protocol title: would preoperative screening for carotid stenosis in
TRANSCRIPT
ACCEPTED VERSION
Thompson, Sarah Kathryn; Sullivan, Thomas Richard; Davies, Ruth A.; Ruszkiewicz, Andrew R. HER-2/neu gene amplification in esophageal adenocarcinoma and its influence on survival, Annals of Surgical Oncology, 2011; 18(7):2010-2017
© Society of Surgical Oncology 2011
http://hdl.handle.net/2440/66257
PERMISSIONS
http://www.springer.com/cda/content/document/cda_downloaddocument/Annals+Instructions+to+Contributors+February+2010+v1.pdf?SGWID=0-0-45-853237-p29577513
An author may self-archive an author-created version of his or her article on his or her own website. He or she may also deposit this version on his or her institution's and funder's (funder designated) repository at the funder's request or as a result of a legal obligation, including his or her final version, provided it is not made publicly available until after 12 months of official publication. He or she may not use the publisher's PDF version that is posted on the Annals website on SpringerLink for the purpose of self-archiving or deposit. Furthermore, the author may only post his or her version provided acknowledgement is given to the original source of publication and a link is inserted to the published article on the Annals-Springer website The link must be accompanied by the following text: "The original publication is available at the Annals website at www.springerlink.com/content/1534-4681.”
7th November 2011

HER-2/neu Gene Amplification in Esophageal Adenocarcinoma and Its Influence on Survival
Sarah K Thompson1 MD FRCSC, Thomas R Sullivan2 BMa&CompSc(Hons), Ruth Davies3
BMedSc, Andrew R Ruszkiewicz3 MD FRCPA
From the 1Discipline of Surgery, University of Adelaide, Adelaide, South Australia,
Australia, the 2Discipline of Public Health, University of Adelaide, Adelaide, South
Australia, Australia, and the 3Division of Tissue Pathology, SA Pathology, Adelaide, South
Australia, Australia
Supported by a 2008 Research Grant from the Society of American Gastroenterologists and
Surgeons (SAGES)
*Correspondence and reprint requests to:
Sarah Thompson MD, Department of Surgery, Level 5, Eleanor Harrald Building, Royal
Adelaide Hospital, Adelaide, South Australia 5000
Phone: +61 8 8222 5516 Fax: +61 8 8222 5896
Email: [email protected]
Running head: HER2 in Esophageal Cancer
Word count: 2,963
Key Words: esophageal cancer, esophagectomy, HER-2/neu gene amplification, c-erbB-2 gene
amplification, SISH, immunohistochemistry, HER-2/neu protein overexpression

HER2 in Esophageal Cancer 1
SYNOPSIS
The incidence and significance of HER-2/neu gene amplification in esophageal adenocarcinoma
is unknown. Only 16% of esophageal adenocarcinoma patients had HER2 gene amplification,
and its presence did not effect survival in this study.

HER2 in Esophageal Cancer 2
ABSTRACT
Introduction: HER-2/neu (c-erbB-2, HER2) gene amplification and protein overexpression
have been associated with poor prognosis in several solid tumors, including breast and gastric
cancer. Its incidence and significance in esophageal adenocarcinoma is unknown. Methods:
Tissue microarrays were successfully constructed from 89 paraffin-embedded archival specimens
of esophageal adenocarcinomas for HER2 gene amplification by silver-enhanced in situ
hybridization (SISH). No patients had undergone neoadjuvant therapy. Protein overexpression
was tested with immunohistochemistry (IHC) using automated immunostaining (Ventana
Benchmark). Incidence of HER2 positivity, correlation to clinicopathological variables in
esophageal cancer patients, and concordance between SISH and IHC were determined. Results:
True HER2 gene amplification was detected in 14 (16%) esophageal cancer specimens, and 92%
of those with high-level HER2 amplification showed positive HER2 protein overexpression. No
significant associations were found among gene amplification and clinicopathological factors.
Five-year survival rates were 57% for esophageal cancer patients with HER2 amplification
compared to 32% without, but the difference in overall survival was not significant (P=0.37).
The correlation between SISH and IHC was statistically significant (P<0.0001). Conclusion:
While molecular targeting may be possible for approximately 16% of esophageal
adenocarcinoma patients, HER2 oncogene amplification did not influence survival in this study.

HER2 in Esophageal Cancer 3
INTRODUCTION
Targeted molecular therapy in upper gastrointestinal cancer has become an increasingly popular
topic over the past few years. In part, this is due to rapid advances in our capability to
characterize tumor biology. Another consideration is our less-than-satisfactory ability to predict
a particular tumor’s response to neoadjuvant therapy. Esophageal adenocarcinoma is an example
of an aggressive cancer in which only one third of patients present with resectable disease. And
of this select group, the average 5-year survival is only 35 to 45%.1 The addition of neoadjuvant
therapy has significantly improved 5-year survivals, but much improvement is still needed.
Targeted molecular therapy may help in this regard.
Human epidermal growth factor receptor gene HER-2/neu (also known as c-erbB-2, now HER2)
was recognized as an important prognostic factor in breast cancer in 1987.2,3 However, its role in
other solid tumors is controversial.4-9 The published frequency of HER2 overexpression in
esophageal cancer ranges from 11 to 73%.10 Reports evaluating its significance are also varied in
their conclusions. Nevertheless an international randomized Phase III trial, evaluating the
survival benefit in gastric or gastro-esophageal junction cancer patients of the humanized anti-
HER2 monoclonal antibody (Trastuzumab), has just been published.11
The aims of our study were 1) to determine the frequency of HER2 gene amplification and
overexpression in esophageal adenocarcinoma; 2) to evaluate the association of HER2 gene
amplification with patient and tumor characteristics and patient survival; and 3) to examine the
correlation between amplification and expression of HER2 using silver-enhanced in situ
hybridization (SISH) and immunohistochemistry (IHC).

HER2 in Esophageal Cancer 4
MATERIALS AND METHODS
Patient Selection
All patients who had undergone a surgical resection for invasive upper gastrointestinal
adenocarcinoma were identified from an Adelaide-wide Esophageal Cancer Surgery audit
database, held at the Royal Adelaide Hospital in Adelaide, Australia. Since July 1997,
prospective follow-up data has been collected and stored in this database. Esophagectomy was
performed by a 2-surgeon synchronous Ivor-Lewis technique via a right antero-lateral
thoracotomy and an upper midline laparotomy, as described previously.12 A conservative lymph
node dissection (removal of all nodes adjacent to the tumor) was performed in all patients,
regardless of operative technique.13 Patients who underwent neoadjuvant therapy were
excluded from this study to obtain a homogeneous cohort of patients in terms of treatment
and to circumvent possible stage migration following chemoradiation therapy. The study
was approved by the Research Ethics Committee at the Royal Adelaide Hospital, Adelaide, South
Australia.
Tissue Microarrays
In a previous study1, we re-examined 240 esophageal cancer pathology specimens to determine
which variables could improve the accuracy of the TNM staging system. During this project, we
also selected appropriate paraffin blocks for construction of tissue microarrays which were used
in this study. To increase our sample size, additional esophageal adenocarcinoma patients
after January 2007 (up until December 2009) were included and appropriate paraffin

HER2 in Esophageal Cancer 5
blocks were selected for review. Specimen identification numbers were obtained from our
database, and the designated paraffin blocks were then retrieved from one of 3 pathology
laboratories: ClinPath Laboratories, Institute for Medical and Veterinary Science, and Adelaide
Pathology Partners. Tissue microarrays were constructed with 2 cores, each 1.0 mm in diameter,
from 2 paraffin blocks (i.e. 4 cores/patient). Representative cores of tumor were selected by
A.R.R. based on each block’s corresponding hematoxylin and eosin (H&E) stained sections.
Other studies have demonstrated the reliability of tissue microarrays in the evaluation of HER2
gene amplification in solid tumors including breast carcinomas.14
Double-Staining for HER2 Amplification and AE1/AE3 Cytokeratin Expression
Tissue microarray sections (4 µm) were cut, mounted on Superfrost Plus coated slides, labeled
and then placed on a fully automated immunohistochemistry (IHC) staining and In Situ
Hybridization (ISH) Ventana Benchmark XT (Roche Diagnostics) instrument. The sections were
incubated with ISH-protease 3 (Roche Diagnostics) for 8 min, washed with reaction buffer
(Roche Diagnostics) followed by denaturation of tissue DNA at 95 °C. The DNA probe for
Human Epidermal Growth Factor Receptor 2 (HER2) (Roche Diagnostics), labeled with
Dinitrophenol (DNP), was then added and hybridization occurred for 6 hours. Rabbit anti-DNP
(Roche Diagnostics) was used to detect the labeled probe followed by visualization with
ultraView silver in situ hybridization (SISH) detection kit (Roche Diagnostics) in accordance
with the manufacturer’s standard procedures.15
The section was then washed in reaction buffer followed by addition of Cell Conditioning 1
(CC1) solution (Roche Diagnostics) for 30 minutes. CC1 was removed, washed, and the primary
HER2 in Esophageal Cancer 6
mouse monoclonal epithelial antibody AE1/AE3 (Dako, Carpinteria, CA) for IHC was then
added for 36 min whilst the slide was heated to 37°C. The monoclonal antibody AE1/AE3 is
widely used because it recognizes a broad range of keratin subtypes expressed in esophageal
carcinomas.16 The ultraView™ Universal Alkaline Phosphatase RED kit (Roche Diagnostics),
used in accordance with the manufacturer’s recommendations, was used to detect the location of
the primary antibody AE1/AE3 followed by counterstaining with hematoxylin 11 (Roche
Diagnostics).
Evaluation of HER2 Gene Amplification
Evaluation of SISH hybridization was performed with conventional light microscopy by a
histopathologist (A.R.R.) and a medical scientist (R.D.). Both were blinded with respect to
patient identification, tumor characteristics on conventional histopathology, and HER2
protein expression. Gene amplification was assessed as per the Australian HER2 Advisory
Board criteria for single HER2 probe testing: diploid = 1 to 2.5 copies/nucleus in more than 50%
of tumor cells; polysomy = 2.5 to 4 copies/nucleus in more than 50% of tumor cells; equivocal
amplification = >4 to 6 copies/nucleus in more than 50% of tumor cells; low-level amplification
= 6 to 10 copies/nucleus in more than 50% of tumor cells; high-level amplification = >10
copies/nucleus in more than 50% of tumor cells. When using the Chromosome 17 probe, the
classification of not amplified was when the HER2/Chromosome 17 ratio was <1.8; equivocal
>1.8 and <2.2; and amplification was >2.2. HER2 and Chromosome 17 assays were performed
on contiguous sections allowing for the identification and exclusion of chromosome 17
polysomy.2,15

HER2 in Esophageal Cancer 7
Staining for HER2 Protein with Immunohistochemistry
Sections (4 µm) of tissue microarrays were cut, mounted on coated slides, labeled, and then
placed on the Ventana Benchmark XT (Roche Diagnostics) for detection of the HER2
oncoprotein. The sections were de-waxed then subjected to pre-treatment with CC1 for 30
minutes. Sections were then washed with reaction buffer followed by incubation with the rabbit
monoclonal primary antibody HER-2/neu (Clone 4B5, Roche Diagnostics) for 28 minutes. On
board detection using ultraView™ Universal DAB kit (Roche Diagnostics), used in accordance
with the manufacturer’s recommendations, was used to detect the location of the primary
antibody HER2 followed by counter stain with hematoxylin 11 (Roche Diagnostics).
Evaluation of HER2 Protein Expression
Evaluation and scoring of HER2-protein expression was performed according to the Dako
HercepTestTM scoring system for breast cancer. This scoring system has been validated for use in
gastric cancer with minor modifications:3,17 0/negative = staining or membranous reactivity in
<10% of cells; 1+/negative = faint membranous reactivity in >10% of cells or cells with
reactivity only in part of their membrane; 2+/equivocal = weak/moderate complete or basolateral
membranous staining in >10% of tumor cells; 3+/positive = strong complete or basolateral
membranous staining in >10% of tumor cells.
Statistical Analysis

HER2 in Esophageal Cancer 8
The presence of HER2 gene amplification and/or protein overexpression was correlated with
clinical outcome. Overall survival was calculated from the date of operation to July 15, 2010 (if
alive) or to the date of death (as recorded from the South Australian Cancer Registry) according
to the Kaplan-Meier method. Fisher’s exact tests were used to compare variables between
the two HER2 amplification groups (present/not present). Survival was compared between
the groups using a log rank test. Differences in survival between the HER2 groups were assessed
using a log-rank test. Correlation between SISH and immunohistochemistry was calculated using
the Kendall Tau-b correlation coefficient.18 Statistical significance was set at the 5% level.
Calculations were performed using SAS Version 9.2 (SAS Institute Inc., Cary, NC, USA).

HER2 in Esophageal Cancer 9
RESULTS
Patients
There were 336 patients who underwent a surgical resection for esophageal cancer between July
1997 and December 2009 identified from the database. The 30-d mortality rate was 4.8%. Of
these, 140 met inclusion criteria of an esophageal adenocarcinoma and no chemoradiotherapy
prior to surgical resection. A further 51 patients were excluded for various reasons, and we were
left with a study population of 89 patients (Figure 1).
Patients’ and tumor characteristics are listed in Table 1. The mean age was 63.9 years (95% CI
61.7-66.1 years). There were 74 men (83%) and 15 women (17%). The median time of patient
follow-up was 20.6 months (627 days). Complete follow-up was available for all 89 patients
with an overall 5-year survival rate of 35%, and a median survival of 22.1 months.
HER2 Amplification or Overexpression
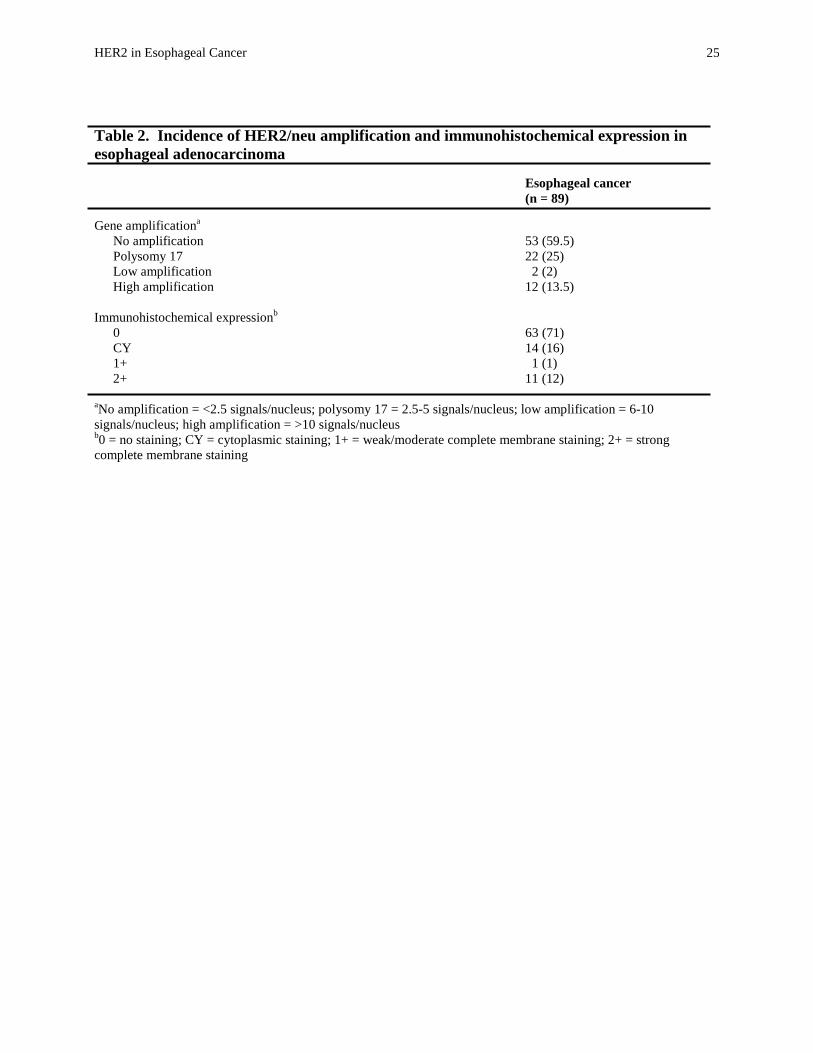
Fourteen esophageal cancer patients had HER2 gene amplification (Figure 2). Similar numbers
of patients had weak/moderate or strong membrane staining for HER2 protein overexpression
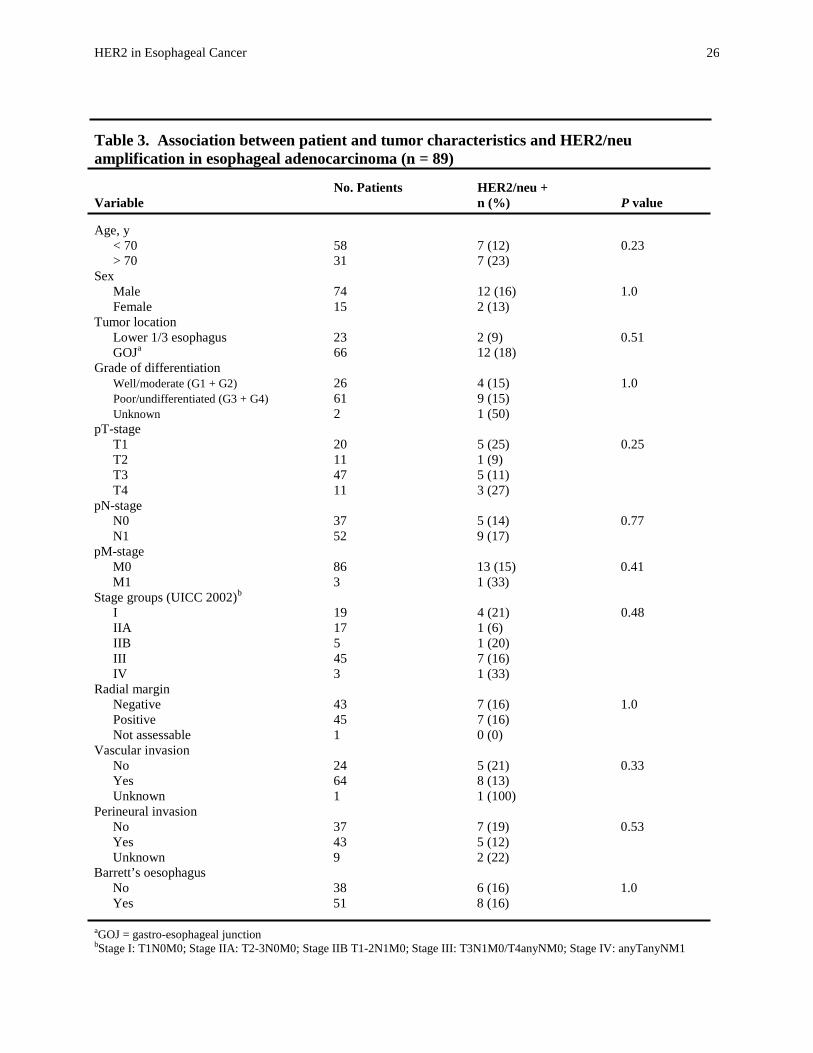
(Table 2). HER2 amplification was seen more commonly in pT1 (25%) and pT4 tumors
(27%) versus pT2 (9%) and pT3 (11%) tumors but this difference was not significant
(P=0.25). The presence of low or high HER2 amplification did not influence any other patient or
tumor characteristic (Table 3). Five-year survival rates were 57% (median, 68.9 months) for
esophageal cancer patients with HER2 amplification compared to 32% (median, 20.6

HER2 in Esophageal Cancer 10
months) without, but the difference in overall survival was not significant (P=0.37) (Figure
3). Similarly, in the Barrett’s cancer subset of patients, there was no significant difference in
overall survival between groups (P=0.29).
Correlation between HER2 Amplification and Overexpression
When SISH results were compared with HER2 immunohistochemical (IHC) data, eleven of
twelve cases (92%) with high-level gene amplification showed positive 3+ protein expression
(Table 4). The remaining case was negative for protein expression. One of two low-level gene
amplification cases was equivocal (2+) on IHC testing, while the other was negative (1+). None
of the diploid nor Polysomy 17 cases showed equivocal or positive protein expression. We did
not classify any cases in the equivocal category for HER2 amplification using SISH. Overall,
there was a significant correlation between SISH and immunohistochemistry for HER2 gene
amplification and expression (P<0.0001). The correlation coefficient between SISH and IHC
was 0.636 (moderate/strong association) (P<0.0001).

HER2 in Esophageal Cancer 11
DISCUSSION
Close to 16% of our esophageal cancer patients had HER2 gene amplification and overexpression
in their primary tumor. The previously quoted range of 11-73% for HER2 overexpression largely
originates from studies conducted in the 1990s, and using primarily immunohistochemistry.19-25
Some of these older studies concluded that HER2 protein overexpression corresponds with poor
survival.19,20 But more recently, studies have examined the frequency of HER2 gene
amplification in esophageal adenocarcinoma at the DNA level using either polymerase
chain reaction (PCR) or some form of in-situ hybridization (ISH).7,10,26-29 Our results
correspond to these latter studies (except one26 with a small sample size of 25) in which
frequencies of HER2 amplification are consistently lower and range from 12-24%.
Unlike one study in esophageal adenocarcinoma10, upon which current Herceptin-based trials
seem to be based, we found no correlation between the presence of HER2 amplification and
patient survival. Nor was there any correlation between HER2 amplification and
clinicopathological factors. Brien et al evaluated HER2 amplification with FISH in 63 Barrett’s
adenocarcinoma patients, and although they found no significant association between HER2
amplification and clinicopathological factors, they reported a significant association between its
presence and poorer survival.10 However, in this study, a low threshold of 4 or more signals
(rather than the currently accepted threshold of 6 or more signals15) per nucleus was used to
determine the presence of HER2 amplification.10 In addition, patients with chromosome 17
polysomy were not excluded. Aneuploidy of chromosome 17, usually involving an increase in
the number of chromosomal copies (i.e. polysomy), has been reported in approximately one third
of breast cancers. However, increased protein expression at the significant 3+ level does not

HER2 in Esophageal Cancer 12
seem to result from this mechanism because HER2 appears to remain normally regulated.26
Some investigators have suggested that controversy regarding the role of HER2 amplification and
its affect on survival might be explained by the failure to distinguish between true HER2 gene
amplification and chromosome 17 polysomy.26,30
In esophageal adenocarcinoma at least, our results seem to be the norm rather than the
exception.22-25,27,29 The lack of any apparent effect of HER2 amplification on patient
survival is supported by the absence of any association between HER2 amplification and
known poor prognostic pathological factors (i.e. pT-stage, pN-stage). Results of the ToGA
(Trastuzumab for Gastric Cancer) trial suggested that HER2-positive patients with
junctional gastro-esophageal cancers were potential responders to anti-HER2 monoclonal
antibody-based therapy.11 However, even the authors of this trial point out that the
survival benefit seen in the HER2-positive group may have been due to the presence of
HER2 overexpression alone rather than the result of HER2-targeted therapy.
Support for HER2 amplification as a prognostic and predictive factor in gastric adenocarcinoma
is also controversial with several studies showing a significant association31, and others not.32
The most recent of these encompassed 924 gastric cancer cases and is the largest study to date
showing that HER2 expression is not related to patient prognosis.33 Unfortunately, the authors
did not confirm their results with in situ hybridization techniques. Similarly, the importance of
HER2 amplification and expression in esophageal squamous cell carcinoma remains unclear.
Soares et al found that 37% of patients were HER2-positive with immunohistochemistry, while
only 19% of these were HER2-positive by FISH criteria. Those positive on FISH were shown to
have significantly poorer survival.5 However, Gibault et al reported overexpression of HER2 in

HER2 in Esophageal Cancer 13
only 2.8% of patients with esophageal squamous cell cancer, and they concluded that HER2
“appears to be of poor interest” as a potential therapeutic target in this type of esophageal
cancer.34
Aside from methodological factors (discussed in greater detail below), we may not have found a
survival advantage in HER2-negative cases due to the clonal divergence of primary tumors and
disseminated tumor cells (DTCs). Klein et al recently reported that HER2 gene amplification
was not conserved between primary tumors and DTCs (i.e. neither the presence nor absence of
HER2 amplification in the primary tumor was predictive for the HER2 status in DTCs of the
same patient). More importantly, they found that HER2 amplification in the primary tumor did
not affect survival, while HER2 amplification in DTCs led to significantly shorter survival
suggesting an increased dependence on HER2 signaling in the latter group.35 This too is
controversial however with Reichelt et al reporting the opposite finding.27 They found
perfect correlation of HER2 amplification using FISH between the primary tumor and
lymph node/distant metastases, and no effect on overall survival.
There are several limitations to our study. Perhaps foremost, our negative findings may relate
to sample size (type II statistical error). Our initial submission to the journal described the
results of 70 esophageal adenocarcinoma patients. We reported a P value of 0.06 when
comparing survival rates between those with HER2 amplification and those without (67%
vs. 28%, respectively). Upon request by the journal, we re-analyzed failed SISH specimens
in an attempt to increase our sample size. With a new total of 89 patients, we found similar
differences in survival (57% with HER2 amplificaiont vs. 32% without) but a much less

HER2 in Esophageal Cancer 14
convincing P value of 0.37 suggesting that HER2 amplification has no influence on survival
(at least in the negative sense).
Second, it is possible that by excluding patients who received neoadjuvant therapy, we
created a selection bias favoring less advanced tumors. However, 65% of the patients in
our study had advanced tumors (pT3 or pT4) due to the more infrequent use of
neoadjuvant therapy in the late 1990s. And in our previous study1, we found no significant
difference in survival between 116 patients treated with surgery alone, and 124 patients
treated with neoadjuvant therapy and surgery (5-year survival rates of 31% vs. 41%,
respectively) (P=0.125). Further studies are needed which include patients who have
received neoadjuvant therapy as well as those with metastatic disease.
As stated above, many prior studies have used immunohistochemistry (IHC) alone to determine
HER2 expression in upper gastrointestinal cancer. However, IHC is susceptible to inter-observer
variability and variations in testing protocols (such as insufficient or prolonged formalin
fixation).2,29 As well, a number of studies in breast cancer have indicated that gene amplification
is a more accurate predictor of survival than gene expression.31,36 Fluorescence in situ
hybridization (FISH) was included in the diagnostic algorithms for HER2 positivity in breast
cancer to reduce inter-observer error and confirm cases with equivocal HerceptTest staining (2+).
However, FISH is a costly technology requiring both a fluorescence microscope and digital
photography, and fluorescent signals will deteriorate over a few weeks.2,31 In addition, a recent
study by Rauser et al highlighted the unreliable detection of low-level HER2 amplification in
Barrett’s cancer using standard FISH in thin (4 μm) tissue sections.37

HER2 in Esophageal Cancer 15
Bright-field in situ hybridization such as silver-enhanced in situ hybridization (SISH) used in our
study is gaining popularity as it requires only a light microscope, and it is fully automated and
rapidly performed. Staining remains stable for a long period and it is relatively easy to interpret.2
An additional advantage over chromogenic in situ hybridization (CISH) is that HER2 and
chromosome 17 assays can be performed on contiguous slides allowing for exclusion of
polysomy rather than locus-specific amplification.2,31 High concordance has been found between
FISH and SISH in breast cancer studies (>95%), and high inter-observer concordance exists with
SISH (93-95%).2,36 We found high concordance between IHC and SISH in this study.

HER2 in Esophageal Cancer 16
CONCLUSION
HER2 gene amplification and overexpression was present in 16% of esophageal
adenocarcinomas. It did not appear to influence survival. Although a subset of esophageal
adenocarcinoma patients may meet the criteria for anti-HER2 monoclonal antibody therapy, it is
too early to suggest that such therapy may decrease disease-free recurrence rates and increase
long-term survival. Future studies should employ reproducible methodology using in situ
hybridization techniques. As well, research into targeted molecular therapies will have to take
into account characteristics of both the primary tumor and disseminated tumor cells.

HER2 in Esophageal Cancer 17
ACKNOWLEDGMENTS
This work was funded by a 2008 Research Grant from the Society of American
Gastroenterologists and Surgeons (SAGES). We would like to thank Professor Glyn Jamieson
for his constructive comments regarding the manuscript. We also appreciate the efforts of
Carolyn Lally, Lorelle Smith, Janet Pinno, and Nicky Ascott in managing the Royal Adelaide
Hospital Esophageal Cancer database.

HER2 in Esophageal Cancer 18
REFERENCES
1. Thompson SK, Ruszkiewicz AR, Jamieson GG, et. al. Improving the accuracy of TNM
staging in esophageal cancer: a pathological review of resected specimens. Ann Surg Oncol
2008; 15:3447-3458.
2. Penault-Llorca F, Bilous M, Dowsett M, Hanna W, Osamura RY, Rüschoff J, van de Vijver
M. Emerging technologies for assessing HER2 amplification. Am J Clin Pathol 2009;
132:539-548.
3. Walker RA, Bartlett JM, Dowsett M, et. al. HER2 testing in the UK: further update to
recommendations. J Clin Pathol 2008; 61:818-824.
4. Boone J, van Hillegersberg R, Offerhaus GJA, van Diest PJ, Borel Rinkes IHM, ten Kate
FJW. Targets for molecular therapy in esophageal squamous cell carcinoma: an
immunohistochemical analysis. Dis Esophagus 2009; 22:496-504.
5. Sato-Kuwabara Y, Neves JI, Fregnani JH, Sallum RA, Soares FA. Evaluation of gene
amplification and protein expression of HER-2/neu in esophageal squamous cell carcinoma
using Fluorescence in situ Hybridization (FISH) and immunohistochemistry. BMC Cancer
2009; 9:6.
6. Arrington AK, Dahlberg PS, Davydova J, Vickers SM, Yamamoto M. ERBB2 suppression
decreases cell growth via apoptosis in gastrointestinal adenocarcinomas. Surgery 2009;
146:213-219.
7. Dahlberg PS, Jacobson BA, Dahal G, Fink JM, Kratzke RA, Maddaus MA, Ferrin LJ.
ERBB2 amplifications in esophageal adenocarcinoma. Ann Thorac Surg 2004; 78:1790-
1800.

HER2 in Esophageal Cancer 19
8. Bekaii-Saab TS, Roda JM, Guenterberg KD, et. al. A phase I trial of paclitaxel and
trastuzumab in combination with interleukin-12 in patients with HER2/neu-expressing
malignancies. Mol Cancer Ther 2009; 8:2983-2991.
9. Lesnikova I, Lidang M, Hamilton-Dutoit S, Koch J. HER2/neu (c-erbB-2) gene amplification
and protein expression are rare in uterine cervical neoplasia: a tissue microarray study of 814
archival specimens. APMIS 2009; 117:737-745.
10. Brien TP, Odze RD, Sheehan CE, McKenna BJ, Ross JS. HER-2/neu gene amplification by
FISH predicts poor survival in Barrett’s esophagus-associated adenocarcinoma. Hum Pathol
2000; 31:35-39.
11. Bang YJ, Cutsem EV, Feyereislova A, et al. Trastuzumab in combination with
chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced
gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label,
randomised controlled trial. Lancet 2010; 376:687-697.
12. Aly A, Jamieson GG, Pyragius M, Devitt PG. Antireflux anastamosis following
oesophagectomy. ANZ J Surg 2004; 74:434-438.
13. Jamieson GG, Lamb PJ, Thompson SK. The role of lymphadenectomy in esophageal cancer.
Ann Surg 2009; 250:206-209.
14. Graham AD, Faratian D, Rae F, Thomas JS. Tissue microarray technology in the routine
assessment of HER-2 status in invasive breast cancer: a prospective study of the use of
immunohistochemistry and fluorescence in situ hybridization. Histopathology 2008; 52:847-
855.
15. Nitta H, Hauss-Wegrzniak B, Lehrkamp M, et. al. Development of automated brightfield
double in situ hybridization (BDISH) application for HER2 gene and chromosome 17
HER2 in Esophageal Cancer 20
centromere (CEN 17) for breast carcinomas and an assay performance comparison to manual
dual color HER2 fluorescence in situ hybridization (FISH). Diagn Pathol 2008; 3:41.
16. Scheuemann P, Hosch SB, Izbicki JR. Cytokeratins and other sensitive markers for
esophageal cancer and metastases. Dis Esophagus 2001; 14:85-90.
17. Hofmann M, Stoss O, Shi D, et. al. Assessment of a HER2 scoring system for gastric cancer:
results from a validation study. Histopathology 2008; 52:797-805.
18. Knight WE. A computer method for calculating Kendall’s Tau with ungrouped data. J Am
Stat Assoc 1966; 61:436-439.
19. Fléjou JF, Paraf F, Muzeau F, Fékété F, Hénin D, Jothy S, Potet F. Expression of c-
erbB-2 oncogene product in Barrett’s adenocarcinoma: pathological and prognostic
correlations. J Clin Pathol 1994; 47:23-26.
20. Nakamura T, Nekarda H, Hoelscher AH, Bollschweiler E, Harbec N, Becker K, Siewert
JR. Prognostic value of DNA ploidy and c-erbB-2 oncoprotein overexpression in
adenocarcinoma of Barrett’s esophagus. Cancer 1994; 73:1785-1794.
21. Jankowski J, Coghill G, Hopwood D, Wormsley KG. Oncogenes and onco-suppressor
gene in adenocarcinoma of the oesophagus. Gut 1992; 33:1033-1038.
22. Friess H, Fukuda A, Tang WH, et al. Concomitant analysis of the epidermal growth
factor receptor family in esophageal cancer: overexpression of epidermal growth factor
receptor mRNA but not of c-erbB-2 and c-erbB-3. World J Surg 1999; 23:1010-1018.
23. Hardwick RH, Barham CP, Ozua P, et al. Immunohistochemical detection of p53 and c-
erbB-2 in oesophageal carcinoma; no correlation with prognosis. Eur J Surg Oncol
1997; 23:30-35.

HER2 in Esophageal Cancer 21
24. Al-Kasspooles M, Moore JH, Orringer MB, Beer DG. Amplification and over-
expression of the EGFR and erbB-2 genes in human esophageal adenocarcinomas. Int J
Cancer 1993; 54:213-219.
25. Duhaylongsod FG, Gottfried MR, Iglehart JD, Vaughn AL, Wolfe WG. The
significance of c-erbB-2 and p53 immunoreactivity in patients with adenocarcinoma of
the esophagus. Ann Surg 1995; 221:677-684.
26. Walch A, Specht K, Bink K, et al. Her-2/neu gene amplification, elevated mRNA
expression, and protein overexpression in the metaplasia-dysplasia-adenocarcinoma
sequence of Barrett’s esophagus. Lab Invest 2001; 81:791-801.
27. Reichelt U, Duesedau P, Tsourlakis MC, et al. Frequent homogeneous HER-2
amplification in primary and metastatic adenocarcinoma of the esophagus. Modern
Pathology 2007; 20:120-129.
28. Geddert H, Zeriouh M, Wolter M, Heise JW, Gabbert HE, Sarbia M. Gene
amplification and protein overexpression of c-erb-b2 in Barrett carcinoma and its
precursor lesions. Am J Clin Pathol 2002; 118:60-66.
29. Tanner M, Hollmén M, Junttila TT, et al. Amplification of HER-2 in gastric carcinoma:
association with Topoisomerase IIα gene amplification, intestinal type, poor prognosis
and sensitivity to trastuzumab. Ann Oncol 2005; 16:273-278.
30. Rosenberg CL. Polysomy 17 and HER-2 amplification: true, true, and unrelated. J Clin
Oncol 2008; 26:4856-4858.
31. Yan B, Yau EX, Bte Omar SS, Ong CW, Pang B, Yeoh KG, Salto-Tellez M. A study of
HER2 gene amplification and protein expression in gastric cancer. J Clin Pathol 2010;
63:839-842.

HER2 in Esophageal Cancer 22
32. Gravalos C, Jimeno A. HER2 in gastric cancer: a new prognostic factor and a novel
therapeutic target. Ann Oncol 2008; 19:1523-1529.
33. Grabsch H, Sivakumar S, Gray S, Gabbert HE, Müller W. HER2 expression in gastric
cancer: rare, heterogeneous and of no prognostic value – conclusions from 924 cases of two
independent series. Cell Oncol 2010; 32:57-65.
34. Gibault L, Metges JP, Conan-Charlet V, et. al. Diffuse EGFR staining is associated with
reduced overall survival in locally advanced oesophageal squamous cell cancer. Br J Cancer
2005; 93:107-115.
35. Klein CA, Stoecklein NH. Lessons from an aggressive cancer: evolutionary dynamics in
esophageal carcinoma. Cancer Res 2009; 69:5285-5288.
36. Francis GD, Jones MA, Beadle GF, Stein SR. Bright-field in situ hybridization for HER2
gene amplification in breast cancer using tissue microarrays: correlation between
chromogenic (CISH) and automated silver-enhanced (SISH) methods with patient outcome.
Diagn Mol Pathol 2009; 18:88-95.
37. Rauser S, Weis R, Braselman H, et. al. Significance of HER2 low-level copy gain in
Barrett’s cancer: implications for fluorescence in situ hybridization testing in tissues. Clin
Cancer Res 2007; 13:5115-5123.

HER2 in Esophageal Cancer 23
FIGURE LEGENDS
Figure 1. Study population.
Figure 2. Formalin-fixed, paraffin-embedded esophageal adenocarcinoma tissue microarrays.
Representative specimen (a, hematoxylin & eosin stain) showing no HER2 protein expression (b,
AE1/AE3 immunohistochemical stain), and no HER2 gene amplification (c, silver-enhanced in
situ hybridization). Second example (a, hematoxylin & eosin stain) showing 3+/positive HER2
protein expression (b, AE1/AE3 immunohistochemical stain), and high-level HER2 gene
amplification (c, silver-enhanced in situ hybridization).
Figure 3. Overall 5-year survival according to the presence or absence of HER2 gene
amplification for 89 patients who underwent surgical resection of esophageal adenocarcinoma.
Although there was a difference in 5-year survival rates between these 2 groups : 57% vs. 32%, it
was not significant (P=0.37).
HER2 in Esophageal Cancer 24
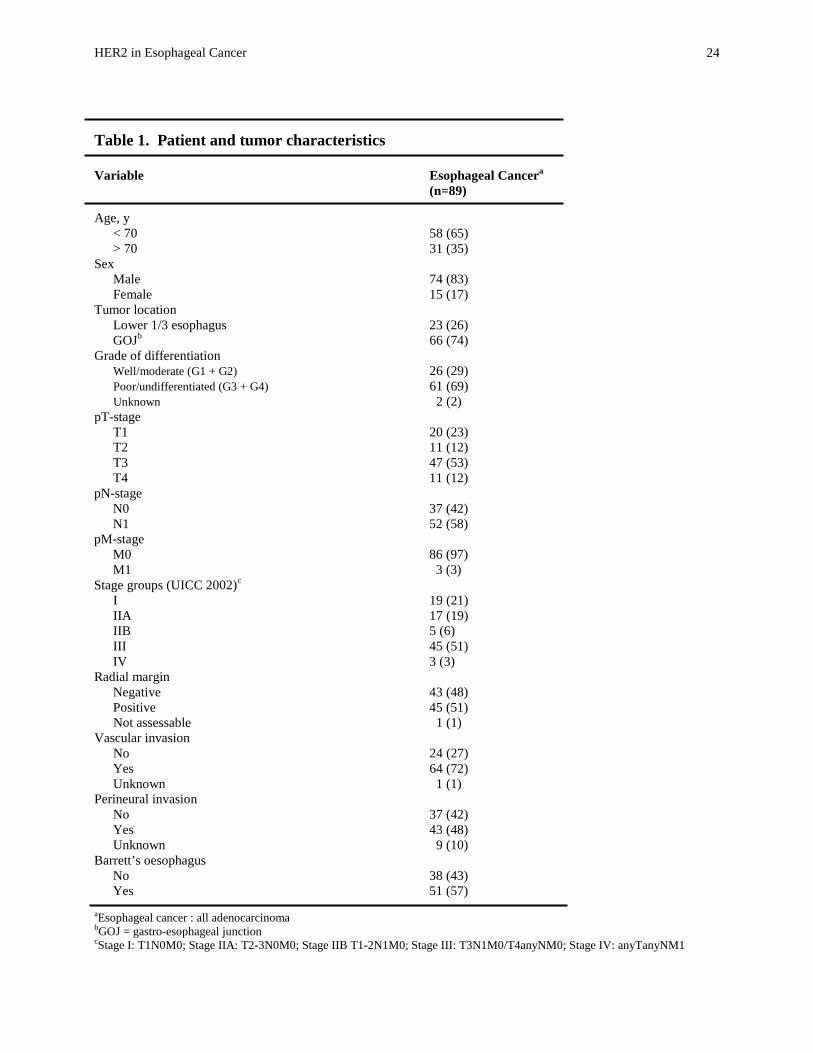
Table 1. Patient and tumor characteristics Variable Esophageal Cancera (n=89)
Age, y < 70 58 (65) > 70 31 (35) Sex Male 74 (83) Female 15 (17) Tumor location Lower 1/3 esophagus 23 (26) GOJb 66 (74) Grade of differentiation Well/moderate (G1 + G2) 26 (29) Poor/undifferentiated (G3 + G4) 61 (69) Unknown 2 (2) pT-stage T1 20 (23) T2 11 (12) T3 47 (53) T4 11 (12) pN-stage N0 37 (42) N1 52 (58) pM-stage M0 86 (97) M1 3 (3) Stage groups (UICC 2002)c I 19 (21) IIA 17 (19) IIB 5 (6) III 45 (51) IV 3 (3) Radial margin Negative 43 (48) Positive 45 (51) Not assessable 1 (1) Vascular invasion No 24 (27) Yes 64 (72) Unknown 1 (1) Perineural invasion No 37 (42) Yes 43 (48) Unknown 9 (10) Barrett’s oesophagus No 38 (43) Yes 51 (57) aEsophageal cancer : all adenocarcinoma bGOJ = gastro-esophageal junction cStage I: T1N0M0; Stage IIA: T2-3N0M0; Stage IIB T1-2N1M0; Stage III: T3N1M0/T4anyNM0; Stage IV: anyTanyNM1
HER2 in Esophageal Cancer 25
Table 2. Incidence of HER2/neu amplification and immunohistochemical expression in esophageal adenocarcinoma
Esophageal cancer (n = 89)
Gene amplificationa No amplification 53 (59.5) Polysomy 17 22 (25) Low amplification 2 (2) High amplification 12 (13.5) Immunohistochemical expressionb 0 63 (71) CY 14 (16) 1+ 1 (1) 2+ 11 (12) aNo amplification = <2.5 signals/nucleus; polysomy 17 = 2.5-5 signals/nucleus; low amplification = 6-10 signals/nucleus; high amplification = >10 signals/nucleus b0 = no staining; CY = cytoplasmic staining; 1+ = weak/moderate complete membrane staining; 2+ = strong complete membrane staining
HER2 in Esophageal Cancer 26
Table 3. Association between patient and tumor characteristics and HER2/neu amplification in esophageal adenocarcinoma (n = 89) No. Patients HER2/neu + Variable n (%) P value
Age, y < 70 58 7 (12) 0.23 > 70 31 7 (23) Sex Male 74 12 (16) 1.0 Female 15 2 (13) Tumor location Lower 1/3 esophagus 23 2 (9) 0.51 GOJa 66 12 (18) Grade of differentiation Well/moderate (G1 + G2) 26 4 (15) 1.0 Poor/undifferentiated (G3 + G4) 61 9 (15) Unknown 2 1 (50) pT-stage T1 20 5 (25) 0.25 T2 11 1 (9) T3 47 5 (11) T4 11 3 (27) pN-stage N0 37 5 (14) 0.77 N1 52 9 (17) pM-stage M0 86 13 (15) 0.41 M1 3 1 (33) Stage groups (UICC 2002)b I 19 4 (21) 0.48 IIA 17 1 (6) IIB 5 1 (20) III 45 7 (16) IV 3 1 (33) Radial margin Negative 43 7 (16) 1.0 Positive 45 7 (16) Not assessable 1 0 (0) Vascular invasion No 24 5 (21) 0.33 Yes 64 8 (13) Unknown 1 1 (100) Perineural invasion No 37 7 (19) 0.53 Yes 43 5 (12) Unknown 9 2 (22) Barrett’s oesophagus No 38 6 (16) 1.0 Yes 51 8 (16) aGOJ = gastro-esophageal junction bStage I: T1N0M0; Stage IIA: T2-3N0M0; Stage IIB T1-2N1M0; Stage III: T3N1M0/T4anyNM0; Stage IV: anyTanyNM1

HER2 in Esophageal Cancer 27
Table 4. Comparative data for SISH HER-2/neu gene copy status and HER-2 IHC (amended HercepTest) in esophageal adenocarcinoma
IHCa 0 IHC 1+ IHC 2+ IHC 3+ (n=63) (n=14) (n=1) (n=11)
Diploid (n = 53) 44 9 0 0 Polysomy 17 (n = 22) 18 4 0 0 Low amplification (n = 2) 0 1 1 0 High amplification (n = 12) 1 0 0 11 SISH = silver in situ hybridization; IHC = immunohistochemistry a0 = negative, 1+= faint or incomplete membrane staining; 2+ = weak/moderate membranous staining; 3+ = strong membranous staining