and results of the commitments made. There may be added value in repeating the case studies in 2013 moving from a rapid assessment to more in depth field studies. This would allow for richer illustration of innovative solutions and impact on beneficiaries. This may increase the understanding of PMNCH as to how it can enhance support at country level.

32
Annex 1: Research questions and methods
The case study in Bangladesh was carried out on 2-9 May 2012. Preparatory work
took place over a period of two weeks prior to this,
Semi-structured interviews were carried out with key informants (annex 1).
Representatives from all seven constituents which had made commitments to the
Global Strategy for Women’s and Children’s Health (Government; donors;
multilateral organizations; NGOs; health-care professional association; research and
training institute; and the private sector) were interviewed. This covered a total of 22
agencies (seven of which were government divisions). Although the government
and donor representation was high, this helped establish better (1) how well the
commitments were understood, given the complex structure and bifurcation of the
system, and (2) the engagement of donors with Government on issues such as
harmonization and alignment which is carried through to the programmes they fund.
Seven interviews were attended by two or more representatives from that
organization.
Key informants were sent the semi-structured questionnaire ahead of the interview
so that they were aware of the structure and range of questions. Not all had time to
look at it but some commented that they found this helpful. They were also sent a
copy of a confidentiality agreement which was to state that they understood the
intent of the interview. The nature of the study was described to the informants.
Time allocation was 30-40 minutes, although some lasted longer (when the
informant agreed to continue).
The semi-structured question guide addressed the key research questions (see
overall introduction). Initial interviews however showed that this was too long and the
constant reference to ‘commitments’ was not useful. Most key informants were
aware of the commitments and said that what they implemented was in line with
what was stated in the commitment (generally made by their global office).
The semi-structured nature of interviews led to informants placing different emphasis
on aspects of implementing commitments. Donors tended to speak more on
coordination mechanisms and barriers to implementation while those directly
implementing activities also spoke on barriers, activities and innovation. In addition,
a separate tool was used to check ‘Progress on implementation of COIA
recommendations’. Some points applied to all but mainly this was asked of donors
and government.
Constituents were requested to supply supporting documentation (reports, briefings)
where seen useful to illustrate innovation or to provide data. Many said they would
forward soft copies after the interview but, despite email reminders, little was
received (with the exception of WHO and WRA).
Field visits were not conducted due to time constraints and the long travel time to
reach what were considered to be the most illustrative projects where innovation at
community level could have been observed.

33
Limitations and Constraints
The short time frame for this country study was the biggest constraint. This included
the lead in time to the country visit which in itself was determined by the deadline for
the report. Not enough information was available prior to the country visit on the
contacts for the constituents. Although WHO was helpful in furnishing names, all
contact information has to be tracked by the national consultant and appointments
made by him. This was very time consuming and demanded more time that that
allocated.
It took considerable time to access the relevant Government documents and many of these were not available until the case study was underway in country. Having these documents earlier would have assisted in the preparation prior to the first interviews. With travel in Dhaka alone being very time consuming, a choice was made to use the 5.5 days solely for interviews, rather than adding in a field visit out of the city. It had originally been proposed that the visit end with a workshop to give feedback and to verify and agree all findings with key informants. However, a decision was taken to limit this to WHO (as the host organization for this study), given the travel time required by other respondents

34
Annex 2: List of Key Informants
Person Position Organization
1
Dr Long Chhun
Dr Rabeya Khatun
Dr Tekendra Karki
Chief Representative
National Professional Officer –MNCAH
Medical Officer (MNCAH)
WHO
2 Dr Shehlina Ahmed Health and Population Advisor DFID
3 Dr Abu Jamil Faisel Project Director/Country Representative
Engender Health
4 Prof. Abul Kalam Azad
ADG-DGHS & Line Director of MIS DGHS
5 Mr David Hasanat Chairman Viyellatex Group Bangladesh
6 Mr Jan Borg Health Advisor Australia AID
7 Md. Ashraf Hossain Director General Ministry of Women and Children Affairs
8 Dr Ashraful Islam Additional Secretary Admin MOHFW
9 Dr Muhiuddin Osmani
Deputy Chief Health Planning Wing, MOHFW
10 Dr Jahangir Hossain
Dr Md. A. Islam
Programme Director- Health
Team Leader MNCH
CARE Bangladesh
11
Dr Bushra Binte Alam
Karar Zunaid Ahsan
Senior Health Specialist
Research Analyst World Bank
12 Dr Ishtiak Mannan Chief of Party Save the Children
13 Ms Peggy Thorpe &
Dr Momena Khatun
First Secretary Development
Health Advisor
High Commission of Canada
(CIDA )
14 Ms Taslima Begum Director Nursing Directorate
15 Dr Syed Abu Jafar Md. Musa
Director Primary Health Care &
Line Director, MNCH DGHS
16 Dr Shams El-Arifeen
Head Child and Adolescent Health Unit
ICDDR,B
17 Dr Lianne Kuppens
Dr Ziaul Matin
Chief Health Sector
Health Officer ( neonatal health) Unicef
18 Hashina Begum Assistant Representative, RH UNFPA
35
19 Mr Takashi Senda
Shoko Sato
Programme Advisor Health
Health Advisor JICA
20 Dr Md. Azizul Alim
Deputy Programme Manager (EOC) Reproductive Health Programme
DGHS
21 Dr Kawsar Afsana Director Health BRAC Health
22 Dr Farhana Ahmad National Coordinator White Ribbon Alliance, Bangladesh

36
Annex 3: List of Commitments
Constituent Stated Commitment Country office response
Government of Bangladesh
Doubling the percentage of births attended by a skilled health worker by 2015 (from the current level of 24.4%) through training an additional 3000 midwives; Staffing all 427 sub-district health centres to provide round-the-clock midwifery services; Upgrading all 59 district hospitals and 70 Mother and Child Welfare Centres as centres of excellence for emergency obstetric care services; Reduce the rate of adolescent pregnancies through social mobilization; Implement the minimum legal age for marriage; Upgrade one third of MNCH centres to provide adolescent friendly sexual and reproductive health services; Halve the unmet need for family planning (from the current level of 18%) by 2015; Ensure universal implementation of the Integrated Management of Childhood Illness Programme.
DFID
It is anticipated that UK aid will save the lives of at least 50,000 women in pregnancy and childbirth, a quarter of a million newborn babies and enable 10 million couples to access modern methods of family planning over the next five years. To achieve this ambitious goal, the UK will double its annual support for Maternal, Newborn and Child Health by 2012, and sustain that level to 2015.
Support to HPNSDP with focus on :
RMNCH – Family planning and prevention of early marriage
H4 +
WHO, UNFPA, UNICEF, UNAIDS and the World Bank commit to mobilize political support for the Global Strategy in the 49 ’Lowest Income Countries’; increasing the speed of the downward trend in maternal and child mortality by strengthening country and regional technical capacity to implement commitments; advocating for equity-focused approaches that include universal access to an integrated essential package of health services for women and children; and to addressing the root causes of ill-health, in particular gender inequality. They further commit to promoting the critical engagement of other sectors such as education, gender, nutrition, water and sanitation, culture and human rights; strengthening ongoing inter-agency collaboration in order to optimize the advocacy for increased and sustained financial resources, as well as linking additional global resources to evidence-based country-driven interventions; and sustaining the momentum of the Global Strategy beyond 2015. See WHO, UNFPA, UNICEF, UNAIDS and the World Bank
WHO As H4+ above

37
Constituent Stated Commitment Country office response
Support to HPNSDP/Government commitments
Focal area: IMNCI, Midwifery, Adolescents and Youth friendly services
UNFPA
As H4 above
Support to HPNSDP/Government commitments
Focal area: Community SBAs and Midwifery
UNICEF
As H4 above
Support to HPNSDP/Government commitments
Focal area: MNCH Supply side
World Bank
As H4 above
Support to HPNSDP/Government commitments
Health systems
Nutrition
AusAID
Australia will invest around US$1.5 billion (A$1.6 billion) over the five years to 2015 on interventions evidence shows will improve maternal and child health outcomes. These will include expanding access to family planning and vaccination services, and funding skilled health workers (including midwives), health facilities and supplies. Australia’s strong focus on. South Asia and effectively performing international organizations will also continue. [on current projections subject to annual budget processes]
Support of MNCH projects that address Service Delivery : Supply and demand side;
JICA
Japan will support the Global Strategy by implementing and advocating a package model by the name of “EMBRACE”, which intends to ensure the continuum of care from pregnancy to post natal stage. Japan also reaffirms its financial commitment made at the G8 Muskoka Summit to provide up to an additional $500 million for maternal, newborn and child health in five years from 2011 will be fulfilled as part of today’s $5 billion commitment.
Implementation and advocating EMBRACE model in close partnership with Government addressing the continuum of care

38
Constituent Stated Commitment Country office response
Canada-CIDA
Canada will provide C$2.85 billion for MNCH by 2015. Canada will focus its efforts on improving the services and care needed to ensure healthy pregnancies and safe delivery, and placing a particular emphasis on meeting the nutritional needs of pregnant women, mothers, newborns and young children. Canada will work to increase access to the high-impact, cost-effective interventions that address the leading killers of children under the age of five. Canada will also commit an additional $540 million over three years to the Global Fund to Fight AIDS, Tuberculosis and Malaria. This is in addition to a total of $978.4 million that Canada has committed and disbursed to the Global Fund since 2002.
Support a portfolio of projects
EmOC
Community skilled birth attendants
IMNCI
Health systems: transport; essential drugs; MNCH service delivery; human resources.
Integrated district-level services
CARE
CARE commits $1.8 billion over the next 5 years to expand successful maternal, newborn and child health programs, with a focus on empowering girls and women to increase gender equity, linking health systems and communities in systems of mutual accountability, and using innovative approaches to reach the most vulnerable populations. By scaling-up programs in countries where it currently operates, CARE aims to aid more than 30 million women of reproductive age by the 2015 Millennium Development Goals deadline.
The new CEO of CARE, Dr Helene Gayle, further renewed CARE’s commitment to MH under the caption “Mothers Matter”
Women’s Empowerment (gender, relationships, etc.)
Responsive Health System
Mobilizing Political Commitment
Community skilled birth attendants
Reduce adolescent pregnancy
Promote minimal age for marriage
Prioritize geographically and socially disadvantaged
Neonatal health
Nutrition
Community support system and organizing for referral
Service gaps supply side
Save the Children
Save the Children commits up to $500 million per year for the next 5 years (including $150 million contributed by private individuals) to: promote policy changes that accelerate progress on MDG4; expand and intensify efforts to integrate
Activities align with global commitment. Focus on:
Training health providers – helping babies breathe

39
Constituent Stated Commitment Country office response
proven technology into health systems to protect newborns in 12 priority countries; train 400,000 health workers; mobilize civil society to hold governments accountable; engage with multi-sector partners to help deliver life-saving programming. Save the Children is also committed to advocating for equity in all health and nutrition programmes to ensure that disproportionate levels of mortality in poor and marginalized groups are no longer tolerated.
Health systems strengthening
Mobilizing local resources and increase community awareness of health. These activities have been linked to the sector programme.
White Ribbon Alliance
White Ribbon Alliance for Safe Motherhood and its members in 148 countries commit to the Global Strategy by engaging local, national, regional, and global organizations and individuals to ensure MNCH is a priority issue for all governments and hold governments accountable to their financial, policy, and implementation commitments through 2015.
As stated :
Advocacy
Accountability
Social mobilization and social awareness
EngenderHealth
Support to Government commitments
Long-term maternal morbidity (fistula),
Linking up EmOC and FP for prevention of fistula
Prevention of maternal mortality due to PPH at the community and facility
Family planning with a focus on long acting (IUD and implant) and permanent methods (tubectomy and NSV)
Postpartum Family Planning.
Addressing reproductive health needs of young married couples.
BRAC
BRAC commits to raise USD 262 million over the next five years in support of programs and projects in Bangladesh and eight other countries: Afghanistan, Pakistan, Uganda, Sierra Leone, South Sudan, Liberia, Tanzania, and Haiti.
Community Skilled birth attendants
Community support groups
Health systems – particularly referral
Viyellatex Group * Bangladesh
The Viyellatex Group has committed to Every Woman Every Child to provide free medical services, including eye care, immunization, and clinical services to 3500 mothers and 1500 children in Bangladesh by 2015, to

40
Constituent Stated Commitment Country office response
provide free ultrasonograms and medicines to 3500 pregnant women, and to start a school for the physically challenged and underprivileged children by July 2012.
ICDDR,B
Research Institute No statement made
Support to Government commitments
Research Institute
Adolescent health
Child health – (diarrhoea in particular)

41
Annex 4: Progress against the COIA’s 10 recommendations
Progress against the COIA’s 10 recommendations for accountability at country level (6 to be achieved by 2012)
To be achieved by 2012
Source used
Progress Other comment (note what steps
have been taken so far if partly complete or any barriers /challenges etc)
Health indicators (see tool 2, annex 5)
11 key indicators for RMNCH, disaggregated for gender and other equity considerations, are being used for the purpose of monitoring progress towards the goals of the Global Strategy.
DHS,
HPNSDP
UNICEF
DFID
Good progress
10 indicators are included in the DHS and results framework of the strategic health plan. All were included prior to 2010 except children 0-59 months with pneumonia receiving antibiotics which was added in 2011.
Antiretroviral prophylaxis among HIV pregnant women is not included.
Country compacts
In order to facilitate resource tracking, “compacts” between country governments and all major development partners are in place that require reporting, based on a format to be agreed in each country, on externally funded expenditures and predictable commitments.
Key informants
Not started (documented discussion but no action)
Other agreements exist and therefore country compact seen by some as unnecessary. Those that do exist include :
Multi-Donor Trust Fund - Formal agreement between the World Bank and Government (the MDTF is administered by the WB) and agreement between WB and other donor partners.
Country cooperation plans endorsed by Government, with project activities then included in bi-annual plan.
Projects endorsed by Government are included in operational plans. If not endorsed therefore, not included in the plan, resulting in considerable delays.
Contracts between donors and their respective implementers.
National oversight: By 2012, all countries have established national accountability mechanisms that are transparent, that are inclusive of all stakeholders, and that recommend remedial action, as required.
Key informants
Good progress
National accountability is through the Annual Programme Review (APR) Mechanism of the Sector Wide Approach which is the tracking and monitoring process for the health sector programme. Activities in RMNCH will be tracked through their respective operational plans which relate to the sector plan. APR carried out with stakeholder consultation including Government, development partners, CSOs, Academia etc. The process includes monitoring, review and remedial action. Remedial action takes the form of recommendations

42
To be achieved by 2012
Source used
Progress Other comment (note what steps
have been taken so far if partly complete or any barriers /challenges etc)
translated into action plans. Action plans are designed by Government and development partners.
Reporting aid for women’s and children’s health: By 2012, development partners request the OECD-DAC to agree on how to improve the Creditor Reporting System so that it can capture, in a timely manner, all reproductive, maternal, newborn and child health spending by development partners. In the interim, development partners and the
OECD implements a simple method for reporting such expenditure.
WHO
WB
Not started
Not recognized by constituents
Global oversight: Starting in 2012 and ending in 2015, an independent
‘‘Expert Review Group’’ is reporting regularly to the United Nations Secretary-General on the results and resources related to the Global Strategy and on progress in implementing this Commission’s recommendations.
Good progress
Externally established
To be achieved by 2013
Transparency: By 2013, all stakeholders are publicly sharing information on commitments, resources provided and results achieved annually, at both national and international levels.
Key
informants
Information is shared on HPNSDP in :
11 thematic task groups (all stakeholders involved)
Health consortium in which donors meet Government once a month.
Local consultative group (LCG) on health co chaired by the Senior Secretary, MOHFW, and representative of development partners – currently from DFID.
Internationally information sharing is agencies own head offices and publishing on web site

43
To be achieved by 2013
To be achieved by 2015
Vital events: By 2015, all countries have taken significant steps to establish a system for registration of births, deaths and causes of death, and have well functioning health information systems that combine data from facilities, administrative sources and surveys.
Director MIS
United Nations
Good progress
Birth certification is an established regulation and children cannot attend school without a birth certificate. However it is not enforced and coverage is variable in rural areas
Deaths are certified and registered at burial but the mechanism for record keeping is local and information is not collated.
Note: Countdown reports only 10% coverage in 2006. This is not updated by countdown
Innovation: By 2015, all countries have integrated the use of Information
and Communication Technologies in their national health information systems and health infrastructure.
Director MIS
United Nations
Underway
Some
elements in place
The planning for a digital data system is complete and the intention is that this is fully incorporated into MIS for robust community/facility data reporting. It is partially operational
Resources tracking: By 2015 country is tracking and reporting, at a minimum, two aggregate resources indicators: Total health expenditure by financing source, per capita; and total reproductive, maternal, newborn and child health expenditure by financing source, per capita.
WB :
National health accounts MOHFW contact
Health economics unit
Not started (documented discussion but no action)
Once Health Economics Unit produced the next round of National Health Accounts (2014), HEU will try to produce sub accounts and RMNCH will be one of them as a priority area.
Recently, Institutional of Health Policy Sri Lanka (Data International conducted the surveys) in collaboration with HEU with funding from ADB and AusAID conducted public health facility survey and exit survey of patients to estimate government spending on MNCH, cost of MNCH services at the facility level, OOP on MNCH services (used HIES data) etc. This study used NHA data as well. Hence, in the next NHA the unit cost data will be useful for estimating RMNCH spending by the government. Bangladesh will participate in the WHO training on tracking RMNCH expenditures.
By 2015 Governments have the capacity to regularly review health spending (including spending on RMNCH) and to relate spending to commitments, human rights, gender and other equity goals and results.
As above
Not started (documented discussion but no action)
By 2015 government will have the capacity to regularly review health spending (including spending on RMNCH) and to relate spending commitments, human rights, gender and other equity goals and results.
Public expenditure review will do gender analysis regularly.

44
Annex 5: Checklist for COIA Recommendations Indicators which have been integrated into national surveys / DHS / MICS and HPNSDP
Global strategy Indicators (11)
Included Yes / No
Date included (i.e. Pre
/post 2010)
Disaggregated by gender / other equity considerations
Comment
Which data collection system/survey has the indicator been added to?
What is the verification used on the indicator?
Maternal mortality ratio Yes Pre 2010 BDHS / HPNSDP
Under-5 child mortality with proportion of newborn deaths
Yes Pre 2010
Wealth Quin only
Not gender
DHS / MIS
Children under 5 which are stunted
Yes Pre 2010 Gender and Wealth Quin
BDHS / HPNSDP
COIA Indicators (8)
Proportion of demand for family planning satisfied
Yes Pre 2010 Age
Wealth Quin
Met need
BDHS / HPNSDP
Antenatal care coverage (At least four times in pregnancy )
Yes Pre 2010 Wealth Quin
Urban / Rural
Not found, not in Operational plans.
Anecdotal comment : highly sensitive issue especially for pregnant women. Considered low prevalence overall therefore not fully acknowledged by Government.
Antiretroviral prophylaxis among HIV positive pregnant women
NO X BDHS / HPNSDP
% of live births attended by Skilled birth attendant
Yes Pre 2010 Wealth Quin
Urban / Rural
BDHS / HPNSDP
Postnatal care for mothers and babies (% that receive care within two days of birth)
Yes Pre 2010 Wealth Quin
Urban / Rural
BDHS / HPNSDP
% of infants 0-5 months exclusively breastfed
Yes Pre 2010 X BDHS / HPNSDP
3 doses of DPT (% of children 12-23 months receiving)
Yes Pre 2010
Gender
Wealth Quin
Urban / Rural
DHS Penta Vaccine
% children 0-59 months with suspected pneumonia receiving antibiotics
Yes 2011
DHS

45
Annex 6: Semi-structured Questionnaire (later modified)
Name of Constituent: Name of Key informant:
The Government priority commitments to the Global Strategy and their priority interventions as set out in the national plan are set out below. Please tick in the boxes on the right which of your / the constituents key RMNCH Activity align with these.
Government commitments to the Global Strategy for Women’s and Children’s health are :
(Bangladesh)
Our key commitments/ activities align with (please tick)
1 Doubling the % of births attended by SBA through training of 3000 midwives
2 Staffing 427 sub district health centres to provide round the clock midwifery
3 Upgrading 59 district hospitals and 70 MNCH welfare centres as centres of excellence in EMOC
4 Reduce rate of Adolescent pregnancies through social mobilization
5 Implement the minimal age for marriage
6 Upgrade one third of MNCH centres to provide adolescent friendly SRH services
7 Half the unmet need for family planning by 2015
8 Ensure universal implementation of IMNC programme.
The Government Priority strategies for RMNCH as reflected in the Strategic plan ( aligned to above)
Alignment (tick)
1 Increasing number of skilled birth attendants
2 Increasing facility based 24hr /7 days service from management of maternal complications
3 Emphasize Long acting permanent methods (LAPM) and unmet needs of family planning
MNCH Elements in HNSDP which add value to HNPSP
4 *Emphasizing MNCH services in the urban slums through separate OP
5 *Prioritizing areas of high maternal mortality , geographically and socially disadvantaged
6 *Women friendly services at the Community clinics and domiciliary level and by NGOs

46
Please give your priority RMNCH commitments and please state why these are priorities for you
Activity Reasons prioritized by you
Partners
Activity Reasons prioritized by you
Partners
7 *Sharing of expertise and facilities between DGHS and DGFP for MNH services
8 *Strengthening sick newborn services including home visits by a trained worker within two days of birth
9 *Rapid and effective referral systems for sick newborns
10 *Mainstream nutrition within the DGHS and DGFP services ( Director General Health Service) **
11 Expanding access and quality of MNCH services
12 Scaling up of Nutrition services to all areas with priority for remote and poor areas in collaboration with the Min. of Local Government, rural development and cooperatives for urban areas.
13 Revitalize various family planning interventions to attain replacement level fertility
14 *Some priorities - Legal framework, mainstreaming gender, equity and voice in the core programmes such as MNCH and nutrition.
1 Strengthening the support systems by increasing the health workforce at Upazila, Union and Community clinic (CC) level
2 Strengthen health systems
3 Strengthening preventative approaches as well as control of CDC’s and NCD’s at all levels
4 Improving MIS with ICT and establishing M&E systems
5 Increasing coverage and quality of services by strengthening intra- and intersectoral and private sector coordination
6 Pursue priority institutional and policy reforms, such as decentralization and Local level planning (LLP), incentives for service providers in hard to reach areas. PPP etc
7 Strengthened collaboration with MOSW, MOCHTA (Chittigong Hill Tracts Affairs) and CHT board, the NGO and private sector to address difficult to reach population

47
Activity Reasons prioritized by you
Partners
Taking 2 commitments ( one which you consider which you consider is high on the agenda and progressing well, and one that is traditionally neglected and faces more constraints) and briefly discuss the process by which these were implemented :
Commitment 1
Reason for selection of this commitment/programme/activity Planning process (harmonized/aligned/coordinated?) Main barriers (acceptability to Government, implementation … ) M&E – accountability framework Successes: lessons to share with other countries Commitment 2 Reason for selection of this commitment/programme/activity Planning process (harmonized/aligned/coordinated ?) Main barriers ( acceptability to Government, implementation … ) M&E – accountability framework Successes: lessons to share with other countries
Please ask all of these key questions, not already covered in the above.
48
1. Is there a transparent accountability mechanisms for commitments in place? Is this inclusive of all
stakeholders and does it include monitoring, review and remedial action? How is this linked to the government bodies? Who oversees this? (Do not ask if clearly covered in first section)
2. What are the main successes or bottlenecks you identify in implementing the commitments to date and what factors influence this? (Do not ask if clearly covered in first section) What lessons would you share with other countries on overcoming barriers?
3. Can you give examples of any successful innovative solutions to accelerating that have been used
to reach beneficiaries as a result of commitments? Have these been integrated into longer term plans with specific funding?
4. Have you signed a country compact with Government? - If yes when? 5. What in your opinion is the greatest value that the Global Strategy and commitments have added
to national policies, investments and service delivery at country level ? 6. Can you say which key global and national events you think have done most to accelerate efforts in
achieving MDG 4 and 5? ( show timeline as prompt) Please add here any additional question for this key informant from Tool 2 . (Progress against COIA recommendations) What is the organization’s long term strategy for maintaining the impact of their commitment?

49
This document is issued for the party which
commissioned it and for specific purposes connected
with the above-captioned project only. It should not be
relied upon by any other party or used for any other
purpose.
We accept no responsibility for the consequences of
this document being relied upon by any other party, or
being used for any other purpose, or containing any
error or omission which is due to an error or omission in
data supplied to us by other parties.
This document contains confidential information and
proprietary intellectual property. It should not be shown
to other parties without consent from us and from the
party which commissioned it.
HLSP, 10 Fleet Place, London EC4M 7RB, United Kingdom T +44 (0)20 7651 0302 F +44 (0)20 7651 0310, W www.hlsp.org