project report on acl
DESCRIPTION
PROJECT REPORT ON ACL INJURIESBY : PIYUSHINTRODUCTIONThe anterior cruciate ligament (ACL) is one of the most important of four strong ligaments connecting the bones of the knee joint. It is often injured. Ligaments are strong, dense structures made of connective tissue that stabilize a joint. They connect bone to bone across the joint.A tear to the anterior cruciate ligament (ACL) results from overstretching of this ligament within the knee. It's usually due to a sudden stoTRANSCRIPT
PROJECT REPORT ON ACL
INJURIES
BY :
PIYUSH
INTRODUCTION
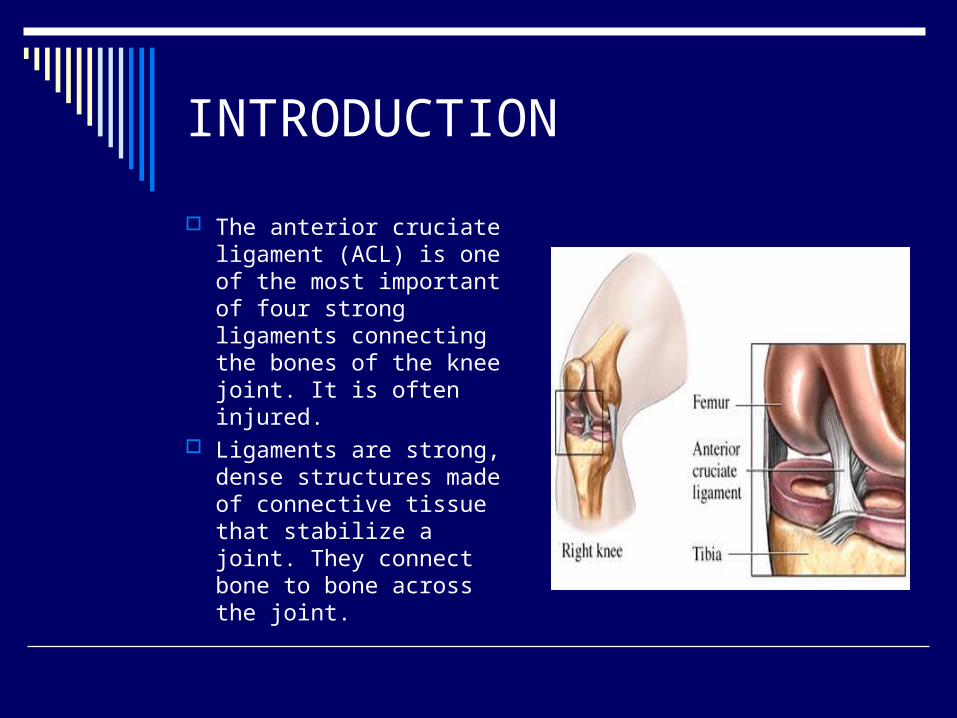
The anterior cruciate ligament (ACL) is one of the most important of four strong ligaments connecting the bones of the knee joint. It is often injured.
Ligaments are strong, dense structures made of connective tissue that stabilize a joint. They connect bone to bone across the joint.
A tear to the anterior cruciate ligament (ACL) results from overstretching of this ligament within the knee. It's usually due to a sudden stop and twisting
motion of the knee, or a force or "blow" to the front of the knee.
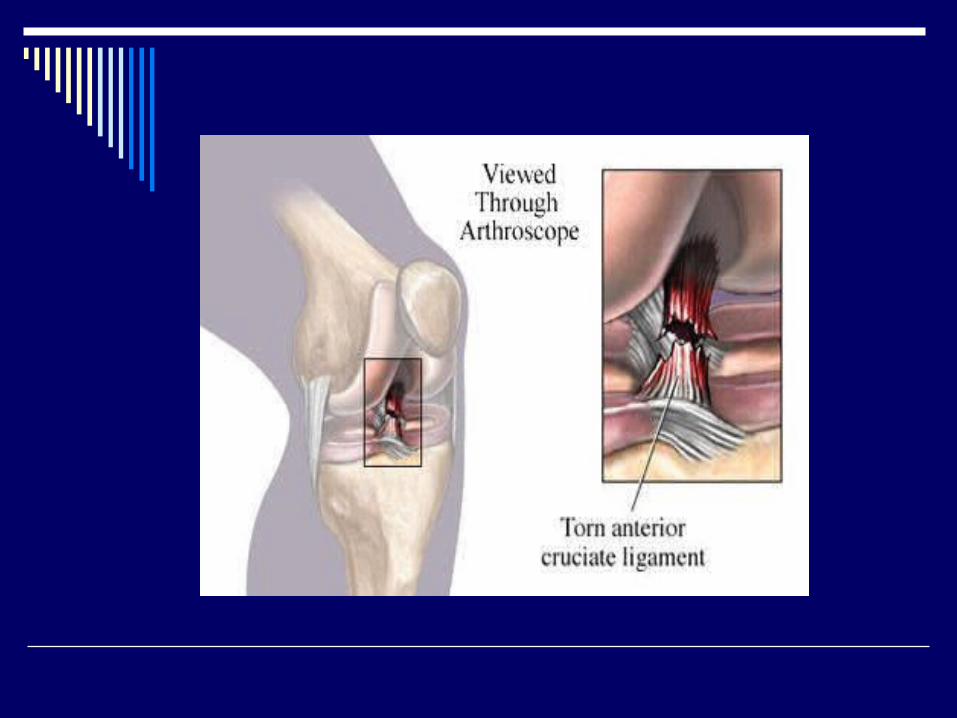
The extent of the tear can be a partial or a complete tear.
Individuals experiencing a tear to the ACL may or may not feel a pop at the time of the injury.
It is often injured together with other structures inside the knee joint.
After the initial injury, the knee may swell and become painful.
Instability or a sensation the knee is "giving out" may be a major complaint following this injury.
ANATOMY
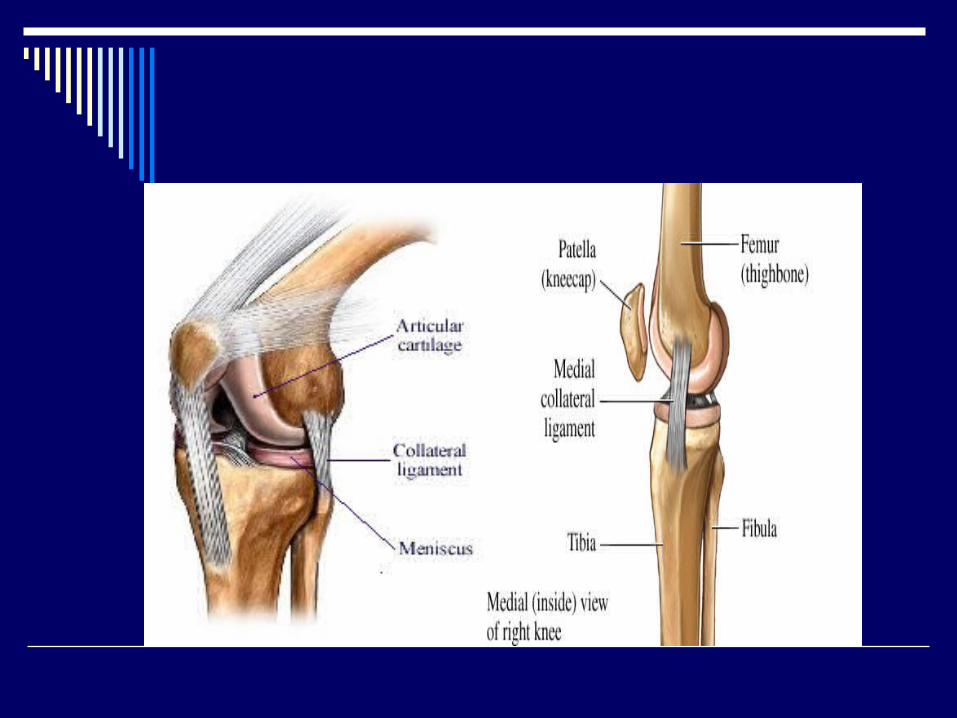
The knee is a hinge joint made up of three bones held firmly together by ligaments that stabilize the joint. The bones that meet at the knee are the upper leg bone (the femur), the lower leg bone (the tibia), and the knee cap (the patella). A smooth protective layer called cartilage, which allows the bones to glide smoothly upon each other, lines the bones inside the joint
The important parts of the knee include Bones and joints Ligaments and tendons Muscles Nerves Blood vessels
Bones and Joints The knee is the meeting place of two
important bones in the leg, the femur (the thighbone) and the tibia (the shinbone). The patella (or kneecap, as it is commonly called) is made of bone and sits in front of the knee.
The knee joint is a synovial joint. Synovial joints are enclosed by a ligament capsule and contain a fluid, called synovial fluid, which lubricates the joint.
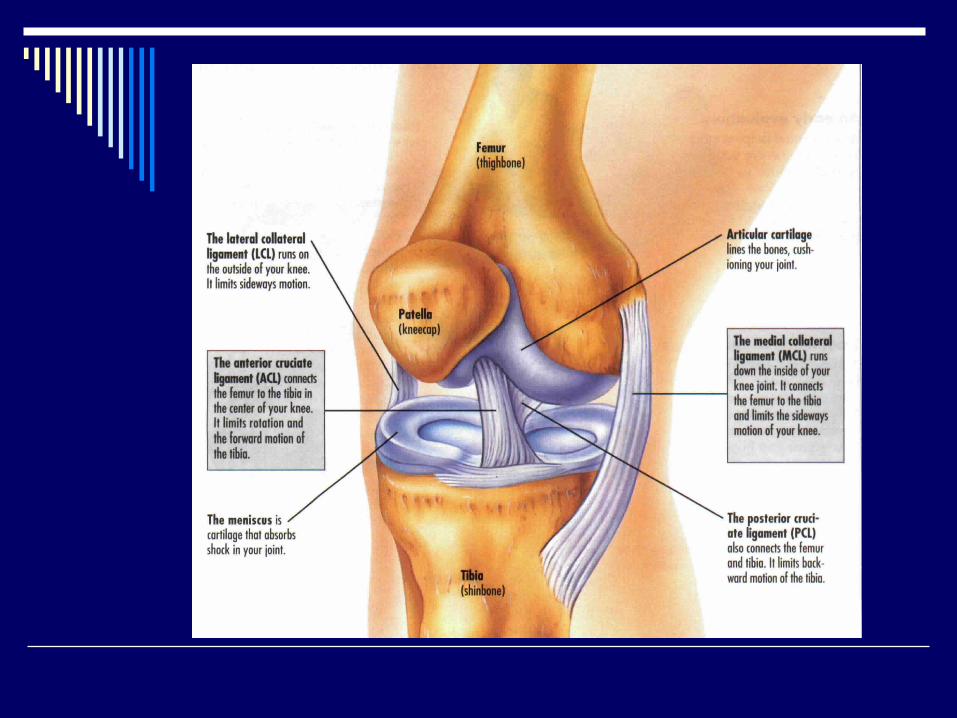
Ligaments MCL (Medial collateral ligament) LCL (Lateral collateral ligament) ACL (Anterior cruciate ligament) PCL (Posterior cruciate ligament) Menisci (Medial & lateral)

MCL : It joins femoral condyle to tibial shaft medially
LCL: It joins femoral condyle to fibular head laterally
The MCL and LCL prevent the knee from moving too far in the side-to-side direction.
ACL : It begins with anterior part of intercondylar area of tibia, runs upwards & backwards, & laterally & is attached to the post part of medial surface of lateral condyle of femur.
PCL : It begins from the post part of intercondylar area of tibia, runs upwards, forwards & medially & is attached to the anterior part of the lateral surface of medial condyle of femur.
The ACL keeps the tibia from sliding too far forward in relation to the femur. The PCL keeps the tibia from sliding too far backward in relation to the femur.
Working together, the two cruciate ligaments control the back-and-forth motion of the knee. The ligaments, all taken together, are the most important structures controlling stability of the knee.
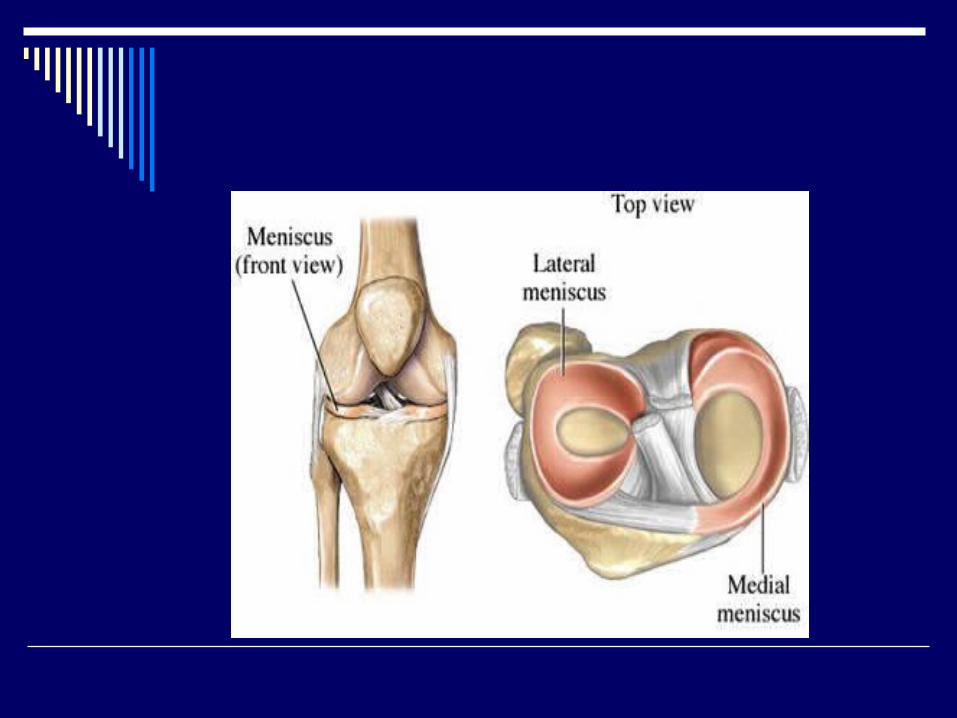
MENISCI Medial meniscus Lateral meniscus
The two menisci of the knee are important for two reasons: They work like a gasket to spread the force
from the weight of the body over a larger area
They help the ligaments with stability of the knee.
Muscles Muscles control the movement of the knee
joint. Rehabilitation of these muscles is most important following an ACL injury or reconstruction.
The major muscles of the knee joint involved with bending and straightening the knee are:
Quadriceps Hamstrings
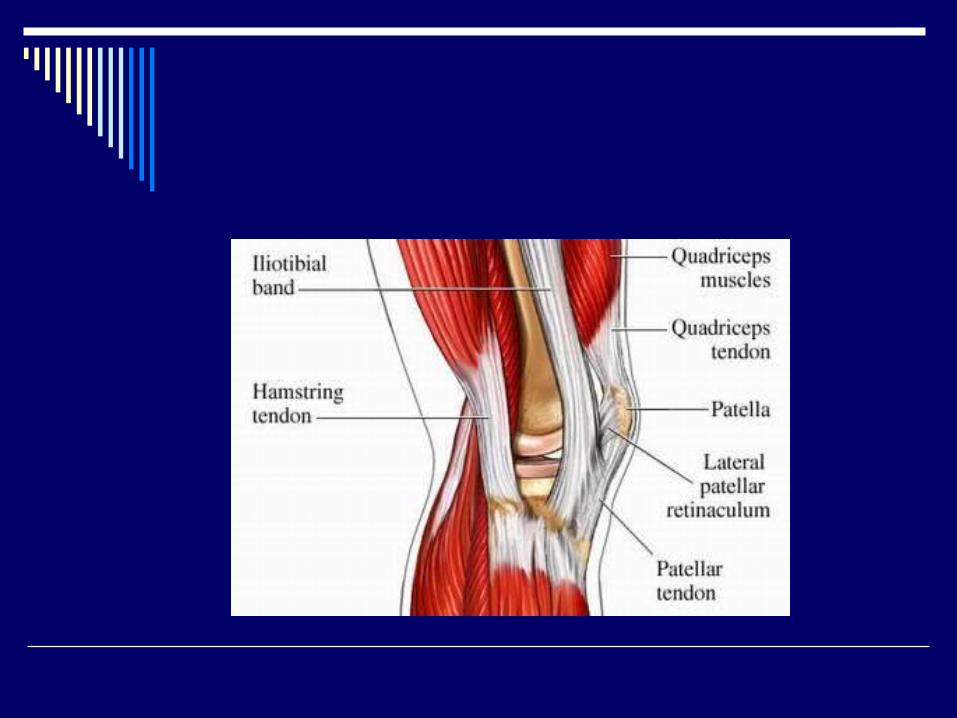
Quadriceps The quadriceps muscle is made up of the four large
muscles at the front of the thigh (these muscles are the rectus femoris, the vastus lateralis, the vastus intermedius, and the vastus medialis).
Hamstrings The hamstring muscles are the muscles at the
back of the upper leg. They flex (bend backward) the lower leg. Individually, the muscles of the hamstrings are the biceps femoris, semitendinosus, and semimembranosus.
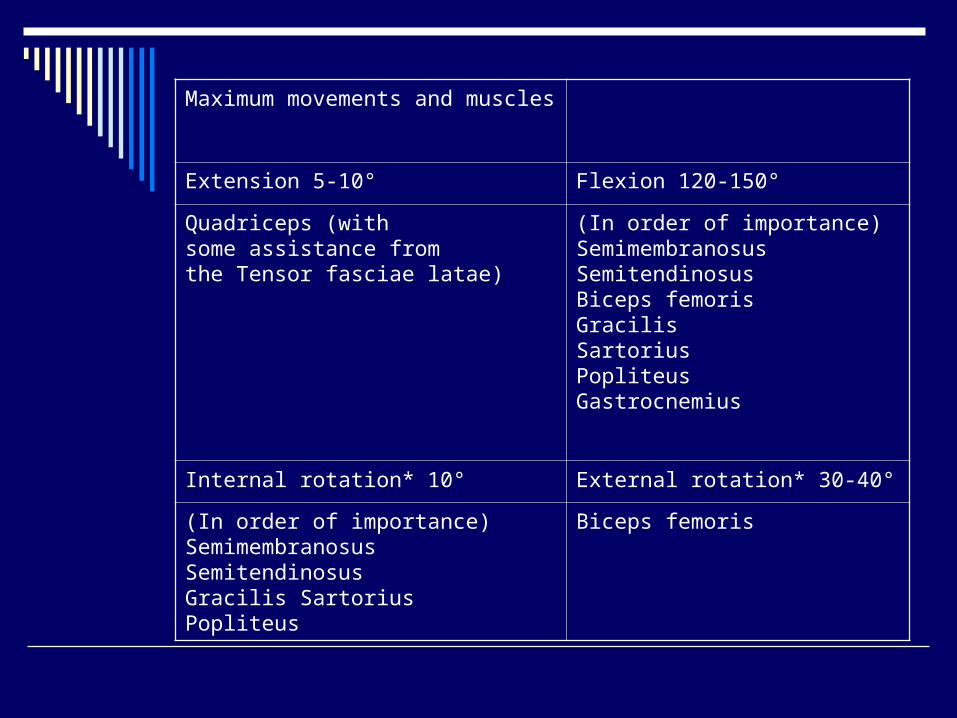
Maximum movements and muscles
Extension 5-10° Flexion 120-150°
Quadriceps (withsome assistance fromthe Tensor fasciae latae)
(In order of importance)SemimembranosusSemitendinosusBiceps femorisGracilisSartoriusPopliteusGastrocnemius
Internal rotation* 10° External rotation* 30-40°
(In order of importance)SemimembranosusSemitendinosusGracilis SartoriusPopliteus
Biceps femoris
CLASSIFICATION OF ACL INJURIES
An anterior cruciate ligament (ACL) injury often is called a sprain
Grade I sprain The fibres of the ligament are stretched, but
there is no tear. There is a little tenderness and swelling. The knee does not feel unstable or give out during
activity
Grade II sprain The fibres of the ligament are partially torn. There is a little tenderness and moderate swelling. The joint may feel unstable or give out during
activity Grade III sprain
The fibres of the ligament are completely torn (ruptured); the ligament itself has torn completely into two parts.
There is tenderness (but not a lot of pain, especially when compared to the seriousness of the injury). There may be a little swelling or a lot of swelling.
The ligament cannot control knee movements. The knee feels unstable or gives out at certain times.
Etiology
Movements of the knee that place a great strain on the ACL can cause damage to the ligament.
Hyperextension of the knee, caused by accidents associated with: Skiing Volleyball Basketball Soccer Football
Pivoting injuries of the knee are seen in sports such as: Football Tennis Basketball Soccer
Non-Athletic-Related Injuries Motor vehicle accidents in which the knee
is forced under the dashboard may also cause rupture of the ACL.
Repeated trauma and wear and tear can be a knee problem at any age causing small tears in the ligament, which over time become complete tears
CLINICAL FEATURES
Feeling or hearing a "pop" in the knee at the time of injury
Sudden instability in the knee (the knee feels wobbly, buckles or gives out) after a jump or change in direction or after a direct blow to the side of the knee
Pain on the outside and back of the knee Knee swelling within the first few hours of the
injury. This may be a sign of bleeding inside the joint (hemarthrosis). Swelling that occurs suddenly is usually a sign of a serious knee injury.
Limited knee movement because of swelling and/or pain
DIAGNOSIS
The diagnosis of an ACL tear is based on
Physical examination, Radiographic Evaluation MRI (Magnetic Resonance Imaging) KT 1000
Physical Examination Thorough history addressing how the
injury occurred and ascertaining when the pain may have first appeared. Questions regarding any earlier knee injuries are important as often ligaments and cartilage structures may have been previously strained. Any previous episodes of knee instability or the knee giving way is important information.
SPECIAL TESTS Laschman’s test Anterior drawer test Pivot shift
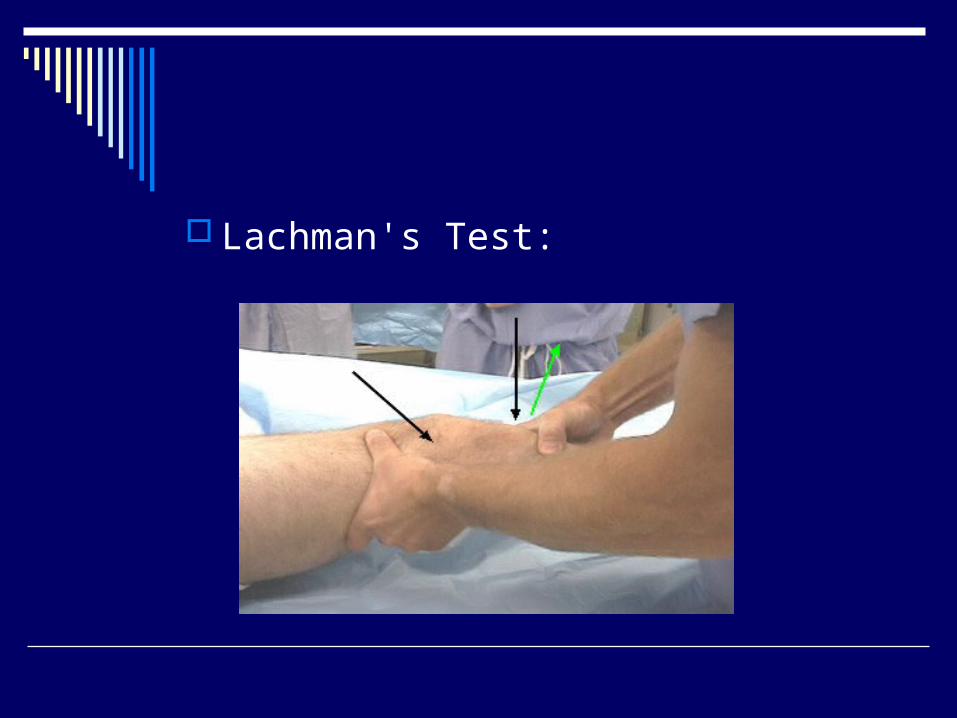
Lachman's Test:
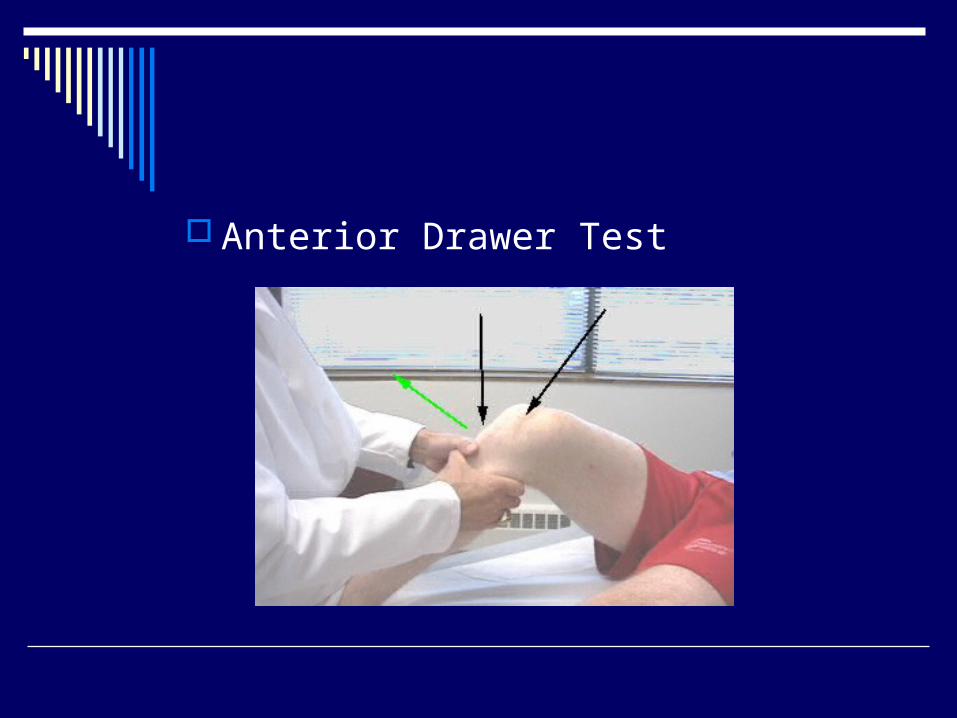
Anterior Drawer Test
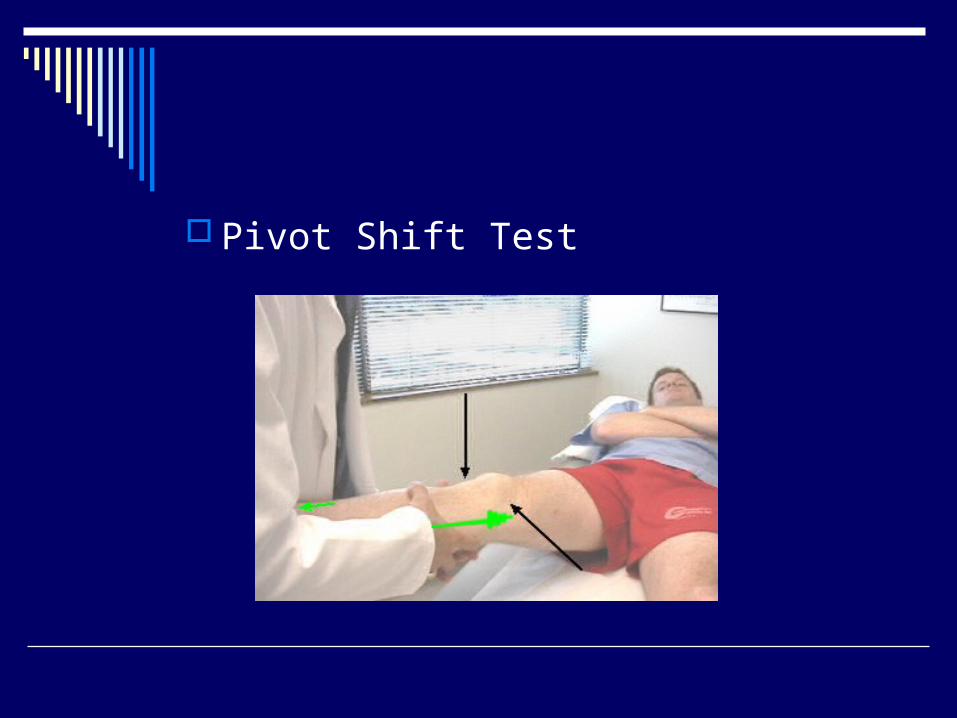
Pivot Shift Test

Radiographic Evaluation
MRI
KT 1000

MANAGEMENT
Immediately After the injury R.I.C.E. treatment is recommended.
Rest Ice Compression Elevation

Conservative treatment Bracing
Rehabilitation Brace Functional Brace
SURGICAL PROCEDURES There are several available operative
procedures: Patellar tendon graft procedure (BPTB) Hamstring graft procedure Allograft procedure
Patellar tendon graft procedure This type of ACL replacement uses the middle third
of the person's own patella tendon and is referred to as a bone-patella-tendon-bone (BPTB) graft.
Hamstring graft procedure Surgeon uses the patient's own hamstring
tendon, either the semitendinosus or gracilis tendons from the same leg.
Allograft procedure Another option is the use of tissue from a
cadaver (a deceased person) called an allograft.
Physiotherapy protocol following ACL reconstruction (BPTB GRAFT)
Day 0 to Day 10 Static quadriceps exercises i.e. tightening
of thigh muscles in order to achieve complete straightening of the knee joint
Ankle toe pump exercise Non weight bearing ambulation with the
help of either a walker or elbow crutches The knee is in a knee brace hence knee
bending & range of motion exercises are not possible & should not be attempted
DAY 11 TO DAY 20 Once all the stitches are removed Range of Motion
exercises are to be started. The knee brace is removed and weight bearing with the help of a stick is allowed.
The exercises are continued as above but with additions, namely:
Sitting at the edge of the bed with the knee bent as far as possible- flexing and extending the knee to increase the range of motion. We should try and increase the range of motion freely without force to at least 90deg by the end of one week.
Standing with the support of a stick in the opposite hand and doing alternate leg standing i.e. marching in one place.
Gait training with a single stick for support. The stick is to be used for two weeks.
DAY 21 onwards Increase the range of motion to 100- 110
deg during the fourth week. Quadriceps strengthening exercises namely
knee tightening, and straight leg raising with the knee in complete extension to start against gentle manual resistance.
Closed chain exercises for quadriceps and hamstring strengthening.
Half squats to increase the range of motion.
Wobble board balancing for quads- hams balancing.
Abductor- adductor strengthening in standing with therabands.
As the strength improves the patient can be weaned off the stick while walking (usually at about 3 weeks from surgery).
The range of motion has to be increased to normal i.e. 135 deg by the end of six weeks from the date of surgery.
Gait training and muscle strengthening exercises to continue with increasing intensity till normal range of motion is achieved and the muscle strength return to 5/5, Ideally the patient comes back for a review with the surgeon/physiotherapist at 10 days post op, then 21 days post-op, then at 6 weeks post op, then at 10 weeks post op, then at 12 weeks post op and finally at 16 weeks post op. By this time the full range of motion and muscle strength should be achieved. Only after getting a clearance from the surgeon should the patient resume any kind of sports activities.
Cryotherapy (ice packs) for the operated knee is very helpful in the initial 3-4 weeks for reduction of pain and swelling.
The knee may continue to feel sore, swollen and stiff for a few months from surgery. This is normal and nothing to worry about.
Car driving maybe resumed after 8 weeks from the date of surgery