prolonged asthmatic responses to inhaled methacholine
TRANSCRIPT
THE JOURNAL OF
ALLERGY AND
CLINICAL IMMUNOLOGY VOLUME 71 NUMBER 4
Original articles
Prolonged asthmatic responses to inhaled methacholine
N. C. Thomson, M.R.C.P., P. O’Byrne, F.R.C.P.(C),* and F. E. Hargreave, F.R.C.P. Hamilton, Ontario, Canada
The pattern of asthmatic response afier inhalation of’atropine and methachoiine was studied rn
.si.w adult usthmatics. After pretreatment with atropine, the provocation concentration of’
methachoiine to cause a full in FEV, qf‘207~ w’as increased,from 0.66 ? 2.09 to 94.90 t I.78
mglml. in the subsequent 7 hr, ,fAr Subjects developed prolonged asthmatic responses. These
occurred qfter concentrations qf methacholine higher than those used clinically but did not
directly relate to the dose of methachoiine or to the increuse in dose qfter atropine. In one
subject the prolonged response was not accompanied by increased methacholine responsiveness
and I~YIS not prevented by pretreatment with cromoiyn sodium (40 mg). These results shoM1 that
high doses qf’methachoiine inhaled qfier pretreatment with atropine can induce prolonged
asthmatic responses but the mechanism is unclear. (J ALLERGY CLIN IMMUNOL 71:357, 1983.)
Inhalation of methacholine is widely used in North America to measure nonspecific bronchial respon- siveness.‘. 2 In the concentrations used in clinical practice the bronchoconstrictor response is short and resolves spontaneously over about 2 hr.”
Methacholine inhalation has also been used to quantitate the bronchial anticholingeric (muscarinic)
From the Firestone Regional Chest and Allergy Unit, Department of Medicine, St. Joseph’s Hospital and McMaster University, Hamilton, Ontario, Canada.
Supported by a grant from the Medical Research Council of Canada.
Received for publication June 8, 1982. Accepted for publication Sept. 27, 1982. Reprint requests to: Dr. F. E. Hargreave, Firestone Regional Chest
and Allergy Unit, St. Joseph’s Hospital, 50 Charlton Ave. East, Hamilton, Ontario, Canada L8N lY4.
*Fellow of the Medical Research Council of Canada.
effect of ipratropium bromide and atropine.“. 3 Re- cently, in such a study, four of 12 asthmatic subjects unexpectedly complained of chest tightness and wheeze between 5 and 12 hr after pretreatment with ipratropium and inhalation of high concentrations of methacholine to overcome the inhibition.4 It was sug- gested that methacholine might induce responses of the late asthmatic type.6 Objective evidence of airflow obstruction was obtained in only one subject, and so it was uncertain as to the pattern, frequency, and possi- ble mechanism(s) of this response. Furthermore, it was possible that the later response was associated with an increase in nonspecific bronchial responsive- ness as has been shown to occur after allergen- induced late asthmatic responses.‘, ’
In the present study we examined the effects on airflow rates of inhaled methacholine, with and with- out atropine pretreatment, over 7 hr in six asthmatics.
Vol. 71, No. 4, pp. 357-362

358 Thomson et al. Il. ALLERGY CCIN. IMMWNCI.. APRIL tSR3
the FEV, and PEF were measured three thuer;. On 2 day<\ they inhaled atropine (5 mgiml. 3 mg nebulized) or saline for 2 min, and after 30 min had a methacboline inhalatttm lest. On the atropine pretreatment day further &opine (2.“; mg/ml) was inhaled for 1 tnin before each second inhalatmn of methacholine. On the third day they inhated saline for I min. and after 30 min had a saline inhalation test carried out as a mcthacholine test. All inhalations were given in ;i single-blind, randomized fashion. Systemic Gde et’ti~t~ (11 atropine were not recorded: in another study tht: same tiosc had no significant effect on heart rate or saliva ~trttpnt. !‘I After the inhalation test on each day the sub,jccts remaincd in the laboratory for I hr and recorded their PFF every ii! min. All stmjects (except no. 4) then left the laboratory and continued to measure their PEP every hour it) 7 hi- ‘The> were instructed not to exerctse, to avoid any trtgger% known to incite asthma. and to use inhaled salbutamol i?(X) gg) should symptoms warrant this, but to record PEF befort* and IO min after its use.
One subject (No.4) attended the laboratory OrI 5 dny$. (.Jn the first two he had a methachoiine test. On the IIICRI: tw:) 11~’ received premeditation: at 0 min with atropinc ( 4 mg nebulized), then at 20 min with placebo (on the third day1 OI eromolyn sodium (40 mg, on the fourth day i. At 30 mm he was given three inhalations of mothacholine (12. 64, mtl
I28 mgiml) at 5 min intervals. F’EV,. vital capac’tty, itnil PEF were measured before and after each inhalation anJ hourly up to 7 hr. On the fifth day he had a mcthachol~nc inhalation test.
Abhr~~~itrtior~r used
FEV,: Forced expired volume in I second PEF: Peak expiratory flow rate PC,,,: Prov,ocation concentration of methacholine
producing a 20’% fall in FEV,
METHODS Subjects
Six adult asthmatic subjects from the Firestone Regional Chest and Allergy Unit were randomly selected for study (Table I). All had histories of episodic dyspnea and wheeze. with relief of symptoms by treatment with a bronchodilator. At the time of the study. symptoms of asthma were either absent or controlled on minimal medication. Inhaled sal- butamol was withheld for at least 8 hr and oral oxytriphyl- line for 24 hr before each test; inhaled heclomethasone di- propionate was continued in the same dose throughout the study, Their FEV, was greater than 76%, of predicted and their methacholine bronchial responsiveness was increased (Table 11). None of the subjects had any other respiratory disease. Three were atopic as indicated by one or more wheal and flare responses to prick skin tests with I6 com- mon allergen extracts: the only allergen to which they were currently exposed was house dust. None had symptoms of a respiratory infection within the preceding 6 wk. All gave written informed consent.
Inhalation tests The drug solutions of atropine sulfate (5 and 2.5 mg/ml)
and tnethacholine hydrochloride were made up in phos- phate-buffered saline with benzyl alcohol I .5% preserva- tive. All solutions were stored at 4” C and inhaled at room temperature. Aerosols were generated by a Wright nebulizer operated at 50 psi, X Limin. to give output of 0. I5 mlimin. The nose was clipped and aerosols inhaled through the mouth by tidal breathing via a loose-fitting face mask.
Methacholine inhalation tests were carried out with a standard technique.‘. !’ Saline was inhaled tirst. followed by doubling concentrations of methacholine from 0.03 to 256 mgiml for 2 min at 5 min intervals. The response was measured as change in FEV, with a Collins 13.5 L, water spirometer; values were recorded before and 0.5 and 1 .S min after each inhalation, and if necessary at 3 min and subsequent intervals of 2 min until the lowest FEV, had been recorded. Inhalations of methacholine were continued until the FEV, had fallen by 20% or more below the lowest postsaline value. The airway response was also measured as change in PEF with a mini-Wright peak flow meter; on each occasion the best of three efforts was recorded. The PC,,, was obtained from the log dose-response curve by linear interpolation of the point above and below the 20% fall in FEV,.
Study design Subjects attended the laboratory on 3 days, at the same
time of day, within 1 wk. They rested for 30 min and then
Analysis Logarithmtc transformation ot PC,,, ULL~ us<~l itsr ;&II
statistical analysis,. Wilcoxon signed-rank text” VI;I\ uacli to . . examme the etfect on PC,,,. FE V, . or PEIS of :itropinr:,
methacholine, or saline. Differences were ~~orrsiclered +ig- nificant if p .:-C 0.05.
RESULTS
Baseline values for FE\‘, and PEF wcrc simiho between study days (Table I. Fig. 1). FEY, (tneart percent change +- SE) increased significantly after at” ropine pretreatment (+X.2 + I .6) compareii with sa- line pretreatment (-1.8 i 0.6; p <: 0.0001). Simi- larly PEF increased significantly after atropine (+8.4 +- 2.6) compared with saline t -- I .5 f (X.4: p < 0.001). Atropine significantly increased the PC1!,, (mean t SE) from 0.66 rt 1 .35 to SM.90 ?- I ,Zo mgiml (p = 0.015; Table If).
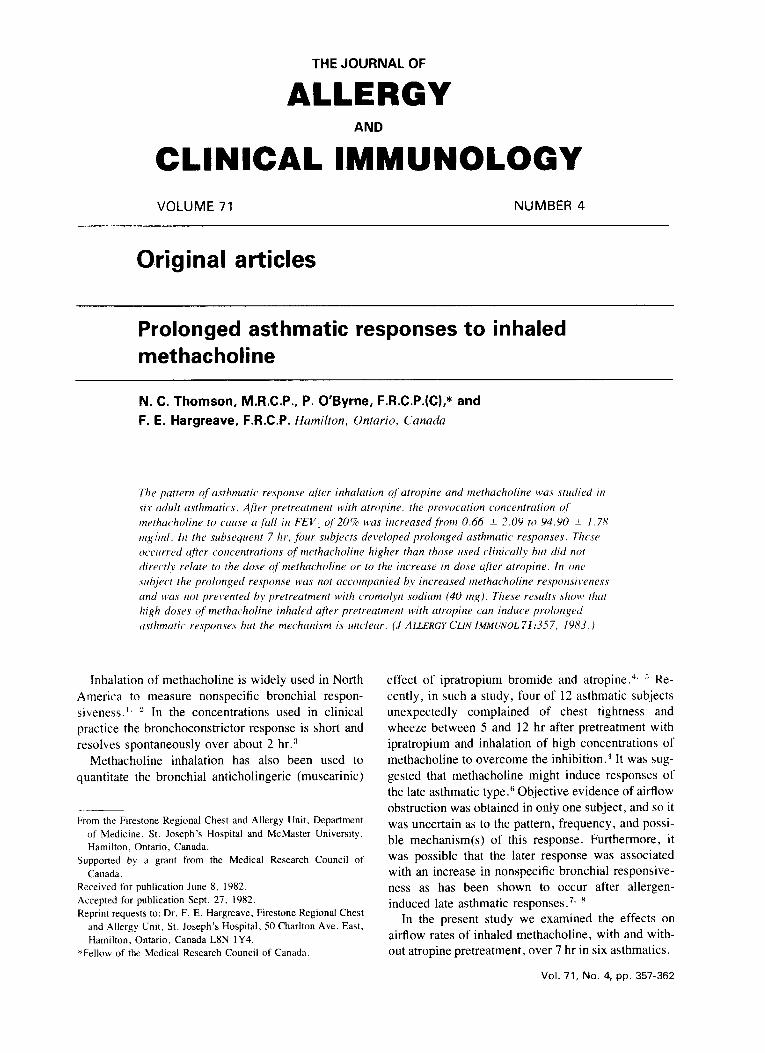
After premeditation with saline. ~~l~t~~~~~~l~~~ stimulated an early asthmatic response; the change in PEF between 2 and 7 hr did not differ significantly from that produced by saline inhalation without metha- choline, with a mean fall of 5.0% and 7.2%. respe~ tively (p = 0.33; Table II, Fig. 1). However, after premeditation with atropine the higher concentrations of methacholine required to reduce the FEV, by XI% resulted in a mean fall in PEF between 2 and 7 hr of 25.8% (p = 0.03; Table II, Fig. 1). This difference
VOLUME 71 NUMBER 4
Prolonged responses to methacholine 359
PEF
0 2 4 6 8 0 2 4 6 8
TIME (hours)
FIG. 1. Absolute values for PEF plotted against time after inhalation (/) of methacholine with pretreatment(P) with saline (3) and atropine (a), and after inhalation of saline after pretreatment with saline (0). S, Salbutamol 200 wg.
occurred because of prolonged asthmatic responses in four subjects with reduction in PEF of greater than 20%. These were associated with cough, chest tight- ness, and wheeze and were reversed by salbutamol (Fig. 1).
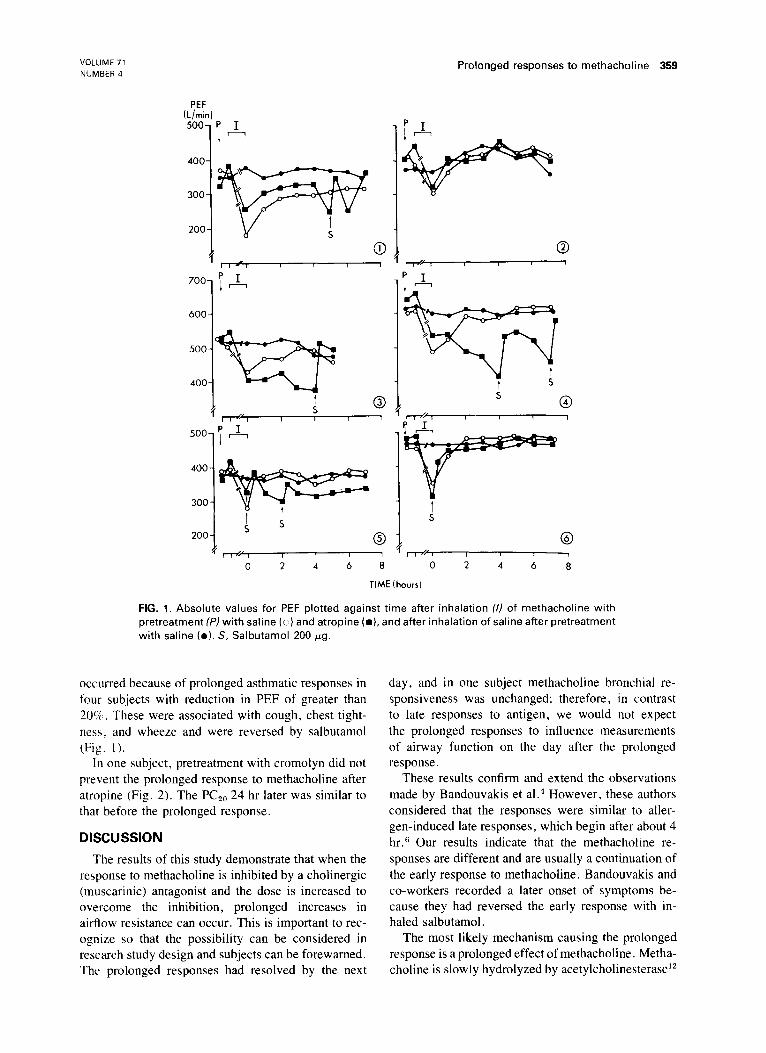
In one subject, pretreatment with cromolyn did not prevent the prolonged response to methacholine after atropine (Fig. 2). The PCTO 24 hr later was similar to that before the prolonged response.
DISCUSSION
The results of this study demonstrate that when the response to methacholine is inhibited by a cholinergic (muscarinic) antagonist and the dose is increased to overcome the inhibition, prolonged increases in airflow resistance can occur. This is important to rec- ognize so that the possibility can be considered in research study design and subjects can be forewarned. The prolonged responses had resolved by the next
day, and in one subject methacholine bronchial re- sponsiveness was unchanged; therefore, in contrast to late responses to antigen, we would not expect the prolonged responses to influence measurements of airway function on the day after the prolonged response.
These results confirm and extend the observations made by Bandouvakis et a1.4 However, these authors considered that the responses were similar to aller- gen-induced late responses, which begin after about 4 hr.” Our results indicate that the methacholine re- sponses are different and are usually a continuation of the early response to methacholine. Bandouvakis and co-workers recorded a later onset of symptoms be- cause they had reversed the early response with in- haled salbutamol.
The most likely mechanism causing the prolonged response is a prolonged effect of methacholine. Metha- choline is slowly hydrolyzed by acetylcholinesterase”

360 Thomson et al.
FEV,
J ALLERGY CLLN. LMMUNOL. APRkL 1483
* s!!fl 50-J I/$ I I I I I I I 1
0 2 4 6 8
TIME ihours]
FIG. 2. Absolute values for FEV, and vital capacity (VC) plotted against time after pretreatment (Pi’ with atropine and placebo (D) or atropine and cromolyn ( I) in subject 4. S, Salbutamol 200 Fg.
TABLE I. Subject characteristics _. .--.-
FEV, Age Height ___----- PEF No. of positive
Subject No. (yr) Sex (cm) L* % Predicted (L/min)* prick skin testst Current medicationS -_-_.--
I 37 F 1.52 1.88 + 0.16 77 348 -t- 23 0 s X00, B 401i 2 65 F 157 1.79 t 0.06 91 398 + 20 0 s 400. 13 800. 0 0M.i 3 54 M 175 2.88 t 0.10 86 523 i- 6 0 s 200 4 29 M 178 3.67 -+ 0.08 86 622 _t lb .% s not LhiiL 5 39 F 160 2.48 t 0.07 93 372 -fr X 9 s 200 6 38 F 152 2.64 7tr 0.06 100 468 _t IO ‘X S not d;uly
---__-.-_.---.-..-...----__^._ _.-.._.-_---_- - -- .-
*Mean + SD.
tPrick skin tests: a positive response indicates at > 2 mm wheal response to one or more of I6 common allergens $Current medication: S = salbutamol (pgiday); B >= beclomethasone dipropionate (pgiday); 0 = oxtriphylline (mg /day).
and the response to it usually takes about 2 hr to reverse.” The much greater (84- to 190-fold) dose required to overcome the inhibitory effect of atropine might take longer to hydrolyze. The intersubject vari- ability was not related to the dose of methacholine or to the degree of increase in dose after atropine, pos- sibly as a result of the small number of subjects stud- ied or differences between individuals in the activity
of acetylcholinesterase, methacholine, or atropine. Other possible mechanisms producing the pro
longed response include mediator release tram mast cells, release of metabolites of arachidonic ~rd, and increased secretions. Cholinergic receptor stimulation has been reported to enhance mediator relsasc from chopped human lung’:’ and from rat mast ~eY1?;,~~ ;\I- though these findings have not been confirmed by
VOLUME 71 NUMBER 4
Prolonged to responses methacholine 361
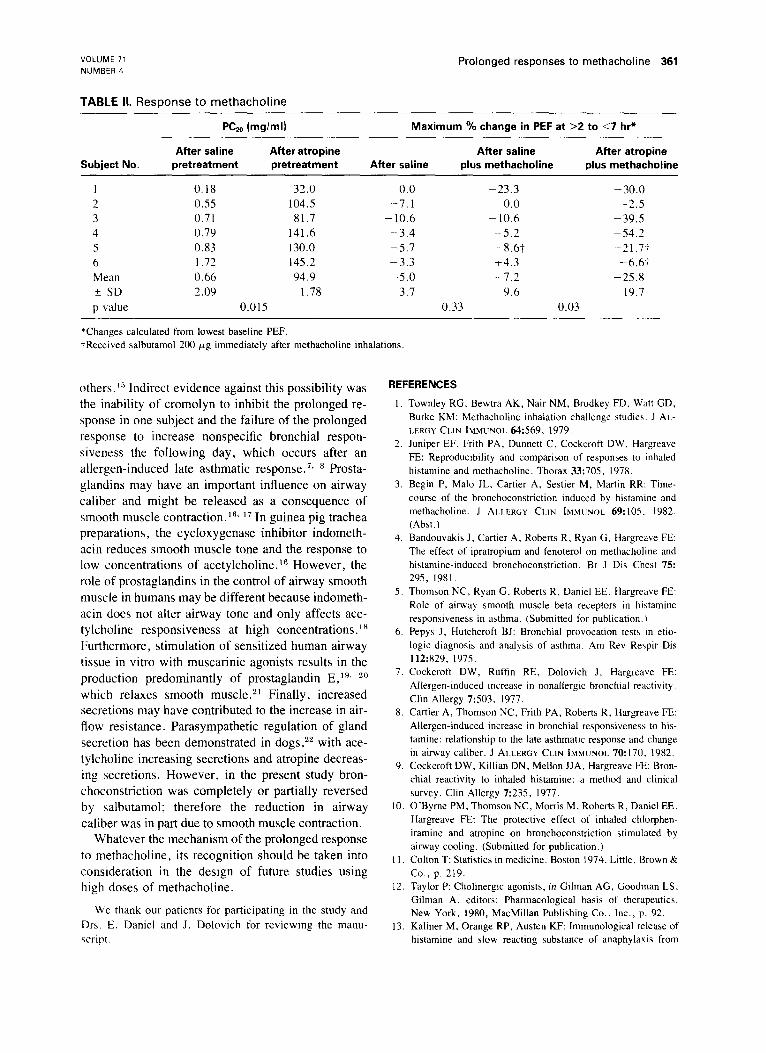
TABLE II. Response to methacholine
PC& (mglml) Maximum % change in PEF at >2 to <7 hr*
After saline After atropine After saline After atropine Subject No. pretreatment pretreatment After saline plus methacholine plus methacholine
I 0.18 32.0 0.0 -23.3 -30.0 2 0.55 104.5 -7.1 0.0 -2.5 3 0.71 81.7 - 10.6 - 10.6 -39.5 4 0.79 141.6 -3.4 -5.2 -54.2 5 0.83 130.0 -5.7 -8.61 -21.7-i. 6 1.72 145.2 -3.3 14.3 -6.6.i Mean 0.66 94.9 -5.0 -7.2 -25.8 t SD 2.09 1.78 3.7 9.6 19.7 p value 0.015 0.33 0.03
*Changes calculated from lowest baseline PEF. iReceived salbutamol 200 pg immediately after methacholine inhalations.
others.‘” Indirect evidence against this possibility was the inability of cromolyn to inhibit the prolonged re- sponse in one subject and the failure of the prolonged response to increase nonspecific bronchial respon- siveness the following day, which occurs after an allergen-induced late asthmatic response.7s B Prosta- glandins may have an important influence on airway caliber and might be released as a consequence of smooth muscle contraction.r6, I7 In guinea pig trachea preparations, the cycloxygenase inhibitor indometh- acin reduces smooth muscle tone and the response to low concentrations of acetylcholine.‘” However, the role of prostaglandins in the control of airway smooth muscle in humans may be different because indometh- acin does not alter airway tone and only affects ace- tylcholine responsiveness at high concentrations.‘* Furthermore, stimulation of sensitized human airway tissue in vitro with muscarinic agonists results in the production predominantly of prostaglandin E,‘“, 2o whit h relaxes smooth muscle .21 Finally, increased secretions may have contributed to the increase in air- flow resistance. Parasympathetic regulation of gland secretion has been demonstrated in dogs,22 with ace- tylcholine increasing secretions and atropine decreas- ing secretions. However, in the present study bron- choconstriction was completely or partially reversed by salbutamol; therefore the reduction in airway caliber was in part due to smooth muscle contraction.
Whatever the mechanism of the prolonged response to methacholine, its recognition should be taken into consideration in the design of future studies using high doses of methacholine.
We thank our patients for participating in the study and Drs. E. Daniel and J. Dolovich for reviewing the manu- script.
REFERENCES
I.
2.
3.
4.
5.
6.
I.
8.
9.
IO.
Il.
12
13
Townley RG, Bewtra AK, Nair NM, Brodkey FD. Watt GD, Burke KM: Methacholine inhalation challenge studies. J AL- LERGY CLIN IMMUNOL 64~569, 1979. Juniper EF, Frith PA, Dunnett C, Cockcroft DW. Hargreave FE: Reproducibility and comparison of responses to inhaled histamine and methacholine. Thorax 33:705, 1978. Begin P, Malo JL, Cattier A, Sestier M, Martin RR. Time- course of the bronchoconstriction induced by histamine and methacholine. J ALLERGY CLIN IMMIJNOL 69:lOS. 1982. (Abst.) Bandouvakis J, Cattier A. Roberts R, Ryan G. Hargreave FE: The effect of ipratropium and fenoterol on methacholine and histamine-induced bronchoconstriction. Br J Dis Chest 75: 295, 1981. Thomson NC, Ryan G, Roberts R, Daniel EE, Hargreave FE: Role of airway smooth muscle beta receptors in htstamine responsiveness in asthma. (Submitted for publication.) Pepys .I. Hutchcroft BJ: Bronchial provocation tests in etio- logic diagnosis and analysis of asthma. Am Rev Respir Dis 112:829, 1975. Cockcroft DW, Ruffin RE, Dolovich J, Hargreave FE: Allergen-induced increase in nonallergic bronchial reactivity. Clin Allergy 7:503, 1977. Cartier A, Thomson NC, Frith PA, Roberts R, Hargreave FE: Allergen-induced increase in bronchial responsiveness to his- tamine: relationship to the late asthmatic response and change in airway caliber. J ALLERGY CLIN IMMUNOL 70~170. 1982. Cockcroft DW, Killian DN, Mellon JJA, Hargreave FE Bron- chial reactivity to inhaled histamine: a method and clinical survey. Clin Allergy 7:235, 1977. O’Byrne PM, Thomson NC, Morris M, Roberts R, Daniel EE, Hargreave FE: The protective effect of inhaled chlorphen- iramine and atropine on bronchoconstriction stimulated by airway cooling. (Submitted for publication.) Colton T: Statistics in medicine. Boston 1974. Little, Brown & Co., p. 219. Taylor P: Cholinergic agonists, in Gilman AG, Goodman LS, Gilman A, editors: Pharmacological basis of therapeutics. New York, 1980, MacMillan Publishing Co., Inc., p. 92. Kaliner M, Orange RP, Austen KF: Immunological release of histamine and slow reacting substance of anaphylaxis from

362 Thomson et al.
human lung. Enhancement by cholingeric and alpha adrenergic stimulation. J Exp Med 136:556, 1972.
14. Fantozzi R, Masini E, Blandina P, Mannaioni PF, Bani-Sacchi T: Release of histamine from rat mast cells by acetycholine.
Nature 273:473, 1978. 15. Foreman JC: The pharmacological control of immediate hy-
persensitivity. Ann Rev Pharmacol Toxicol 21:63, 1981.
16. Orehek J. Douglas JJ, Bouhuys A: Contractile responses ofthe guinea pig trachea in vitro: modification by prostaglandin synthesis-inhibiting drugs. J Pharmacol Exp ‘fher 1945.54,
1975. 17. Orehek J. Douglas JJ, Lewis AJ, Bouhuys A: Prostaglandin
regulation of airway smooth muscle tone. Nature 24584.
1973.
Am. J. Urihi. April 1983
18. Brink C, Grimaud C, Guillot C, Orehek J: The interaction between indomethacin and contractile agents on human iso
lated airway muscle. Br J Pharmacol 69:383. 19X0 19. Steel L, Platson L. Kaliner M: Prostaglandin peneration b>
human and guinea pig lung tissue: comparison of parenchymal and airway responses. J ALI EKGY CI IN IKVW\~I 6&28?.
1979. 71) Adkinson NF, Newball HH, Findlay S, Adams K i.icirrcnatcw
LM: Anaphylactic release of prostaglandins I‘rm hw~~n iurrr:
in vitro. Am Rev Respir Dis 121:91 1. 1481). 7 I. Sweatman WJF. Collier HOJ: Effects of pto~tagianchn~ $10
human bronchial muscle. Nature 217:69. 1968 22. Nadel JA: Regulation of fluid and mucous wcrctaw, iti ;r~?’
way\ J AILERGY CLIN IMMI’NOL 67:417. l98!