prospectus - final version
TRANSCRIPT

8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 1/19
RUNNING HEAD: Video Self Modeling for children with ASD
Video Self-Modeling and its Applications
For Intervention-Resistant Children with Autism
Nathan Missen
Duquesne University
8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 2/19
Video Self Modeling for children with ASD
Abstract
Autism Spectrum Disorder (ASD) is associated with a number of developmental delays.
Such delays often manifested as unconventional and/or inappropriate behaviors. These
behaviors serve to frustrate teachers, educators and parents alike. The behavior targeted
for this study was personal boundary violations. Three participants, each with ASD, took
part in an intervention aimed to address such behaviors through Video Self-Modeling
(VSM). VSM was chosen as it is congruent with several common characteristics of the
ASD population as well as Bandura’s theory of modeling (1977) and self-efficacy (1997).
A multiple baseline across subject design was utilized to assess the effect of the
intervention. Results indicate that VSM was effective in changing targeted behaviors for
these participants. Limitations and notions for future research are also noted.
8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 3/19
Video Self Modeling for children with ASD
Video Self-Modeling and its Applications
For Intervention-Resistant Children with Autism
Nathan Missen
Duquesne University
Autism Spectrum Disorders are characterized by a predictable pattern of
deficiencies in several developmental areas. Paucities in language utilization, social
interaction and overall communication skills are among the most prominent noted
(Buggey, 2005; Coyle, 2004; Sherer, 2001). Weaknesses in attentional capacity
(Courchenese et al., 1994), greater variability in affect regulation and affective coping
skills (Konstantareas & Stewart, 2006) as well as motivation (Koegel, Koegel &
McNerney, 2001) have also been observed. Such weaknesses often manifest as atypical
or unconventional behaviors: inappropriate proxemics, bizarre verbalizations, impaired
pragmatics, etc. Such behaviors serve to frustrate educators, family members and mental
health service providers alike in their efforts to address the needs of this particular
population.
In order to ameliorate the disadvantages theses children are exposed to, and
facilitate normalization and mainstreaming into the typical population, various forms of
treatment have been generated and implemented. Medical treatments have been reported
as being only marginally effective (Graham, Turk & Verhulst, 1999), while physiology
based approaches – such as the Gluten Free/Casein Free (GF/CF) diet and vitamin
therapy – and sensory based approaches – for example, music therapy and sensory
integration therapy – have produced mixed results, yet still maintain loyal followings
8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 4/19
Video Self Modeling for children with ASD
(Buggey et al., 1999). The most efficacious approach at this point seems to be a
psychological paradigm with a strong behaviorist component (Buggey et al., 1999).
One of the most published and well-researched psychobehavioral methodologies
is the Lovaas method (now more commonly known as Discrete Trial Training, which
falls under the umbrella of Applied Behavior Analysis). The popularity of this method
stems from a study published by Lovaas (1987), in which three groups of pre-schoolers
were exposed to varying intensities of behavioral intervention over a two-year period.
Those who received more intensive services (40 hours per week) compared to less
intensive services (10 hours per week) showed more substantial behavioral progress. In
addition, forty-seven percent of the intensive group passed the first grade with normally
developing peers. Drawbacks of this methodology are the long term, intensive nature of
the treatment, as well as retrospective criticisms of Lovaas’s study (Gresham &
MacMiliar, 1998)
Thus, the search for an effective and efficient method of intervention continues. A
relatively recent genre to emerge is that of video modeling (VM), and in particular, video
self modeling (VSM). Briefly, VM and VSM are both techniques aimed at producing
positive adaptive behavioral change; children watch models (either “self” or “others”)
demonstrating only the desired behavior and then subsequently imitating it (Bellini &
Akullian, 2007; Charlop-Christy, Le & Freeman, 2000; Coyle & Cole, 2004). VSM and
VM have proven to be an efficacious treatment for a multitude of skills and behaviors,
ranging from math skills (Buggey et al., 1999) to athletic performance (Bellini &
Akullian, 2007) and even selective mutism (Charlop-Christy et al., 2000). A recent meta-
analysis of schools based social skills interventions for children and young adults with
8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 5/19
Video Self Modeling for children with ASD
Autism yielded a mean Percentage of non-overlapping points (PND) of 80%, indicating
that VSM/VM is an ‘effective’ treatment (Bellini et al, 2007)
Why should video modeling be effective for children with autism? As previously
noted, individuals on the autistic spectrum display not only the core deficiencies in
language, social interactions and overall communication skills, but also concomitant
difficulties in attention and regulation. A number of suggestions have been generated to
address this: 1) VSM, in comparison with other intervention treatments, demands
relatively minimal attention and language output – two areas in which ASD individuals
typically struggle (videos are usually short, and participants are not required to produce
specific verbal responses), 2) children are directed to a small spatial area (i.e. a television
screen) to maximize focus and minimize distractions 3) a significant portion of people
with ASD are visually oriented learners, and reap relatively higher benefits from
interventions presented in this modality. A quote from Grandin (1996), an adult with
autism, illuminates this:
I think in pictures. Words are like a second language to me. I translate both
spoken and written words into full color movies, complete with sound, which run like a
VCR tape in my head. When somebody speaks to me, his words are instantly translated
into pictures (p.1)
While not representative of typical individual with Autism, Grandin’s testimonial
does give some insight into the think process of those on the spectrum, and why VM and
VSM may be effective for such individuals.
These suggestions, while possibly true in whole or in part, are not sufficiently
detailed or researched to such a degree as to be discrete theoretical entities. One postulate
8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 6/19
Video Self Modeling for children with ASD
that is sufficiently detailed that is also applicable to VSM is Bandura’s Social Learning
theory (Bandura, 1977). Bandura observed that children could accurately imitate the
actions of others through viewing their behavior, rather than personal experience. Ina
addition, actions were sometimes performed in settings other than the original (i.e.
generalization). Bandura also noted that attention and motivation were essential for
effective modeling. Children are more likely to pay attention to models they a) perceive
as competent and b) are similar to themselves in some manner, according to Bandura.
Another important component of Social Learning theory is self-efficacy. Self
efficacy refers to “…people’s beliefs about their capabilities to produce designated levels
of performance that exercise influence over events that affect their lives. Self-efficacy
beliefs determine how people think, feel, motivate themselves and behave” (Bandura,
1997). Individuals can obtain and enhance beliefs about self-efficacy thorough external
aid and support, but the most resilient and potent reinforcement of self-efficacy spring
from observations of one’s own success.
Thus, VM and in particular VSM, contain the components for a high probability
of success in addressing behavioral needs for children with ASD. It does not demand a
high intensity of processing from the participants, it is provided in a (possibly) preferred
modality and enhances self-efficacy through effective modeling. Furthermore, there is
literature to suggest that it is effective in addressing behavioral needs, and it is more time
efficient and cost-effective than other treatments with comparable timeframes (Bellini &
Akullian, 2007).
Purpose
The purpose of this study was threefold: (a) to validate the existing research base
8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 7/19
Video Self Modeling for children with ASD
through replication (b) to ascertain if VSM could effectively address challenging
behaviors for across students whom have proven to be resistant to a number of
interventions and (c) evaluate if VSM could generalize behaviors across settings.
Method
Participants
Three male children who attended a suburban public middle school were the focus
of this study. All children in this study met the DSM criteria for ASD, and were receiving
special education services when this study was initiated. A medical professional had
diagnosed each child independent of the researchers. To confirm their diagnosis and
gauge the extent of their abilities, the Childhood Autism Rating Scale – 2 nd edition
(CARS-2) and the Gilliam Autism Rating Scale (GARS-2) were utilized. Since this study
was directed at improving a particular aspect of social skills, the Social Responsiveness
Scale (SRS) was also administered to teachers. All parents were offered to complete the
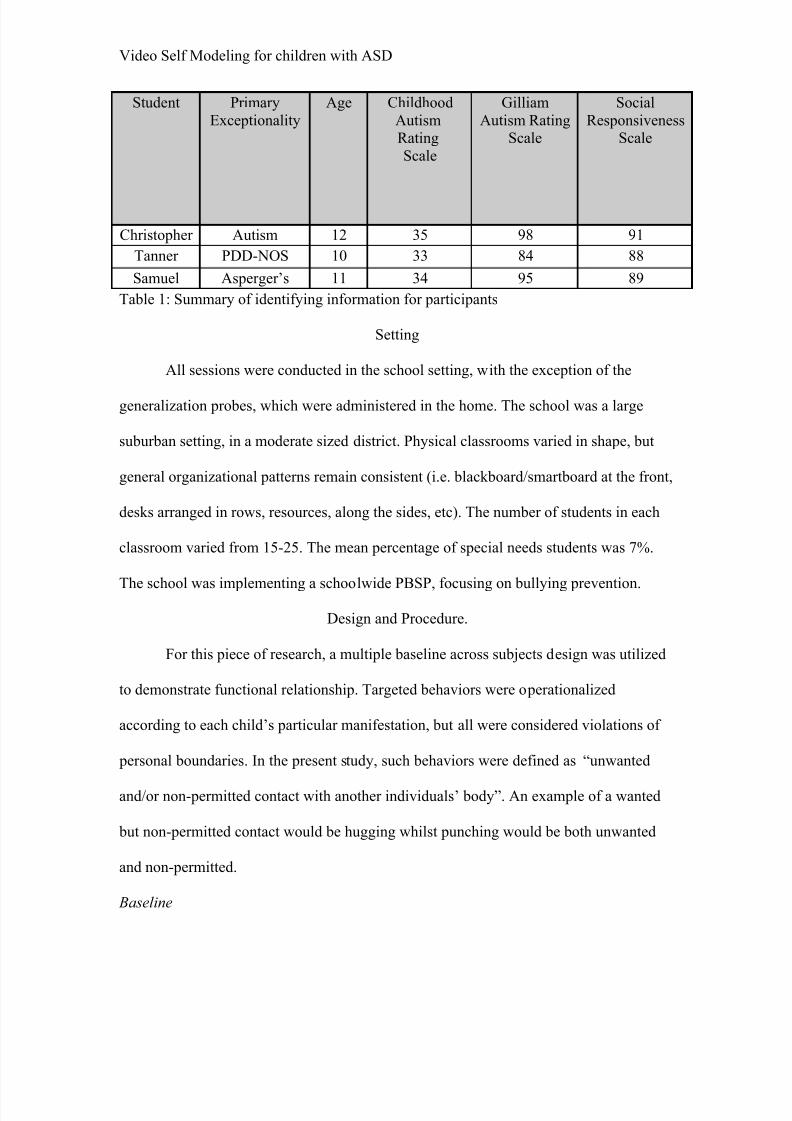
SRS but declined. Background information is summarized in Table 1.
Families of the children with ASD were contacted and invited to a meeting to
discuss the study. At this meeting, the VSM procedure was explained, and parents were
given the opportunity to ask questions and voice any concerns they had. Parents were
also asked open ended questions to determine what behaviors they would like to see
changed, which behaviors were the most important to change as well as what skills they
would like their children to learn. This was done in order to establish a degree of social
validity. Researchers also explained to the parents that generalization measures would be
carried in the home setting on a regular basis. Ultimately, all parents decided to consent
to participation in the study.
8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 8/19
Video Self Modeling for children with ASD
Christopher was a 12 year old white male who was diagnosed with Autism 2
years and 5 months of age by a psychologist under contract with a wraparound agency, as
well as Oppositional Defiance Disorder at age 5. His diagnosis was confirmed by a
CARS score of 35 and his GARS score of 98. Social skills deficit was exemplified in
Christopher’s SRS score of 91. Christopher was able to participate in the regular
education classroom setting with modified instruction and preferential seating. Behaviors
of concerns, according to teacher and parent responses, centre on inappropriate
proxemics; that is, Christopher violated personal boundaries. To be more specific, he
hugged without permission and often poked people repeatedly for attention. When
stressed, he ‘karate chopped’ teachers and students and headbutt them as well.
Christopher had received numerous interventions in the past, including peer monitoring
and contingent reinforcement. Interventions were discontinued after limited success. He
is currently on a Positive Behavior Support Plan (PBSP) and has an Individualized
Education Plan (IEP). Christopher also receives several hours a week of Therapeutic
Support Staff provided by a wraparound agency. Christopher lives with his mother and
younger brother.
Tanner was a 10 year old white male who was diagnosed with Pervasive
Developmental Disorder – Not Otherwise Specified (PDD-NOS) at 3 years, 7 months by
a pediatrician. Tanner was also diagnosed with Gastroesophageal reflux disease (GERD)
at 4 years. A CARS score of 33 combined with a GARS score of 84 confirmed his
diagnosis of PDD-NOS. An SRS score of 88 reflected Tanner’s social skill impairment.
Tanner was able to function in his classroom with variety of instructional and schedule
accommodations (e.g. regular sensory breaks and the use of a colored timer to assist in
8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 9/19
Video Self Modeling for children with ASD
waiting behaviors). Tanner’s area of concern was unsuitable touching behavior; in
particular, he would run his fingers through people’s hair as well as repeatedly stroke
clothing items made out of fur. Tanner has had numerous interventions in the past,
including behavior management focusing on appropriate replacement behavior (i.e. the
usage of a sensory fidget toy) as well as a contingent reinforcement system. Each
intervention met with limited success and was discontinued shortly thereafter. Tanner is
currently on a PBSP and has an IEP. He does not receive any services outside of school.
He lives with both of his parents as well as an older brother and younger sister.
Samuel was a 11 year old white male who was diagnosed with Asperger’s
Syndrome at age 4 years, 5 months by a hospital psychologist. He had carried a previous
diagnosis of PDD-NOS. Samuel also carried a diagnosis of Attention Deficit
Hyperactivity Disorder – Predominantly Inattentive type (ADHD-PI), which was given at
age 6. The diagnosis of Asperger’s was validated through a CARS score of 34 and a
GARS score of 95. Samuel’s lack of social skills was reflected in his SRS score of 89.
Samuel is able to participate in the general education classroom when provide with
behavioral and instructional modifications that specifically address his attentional
challenges. These interventions have met with continuing, but intermittent success.
However, there have been no interventions that have specifically targeted his undesirable
physical communication behaviors; such behaviors include squeezing, pinching, poking
as well as occasional punching. He has been referred to the office for squeezing a
female’s student breasts. No further disciplinary action was taken. Samuel is currently on
a PBSP and an IEP. Samuel lives at home with is father and older brother.
8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 10/19
Video Self Modeling for children with ASD
Student Primary
Exceptionality
Age Childhood
AutismRating
Scale
Gilliam
Autism RatingScale
Social
ResponsivenessScale
Christopher Autism 12 35 98 91
Tanner PDD-NOS 10 33 84 88
Samuel Asperger’s 11 34 95 89
Table 1: Summary of identifying information for participants
Setting
All sessions were conducted in the school setting, with the exception of the
generalization probes, which were administered in the home. The school was a large
suburban setting, in a moderate sized district. Physical classrooms varied in shape, but
general organizational patterns remain consistent (i.e. blackboard/smartboard at the front,
desks arranged in rows, resources, along the sides, etc). The number of students in each
classroom varied from 15-25. The mean percentage of special needs students was 7%.
The school was implementing a schoolwide PBSP, focusing on bullying prevention.
Design and Procedure.
For this piece of research, a multiple baseline across subjects design was utilized
to demonstrate functional relationship. Targeted behaviors were operationalized
according to each child’s particular manifestation, but all were considered violations of
personal boundaries. In the present study, such behaviors were defined as “unwanted
and/or non-permitted contact with another individuals’ body”. An example of a wanted
but non-permitted contact would be hugging whilst punching would be both unwanted
and non-permitted.
Baseline
8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 11/19
Video Self Modeling for children with ASD
During the baseline phase, observations were conducted on each student, five
times a week, until a consistent rate of behavior was determined and interrater reliability
established; this process took 2 weeks. 45 minute observations were carried out by the
researcher and a graduate student trained in observation methods. Data was collected in
the form of frequency counts, with parameters explicitly defined for each target behavior.
The setting for each student was their regular education classroom, as well as
lunchtime/recess. Interrater reliability was assessed by calculating percentage agreement;
dividing the total number of agreements by the total number of incidents. Interrater
reliability was assessed at the end of each week; a mean percentage of 95% was yielded.
Discrepancies were due to omission. Pre-generalization observations were also carried
out in the home setting twice a week; observation, duration and reliability procedures
were identical. An interrater reliability of 93% was found for home setting observations.
Video Production: Filming
The self as model tape was produced with the researchers and the participants. It
was decided to utilize a naturalistic, rather than scripted approach, as all the participants
were capable of producing the behaviors and that viewing themselves as models may be
more congruent with Bandura’s theory of self-efficacy. To desensitize the participants to
the video-making process, promotional videos of each class were made. All students from
each class were present in the videos. Approximately one week before the intervention
period, targeted recording procedures began, in which the researcher began filming the
child in the classroom and cafeteria settings. The aim of this was to capture enough
adaptive interactions bereft of personal boundary violations to produce a short film. All
filming was done using a Sony Digital Handicam.
8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 12/19
Video Self Modeling for children with ASD
Video Production: Post-Filming
After enough material was captured, the editing process began. All editing was
done using iMovie software on a MacBook Pro. Digital video material was edited so that
only adaptive, socially convention interactions were available for viewing; all target
behaviors were eliminated. The material was then further edited to give the appearance of
natural, smooth interactions. Finally, intertitles were added to the start and end of the
final version (e.g. “Let’s watch Christopher have a conversation” “Let’s see how Samuel
does at lunchtime” “Good Job, Tanner!”) along with flattering freeze-frames of each
student. Fading was used throughout the videos when an appropriate segue was not
filmed.
Intervention
After a 3 minute video was produced for each student, copies were distributed to
their teachers. The teacher and the student then viewed the video daily, in an empty
classroom, before the lessons started for the day. No other students were present during
the viewing. Initially, teachers drew attention to the student’s good behavior however,
this was discouraged so as not to endanger intervention reliability. Researchers were
present during 35% of Christopher’s interventions sessions, 37% for Tanner’s and 33%
for Samuel’s. Procedural integrity was calculated at 100%.
Intervention data was then collected three times a week. Data collection procedures were
identical to baseline. At the end of each week, the researcher as well as the graduate
student met to compare collection results. Interrater reliability was calculated with the
same method as in baseline; 96% agreement rate was yielded. Generalization data was
also collected in the home setting twice a week; interrater reliability was at 97%.
8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 13/19
Video Self Modeling for children with ASD
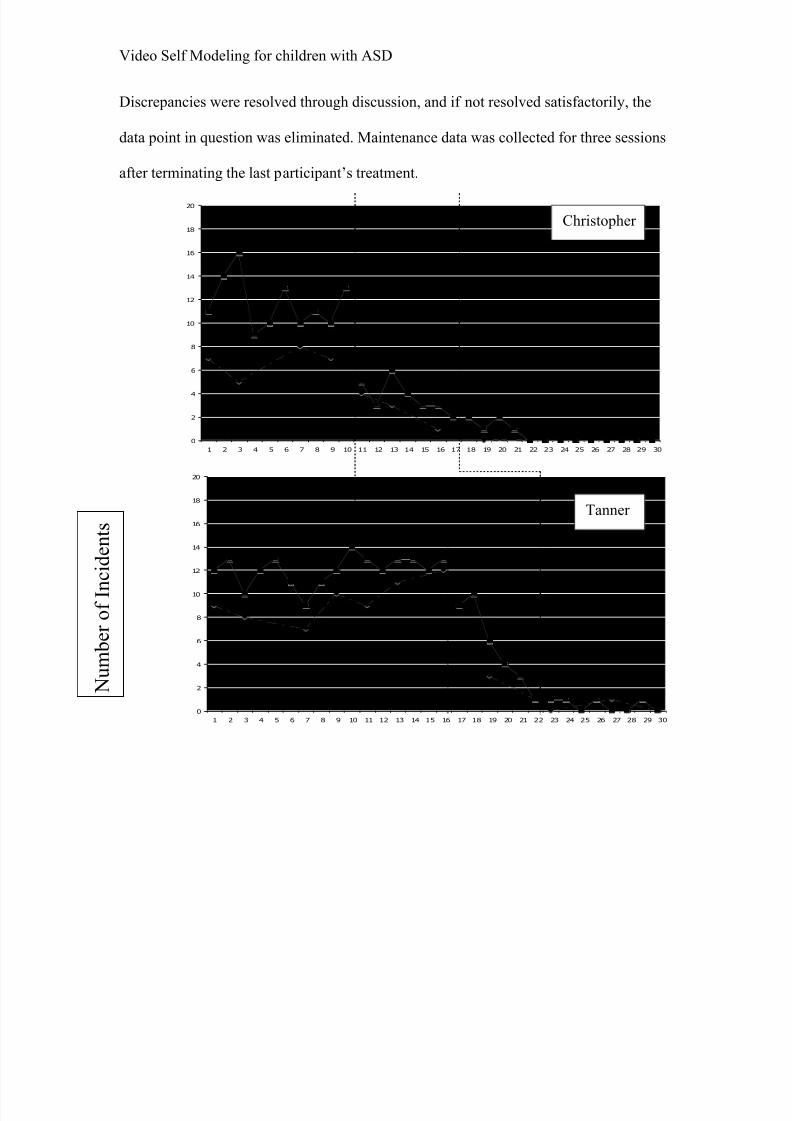
Discrepancies were resolved through discussion, and if not resolved satisfactorily, the
data point in question was eliminated. Maintenance data was collected for three sessions
after terminating the last participant’s treatment.
0
2
4
6
8
10
12
14
16
18
20
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
0
2
4
6
8
10
12
14
16
18
20
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
Numbero
fIn
ciden
ts
Christopher
Tanner
8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 14/19
Video Self Modeling for children with ASD
0
2
4
6
8
10
12
14
16
18
20
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
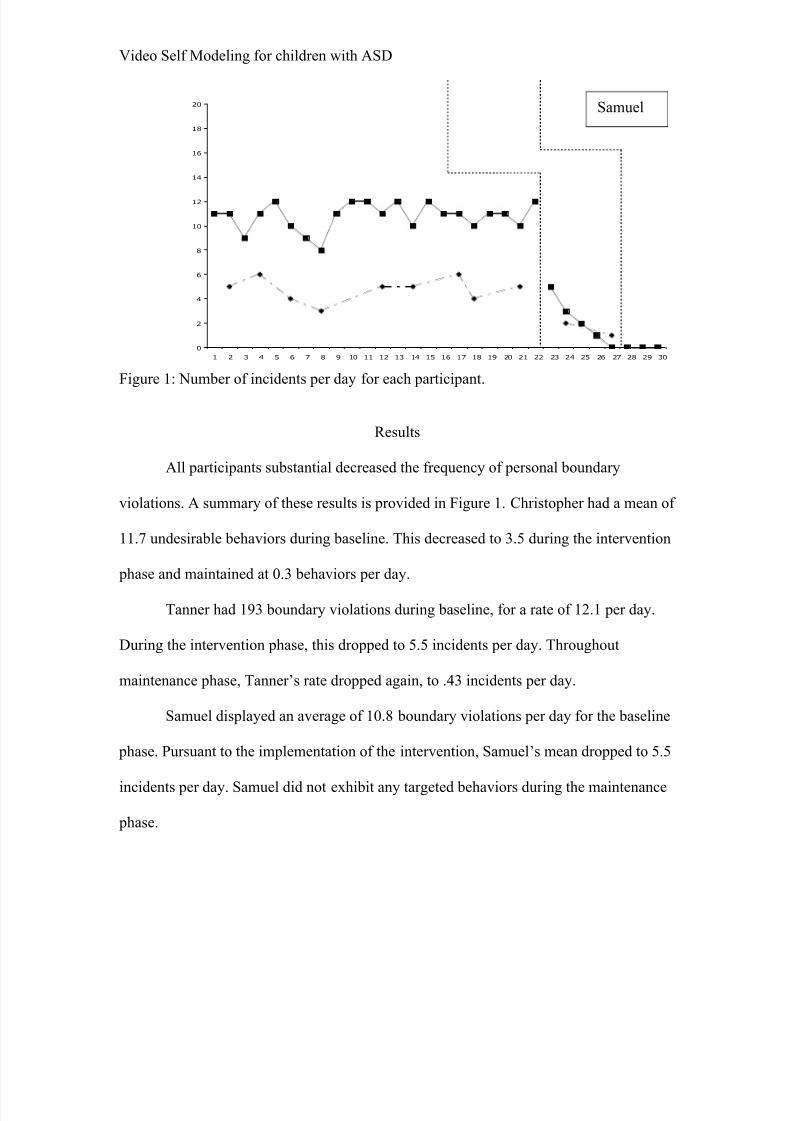
Figure 1: Number of incidents per day for each participant.
Results
All participants substantial decreased the frequency of personal boundary
violations. A summary of these results is provided in Figure 1. Christopher had a mean of
11.7 undesirable behaviors during baseline. This decreased to 3.5 during the intervention
phase and maintained at 0.3 behaviors per day.
Tanner had 193 boundary violations during baseline, for a rate of 12.1 per day.
During the intervention phase, this dropped to 5.5 incidents per day. Throughout
maintenance phase, Tanner’s rate dropped again, to .43 incidents per day.
Samuel displayed an average of 10.8 boundary violations per day for the baseline
phase. Pursuant to the implementation of the intervention, Samuel’s mean dropped to 5.5
incidents per day. Samuel did not exhibit any targeted behaviors during the maintenance
phase.
Samuel
8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 15/19
Video Self Modeling for children with ASD
Discussion
The implementation of video self modeling intervention to reduce personal
boundary violations with participants diagnosed with ASD and who were resistant to
other form of treatment seemed to be successful across settings and participants. Changes
observed in the classroom mirrored changes displayed in the home. These results support
previous finding concerning VSM
A follow up semi-structured interview with teachers indicated that the procedure
was positive overall. All teachers reported satisfaction with the outcomes of the study.
One teacher in particular noted that her classroom “felt more manageable” and that the
student had become a “role model” for other children in the class. Each teacher replied
that they would implement the intervention again if given another opportunity to do so.
Follow-up procedures with parents indicated a similar level of satisfaction. Each
parent was happy with the results of the intervention, and felt that it was both effective
and appropriate. A parent indicated that the change in her child was “practically life-
changing”. Another parent requested instructions and materials on how to generate their
own video tape to address other behavioral concerns.
Several other positive features of VSM also became apparent in this study. The
procedure is relatively non-intrusive; students did not miss any academic instruction due
to the implementation of this intervention. In addition, VSM is easy to implement and
does not require a substantial amount of time to carry out. A final positive aspect is that it
can produce change in a relatively short amount of time.
However, this study does have several limitations. A constant threat to single-
subject designs are the small number of participants, as well as the characteristics of each
8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 16/19
Video Self Modeling for children with ASD
participant. Every child in this study, whilst being diagnosed with a form of ASD, did not
display similar manifestations of ASD. Furthermore, each child also had differing
comorbid conditions. While this may point to the robustness of the intervention, it can
also mean that each participant may have been more (or less) able to respond to the
intervention. Further experiments with more homogenous participants may resolve this
limitation.
There was also the possibility of contamination in this study. Even though
teachers were briefed about confidentiality and impartiality, the filming took place with
the indirect participation and knowledge of other students. This may have resulted in
students changing their behavior responses to the participants.
A final limitation with this study is a possible Hawthorne effect, particularly in
the home setting. While researchers may have been able to blend in somewhat in the
school setting, it was more apparent in the home setting. There is a very real possibility
that participants may have modified their behavior due to the effect o f being studied. To
avoid this, one solution would be to have researchers investigate if parents could be
trained in observation procedures. However, this does raise bias issues.
In the future, it would be useful to assess the viability of VSM with a broader
range of functionality; for example, children who are non-verbal and ASD. In addition,
carrying out this intervention with an older age group may be enlightening, considering
the effects of peers and peer group dynamics; it may prove that peers are a more
efficacious model at that age. Finally, other individuals (such as guidance counselors,
teacher assistants, etc) who are more familiar with the school system may be in a better
position to implement and oversee this intervention. In general, it is important to continue

8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 17/19
Video Self Modeling for children with ASD
to modify interventions to suit the needs of this unique and important population in the
schools.
8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 18/19
Video Self Modeling for children with ASD
References:
Bandura, A. (1977 ). Social Learning Theory. New York, NY: General Learning
Press.
Bandura, A. (1997). Self-efficacy: The exercise of control . New York, NY: W.H.
Freeman.
Bellini, S., Peters, J., Benner, L., & Hopf, A. (2007). A Meta-Analysis of School
Based Social Skills Interventions for Children With Autism Spectrum Disorders.
Remedial and Special Education, 28(3), 153-162.
Bellini, S., & Akullian, J. (2007). A Meta-Analysis of Video Modeling and Video
Self-Modeling Interventions for Children and Adolescents With Autism Spectrum
Disorders. Exceptional Children, 73(3), 264-287.
Buggey, T. (2005). Video Self-Modeling Applications With Students With
Autism Spectrum Disorder in a Small Private School Setting. Focus on Autism and Other
Developmental Disabilities, Retrieved from ERIC database.
Buggey, T., Toombs, K., Gardener, P., & Cervetti, M. (1999). Training
responding behaviors in students with autism: Using videotaped self-modeling. Journal
of Positive Behavior Interventions, 1(4), 205-214.
Charlop-Christy, M.H, Le, L. & Freeman, K. A. (2000). A Comparison of Video
Modeling with In Vivo Modeling for Teaching Children with Autism. Journal of Autism
and Developmental Disorders, 30(6), 537-52.
Courchesne, E., Townsend, J., Akshoomoff, N., Saitoh, O., Yeung-Courchesne,
R., Lincoln, A., Haas, R., Schreibman, L. & Lau, L. (1994). Impairment in shifting
attention in autistic and cerebellar patients. Behavioral neuroscience, 108, 1-17
8/8/2019 Prospectus - Final Version
http://slidepdf.com/reader/full/prospectus-final-version 19/19
Video Self Modeling for children with ASD
Coyle, C., & Cole, P. (2004). A Videotaped Self-Modelling and Self-Monitoring
Treatment Program to Decrease Off-Task Behaviour in Children with Autism. Journal of
Intellectual and Developmental Disability, 29(1), 3-16.
Graham, P., Turk, J., & Verhulst, F. (1999). Child psychiatry: a developmental
approach, 3rd edn, New York, NY: Oxford University Press.
Grandin, T. (1996). Thinking in pictures and other reports from my life with
autism. New York, NY: Vintage.
Gresham, F.M., & MacMillar, D.L. (1998) Early intervention project: Can its
claims be substantiated and its effects replicated? Journal of Autism and Developmental
Disorders,28(1), 5-13.
Lovaas, O.I. (1987). Behavioral treatment and normal educational and intellectual
functioning in young autistic children. Journal of Consulting and Clinical Psychology,
55(1), 3-9.
Sherer, M., Pierce, K.L., Paredes, S., Kisacky, K.L.,; Ingersoll, B. & Schreibman,
L. (2001). Enhancing conversation skills in children with autism via video technology:
Which is better, 'Self' or 'Other' as a model? Behavior Modification, 25(1), 140-158.