prospective randomized controlled clinical and histopathological study of acne vulgaris treated...
TRANSCRIPT

DERMATOLOGIC SURGERY
Prospective randomized controlled clinical andhistopathological study of acne vulgaris treated
with dual mode of quasi-long pulse and Q-switched1064-nm Nd:YAG laser assisted with a topically
applied carbon suspension
Jae Yoon Jung, MD,a,b Jong Soo Hong, MD,a,b Chang Ho Ahn, MD,a Ji Young Yoon, MSc,b
Hyuck Hoon Kwon, MD,a,b and Dae Hun Suh, MD, PhDa,b
Seoul, Korea
From
C
N
Fund
Conf
Acce
626
Background: Acne treatments using laser and light devices have been reported to have varying degrees ofefficacy. However, there has been no study of treatment of acne using a dual mode (quasi-long pulse andQ-switched mode) 1064-nm Nd:YAG laser assisted with a topically applied carbon suspension.
Objective: To evaluate the clinical efficacy, safety, and histological changes of new laser treatment methodfor acne vulgaris.
Methods: Twenty-two patients received 3 sessions of quasi-long pulse and Q-switched Nd:YAG lasertreatment assisted with a topically applied carbon suspension at 2-week intervals in a randomized split facemanner.
Results: At the final visit, the inflammatory acne lesions were reduced on the laser-treated side by 58.6%(P\.001), but increased on the untreated side by 5%. The noninflammatory acne lesions were reduced onthe laser-treated side by 52.4% (P \ .001). Sebum output reduction, inflammatory cell and cytokinereductions, a decrease of the thickness of a perifollicular stratum corneum and a full epithelium, and skinrejuvenation effect were found. The histopathologic examination of the acne lesions showed decreasedinflammation and immunostaining intensity for interleukin 8, matrix metalloproteinase-9, toll-like receptor-2, and nuclear factor kappa B, and tumor necrosis factor alpha was reduced significantly. No severe adversereactions were reported. All patients reported mild transient erythema that disappeared in a few hours.
Limitations: The number of subjects studied was small.
Conclusions: This laser treatment was rapid and effective for treating not only the inflammatory but alsothe noninflammatory acne lesions when compared with the control side. The histopathologic findingscorrelated well with the clinical acne grade and treatment response. This novel laser treatment appears tobe safe and effective for acne treatment. ( J Am Acad Dermatol 2012;66:626-33.)
Key words: acne; histopathologic examination; Nd:YAG laser; sebum output.
INTRODUCTIONAcne is one of the most common inflammatory
skin disorders. It affects about 80% of adolescentsand young adults.1,2 Acne treatments using laser and
the Department of Dermatology, Seoul National University
ollege of Medicine,a and Acne Research Laboratory, Seoul
ational University Hospital.b
ing sources: None.
licts of interest: None declared.
pted for publication August 12, 2011.
light devices have been reported to have varyingdegrees of efficacy. Red and blue light therapies,3-5
the 585- and 595-nm pulsed dye laser (PDL),6-8
the 1320-nm neodymium:yttrium-aluminum-garnet
Reprint requests: Dae Hun Suh, Department of Dermatology,
Seoul National University Hospital, 28 Yongon-dong,
Chongno-gu, Seoul, 110-744, Korea. E-mail: [email protected].
Published online October 28, 2011.
0190-9622/$36.00
� 2012 by the American Academy of Dermatology, Inc.
doi:10.1016/j.jaad.2011.08.031

J AM ACAD DERMATOL
VOLUME 66, NUMBER 4Jung et al 627
(Nd-YAG) laser,9 the 1450-nm diode laser,10 and theintense pulsed light (IPL) have been reported to havetherapeutic effects in patients with acne vulgaris.
Lasers may be a good alternative therapeuticmodality for those patients who fail to respond toor could not tolerate other acne treatments. Thetherapeutic mechanism of lasers is associated with
CAPSULE SUMMARY
d We performed a randomized controlledtrial with a dual mode of quasi-longpulse and Q-switched 1064-nm Nd:YAGlaser assisted with a topically appliedcarbon suspension in the patients withacne vulgaris.
d After 3 sessions of treatment, theinflammatory and noninflammatory acnelesions were reduced by 58.6% and52.4%, respectively.
d This laser treatment appears to be safeand effective for treating not only theinflammatory but also thenoninflammatory acne lesions.
the wavelengths, energypower, and pulse duration.However, the anti-acnemechanisms associated withsome lasers remain largelyunknown and need to beelucidated.
The Q-switched 1064-nmNd:YAG laser is commonlyused for pigment and tattoolesions. In addition, it hasbeen shown that the 1064-nm Q-switched Nd:YAGlaser with topical carbonsuspension provides satis-factory clinical results forthe treatment of periocularand perioral rhytides.11,12
Furthermore, treatment witha topical carbon suspension
has shown improvement in post-acne scarring andfacial wrinkles. The Q-switched 1064-nm Nd:YAGlaser is not a modality usually associated with acnetreatment, but careful manipulation of the beamparameters or combination with an exogenousartificial chromophore, such as topical carbon lo-tion serving as a photoenhancer, has been associ-ated with significant improvements in acne. Whenthe 1064-nm Nd:YAG laser is used for treatmentat two very different pulse widths, such as thequasi-long pulse and the Q-switched pulse, theabsorption characteristics of carbon at 1064 nm arecapable of producing totally different biologicaleffects. At these parameters the Nd:YAG laser mightbe effective for treatment of inflammatory acne.The aim of the present study was to evaluate theclinical efficacy, safety, and histological changescaused by the Q-switched and quasi long-pulsed1064-nm Nd:YAG laser for the treatment of mild tomoderate facial acne in Korean patients. To ourknowledge, this is the first report of the 1064-nmNd:YAG laser and a carbon suspension used for thetreatment of acne vulgaris.
METHODSStudy design and subjects
This study was designed as an 8-week, prospec-tive, split-face, single-blind, and randomized
controlled trial. The study was conducted in accor-dance with the Declaration of Helsinki and wasapproved by the Institutional Review Board of theSeoul National University Hospital (InstitutionalReview Board approval No. D-1003-003-067).Written informed consent was obtained from allsubjects prior to enrollment. Subjects were not
allowed to use any systemic,topical, or phototherapy-based acne treatment duringthe course of this study. Theexclusion criteria were preg-nancy and prior acne ther-apy, including isotretinointherapy within 6 months,systemic antibiotic therapy(for any indication) within1 month, and topical acnepreparations or intralesionalsteroid injections within1 month of starting lasertreatment.
Twenty-two patients withacne, 4 men and 18 women,were enrolled in this study.Their mean age was 25.4years and ranged from 19 to
34 years. The volunteers had Fitzpatrick skin typesIII-V. One side of the face was treated, except for theupper eyelids, eyebrows, and lips.
Preparation of the face and laser treatmenttechnique
At the first and subsequent treatment sessions,prior to each treatment, the patient’s face waswashed with the same cleanser. The carbon lotionwas applied evenly over one half of the face to betreated and allowed to penetrate the skin and hairfollicles for 20 minutes.
The laser source was a dual pulsed Q-switchedNd:YAG laser (Spectra VRM III, Lutronic, Ilsan,Korea). The laser energy was delivered with a7-mm diameter spot-sized handpiece at a repetitionrate of 10 Hz. Two different pulse widths were used.Single pass with minimal overlapping was carriedout on the treatment side of the face with a quasilong-pulse of 300 microseconds. The fluence was 1.8to 2.0J/cm2. Since multiple overlapping passes caninduce too much of a thermal effect and cause first-degree burns, overlap was minimized during the firstpass.
After the treatment described abovewas done, thelaser was set to Q-switched mode, with pulse widthof 5 nanoseconds and initial fluence of 1.8 J/cm2. Aspatient tolerance improves, the fluence may be
Abbreviations used:
H&E: hematoxylin and eosinHSP: heat shock proteinIL: interleukinMMP: matrix metalloproteinaseNd:YAG: neodymium:yttrium-aluminium-garnetNF-kB: nuclear factor kappa-light-chain-
enhancer of activated B cellsPDL: pulsed dye laserTGF-b: transforming growth factor betaTLR: toll like receptorTNF-a: tumor necrosis factor alphaVAS: visual analogue scale
J AM ACAD DERMATOL
APRIL 2012628 Jung et al
increased up to 2.3 J/cm2 or as close to this value aspossible. All of the areas to be treated were coveredin 3 passes (horizontal, vertical, and diagonal) with30% overlapping until the popping sound was nolonger heard. The immediate posttreatment endpoint was an even mild erythema over the entiretreated area.
Study treatment and clinical outcomeassessments
Patient follow-up was scheduled at 2-week inter-vals during the 4-week treatment period (3 treatmentsessions) and at 4-week interval after the final session(total study duration, 8 weeks from treatment com-mencement). Standardized digital photographs weretaken before the treatment and at every follow-upvisit using identical camera settings (D70, Nikon,Tokyo, Japan) and lighting conditions. Clinical as-sessments were performed by two independentdermatologists (D. H. S. and J. Y. J.), and includedinflammatory and noninflammatory acne counts aswell as acne severity evaluations based on Cunliffe’sgrading system.13
Adverse reactions were recorded at every follow-up visit.
Skin sebum content measurementBoth cheeks (the most prominent area of the
zygoma) were selected for measurement area. Atleast 5 hours after washing the face with soap, sebumwas collected from each site on a plastic Sebumeterstrip (Skin-O-Mat, Cosmomed GmbH, Germany)using a constant pressure for 30 seconds. After theface had been washed, further face washing, use ofcosmetics or any other topical products were notpermitted until assessment.
Histopathology and immunohistologyFor the histological analysis, 2-mm punch biopsy
specimenswere obtained from the treated acne areasbefore treatment and at the final visit. The sections
were stained with hematoxylin-eosin (H&E) andMasson’s trichrome. Reviewing the H&E-stainedslide, the thickness of the perifollicular epidermisand stratum corneum was measured.
Tissue samples were processed to immunohisto-chemical staining for interleukin (IL) 8, transforminggrowth factor (TGF)-b1, matrix metalloproteinase(MMP)-9, toll-like receptor (TLR)-2, nuclear factor(NF)-kB, tumor necrosis factor (TNF)-a, and procol-lagen-1.
The severity of inflammation on the H&E stain-ing was ranked by using a 5-point scale, from 0(no inflammation) to 4 (very severe inflammation).The immunohistological staining intensities werealso ranked by using a 5-point scale from 0(unstained) to 4 (very intensively stained). Theskin biopsy and histopathological evaluations wereperformed by two independent dermatologists(J. S. H. and C. H. A.).
Patient’s subjective evaluation of effectivenessand pain
The patient subjective self-assessments of theacne severity and satisfaction with the treatmentwere performed using the visual analogue scale(VAS), which ranged from 0 (disease-free status) to10 (initial visit acne status). Accordingly, when theacne was aggravated compared to the initial visits,the VAS scores exceeded 10.
Pain intensityeassociated laser treatment was alsoassessed by means of a numeric scale ranging from 0to 10 (0: no pain and 10: worst imaginable pain).
Statistical analysisSPSS software (version 12.0, SPSS Inc, Chicago, IL)
was used throughout. The Friedman test was used todetermine the significance of the percent change ininflammatory and noninflammatory acne lesioncounts from baseline as well as changes in acneseverity, patient subjective evaluations, and histopa-thology. Differences between the results obtainedfrom the laser treatment side and the observationside were analyzed by using the Wilcoxon signed-rank test. Statistical significance was accepted at Pvalues less than .05.
RESULTSTwenty (4 men, 16 women) of 22 initially enrolled
subjects completed the study; two dropped out forpersonal reasons. The mean age of subjects was 25.4years; the subjects had Fitzpatrick skin types III-V.The patients were randomized to receive laser treat-ment on one half of the face, whereas the other sideof the face was observed.
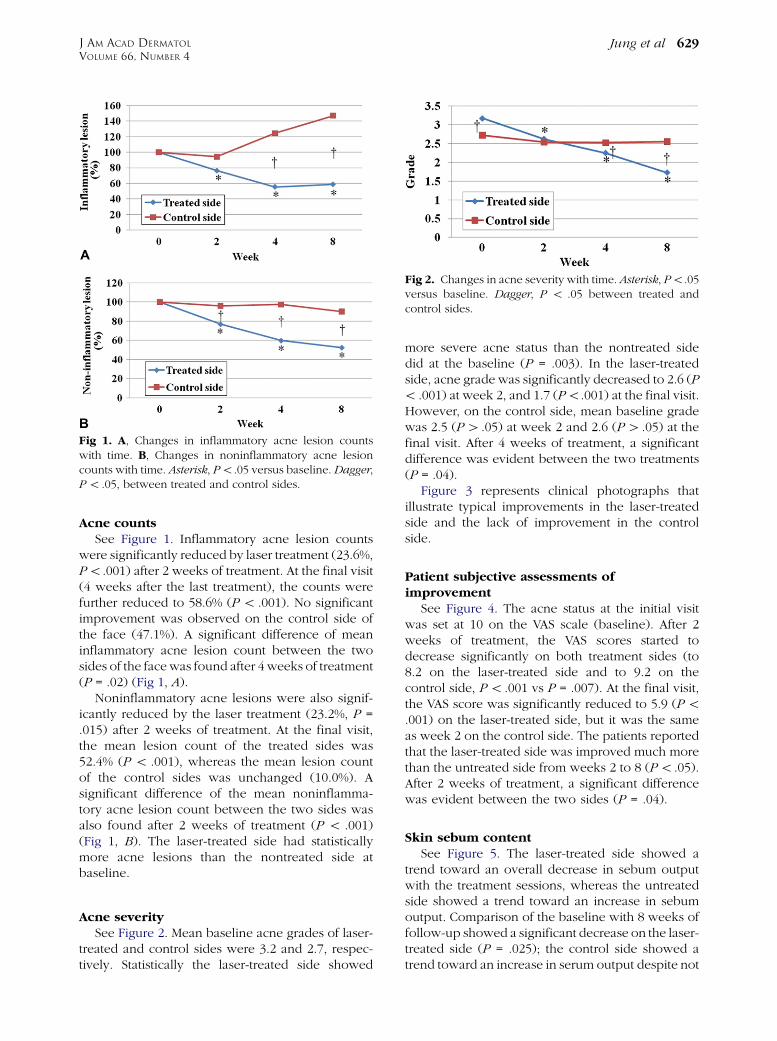
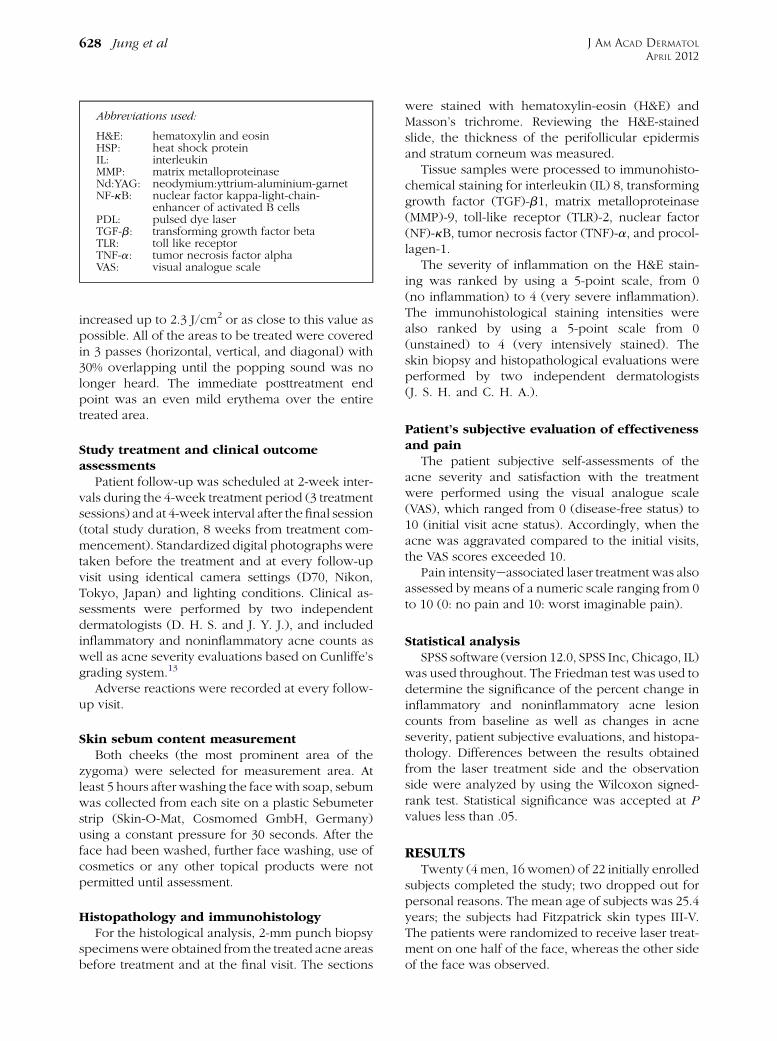
Fig 1. A, Changes in inflammatory acne lesion countswith time. B, Changes in noninflammatory acne lesioncounts with time. Asterisk, P\.05 versus baseline. Dagger,P\ .05, between treated and control sides.
Fig 2. Changes in acne severity with time. Asterisk, P\.05versus baseline. Dagger, P \ .05 between treated andcontrol sides.
J AM ACAD DERMATOL
VOLUME 66, NUMBER 4Jung et al 629
Acne countsSee Figure 1. Inflammatory acne lesion counts
were significantly reduced by laser treatment (23.6%,P\.001) after 2 weeks of treatment. At the final visit(4 weeks after the last treatment), the counts werefurther reduced to 58.6% (P\ .001). No significantimprovement was observed on the control side ofthe face (47.1%). A significant difference of meaninflammatory acne lesion count between the twosides of the facewas found after 4 weeks of treatment(P = .02) (Fig 1, A).
Noninflammatory acne lesions were also signif-icantly reduced by the laser treatment (23.2%, P =.015) after 2 weeks of treatment. At the final visit,the mean lesion count of the treated sides was52.4% (P \ .001), whereas the mean lesion countof the control sides was unchanged (10.0%). Asignificant difference of the mean noninflamma-tory acne lesion count between the two sides wasalso found after 2 weeks of treatment (P \ .001)(Fig 1, B). The laser-treated side had statisticallymore acne lesions than the nontreated side atbaseline.
Acne severitySee Figure 2. Mean baseline acne grades of laser-
treated and control sides were 3.2 and 2.7, respec-tively. Statistically the laser-treated side showed
more severe acne status than the nontreated sidedid at the baseline (P = .003). In the laser-treatedside, acne grade was significantly decreased to 2.6 (P\ .001) at week 2, and 1.7 (P\.001) at the final visit.However, on the control side, mean baseline gradewas 2.5 (P[ .05) at week 2 and 2.6 (P[ .05) at thefinal visit. After 4 weeks of treatment, a significantdifference was evident between the two treatments(P = .04).
Figure 3 represents clinical photographs thatillustrate typical improvements in the laser-treatedside and the lack of improvement in the controlside.
Patient subjective assessments ofimprovement
See Figure 4. The acne status at the initial visitwas set at 10 on the VAS scale (baseline). After 2weeks of treatment, the VAS scores started todecrease significantly on both treatment sides (to8.2 on the laser-treated side and to 9.2 on thecontrol side, P\ .001 vs P = .007). At the final visit,the VAS score was significantly reduced to 5.9 (P\.001) on the laser-treated side, but it was the sameas week 2 on the control side. The patients reportedthat the laser-treated side was improved much morethan the untreated side from weeks 2 to 8 (P\ .05).After 2 weeks of treatment, a significant differencewas evident between the two sides (P = .04).
Skin sebum contentSee Figure 5. The laser-treated side showed a
trend toward an overall decrease in sebum outputwith the treatment sessions, whereas the untreatedside showed a trend toward an increase in sebumoutput. Comparison of the baseline with 8 weeks offollow-up showed a significant decrease on the laser-treated side (P = .025); the control side showed atrend toward an increase in serum output despite not

Fig 3. A 29-year-old man with acne vulgaris: Control side (A and B), treated side (C and D),before treatment (A and C), without any treatment (B), and 4 weeks after 3 laser treatmentsessions (D). Clinical improvements were observed on the laser-treated side only.
J AM ACAD DERMATOL
APRIL 2012630 Jung et al
reaching statistical significance (P [ .05). After 4weeks of treatment, a significant difference wasfound between the two sides (P = .001).
Histopathology and immunohistologySee Figure 6. H&E staining scores demonstrated
reductions in inflammation after laser treatment. Atbaseline, the mean severity of inflammation was3.3, and it decreased to 1.6 (P = .011) at the finalvisit. At baseline, the mean thickness of the
perifollicular epidermis was 134.2 �m and that ofthe perifollicular stratum corneum was 25.9 �m. Atthe final visit, mean thicknesses were significantlydecreased to 97.3 �m (P = .018) and 18.4 �m (P =.028), respectively. The mean immunohistochemi-cal staining intensity for IL-8 (2.9 / 1.6, P = .017),MMP-9 (2.8 / 1.6, P = .027), TLR-2 (2.9 / 1.8, P =.017), NF-kB (2.8 / 1.8, P = 0.017), and TNF-a(2.3 / 1.4, P = .042) was reduced; these findingswere statistically significant.

Fig 4. Changes in patients’ subjective assessment of acneseverity (VAS) with time. Asterisk, P\ .05 versus baseline.Dagger, P\ .05, between the two sides.
Fig 5. Changes in sebum output level with time. Asterisk,P\ .05 versus baseline. Dagger, P\ .05 between the twosides.
Fig 6. Histopathologic inflammation severity and immu-nohistochemical staining intensities for nontreated andlaser-treated sides at baseline versus 4 weeks after 3 lasertreatments. Asterisk, P\ .05 versus baseline.
J AM ACAD DERMATOL
VOLUME 66, NUMBER 4Jung et al 631
Side effects and safetyNo severe adverse reactions were reported. All
patients reported mild transient erythema that dis-appeared 2 to 3 hours later. Fifteen patients (75%)reported mild dryness and desquamation of thetreated side; however, these findings were resolvedspontaneously within a few days. Though no re-gional anesthesia was used, patients reported thatthey felt only mild pain (mean VAS score of pain wasapproximately 2;3 at each session)
DISCUSSIONThe need for new and alternative treatments for
acne has led to the use of many types of lights andlasers. The mechanism of action relies on thewavelength, pulse width, and energy fluence ofthe lights and lasers. The visible light spectrum,including red and blue light3-5 and pulsed dye laser(PDL),6-9 can cause the photodestruction ofPropionibacterium acnes activating protoporphyrinIX. In addition, near- and mid-infrared lasers, suchas 1064-nm, 1320-nm, and 1450-nm lasers, cancause damage to the sebaceous glands penetratinginto the dermis.7,9,10,14
The 1064-nm Nd:YAG laser can penetrate thedermis deeply and cause diffuse heating of dermal
tissues without damaging the epidermis. The 1064-nm Nd:YAG lasers have been reported to be effec-tive in the treatment of acne scars, rhytides, andphotorejuvenation.15-18 However, the efficacy ofQ-switched 1064-nm Nd:YAG lasers on inflamma-tory and noninflammatory lesions of acne vulgarishave not been evaluated.
In the present study, it was shown that the dualmode of the quasi-long pulse and Q-switched 1064-nm Nd:YAG laser and a topically applied carbonsuspension were highly effective for treating boththe inflammatory and noninflammatory acne lesions.Significant reductions in the acne lesion counts wereobserved on the laser-treated side starting fromweek2 in the noninflammatory lesion and from week 4 inthe inflammatory lesion. Furthermore, these treat-ment effects were sustained at 4 weeks after the finaltreatment. The acne severity followed the samepattern of improvement. Although the treatmentside of the face was randomly allocated, the laser-treated side had significantly more acne lesions thanthe untreated side. However, the severity pattern ofacne lesions was reversed from week 4 for theinflammatory lesions and week 2 for the noninflam-matory lesions. The patient subjective assessments ofimprovement also showed greater satisfaction withthe laser-treated side than the untreated side.
The topical carbon suspension used containedpurified carbon particles; it served as an exogenousartificial chromophore. The 1064-nm Nd:YAG laserlight has been shown to be strongly absorbed bycarbon, in contrast to other cutaneous chromo-phores such as melanin. When the carbon suspen-sion is applied, the carbon particles are distributed tothe stratum corneum, and some of them also pene-trated into the hair follicles. When activated by thelaser light, the carbon undergoes a rapid temperatureincrease, thereby heating and damaging the folliclesand surrounding structures such as sebaceous gland.In this study, the 1064 nm-Nd:YAG laser system that

J AM ACAD DERMATOL
APRIL 2012632 Jung et al
combined a 300-microsecond quasi-long pulsewidth and 5-nanosecond pulse width was used.The first pass of the technique used was a relativelylong pulse of 300 microseconds. The first pass waswell absorbed and heated the applied carbon parti-cles on the skin with subablative low fluencies (\2.5J/cm2) without explosion. The carbon particles se-lectively absorb almost all the incident 1064-nmphoton energy and transform it into heat energy.The energy could be associated with nonspecificcoagulation or nonselective mild photothermolysis,in the epidermis, upper dermis, and the piloseba-ceous units. As a result, the first treatment coursemight inactivate P acnes by heat damage and alterthe acne patients’ immunobiological response to theP acnes. In addition, it might help to control thedermal inflammation associated with the inflamma-tory acne lesions. Since the sebaceous glands are alsothermally ablated, it might help reduce the nonin-flammatory acne lesions and sebum output. Thermalinjury to the dermis might affect the vasculature andinitiate a cascade of events that includes fibroblasticproliferation and dermal matrix rearrangement in-duced by various proteins, such as the heat shockprotein (HSP) 70, IL-6, TGF- b, and procollagen.7,8,19
In addition, it might help skin tightening and reducethe appearance of superficial acne scars.
The second pass was delivered at a Q-switchedpulse width of 5 nanoseconds, which produced highincident irradiance at 1.5 to 2.0 J/cm2. As a result, thestratum corneum and other parts of the upperepidermis were superficially ablated, which wasrepeated several times. The peeling effect likelycleans off the skin surface and the plugged pores.This is effective for the improvement of comedones.For the second pass, the Q-switched 1064-nmNd:YAG laser treatment might also increase collagensynthesis similar to the first pass.19
Sebum output was significantly decreased on thelaser-treated side at week 8, and a significant differ-ence was noted between the sides from week 4.Although the data are not presented, the sebaceousgland size and number were also decreased on thelaser-treated side. Many patients reported a sensationof dryness. Reduction of the sebum output levelsmight have been mainly caused by the first proce-dure using 300-microsecond pulse duration lasertreatment secondary to sebaceous gland damage andthe decrease of sebum output likely led to theimprovement of the noninflammatory acne lesions.
Both the perifollicular epidermal thickness andstratum corneum thickness were significantly de-creased to 72.5% (P = .018) and 71.0% (P = .028),respectively. They were measured using H&E slidesof the acne lesions. The peeling effect of the
Q-switched mode phase might lead to the correctionof hypercornification of follicular epithelium withthe development of a keratin plug blocking outflowof sebum to the skin surface.
The histology studies showed that the H&E-stained acne lesions had significantly reduced in-flammation on the laser-treated side; however, therewas no significant change on the control side.Immunostaining for IL-8, MMP-9, TLR-2, NF-kB,and TNF-a were significantly reduced. NF-kB is acritical transcription factor for up-regulation of manyproinflammatory cytokine genes, and it is activatedin inflammatory acne lesions in vivo.20-22 NF-kBinduces inflammatory cytokine genes, such asTNF-a and IL-1, which also stimulate the productionof secondary cytokines, such as IL-8. Increased IL-8expression, in the skin, has been reported to besignificantly associated with epidermal hyperplasia,follicular hyperkeratosis, and acne inflammation.7
AP-1, another important transcription factor associ-ated with inflammation and activation, inducesMMP-1, -8, -9,13,23-25 which degrade dermal matrix.P acnes triggers inflammatory cytokine responses inacne by activation of TLR-2.26 The decrease of theseproteins suggests the effectiveness of laser treatmentin this study at the level of gene transcription.
Patients felt only mild tenderness, dryness, andtransient redness without major complication. Thedowntime caused by this laser treatment wasminimal.
In conclusion, the dual mode of the quasi-longpulse and Q-switched Nd:YAG laser treatment as-sisted with a topically applied carbon suspensionacted quickly, and it was effective for treating notonly inflammatory but noninflammatory acne le-sions compared with the untreated side of the face.The histopathological findings correlated with theclinical acne grade and treatment response. Theresults showed sebum output reduction caused bysebaceous gland destruction, inflammatory cell andcytokine reductions, and decrease of perifollicularstratum corneum and epithelium. No serious sideeffects were observed. Therefore the dual mode ofthe quasi-long pulse and Q-switched Nd:YAG lasertreatment assisted with a topically applied carbonsuspension may provide a novel approach that issafe and effective for the acne.
REFERENCES
1. Leyden JJ. Therapy for acne vulgaris. N Engl J Med 1997;336:
1156-62.
2. Goodman G. Acne—natural history, facts and myths. Aust Fam
Physician 2006;35:613-6.
3. Na JI, Suh DH. Red light phototherapy alone is effective for
acne vulgaris: randomized, single-blinded clinical trial. Derma-
tol Surg 2007;33:1228-33.

J AM ACAD DERMATOL
VOLUME 66, NUMBER 4Jung et al 633
4. Papageorgiou P, Katsambas A, Chu A. Phototherapy with blue
(415 nm) and red (660 nm) light in the treatment of acne
vulgaris. Br J Dermatol 2000;142:973-8.
5. Sigurdsson V, Knulst AC, van Weelden H. Phototherapy of acne
vulgaris with visible light. Dermatology 1997;194:256-60.
6. Orringer JS, Kang S, Hamilton T, Schumacher W, Cho S,
Hammerberg C, et al. Treatment of acne vulgaris with a
pulsed dye laser: a randomized controlled trial. JAMA 2004;
291:2834-9.
7. Jung JY, Choi YS, Yoon MY, Min SU, Suh DH. Comparison of a
pulsed dye laser and a combined 585/1,064-nm laser in the
treatment of acne vulgaris. Dermatol Surg 2009;35:1181-7.
8. Seaton ED, Charakida A, Mouser PE, Grace I, Clement RM, Chu
AC. Pulsed-dye laser treatment for inflammatory acne vulgaris:
randomised controlled trial. Lancet 2003;362:1347-52.
9. Orringer JS, Kang S, Maier L, Johnson TM, Sachs DL, Karimipour
DJ, et al. A randomized, controlled, split-face clinical trial of
1320-nm Nd:YAG laser therapy in the treatment of acne
vulgaris. J Am Acad Dermatol 2007;56:432-8.
10. Glaich AS, Friedman PM, Jih MH, Goldberg LH. Treatment of
inflammatory facial acne vulgaris with combination 595-nm
pulsed-dye laser with dynamic-cooling-device and 1,450-nm
diode laser. Lasers Surg Med 2006;38:177-80.
11. Goldberg DJ, Whitworth J. Laser skin resurfacing with the
Q-switched Nd:YAG laser. Dermatol Surg 1997;23:903-6, dis-
cussion 906-7.
12. Sumian CC, Pitre FB, Gauthier BE, Bouclier M, Mordon SR. Laser
skin resurfacing using a frequency doubled Nd:YAG laser after
topical application of an exogenous chromophore. Lasers Surg
Med 1999;25:43-50.
13. O’Brien SC, Lewis JB, Cunliffe WJ. The Leeds revised acne
grading system. J Dermatol Treat 1998;9:215-20.
14. Trelles MA, Allones I, Luna R. Facial rejuvenation with a
nonablative 1320 nm Nd:YAG laser: a preliminary clinical and
histologic evaluation. Dermatol Surg 2001;27:111-6.
15. Friedman PM, Jih MH, Skover GR, Payonk GS, Kimyai-Asadi A,
Geronemus RG. Treatment of atrophic facial acne scars with
the 1064-nm Q-switched Nd:YAG laser: six-month follow-up
study. Arch Dermatol 2004;140:1337-41.
16. Keller R, Belda Junior W, Valente NY, Rodrigues CJ. Non-
ablative 1,064-nm Nd:YAG laser for treating atrophic facial
acne scars: histologic and clinical analysis. Dermatol Surg
2007;33:1470-6.
17. Lee DH, Choi YS, Min SU, Yoon MY, Suh DH. Comparison of a
585-nm pulsed dye laser and a 1064-nm Nd:YAG laser for the
treatment of acne scars: a randomized split-face clinical study.
J Am Acad Dermatol 2009;60:801-7.
18. Min SU, Choi YS, Lee DH, Yoon MY, Suh DH. Comparison of a
long-pulse Nd:YAG laser and a combined 585/1,064-nm laser
for the treatment of acne scars: a randomized split-face clinical
study. Dermatol Surg 2009;35:1720-7.
19. Alam M, Hsu TS, Dover JS, Wrone DA, Arndt KA. Nonablative
laser and light treatments: histology and tissue effects—a
review. Lasers Surg Med 2003;33:30-9.
20. Kang S, Cho S, Chung JH, Hammerberg C, Fisher GJ, Voorhees
JJ. Inflammation and extracellular matrix degradation medi-
ated by activated transcription factors nuclear factor-kappaB
and activator protein-1 in inflammatory acne lesions in vivo.
Am J Pathol 2005;166:1691-9.
21. Yamamoto Y, Gaynor RB. Role of the NF-kappaB pathway in
the pathogenesis of human disease states. Curr Mol Med 2001;
1:287-96.
22. Boone DL, Lee EG, Libby S, Gibson PJ, Chien M, Chan F, et al.
Recent advances in understanding NF-kappaB regulation.
Inflamm Bowel Dis 2002;8:201-12.
23. Angel P, Karin M. Specific members of the Jun protein family
regulate collagenase expression in response to various extra-
cellular stimuli. Matrix Suppl 1992;1:156-64.
24. Crowe DL, Tsang KJ, Shemirani B. Jun N-terminal kinase
1 mediates transcriptional induction of matrix metalloprotei-
nase 9 expression. Neoplasia 2001;3:27-32.
25. Birkedal-Hansen H, Moore WG, Bodden MK, Windsor LJ,
Birkedal-Hansen B, DeCarlo A, et al. Matrix metalloproteinases:
a review. Crit Rev Oral Biol Med 1993;4:197-250.
26. Kim J, Ochoa MT, Krutzik SR, Takeuchi O, Uematsu S, Legaspi
AJ, et al. Activation of toll-like receptor 2 in acne triggers
inflammatory cytokine responses. J Immunol 2002;169:
1535-41.