prostate cancer - 2012 241,740 new cases 29 % of all new male cancer cases 28,170 deaths lifetime...
TRANSCRIPT

PROSTATE CANCER - 2012
• 241,740 new cases
• 29 % of all new male cancer cases
• 28,170 deaths
• Lifetime risk of prostate cancer 1:5
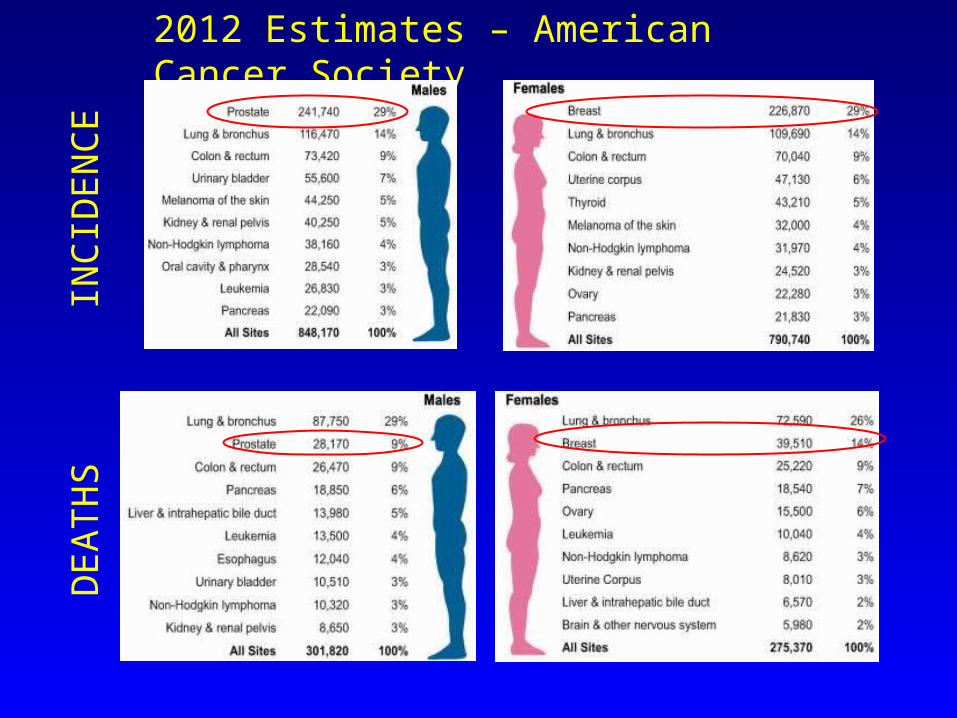
2012 Estimates – American Cancer Society
INC
IDE
NC
ED
EA
TH
S

PROSTATE CANCER
050,000
100,000150,000200,000250,000300,000350,000
# o
f p
atie
nts
19921994199619982000200220042006200820102012
Year
New CasesDeaths

PROSTATE CANCER
• 30% of men > 50 years old have CaP at autopsy
• Lifetime risk of malignancy in 50y/o - 42%
• Lifetime risk of CLINICAL CaP - 19 %
• Risk of dying from CaP - 2.9%
• UNIQUE DISCREPANCY OF PREVALENCE versus CLINICAL

U.S. Preventive Services Task Force(Draft report: 10/11/2011)
• Recommends against screening for prostate specific antigen
• Moderate or high certainty that no net benefit or harms outweigh benefits
• Grade D recommendation – discourage the use of this service- applies to all
healthy men.

U.S. Preventive Services Task Force(Draft report: 10/11/2011)
• Relied heavily on meta-analyses combining high and low quality evidence
• Used overall mortality rather than cancer specific mortality
• Considered only intention to treat
• Did not consider risk stratification or longer duration of followup

USPSTF on Prostate Ca Screening: FINAL REPORT
• Class D recommendation: Screening for prostate cancer should be actively discouraged
• Committee of primary care physicians; headed by pediatrician
• No Urological or Oncology consultants
• Same group: No mammograms age 40-50
Promulgated May, 2012

Effect of USPSTF Recommendation on Metastatic Prostate Ca
• SEER data 1983-1995 vs. 2006-2008
• Adj. for age, race, geographic variation
• Computed # of men who presented w/ M1 in SEER 9 registries area in 2008
• Expected/observed ratio M1 in 2008 = 3.1
• If USPSTF rec. applied to US population =
25,000 vs. 8000 CaP pts. with metastases
Scosyrev E…Messing EM. Cancer Online (July 30, 2012)

PLCO - CaP Screening Trial• 76,693 men• Randomized to annual screen vs. usual practice• At 7-10 years, death rate low and not different
Findings per 10,000 pt. yrs.
Screened
(38,343 pts.)
Control
(38,350 pts.)
Incidence of CaP
116
(2820 cancers)
95
(2322 cancers)
CaP Deaths 2.0 (50 deaths) 1.7 (44 deaths)
Andriole GL et al NEJM 360:1310, 2009.

PLCO - CaP Screening Trial
• Contamination (40-52%)
• # of patients “pre-screened”
• Short followup for mortality
• Wide confidence bars
• Percent of controls with higher stage/grade
Andriole GL et al NEJM 360:1310, 2009.

EORTC Randomized CaP Screening Study
• 162,387 men age 55-69 years• Screened every 4 years; cutpoint PSA > 3.0• * 20% reduction in CaP deaths ( p = 0.04)
Findings Screened
(72, 890 pts)
Control
(89,353 pts)
Incidence CaP 8.2% 4.8%
CaP Deaths 214* 326*
Schroder FH et al. NEJM 360:1320, 2009.

EORTC Randomized CaP Screening Study - Conclusions
• High rate of overdiagnosis (8.2 vs. 4.8%)
• PSA screening reduced CaP deaths (p =.04)
• Death risk difference 0.71/1000 men
• 1410 men screened/48 Rx to prevent 1 death
• Benefit of screening: Age 55-69 years
• 41% reduction in adverse features (p <0.001)
Schroder FH et al. NEJM 360:1320, 2009.

Göteborg CaP Screening Study
• Randomized population-based 1:1 (59 y/o)
• 20,000 men PSA testing every 2 years
• Median followup 14 years
• Dx CaP: 12.7% vs 8.2% (p < 0.0001)
• CaP deaths 0.56 in screened men (p=0.002)
• 293 screened; 12 dx to prevent 1 CaP death
Hugosson J et al . Lancet Oncol 11: 725, 2010.

CONCLUSIONS
• Careful analysis SUPPORTS screening for CaP
• Problem is overtreatment, not overdiagnosis
• Better predictors of aggressiveness would limit overtreatment
• Less morbid therapies would diminish problems with overtreatment
• Controversies about prostate cancer will persist


12-core Biopsy Technique

Gleason Pathologic Grading System
Gleason DF. In: Tannenbaum M, ed. Urologic Pathology: The Prostate.Philadelphia, Pa: Lea & Febiger; 1977:171-197.
X
X

Clinical T(umor) Stage
• T1a/b – Incidental CaP after TURP
• T1c - Discovered by PSA; no nodule
• T2a – Prostate nodule < ½ of 1 side
• T2b – Prostate nodule > ½ of 1 side
• T2c – Prostate nodules both sides
• T3a – CaP through capsule 1 or both sides
• T3b – Seminal vesicle invasion

RISK STRATIFICATIONRisk Grp. PSA Gleason T-stage
Low 10 & 7 & T1c/T2a
Intermed. 10-20 or 7 or T2b
High >20 or 8-10 or T2c /+
or > 2 ng in past year

PROSTATE CANCERMgt: LOCALIZED CaP
• Active Surveillance
• Radical Radiation Therapy
• Radical Prostatectomy
• Factors:• Age and health of patient
• Extent of disease
• Morbidity

Watchful Waiting - Localized CaP
Albertson PC et al. JAMA 293:2095-2101, 2005

Active Surveillance - Candidates
• > age 70-75 (?? Age 65 +)
• Intercurrent illness or comorbidities
• Gleason 3 +3 on few biopsies
• Low stage (T2 or <)
• Low PSA with slow rise on serial study
• Understand need for periodic biopsies

Watchful Waiting vs. RRP
Bill-Axelson et al NEJM 352:1977, 2005

PIVOT TRIAL: Observation vs. Radical Prostatectomy
• 731 men, randomized, 1994-2002• Mean age 67; Intention to treat analysis• Median followup: 10 years• All cause MR: 47% vs. 49.9%• CaP MR: 5.8% vs. 8.4% (p = 0.09)• ↓ all cause MR if PSA >10 and
possibly intermediate/high risk CaP
Wilt,TJ et al. NEJM 2012; 367:203

PIVOT TRIAL: Observation vs. Radical Prostatectomy
• Original goal 2000 pts
• Median age older (67 y/o); only 50% T1c
• VA population with ↑ comorbidities
• 25% of pts. for RRP did not undergo Rx
• 10% of pts. for obs. underwent RRP
• Bone mets in obs. - 10% vs. 4.7%
Wilt,TJ et al. NEJM 2012; 367:203

Open Radical Prostatectomy
• 2 ½ hour operation
• 2 day hospitalization
• Catheter x 1 week
• Recovery 3-4 weeks
• Palpation of prostate
http://www.orlive.com/brighamandwomens/videos

Robotic Radical Prostatectomy
• 2-3 hour operation
• 1 day hospitalization
• Catheter x 1 week
• Recovery 2-3 weeks
• Long learning curve (minimum 300)
• No palpation of prostate

Radical Prostatectomy
Advantages• Definitive therapy to
remove primary tumor• Stage dependent• Allows for pathological
staging • Better prognosis
determination• Nerve sparing• Psychological impact
Disadvantages• Major inpatient surgery
– Bleeding during surgery
• Incontinence• Persistent erectile
dysfunction• Bowel complications• Anastomotic stricture• Recovery period – loss of
human capital
Eastham JA, Scardino PT. Campbell’s Urology. 8th ed. Philadelphia, Pa: WB Saunders; 2002:3080,3091,3126.

External Beam Radiation Therapy (EBRT)
3D ConformalAdvantages• Efficacy equal to
prostatectomy at 5 years• Outpatient procedure• More precise treatment
target - less side effects than nonconformal
• Painless procedure • Allows escalation of RT
dose to 81 Gy• No loss in human capital
Disadvantages• Acute/chronic bowel
complications• Incontinence• Persistent erectile
dysfunction • Daily treatments for
7-8 weeks
D’Amico, AV, et al. Campbell’s Urology. 8th ed. Philadelphia, Pa: WB Saunders; 2002:3152.Zelefsky MJ, et al. J Urol. 2001;166:876-881.

Intensity Modulated RT (IMRT)
• Inverse treatment planning• Computer controlled RT intensity• Mathematical optimization technique utilized• Enables further delivery of minimal and maximal
dose RT vs 3-D EBRT• Less rectal complications than 3-D and conventional
EBRT• Allows escalation of the RT dose to 86.4 Gy• Limited availability
D’Amico, AV, et al. Campbell’s Urology. 8th ed. Philadelphia, Pa: WB Saunders; 2002:3155.Zelefsky MJ, et al. J of Urol. 2001;166:876-881.

Brachytherapy
Advantages • Efficacy approaching that
of EBRT or surgery (short term)
• Procedure completed in one session
• Outpatient procedure• Delivers higher doses
radiation over shorter period of time
Disadvantages • Urinary voiding symptoms• Rectal discomfort• Edema • Persistent erectile dysfunction• Migration of seeds • Variability of duration of action• Epidural or general anesthesia• Unknown long-term effectiveness
(10-year effectiveness)
D’Amico, AV, et al. Campbell’s Urology. 8th ed. Philadelphia, Pa: WB Saunders; 2002:3158.Grimm PD, et al. Int J Radiat Oncol Biol Phys. 2001;51:31-40.Beyer DC, et al. Radiother Oncol. 2000;57:263-267.Blasko JC, et al. Radiother Oncol. 2000;57;273-278.

MGT. of Localized CaP
• Optimal Rx of local disease controversial• Radical prostatectomy is the most proven
method for long term survival• Quality of life is an important consideration• Further improvements in survival depend on
development of effective adjuvant Rx