provider press - bluecrossmn · 2020. 2. 12. · provider press icd-10 coding update and final...
TRANSCRIPT

Provider Press
ICD-10 CODING UPDATE AND FINAL REMINDERS Note The information below was also published on August 5 2015 in Provider Bulletin P30-15 The ICD-10 federal compliance date of October 1 2015 is almost here The help you with your final preparations for the impacts of ICD-10 Blue Cross and Blue Shield of Minnesota and Blue Plus (Blue Cross) is publishing some new information and final reminders New Information bull BeginningOctober12015whensubmittingproceduresforpriorauthorization(PA)
requestsyoumustsubmittheICD-10diagnosiscodePArequestssubmittedbeforeOctober12015mustbesubmittedwiththeICD-9diagnosiscode
bull ProviderPolicyandProcedureManualreferencestoICD-9codeswillbeupdatedtoreflect the appropriate ICD-10 codes We anticipate completing the updates no later thanSeptember12015Toaccessthemanualgotoprovidersbluecrossmncom and select ldquoForms amp Publicationsrdquo then ldquomanualsrdquo
bull ReimbursementpolicyreferencestoICD-9codeswillbeupdatedtoalsoreflecttheappropriateICD-10codesTheupdateswillbecompletedpriortoOctober12015ToaccessreimbursementpolicydocumentsgototheldquoToolsandResourcesrdquosectionofprovidersbluecrossmncom
bull ProvidershavingdifficultywithclaimsubmissionsoftwareafterthecompliancedatemayusethefreeofchargeclaimsubmissionentryontheAvailityproviderportaltosubmittheir claims This process does require registration but is easy to use and is fully tested for ICD-10 functionality For more information visit availitycom
Coding RemindersCode all diagnosis and procedures to the greatest level of specificity possible Medical record documentation must support the code selection on the claim transactions
General Billing RemindersDue to the impacts to our members Blue Cross will not extend the timely filing deadlines or advance payments to any providers who fail to comply with the ICD-10 mandate Claims mustbesubmittedtimelytoBlueCrossAnyclaimsreceivedafterthetimelyfilingperiodspecifiedinyourParticipatingProviderServiceAgreementwillbedeniedasproviderliabilityPlease work with your software vendor and clearinghouse to make sure you are ready to submit ICD-10 coded claims by the compliance date
Onlyoneversionofthecodeset(ICD-9orICD-10)isallowedpersubmittedclaimICD-9onlymustbeusedonclaimswithservicedatesandinpatientdischargedatespriortoOctober12015ICD-10onlymustbeusedonclaimswithservicedatesandinpatientdischargedatesOctober12015andafter
ClaimswithservicedatesspanningOctober12015mustbesubmittedastwoseparateclaims transactions with the exception of inpatient services Please refer to CMS MLN Matters publication for more information
Provider Press
Provider Press is a quarterly newsletter available online at providersbluecrossmncom Issues are published in March June September and December
Inside preview
Front cover article 1 4 FYI2-3 Coding Corner 4 HealthLiteracy5 QualityImprovement6-9Medical and Behavioral HealthPolicyUpdate10-22
Sept 2015 Vol 19 No 3
Provider information
continued on page 4
September 2015 2
Provider Demographic Change Form
The Provider Demographic Change form needs to be completed when your address phone number hospital affiliation or office hours change Go to providersbluecrossmncom and enter ldquoprovider demographic change formrdquo in the search window to obtain the form Completed forms can be
Emailed to ProviderDatabluecrossmncom
Faxed to (651) 662-6684
Mailed to Blue Cross and Blue Shield of Minnesota PDOR316 POBox64560 StPaulMN55164-0560
FYI
PUbLICATIONS AvAILAbLE ONLINE
ThefollowingisalistofQuickPointsandBulletinspublishedfromJune2015toAugust2015thatareavailableonlineatprovidersbluecrossmncom AsareminderBulletinsaremailedtoallparticipatingprovidersaffectedbytheinformation Quick Points are available only on our website unless noted otherwise in the bottom left corner of the publication
QUICk POINTS TITLEQP13-15 Provider Cost Data Update
QP14-15 Update to Buprenorphine and BuprenorphineNaloxone (BunavailtradeSuboxoneregZubsolvreg)PriorAuthorizationandQuantityLimitCriteria
QP15-15 Update to NuvigilregArmodafinilProvigilregModafinilPriorAuthorizationandQuantity Limit Criteria
QP16-15 ICD-10 Provider Partner Testing Summary
QP17-15 WhoisBlueLinkTPA
bULLETINS TITLEP21-15 NewClaimsFilingRulesforAirAmbulanceProviders
P22-15 July2015HCPCSCodeUpdates
P23-15 MedicalNecessityReviewCriteriaUpdateforMHCPSubscribers
P24-15 MentalHealthServicesRequirementforMinnesotaHealthCarePrograms(MHCP) Subscribers
P25-15 NewDrug-relatedPriorAuthorizationCriteriaProproteinConvertaseSubtilisinKexinType9(PCSK9)InhibitorsforFamilialHypercholesterolemiaPAwithQuantityLimit
P26-15 UpdateonKneeArthroplastyCriteriaforMHCPSubscribers
P27-15 Non-CoveredMedicareServicesandOrganizationDeterminationUpdateforPlatinumBlue Subscribers
P28-15 Facility Place of Service Changes
P29-15 MedicareTrainingandEducationRequirements
P30-15 ICD-10CodingUpdateandFinalReminders
P31-15 Common Carrier and Special Transportation Providers Billing Code Updates
FYIHELPFUL PHONE NUMbERSBLUELINE (voice response unit) (651) 662-5200 or 1-800-262-0820
BlueCardreg member benefits or eligibility 1-800-676-BLUE (2583)
FEPreg (voice response unit) (651) 662-5044 or 1-800-859-2128
Availity 1-800-282-4548
Provider services (651) 662-5200 or 1-800-262-0820
Please verify these numbers are correctly programmed into your office phones
September 2015 3
FYI
PROvIDER MANUAL UPDATES The following is a list of Blue Cross and Blue Shield of Minnesota provider manuals thathavebeenupdatedfromJune2015toAugust2015Asareminderprovidermanuals are available online at providersbluecrossmncom To view the manuals select ldquoForms amp publicationsrdquo then ldquomanualsrdquo Updates to the manuals are documented in the ldquoSummary of changesrdquo section of the online manuals
MANUAL NAME
CHAPTER NUMbER AND TITLE
CHANGE
Provider Policy and Procedure Manual
Chapter 11 Coding Policies and Guidelines Medical Services section
Topic of ldquoNon-covered Tobacco Treatmentsrdquo was deleted
Provider Policy and Procedure Manual
Chapter 11 Coding Policies and Guidelines Public Programs section
Content change to Transportation Services (Formerly titled Special Transportation)
Provider Policy and Procedure Manual
Allchapters ReferencestoICD-9codeswillbeupdatedtoreflect the appropriate ICD-10 codes Note We anticipate completing all the updates nolaterthanSeptember12015
REALLy SIMPLE SyNDICATION Not all provider publications are mailed out to providers The majority of our informational Quick Points and the quarterly Provider Press are posted to our website for providers to view Providers frequently ask us how they can be advised when new publications are added to the website at providersbluecrossmncom
ProviderscansignuptogetRSS(reallysimplesyndication)feedsofourlatestnewsreleasesandupdatestoprovider-relatedformsandpublicationsAsampleofthefeeds that can be requested includes
bull Bulletinsbull Forms admin updates and contractingbull Forms credentialingbull Formspre-certificationandpre-authorizationbull Manualsbull Provider Press
bull Quick Points
Go to providersbluecrossmncomandenterldquoRSSrdquointhesearchwindowtolearnmoreaboutRSSQuestionsaboutRSSfeedsspecifictoyourinternalsystemsshould be directed to your IT support area
2015 HOLIDAy SCHEDULEProvider services will be closed on the following days
in2015
Monday September 7
ThursdayNovember26
FridayNovember27
ThursdayDecember24
FridayDecember25
With the exception of the dates stated above representatives answering the provider services numbers are available to assistyou8amto5pmMonday through Thursday and9amto5pmonFriday
September 2015 4
CodINg CorNer
REPLACEMENT CLAIM REMINDERWhendoIneedareplacementclaimWellareyoumakingchangestoaclaimthatwaspreviouslyprocessedIfyesyouwillneedtosendinareplacementclaimThisincludes
bull changing a date of service
bull adding or changing a procedure
bull adding or changing a diagnosis
bull removing a modifier
bull adding a modifier
Note that when adding modifiers -24 -25 -57 -59 -78 andor 79 medical notes supporting the modifier also need to be sent with the replacement claim
SeeProviderBulletinP28-14datedOctober12014formoreinformation
26 OR TC USENot every code in particular radiology codes has a professional component (reported witha-26modifier)andtechnicalcomponent(reportedwithandashTCmodifier)ForexampleCPTcode77387isldquoGuidanceforlocalizationoftargetvolumefordeliveryof radiation treatment delivery includes intrafraction tracking when performedrdquo This code does not have a professional or technical component Thus if it is submitted with acomponentmodifier(-26or-TC)itwillbedeniedbecauseaninvalidmodifierwasappended to the service
ICD-10 CODING UPDATE AND FINAL REMINDERS continued from page 1
httpwwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesDownloadsSE1325pdf
UsethecorrectcodequalifierindicatingwhetherthecodeisICD-9orICD-10forthecode setbeingreportedintheHIPAAtransaction
Reviewyourclaimacknowledgementreportstimelytoensureclaimshavebeencorrectlysubmitted and accepted by Blue Cross Claims rejected on these reports must be corrected and submitted again Claims rejected on acknowledgment reports are not considered submitted for timely filing purposes
AdditionalinformationisavailableundertheICD-10compliancelinkonourwebsiteatprovidersbluecrossmncom
Questions
If you have questions please contact provider services at (651) 662-5200 or 1-800-262-0820
THE HCPCS ARE COMING THE HCPCS ARE COMING Itrsquos not just the ICD codes that will be the coding stars onOctober12015HCPCScodes are updated as well on that fall date Blue Cross will publish a Provider Bulletin closer to the October12015effectivedate that provides more details
September 2015 5
HeALTH LITerACY
Try both aleve 2pills bid with flexeril at hs
Asahealthcareprofessionalyouprobablyunderstandexactlywhatthedoctorwhosentthismessage was saying Take 2 Aleve pills 2 times a day and take 1 Flexeril pill at bedtime But the patient who received it had no idea what the doctor was saying Most people donrsquot Clear communication increases patient safety and adherence to treatment plans
OctoberishealthliteracymonthHerearesomeactivitiesthatyourpracticecliniccanincorporate to help make a healthy difference in your patientrsquos lives
Use the Teach Back method also known as the ldquoshow-merdquo technique to ensure that patients (or care takers) understand their treatment plan and what they need to do Think aboutdoingasimpleteachbacktrainingatyourpracticeduringthemonthofOctoberClickhere for a program ready to use from the Minnesota Health Literacy Partnership
Promote the Ask Me 3 program from the National Patient Safety Foundation which focuses onpatientunderstandingof3simplequestions
1)Whatismymainproblem
2)WhatdoIneedtodo
3)Whyisitimportantformetodothis
You can use these questions to help guide the information you provide during visits with your patients Make sure they know the answer to these questions before they leave your office ConsiderdisplayingpostersandbrochuresthroughoutyourofficeduringOctobertoremindstaffaboutthe3questionsFormoreinformationonAskMe3clickhere
Review your own patient education materials Select a few of the patient education materials that you commonly use in your practice and review them using one of the health literacytoolsfromtheOfficeofDiseasePreventionandHealthPromotionPerhapsformateam to review the pieces together Click hereforresourcesOrcontactusifyouwantacopy of the tool used at Blue Cross
To learn more about building a culture of health literacy and using plain language at your practice please send an email to AlishaOdhiambobluecrossmncomAdditionalinformationcan also be found online at httphealthliteracymnorg
September 2015 6
QuALITY ImproVemeNT
PCC QUALITy OF CARE COMPLAINT REPORTProviders are required to complete the Blue Plus Quality of Care Complaint report forallwrittenandverbalcomplaintsfromBluePlusPrepaidMedicalAssistanceProgram and MinnesotaCare subscribers on a quarterly basis per Minnesota Department of Health regulations Complaints logged at the provider offices are to be investigated and resolved by the providerrsquos office whenever possible
ThesecomplaintsarereportedtoBluePlusinJanuaryAprilJulyandOctoberfor the preceding three months The Primary Care Clinic (PCC) must submit a quarterly report even if the facility does not receive any complaints for the quarter YourcontractoutlinestheproceduresrequiredforyourQualityofCare(QOC)PCCcomplaint reporting adherence agreement
Complaints should no longer be directed to the attention of a single designated personSendingyourPCCQOCcomplaintreportformtoanysourcenotlistedbelowmaydelaytheprocessingofyourPCCQOCcomplaintreport
ToaccessthePCCBluePlusQualityofCareComplaintReportFormgoto providersbluecrossmncom and select ldquoForms amp publicationsrdquo then ldquoforms - clinical operationsrdquo
Submit quarterly PCC QOC reports using one of these methods
Email pcccomplaintbluecrossmncom
Secure fax line (651) 662-4004
Mail Blue Plus AttnQualityHealthManagementDept R472 POBox64179 StPaulMN55164-0179
UTILIzATION MANAGEMENT STATEMENTUtilizationManagement(UM)decisionmakingisbasedonlyonappropriatenessofcareand service and on existing coverage provisions Blue Cross does not compensate providers practitioners or other individuals making UM decisions for denial of coverage or services We do not offer incentives to decision makers to encourage denial of coverage or services that would result in less than appropriate care
September 2015 7
QuALITY ImproVemeNT
CLINICAL PRACTICE GUIDELINES Blue Cross believes that the use of clinical practice guidelines is a key component of Quality Improvement Each year Blue Crossrsquo Clinical Practice Quality Committee (a designee of the Quality Council) approves the adoption of select guidelines that are used to support various programs and initiatives The guidelines do not substitute for sound clinical judgment however they are intended to assist clinicians in understanding key processes for improvement efforts
Clinical Practice Guidelines with hyperlinks are available in Chapter Three of the Blue Cross Provider Policy and Procedure Manual To access the manual go to providersbluecrossmncom and select ldquoForms and Publicationsrdquo then ldquoManualsrdquo
Recommended sources BlueCrossrecognizesthefollowingsourcesforClinicalPracticeGuidelinesfora variety of areas of clinical practice
bullUSPSTFUSPreventiveServicesTaskForce httpwwwuspreventiveservicestaskforceorgbrowseRecIndex
bullAAPAmericanAcademyofPediatricsincludingBrightFutures httppediatricsaappublicationsorgsearchflag=practice_guidelinesampsubmit=yesampx=18ampy=8ampformat=standardamphits=30ampsortspec=dateampsubmit=Gohttppediatricsaappublicationsorgsearchflag=practice_guidelinesampsubmit=yesampx=18ampy=8ampformat=standardamphits=30ampsortspec=dateampsubmit=Go
httpbrightfuturesaaporg
bullICSIInstituteforClinicalSystemsImprovement httpswwwicsiorgguidelines__moreguidelines_a_to_z
Specific guidelines Specific guidelines recommended by Blue Cross include the following
bullBehavioralHealth-ADHD-DiagnosisEvaluationandTreatmentofAttention-DeficitHyperactivityDisorderinChildrenandAdolescents(AAP)-DepressionScreeninginAdults(USPSTF)
bullNon-PreventiveAcuteorChronicConditions-DiabetesndashDiagnosisandManagementofType2DiabetesMellitusinAdults(ICSI)-AsthmandashDiagnosisandManagementofAsthma(ICSI)
bullPreventiveCareGuidelines-PreventiveServicesforAdults(ICSI)-PreventiveServicesChildrenandAdolescents(ICSIandBrightFutures)-RoutinePrenatalCare(ICSI)
Questions concerning Clinical Practice Guidelines can be directed to Eileen Johnson Director Quality and Health Management at (651) 662-4224Acopyoftheclinicalpractice guidelines with hyperlinks is also available by calling Eileen Johnson
September 2015 8
QuALITY ImproVemeNT
bLUE PLUS MEDICAL RECORD DOCUMENTATION REvIEwAdvance Directives
Anadvancedirectiveprovidesanopportunityforadultsofanyagetomaketheirhealthcare wishes known if or when a potential life-threatening event occurs and they are unabletoverbalizetheirwishesatthetimeoftheevent
ArepresentativesamplereviewofourBluePlusmembersrsquomedicalrecordsfordatesofservicein2014hasbeencompletedandtheresultsarebelowWeencourageprovidersto discuss the benefits of completing an advance directive with all our adult members
TOTAL MEMbERS IN SAMPLE
ADvANCE DIRECTIvE PRESENT OR DISCUSSED
AGE RANGE FOR MEMbERS wITH DISCUSSION
MedicareMedicaid Eligible(MSHO)
300 187(62) Avg83Range67-107
Medicaid 600 61(10) Avg48Range20-64
Body Mass Index (BMI) And Counseling For Obesity
Documentation of a memberrsquos BMI is the first step towards addressing the prevalence of obesity in our society Blue Plus completed a review of a sample of Blue Plus membersrsquomedicalrecordswithdatesofservicein2014toevaluatedocumentationofBMIvalueandcounselingforobesityObesityisdefinedasaBMIover30TheresultsareshownbelowOne-thirdofMedicaidmembersdefinedasobesehad documentation of a discussion with their provider concerning their weight management
TOTAL MEMbERS
bMI DOCUMENTED
bMI gt 30 (IF DOCUMENTED)
IF bMI gt 30 ADvISED ON wEIGHT MANAGEMENT
AvERAGE bMI FOR MEMbERS wITH DISCUSSION
MedicareMedicaid Eligible(MSHO)
300 183(61) 70(38) 6(9) Avg3603 Range3089-501
Medicaid 600 550(92) 237(43) 93(39) Avg3807 Range2676-710
Total 900 733(81) 307(42) 99(32) Avg3795
continued on next page
September 2015 9
bLUE PLUS MEDICAL RECORD DOCUMENTATION REvIEw continuedfrompage8
Tobacco Use Assessment And Counseling
AsampleofmedicalrecordswerereviewedtodeterminetobaccouseamongourBlue Plus members and discussions promoting tobacco cessation during a provider visitin2014Whiletobaccouseappearstoberoutinelyassessedatleastonceduring2014onlyhalfofourmembershavedocumentationofprovidereffortsinaddressingthis health concern
TOTAL MEMbERS
ASSESSED FOR TObACCO USE
TObACCO USE AvERAGE AGE OF TObACCO USERS
DISCUSSION ANDOR Rx ASSISTANCE
MSHO 300 281(93) 24(85) Avg75(67-87)
10(42)
PMAPMNCARE 600 518(86) 164(32) Avg44(20-64)
89(54)
Total 900 799(89) 188(24) Avg49 (20-87)
99(53)
These reviews were completed to encourage providers to open the door to meaningful discussions with their patients on important health issues If you have any questions concerning this article please send an email to the Quality and Health Management department co Sheiladalenbluecrossmncom
Better Care Through Quality Improvement
Every year Blue Cross and Blue Shield of Minnesota (Blue Cross) reviews the care delivered to our subscribers This review determines the goals for the quality program The program currently has many goals to improve health services
Making sure our subscribers receive preventive services and health screenings making sure people with health problems like heart disease receive treatment and improving the customer service experience are just a few of the goals in the program
More detailed information is available about Blue Crossrsquo process and outcomes in meeting quality improvement goals related to subscriber care and service You can see more information about our quality improvement program at bluecrossmncom Enter ldquoquality improvement programrdquo in the search field If you are unable to access the website please contact Eileen Johnson Director | AccreditationampQualityImprovementat(651) 662-4224 to request information about the Quality Improvement Program
QuALITY ImproVemeNT
September 2015 10
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
Medical and behavioral health policies are available for your use and review on the Blue Cross and Blue Shield of Minnesota website at providersbluecrossmncom From this site there are two ways to access medical policy information depending on the patientrsquos Blue Plan membership
For out-of-area Blue Plan patients SelectldquoMedicalPolicyPreCertPreAuthRouterrdquoandclickGoYouwillbetakentothepagewhereyouselecteithermedicalpolicyorpre-certificationpriorauthorizationandenterthepatientrsquosthree-letteralphaprefixasfoundontheirmemberidentificationcardandclickGoOnceyouaccepttherequirementsyouwillberoutedtothepatientrsquoshomeplanwhereyoucanaccessmedicalpolicyorpre-certificationpre-authorizationinformation
For local Blue Cross and Blue Shield of Minnesota plan patients SelectldquoMedicalpolicyrdquo(undertheToolsampResources)readandaccepttheBlueCrossMedicalPolicyStatementandthenselectldquoViewAllActivePoliciesrdquoYouhavenownavigatedtotheBlueCrossandBlueShieldofMinnesotaMedicaland Behavioral Health Policy Manual where there are several selections to assist with your inquiry
The ldquoWhatrsquos Newrdquo section identifies our latest new or revised policies approved by Blue Crossrsquo Medical and Behavioral Health Policy Committee at least 50 days ago These policies are now effective and providers should begin following thesepoliciesimmediatelyThesepoliciesalsoappearintheldquoActivePolicyrdquosectionoftheMedicalandBehavioralHealthPolicy Manual
The ldquoUpcoming Policiesrdquo section lists new or revised policies approved by the Blue Cross Medical and Behavioral Health Policy Committee and are effective 50 days from the date they were posted to the ldquoUpcoming Policiesrdquo section of the Medical and Behavioral Health Policy Manual
TheldquoActivePolicyrdquosectioncontainstheentirelistofpolicieseffectiveatthetimeofyourinquiryPleasenoteDHSPrograms(CoverageGuidelinesforDHSPrograms-MHCPManual)andMedicareContractors(PartAndashNationalGovernmentServices[NGS]PartBndashNationalGovernmentServices[NGS]HomeHealthandHospicendashNationalGovernmentServices[NGS]DurableMedicalEquipmentMedicareAdministrativeContractorndashNationalGovernmentServices[NGS]andTheCentersforMedicareandMedicaidServicesndashCMS)haveseparatesections
TheldquoPre-CertificationPre-Authorizationrdquosectionidentifiesvariousservicesproceduresprescriptiondrugsandmedicaldevicesthatrequirepre-certificationpre-authorizationThefollowingPre-CertificationPre-AuthorizationListsareprovidedforreviewCommercial(includingBlueLinkTPA)MNGovernmentProgramsandMedicarePlansTheselistsarenotexclusive to medical policy services only they encompass other services that are subject to pre-certification pre-authorizationrequirements
If you have additional questions regarding medical or behavioral health policy issues call provider services at (651) 662-5200 or 1-800-262-0820 for assistance
September 2015 11
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
MEDICAL AND bEHAvIORAL HEALTH POLICy ACTIvITy
Policies Effective 072015 Notification Posted 052815
Policies developedNone
Policies revisedPneumatic Compression Devices in the Outpatient or Home Setting
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentoflymphedemaintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet 1 The patient has undergone a four-week trial of conservative therapy which includes a Use of an appropriate compression bandage system or compression garment bExerciseAND c Elevation of the limb AND 2 Thetreatingphysiciandeterminesthatnosignificantimprovementhasoccurredorsignificantsymptomsremain
following the four-week trialbull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (non-programmable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps) OR
2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompressiontreatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentofchronicvenousinsufficiencyofthelowerextremitiesintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet
1 The patient has one or more venous stasis ulcers AND 2 ThepatienthasundergoneatrialofconservativetherapyforaminimumofsixmonthswhichincludesALLofthe
following a The use of an appropriate compression bandage system or compression garment bAppropriatedressingsforthewound c Exercise and d Elevation of the limb AND 3 Thetreatingphysiciandeterminesthatthevenousstasisulcerhasfailedtoheal
September 2015 12
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
bull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (nonprogrammable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
OR 2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompression
treatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingmaybeconsideredMEDICALLYNECESSARYinpatientswhohaveundergoneasurgicalprocedurewhenBOTH1and2aremet
1 Patient meets one or more of the following a Major surgery (eg total hip arthroplasty total knee arthroplasty hip fracture repair open abdominal or open
pelvic procedure OR b Patient is at moderate to severe risk of VTE Examples include i Patient is not able to walk unassisted or is bedridden ii Agegreaterthan60yearsanesthesiaatleast2hoursandbedrestatleast4daysduringcurrentepisodeofcare iii Inpatientstayofmorethan2daysduringcurrentepisodeofcare iv Central venous access during current episode of care v Sepsis during current episode of care viActivecancerorcancertreatment vii Significant comorbidity such as recent myocardial infarction congestive heart failure cerebrovascular disease
moderate to severe chronic obstructive pulmonary disease moderate to severe liver disease moderate to severe chronic kidney disease
viiiPregnancy or post-partum state (lt 1 month) ix Hypercoagulable state (eg Factor V Leiden antithrombin III deficiency protein C or S deficiency
antiphospholipidsyndromedysfibrinolysisprothrombin20210defect) x Prior VTE AND 2Thepatienthasacontraindicationtopharmacologicanticoagulantssuchasbeingathigh-riskforbleedingRisk
factors for bleeding include a Bleeding disorder such as hemophilia bActiveliverdisease c Severe renal failure d Previous major bleed (and previous bleeding risk similar to current risk) e Concomitant antiplatelet agent f History of or difficult-to-control surgical bleeding during the current operative procedure extensive surgical
dissection and revision surgery bull Outpatientorhomeuseofpneumaticcompressiondevicesforpost-surgicalVTEprophylaxisisconsideredNOTMEDICALLYNECESSARYforpatientswhohaveundergoneasurgicalprocedurewithalowriskforVTEandwhohaveno additional risk factors for VTE Examples of lower risk surgical procedures include but are not limited to laparoscopic cholecystectomy appendectomy transurethral prostatectomy and inguinal herniorrhaphy
September 2015 13
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingisconsideredINVESTIGATIVEforallotherindications including but not limited to treatment of arterial insufficiency (e g peripheral arterial disease) and restless legs syndrome due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Angioplasty andor Stenting for Intracranial Aneurysms and Atherosclerosis
bull IntracranialstentplacementmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranial aneurysms for patients when surgical treatment is not feasible and standard endovascular techniques do not allowforcompleteisolationoftheaneurysmegwide-neckaneurysm(4mmormore)orsack-to-neckratiolessthan21
bull IntracranialflowdivertingstentswithFDAapprovalforthetreatmentofintracranialaneurysmsmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranialaneurysmsthatarelargeorgiantwide-necked(aneurysmsizeof10mmormoreandaneckdiameterof4mmormore)intheinternalcarotidarteryfrom the petrous to the superior hypophyseal segments and which are not amenable to surgical treatment or standard endovascular therapy
bull IntracranialstentplacementisconsideredINVESTIGATIVEinthetreatmentofintracranialaneurysmsexceptasnotedabove due to the lack of clinical evidence demonstrating its impact on improved health outcomes
bull PercutaneoustransluminalangioplastywithorwithoutstentingisconsideredINVESTIGATIVEforthetreatmentofintracranial atherosclerosis due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Surgical Treatment of Femoroacetabular Impingement
bull OpenorarthroscopictreatmentoffemoroacetabularimpingementmaybeconsideredMEDICALLYNECESSARYwhenALLofthefollowingconditionsaremet
AAge Patientisskeletallymaturewithdocumentedclosureofgrowthplates(eg15yearsorolder) B Symptoms 1 Moderate-to-severe hip pain that is worsened by flexion activities (eg squatting or prolonged sitting) and which
significantlylimitsactivitiesAND 2Painwhichisunresponsiveorrecursafteratrialofconservativetherapylastingatleast3months(including
activitymodificationsrestrictionofathleticpursuitsandavoidanceofsymptomaticmotion)AND 3Positiveimpingementsignispresentonclinicalexamination(painelicitedwith90degreesofflexionandinternal
rotation and adduction of the femur) C Imaging 1Imagingstudies(egx-raysMRI)confirmthediagnosisofacamorpincer-typeFAIExamplesofmorphology
indicativeofFAIinclude a pistol-grip deformity
b femoralhead-neckoffsetwithanalphaanglegreaterthan50degrees c a positive wall sign d acetabular retroversion (overcoverage with crossover sign) e coxa profunda or protrusion f damage of the acetabular rim AND 2Noevidenceofadvancedosteoarthritis(definedasTonnisgradeIIorIIIorjointspaceoflessthan2mm)AND 3Noevidenceofsevere(modifiedOuterbridgegradeIV)chondraldamagebull Surgicaltreatmentoffemoroacetabularimpingement(FAI)isconsideredINVESTIGATIVEinallothersituations
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 14
Policies inactivatedTobacco Cessation Treatments
Policies Effective 081715 Notification Posted 062515
Policies developedNone
Policies revisedTreatment of Obstructive Sleep Apnea and Snoring in Adults bull Medical Management
A IntraoralAppliances Intraoral appliances (eg mandibular advancingpositioning devices or tongue-retaining devices) may be considered
MEDICALLYNECESSARYwhenALLofthefollowingcriteriaaremet 1PatienthasbeendiagnosedwithOSAdefinedby a AnAHIorRDIof15orgreatereventsperhour OR bAnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms i Excessive daytime sleepiness ii Documented hypertension iii Ischemic heart disease iv History of stroke AND 2Thereisabsenceoftemporomandibulardysfunctionorperiodontaldisease AND 3ThedeviceisprescribedafteradiagnosisofOSAhasbeenestablishedbyaphysicianwhoiseitheradiplomate
oftheAmericanBoardofSleepMedicinearecognizedsubspecialtyoftheAmericanBoardofMedicalSpecialties(ABMS)oranactivestaffmemberofasleepcenterorlaboratoryaccreditedbytheAmericanAcademyofSleepMedicine(AASM)orTheJointCommission
AND 4 The device is custom-fitted by qualified dental personnel under the direction of a Doctor of Dental Surgery (DDS)
or Doctor of Dental Medicine (DMD) B ContinuousPositiveAirwayPressure(CPAP) Continuouspositiveairwaypressure(CPAP)maybeconsideredMEDICALLYNECESSARYinpatientswith
confirmedOSAwith 1AnAHIorRDIof15eventsperhourorgreater OR 2AnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms a Excessive daytime sleepiness b Documented hypertension c Ischemic heart disease d History of stroke
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 15
C Bi-levelPositiveAirwayPressure(BiPAP) BiPAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPAND 2HavefailedapriortrialofCPAPOR 3ForwhomBiPAPisfoundtobemoreeffectivethanCPAPinthesleeplaboratory D Auto-AdjustingPAP(APAP) APAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPaboveAND 2HaveacontraindicationtoCPAPhavefailedapriortrialofCPAPORareundergoingatrialofAPAPtotitrate CPAP AND 3Havenoevidencebyhistoryorphysicalexaminationofthefollowingconditions a Central sleep apnea b Congestive heart failure c Chronic pulmonary disease such as chronic obstructive pulmonary disease d Pulmonary hypertension e Obesityhypoventilationsyndromeorotherconditionwhichmaycausenocturnalarterialoxyhemoglobin desaturationbull Surgical Management A Uvulopalatopharyngoplasty(UPPP) UPPPmaybeconsideredMEDICALLYNECESSARYwhenallthefollowingcriteriaaremet 1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a BMI less than 40 AND bAtrialoforalappliancetherapyhasfailedorthepatientisnotacandidateforanoralappliance AND c PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hoursper nightforthree(3)monthsofPAPusage B Maxillofacial Procedures Maxillofacial surgical procedures such as inferior sagittal mandibular osteotomy and genioglossal advancement
withorwithouthyoidmyotomyandsuspensionormandibular-maxillaryadvancement(MMA)maybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a Objectiveevidenceofhypopharyngealobstructiondocumentedbyeitherfiberopticexaminationor cephalometric radiographs AND
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 16
b PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hourspernightforthree(3)monthsofPAPusage
bull Treatment of Snoring TreatmentofsnoringisconsideredNOTMEDICALLYNECESSARYbecausesimplesnoringintheabsenceof
documented obstructive sleep apnea is not considered a medical condition Therefore all procedures for the sole or adjunctivetreatmentofsnoringareconsideredNOTMEDICALLYNECESSARYincludingbutnotlimitedto
A Uvulopalatopharyngoplasty(UPPP) B Uvulectomy C Laser-assisteduvulopalatoplasty(LAUP) D Radiofrequencyvolumetricreductionofthepalataltissues E Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues F Palatal stiffening procedures including but not limited to cautery-assisted palatal stiffening operation and the
implantation of palatal implants G Tongue base suspensionbull Investigative Indications ThefollowingtreatmentsareconsideredINVESTIGATIVEduetoalackofevidencedemonstratingimprovedhealth outcomes AUPPPforanyconditionotherthanobstructivesleepapneaorsnoring B ExpiratoryPositiveAirwayPressure(EPAP)includingtheProventregdevice C OralpressuretherapydevicesincludingbutnotlimitedtotheWinxTMsystem D Atrialpacing EAllothersurgicalproceduresforthesoleoradjunctivetreatmentofobstructivesleepapneaupperairwayresistance
syndrome including but not limited to 1 Uvulectomy 2Laser-assisteduvulopalatoplasty(LAUP) 3Radiofrequencyvolumetricreductionofthepalataltissues 4Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues 5Palatalstiffeningproceduresincludingbutnotlimitedtocautery-assistedpalatalstiffeningoperationandthe
implantation of palatal implants 6 Tongue base suspension 7 Implantable hypoglossal nerve stimulators Respiratory Syncytial Virus (RSV) Prophylaxis bull INITIALRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVfortheinitialRSVseasonmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A ChronicLungDisease(CLD)ofPrematurity 1Infantwasbornatlt32weeks0daysgestationAND 2Infantisle12monthsofageattheonsetofRSVseasonAND 3Infantrequiresgt21oxygenforatleastthefirst28daysafterbirth B Congenital Heart Disease (CHD) 1 Infant is le12monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 17
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
a AcyanoticCHDwhentheinfantisreceivingmedicationtocontrolcongestiveheartfailureandwillrequireacardiacsurgicalprocedureOR
b CyanoticCHDwhenpalivizumabisrecommendedafterconsultationwithapediatriccardiologistOR c Diagnosis of moderate to severe pulmonary hypertension OR 2Childislt24monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing a ChildundergoescardiactransplantationduringtheRSVseasonOR b ChildisreceivingRSVprophylaxisandcontinuestorequireprophylaxisafterasurgicalprocedureinvolving cardiac bypass or at the conclusion of extracorporeal membrane oxygenation C AnatomicPulmonaryAbnormalitiesORNeuromuscularDisorder(egcerebralpalsymusculardystrophy) 1 Infant is le12monthsofageattheonsetofRSVseasonAND 2Infanthasimpairedabilitytoclearsecretionsfromtheupperairway D Cystic Fibrosis 1 Infant is le12monthsofageattheonsetofRSVseasonwithevidenceofCLDandormalnutrition E Immunocompromised Status 1Childislt24monthsofageattheonsetofRSVseasonAND 2Childisprofoundlyimmunocompromised(egduetosolidorgantransplantationhematopoieticstem-cell
transplantation or chemotherapy) F Prematurity without CLD or CHD 1Infantwasbornatlt29weeks0daysgestation(ie28weeks6daysorless)AND 2Infantislt12monthsofageattheonsetofRSVseasonbull SECONDRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVforthepatientrsquossecondyearoftreatmentmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A CLDofPrematurity 1Childwasbornatlt32weeks0daysgestationAND 2Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonAND 3ChildcontinuestorequireatleastONEofthefollowingwithinsix(6)monthsofthestartofthesecondRSV season a SupplementaloxygenOR b ChronicsystemiccorticosteroidtherapyOR c DiuretictherapyOR d Bronchodilator therapy B Cystic Fibrosis 1Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonwithevidenceofCLDandor malnutritionbull AdministrationofRSVProphylaxis A Whentheappropriatecriteriaabovearemetamaximumoffive(5)monthlydosesofpalivizumab(Synagisreg)will
becoveredperRSVseason(definedasNovember1stthroughMarch31st) B Thefirstmonthlydoseofpalivizumab(Synagisreg)willbeapprovedforcoverageofadministrationonorafter
November 1st C Apost-operativedoseofpalivizumab(Synagisreg)willbecoveredforchildrenlt24monthswhoarereceiving
RSVprophylaxisandcontinuetorequireprophylaxisafterasurgicalprocedureinvolvingcardiacbypassorattheconclusion of extracorporeal membrane oxygenation
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 2
Provider Demographic Change Form
The Provider Demographic Change form needs to be completed when your address phone number hospital affiliation or office hours change Go to providersbluecrossmncom and enter ldquoprovider demographic change formrdquo in the search window to obtain the form Completed forms can be
Emailed to ProviderDatabluecrossmncom
Faxed to (651) 662-6684
Mailed to Blue Cross and Blue Shield of Minnesota PDOR316 POBox64560 StPaulMN55164-0560
FYI
PUbLICATIONS AvAILAbLE ONLINE
ThefollowingisalistofQuickPointsandBulletinspublishedfromJune2015toAugust2015thatareavailableonlineatprovidersbluecrossmncom AsareminderBulletinsaremailedtoallparticipatingprovidersaffectedbytheinformation Quick Points are available only on our website unless noted otherwise in the bottom left corner of the publication
QUICk POINTS TITLEQP13-15 Provider Cost Data Update
QP14-15 Update to Buprenorphine and BuprenorphineNaloxone (BunavailtradeSuboxoneregZubsolvreg)PriorAuthorizationandQuantityLimitCriteria
QP15-15 Update to NuvigilregArmodafinilProvigilregModafinilPriorAuthorizationandQuantity Limit Criteria
QP16-15 ICD-10 Provider Partner Testing Summary
QP17-15 WhoisBlueLinkTPA
bULLETINS TITLEP21-15 NewClaimsFilingRulesforAirAmbulanceProviders
P22-15 July2015HCPCSCodeUpdates
P23-15 MedicalNecessityReviewCriteriaUpdateforMHCPSubscribers
P24-15 MentalHealthServicesRequirementforMinnesotaHealthCarePrograms(MHCP) Subscribers
P25-15 NewDrug-relatedPriorAuthorizationCriteriaProproteinConvertaseSubtilisinKexinType9(PCSK9)InhibitorsforFamilialHypercholesterolemiaPAwithQuantityLimit
P26-15 UpdateonKneeArthroplastyCriteriaforMHCPSubscribers
P27-15 Non-CoveredMedicareServicesandOrganizationDeterminationUpdateforPlatinumBlue Subscribers
P28-15 Facility Place of Service Changes
P29-15 MedicareTrainingandEducationRequirements
P30-15 ICD-10CodingUpdateandFinalReminders
P31-15 Common Carrier and Special Transportation Providers Billing Code Updates
FYIHELPFUL PHONE NUMbERSBLUELINE (voice response unit) (651) 662-5200 or 1-800-262-0820
BlueCardreg member benefits or eligibility 1-800-676-BLUE (2583)
FEPreg (voice response unit) (651) 662-5044 or 1-800-859-2128
Availity 1-800-282-4548
Provider services (651) 662-5200 or 1-800-262-0820
Please verify these numbers are correctly programmed into your office phones
September 2015 3
FYI
PROvIDER MANUAL UPDATES The following is a list of Blue Cross and Blue Shield of Minnesota provider manuals thathavebeenupdatedfromJune2015toAugust2015Asareminderprovidermanuals are available online at providersbluecrossmncom To view the manuals select ldquoForms amp publicationsrdquo then ldquomanualsrdquo Updates to the manuals are documented in the ldquoSummary of changesrdquo section of the online manuals
MANUAL NAME
CHAPTER NUMbER AND TITLE
CHANGE
Provider Policy and Procedure Manual
Chapter 11 Coding Policies and Guidelines Medical Services section
Topic of ldquoNon-covered Tobacco Treatmentsrdquo was deleted
Provider Policy and Procedure Manual
Chapter 11 Coding Policies and Guidelines Public Programs section
Content change to Transportation Services (Formerly titled Special Transportation)
Provider Policy and Procedure Manual
Allchapters ReferencestoICD-9codeswillbeupdatedtoreflect the appropriate ICD-10 codes Note We anticipate completing all the updates nolaterthanSeptember12015
REALLy SIMPLE SyNDICATION Not all provider publications are mailed out to providers The majority of our informational Quick Points and the quarterly Provider Press are posted to our website for providers to view Providers frequently ask us how they can be advised when new publications are added to the website at providersbluecrossmncom
ProviderscansignuptogetRSS(reallysimplesyndication)feedsofourlatestnewsreleasesandupdatestoprovider-relatedformsandpublicationsAsampleofthefeeds that can be requested includes
bull Bulletinsbull Forms admin updates and contractingbull Forms credentialingbull Formspre-certificationandpre-authorizationbull Manualsbull Provider Press
bull Quick Points
Go to providersbluecrossmncomandenterldquoRSSrdquointhesearchwindowtolearnmoreaboutRSSQuestionsaboutRSSfeedsspecifictoyourinternalsystemsshould be directed to your IT support area
2015 HOLIDAy SCHEDULEProvider services will be closed on the following days
in2015
Monday September 7
ThursdayNovember26
FridayNovember27
ThursdayDecember24
FridayDecember25
With the exception of the dates stated above representatives answering the provider services numbers are available to assistyou8amto5pmMonday through Thursday and9amto5pmonFriday
September 2015 4
CodINg CorNer
REPLACEMENT CLAIM REMINDERWhendoIneedareplacementclaimWellareyoumakingchangestoaclaimthatwaspreviouslyprocessedIfyesyouwillneedtosendinareplacementclaimThisincludes
bull changing a date of service
bull adding or changing a procedure
bull adding or changing a diagnosis
bull removing a modifier
bull adding a modifier
Note that when adding modifiers -24 -25 -57 -59 -78 andor 79 medical notes supporting the modifier also need to be sent with the replacement claim
SeeProviderBulletinP28-14datedOctober12014formoreinformation
26 OR TC USENot every code in particular radiology codes has a professional component (reported witha-26modifier)andtechnicalcomponent(reportedwithandashTCmodifier)ForexampleCPTcode77387isldquoGuidanceforlocalizationoftargetvolumefordeliveryof radiation treatment delivery includes intrafraction tracking when performedrdquo This code does not have a professional or technical component Thus if it is submitted with acomponentmodifier(-26or-TC)itwillbedeniedbecauseaninvalidmodifierwasappended to the service
ICD-10 CODING UPDATE AND FINAL REMINDERS continued from page 1
httpwwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesDownloadsSE1325pdf
UsethecorrectcodequalifierindicatingwhetherthecodeisICD-9orICD-10forthecode setbeingreportedintheHIPAAtransaction
Reviewyourclaimacknowledgementreportstimelytoensureclaimshavebeencorrectlysubmitted and accepted by Blue Cross Claims rejected on these reports must be corrected and submitted again Claims rejected on acknowledgment reports are not considered submitted for timely filing purposes
AdditionalinformationisavailableundertheICD-10compliancelinkonourwebsiteatprovidersbluecrossmncom
Questions
If you have questions please contact provider services at (651) 662-5200 or 1-800-262-0820
THE HCPCS ARE COMING THE HCPCS ARE COMING Itrsquos not just the ICD codes that will be the coding stars onOctober12015HCPCScodes are updated as well on that fall date Blue Cross will publish a Provider Bulletin closer to the October12015effectivedate that provides more details
September 2015 5
HeALTH LITerACY
Try both aleve 2pills bid with flexeril at hs
Asahealthcareprofessionalyouprobablyunderstandexactlywhatthedoctorwhosentthismessage was saying Take 2 Aleve pills 2 times a day and take 1 Flexeril pill at bedtime But the patient who received it had no idea what the doctor was saying Most people donrsquot Clear communication increases patient safety and adherence to treatment plans
OctoberishealthliteracymonthHerearesomeactivitiesthatyourpracticecliniccanincorporate to help make a healthy difference in your patientrsquos lives
Use the Teach Back method also known as the ldquoshow-merdquo technique to ensure that patients (or care takers) understand their treatment plan and what they need to do Think aboutdoingasimpleteachbacktrainingatyourpracticeduringthemonthofOctoberClickhere for a program ready to use from the Minnesota Health Literacy Partnership
Promote the Ask Me 3 program from the National Patient Safety Foundation which focuses onpatientunderstandingof3simplequestions
1)Whatismymainproblem
2)WhatdoIneedtodo
3)Whyisitimportantformetodothis
You can use these questions to help guide the information you provide during visits with your patients Make sure they know the answer to these questions before they leave your office ConsiderdisplayingpostersandbrochuresthroughoutyourofficeduringOctobertoremindstaffaboutthe3questionsFormoreinformationonAskMe3clickhere
Review your own patient education materials Select a few of the patient education materials that you commonly use in your practice and review them using one of the health literacytoolsfromtheOfficeofDiseasePreventionandHealthPromotionPerhapsformateam to review the pieces together Click hereforresourcesOrcontactusifyouwantacopy of the tool used at Blue Cross
To learn more about building a culture of health literacy and using plain language at your practice please send an email to AlishaOdhiambobluecrossmncomAdditionalinformationcan also be found online at httphealthliteracymnorg
September 2015 6
QuALITY ImproVemeNT
PCC QUALITy OF CARE COMPLAINT REPORTProviders are required to complete the Blue Plus Quality of Care Complaint report forallwrittenandverbalcomplaintsfromBluePlusPrepaidMedicalAssistanceProgram and MinnesotaCare subscribers on a quarterly basis per Minnesota Department of Health regulations Complaints logged at the provider offices are to be investigated and resolved by the providerrsquos office whenever possible
ThesecomplaintsarereportedtoBluePlusinJanuaryAprilJulyandOctoberfor the preceding three months The Primary Care Clinic (PCC) must submit a quarterly report even if the facility does not receive any complaints for the quarter YourcontractoutlinestheproceduresrequiredforyourQualityofCare(QOC)PCCcomplaint reporting adherence agreement
Complaints should no longer be directed to the attention of a single designated personSendingyourPCCQOCcomplaintreportformtoanysourcenotlistedbelowmaydelaytheprocessingofyourPCCQOCcomplaintreport
ToaccessthePCCBluePlusQualityofCareComplaintReportFormgoto providersbluecrossmncom and select ldquoForms amp publicationsrdquo then ldquoforms - clinical operationsrdquo
Submit quarterly PCC QOC reports using one of these methods
Email pcccomplaintbluecrossmncom
Secure fax line (651) 662-4004
Mail Blue Plus AttnQualityHealthManagementDept R472 POBox64179 StPaulMN55164-0179
UTILIzATION MANAGEMENT STATEMENTUtilizationManagement(UM)decisionmakingisbasedonlyonappropriatenessofcareand service and on existing coverage provisions Blue Cross does not compensate providers practitioners or other individuals making UM decisions for denial of coverage or services We do not offer incentives to decision makers to encourage denial of coverage or services that would result in less than appropriate care
September 2015 7
QuALITY ImproVemeNT
CLINICAL PRACTICE GUIDELINES Blue Cross believes that the use of clinical practice guidelines is a key component of Quality Improvement Each year Blue Crossrsquo Clinical Practice Quality Committee (a designee of the Quality Council) approves the adoption of select guidelines that are used to support various programs and initiatives The guidelines do not substitute for sound clinical judgment however they are intended to assist clinicians in understanding key processes for improvement efforts
Clinical Practice Guidelines with hyperlinks are available in Chapter Three of the Blue Cross Provider Policy and Procedure Manual To access the manual go to providersbluecrossmncom and select ldquoForms and Publicationsrdquo then ldquoManualsrdquo
Recommended sources BlueCrossrecognizesthefollowingsourcesforClinicalPracticeGuidelinesfora variety of areas of clinical practice
bullUSPSTFUSPreventiveServicesTaskForce httpwwwuspreventiveservicestaskforceorgbrowseRecIndex
bullAAPAmericanAcademyofPediatricsincludingBrightFutures httppediatricsaappublicationsorgsearchflag=practice_guidelinesampsubmit=yesampx=18ampy=8ampformat=standardamphits=30ampsortspec=dateampsubmit=Gohttppediatricsaappublicationsorgsearchflag=practice_guidelinesampsubmit=yesampx=18ampy=8ampformat=standardamphits=30ampsortspec=dateampsubmit=Go
httpbrightfuturesaaporg
bullICSIInstituteforClinicalSystemsImprovement httpswwwicsiorgguidelines__moreguidelines_a_to_z
Specific guidelines Specific guidelines recommended by Blue Cross include the following
bullBehavioralHealth-ADHD-DiagnosisEvaluationandTreatmentofAttention-DeficitHyperactivityDisorderinChildrenandAdolescents(AAP)-DepressionScreeninginAdults(USPSTF)
bullNon-PreventiveAcuteorChronicConditions-DiabetesndashDiagnosisandManagementofType2DiabetesMellitusinAdults(ICSI)-AsthmandashDiagnosisandManagementofAsthma(ICSI)
bullPreventiveCareGuidelines-PreventiveServicesforAdults(ICSI)-PreventiveServicesChildrenandAdolescents(ICSIandBrightFutures)-RoutinePrenatalCare(ICSI)
Questions concerning Clinical Practice Guidelines can be directed to Eileen Johnson Director Quality and Health Management at (651) 662-4224Acopyoftheclinicalpractice guidelines with hyperlinks is also available by calling Eileen Johnson
September 2015 8
QuALITY ImproVemeNT
bLUE PLUS MEDICAL RECORD DOCUMENTATION REvIEwAdvance Directives
Anadvancedirectiveprovidesanopportunityforadultsofanyagetomaketheirhealthcare wishes known if or when a potential life-threatening event occurs and they are unabletoverbalizetheirwishesatthetimeoftheevent
ArepresentativesamplereviewofourBluePlusmembersrsquomedicalrecordsfordatesofservicein2014hasbeencompletedandtheresultsarebelowWeencourageprovidersto discuss the benefits of completing an advance directive with all our adult members
TOTAL MEMbERS IN SAMPLE
ADvANCE DIRECTIvE PRESENT OR DISCUSSED
AGE RANGE FOR MEMbERS wITH DISCUSSION
MedicareMedicaid Eligible(MSHO)
300 187(62) Avg83Range67-107
Medicaid 600 61(10) Avg48Range20-64
Body Mass Index (BMI) And Counseling For Obesity
Documentation of a memberrsquos BMI is the first step towards addressing the prevalence of obesity in our society Blue Plus completed a review of a sample of Blue Plus membersrsquomedicalrecordswithdatesofservicein2014toevaluatedocumentationofBMIvalueandcounselingforobesityObesityisdefinedasaBMIover30TheresultsareshownbelowOne-thirdofMedicaidmembersdefinedasobesehad documentation of a discussion with their provider concerning their weight management
TOTAL MEMbERS
bMI DOCUMENTED
bMI gt 30 (IF DOCUMENTED)
IF bMI gt 30 ADvISED ON wEIGHT MANAGEMENT
AvERAGE bMI FOR MEMbERS wITH DISCUSSION
MedicareMedicaid Eligible(MSHO)
300 183(61) 70(38) 6(9) Avg3603 Range3089-501
Medicaid 600 550(92) 237(43) 93(39) Avg3807 Range2676-710
Total 900 733(81) 307(42) 99(32) Avg3795
continued on next page
September 2015 9
bLUE PLUS MEDICAL RECORD DOCUMENTATION REvIEw continuedfrompage8
Tobacco Use Assessment And Counseling
AsampleofmedicalrecordswerereviewedtodeterminetobaccouseamongourBlue Plus members and discussions promoting tobacco cessation during a provider visitin2014Whiletobaccouseappearstoberoutinelyassessedatleastonceduring2014onlyhalfofourmembershavedocumentationofprovidereffortsinaddressingthis health concern
TOTAL MEMbERS
ASSESSED FOR TObACCO USE
TObACCO USE AvERAGE AGE OF TObACCO USERS
DISCUSSION ANDOR Rx ASSISTANCE
MSHO 300 281(93) 24(85) Avg75(67-87)
10(42)
PMAPMNCARE 600 518(86) 164(32) Avg44(20-64)
89(54)
Total 900 799(89) 188(24) Avg49 (20-87)
99(53)
These reviews were completed to encourage providers to open the door to meaningful discussions with their patients on important health issues If you have any questions concerning this article please send an email to the Quality and Health Management department co Sheiladalenbluecrossmncom
Better Care Through Quality Improvement
Every year Blue Cross and Blue Shield of Minnesota (Blue Cross) reviews the care delivered to our subscribers This review determines the goals for the quality program The program currently has many goals to improve health services
Making sure our subscribers receive preventive services and health screenings making sure people with health problems like heart disease receive treatment and improving the customer service experience are just a few of the goals in the program
More detailed information is available about Blue Crossrsquo process and outcomes in meeting quality improvement goals related to subscriber care and service You can see more information about our quality improvement program at bluecrossmncom Enter ldquoquality improvement programrdquo in the search field If you are unable to access the website please contact Eileen Johnson Director | AccreditationampQualityImprovementat(651) 662-4224 to request information about the Quality Improvement Program
QuALITY ImproVemeNT
September 2015 10
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
Medical and behavioral health policies are available for your use and review on the Blue Cross and Blue Shield of Minnesota website at providersbluecrossmncom From this site there are two ways to access medical policy information depending on the patientrsquos Blue Plan membership
For out-of-area Blue Plan patients SelectldquoMedicalPolicyPreCertPreAuthRouterrdquoandclickGoYouwillbetakentothepagewhereyouselecteithermedicalpolicyorpre-certificationpriorauthorizationandenterthepatientrsquosthree-letteralphaprefixasfoundontheirmemberidentificationcardandclickGoOnceyouaccepttherequirementsyouwillberoutedtothepatientrsquoshomeplanwhereyoucanaccessmedicalpolicyorpre-certificationpre-authorizationinformation
For local Blue Cross and Blue Shield of Minnesota plan patients SelectldquoMedicalpolicyrdquo(undertheToolsampResources)readandaccepttheBlueCrossMedicalPolicyStatementandthenselectldquoViewAllActivePoliciesrdquoYouhavenownavigatedtotheBlueCrossandBlueShieldofMinnesotaMedicaland Behavioral Health Policy Manual where there are several selections to assist with your inquiry
The ldquoWhatrsquos Newrdquo section identifies our latest new or revised policies approved by Blue Crossrsquo Medical and Behavioral Health Policy Committee at least 50 days ago These policies are now effective and providers should begin following thesepoliciesimmediatelyThesepoliciesalsoappearintheldquoActivePolicyrdquosectionoftheMedicalandBehavioralHealthPolicy Manual
The ldquoUpcoming Policiesrdquo section lists new or revised policies approved by the Blue Cross Medical and Behavioral Health Policy Committee and are effective 50 days from the date they were posted to the ldquoUpcoming Policiesrdquo section of the Medical and Behavioral Health Policy Manual
TheldquoActivePolicyrdquosectioncontainstheentirelistofpolicieseffectiveatthetimeofyourinquiryPleasenoteDHSPrograms(CoverageGuidelinesforDHSPrograms-MHCPManual)andMedicareContractors(PartAndashNationalGovernmentServices[NGS]PartBndashNationalGovernmentServices[NGS]HomeHealthandHospicendashNationalGovernmentServices[NGS]DurableMedicalEquipmentMedicareAdministrativeContractorndashNationalGovernmentServices[NGS]andTheCentersforMedicareandMedicaidServicesndashCMS)haveseparatesections
TheldquoPre-CertificationPre-Authorizationrdquosectionidentifiesvariousservicesproceduresprescriptiondrugsandmedicaldevicesthatrequirepre-certificationpre-authorizationThefollowingPre-CertificationPre-AuthorizationListsareprovidedforreviewCommercial(includingBlueLinkTPA)MNGovernmentProgramsandMedicarePlansTheselistsarenotexclusive to medical policy services only they encompass other services that are subject to pre-certification pre-authorizationrequirements
If you have additional questions regarding medical or behavioral health policy issues call provider services at (651) 662-5200 or 1-800-262-0820 for assistance
September 2015 11
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
MEDICAL AND bEHAvIORAL HEALTH POLICy ACTIvITy
Policies Effective 072015 Notification Posted 052815
Policies developedNone
Policies revisedPneumatic Compression Devices in the Outpatient or Home Setting
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentoflymphedemaintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet 1 The patient has undergone a four-week trial of conservative therapy which includes a Use of an appropriate compression bandage system or compression garment bExerciseAND c Elevation of the limb AND 2 Thetreatingphysiciandeterminesthatnosignificantimprovementhasoccurredorsignificantsymptomsremain
following the four-week trialbull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (non-programmable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps) OR
2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompressiontreatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentofchronicvenousinsufficiencyofthelowerextremitiesintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet
1 The patient has one or more venous stasis ulcers AND 2 ThepatienthasundergoneatrialofconservativetherapyforaminimumofsixmonthswhichincludesALLofthe
following a The use of an appropriate compression bandage system or compression garment bAppropriatedressingsforthewound c Exercise and d Elevation of the limb AND 3 Thetreatingphysiciandeterminesthatthevenousstasisulcerhasfailedtoheal
September 2015 12
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
bull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (nonprogrammable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
OR 2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompression
treatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingmaybeconsideredMEDICALLYNECESSARYinpatientswhohaveundergoneasurgicalprocedurewhenBOTH1and2aremet
1 Patient meets one or more of the following a Major surgery (eg total hip arthroplasty total knee arthroplasty hip fracture repair open abdominal or open
pelvic procedure OR b Patient is at moderate to severe risk of VTE Examples include i Patient is not able to walk unassisted or is bedridden ii Agegreaterthan60yearsanesthesiaatleast2hoursandbedrestatleast4daysduringcurrentepisodeofcare iii Inpatientstayofmorethan2daysduringcurrentepisodeofcare iv Central venous access during current episode of care v Sepsis during current episode of care viActivecancerorcancertreatment vii Significant comorbidity such as recent myocardial infarction congestive heart failure cerebrovascular disease
moderate to severe chronic obstructive pulmonary disease moderate to severe liver disease moderate to severe chronic kidney disease
viiiPregnancy or post-partum state (lt 1 month) ix Hypercoagulable state (eg Factor V Leiden antithrombin III deficiency protein C or S deficiency
antiphospholipidsyndromedysfibrinolysisprothrombin20210defect) x Prior VTE AND 2Thepatienthasacontraindicationtopharmacologicanticoagulantssuchasbeingathigh-riskforbleedingRisk
factors for bleeding include a Bleeding disorder such as hemophilia bActiveliverdisease c Severe renal failure d Previous major bleed (and previous bleeding risk similar to current risk) e Concomitant antiplatelet agent f History of or difficult-to-control surgical bleeding during the current operative procedure extensive surgical
dissection and revision surgery bull Outpatientorhomeuseofpneumaticcompressiondevicesforpost-surgicalVTEprophylaxisisconsideredNOTMEDICALLYNECESSARYforpatientswhohaveundergoneasurgicalprocedurewithalowriskforVTEandwhohaveno additional risk factors for VTE Examples of lower risk surgical procedures include but are not limited to laparoscopic cholecystectomy appendectomy transurethral prostatectomy and inguinal herniorrhaphy
September 2015 13
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingisconsideredINVESTIGATIVEforallotherindications including but not limited to treatment of arterial insufficiency (e g peripheral arterial disease) and restless legs syndrome due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Angioplasty andor Stenting for Intracranial Aneurysms and Atherosclerosis
bull IntracranialstentplacementmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranial aneurysms for patients when surgical treatment is not feasible and standard endovascular techniques do not allowforcompleteisolationoftheaneurysmegwide-neckaneurysm(4mmormore)orsack-to-neckratiolessthan21
bull IntracranialflowdivertingstentswithFDAapprovalforthetreatmentofintracranialaneurysmsmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranialaneurysmsthatarelargeorgiantwide-necked(aneurysmsizeof10mmormoreandaneckdiameterof4mmormore)intheinternalcarotidarteryfrom the petrous to the superior hypophyseal segments and which are not amenable to surgical treatment or standard endovascular therapy
bull IntracranialstentplacementisconsideredINVESTIGATIVEinthetreatmentofintracranialaneurysmsexceptasnotedabove due to the lack of clinical evidence demonstrating its impact on improved health outcomes
bull PercutaneoustransluminalangioplastywithorwithoutstentingisconsideredINVESTIGATIVEforthetreatmentofintracranial atherosclerosis due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Surgical Treatment of Femoroacetabular Impingement
bull OpenorarthroscopictreatmentoffemoroacetabularimpingementmaybeconsideredMEDICALLYNECESSARYwhenALLofthefollowingconditionsaremet
AAge Patientisskeletallymaturewithdocumentedclosureofgrowthplates(eg15yearsorolder) B Symptoms 1 Moderate-to-severe hip pain that is worsened by flexion activities (eg squatting or prolonged sitting) and which
significantlylimitsactivitiesAND 2Painwhichisunresponsiveorrecursafteratrialofconservativetherapylastingatleast3months(including
activitymodificationsrestrictionofathleticpursuitsandavoidanceofsymptomaticmotion)AND 3Positiveimpingementsignispresentonclinicalexamination(painelicitedwith90degreesofflexionandinternal
rotation and adduction of the femur) C Imaging 1Imagingstudies(egx-raysMRI)confirmthediagnosisofacamorpincer-typeFAIExamplesofmorphology
indicativeofFAIinclude a pistol-grip deformity
b femoralhead-neckoffsetwithanalphaanglegreaterthan50degrees c a positive wall sign d acetabular retroversion (overcoverage with crossover sign) e coxa profunda or protrusion f damage of the acetabular rim AND 2Noevidenceofadvancedosteoarthritis(definedasTonnisgradeIIorIIIorjointspaceoflessthan2mm)AND 3Noevidenceofsevere(modifiedOuterbridgegradeIV)chondraldamagebull Surgicaltreatmentoffemoroacetabularimpingement(FAI)isconsideredINVESTIGATIVEinallothersituations
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 14
Policies inactivatedTobacco Cessation Treatments
Policies Effective 081715 Notification Posted 062515
Policies developedNone
Policies revisedTreatment of Obstructive Sleep Apnea and Snoring in Adults bull Medical Management
A IntraoralAppliances Intraoral appliances (eg mandibular advancingpositioning devices or tongue-retaining devices) may be considered
MEDICALLYNECESSARYwhenALLofthefollowingcriteriaaremet 1PatienthasbeendiagnosedwithOSAdefinedby a AnAHIorRDIof15orgreatereventsperhour OR bAnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms i Excessive daytime sleepiness ii Documented hypertension iii Ischemic heart disease iv History of stroke AND 2Thereisabsenceoftemporomandibulardysfunctionorperiodontaldisease AND 3ThedeviceisprescribedafteradiagnosisofOSAhasbeenestablishedbyaphysicianwhoiseitheradiplomate
oftheAmericanBoardofSleepMedicinearecognizedsubspecialtyoftheAmericanBoardofMedicalSpecialties(ABMS)oranactivestaffmemberofasleepcenterorlaboratoryaccreditedbytheAmericanAcademyofSleepMedicine(AASM)orTheJointCommission
AND 4 The device is custom-fitted by qualified dental personnel under the direction of a Doctor of Dental Surgery (DDS)
or Doctor of Dental Medicine (DMD) B ContinuousPositiveAirwayPressure(CPAP) Continuouspositiveairwaypressure(CPAP)maybeconsideredMEDICALLYNECESSARYinpatientswith
confirmedOSAwith 1AnAHIorRDIof15eventsperhourorgreater OR 2AnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms a Excessive daytime sleepiness b Documented hypertension c Ischemic heart disease d History of stroke
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 15
C Bi-levelPositiveAirwayPressure(BiPAP) BiPAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPAND 2HavefailedapriortrialofCPAPOR 3ForwhomBiPAPisfoundtobemoreeffectivethanCPAPinthesleeplaboratory D Auto-AdjustingPAP(APAP) APAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPaboveAND 2HaveacontraindicationtoCPAPhavefailedapriortrialofCPAPORareundergoingatrialofAPAPtotitrate CPAP AND 3Havenoevidencebyhistoryorphysicalexaminationofthefollowingconditions a Central sleep apnea b Congestive heart failure c Chronic pulmonary disease such as chronic obstructive pulmonary disease d Pulmonary hypertension e Obesityhypoventilationsyndromeorotherconditionwhichmaycausenocturnalarterialoxyhemoglobin desaturationbull Surgical Management A Uvulopalatopharyngoplasty(UPPP) UPPPmaybeconsideredMEDICALLYNECESSARYwhenallthefollowingcriteriaaremet 1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a BMI less than 40 AND bAtrialoforalappliancetherapyhasfailedorthepatientisnotacandidateforanoralappliance AND c PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hoursper nightforthree(3)monthsofPAPusage B Maxillofacial Procedures Maxillofacial surgical procedures such as inferior sagittal mandibular osteotomy and genioglossal advancement
withorwithouthyoidmyotomyandsuspensionormandibular-maxillaryadvancement(MMA)maybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a Objectiveevidenceofhypopharyngealobstructiondocumentedbyeitherfiberopticexaminationor cephalometric radiographs AND
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 16
b PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hourspernightforthree(3)monthsofPAPusage
bull Treatment of Snoring TreatmentofsnoringisconsideredNOTMEDICALLYNECESSARYbecausesimplesnoringintheabsenceof
documented obstructive sleep apnea is not considered a medical condition Therefore all procedures for the sole or adjunctivetreatmentofsnoringareconsideredNOTMEDICALLYNECESSARYincludingbutnotlimitedto
A Uvulopalatopharyngoplasty(UPPP) B Uvulectomy C Laser-assisteduvulopalatoplasty(LAUP) D Radiofrequencyvolumetricreductionofthepalataltissues E Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues F Palatal stiffening procedures including but not limited to cautery-assisted palatal stiffening operation and the
implantation of palatal implants G Tongue base suspensionbull Investigative Indications ThefollowingtreatmentsareconsideredINVESTIGATIVEduetoalackofevidencedemonstratingimprovedhealth outcomes AUPPPforanyconditionotherthanobstructivesleepapneaorsnoring B ExpiratoryPositiveAirwayPressure(EPAP)includingtheProventregdevice C OralpressuretherapydevicesincludingbutnotlimitedtotheWinxTMsystem D Atrialpacing EAllothersurgicalproceduresforthesoleoradjunctivetreatmentofobstructivesleepapneaupperairwayresistance
syndrome including but not limited to 1 Uvulectomy 2Laser-assisteduvulopalatoplasty(LAUP) 3Radiofrequencyvolumetricreductionofthepalataltissues 4Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues 5Palatalstiffeningproceduresincludingbutnotlimitedtocautery-assistedpalatalstiffeningoperationandthe
implantation of palatal implants 6 Tongue base suspension 7 Implantable hypoglossal nerve stimulators Respiratory Syncytial Virus (RSV) Prophylaxis bull INITIALRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVfortheinitialRSVseasonmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A ChronicLungDisease(CLD)ofPrematurity 1Infantwasbornatlt32weeks0daysgestationAND 2Infantisle12monthsofageattheonsetofRSVseasonAND 3Infantrequiresgt21oxygenforatleastthefirst28daysafterbirth B Congenital Heart Disease (CHD) 1 Infant is le12monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 17
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
a AcyanoticCHDwhentheinfantisreceivingmedicationtocontrolcongestiveheartfailureandwillrequireacardiacsurgicalprocedureOR
b CyanoticCHDwhenpalivizumabisrecommendedafterconsultationwithapediatriccardiologistOR c Diagnosis of moderate to severe pulmonary hypertension OR 2Childislt24monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing a ChildundergoescardiactransplantationduringtheRSVseasonOR b ChildisreceivingRSVprophylaxisandcontinuestorequireprophylaxisafterasurgicalprocedureinvolving cardiac bypass or at the conclusion of extracorporeal membrane oxygenation C AnatomicPulmonaryAbnormalitiesORNeuromuscularDisorder(egcerebralpalsymusculardystrophy) 1 Infant is le12monthsofageattheonsetofRSVseasonAND 2Infanthasimpairedabilitytoclearsecretionsfromtheupperairway D Cystic Fibrosis 1 Infant is le12monthsofageattheonsetofRSVseasonwithevidenceofCLDandormalnutrition E Immunocompromised Status 1Childislt24monthsofageattheonsetofRSVseasonAND 2Childisprofoundlyimmunocompromised(egduetosolidorgantransplantationhematopoieticstem-cell
transplantation or chemotherapy) F Prematurity without CLD or CHD 1Infantwasbornatlt29weeks0daysgestation(ie28weeks6daysorless)AND 2Infantislt12monthsofageattheonsetofRSVseasonbull SECONDRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVforthepatientrsquossecondyearoftreatmentmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A CLDofPrematurity 1Childwasbornatlt32weeks0daysgestationAND 2Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonAND 3ChildcontinuestorequireatleastONEofthefollowingwithinsix(6)monthsofthestartofthesecondRSV season a SupplementaloxygenOR b ChronicsystemiccorticosteroidtherapyOR c DiuretictherapyOR d Bronchodilator therapy B Cystic Fibrosis 1Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonwithevidenceofCLDandor malnutritionbull AdministrationofRSVProphylaxis A Whentheappropriatecriteriaabovearemetamaximumoffive(5)monthlydosesofpalivizumab(Synagisreg)will
becoveredperRSVseason(definedasNovember1stthroughMarch31st) B Thefirstmonthlydoseofpalivizumab(Synagisreg)willbeapprovedforcoverageofadministrationonorafter
November 1st C Apost-operativedoseofpalivizumab(Synagisreg)willbecoveredforchildrenlt24monthswhoarereceiving
RSVprophylaxisandcontinuetorequireprophylaxisafterasurgicalprocedureinvolvingcardiacbypassorattheconclusion of extracorporeal membrane oxygenation
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring
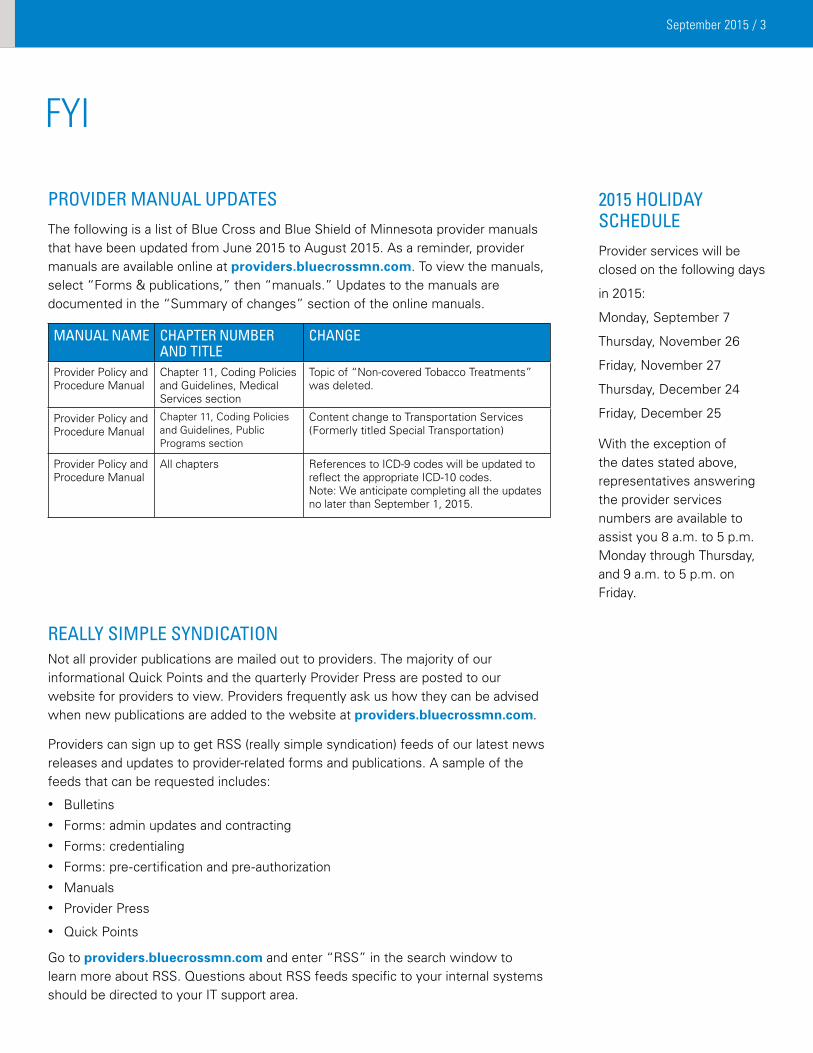
September 2015 3
FYI
PROvIDER MANUAL UPDATES The following is a list of Blue Cross and Blue Shield of Minnesota provider manuals thathavebeenupdatedfromJune2015toAugust2015Asareminderprovidermanuals are available online at providersbluecrossmncom To view the manuals select ldquoForms amp publicationsrdquo then ldquomanualsrdquo Updates to the manuals are documented in the ldquoSummary of changesrdquo section of the online manuals
MANUAL NAME
CHAPTER NUMbER AND TITLE
CHANGE
Provider Policy and Procedure Manual
Chapter 11 Coding Policies and Guidelines Medical Services section
Topic of ldquoNon-covered Tobacco Treatmentsrdquo was deleted
Provider Policy and Procedure Manual
Chapter 11 Coding Policies and Guidelines Public Programs section
Content change to Transportation Services (Formerly titled Special Transportation)
Provider Policy and Procedure Manual
Allchapters ReferencestoICD-9codeswillbeupdatedtoreflect the appropriate ICD-10 codes Note We anticipate completing all the updates nolaterthanSeptember12015
REALLy SIMPLE SyNDICATION Not all provider publications are mailed out to providers The majority of our informational Quick Points and the quarterly Provider Press are posted to our website for providers to view Providers frequently ask us how they can be advised when new publications are added to the website at providersbluecrossmncom
ProviderscansignuptogetRSS(reallysimplesyndication)feedsofourlatestnewsreleasesandupdatestoprovider-relatedformsandpublicationsAsampleofthefeeds that can be requested includes
bull Bulletinsbull Forms admin updates and contractingbull Forms credentialingbull Formspre-certificationandpre-authorizationbull Manualsbull Provider Press
bull Quick Points
Go to providersbluecrossmncomandenterldquoRSSrdquointhesearchwindowtolearnmoreaboutRSSQuestionsaboutRSSfeedsspecifictoyourinternalsystemsshould be directed to your IT support area
2015 HOLIDAy SCHEDULEProvider services will be closed on the following days
in2015
Monday September 7
ThursdayNovember26
FridayNovember27
ThursdayDecember24
FridayDecember25
With the exception of the dates stated above representatives answering the provider services numbers are available to assistyou8amto5pmMonday through Thursday and9amto5pmonFriday
September 2015 4
CodINg CorNer
REPLACEMENT CLAIM REMINDERWhendoIneedareplacementclaimWellareyoumakingchangestoaclaimthatwaspreviouslyprocessedIfyesyouwillneedtosendinareplacementclaimThisincludes
bull changing a date of service
bull adding or changing a procedure
bull adding or changing a diagnosis
bull removing a modifier
bull adding a modifier
Note that when adding modifiers -24 -25 -57 -59 -78 andor 79 medical notes supporting the modifier also need to be sent with the replacement claim
SeeProviderBulletinP28-14datedOctober12014formoreinformation
26 OR TC USENot every code in particular radiology codes has a professional component (reported witha-26modifier)andtechnicalcomponent(reportedwithandashTCmodifier)ForexampleCPTcode77387isldquoGuidanceforlocalizationoftargetvolumefordeliveryof radiation treatment delivery includes intrafraction tracking when performedrdquo This code does not have a professional or technical component Thus if it is submitted with acomponentmodifier(-26or-TC)itwillbedeniedbecauseaninvalidmodifierwasappended to the service
ICD-10 CODING UPDATE AND FINAL REMINDERS continued from page 1
httpwwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesDownloadsSE1325pdf
UsethecorrectcodequalifierindicatingwhetherthecodeisICD-9orICD-10forthecode setbeingreportedintheHIPAAtransaction
Reviewyourclaimacknowledgementreportstimelytoensureclaimshavebeencorrectlysubmitted and accepted by Blue Cross Claims rejected on these reports must be corrected and submitted again Claims rejected on acknowledgment reports are not considered submitted for timely filing purposes
AdditionalinformationisavailableundertheICD-10compliancelinkonourwebsiteatprovidersbluecrossmncom
Questions
If you have questions please contact provider services at (651) 662-5200 or 1-800-262-0820
THE HCPCS ARE COMING THE HCPCS ARE COMING Itrsquos not just the ICD codes that will be the coding stars onOctober12015HCPCScodes are updated as well on that fall date Blue Cross will publish a Provider Bulletin closer to the October12015effectivedate that provides more details
September 2015 5
HeALTH LITerACY
Try both aleve 2pills bid with flexeril at hs
Asahealthcareprofessionalyouprobablyunderstandexactlywhatthedoctorwhosentthismessage was saying Take 2 Aleve pills 2 times a day and take 1 Flexeril pill at bedtime But the patient who received it had no idea what the doctor was saying Most people donrsquot Clear communication increases patient safety and adherence to treatment plans
OctoberishealthliteracymonthHerearesomeactivitiesthatyourpracticecliniccanincorporate to help make a healthy difference in your patientrsquos lives
Use the Teach Back method also known as the ldquoshow-merdquo technique to ensure that patients (or care takers) understand their treatment plan and what they need to do Think aboutdoingasimpleteachbacktrainingatyourpracticeduringthemonthofOctoberClickhere for a program ready to use from the Minnesota Health Literacy Partnership
Promote the Ask Me 3 program from the National Patient Safety Foundation which focuses onpatientunderstandingof3simplequestions
1)Whatismymainproblem
2)WhatdoIneedtodo
3)Whyisitimportantformetodothis
You can use these questions to help guide the information you provide during visits with your patients Make sure they know the answer to these questions before they leave your office ConsiderdisplayingpostersandbrochuresthroughoutyourofficeduringOctobertoremindstaffaboutthe3questionsFormoreinformationonAskMe3clickhere
Review your own patient education materials Select a few of the patient education materials that you commonly use in your practice and review them using one of the health literacytoolsfromtheOfficeofDiseasePreventionandHealthPromotionPerhapsformateam to review the pieces together Click hereforresourcesOrcontactusifyouwantacopy of the tool used at Blue Cross
To learn more about building a culture of health literacy and using plain language at your practice please send an email to AlishaOdhiambobluecrossmncomAdditionalinformationcan also be found online at httphealthliteracymnorg
September 2015 6
QuALITY ImproVemeNT
PCC QUALITy OF CARE COMPLAINT REPORTProviders are required to complete the Blue Plus Quality of Care Complaint report forallwrittenandverbalcomplaintsfromBluePlusPrepaidMedicalAssistanceProgram and MinnesotaCare subscribers on a quarterly basis per Minnesota Department of Health regulations Complaints logged at the provider offices are to be investigated and resolved by the providerrsquos office whenever possible
ThesecomplaintsarereportedtoBluePlusinJanuaryAprilJulyandOctoberfor the preceding three months The Primary Care Clinic (PCC) must submit a quarterly report even if the facility does not receive any complaints for the quarter YourcontractoutlinestheproceduresrequiredforyourQualityofCare(QOC)PCCcomplaint reporting adherence agreement
Complaints should no longer be directed to the attention of a single designated personSendingyourPCCQOCcomplaintreportformtoanysourcenotlistedbelowmaydelaytheprocessingofyourPCCQOCcomplaintreport
ToaccessthePCCBluePlusQualityofCareComplaintReportFormgoto providersbluecrossmncom and select ldquoForms amp publicationsrdquo then ldquoforms - clinical operationsrdquo
Submit quarterly PCC QOC reports using one of these methods
Email pcccomplaintbluecrossmncom
Secure fax line (651) 662-4004
Mail Blue Plus AttnQualityHealthManagementDept R472 POBox64179 StPaulMN55164-0179
UTILIzATION MANAGEMENT STATEMENTUtilizationManagement(UM)decisionmakingisbasedonlyonappropriatenessofcareand service and on existing coverage provisions Blue Cross does not compensate providers practitioners or other individuals making UM decisions for denial of coverage or services We do not offer incentives to decision makers to encourage denial of coverage or services that would result in less than appropriate care
September 2015 7
QuALITY ImproVemeNT
CLINICAL PRACTICE GUIDELINES Blue Cross believes that the use of clinical practice guidelines is a key component of Quality Improvement Each year Blue Crossrsquo Clinical Practice Quality Committee (a designee of the Quality Council) approves the adoption of select guidelines that are used to support various programs and initiatives The guidelines do not substitute for sound clinical judgment however they are intended to assist clinicians in understanding key processes for improvement efforts
Clinical Practice Guidelines with hyperlinks are available in Chapter Three of the Blue Cross Provider Policy and Procedure Manual To access the manual go to providersbluecrossmncom and select ldquoForms and Publicationsrdquo then ldquoManualsrdquo
Recommended sources BlueCrossrecognizesthefollowingsourcesforClinicalPracticeGuidelinesfora variety of areas of clinical practice
bullUSPSTFUSPreventiveServicesTaskForce httpwwwuspreventiveservicestaskforceorgbrowseRecIndex
bullAAPAmericanAcademyofPediatricsincludingBrightFutures httppediatricsaappublicationsorgsearchflag=practice_guidelinesampsubmit=yesampx=18ampy=8ampformat=standardamphits=30ampsortspec=dateampsubmit=Gohttppediatricsaappublicationsorgsearchflag=practice_guidelinesampsubmit=yesampx=18ampy=8ampformat=standardamphits=30ampsortspec=dateampsubmit=Go
httpbrightfuturesaaporg
bullICSIInstituteforClinicalSystemsImprovement httpswwwicsiorgguidelines__moreguidelines_a_to_z
Specific guidelines Specific guidelines recommended by Blue Cross include the following
bullBehavioralHealth-ADHD-DiagnosisEvaluationandTreatmentofAttention-DeficitHyperactivityDisorderinChildrenandAdolescents(AAP)-DepressionScreeninginAdults(USPSTF)
bullNon-PreventiveAcuteorChronicConditions-DiabetesndashDiagnosisandManagementofType2DiabetesMellitusinAdults(ICSI)-AsthmandashDiagnosisandManagementofAsthma(ICSI)
bullPreventiveCareGuidelines-PreventiveServicesforAdults(ICSI)-PreventiveServicesChildrenandAdolescents(ICSIandBrightFutures)-RoutinePrenatalCare(ICSI)
Questions concerning Clinical Practice Guidelines can be directed to Eileen Johnson Director Quality and Health Management at (651) 662-4224Acopyoftheclinicalpractice guidelines with hyperlinks is also available by calling Eileen Johnson
September 2015 8
QuALITY ImproVemeNT
bLUE PLUS MEDICAL RECORD DOCUMENTATION REvIEwAdvance Directives
Anadvancedirectiveprovidesanopportunityforadultsofanyagetomaketheirhealthcare wishes known if or when a potential life-threatening event occurs and they are unabletoverbalizetheirwishesatthetimeoftheevent
ArepresentativesamplereviewofourBluePlusmembersrsquomedicalrecordsfordatesofservicein2014hasbeencompletedandtheresultsarebelowWeencourageprovidersto discuss the benefits of completing an advance directive with all our adult members
TOTAL MEMbERS IN SAMPLE
ADvANCE DIRECTIvE PRESENT OR DISCUSSED
AGE RANGE FOR MEMbERS wITH DISCUSSION
MedicareMedicaid Eligible(MSHO)
300 187(62) Avg83Range67-107
Medicaid 600 61(10) Avg48Range20-64
Body Mass Index (BMI) And Counseling For Obesity
Documentation of a memberrsquos BMI is the first step towards addressing the prevalence of obesity in our society Blue Plus completed a review of a sample of Blue Plus membersrsquomedicalrecordswithdatesofservicein2014toevaluatedocumentationofBMIvalueandcounselingforobesityObesityisdefinedasaBMIover30TheresultsareshownbelowOne-thirdofMedicaidmembersdefinedasobesehad documentation of a discussion with their provider concerning their weight management
TOTAL MEMbERS
bMI DOCUMENTED
bMI gt 30 (IF DOCUMENTED)
IF bMI gt 30 ADvISED ON wEIGHT MANAGEMENT
AvERAGE bMI FOR MEMbERS wITH DISCUSSION
MedicareMedicaid Eligible(MSHO)
300 183(61) 70(38) 6(9) Avg3603 Range3089-501
Medicaid 600 550(92) 237(43) 93(39) Avg3807 Range2676-710
Total 900 733(81) 307(42) 99(32) Avg3795
continued on next page
September 2015 9
bLUE PLUS MEDICAL RECORD DOCUMENTATION REvIEw continuedfrompage8
Tobacco Use Assessment And Counseling
AsampleofmedicalrecordswerereviewedtodeterminetobaccouseamongourBlue Plus members and discussions promoting tobacco cessation during a provider visitin2014Whiletobaccouseappearstoberoutinelyassessedatleastonceduring2014onlyhalfofourmembershavedocumentationofprovidereffortsinaddressingthis health concern
TOTAL MEMbERS
ASSESSED FOR TObACCO USE
TObACCO USE AvERAGE AGE OF TObACCO USERS
DISCUSSION ANDOR Rx ASSISTANCE
MSHO 300 281(93) 24(85) Avg75(67-87)
10(42)
PMAPMNCARE 600 518(86) 164(32) Avg44(20-64)
89(54)
Total 900 799(89) 188(24) Avg49 (20-87)
99(53)
These reviews were completed to encourage providers to open the door to meaningful discussions with their patients on important health issues If you have any questions concerning this article please send an email to the Quality and Health Management department co Sheiladalenbluecrossmncom
Better Care Through Quality Improvement
Every year Blue Cross and Blue Shield of Minnesota (Blue Cross) reviews the care delivered to our subscribers This review determines the goals for the quality program The program currently has many goals to improve health services
Making sure our subscribers receive preventive services and health screenings making sure people with health problems like heart disease receive treatment and improving the customer service experience are just a few of the goals in the program
More detailed information is available about Blue Crossrsquo process and outcomes in meeting quality improvement goals related to subscriber care and service You can see more information about our quality improvement program at bluecrossmncom Enter ldquoquality improvement programrdquo in the search field If you are unable to access the website please contact Eileen Johnson Director | AccreditationampQualityImprovementat(651) 662-4224 to request information about the Quality Improvement Program
QuALITY ImproVemeNT
September 2015 10
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
Medical and behavioral health policies are available for your use and review on the Blue Cross and Blue Shield of Minnesota website at providersbluecrossmncom From this site there are two ways to access medical policy information depending on the patientrsquos Blue Plan membership
For out-of-area Blue Plan patients SelectldquoMedicalPolicyPreCertPreAuthRouterrdquoandclickGoYouwillbetakentothepagewhereyouselecteithermedicalpolicyorpre-certificationpriorauthorizationandenterthepatientrsquosthree-letteralphaprefixasfoundontheirmemberidentificationcardandclickGoOnceyouaccepttherequirementsyouwillberoutedtothepatientrsquoshomeplanwhereyoucanaccessmedicalpolicyorpre-certificationpre-authorizationinformation
For local Blue Cross and Blue Shield of Minnesota plan patients SelectldquoMedicalpolicyrdquo(undertheToolsampResources)readandaccepttheBlueCrossMedicalPolicyStatementandthenselectldquoViewAllActivePoliciesrdquoYouhavenownavigatedtotheBlueCrossandBlueShieldofMinnesotaMedicaland Behavioral Health Policy Manual where there are several selections to assist with your inquiry
The ldquoWhatrsquos Newrdquo section identifies our latest new or revised policies approved by Blue Crossrsquo Medical and Behavioral Health Policy Committee at least 50 days ago These policies are now effective and providers should begin following thesepoliciesimmediatelyThesepoliciesalsoappearintheldquoActivePolicyrdquosectionoftheMedicalandBehavioralHealthPolicy Manual
The ldquoUpcoming Policiesrdquo section lists new or revised policies approved by the Blue Cross Medical and Behavioral Health Policy Committee and are effective 50 days from the date they were posted to the ldquoUpcoming Policiesrdquo section of the Medical and Behavioral Health Policy Manual
TheldquoActivePolicyrdquosectioncontainstheentirelistofpolicieseffectiveatthetimeofyourinquiryPleasenoteDHSPrograms(CoverageGuidelinesforDHSPrograms-MHCPManual)andMedicareContractors(PartAndashNationalGovernmentServices[NGS]PartBndashNationalGovernmentServices[NGS]HomeHealthandHospicendashNationalGovernmentServices[NGS]DurableMedicalEquipmentMedicareAdministrativeContractorndashNationalGovernmentServices[NGS]andTheCentersforMedicareandMedicaidServicesndashCMS)haveseparatesections
TheldquoPre-CertificationPre-Authorizationrdquosectionidentifiesvariousservicesproceduresprescriptiondrugsandmedicaldevicesthatrequirepre-certificationpre-authorizationThefollowingPre-CertificationPre-AuthorizationListsareprovidedforreviewCommercial(includingBlueLinkTPA)MNGovernmentProgramsandMedicarePlansTheselistsarenotexclusive to medical policy services only they encompass other services that are subject to pre-certification pre-authorizationrequirements
If you have additional questions regarding medical or behavioral health policy issues call provider services at (651) 662-5200 or 1-800-262-0820 for assistance
September 2015 11
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
MEDICAL AND bEHAvIORAL HEALTH POLICy ACTIvITy
Policies Effective 072015 Notification Posted 052815
Policies developedNone
Policies revisedPneumatic Compression Devices in the Outpatient or Home Setting
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentoflymphedemaintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet 1 The patient has undergone a four-week trial of conservative therapy which includes a Use of an appropriate compression bandage system or compression garment bExerciseAND c Elevation of the limb AND 2 Thetreatingphysiciandeterminesthatnosignificantimprovementhasoccurredorsignificantsymptomsremain
following the four-week trialbull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (non-programmable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps) OR
2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompressiontreatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentofchronicvenousinsufficiencyofthelowerextremitiesintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet
1 The patient has one or more venous stasis ulcers AND 2 ThepatienthasundergoneatrialofconservativetherapyforaminimumofsixmonthswhichincludesALLofthe
following a The use of an appropriate compression bandage system or compression garment bAppropriatedressingsforthewound c Exercise and d Elevation of the limb AND 3 Thetreatingphysiciandeterminesthatthevenousstasisulcerhasfailedtoheal
September 2015 12
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
bull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (nonprogrammable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
OR 2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompression
treatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingmaybeconsideredMEDICALLYNECESSARYinpatientswhohaveundergoneasurgicalprocedurewhenBOTH1and2aremet
1 Patient meets one or more of the following a Major surgery (eg total hip arthroplasty total knee arthroplasty hip fracture repair open abdominal or open
pelvic procedure OR b Patient is at moderate to severe risk of VTE Examples include i Patient is not able to walk unassisted or is bedridden ii Agegreaterthan60yearsanesthesiaatleast2hoursandbedrestatleast4daysduringcurrentepisodeofcare iii Inpatientstayofmorethan2daysduringcurrentepisodeofcare iv Central venous access during current episode of care v Sepsis during current episode of care viActivecancerorcancertreatment vii Significant comorbidity such as recent myocardial infarction congestive heart failure cerebrovascular disease
moderate to severe chronic obstructive pulmonary disease moderate to severe liver disease moderate to severe chronic kidney disease
viiiPregnancy or post-partum state (lt 1 month) ix Hypercoagulable state (eg Factor V Leiden antithrombin III deficiency protein C or S deficiency
antiphospholipidsyndromedysfibrinolysisprothrombin20210defect) x Prior VTE AND 2Thepatienthasacontraindicationtopharmacologicanticoagulantssuchasbeingathigh-riskforbleedingRisk
factors for bleeding include a Bleeding disorder such as hemophilia bActiveliverdisease c Severe renal failure d Previous major bleed (and previous bleeding risk similar to current risk) e Concomitant antiplatelet agent f History of or difficult-to-control surgical bleeding during the current operative procedure extensive surgical
dissection and revision surgery bull Outpatientorhomeuseofpneumaticcompressiondevicesforpost-surgicalVTEprophylaxisisconsideredNOTMEDICALLYNECESSARYforpatientswhohaveundergoneasurgicalprocedurewithalowriskforVTEandwhohaveno additional risk factors for VTE Examples of lower risk surgical procedures include but are not limited to laparoscopic cholecystectomy appendectomy transurethral prostatectomy and inguinal herniorrhaphy
September 2015 13
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingisconsideredINVESTIGATIVEforallotherindications including but not limited to treatment of arterial insufficiency (e g peripheral arterial disease) and restless legs syndrome due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Angioplasty andor Stenting for Intracranial Aneurysms and Atherosclerosis
bull IntracranialstentplacementmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranial aneurysms for patients when surgical treatment is not feasible and standard endovascular techniques do not allowforcompleteisolationoftheaneurysmegwide-neckaneurysm(4mmormore)orsack-to-neckratiolessthan21
bull IntracranialflowdivertingstentswithFDAapprovalforthetreatmentofintracranialaneurysmsmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranialaneurysmsthatarelargeorgiantwide-necked(aneurysmsizeof10mmormoreandaneckdiameterof4mmormore)intheinternalcarotidarteryfrom the petrous to the superior hypophyseal segments and which are not amenable to surgical treatment or standard endovascular therapy
bull IntracranialstentplacementisconsideredINVESTIGATIVEinthetreatmentofintracranialaneurysmsexceptasnotedabove due to the lack of clinical evidence demonstrating its impact on improved health outcomes
bull PercutaneoustransluminalangioplastywithorwithoutstentingisconsideredINVESTIGATIVEforthetreatmentofintracranial atherosclerosis due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Surgical Treatment of Femoroacetabular Impingement
bull OpenorarthroscopictreatmentoffemoroacetabularimpingementmaybeconsideredMEDICALLYNECESSARYwhenALLofthefollowingconditionsaremet
AAge Patientisskeletallymaturewithdocumentedclosureofgrowthplates(eg15yearsorolder) B Symptoms 1 Moderate-to-severe hip pain that is worsened by flexion activities (eg squatting or prolonged sitting) and which
significantlylimitsactivitiesAND 2Painwhichisunresponsiveorrecursafteratrialofconservativetherapylastingatleast3months(including
activitymodificationsrestrictionofathleticpursuitsandavoidanceofsymptomaticmotion)AND 3Positiveimpingementsignispresentonclinicalexamination(painelicitedwith90degreesofflexionandinternal
rotation and adduction of the femur) C Imaging 1Imagingstudies(egx-raysMRI)confirmthediagnosisofacamorpincer-typeFAIExamplesofmorphology
indicativeofFAIinclude a pistol-grip deformity
b femoralhead-neckoffsetwithanalphaanglegreaterthan50degrees c a positive wall sign d acetabular retroversion (overcoverage with crossover sign) e coxa profunda or protrusion f damage of the acetabular rim AND 2Noevidenceofadvancedosteoarthritis(definedasTonnisgradeIIorIIIorjointspaceoflessthan2mm)AND 3Noevidenceofsevere(modifiedOuterbridgegradeIV)chondraldamagebull Surgicaltreatmentoffemoroacetabularimpingement(FAI)isconsideredINVESTIGATIVEinallothersituations
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 14
Policies inactivatedTobacco Cessation Treatments
Policies Effective 081715 Notification Posted 062515
Policies developedNone
Policies revisedTreatment of Obstructive Sleep Apnea and Snoring in Adults bull Medical Management
A IntraoralAppliances Intraoral appliances (eg mandibular advancingpositioning devices or tongue-retaining devices) may be considered
MEDICALLYNECESSARYwhenALLofthefollowingcriteriaaremet 1PatienthasbeendiagnosedwithOSAdefinedby a AnAHIorRDIof15orgreatereventsperhour OR bAnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms i Excessive daytime sleepiness ii Documented hypertension iii Ischemic heart disease iv History of stroke AND 2Thereisabsenceoftemporomandibulardysfunctionorperiodontaldisease AND 3ThedeviceisprescribedafteradiagnosisofOSAhasbeenestablishedbyaphysicianwhoiseitheradiplomate
oftheAmericanBoardofSleepMedicinearecognizedsubspecialtyoftheAmericanBoardofMedicalSpecialties(ABMS)oranactivestaffmemberofasleepcenterorlaboratoryaccreditedbytheAmericanAcademyofSleepMedicine(AASM)orTheJointCommission
AND 4 The device is custom-fitted by qualified dental personnel under the direction of a Doctor of Dental Surgery (DDS)
or Doctor of Dental Medicine (DMD) B ContinuousPositiveAirwayPressure(CPAP) Continuouspositiveairwaypressure(CPAP)maybeconsideredMEDICALLYNECESSARYinpatientswith
confirmedOSAwith 1AnAHIorRDIof15eventsperhourorgreater OR 2AnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms a Excessive daytime sleepiness b Documented hypertension c Ischemic heart disease d History of stroke
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 15
C Bi-levelPositiveAirwayPressure(BiPAP) BiPAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPAND 2HavefailedapriortrialofCPAPOR 3ForwhomBiPAPisfoundtobemoreeffectivethanCPAPinthesleeplaboratory D Auto-AdjustingPAP(APAP) APAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPaboveAND 2HaveacontraindicationtoCPAPhavefailedapriortrialofCPAPORareundergoingatrialofAPAPtotitrate CPAP AND 3Havenoevidencebyhistoryorphysicalexaminationofthefollowingconditions a Central sleep apnea b Congestive heart failure c Chronic pulmonary disease such as chronic obstructive pulmonary disease d Pulmonary hypertension e Obesityhypoventilationsyndromeorotherconditionwhichmaycausenocturnalarterialoxyhemoglobin desaturationbull Surgical Management A Uvulopalatopharyngoplasty(UPPP) UPPPmaybeconsideredMEDICALLYNECESSARYwhenallthefollowingcriteriaaremet 1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a BMI less than 40 AND bAtrialoforalappliancetherapyhasfailedorthepatientisnotacandidateforanoralappliance AND c PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hoursper nightforthree(3)monthsofPAPusage B Maxillofacial Procedures Maxillofacial surgical procedures such as inferior sagittal mandibular osteotomy and genioglossal advancement
withorwithouthyoidmyotomyandsuspensionormandibular-maxillaryadvancement(MMA)maybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a Objectiveevidenceofhypopharyngealobstructiondocumentedbyeitherfiberopticexaminationor cephalometric radiographs AND
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 16
b PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hourspernightforthree(3)monthsofPAPusage
bull Treatment of Snoring TreatmentofsnoringisconsideredNOTMEDICALLYNECESSARYbecausesimplesnoringintheabsenceof
documented obstructive sleep apnea is not considered a medical condition Therefore all procedures for the sole or adjunctivetreatmentofsnoringareconsideredNOTMEDICALLYNECESSARYincludingbutnotlimitedto
A Uvulopalatopharyngoplasty(UPPP) B Uvulectomy C Laser-assisteduvulopalatoplasty(LAUP) D Radiofrequencyvolumetricreductionofthepalataltissues E Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues F Palatal stiffening procedures including but not limited to cautery-assisted palatal stiffening operation and the
implantation of palatal implants G Tongue base suspensionbull Investigative Indications ThefollowingtreatmentsareconsideredINVESTIGATIVEduetoalackofevidencedemonstratingimprovedhealth outcomes AUPPPforanyconditionotherthanobstructivesleepapneaorsnoring B ExpiratoryPositiveAirwayPressure(EPAP)includingtheProventregdevice C OralpressuretherapydevicesincludingbutnotlimitedtotheWinxTMsystem D Atrialpacing EAllothersurgicalproceduresforthesoleoradjunctivetreatmentofobstructivesleepapneaupperairwayresistance
syndrome including but not limited to 1 Uvulectomy 2Laser-assisteduvulopalatoplasty(LAUP) 3Radiofrequencyvolumetricreductionofthepalataltissues 4Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues 5Palatalstiffeningproceduresincludingbutnotlimitedtocautery-assistedpalatalstiffeningoperationandthe
implantation of palatal implants 6 Tongue base suspension 7 Implantable hypoglossal nerve stimulators Respiratory Syncytial Virus (RSV) Prophylaxis bull INITIALRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVfortheinitialRSVseasonmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A ChronicLungDisease(CLD)ofPrematurity 1Infantwasbornatlt32weeks0daysgestationAND 2Infantisle12monthsofageattheonsetofRSVseasonAND 3Infantrequiresgt21oxygenforatleastthefirst28daysafterbirth B Congenital Heart Disease (CHD) 1 Infant is le12monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 17
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
a AcyanoticCHDwhentheinfantisreceivingmedicationtocontrolcongestiveheartfailureandwillrequireacardiacsurgicalprocedureOR
b CyanoticCHDwhenpalivizumabisrecommendedafterconsultationwithapediatriccardiologistOR c Diagnosis of moderate to severe pulmonary hypertension OR 2Childislt24monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing a ChildundergoescardiactransplantationduringtheRSVseasonOR b ChildisreceivingRSVprophylaxisandcontinuestorequireprophylaxisafterasurgicalprocedureinvolving cardiac bypass or at the conclusion of extracorporeal membrane oxygenation C AnatomicPulmonaryAbnormalitiesORNeuromuscularDisorder(egcerebralpalsymusculardystrophy) 1 Infant is le12monthsofageattheonsetofRSVseasonAND 2Infanthasimpairedabilitytoclearsecretionsfromtheupperairway D Cystic Fibrosis 1 Infant is le12monthsofageattheonsetofRSVseasonwithevidenceofCLDandormalnutrition E Immunocompromised Status 1Childislt24monthsofageattheonsetofRSVseasonAND 2Childisprofoundlyimmunocompromised(egduetosolidorgantransplantationhematopoieticstem-cell
transplantation or chemotherapy) F Prematurity without CLD or CHD 1Infantwasbornatlt29weeks0daysgestation(ie28weeks6daysorless)AND 2Infantislt12monthsofageattheonsetofRSVseasonbull SECONDRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVforthepatientrsquossecondyearoftreatmentmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A CLDofPrematurity 1Childwasbornatlt32weeks0daysgestationAND 2Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonAND 3ChildcontinuestorequireatleastONEofthefollowingwithinsix(6)monthsofthestartofthesecondRSV season a SupplementaloxygenOR b ChronicsystemiccorticosteroidtherapyOR c DiuretictherapyOR d Bronchodilator therapy B Cystic Fibrosis 1Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonwithevidenceofCLDandor malnutritionbull AdministrationofRSVProphylaxis A Whentheappropriatecriteriaabovearemetamaximumoffive(5)monthlydosesofpalivizumab(Synagisreg)will
becoveredperRSVseason(definedasNovember1stthroughMarch31st) B Thefirstmonthlydoseofpalivizumab(Synagisreg)willbeapprovedforcoverageofadministrationonorafter
November 1st C Apost-operativedoseofpalivizumab(Synagisreg)willbecoveredforchildrenlt24monthswhoarereceiving
RSVprophylaxisandcontinuetorequireprophylaxisafterasurgicalprocedureinvolvingcardiacbypassorattheconclusion of extracorporeal membrane oxygenation
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 4
CodINg CorNer
REPLACEMENT CLAIM REMINDERWhendoIneedareplacementclaimWellareyoumakingchangestoaclaimthatwaspreviouslyprocessedIfyesyouwillneedtosendinareplacementclaimThisincludes
bull changing a date of service
bull adding or changing a procedure
bull adding or changing a diagnosis
bull removing a modifier
bull adding a modifier
Note that when adding modifiers -24 -25 -57 -59 -78 andor 79 medical notes supporting the modifier also need to be sent with the replacement claim
SeeProviderBulletinP28-14datedOctober12014formoreinformation
26 OR TC USENot every code in particular radiology codes has a professional component (reported witha-26modifier)andtechnicalcomponent(reportedwithandashTCmodifier)ForexampleCPTcode77387isldquoGuidanceforlocalizationoftargetvolumefordeliveryof radiation treatment delivery includes intrafraction tracking when performedrdquo This code does not have a professional or technical component Thus if it is submitted with acomponentmodifier(-26or-TC)itwillbedeniedbecauseaninvalidmodifierwasappended to the service
ICD-10 CODING UPDATE AND FINAL REMINDERS continued from page 1
httpwwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesDownloadsSE1325pdf
UsethecorrectcodequalifierindicatingwhetherthecodeisICD-9orICD-10forthecode setbeingreportedintheHIPAAtransaction
Reviewyourclaimacknowledgementreportstimelytoensureclaimshavebeencorrectlysubmitted and accepted by Blue Cross Claims rejected on these reports must be corrected and submitted again Claims rejected on acknowledgment reports are not considered submitted for timely filing purposes
AdditionalinformationisavailableundertheICD-10compliancelinkonourwebsiteatprovidersbluecrossmncom
Questions
If you have questions please contact provider services at (651) 662-5200 or 1-800-262-0820
THE HCPCS ARE COMING THE HCPCS ARE COMING Itrsquos not just the ICD codes that will be the coding stars onOctober12015HCPCScodes are updated as well on that fall date Blue Cross will publish a Provider Bulletin closer to the October12015effectivedate that provides more details
September 2015 5
HeALTH LITerACY
Try both aleve 2pills bid with flexeril at hs
Asahealthcareprofessionalyouprobablyunderstandexactlywhatthedoctorwhosentthismessage was saying Take 2 Aleve pills 2 times a day and take 1 Flexeril pill at bedtime But the patient who received it had no idea what the doctor was saying Most people donrsquot Clear communication increases patient safety and adherence to treatment plans
OctoberishealthliteracymonthHerearesomeactivitiesthatyourpracticecliniccanincorporate to help make a healthy difference in your patientrsquos lives
Use the Teach Back method also known as the ldquoshow-merdquo technique to ensure that patients (or care takers) understand their treatment plan and what they need to do Think aboutdoingasimpleteachbacktrainingatyourpracticeduringthemonthofOctoberClickhere for a program ready to use from the Minnesota Health Literacy Partnership
Promote the Ask Me 3 program from the National Patient Safety Foundation which focuses onpatientunderstandingof3simplequestions
1)Whatismymainproblem
2)WhatdoIneedtodo
3)Whyisitimportantformetodothis
You can use these questions to help guide the information you provide during visits with your patients Make sure they know the answer to these questions before they leave your office ConsiderdisplayingpostersandbrochuresthroughoutyourofficeduringOctobertoremindstaffaboutthe3questionsFormoreinformationonAskMe3clickhere
Review your own patient education materials Select a few of the patient education materials that you commonly use in your practice and review them using one of the health literacytoolsfromtheOfficeofDiseasePreventionandHealthPromotionPerhapsformateam to review the pieces together Click hereforresourcesOrcontactusifyouwantacopy of the tool used at Blue Cross
To learn more about building a culture of health literacy and using plain language at your practice please send an email to AlishaOdhiambobluecrossmncomAdditionalinformationcan also be found online at httphealthliteracymnorg
September 2015 6
QuALITY ImproVemeNT
PCC QUALITy OF CARE COMPLAINT REPORTProviders are required to complete the Blue Plus Quality of Care Complaint report forallwrittenandverbalcomplaintsfromBluePlusPrepaidMedicalAssistanceProgram and MinnesotaCare subscribers on a quarterly basis per Minnesota Department of Health regulations Complaints logged at the provider offices are to be investigated and resolved by the providerrsquos office whenever possible
ThesecomplaintsarereportedtoBluePlusinJanuaryAprilJulyandOctoberfor the preceding three months The Primary Care Clinic (PCC) must submit a quarterly report even if the facility does not receive any complaints for the quarter YourcontractoutlinestheproceduresrequiredforyourQualityofCare(QOC)PCCcomplaint reporting adherence agreement
Complaints should no longer be directed to the attention of a single designated personSendingyourPCCQOCcomplaintreportformtoanysourcenotlistedbelowmaydelaytheprocessingofyourPCCQOCcomplaintreport
ToaccessthePCCBluePlusQualityofCareComplaintReportFormgoto providersbluecrossmncom and select ldquoForms amp publicationsrdquo then ldquoforms - clinical operationsrdquo
Submit quarterly PCC QOC reports using one of these methods
Email pcccomplaintbluecrossmncom
Secure fax line (651) 662-4004
Mail Blue Plus AttnQualityHealthManagementDept R472 POBox64179 StPaulMN55164-0179
UTILIzATION MANAGEMENT STATEMENTUtilizationManagement(UM)decisionmakingisbasedonlyonappropriatenessofcareand service and on existing coverage provisions Blue Cross does not compensate providers practitioners or other individuals making UM decisions for denial of coverage or services We do not offer incentives to decision makers to encourage denial of coverage or services that would result in less than appropriate care
September 2015 7
QuALITY ImproVemeNT
CLINICAL PRACTICE GUIDELINES Blue Cross believes that the use of clinical practice guidelines is a key component of Quality Improvement Each year Blue Crossrsquo Clinical Practice Quality Committee (a designee of the Quality Council) approves the adoption of select guidelines that are used to support various programs and initiatives The guidelines do not substitute for sound clinical judgment however they are intended to assist clinicians in understanding key processes for improvement efforts
Clinical Practice Guidelines with hyperlinks are available in Chapter Three of the Blue Cross Provider Policy and Procedure Manual To access the manual go to providersbluecrossmncom and select ldquoForms and Publicationsrdquo then ldquoManualsrdquo
Recommended sources BlueCrossrecognizesthefollowingsourcesforClinicalPracticeGuidelinesfora variety of areas of clinical practice
bullUSPSTFUSPreventiveServicesTaskForce httpwwwuspreventiveservicestaskforceorgbrowseRecIndex
bullAAPAmericanAcademyofPediatricsincludingBrightFutures httppediatricsaappublicationsorgsearchflag=practice_guidelinesampsubmit=yesampx=18ampy=8ampformat=standardamphits=30ampsortspec=dateampsubmit=Gohttppediatricsaappublicationsorgsearchflag=practice_guidelinesampsubmit=yesampx=18ampy=8ampformat=standardamphits=30ampsortspec=dateampsubmit=Go
httpbrightfuturesaaporg
bullICSIInstituteforClinicalSystemsImprovement httpswwwicsiorgguidelines__moreguidelines_a_to_z
Specific guidelines Specific guidelines recommended by Blue Cross include the following
bullBehavioralHealth-ADHD-DiagnosisEvaluationandTreatmentofAttention-DeficitHyperactivityDisorderinChildrenandAdolescents(AAP)-DepressionScreeninginAdults(USPSTF)
bullNon-PreventiveAcuteorChronicConditions-DiabetesndashDiagnosisandManagementofType2DiabetesMellitusinAdults(ICSI)-AsthmandashDiagnosisandManagementofAsthma(ICSI)
bullPreventiveCareGuidelines-PreventiveServicesforAdults(ICSI)-PreventiveServicesChildrenandAdolescents(ICSIandBrightFutures)-RoutinePrenatalCare(ICSI)
Questions concerning Clinical Practice Guidelines can be directed to Eileen Johnson Director Quality and Health Management at (651) 662-4224Acopyoftheclinicalpractice guidelines with hyperlinks is also available by calling Eileen Johnson
September 2015 8
QuALITY ImproVemeNT
bLUE PLUS MEDICAL RECORD DOCUMENTATION REvIEwAdvance Directives
Anadvancedirectiveprovidesanopportunityforadultsofanyagetomaketheirhealthcare wishes known if or when a potential life-threatening event occurs and they are unabletoverbalizetheirwishesatthetimeoftheevent
ArepresentativesamplereviewofourBluePlusmembersrsquomedicalrecordsfordatesofservicein2014hasbeencompletedandtheresultsarebelowWeencourageprovidersto discuss the benefits of completing an advance directive with all our adult members
TOTAL MEMbERS IN SAMPLE
ADvANCE DIRECTIvE PRESENT OR DISCUSSED
AGE RANGE FOR MEMbERS wITH DISCUSSION
MedicareMedicaid Eligible(MSHO)
300 187(62) Avg83Range67-107
Medicaid 600 61(10) Avg48Range20-64
Body Mass Index (BMI) And Counseling For Obesity
Documentation of a memberrsquos BMI is the first step towards addressing the prevalence of obesity in our society Blue Plus completed a review of a sample of Blue Plus membersrsquomedicalrecordswithdatesofservicein2014toevaluatedocumentationofBMIvalueandcounselingforobesityObesityisdefinedasaBMIover30TheresultsareshownbelowOne-thirdofMedicaidmembersdefinedasobesehad documentation of a discussion with their provider concerning their weight management
TOTAL MEMbERS
bMI DOCUMENTED
bMI gt 30 (IF DOCUMENTED)
IF bMI gt 30 ADvISED ON wEIGHT MANAGEMENT
AvERAGE bMI FOR MEMbERS wITH DISCUSSION
MedicareMedicaid Eligible(MSHO)
300 183(61) 70(38) 6(9) Avg3603 Range3089-501
Medicaid 600 550(92) 237(43) 93(39) Avg3807 Range2676-710
Total 900 733(81) 307(42) 99(32) Avg3795
continued on next page
September 2015 9
bLUE PLUS MEDICAL RECORD DOCUMENTATION REvIEw continuedfrompage8
Tobacco Use Assessment And Counseling
AsampleofmedicalrecordswerereviewedtodeterminetobaccouseamongourBlue Plus members and discussions promoting tobacco cessation during a provider visitin2014Whiletobaccouseappearstoberoutinelyassessedatleastonceduring2014onlyhalfofourmembershavedocumentationofprovidereffortsinaddressingthis health concern
TOTAL MEMbERS
ASSESSED FOR TObACCO USE
TObACCO USE AvERAGE AGE OF TObACCO USERS
DISCUSSION ANDOR Rx ASSISTANCE
MSHO 300 281(93) 24(85) Avg75(67-87)
10(42)
PMAPMNCARE 600 518(86) 164(32) Avg44(20-64)
89(54)
Total 900 799(89) 188(24) Avg49 (20-87)
99(53)
These reviews were completed to encourage providers to open the door to meaningful discussions with their patients on important health issues If you have any questions concerning this article please send an email to the Quality and Health Management department co Sheiladalenbluecrossmncom
Better Care Through Quality Improvement
Every year Blue Cross and Blue Shield of Minnesota (Blue Cross) reviews the care delivered to our subscribers This review determines the goals for the quality program The program currently has many goals to improve health services
Making sure our subscribers receive preventive services and health screenings making sure people with health problems like heart disease receive treatment and improving the customer service experience are just a few of the goals in the program
More detailed information is available about Blue Crossrsquo process and outcomes in meeting quality improvement goals related to subscriber care and service You can see more information about our quality improvement program at bluecrossmncom Enter ldquoquality improvement programrdquo in the search field If you are unable to access the website please contact Eileen Johnson Director | AccreditationampQualityImprovementat(651) 662-4224 to request information about the Quality Improvement Program
QuALITY ImproVemeNT
September 2015 10
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
Medical and behavioral health policies are available for your use and review on the Blue Cross and Blue Shield of Minnesota website at providersbluecrossmncom From this site there are two ways to access medical policy information depending on the patientrsquos Blue Plan membership
For out-of-area Blue Plan patients SelectldquoMedicalPolicyPreCertPreAuthRouterrdquoandclickGoYouwillbetakentothepagewhereyouselecteithermedicalpolicyorpre-certificationpriorauthorizationandenterthepatientrsquosthree-letteralphaprefixasfoundontheirmemberidentificationcardandclickGoOnceyouaccepttherequirementsyouwillberoutedtothepatientrsquoshomeplanwhereyoucanaccessmedicalpolicyorpre-certificationpre-authorizationinformation
For local Blue Cross and Blue Shield of Minnesota plan patients SelectldquoMedicalpolicyrdquo(undertheToolsampResources)readandaccepttheBlueCrossMedicalPolicyStatementandthenselectldquoViewAllActivePoliciesrdquoYouhavenownavigatedtotheBlueCrossandBlueShieldofMinnesotaMedicaland Behavioral Health Policy Manual where there are several selections to assist with your inquiry
The ldquoWhatrsquos Newrdquo section identifies our latest new or revised policies approved by Blue Crossrsquo Medical and Behavioral Health Policy Committee at least 50 days ago These policies are now effective and providers should begin following thesepoliciesimmediatelyThesepoliciesalsoappearintheldquoActivePolicyrdquosectionoftheMedicalandBehavioralHealthPolicy Manual
The ldquoUpcoming Policiesrdquo section lists new or revised policies approved by the Blue Cross Medical and Behavioral Health Policy Committee and are effective 50 days from the date they were posted to the ldquoUpcoming Policiesrdquo section of the Medical and Behavioral Health Policy Manual
TheldquoActivePolicyrdquosectioncontainstheentirelistofpolicieseffectiveatthetimeofyourinquiryPleasenoteDHSPrograms(CoverageGuidelinesforDHSPrograms-MHCPManual)andMedicareContractors(PartAndashNationalGovernmentServices[NGS]PartBndashNationalGovernmentServices[NGS]HomeHealthandHospicendashNationalGovernmentServices[NGS]DurableMedicalEquipmentMedicareAdministrativeContractorndashNationalGovernmentServices[NGS]andTheCentersforMedicareandMedicaidServicesndashCMS)haveseparatesections
TheldquoPre-CertificationPre-Authorizationrdquosectionidentifiesvariousservicesproceduresprescriptiondrugsandmedicaldevicesthatrequirepre-certificationpre-authorizationThefollowingPre-CertificationPre-AuthorizationListsareprovidedforreviewCommercial(includingBlueLinkTPA)MNGovernmentProgramsandMedicarePlansTheselistsarenotexclusive to medical policy services only they encompass other services that are subject to pre-certification pre-authorizationrequirements
If you have additional questions regarding medical or behavioral health policy issues call provider services at (651) 662-5200 or 1-800-262-0820 for assistance
September 2015 11
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
MEDICAL AND bEHAvIORAL HEALTH POLICy ACTIvITy
Policies Effective 072015 Notification Posted 052815
Policies developedNone
Policies revisedPneumatic Compression Devices in the Outpatient or Home Setting
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentoflymphedemaintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet 1 The patient has undergone a four-week trial of conservative therapy which includes a Use of an appropriate compression bandage system or compression garment bExerciseAND c Elevation of the limb AND 2 Thetreatingphysiciandeterminesthatnosignificantimprovementhasoccurredorsignificantsymptomsremain
following the four-week trialbull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (non-programmable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps) OR
2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompressiontreatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentofchronicvenousinsufficiencyofthelowerextremitiesintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet
1 The patient has one or more venous stasis ulcers AND 2 ThepatienthasundergoneatrialofconservativetherapyforaminimumofsixmonthswhichincludesALLofthe
following a The use of an appropriate compression bandage system or compression garment bAppropriatedressingsforthewound c Exercise and d Elevation of the limb AND 3 Thetreatingphysiciandeterminesthatthevenousstasisulcerhasfailedtoheal
September 2015 12
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
bull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (nonprogrammable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
OR 2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompression
treatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingmaybeconsideredMEDICALLYNECESSARYinpatientswhohaveundergoneasurgicalprocedurewhenBOTH1and2aremet
1 Patient meets one or more of the following a Major surgery (eg total hip arthroplasty total knee arthroplasty hip fracture repair open abdominal or open
pelvic procedure OR b Patient is at moderate to severe risk of VTE Examples include i Patient is not able to walk unassisted or is bedridden ii Agegreaterthan60yearsanesthesiaatleast2hoursandbedrestatleast4daysduringcurrentepisodeofcare iii Inpatientstayofmorethan2daysduringcurrentepisodeofcare iv Central venous access during current episode of care v Sepsis during current episode of care viActivecancerorcancertreatment vii Significant comorbidity such as recent myocardial infarction congestive heart failure cerebrovascular disease
moderate to severe chronic obstructive pulmonary disease moderate to severe liver disease moderate to severe chronic kidney disease
viiiPregnancy or post-partum state (lt 1 month) ix Hypercoagulable state (eg Factor V Leiden antithrombin III deficiency protein C or S deficiency
antiphospholipidsyndromedysfibrinolysisprothrombin20210defect) x Prior VTE AND 2Thepatienthasacontraindicationtopharmacologicanticoagulantssuchasbeingathigh-riskforbleedingRisk
factors for bleeding include a Bleeding disorder such as hemophilia bActiveliverdisease c Severe renal failure d Previous major bleed (and previous bleeding risk similar to current risk) e Concomitant antiplatelet agent f History of or difficult-to-control surgical bleeding during the current operative procedure extensive surgical
dissection and revision surgery bull Outpatientorhomeuseofpneumaticcompressiondevicesforpost-surgicalVTEprophylaxisisconsideredNOTMEDICALLYNECESSARYforpatientswhohaveundergoneasurgicalprocedurewithalowriskforVTEandwhohaveno additional risk factors for VTE Examples of lower risk surgical procedures include but are not limited to laparoscopic cholecystectomy appendectomy transurethral prostatectomy and inguinal herniorrhaphy
September 2015 13
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingisconsideredINVESTIGATIVEforallotherindications including but not limited to treatment of arterial insufficiency (e g peripheral arterial disease) and restless legs syndrome due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Angioplasty andor Stenting for Intracranial Aneurysms and Atherosclerosis
bull IntracranialstentplacementmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranial aneurysms for patients when surgical treatment is not feasible and standard endovascular techniques do not allowforcompleteisolationoftheaneurysmegwide-neckaneurysm(4mmormore)orsack-to-neckratiolessthan21
bull IntracranialflowdivertingstentswithFDAapprovalforthetreatmentofintracranialaneurysmsmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranialaneurysmsthatarelargeorgiantwide-necked(aneurysmsizeof10mmormoreandaneckdiameterof4mmormore)intheinternalcarotidarteryfrom the petrous to the superior hypophyseal segments and which are not amenable to surgical treatment or standard endovascular therapy
bull IntracranialstentplacementisconsideredINVESTIGATIVEinthetreatmentofintracranialaneurysmsexceptasnotedabove due to the lack of clinical evidence demonstrating its impact on improved health outcomes
bull PercutaneoustransluminalangioplastywithorwithoutstentingisconsideredINVESTIGATIVEforthetreatmentofintracranial atherosclerosis due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Surgical Treatment of Femoroacetabular Impingement
bull OpenorarthroscopictreatmentoffemoroacetabularimpingementmaybeconsideredMEDICALLYNECESSARYwhenALLofthefollowingconditionsaremet
AAge Patientisskeletallymaturewithdocumentedclosureofgrowthplates(eg15yearsorolder) B Symptoms 1 Moderate-to-severe hip pain that is worsened by flexion activities (eg squatting or prolonged sitting) and which
significantlylimitsactivitiesAND 2Painwhichisunresponsiveorrecursafteratrialofconservativetherapylastingatleast3months(including
activitymodificationsrestrictionofathleticpursuitsandavoidanceofsymptomaticmotion)AND 3Positiveimpingementsignispresentonclinicalexamination(painelicitedwith90degreesofflexionandinternal
rotation and adduction of the femur) C Imaging 1Imagingstudies(egx-raysMRI)confirmthediagnosisofacamorpincer-typeFAIExamplesofmorphology
indicativeofFAIinclude a pistol-grip deformity
b femoralhead-neckoffsetwithanalphaanglegreaterthan50degrees c a positive wall sign d acetabular retroversion (overcoverage with crossover sign) e coxa profunda or protrusion f damage of the acetabular rim AND 2Noevidenceofadvancedosteoarthritis(definedasTonnisgradeIIorIIIorjointspaceoflessthan2mm)AND 3Noevidenceofsevere(modifiedOuterbridgegradeIV)chondraldamagebull Surgicaltreatmentoffemoroacetabularimpingement(FAI)isconsideredINVESTIGATIVEinallothersituations
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 14
Policies inactivatedTobacco Cessation Treatments
Policies Effective 081715 Notification Posted 062515
Policies developedNone
Policies revisedTreatment of Obstructive Sleep Apnea and Snoring in Adults bull Medical Management
A IntraoralAppliances Intraoral appliances (eg mandibular advancingpositioning devices or tongue-retaining devices) may be considered
MEDICALLYNECESSARYwhenALLofthefollowingcriteriaaremet 1PatienthasbeendiagnosedwithOSAdefinedby a AnAHIorRDIof15orgreatereventsperhour OR bAnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms i Excessive daytime sleepiness ii Documented hypertension iii Ischemic heart disease iv History of stroke AND 2Thereisabsenceoftemporomandibulardysfunctionorperiodontaldisease AND 3ThedeviceisprescribedafteradiagnosisofOSAhasbeenestablishedbyaphysicianwhoiseitheradiplomate
oftheAmericanBoardofSleepMedicinearecognizedsubspecialtyoftheAmericanBoardofMedicalSpecialties(ABMS)oranactivestaffmemberofasleepcenterorlaboratoryaccreditedbytheAmericanAcademyofSleepMedicine(AASM)orTheJointCommission
AND 4 The device is custom-fitted by qualified dental personnel under the direction of a Doctor of Dental Surgery (DDS)
or Doctor of Dental Medicine (DMD) B ContinuousPositiveAirwayPressure(CPAP) Continuouspositiveairwaypressure(CPAP)maybeconsideredMEDICALLYNECESSARYinpatientswith
confirmedOSAwith 1AnAHIorRDIof15eventsperhourorgreater OR 2AnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms a Excessive daytime sleepiness b Documented hypertension c Ischemic heart disease d History of stroke
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 15
C Bi-levelPositiveAirwayPressure(BiPAP) BiPAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPAND 2HavefailedapriortrialofCPAPOR 3ForwhomBiPAPisfoundtobemoreeffectivethanCPAPinthesleeplaboratory D Auto-AdjustingPAP(APAP) APAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPaboveAND 2HaveacontraindicationtoCPAPhavefailedapriortrialofCPAPORareundergoingatrialofAPAPtotitrate CPAP AND 3Havenoevidencebyhistoryorphysicalexaminationofthefollowingconditions a Central sleep apnea b Congestive heart failure c Chronic pulmonary disease such as chronic obstructive pulmonary disease d Pulmonary hypertension e Obesityhypoventilationsyndromeorotherconditionwhichmaycausenocturnalarterialoxyhemoglobin desaturationbull Surgical Management A Uvulopalatopharyngoplasty(UPPP) UPPPmaybeconsideredMEDICALLYNECESSARYwhenallthefollowingcriteriaaremet 1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a BMI less than 40 AND bAtrialoforalappliancetherapyhasfailedorthepatientisnotacandidateforanoralappliance AND c PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hoursper nightforthree(3)monthsofPAPusage B Maxillofacial Procedures Maxillofacial surgical procedures such as inferior sagittal mandibular osteotomy and genioglossal advancement
withorwithouthyoidmyotomyandsuspensionormandibular-maxillaryadvancement(MMA)maybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a Objectiveevidenceofhypopharyngealobstructiondocumentedbyeitherfiberopticexaminationor cephalometric radiographs AND
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 16
b PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hourspernightforthree(3)monthsofPAPusage
bull Treatment of Snoring TreatmentofsnoringisconsideredNOTMEDICALLYNECESSARYbecausesimplesnoringintheabsenceof
documented obstructive sleep apnea is not considered a medical condition Therefore all procedures for the sole or adjunctivetreatmentofsnoringareconsideredNOTMEDICALLYNECESSARYincludingbutnotlimitedto
A Uvulopalatopharyngoplasty(UPPP) B Uvulectomy C Laser-assisteduvulopalatoplasty(LAUP) D Radiofrequencyvolumetricreductionofthepalataltissues E Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues F Palatal stiffening procedures including but not limited to cautery-assisted palatal stiffening operation and the
implantation of palatal implants G Tongue base suspensionbull Investigative Indications ThefollowingtreatmentsareconsideredINVESTIGATIVEduetoalackofevidencedemonstratingimprovedhealth outcomes AUPPPforanyconditionotherthanobstructivesleepapneaorsnoring B ExpiratoryPositiveAirwayPressure(EPAP)includingtheProventregdevice C OralpressuretherapydevicesincludingbutnotlimitedtotheWinxTMsystem D Atrialpacing EAllothersurgicalproceduresforthesoleoradjunctivetreatmentofobstructivesleepapneaupperairwayresistance
syndrome including but not limited to 1 Uvulectomy 2Laser-assisteduvulopalatoplasty(LAUP) 3Radiofrequencyvolumetricreductionofthepalataltissues 4Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues 5Palatalstiffeningproceduresincludingbutnotlimitedtocautery-assistedpalatalstiffeningoperationandthe
implantation of palatal implants 6 Tongue base suspension 7 Implantable hypoglossal nerve stimulators Respiratory Syncytial Virus (RSV) Prophylaxis bull INITIALRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVfortheinitialRSVseasonmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A ChronicLungDisease(CLD)ofPrematurity 1Infantwasbornatlt32weeks0daysgestationAND 2Infantisle12monthsofageattheonsetofRSVseasonAND 3Infantrequiresgt21oxygenforatleastthefirst28daysafterbirth B Congenital Heart Disease (CHD) 1 Infant is le12monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 17
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
a AcyanoticCHDwhentheinfantisreceivingmedicationtocontrolcongestiveheartfailureandwillrequireacardiacsurgicalprocedureOR
b CyanoticCHDwhenpalivizumabisrecommendedafterconsultationwithapediatriccardiologistOR c Diagnosis of moderate to severe pulmonary hypertension OR 2Childislt24monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing a ChildundergoescardiactransplantationduringtheRSVseasonOR b ChildisreceivingRSVprophylaxisandcontinuestorequireprophylaxisafterasurgicalprocedureinvolving cardiac bypass or at the conclusion of extracorporeal membrane oxygenation C AnatomicPulmonaryAbnormalitiesORNeuromuscularDisorder(egcerebralpalsymusculardystrophy) 1 Infant is le12monthsofageattheonsetofRSVseasonAND 2Infanthasimpairedabilitytoclearsecretionsfromtheupperairway D Cystic Fibrosis 1 Infant is le12monthsofageattheonsetofRSVseasonwithevidenceofCLDandormalnutrition E Immunocompromised Status 1Childislt24monthsofageattheonsetofRSVseasonAND 2Childisprofoundlyimmunocompromised(egduetosolidorgantransplantationhematopoieticstem-cell
transplantation or chemotherapy) F Prematurity without CLD or CHD 1Infantwasbornatlt29weeks0daysgestation(ie28weeks6daysorless)AND 2Infantislt12monthsofageattheonsetofRSVseasonbull SECONDRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVforthepatientrsquossecondyearoftreatmentmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A CLDofPrematurity 1Childwasbornatlt32weeks0daysgestationAND 2Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonAND 3ChildcontinuestorequireatleastONEofthefollowingwithinsix(6)monthsofthestartofthesecondRSV season a SupplementaloxygenOR b ChronicsystemiccorticosteroidtherapyOR c DiuretictherapyOR d Bronchodilator therapy B Cystic Fibrosis 1Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonwithevidenceofCLDandor malnutritionbull AdministrationofRSVProphylaxis A Whentheappropriatecriteriaabovearemetamaximumoffive(5)monthlydosesofpalivizumab(Synagisreg)will
becoveredperRSVseason(definedasNovember1stthroughMarch31st) B Thefirstmonthlydoseofpalivizumab(Synagisreg)willbeapprovedforcoverageofadministrationonorafter
November 1st C Apost-operativedoseofpalivizumab(Synagisreg)willbecoveredforchildrenlt24monthswhoarereceiving
RSVprophylaxisandcontinuetorequireprophylaxisafterasurgicalprocedureinvolvingcardiacbypassorattheconclusion of extracorporeal membrane oxygenation
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 5
HeALTH LITerACY
Try both aleve 2pills bid with flexeril at hs
Asahealthcareprofessionalyouprobablyunderstandexactlywhatthedoctorwhosentthismessage was saying Take 2 Aleve pills 2 times a day and take 1 Flexeril pill at bedtime But the patient who received it had no idea what the doctor was saying Most people donrsquot Clear communication increases patient safety and adherence to treatment plans
OctoberishealthliteracymonthHerearesomeactivitiesthatyourpracticecliniccanincorporate to help make a healthy difference in your patientrsquos lives
Use the Teach Back method also known as the ldquoshow-merdquo technique to ensure that patients (or care takers) understand their treatment plan and what they need to do Think aboutdoingasimpleteachbacktrainingatyourpracticeduringthemonthofOctoberClickhere for a program ready to use from the Minnesota Health Literacy Partnership
Promote the Ask Me 3 program from the National Patient Safety Foundation which focuses onpatientunderstandingof3simplequestions
1)Whatismymainproblem
2)WhatdoIneedtodo
3)Whyisitimportantformetodothis
You can use these questions to help guide the information you provide during visits with your patients Make sure they know the answer to these questions before they leave your office ConsiderdisplayingpostersandbrochuresthroughoutyourofficeduringOctobertoremindstaffaboutthe3questionsFormoreinformationonAskMe3clickhere
Review your own patient education materials Select a few of the patient education materials that you commonly use in your practice and review them using one of the health literacytoolsfromtheOfficeofDiseasePreventionandHealthPromotionPerhapsformateam to review the pieces together Click hereforresourcesOrcontactusifyouwantacopy of the tool used at Blue Cross
To learn more about building a culture of health literacy and using plain language at your practice please send an email to AlishaOdhiambobluecrossmncomAdditionalinformationcan also be found online at httphealthliteracymnorg
September 2015 6
QuALITY ImproVemeNT
PCC QUALITy OF CARE COMPLAINT REPORTProviders are required to complete the Blue Plus Quality of Care Complaint report forallwrittenandverbalcomplaintsfromBluePlusPrepaidMedicalAssistanceProgram and MinnesotaCare subscribers on a quarterly basis per Minnesota Department of Health regulations Complaints logged at the provider offices are to be investigated and resolved by the providerrsquos office whenever possible
ThesecomplaintsarereportedtoBluePlusinJanuaryAprilJulyandOctoberfor the preceding three months The Primary Care Clinic (PCC) must submit a quarterly report even if the facility does not receive any complaints for the quarter YourcontractoutlinestheproceduresrequiredforyourQualityofCare(QOC)PCCcomplaint reporting adherence agreement
Complaints should no longer be directed to the attention of a single designated personSendingyourPCCQOCcomplaintreportformtoanysourcenotlistedbelowmaydelaytheprocessingofyourPCCQOCcomplaintreport
ToaccessthePCCBluePlusQualityofCareComplaintReportFormgoto providersbluecrossmncom and select ldquoForms amp publicationsrdquo then ldquoforms - clinical operationsrdquo
Submit quarterly PCC QOC reports using one of these methods
Email pcccomplaintbluecrossmncom
Secure fax line (651) 662-4004
Mail Blue Plus AttnQualityHealthManagementDept R472 POBox64179 StPaulMN55164-0179
UTILIzATION MANAGEMENT STATEMENTUtilizationManagement(UM)decisionmakingisbasedonlyonappropriatenessofcareand service and on existing coverage provisions Blue Cross does not compensate providers practitioners or other individuals making UM decisions for denial of coverage or services We do not offer incentives to decision makers to encourage denial of coverage or services that would result in less than appropriate care
September 2015 7
QuALITY ImproVemeNT
CLINICAL PRACTICE GUIDELINES Blue Cross believes that the use of clinical practice guidelines is a key component of Quality Improvement Each year Blue Crossrsquo Clinical Practice Quality Committee (a designee of the Quality Council) approves the adoption of select guidelines that are used to support various programs and initiatives The guidelines do not substitute for sound clinical judgment however they are intended to assist clinicians in understanding key processes for improvement efforts
Clinical Practice Guidelines with hyperlinks are available in Chapter Three of the Blue Cross Provider Policy and Procedure Manual To access the manual go to providersbluecrossmncom and select ldquoForms and Publicationsrdquo then ldquoManualsrdquo
Recommended sources BlueCrossrecognizesthefollowingsourcesforClinicalPracticeGuidelinesfora variety of areas of clinical practice
bullUSPSTFUSPreventiveServicesTaskForce httpwwwuspreventiveservicestaskforceorgbrowseRecIndex
bullAAPAmericanAcademyofPediatricsincludingBrightFutures httppediatricsaappublicationsorgsearchflag=practice_guidelinesampsubmit=yesampx=18ampy=8ampformat=standardamphits=30ampsortspec=dateampsubmit=Gohttppediatricsaappublicationsorgsearchflag=practice_guidelinesampsubmit=yesampx=18ampy=8ampformat=standardamphits=30ampsortspec=dateampsubmit=Go
httpbrightfuturesaaporg
bullICSIInstituteforClinicalSystemsImprovement httpswwwicsiorgguidelines__moreguidelines_a_to_z
Specific guidelines Specific guidelines recommended by Blue Cross include the following
bullBehavioralHealth-ADHD-DiagnosisEvaluationandTreatmentofAttention-DeficitHyperactivityDisorderinChildrenandAdolescents(AAP)-DepressionScreeninginAdults(USPSTF)
bullNon-PreventiveAcuteorChronicConditions-DiabetesndashDiagnosisandManagementofType2DiabetesMellitusinAdults(ICSI)-AsthmandashDiagnosisandManagementofAsthma(ICSI)
bullPreventiveCareGuidelines-PreventiveServicesforAdults(ICSI)-PreventiveServicesChildrenandAdolescents(ICSIandBrightFutures)-RoutinePrenatalCare(ICSI)
Questions concerning Clinical Practice Guidelines can be directed to Eileen Johnson Director Quality and Health Management at (651) 662-4224Acopyoftheclinicalpractice guidelines with hyperlinks is also available by calling Eileen Johnson
September 2015 8
QuALITY ImproVemeNT
bLUE PLUS MEDICAL RECORD DOCUMENTATION REvIEwAdvance Directives
Anadvancedirectiveprovidesanopportunityforadultsofanyagetomaketheirhealthcare wishes known if or when a potential life-threatening event occurs and they are unabletoverbalizetheirwishesatthetimeoftheevent
ArepresentativesamplereviewofourBluePlusmembersrsquomedicalrecordsfordatesofservicein2014hasbeencompletedandtheresultsarebelowWeencourageprovidersto discuss the benefits of completing an advance directive with all our adult members
TOTAL MEMbERS IN SAMPLE
ADvANCE DIRECTIvE PRESENT OR DISCUSSED
AGE RANGE FOR MEMbERS wITH DISCUSSION
MedicareMedicaid Eligible(MSHO)
300 187(62) Avg83Range67-107
Medicaid 600 61(10) Avg48Range20-64
Body Mass Index (BMI) And Counseling For Obesity
Documentation of a memberrsquos BMI is the first step towards addressing the prevalence of obesity in our society Blue Plus completed a review of a sample of Blue Plus membersrsquomedicalrecordswithdatesofservicein2014toevaluatedocumentationofBMIvalueandcounselingforobesityObesityisdefinedasaBMIover30TheresultsareshownbelowOne-thirdofMedicaidmembersdefinedasobesehad documentation of a discussion with their provider concerning their weight management
TOTAL MEMbERS
bMI DOCUMENTED
bMI gt 30 (IF DOCUMENTED)
IF bMI gt 30 ADvISED ON wEIGHT MANAGEMENT
AvERAGE bMI FOR MEMbERS wITH DISCUSSION
MedicareMedicaid Eligible(MSHO)
300 183(61) 70(38) 6(9) Avg3603 Range3089-501
Medicaid 600 550(92) 237(43) 93(39) Avg3807 Range2676-710
Total 900 733(81) 307(42) 99(32) Avg3795
continued on next page
September 2015 9
bLUE PLUS MEDICAL RECORD DOCUMENTATION REvIEw continuedfrompage8
Tobacco Use Assessment And Counseling
AsampleofmedicalrecordswerereviewedtodeterminetobaccouseamongourBlue Plus members and discussions promoting tobacco cessation during a provider visitin2014Whiletobaccouseappearstoberoutinelyassessedatleastonceduring2014onlyhalfofourmembershavedocumentationofprovidereffortsinaddressingthis health concern
TOTAL MEMbERS
ASSESSED FOR TObACCO USE
TObACCO USE AvERAGE AGE OF TObACCO USERS
DISCUSSION ANDOR Rx ASSISTANCE
MSHO 300 281(93) 24(85) Avg75(67-87)
10(42)
PMAPMNCARE 600 518(86) 164(32) Avg44(20-64)
89(54)
Total 900 799(89) 188(24) Avg49 (20-87)
99(53)
These reviews were completed to encourage providers to open the door to meaningful discussions with their patients on important health issues If you have any questions concerning this article please send an email to the Quality and Health Management department co Sheiladalenbluecrossmncom
Better Care Through Quality Improvement
Every year Blue Cross and Blue Shield of Minnesota (Blue Cross) reviews the care delivered to our subscribers This review determines the goals for the quality program The program currently has many goals to improve health services
Making sure our subscribers receive preventive services and health screenings making sure people with health problems like heart disease receive treatment and improving the customer service experience are just a few of the goals in the program
More detailed information is available about Blue Crossrsquo process and outcomes in meeting quality improvement goals related to subscriber care and service You can see more information about our quality improvement program at bluecrossmncom Enter ldquoquality improvement programrdquo in the search field If you are unable to access the website please contact Eileen Johnson Director | AccreditationampQualityImprovementat(651) 662-4224 to request information about the Quality Improvement Program
QuALITY ImproVemeNT
September 2015 10
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
Medical and behavioral health policies are available for your use and review on the Blue Cross and Blue Shield of Minnesota website at providersbluecrossmncom From this site there are two ways to access medical policy information depending on the patientrsquos Blue Plan membership
For out-of-area Blue Plan patients SelectldquoMedicalPolicyPreCertPreAuthRouterrdquoandclickGoYouwillbetakentothepagewhereyouselecteithermedicalpolicyorpre-certificationpriorauthorizationandenterthepatientrsquosthree-letteralphaprefixasfoundontheirmemberidentificationcardandclickGoOnceyouaccepttherequirementsyouwillberoutedtothepatientrsquoshomeplanwhereyoucanaccessmedicalpolicyorpre-certificationpre-authorizationinformation
For local Blue Cross and Blue Shield of Minnesota plan patients SelectldquoMedicalpolicyrdquo(undertheToolsampResources)readandaccepttheBlueCrossMedicalPolicyStatementandthenselectldquoViewAllActivePoliciesrdquoYouhavenownavigatedtotheBlueCrossandBlueShieldofMinnesotaMedicaland Behavioral Health Policy Manual where there are several selections to assist with your inquiry
The ldquoWhatrsquos Newrdquo section identifies our latest new or revised policies approved by Blue Crossrsquo Medical and Behavioral Health Policy Committee at least 50 days ago These policies are now effective and providers should begin following thesepoliciesimmediatelyThesepoliciesalsoappearintheldquoActivePolicyrdquosectionoftheMedicalandBehavioralHealthPolicy Manual
The ldquoUpcoming Policiesrdquo section lists new or revised policies approved by the Blue Cross Medical and Behavioral Health Policy Committee and are effective 50 days from the date they were posted to the ldquoUpcoming Policiesrdquo section of the Medical and Behavioral Health Policy Manual
TheldquoActivePolicyrdquosectioncontainstheentirelistofpolicieseffectiveatthetimeofyourinquiryPleasenoteDHSPrograms(CoverageGuidelinesforDHSPrograms-MHCPManual)andMedicareContractors(PartAndashNationalGovernmentServices[NGS]PartBndashNationalGovernmentServices[NGS]HomeHealthandHospicendashNationalGovernmentServices[NGS]DurableMedicalEquipmentMedicareAdministrativeContractorndashNationalGovernmentServices[NGS]andTheCentersforMedicareandMedicaidServicesndashCMS)haveseparatesections
TheldquoPre-CertificationPre-Authorizationrdquosectionidentifiesvariousservicesproceduresprescriptiondrugsandmedicaldevicesthatrequirepre-certificationpre-authorizationThefollowingPre-CertificationPre-AuthorizationListsareprovidedforreviewCommercial(includingBlueLinkTPA)MNGovernmentProgramsandMedicarePlansTheselistsarenotexclusive to medical policy services only they encompass other services that are subject to pre-certification pre-authorizationrequirements
If you have additional questions regarding medical or behavioral health policy issues call provider services at (651) 662-5200 or 1-800-262-0820 for assistance
September 2015 11
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
MEDICAL AND bEHAvIORAL HEALTH POLICy ACTIvITy
Policies Effective 072015 Notification Posted 052815
Policies developedNone
Policies revisedPneumatic Compression Devices in the Outpatient or Home Setting
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentoflymphedemaintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet 1 The patient has undergone a four-week trial of conservative therapy which includes a Use of an appropriate compression bandage system or compression garment bExerciseAND c Elevation of the limb AND 2 Thetreatingphysiciandeterminesthatnosignificantimprovementhasoccurredorsignificantsymptomsremain
following the four-week trialbull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (non-programmable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps) OR
2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompressiontreatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentofchronicvenousinsufficiencyofthelowerextremitiesintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet
1 The patient has one or more venous stasis ulcers AND 2 ThepatienthasundergoneatrialofconservativetherapyforaminimumofsixmonthswhichincludesALLofthe
following a The use of an appropriate compression bandage system or compression garment bAppropriatedressingsforthewound c Exercise and d Elevation of the limb AND 3 Thetreatingphysiciandeterminesthatthevenousstasisulcerhasfailedtoheal
September 2015 12
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
bull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (nonprogrammable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
OR 2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompression
treatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingmaybeconsideredMEDICALLYNECESSARYinpatientswhohaveundergoneasurgicalprocedurewhenBOTH1and2aremet
1 Patient meets one or more of the following a Major surgery (eg total hip arthroplasty total knee arthroplasty hip fracture repair open abdominal or open
pelvic procedure OR b Patient is at moderate to severe risk of VTE Examples include i Patient is not able to walk unassisted or is bedridden ii Agegreaterthan60yearsanesthesiaatleast2hoursandbedrestatleast4daysduringcurrentepisodeofcare iii Inpatientstayofmorethan2daysduringcurrentepisodeofcare iv Central venous access during current episode of care v Sepsis during current episode of care viActivecancerorcancertreatment vii Significant comorbidity such as recent myocardial infarction congestive heart failure cerebrovascular disease
moderate to severe chronic obstructive pulmonary disease moderate to severe liver disease moderate to severe chronic kidney disease
viiiPregnancy or post-partum state (lt 1 month) ix Hypercoagulable state (eg Factor V Leiden antithrombin III deficiency protein C or S deficiency
antiphospholipidsyndromedysfibrinolysisprothrombin20210defect) x Prior VTE AND 2Thepatienthasacontraindicationtopharmacologicanticoagulantssuchasbeingathigh-riskforbleedingRisk
factors for bleeding include a Bleeding disorder such as hemophilia bActiveliverdisease c Severe renal failure d Previous major bleed (and previous bleeding risk similar to current risk) e Concomitant antiplatelet agent f History of or difficult-to-control surgical bleeding during the current operative procedure extensive surgical
dissection and revision surgery bull Outpatientorhomeuseofpneumaticcompressiondevicesforpost-surgicalVTEprophylaxisisconsideredNOTMEDICALLYNECESSARYforpatientswhohaveundergoneasurgicalprocedurewithalowriskforVTEandwhohaveno additional risk factors for VTE Examples of lower risk surgical procedures include but are not limited to laparoscopic cholecystectomy appendectomy transurethral prostatectomy and inguinal herniorrhaphy
September 2015 13
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingisconsideredINVESTIGATIVEforallotherindications including but not limited to treatment of arterial insufficiency (e g peripheral arterial disease) and restless legs syndrome due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Angioplasty andor Stenting for Intracranial Aneurysms and Atherosclerosis
bull IntracranialstentplacementmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranial aneurysms for patients when surgical treatment is not feasible and standard endovascular techniques do not allowforcompleteisolationoftheaneurysmegwide-neckaneurysm(4mmormore)orsack-to-neckratiolessthan21
bull IntracranialflowdivertingstentswithFDAapprovalforthetreatmentofintracranialaneurysmsmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranialaneurysmsthatarelargeorgiantwide-necked(aneurysmsizeof10mmormoreandaneckdiameterof4mmormore)intheinternalcarotidarteryfrom the petrous to the superior hypophyseal segments and which are not amenable to surgical treatment or standard endovascular therapy
bull IntracranialstentplacementisconsideredINVESTIGATIVEinthetreatmentofintracranialaneurysmsexceptasnotedabove due to the lack of clinical evidence demonstrating its impact on improved health outcomes
bull PercutaneoustransluminalangioplastywithorwithoutstentingisconsideredINVESTIGATIVEforthetreatmentofintracranial atherosclerosis due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Surgical Treatment of Femoroacetabular Impingement
bull OpenorarthroscopictreatmentoffemoroacetabularimpingementmaybeconsideredMEDICALLYNECESSARYwhenALLofthefollowingconditionsaremet
AAge Patientisskeletallymaturewithdocumentedclosureofgrowthplates(eg15yearsorolder) B Symptoms 1 Moderate-to-severe hip pain that is worsened by flexion activities (eg squatting or prolonged sitting) and which
significantlylimitsactivitiesAND 2Painwhichisunresponsiveorrecursafteratrialofconservativetherapylastingatleast3months(including
activitymodificationsrestrictionofathleticpursuitsandavoidanceofsymptomaticmotion)AND 3Positiveimpingementsignispresentonclinicalexamination(painelicitedwith90degreesofflexionandinternal
rotation and adduction of the femur) C Imaging 1Imagingstudies(egx-raysMRI)confirmthediagnosisofacamorpincer-typeFAIExamplesofmorphology
indicativeofFAIinclude a pistol-grip deformity
b femoralhead-neckoffsetwithanalphaanglegreaterthan50degrees c a positive wall sign d acetabular retroversion (overcoverage with crossover sign) e coxa profunda or protrusion f damage of the acetabular rim AND 2Noevidenceofadvancedosteoarthritis(definedasTonnisgradeIIorIIIorjointspaceoflessthan2mm)AND 3Noevidenceofsevere(modifiedOuterbridgegradeIV)chondraldamagebull Surgicaltreatmentoffemoroacetabularimpingement(FAI)isconsideredINVESTIGATIVEinallothersituations
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 14
Policies inactivatedTobacco Cessation Treatments
Policies Effective 081715 Notification Posted 062515
Policies developedNone
Policies revisedTreatment of Obstructive Sleep Apnea and Snoring in Adults bull Medical Management
A IntraoralAppliances Intraoral appliances (eg mandibular advancingpositioning devices or tongue-retaining devices) may be considered
MEDICALLYNECESSARYwhenALLofthefollowingcriteriaaremet 1PatienthasbeendiagnosedwithOSAdefinedby a AnAHIorRDIof15orgreatereventsperhour OR bAnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms i Excessive daytime sleepiness ii Documented hypertension iii Ischemic heart disease iv History of stroke AND 2Thereisabsenceoftemporomandibulardysfunctionorperiodontaldisease AND 3ThedeviceisprescribedafteradiagnosisofOSAhasbeenestablishedbyaphysicianwhoiseitheradiplomate
oftheAmericanBoardofSleepMedicinearecognizedsubspecialtyoftheAmericanBoardofMedicalSpecialties(ABMS)oranactivestaffmemberofasleepcenterorlaboratoryaccreditedbytheAmericanAcademyofSleepMedicine(AASM)orTheJointCommission
AND 4 The device is custom-fitted by qualified dental personnel under the direction of a Doctor of Dental Surgery (DDS)
or Doctor of Dental Medicine (DMD) B ContinuousPositiveAirwayPressure(CPAP) Continuouspositiveairwaypressure(CPAP)maybeconsideredMEDICALLYNECESSARYinpatientswith
confirmedOSAwith 1AnAHIorRDIof15eventsperhourorgreater OR 2AnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms a Excessive daytime sleepiness b Documented hypertension c Ischemic heart disease d History of stroke
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 15
C Bi-levelPositiveAirwayPressure(BiPAP) BiPAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPAND 2HavefailedapriortrialofCPAPOR 3ForwhomBiPAPisfoundtobemoreeffectivethanCPAPinthesleeplaboratory D Auto-AdjustingPAP(APAP) APAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPaboveAND 2HaveacontraindicationtoCPAPhavefailedapriortrialofCPAPORareundergoingatrialofAPAPtotitrate CPAP AND 3Havenoevidencebyhistoryorphysicalexaminationofthefollowingconditions a Central sleep apnea b Congestive heart failure c Chronic pulmonary disease such as chronic obstructive pulmonary disease d Pulmonary hypertension e Obesityhypoventilationsyndromeorotherconditionwhichmaycausenocturnalarterialoxyhemoglobin desaturationbull Surgical Management A Uvulopalatopharyngoplasty(UPPP) UPPPmaybeconsideredMEDICALLYNECESSARYwhenallthefollowingcriteriaaremet 1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a BMI less than 40 AND bAtrialoforalappliancetherapyhasfailedorthepatientisnotacandidateforanoralappliance AND c PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hoursper nightforthree(3)monthsofPAPusage B Maxillofacial Procedures Maxillofacial surgical procedures such as inferior sagittal mandibular osteotomy and genioglossal advancement
withorwithouthyoidmyotomyandsuspensionormandibular-maxillaryadvancement(MMA)maybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a Objectiveevidenceofhypopharyngealobstructiondocumentedbyeitherfiberopticexaminationor cephalometric radiographs AND
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 16
b PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hourspernightforthree(3)monthsofPAPusage
bull Treatment of Snoring TreatmentofsnoringisconsideredNOTMEDICALLYNECESSARYbecausesimplesnoringintheabsenceof
documented obstructive sleep apnea is not considered a medical condition Therefore all procedures for the sole or adjunctivetreatmentofsnoringareconsideredNOTMEDICALLYNECESSARYincludingbutnotlimitedto
A Uvulopalatopharyngoplasty(UPPP) B Uvulectomy C Laser-assisteduvulopalatoplasty(LAUP) D Radiofrequencyvolumetricreductionofthepalataltissues E Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues F Palatal stiffening procedures including but not limited to cautery-assisted palatal stiffening operation and the
implantation of palatal implants G Tongue base suspensionbull Investigative Indications ThefollowingtreatmentsareconsideredINVESTIGATIVEduetoalackofevidencedemonstratingimprovedhealth outcomes AUPPPforanyconditionotherthanobstructivesleepapneaorsnoring B ExpiratoryPositiveAirwayPressure(EPAP)includingtheProventregdevice C OralpressuretherapydevicesincludingbutnotlimitedtotheWinxTMsystem D Atrialpacing EAllothersurgicalproceduresforthesoleoradjunctivetreatmentofobstructivesleepapneaupperairwayresistance
syndrome including but not limited to 1 Uvulectomy 2Laser-assisteduvulopalatoplasty(LAUP) 3Radiofrequencyvolumetricreductionofthepalataltissues 4Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues 5Palatalstiffeningproceduresincludingbutnotlimitedtocautery-assistedpalatalstiffeningoperationandthe
implantation of palatal implants 6 Tongue base suspension 7 Implantable hypoglossal nerve stimulators Respiratory Syncytial Virus (RSV) Prophylaxis bull INITIALRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVfortheinitialRSVseasonmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A ChronicLungDisease(CLD)ofPrematurity 1Infantwasbornatlt32weeks0daysgestationAND 2Infantisle12monthsofageattheonsetofRSVseasonAND 3Infantrequiresgt21oxygenforatleastthefirst28daysafterbirth B Congenital Heart Disease (CHD) 1 Infant is le12monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 17
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
a AcyanoticCHDwhentheinfantisreceivingmedicationtocontrolcongestiveheartfailureandwillrequireacardiacsurgicalprocedureOR
b CyanoticCHDwhenpalivizumabisrecommendedafterconsultationwithapediatriccardiologistOR c Diagnosis of moderate to severe pulmonary hypertension OR 2Childislt24monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing a ChildundergoescardiactransplantationduringtheRSVseasonOR b ChildisreceivingRSVprophylaxisandcontinuestorequireprophylaxisafterasurgicalprocedureinvolving cardiac bypass or at the conclusion of extracorporeal membrane oxygenation C AnatomicPulmonaryAbnormalitiesORNeuromuscularDisorder(egcerebralpalsymusculardystrophy) 1 Infant is le12monthsofageattheonsetofRSVseasonAND 2Infanthasimpairedabilitytoclearsecretionsfromtheupperairway D Cystic Fibrosis 1 Infant is le12monthsofageattheonsetofRSVseasonwithevidenceofCLDandormalnutrition E Immunocompromised Status 1Childislt24monthsofageattheonsetofRSVseasonAND 2Childisprofoundlyimmunocompromised(egduetosolidorgantransplantationhematopoieticstem-cell
transplantation or chemotherapy) F Prematurity without CLD or CHD 1Infantwasbornatlt29weeks0daysgestation(ie28weeks6daysorless)AND 2Infantislt12monthsofageattheonsetofRSVseasonbull SECONDRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVforthepatientrsquossecondyearoftreatmentmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A CLDofPrematurity 1Childwasbornatlt32weeks0daysgestationAND 2Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonAND 3ChildcontinuestorequireatleastONEofthefollowingwithinsix(6)monthsofthestartofthesecondRSV season a SupplementaloxygenOR b ChronicsystemiccorticosteroidtherapyOR c DiuretictherapyOR d Bronchodilator therapy B Cystic Fibrosis 1Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonwithevidenceofCLDandor malnutritionbull AdministrationofRSVProphylaxis A Whentheappropriatecriteriaabovearemetamaximumoffive(5)monthlydosesofpalivizumab(Synagisreg)will
becoveredperRSVseason(definedasNovember1stthroughMarch31st) B Thefirstmonthlydoseofpalivizumab(Synagisreg)willbeapprovedforcoverageofadministrationonorafter
November 1st C Apost-operativedoseofpalivizumab(Synagisreg)willbecoveredforchildrenlt24monthswhoarereceiving
RSVprophylaxisandcontinuetorequireprophylaxisafterasurgicalprocedureinvolvingcardiacbypassorattheconclusion of extracorporeal membrane oxygenation
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 6
QuALITY ImproVemeNT
PCC QUALITy OF CARE COMPLAINT REPORTProviders are required to complete the Blue Plus Quality of Care Complaint report forallwrittenandverbalcomplaintsfromBluePlusPrepaidMedicalAssistanceProgram and MinnesotaCare subscribers on a quarterly basis per Minnesota Department of Health regulations Complaints logged at the provider offices are to be investigated and resolved by the providerrsquos office whenever possible
ThesecomplaintsarereportedtoBluePlusinJanuaryAprilJulyandOctoberfor the preceding three months The Primary Care Clinic (PCC) must submit a quarterly report even if the facility does not receive any complaints for the quarter YourcontractoutlinestheproceduresrequiredforyourQualityofCare(QOC)PCCcomplaint reporting adherence agreement
Complaints should no longer be directed to the attention of a single designated personSendingyourPCCQOCcomplaintreportformtoanysourcenotlistedbelowmaydelaytheprocessingofyourPCCQOCcomplaintreport
ToaccessthePCCBluePlusQualityofCareComplaintReportFormgoto providersbluecrossmncom and select ldquoForms amp publicationsrdquo then ldquoforms - clinical operationsrdquo
Submit quarterly PCC QOC reports using one of these methods
Email pcccomplaintbluecrossmncom
Secure fax line (651) 662-4004
Mail Blue Plus AttnQualityHealthManagementDept R472 POBox64179 StPaulMN55164-0179
UTILIzATION MANAGEMENT STATEMENTUtilizationManagement(UM)decisionmakingisbasedonlyonappropriatenessofcareand service and on existing coverage provisions Blue Cross does not compensate providers practitioners or other individuals making UM decisions for denial of coverage or services We do not offer incentives to decision makers to encourage denial of coverage or services that would result in less than appropriate care
September 2015 7
QuALITY ImproVemeNT
CLINICAL PRACTICE GUIDELINES Blue Cross believes that the use of clinical practice guidelines is a key component of Quality Improvement Each year Blue Crossrsquo Clinical Practice Quality Committee (a designee of the Quality Council) approves the adoption of select guidelines that are used to support various programs and initiatives The guidelines do not substitute for sound clinical judgment however they are intended to assist clinicians in understanding key processes for improvement efforts
Clinical Practice Guidelines with hyperlinks are available in Chapter Three of the Blue Cross Provider Policy and Procedure Manual To access the manual go to providersbluecrossmncom and select ldquoForms and Publicationsrdquo then ldquoManualsrdquo
Recommended sources BlueCrossrecognizesthefollowingsourcesforClinicalPracticeGuidelinesfora variety of areas of clinical practice
bullUSPSTFUSPreventiveServicesTaskForce httpwwwuspreventiveservicestaskforceorgbrowseRecIndex
bullAAPAmericanAcademyofPediatricsincludingBrightFutures httppediatricsaappublicationsorgsearchflag=practice_guidelinesampsubmit=yesampx=18ampy=8ampformat=standardamphits=30ampsortspec=dateampsubmit=Gohttppediatricsaappublicationsorgsearchflag=practice_guidelinesampsubmit=yesampx=18ampy=8ampformat=standardamphits=30ampsortspec=dateampsubmit=Go
httpbrightfuturesaaporg
bullICSIInstituteforClinicalSystemsImprovement httpswwwicsiorgguidelines__moreguidelines_a_to_z
Specific guidelines Specific guidelines recommended by Blue Cross include the following
bullBehavioralHealth-ADHD-DiagnosisEvaluationandTreatmentofAttention-DeficitHyperactivityDisorderinChildrenandAdolescents(AAP)-DepressionScreeninginAdults(USPSTF)
bullNon-PreventiveAcuteorChronicConditions-DiabetesndashDiagnosisandManagementofType2DiabetesMellitusinAdults(ICSI)-AsthmandashDiagnosisandManagementofAsthma(ICSI)
bullPreventiveCareGuidelines-PreventiveServicesforAdults(ICSI)-PreventiveServicesChildrenandAdolescents(ICSIandBrightFutures)-RoutinePrenatalCare(ICSI)
Questions concerning Clinical Practice Guidelines can be directed to Eileen Johnson Director Quality and Health Management at (651) 662-4224Acopyoftheclinicalpractice guidelines with hyperlinks is also available by calling Eileen Johnson
September 2015 8
QuALITY ImproVemeNT
bLUE PLUS MEDICAL RECORD DOCUMENTATION REvIEwAdvance Directives
Anadvancedirectiveprovidesanopportunityforadultsofanyagetomaketheirhealthcare wishes known if or when a potential life-threatening event occurs and they are unabletoverbalizetheirwishesatthetimeoftheevent
ArepresentativesamplereviewofourBluePlusmembersrsquomedicalrecordsfordatesofservicein2014hasbeencompletedandtheresultsarebelowWeencourageprovidersto discuss the benefits of completing an advance directive with all our adult members
TOTAL MEMbERS IN SAMPLE
ADvANCE DIRECTIvE PRESENT OR DISCUSSED
AGE RANGE FOR MEMbERS wITH DISCUSSION
MedicareMedicaid Eligible(MSHO)
300 187(62) Avg83Range67-107
Medicaid 600 61(10) Avg48Range20-64
Body Mass Index (BMI) And Counseling For Obesity
Documentation of a memberrsquos BMI is the first step towards addressing the prevalence of obesity in our society Blue Plus completed a review of a sample of Blue Plus membersrsquomedicalrecordswithdatesofservicein2014toevaluatedocumentationofBMIvalueandcounselingforobesityObesityisdefinedasaBMIover30TheresultsareshownbelowOne-thirdofMedicaidmembersdefinedasobesehad documentation of a discussion with their provider concerning their weight management
TOTAL MEMbERS
bMI DOCUMENTED
bMI gt 30 (IF DOCUMENTED)
IF bMI gt 30 ADvISED ON wEIGHT MANAGEMENT
AvERAGE bMI FOR MEMbERS wITH DISCUSSION
MedicareMedicaid Eligible(MSHO)
300 183(61) 70(38) 6(9) Avg3603 Range3089-501
Medicaid 600 550(92) 237(43) 93(39) Avg3807 Range2676-710
Total 900 733(81) 307(42) 99(32) Avg3795
continued on next page
September 2015 9
bLUE PLUS MEDICAL RECORD DOCUMENTATION REvIEw continuedfrompage8
Tobacco Use Assessment And Counseling
AsampleofmedicalrecordswerereviewedtodeterminetobaccouseamongourBlue Plus members and discussions promoting tobacco cessation during a provider visitin2014Whiletobaccouseappearstoberoutinelyassessedatleastonceduring2014onlyhalfofourmembershavedocumentationofprovidereffortsinaddressingthis health concern
TOTAL MEMbERS
ASSESSED FOR TObACCO USE
TObACCO USE AvERAGE AGE OF TObACCO USERS
DISCUSSION ANDOR Rx ASSISTANCE
MSHO 300 281(93) 24(85) Avg75(67-87)
10(42)
PMAPMNCARE 600 518(86) 164(32) Avg44(20-64)
89(54)
Total 900 799(89) 188(24) Avg49 (20-87)
99(53)
These reviews were completed to encourage providers to open the door to meaningful discussions with their patients on important health issues If you have any questions concerning this article please send an email to the Quality and Health Management department co Sheiladalenbluecrossmncom
Better Care Through Quality Improvement
Every year Blue Cross and Blue Shield of Minnesota (Blue Cross) reviews the care delivered to our subscribers This review determines the goals for the quality program The program currently has many goals to improve health services
Making sure our subscribers receive preventive services and health screenings making sure people with health problems like heart disease receive treatment and improving the customer service experience are just a few of the goals in the program
More detailed information is available about Blue Crossrsquo process and outcomes in meeting quality improvement goals related to subscriber care and service You can see more information about our quality improvement program at bluecrossmncom Enter ldquoquality improvement programrdquo in the search field If you are unable to access the website please contact Eileen Johnson Director | AccreditationampQualityImprovementat(651) 662-4224 to request information about the Quality Improvement Program
QuALITY ImproVemeNT
September 2015 10
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
Medical and behavioral health policies are available for your use and review on the Blue Cross and Blue Shield of Minnesota website at providersbluecrossmncom From this site there are two ways to access medical policy information depending on the patientrsquos Blue Plan membership
For out-of-area Blue Plan patients SelectldquoMedicalPolicyPreCertPreAuthRouterrdquoandclickGoYouwillbetakentothepagewhereyouselecteithermedicalpolicyorpre-certificationpriorauthorizationandenterthepatientrsquosthree-letteralphaprefixasfoundontheirmemberidentificationcardandclickGoOnceyouaccepttherequirementsyouwillberoutedtothepatientrsquoshomeplanwhereyoucanaccessmedicalpolicyorpre-certificationpre-authorizationinformation
For local Blue Cross and Blue Shield of Minnesota plan patients SelectldquoMedicalpolicyrdquo(undertheToolsampResources)readandaccepttheBlueCrossMedicalPolicyStatementandthenselectldquoViewAllActivePoliciesrdquoYouhavenownavigatedtotheBlueCrossandBlueShieldofMinnesotaMedicaland Behavioral Health Policy Manual where there are several selections to assist with your inquiry
The ldquoWhatrsquos Newrdquo section identifies our latest new or revised policies approved by Blue Crossrsquo Medical and Behavioral Health Policy Committee at least 50 days ago These policies are now effective and providers should begin following thesepoliciesimmediatelyThesepoliciesalsoappearintheldquoActivePolicyrdquosectionoftheMedicalandBehavioralHealthPolicy Manual
The ldquoUpcoming Policiesrdquo section lists new or revised policies approved by the Blue Cross Medical and Behavioral Health Policy Committee and are effective 50 days from the date they were posted to the ldquoUpcoming Policiesrdquo section of the Medical and Behavioral Health Policy Manual
TheldquoActivePolicyrdquosectioncontainstheentirelistofpolicieseffectiveatthetimeofyourinquiryPleasenoteDHSPrograms(CoverageGuidelinesforDHSPrograms-MHCPManual)andMedicareContractors(PartAndashNationalGovernmentServices[NGS]PartBndashNationalGovernmentServices[NGS]HomeHealthandHospicendashNationalGovernmentServices[NGS]DurableMedicalEquipmentMedicareAdministrativeContractorndashNationalGovernmentServices[NGS]andTheCentersforMedicareandMedicaidServicesndashCMS)haveseparatesections
TheldquoPre-CertificationPre-Authorizationrdquosectionidentifiesvariousservicesproceduresprescriptiondrugsandmedicaldevicesthatrequirepre-certificationpre-authorizationThefollowingPre-CertificationPre-AuthorizationListsareprovidedforreviewCommercial(includingBlueLinkTPA)MNGovernmentProgramsandMedicarePlansTheselistsarenotexclusive to medical policy services only they encompass other services that are subject to pre-certification pre-authorizationrequirements
If you have additional questions regarding medical or behavioral health policy issues call provider services at (651) 662-5200 or 1-800-262-0820 for assistance
September 2015 11
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
MEDICAL AND bEHAvIORAL HEALTH POLICy ACTIvITy
Policies Effective 072015 Notification Posted 052815
Policies developedNone
Policies revisedPneumatic Compression Devices in the Outpatient or Home Setting
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentoflymphedemaintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet 1 The patient has undergone a four-week trial of conservative therapy which includes a Use of an appropriate compression bandage system or compression garment bExerciseAND c Elevation of the limb AND 2 Thetreatingphysiciandeterminesthatnosignificantimprovementhasoccurredorsignificantsymptomsremain
following the four-week trialbull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (non-programmable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps) OR
2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompressiontreatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentofchronicvenousinsufficiencyofthelowerextremitiesintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet
1 The patient has one or more venous stasis ulcers AND 2 ThepatienthasundergoneatrialofconservativetherapyforaminimumofsixmonthswhichincludesALLofthe
following a The use of an appropriate compression bandage system or compression garment bAppropriatedressingsforthewound c Exercise and d Elevation of the limb AND 3 Thetreatingphysiciandeterminesthatthevenousstasisulcerhasfailedtoheal
September 2015 12
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
bull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (nonprogrammable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
OR 2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompression
treatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingmaybeconsideredMEDICALLYNECESSARYinpatientswhohaveundergoneasurgicalprocedurewhenBOTH1and2aremet
1 Patient meets one or more of the following a Major surgery (eg total hip arthroplasty total knee arthroplasty hip fracture repair open abdominal or open
pelvic procedure OR b Patient is at moderate to severe risk of VTE Examples include i Patient is not able to walk unassisted or is bedridden ii Agegreaterthan60yearsanesthesiaatleast2hoursandbedrestatleast4daysduringcurrentepisodeofcare iii Inpatientstayofmorethan2daysduringcurrentepisodeofcare iv Central venous access during current episode of care v Sepsis during current episode of care viActivecancerorcancertreatment vii Significant comorbidity such as recent myocardial infarction congestive heart failure cerebrovascular disease
moderate to severe chronic obstructive pulmonary disease moderate to severe liver disease moderate to severe chronic kidney disease
viiiPregnancy or post-partum state (lt 1 month) ix Hypercoagulable state (eg Factor V Leiden antithrombin III deficiency protein C or S deficiency
antiphospholipidsyndromedysfibrinolysisprothrombin20210defect) x Prior VTE AND 2Thepatienthasacontraindicationtopharmacologicanticoagulantssuchasbeingathigh-riskforbleedingRisk
factors for bleeding include a Bleeding disorder such as hemophilia bActiveliverdisease c Severe renal failure d Previous major bleed (and previous bleeding risk similar to current risk) e Concomitant antiplatelet agent f History of or difficult-to-control surgical bleeding during the current operative procedure extensive surgical
dissection and revision surgery bull Outpatientorhomeuseofpneumaticcompressiondevicesforpost-surgicalVTEprophylaxisisconsideredNOTMEDICALLYNECESSARYforpatientswhohaveundergoneasurgicalprocedurewithalowriskforVTEandwhohaveno additional risk factors for VTE Examples of lower risk surgical procedures include but are not limited to laparoscopic cholecystectomy appendectomy transurethral prostatectomy and inguinal herniorrhaphy
September 2015 13
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingisconsideredINVESTIGATIVEforallotherindications including but not limited to treatment of arterial insufficiency (e g peripheral arterial disease) and restless legs syndrome due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Angioplasty andor Stenting for Intracranial Aneurysms and Atherosclerosis
bull IntracranialstentplacementmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranial aneurysms for patients when surgical treatment is not feasible and standard endovascular techniques do not allowforcompleteisolationoftheaneurysmegwide-neckaneurysm(4mmormore)orsack-to-neckratiolessthan21
bull IntracranialflowdivertingstentswithFDAapprovalforthetreatmentofintracranialaneurysmsmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranialaneurysmsthatarelargeorgiantwide-necked(aneurysmsizeof10mmormoreandaneckdiameterof4mmormore)intheinternalcarotidarteryfrom the petrous to the superior hypophyseal segments and which are not amenable to surgical treatment or standard endovascular therapy
bull IntracranialstentplacementisconsideredINVESTIGATIVEinthetreatmentofintracranialaneurysmsexceptasnotedabove due to the lack of clinical evidence demonstrating its impact on improved health outcomes
bull PercutaneoustransluminalangioplastywithorwithoutstentingisconsideredINVESTIGATIVEforthetreatmentofintracranial atherosclerosis due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Surgical Treatment of Femoroacetabular Impingement
bull OpenorarthroscopictreatmentoffemoroacetabularimpingementmaybeconsideredMEDICALLYNECESSARYwhenALLofthefollowingconditionsaremet
AAge Patientisskeletallymaturewithdocumentedclosureofgrowthplates(eg15yearsorolder) B Symptoms 1 Moderate-to-severe hip pain that is worsened by flexion activities (eg squatting or prolonged sitting) and which
significantlylimitsactivitiesAND 2Painwhichisunresponsiveorrecursafteratrialofconservativetherapylastingatleast3months(including
activitymodificationsrestrictionofathleticpursuitsandavoidanceofsymptomaticmotion)AND 3Positiveimpingementsignispresentonclinicalexamination(painelicitedwith90degreesofflexionandinternal
rotation and adduction of the femur) C Imaging 1Imagingstudies(egx-raysMRI)confirmthediagnosisofacamorpincer-typeFAIExamplesofmorphology
indicativeofFAIinclude a pistol-grip deformity
b femoralhead-neckoffsetwithanalphaanglegreaterthan50degrees c a positive wall sign d acetabular retroversion (overcoverage with crossover sign) e coxa profunda or protrusion f damage of the acetabular rim AND 2Noevidenceofadvancedosteoarthritis(definedasTonnisgradeIIorIIIorjointspaceoflessthan2mm)AND 3Noevidenceofsevere(modifiedOuterbridgegradeIV)chondraldamagebull Surgicaltreatmentoffemoroacetabularimpingement(FAI)isconsideredINVESTIGATIVEinallothersituations
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 14
Policies inactivatedTobacco Cessation Treatments
Policies Effective 081715 Notification Posted 062515
Policies developedNone
Policies revisedTreatment of Obstructive Sleep Apnea and Snoring in Adults bull Medical Management
A IntraoralAppliances Intraoral appliances (eg mandibular advancingpositioning devices or tongue-retaining devices) may be considered
MEDICALLYNECESSARYwhenALLofthefollowingcriteriaaremet 1PatienthasbeendiagnosedwithOSAdefinedby a AnAHIorRDIof15orgreatereventsperhour OR bAnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms i Excessive daytime sleepiness ii Documented hypertension iii Ischemic heart disease iv History of stroke AND 2Thereisabsenceoftemporomandibulardysfunctionorperiodontaldisease AND 3ThedeviceisprescribedafteradiagnosisofOSAhasbeenestablishedbyaphysicianwhoiseitheradiplomate
oftheAmericanBoardofSleepMedicinearecognizedsubspecialtyoftheAmericanBoardofMedicalSpecialties(ABMS)oranactivestaffmemberofasleepcenterorlaboratoryaccreditedbytheAmericanAcademyofSleepMedicine(AASM)orTheJointCommission
AND 4 The device is custom-fitted by qualified dental personnel under the direction of a Doctor of Dental Surgery (DDS)
or Doctor of Dental Medicine (DMD) B ContinuousPositiveAirwayPressure(CPAP) Continuouspositiveairwaypressure(CPAP)maybeconsideredMEDICALLYNECESSARYinpatientswith
confirmedOSAwith 1AnAHIorRDIof15eventsperhourorgreater OR 2AnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms a Excessive daytime sleepiness b Documented hypertension c Ischemic heart disease d History of stroke
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 15
C Bi-levelPositiveAirwayPressure(BiPAP) BiPAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPAND 2HavefailedapriortrialofCPAPOR 3ForwhomBiPAPisfoundtobemoreeffectivethanCPAPinthesleeplaboratory D Auto-AdjustingPAP(APAP) APAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPaboveAND 2HaveacontraindicationtoCPAPhavefailedapriortrialofCPAPORareundergoingatrialofAPAPtotitrate CPAP AND 3Havenoevidencebyhistoryorphysicalexaminationofthefollowingconditions a Central sleep apnea b Congestive heart failure c Chronic pulmonary disease such as chronic obstructive pulmonary disease d Pulmonary hypertension e Obesityhypoventilationsyndromeorotherconditionwhichmaycausenocturnalarterialoxyhemoglobin desaturationbull Surgical Management A Uvulopalatopharyngoplasty(UPPP) UPPPmaybeconsideredMEDICALLYNECESSARYwhenallthefollowingcriteriaaremet 1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a BMI less than 40 AND bAtrialoforalappliancetherapyhasfailedorthepatientisnotacandidateforanoralappliance AND c PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hoursper nightforthree(3)monthsofPAPusage B Maxillofacial Procedures Maxillofacial surgical procedures such as inferior sagittal mandibular osteotomy and genioglossal advancement
withorwithouthyoidmyotomyandsuspensionormandibular-maxillaryadvancement(MMA)maybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a Objectiveevidenceofhypopharyngealobstructiondocumentedbyeitherfiberopticexaminationor cephalometric radiographs AND
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 16
b PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hourspernightforthree(3)monthsofPAPusage
bull Treatment of Snoring TreatmentofsnoringisconsideredNOTMEDICALLYNECESSARYbecausesimplesnoringintheabsenceof
documented obstructive sleep apnea is not considered a medical condition Therefore all procedures for the sole or adjunctivetreatmentofsnoringareconsideredNOTMEDICALLYNECESSARYincludingbutnotlimitedto
A Uvulopalatopharyngoplasty(UPPP) B Uvulectomy C Laser-assisteduvulopalatoplasty(LAUP) D Radiofrequencyvolumetricreductionofthepalataltissues E Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues F Palatal stiffening procedures including but not limited to cautery-assisted palatal stiffening operation and the
implantation of palatal implants G Tongue base suspensionbull Investigative Indications ThefollowingtreatmentsareconsideredINVESTIGATIVEduetoalackofevidencedemonstratingimprovedhealth outcomes AUPPPforanyconditionotherthanobstructivesleepapneaorsnoring B ExpiratoryPositiveAirwayPressure(EPAP)includingtheProventregdevice C OralpressuretherapydevicesincludingbutnotlimitedtotheWinxTMsystem D Atrialpacing EAllothersurgicalproceduresforthesoleoradjunctivetreatmentofobstructivesleepapneaupperairwayresistance
syndrome including but not limited to 1 Uvulectomy 2Laser-assisteduvulopalatoplasty(LAUP) 3Radiofrequencyvolumetricreductionofthepalataltissues 4Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues 5Palatalstiffeningproceduresincludingbutnotlimitedtocautery-assistedpalatalstiffeningoperationandthe
implantation of palatal implants 6 Tongue base suspension 7 Implantable hypoglossal nerve stimulators Respiratory Syncytial Virus (RSV) Prophylaxis bull INITIALRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVfortheinitialRSVseasonmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A ChronicLungDisease(CLD)ofPrematurity 1Infantwasbornatlt32weeks0daysgestationAND 2Infantisle12monthsofageattheonsetofRSVseasonAND 3Infantrequiresgt21oxygenforatleastthefirst28daysafterbirth B Congenital Heart Disease (CHD) 1 Infant is le12monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 17
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
a AcyanoticCHDwhentheinfantisreceivingmedicationtocontrolcongestiveheartfailureandwillrequireacardiacsurgicalprocedureOR
b CyanoticCHDwhenpalivizumabisrecommendedafterconsultationwithapediatriccardiologistOR c Diagnosis of moderate to severe pulmonary hypertension OR 2Childislt24monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing a ChildundergoescardiactransplantationduringtheRSVseasonOR b ChildisreceivingRSVprophylaxisandcontinuestorequireprophylaxisafterasurgicalprocedureinvolving cardiac bypass or at the conclusion of extracorporeal membrane oxygenation C AnatomicPulmonaryAbnormalitiesORNeuromuscularDisorder(egcerebralpalsymusculardystrophy) 1 Infant is le12monthsofageattheonsetofRSVseasonAND 2Infanthasimpairedabilitytoclearsecretionsfromtheupperairway D Cystic Fibrosis 1 Infant is le12monthsofageattheonsetofRSVseasonwithevidenceofCLDandormalnutrition E Immunocompromised Status 1Childislt24monthsofageattheonsetofRSVseasonAND 2Childisprofoundlyimmunocompromised(egduetosolidorgantransplantationhematopoieticstem-cell
transplantation or chemotherapy) F Prematurity without CLD or CHD 1Infantwasbornatlt29weeks0daysgestation(ie28weeks6daysorless)AND 2Infantislt12monthsofageattheonsetofRSVseasonbull SECONDRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVforthepatientrsquossecondyearoftreatmentmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A CLDofPrematurity 1Childwasbornatlt32weeks0daysgestationAND 2Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonAND 3ChildcontinuestorequireatleastONEofthefollowingwithinsix(6)monthsofthestartofthesecondRSV season a SupplementaloxygenOR b ChronicsystemiccorticosteroidtherapyOR c DiuretictherapyOR d Bronchodilator therapy B Cystic Fibrosis 1Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonwithevidenceofCLDandor malnutritionbull AdministrationofRSVProphylaxis A Whentheappropriatecriteriaabovearemetamaximumoffive(5)monthlydosesofpalivizumab(Synagisreg)will
becoveredperRSVseason(definedasNovember1stthroughMarch31st) B Thefirstmonthlydoseofpalivizumab(Synagisreg)willbeapprovedforcoverageofadministrationonorafter
November 1st C Apost-operativedoseofpalivizumab(Synagisreg)willbecoveredforchildrenlt24monthswhoarereceiving
RSVprophylaxisandcontinuetorequireprophylaxisafterasurgicalprocedureinvolvingcardiacbypassorattheconclusion of extracorporeal membrane oxygenation
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 7
QuALITY ImproVemeNT
CLINICAL PRACTICE GUIDELINES Blue Cross believes that the use of clinical practice guidelines is a key component of Quality Improvement Each year Blue Crossrsquo Clinical Practice Quality Committee (a designee of the Quality Council) approves the adoption of select guidelines that are used to support various programs and initiatives The guidelines do not substitute for sound clinical judgment however they are intended to assist clinicians in understanding key processes for improvement efforts
Clinical Practice Guidelines with hyperlinks are available in Chapter Three of the Blue Cross Provider Policy and Procedure Manual To access the manual go to providersbluecrossmncom and select ldquoForms and Publicationsrdquo then ldquoManualsrdquo
Recommended sources BlueCrossrecognizesthefollowingsourcesforClinicalPracticeGuidelinesfora variety of areas of clinical practice
bullUSPSTFUSPreventiveServicesTaskForce httpwwwuspreventiveservicestaskforceorgbrowseRecIndex
bullAAPAmericanAcademyofPediatricsincludingBrightFutures httppediatricsaappublicationsorgsearchflag=practice_guidelinesampsubmit=yesampx=18ampy=8ampformat=standardamphits=30ampsortspec=dateampsubmit=Gohttppediatricsaappublicationsorgsearchflag=practice_guidelinesampsubmit=yesampx=18ampy=8ampformat=standardamphits=30ampsortspec=dateampsubmit=Go
httpbrightfuturesaaporg
bullICSIInstituteforClinicalSystemsImprovement httpswwwicsiorgguidelines__moreguidelines_a_to_z
Specific guidelines Specific guidelines recommended by Blue Cross include the following
bullBehavioralHealth-ADHD-DiagnosisEvaluationandTreatmentofAttention-DeficitHyperactivityDisorderinChildrenandAdolescents(AAP)-DepressionScreeninginAdults(USPSTF)
bullNon-PreventiveAcuteorChronicConditions-DiabetesndashDiagnosisandManagementofType2DiabetesMellitusinAdults(ICSI)-AsthmandashDiagnosisandManagementofAsthma(ICSI)
bullPreventiveCareGuidelines-PreventiveServicesforAdults(ICSI)-PreventiveServicesChildrenandAdolescents(ICSIandBrightFutures)-RoutinePrenatalCare(ICSI)
Questions concerning Clinical Practice Guidelines can be directed to Eileen Johnson Director Quality and Health Management at (651) 662-4224Acopyoftheclinicalpractice guidelines with hyperlinks is also available by calling Eileen Johnson
September 2015 8
QuALITY ImproVemeNT
bLUE PLUS MEDICAL RECORD DOCUMENTATION REvIEwAdvance Directives
Anadvancedirectiveprovidesanopportunityforadultsofanyagetomaketheirhealthcare wishes known if or when a potential life-threatening event occurs and they are unabletoverbalizetheirwishesatthetimeoftheevent
ArepresentativesamplereviewofourBluePlusmembersrsquomedicalrecordsfordatesofservicein2014hasbeencompletedandtheresultsarebelowWeencourageprovidersto discuss the benefits of completing an advance directive with all our adult members
TOTAL MEMbERS IN SAMPLE
ADvANCE DIRECTIvE PRESENT OR DISCUSSED
AGE RANGE FOR MEMbERS wITH DISCUSSION
MedicareMedicaid Eligible(MSHO)
300 187(62) Avg83Range67-107
Medicaid 600 61(10) Avg48Range20-64
Body Mass Index (BMI) And Counseling For Obesity
Documentation of a memberrsquos BMI is the first step towards addressing the prevalence of obesity in our society Blue Plus completed a review of a sample of Blue Plus membersrsquomedicalrecordswithdatesofservicein2014toevaluatedocumentationofBMIvalueandcounselingforobesityObesityisdefinedasaBMIover30TheresultsareshownbelowOne-thirdofMedicaidmembersdefinedasobesehad documentation of a discussion with their provider concerning their weight management
TOTAL MEMbERS
bMI DOCUMENTED
bMI gt 30 (IF DOCUMENTED)
IF bMI gt 30 ADvISED ON wEIGHT MANAGEMENT
AvERAGE bMI FOR MEMbERS wITH DISCUSSION
MedicareMedicaid Eligible(MSHO)
300 183(61) 70(38) 6(9) Avg3603 Range3089-501
Medicaid 600 550(92) 237(43) 93(39) Avg3807 Range2676-710
Total 900 733(81) 307(42) 99(32) Avg3795
continued on next page
September 2015 9
bLUE PLUS MEDICAL RECORD DOCUMENTATION REvIEw continuedfrompage8
Tobacco Use Assessment And Counseling
AsampleofmedicalrecordswerereviewedtodeterminetobaccouseamongourBlue Plus members and discussions promoting tobacco cessation during a provider visitin2014Whiletobaccouseappearstoberoutinelyassessedatleastonceduring2014onlyhalfofourmembershavedocumentationofprovidereffortsinaddressingthis health concern
TOTAL MEMbERS
ASSESSED FOR TObACCO USE
TObACCO USE AvERAGE AGE OF TObACCO USERS
DISCUSSION ANDOR Rx ASSISTANCE
MSHO 300 281(93) 24(85) Avg75(67-87)
10(42)
PMAPMNCARE 600 518(86) 164(32) Avg44(20-64)
89(54)
Total 900 799(89) 188(24) Avg49 (20-87)
99(53)
These reviews were completed to encourage providers to open the door to meaningful discussions with their patients on important health issues If you have any questions concerning this article please send an email to the Quality and Health Management department co Sheiladalenbluecrossmncom
Better Care Through Quality Improvement
Every year Blue Cross and Blue Shield of Minnesota (Blue Cross) reviews the care delivered to our subscribers This review determines the goals for the quality program The program currently has many goals to improve health services
Making sure our subscribers receive preventive services and health screenings making sure people with health problems like heart disease receive treatment and improving the customer service experience are just a few of the goals in the program
More detailed information is available about Blue Crossrsquo process and outcomes in meeting quality improvement goals related to subscriber care and service You can see more information about our quality improvement program at bluecrossmncom Enter ldquoquality improvement programrdquo in the search field If you are unable to access the website please contact Eileen Johnson Director | AccreditationampQualityImprovementat(651) 662-4224 to request information about the Quality Improvement Program
QuALITY ImproVemeNT
September 2015 10
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
Medical and behavioral health policies are available for your use and review on the Blue Cross and Blue Shield of Minnesota website at providersbluecrossmncom From this site there are two ways to access medical policy information depending on the patientrsquos Blue Plan membership
For out-of-area Blue Plan patients SelectldquoMedicalPolicyPreCertPreAuthRouterrdquoandclickGoYouwillbetakentothepagewhereyouselecteithermedicalpolicyorpre-certificationpriorauthorizationandenterthepatientrsquosthree-letteralphaprefixasfoundontheirmemberidentificationcardandclickGoOnceyouaccepttherequirementsyouwillberoutedtothepatientrsquoshomeplanwhereyoucanaccessmedicalpolicyorpre-certificationpre-authorizationinformation
For local Blue Cross and Blue Shield of Minnesota plan patients SelectldquoMedicalpolicyrdquo(undertheToolsampResources)readandaccepttheBlueCrossMedicalPolicyStatementandthenselectldquoViewAllActivePoliciesrdquoYouhavenownavigatedtotheBlueCrossandBlueShieldofMinnesotaMedicaland Behavioral Health Policy Manual where there are several selections to assist with your inquiry
The ldquoWhatrsquos Newrdquo section identifies our latest new or revised policies approved by Blue Crossrsquo Medical and Behavioral Health Policy Committee at least 50 days ago These policies are now effective and providers should begin following thesepoliciesimmediatelyThesepoliciesalsoappearintheldquoActivePolicyrdquosectionoftheMedicalandBehavioralHealthPolicy Manual
The ldquoUpcoming Policiesrdquo section lists new or revised policies approved by the Blue Cross Medical and Behavioral Health Policy Committee and are effective 50 days from the date they were posted to the ldquoUpcoming Policiesrdquo section of the Medical and Behavioral Health Policy Manual
TheldquoActivePolicyrdquosectioncontainstheentirelistofpolicieseffectiveatthetimeofyourinquiryPleasenoteDHSPrograms(CoverageGuidelinesforDHSPrograms-MHCPManual)andMedicareContractors(PartAndashNationalGovernmentServices[NGS]PartBndashNationalGovernmentServices[NGS]HomeHealthandHospicendashNationalGovernmentServices[NGS]DurableMedicalEquipmentMedicareAdministrativeContractorndashNationalGovernmentServices[NGS]andTheCentersforMedicareandMedicaidServicesndashCMS)haveseparatesections
TheldquoPre-CertificationPre-Authorizationrdquosectionidentifiesvariousservicesproceduresprescriptiondrugsandmedicaldevicesthatrequirepre-certificationpre-authorizationThefollowingPre-CertificationPre-AuthorizationListsareprovidedforreviewCommercial(includingBlueLinkTPA)MNGovernmentProgramsandMedicarePlansTheselistsarenotexclusive to medical policy services only they encompass other services that are subject to pre-certification pre-authorizationrequirements
If you have additional questions regarding medical or behavioral health policy issues call provider services at (651) 662-5200 or 1-800-262-0820 for assistance
September 2015 11
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
MEDICAL AND bEHAvIORAL HEALTH POLICy ACTIvITy
Policies Effective 072015 Notification Posted 052815
Policies developedNone
Policies revisedPneumatic Compression Devices in the Outpatient or Home Setting
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentoflymphedemaintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet 1 The patient has undergone a four-week trial of conservative therapy which includes a Use of an appropriate compression bandage system or compression garment bExerciseAND c Elevation of the limb AND 2 Thetreatingphysiciandeterminesthatnosignificantimprovementhasoccurredorsignificantsymptomsremain
following the four-week trialbull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (non-programmable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps) OR
2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompressiontreatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentofchronicvenousinsufficiencyofthelowerextremitiesintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet
1 The patient has one or more venous stasis ulcers AND 2 ThepatienthasundergoneatrialofconservativetherapyforaminimumofsixmonthswhichincludesALLofthe
following a The use of an appropriate compression bandage system or compression garment bAppropriatedressingsforthewound c Exercise and d Elevation of the limb AND 3 Thetreatingphysiciandeterminesthatthevenousstasisulcerhasfailedtoheal
September 2015 12
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
bull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (nonprogrammable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
OR 2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompression
treatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingmaybeconsideredMEDICALLYNECESSARYinpatientswhohaveundergoneasurgicalprocedurewhenBOTH1and2aremet
1 Patient meets one or more of the following a Major surgery (eg total hip arthroplasty total knee arthroplasty hip fracture repair open abdominal or open
pelvic procedure OR b Patient is at moderate to severe risk of VTE Examples include i Patient is not able to walk unassisted or is bedridden ii Agegreaterthan60yearsanesthesiaatleast2hoursandbedrestatleast4daysduringcurrentepisodeofcare iii Inpatientstayofmorethan2daysduringcurrentepisodeofcare iv Central venous access during current episode of care v Sepsis during current episode of care viActivecancerorcancertreatment vii Significant comorbidity such as recent myocardial infarction congestive heart failure cerebrovascular disease
moderate to severe chronic obstructive pulmonary disease moderate to severe liver disease moderate to severe chronic kidney disease
viiiPregnancy or post-partum state (lt 1 month) ix Hypercoagulable state (eg Factor V Leiden antithrombin III deficiency protein C or S deficiency
antiphospholipidsyndromedysfibrinolysisprothrombin20210defect) x Prior VTE AND 2Thepatienthasacontraindicationtopharmacologicanticoagulantssuchasbeingathigh-riskforbleedingRisk
factors for bleeding include a Bleeding disorder such as hemophilia bActiveliverdisease c Severe renal failure d Previous major bleed (and previous bleeding risk similar to current risk) e Concomitant antiplatelet agent f History of or difficult-to-control surgical bleeding during the current operative procedure extensive surgical
dissection and revision surgery bull Outpatientorhomeuseofpneumaticcompressiondevicesforpost-surgicalVTEprophylaxisisconsideredNOTMEDICALLYNECESSARYforpatientswhohaveundergoneasurgicalprocedurewithalowriskforVTEandwhohaveno additional risk factors for VTE Examples of lower risk surgical procedures include but are not limited to laparoscopic cholecystectomy appendectomy transurethral prostatectomy and inguinal herniorrhaphy
September 2015 13
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingisconsideredINVESTIGATIVEforallotherindications including but not limited to treatment of arterial insufficiency (e g peripheral arterial disease) and restless legs syndrome due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Angioplasty andor Stenting for Intracranial Aneurysms and Atherosclerosis
bull IntracranialstentplacementmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranial aneurysms for patients when surgical treatment is not feasible and standard endovascular techniques do not allowforcompleteisolationoftheaneurysmegwide-neckaneurysm(4mmormore)orsack-to-neckratiolessthan21
bull IntracranialflowdivertingstentswithFDAapprovalforthetreatmentofintracranialaneurysmsmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranialaneurysmsthatarelargeorgiantwide-necked(aneurysmsizeof10mmormoreandaneckdiameterof4mmormore)intheinternalcarotidarteryfrom the petrous to the superior hypophyseal segments and which are not amenable to surgical treatment or standard endovascular therapy
bull IntracranialstentplacementisconsideredINVESTIGATIVEinthetreatmentofintracranialaneurysmsexceptasnotedabove due to the lack of clinical evidence demonstrating its impact on improved health outcomes
bull PercutaneoustransluminalangioplastywithorwithoutstentingisconsideredINVESTIGATIVEforthetreatmentofintracranial atherosclerosis due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Surgical Treatment of Femoroacetabular Impingement
bull OpenorarthroscopictreatmentoffemoroacetabularimpingementmaybeconsideredMEDICALLYNECESSARYwhenALLofthefollowingconditionsaremet
AAge Patientisskeletallymaturewithdocumentedclosureofgrowthplates(eg15yearsorolder) B Symptoms 1 Moderate-to-severe hip pain that is worsened by flexion activities (eg squatting or prolonged sitting) and which
significantlylimitsactivitiesAND 2Painwhichisunresponsiveorrecursafteratrialofconservativetherapylastingatleast3months(including
activitymodificationsrestrictionofathleticpursuitsandavoidanceofsymptomaticmotion)AND 3Positiveimpingementsignispresentonclinicalexamination(painelicitedwith90degreesofflexionandinternal
rotation and adduction of the femur) C Imaging 1Imagingstudies(egx-raysMRI)confirmthediagnosisofacamorpincer-typeFAIExamplesofmorphology
indicativeofFAIinclude a pistol-grip deformity
b femoralhead-neckoffsetwithanalphaanglegreaterthan50degrees c a positive wall sign d acetabular retroversion (overcoverage with crossover sign) e coxa profunda or protrusion f damage of the acetabular rim AND 2Noevidenceofadvancedosteoarthritis(definedasTonnisgradeIIorIIIorjointspaceoflessthan2mm)AND 3Noevidenceofsevere(modifiedOuterbridgegradeIV)chondraldamagebull Surgicaltreatmentoffemoroacetabularimpingement(FAI)isconsideredINVESTIGATIVEinallothersituations
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 14
Policies inactivatedTobacco Cessation Treatments
Policies Effective 081715 Notification Posted 062515
Policies developedNone
Policies revisedTreatment of Obstructive Sleep Apnea and Snoring in Adults bull Medical Management
A IntraoralAppliances Intraoral appliances (eg mandibular advancingpositioning devices or tongue-retaining devices) may be considered
MEDICALLYNECESSARYwhenALLofthefollowingcriteriaaremet 1PatienthasbeendiagnosedwithOSAdefinedby a AnAHIorRDIof15orgreatereventsperhour OR bAnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms i Excessive daytime sleepiness ii Documented hypertension iii Ischemic heart disease iv History of stroke AND 2Thereisabsenceoftemporomandibulardysfunctionorperiodontaldisease AND 3ThedeviceisprescribedafteradiagnosisofOSAhasbeenestablishedbyaphysicianwhoiseitheradiplomate
oftheAmericanBoardofSleepMedicinearecognizedsubspecialtyoftheAmericanBoardofMedicalSpecialties(ABMS)oranactivestaffmemberofasleepcenterorlaboratoryaccreditedbytheAmericanAcademyofSleepMedicine(AASM)orTheJointCommission
AND 4 The device is custom-fitted by qualified dental personnel under the direction of a Doctor of Dental Surgery (DDS)
or Doctor of Dental Medicine (DMD) B ContinuousPositiveAirwayPressure(CPAP) Continuouspositiveairwaypressure(CPAP)maybeconsideredMEDICALLYNECESSARYinpatientswith
confirmedOSAwith 1AnAHIorRDIof15eventsperhourorgreater OR 2AnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms a Excessive daytime sleepiness b Documented hypertension c Ischemic heart disease d History of stroke
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 15
C Bi-levelPositiveAirwayPressure(BiPAP) BiPAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPAND 2HavefailedapriortrialofCPAPOR 3ForwhomBiPAPisfoundtobemoreeffectivethanCPAPinthesleeplaboratory D Auto-AdjustingPAP(APAP) APAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPaboveAND 2HaveacontraindicationtoCPAPhavefailedapriortrialofCPAPORareundergoingatrialofAPAPtotitrate CPAP AND 3Havenoevidencebyhistoryorphysicalexaminationofthefollowingconditions a Central sleep apnea b Congestive heart failure c Chronic pulmonary disease such as chronic obstructive pulmonary disease d Pulmonary hypertension e Obesityhypoventilationsyndromeorotherconditionwhichmaycausenocturnalarterialoxyhemoglobin desaturationbull Surgical Management A Uvulopalatopharyngoplasty(UPPP) UPPPmaybeconsideredMEDICALLYNECESSARYwhenallthefollowingcriteriaaremet 1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a BMI less than 40 AND bAtrialoforalappliancetherapyhasfailedorthepatientisnotacandidateforanoralappliance AND c PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hoursper nightforthree(3)monthsofPAPusage B Maxillofacial Procedures Maxillofacial surgical procedures such as inferior sagittal mandibular osteotomy and genioglossal advancement
withorwithouthyoidmyotomyandsuspensionormandibular-maxillaryadvancement(MMA)maybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a Objectiveevidenceofhypopharyngealobstructiondocumentedbyeitherfiberopticexaminationor cephalometric radiographs AND
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 16
b PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hourspernightforthree(3)monthsofPAPusage
bull Treatment of Snoring TreatmentofsnoringisconsideredNOTMEDICALLYNECESSARYbecausesimplesnoringintheabsenceof
documented obstructive sleep apnea is not considered a medical condition Therefore all procedures for the sole or adjunctivetreatmentofsnoringareconsideredNOTMEDICALLYNECESSARYincludingbutnotlimitedto
A Uvulopalatopharyngoplasty(UPPP) B Uvulectomy C Laser-assisteduvulopalatoplasty(LAUP) D Radiofrequencyvolumetricreductionofthepalataltissues E Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues F Palatal stiffening procedures including but not limited to cautery-assisted palatal stiffening operation and the
implantation of palatal implants G Tongue base suspensionbull Investigative Indications ThefollowingtreatmentsareconsideredINVESTIGATIVEduetoalackofevidencedemonstratingimprovedhealth outcomes AUPPPforanyconditionotherthanobstructivesleepapneaorsnoring B ExpiratoryPositiveAirwayPressure(EPAP)includingtheProventregdevice C OralpressuretherapydevicesincludingbutnotlimitedtotheWinxTMsystem D Atrialpacing EAllothersurgicalproceduresforthesoleoradjunctivetreatmentofobstructivesleepapneaupperairwayresistance
syndrome including but not limited to 1 Uvulectomy 2Laser-assisteduvulopalatoplasty(LAUP) 3Radiofrequencyvolumetricreductionofthepalataltissues 4Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues 5Palatalstiffeningproceduresincludingbutnotlimitedtocautery-assistedpalatalstiffeningoperationandthe
implantation of palatal implants 6 Tongue base suspension 7 Implantable hypoglossal nerve stimulators Respiratory Syncytial Virus (RSV) Prophylaxis bull INITIALRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVfortheinitialRSVseasonmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A ChronicLungDisease(CLD)ofPrematurity 1Infantwasbornatlt32weeks0daysgestationAND 2Infantisle12monthsofageattheonsetofRSVseasonAND 3Infantrequiresgt21oxygenforatleastthefirst28daysafterbirth B Congenital Heart Disease (CHD) 1 Infant is le12monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 17
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
a AcyanoticCHDwhentheinfantisreceivingmedicationtocontrolcongestiveheartfailureandwillrequireacardiacsurgicalprocedureOR
b CyanoticCHDwhenpalivizumabisrecommendedafterconsultationwithapediatriccardiologistOR c Diagnosis of moderate to severe pulmonary hypertension OR 2Childislt24monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing a ChildundergoescardiactransplantationduringtheRSVseasonOR b ChildisreceivingRSVprophylaxisandcontinuestorequireprophylaxisafterasurgicalprocedureinvolving cardiac bypass or at the conclusion of extracorporeal membrane oxygenation C AnatomicPulmonaryAbnormalitiesORNeuromuscularDisorder(egcerebralpalsymusculardystrophy) 1 Infant is le12monthsofageattheonsetofRSVseasonAND 2Infanthasimpairedabilitytoclearsecretionsfromtheupperairway D Cystic Fibrosis 1 Infant is le12monthsofageattheonsetofRSVseasonwithevidenceofCLDandormalnutrition E Immunocompromised Status 1Childislt24monthsofageattheonsetofRSVseasonAND 2Childisprofoundlyimmunocompromised(egduetosolidorgantransplantationhematopoieticstem-cell
transplantation or chemotherapy) F Prematurity without CLD or CHD 1Infantwasbornatlt29weeks0daysgestation(ie28weeks6daysorless)AND 2Infantislt12monthsofageattheonsetofRSVseasonbull SECONDRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVforthepatientrsquossecondyearoftreatmentmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A CLDofPrematurity 1Childwasbornatlt32weeks0daysgestationAND 2Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonAND 3ChildcontinuestorequireatleastONEofthefollowingwithinsix(6)monthsofthestartofthesecondRSV season a SupplementaloxygenOR b ChronicsystemiccorticosteroidtherapyOR c DiuretictherapyOR d Bronchodilator therapy B Cystic Fibrosis 1Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonwithevidenceofCLDandor malnutritionbull AdministrationofRSVProphylaxis A Whentheappropriatecriteriaabovearemetamaximumoffive(5)monthlydosesofpalivizumab(Synagisreg)will
becoveredperRSVseason(definedasNovember1stthroughMarch31st) B Thefirstmonthlydoseofpalivizumab(Synagisreg)willbeapprovedforcoverageofadministrationonorafter
November 1st C Apost-operativedoseofpalivizumab(Synagisreg)willbecoveredforchildrenlt24monthswhoarereceiving
RSVprophylaxisandcontinuetorequireprophylaxisafterasurgicalprocedureinvolvingcardiacbypassorattheconclusion of extracorporeal membrane oxygenation
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 8
QuALITY ImproVemeNT
bLUE PLUS MEDICAL RECORD DOCUMENTATION REvIEwAdvance Directives
Anadvancedirectiveprovidesanopportunityforadultsofanyagetomaketheirhealthcare wishes known if or when a potential life-threatening event occurs and they are unabletoverbalizetheirwishesatthetimeoftheevent
ArepresentativesamplereviewofourBluePlusmembersrsquomedicalrecordsfordatesofservicein2014hasbeencompletedandtheresultsarebelowWeencourageprovidersto discuss the benefits of completing an advance directive with all our adult members
TOTAL MEMbERS IN SAMPLE
ADvANCE DIRECTIvE PRESENT OR DISCUSSED
AGE RANGE FOR MEMbERS wITH DISCUSSION
MedicareMedicaid Eligible(MSHO)
300 187(62) Avg83Range67-107
Medicaid 600 61(10) Avg48Range20-64
Body Mass Index (BMI) And Counseling For Obesity
Documentation of a memberrsquos BMI is the first step towards addressing the prevalence of obesity in our society Blue Plus completed a review of a sample of Blue Plus membersrsquomedicalrecordswithdatesofservicein2014toevaluatedocumentationofBMIvalueandcounselingforobesityObesityisdefinedasaBMIover30TheresultsareshownbelowOne-thirdofMedicaidmembersdefinedasobesehad documentation of a discussion with their provider concerning their weight management
TOTAL MEMbERS
bMI DOCUMENTED
bMI gt 30 (IF DOCUMENTED)
IF bMI gt 30 ADvISED ON wEIGHT MANAGEMENT
AvERAGE bMI FOR MEMbERS wITH DISCUSSION
MedicareMedicaid Eligible(MSHO)
300 183(61) 70(38) 6(9) Avg3603 Range3089-501
Medicaid 600 550(92) 237(43) 93(39) Avg3807 Range2676-710
Total 900 733(81) 307(42) 99(32) Avg3795
continued on next page
September 2015 9
bLUE PLUS MEDICAL RECORD DOCUMENTATION REvIEw continuedfrompage8
Tobacco Use Assessment And Counseling
AsampleofmedicalrecordswerereviewedtodeterminetobaccouseamongourBlue Plus members and discussions promoting tobacco cessation during a provider visitin2014Whiletobaccouseappearstoberoutinelyassessedatleastonceduring2014onlyhalfofourmembershavedocumentationofprovidereffortsinaddressingthis health concern
TOTAL MEMbERS
ASSESSED FOR TObACCO USE
TObACCO USE AvERAGE AGE OF TObACCO USERS
DISCUSSION ANDOR Rx ASSISTANCE
MSHO 300 281(93) 24(85) Avg75(67-87)
10(42)
PMAPMNCARE 600 518(86) 164(32) Avg44(20-64)
89(54)
Total 900 799(89) 188(24) Avg49 (20-87)
99(53)
These reviews were completed to encourage providers to open the door to meaningful discussions with their patients on important health issues If you have any questions concerning this article please send an email to the Quality and Health Management department co Sheiladalenbluecrossmncom
Better Care Through Quality Improvement
Every year Blue Cross and Blue Shield of Minnesota (Blue Cross) reviews the care delivered to our subscribers This review determines the goals for the quality program The program currently has many goals to improve health services
Making sure our subscribers receive preventive services and health screenings making sure people with health problems like heart disease receive treatment and improving the customer service experience are just a few of the goals in the program
More detailed information is available about Blue Crossrsquo process and outcomes in meeting quality improvement goals related to subscriber care and service You can see more information about our quality improvement program at bluecrossmncom Enter ldquoquality improvement programrdquo in the search field If you are unable to access the website please contact Eileen Johnson Director | AccreditationampQualityImprovementat(651) 662-4224 to request information about the Quality Improvement Program
QuALITY ImproVemeNT
September 2015 10
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
Medical and behavioral health policies are available for your use and review on the Blue Cross and Blue Shield of Minnesota website at providersbluecrossmncom From this site there are two ways to access medical policy information depending on the patientrsquos Blue Plan membership
For out-of-area Blue Plan patients SelectldquoMedicalPolicyPreCertPreAuthRouterrdquoandclickGoYouwillbetakentothepagewhereyouselecteithermedicalpolicyorpre-certificationpriorauthorizationandenterthepatientrsquosthree-letteralphaprefixasfoundontheirmemberidentificationcardandclickGoOnceyouaccepttherequirementsyouwillberoutedtothepatientrsquoshomeplanwhereyoucanaccessmedicalpolicyorpre-certificationpre-authorizationinformation
For local Blue Cross and Blue Shield of Minnesota plan patients SelectldquoMedicalpolicyrdquo(undertheToolsampResources)readandaccepttheBlueCrossMedicalPolicyStatementandthenselectldquoViewAllActivePoliciesrdquoYouhavenownavigatedtotheBlueCrossandBlueShieldofMinnesotaMedicaland Behavioral Health Policy Manual where there are several selections to assist with your inquiry
The ldquoWhatrsquos Newrdquo section identifies our latest new or revised policies approved by Blue Crossrsquo Medical and Behavioral Health Policy Committee at least 50 days ago These policies are now effective and providers should begin following thesepoliciesimmediatelyThesepoliciesalsoappearintheldquoActivePolicyrdquosectionoftheMedicalandBehavioralHealthPolicy Manual
The ldquoUpcoming Policiesrdquo section lists new or revised policies approved by the Blue Cross Medical and Behavioral Health Policy Committee and are effective 50 days from the date they were posted to the ldquoUpcoming Policiesrdquo section of the Medical and Behavioral Health Policy Manual
TheldquoActivePolicyrdquosectioncontainstheentirelistofpolicieseffectiveatthetimeofyourinquiryPleasenoteDHSPrograms(CoverageGuidelinesforDHSPrograms-MHCPManual)andMedicareContractors(PartAndashNationalGovernmentServices[NGS]PartBndashNationalGovernmentServices[NGS]HomeHealthandHospicendashNationalGovernmentServices[NGS]DurableMedicalEquipmentMedicareAdministrativeContractorndashNationalGovernmentServices[NGS]andTheCentersforMedicareandMedicaidServicesndashCMS)haveseparatesections
TheldquoPre-CertificationPre-Authorizationrdquosectionidentifiesvariousservicesproceduresprescriptiondrugsandmedicaldevicesthatrequirepre-certificationpre-authorizationThefollowingPre-CertificationPre-AuthorizationListsareprovidedforreviewCommercial(includingBlueLinkTPA)MNGovernmentProgramsandMedicarePlansTheselistsarenotexclusive to medical policy services only they encompass other services that are subject to pre-certification pre-authorizationrequirements
If you have additional questions regarding medical or behavioral health policy issues call provider services at (651) 662-5200 or 1-800-262-0820 for assistance
September 2015 11
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
MEDICAL AND bEHAvIORAL HEALTH POLICy ACTIvITy
Policies Effective 072015 Notification Posted 052815
Policies developedNone
Policies revisedPneumatic Compression Devices in the Outpatient or Home Setting
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentoflymphedemaintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet 1 The patient has undergone a four-week trial of conservative therapy which includes a Use of an appropriate compression bandage system or compression garment bExerciseAND c Elevation of the limb AND 2 Thetreatingphysiciandeterminesthatnosignificantimprovementhasoccurredorsignificantsymptomsremain
following the four-week trialbull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (non-programmable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps) OR
2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompressiontreatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentofchronicvenousinsufficiencyofthelowerextremitiesintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet
1 The patient has one or more venous stasis ulcers AND 2 ThepatienthasundergoneatrialofconservativetherapyforaminimumofsixmonthswhichincludesALLofthe
following a The use of an appropriate compression bandage system or compression garment bAppropriatedressingsforthewound c Exercise and d Elevation of the limb AND 3 Thetreatingphysiciandeterminesthatthevenousstasisulcerhasfailedtoheal
September 2015 12
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
bull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (nonprogrammable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
OR 2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompression
treatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingmaybeconsideredMEDICALLYNECESSARYinpatientswhohaveundergoneasurgicalprocedurewhenBOTH1and2aremet
1 Patient meets one or more of the following a Major surgery (eg total hip arthroplasty total knee arthroplasty hip fracture repair open abdominal or open
pelvic procedure OR b Patient is at moderate to severe risk of VTE Examples include i Patient is not able to walk unassisted or is bedridden ii Agegreaterthan60yearsanesthesiaatleast2hoursandbedrestatleast4daysduringcurrentepisodeofcare iii Inpatientstayofmorethan2daysduringcurrentepisodeofcare iv Central venous access during current episode of care v Sepsis during current episode of care viActivecancerorcancertreatment vii Significant comorbidity such as recent myocardial infarction congestive heart failure cerebrovascular disease
moderate to severe chronic obstructive pulmonary disease moderate to severe liver disease moderate to severe chronic kidney disease
viiiPregnancy or post-partum state (lt 1 month) ix Hypercoagulable state (eg Factor V Leiden antithrombin III deficiency protein C or S deficiency
antiphospholipidsyndromedysfibrinolysisprothrombin20210defect) x Prior VTE AND 2Thepatienthasacontraindicationtopharmacologicanticoagulantssuchasbeingathigh-riskforbleedingRisk
factors for bleeding include a Bleeding disorder such as hemophilia bActiveliverdisease c Severe renal failure d Previous major bleed (and previous bleeding risk similar to current risk) e Concomitant antiplatelet agent f History of or difficult-to-control surgical bleeding during the current operative procedure extensive surgical
dissection and revision surgery bull Outpatientorhomeuseofpneumaticcompressiondevicesforpost-surgicalVTEprophylaxisisconsideredNOTMEDICALLYNECESSARYforpatientswhohaveundergoneasurgicalprocedurewithalowriskforVTEandwhohaveno additional risk factors for VTE Examples of lower risk surgical procedures include but are not limited to laparoscopic cholecystectomy appendectomy transurethral prostatectomy and inguinal herniorrhaphy
September 2015 13
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingisconsideredINVESTIGATIVEforallotherindications including but not limited to treatment of arterial insufficiency (e g peripheral arterial disease) and restless legs syndrome due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Angioplasty andor Stenting for Intracranial Aneurysms and Atherosclerosis
bull IntracranialstentplacementmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranial aneurysms for patients when surgical treatment is not feasible and standard endovascular techniques do not allowforcompleteisolationoftheaneurysmegwide-neckaneurysm(4mmormore)orsack-to-neckratiolessthan21
bull IntracranialflowdivertingstentswithFDAapprovalforthetreatmentofintracranialaneurysmsmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranialaneurysmsthatarelargeorgiantwide-necked(aneurysmsizeof10mmormoreandaneckdiameterof4mmormore)intheinternalcarotidarteryfrom the petrous to the superior hypophyseal segments and which are not amenable to surgical treatment or standard endovascular therapy
bull IntracranialstentplacementisconsideredINVESTIGATIVEinthetreatmentofintracranialaneurysmsexceptasnotedabove due to the lack of clinical evidence demonstrating its impact on improved health outcomes
bull PercutaneoustransluminalangioplastywithorwithoutstentingisconsideredINVESTIGATIVEforthetreatmentofintracranial atherosclerosis due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Surgical Treatment of Femoroacetabular Impingement
bull OpenorarthroscopictreatmentoffemoroacetabularimpingementmaybeconsideredMEDICALLYNECESSARYwhenALLofthefollowingconditionsaremet
AAge Patientisskeletallymaturewithdocumentedclosureofgrowthplates(eg15yearsorolder) B Symptoms 1 Moderate-to-severe hip pain that is worsened by flexion activities (eg squatting or prolonged sitting) and which
significantlylimitsactivitiesAND 2Painwhichisunresponsiveorrecursafteratrialofconservativetherapylastingatleast3months(including
activitymodificationsrestrictionofathleticpursuitsandavoidanceofsymptomaticmotion)AND 3Positiveimpingementsignispresentonclinicalexamination(painelicitedwith90degreesofflexionandinternal
rotation and adduction of the femur) C Imaging 1Imagingstudies(egx-raysMRI)confirmthediagnosisofacamorpincer-typeFAIExamplesofmorphology
indicativeofFAIinclude a pistol-grip deformity
b femoralhead-neckoffsetwithanalphaanglegreaterthan50degrees c a positive wall sign d acetabular retroversion (overcoverage with crossover sign) e coxa profunda or protrusion f damage of the acetabular rim AND 2Noevidenceofadvancedosteoarthritis(definedasTonnisgradeIIorIIIorjointspaceoflessthan2mm)AND 3Noevidenceofsevere(modifiedOuterbridgegradeIV)chondraldamagebull Surgicaltreatmentoffemoroacetabularimpingement(FAI)isconsideredINVESTIGATIVEinallothersituations
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 14
Policies inactivatedTobacco Cessation Treatments
Policies Effective 081715 Notification Posted 062515
Policies developedNone
Policies revisedTreatment of Obstructive Sleep Apnea and Snoring in Adults bull Medical Management
A IntraoralAppliances Intraoral appliances (eg mandibular advancingpositioning devices or tongue-retaining devices) may be considered
MEDICALLYNECESSARYwhenALLofthefollowingcriteriaaremet 1PatienthasbeendiagnosedwithOSAdefinedby a AnAHIorRDIof15orgreatereventsperhour OR bAnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms i Excessive daytime sleepiness ii Documented hypertension iii Ischemic heart disease iv History of stroke AND 2Thereisabsenceoftemporomandibulardysfunctionorperiodontaldisease AND 3ThedeviceisprescribedafteradiagnosisofOSAhasbeenestablishedbyaphysicianwhoiseitheradiplomate
oftheAmericanBoardofSleepMedicinearecognizedsubspecialtyoftheAmericanBoardofMedicalSpecialties(ABMS)oranactivestaffmemberofasleepcenterorlaboratoryaccreditedbytheAmericanAcademyofSleepMedicine(AASM)orTheJointCommission
AND 4 The device is custom-fitted by qualified dental personnel under the direction of a Doctor of Dental Surgery (DDS)
or Doctor of Dental Medicine (DMD) B ContinuousPositiveAirwayPressure(CPAP) Continuouspositiveairwaypressure(CPAP)maybeconsideredMEDICALLYNECESSARYinpatientswith
confirmedOSAwith 1AnAHIorRDIof15eventsperhourorgreater OR 2AnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms a Excessive daytime sleepiness b Documented hypertension c Ischemic heart disease d History of stroke
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 15
C Bi-levelPositiveAirwayPressure(BiPAP) BiPAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPAND 2HavefailedapriortrialofCPAPOR 3ForwhomBiPAPisfoundtobemoreeffectivethanCPAPinthesleeplaboratory D Auto-AdjustingPAP(APAP) APAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPaboveAND 2HaveacontraindicationtoCPAPhavefailedapriortrialofCPAPORareundergoingatrialofAPAPtotitrate CPAP AND 3Havenoevidencebyhistoryorphysicalexaminationofthefollowingconditions a Central sleep apnea b Congestive heart failure c Chronic pulmonary disease such as chronic obstructive pulmonary disease d Pulmonary hypertension e Obesityhypoventilationsyndromeorotherconditionwhichmaycausenocturnalarterialoxyhemoglobin desaturationbull Surgical Management A Uvulopalatopharyngoplasty(UPPP) UPPPmaybeconsideredMEDICALLYNECESSARYwhenallthefollowingcriteriaaremet 1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a BMI less than 40 AND bAtrialoforalappliancetherapyhasfailedorthepatientisnotacandidateforanoralappliance AND c PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hoursper nightforthree(3)monthsofPAPusage B Maxillofacial Procedures Maxillofacial surgical procedures such as inferior sagittal mandibular osteotomy and genioglossal advancement
withorwithouthyoidmyotomyandsuspensionormandibular-maxillaryadvancement(MMA)maybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a Objectiveevidenceofhypopharyngealobstructiondocumentedbyeitherfiberopticexaminationor cephalometric radiographs AND
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 16
b PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hourspernightforthree(3)monthsofPAPusage
bull Treatment of Snoring TreatmentofsnoringisconsideredNOTMEDICALLYNECESSARYbecausesimplesnoringintheabsenceof
documented obstructive sleep apnea is not considered a medical condition Therefore all procedures for the sole or adjunctivetreatmentofsnoringareconsideredNOTMEDICALLYNECESSARYincludingbutnotlimitedto
A Uvulopalatopharyngoplasty(UPPP) B Uvulectomy C Laser-assisteduvulopalatoplasty(LAUP) D Radiofrequencyvolumetricreductionofthepalataltissues E Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues F Palatal stiffening procedures including but not limited to cautery-assisted palatal stiffening operation and the
implantation of palatal implants G Tongue base suspensionbull Investigative Indications ThefollowingtreatmentsareconsideredINVESTIGATIVEduetoalackofevidencedemonstratingimprovedhealth outcomes AUPPPforanyconditionotherthanobstructivesleepapneaorsnoring B ExpiratoryPositiveAirwayPressure(EPAP)includingtheProventregdevice C OralpressuretherapydevicesincludingbutnotlimitedtotheWinxTMsystem D Atrialpacing EAllothersurgicalproceduresforthesoleoradjunctivetreatmentofobstructivesleepapneaupperairwayresistance
syndrome including but not limited to 1 Uvulectomy 2Laser-assisteduvulopalatoplasty(LAUP) 3Radiofrequencyvolumetricreductionofthepalataltissues 4Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues 5Palatalstiffeningproceduresincludingbutnotlimitedtocautery-assistedpalatalstiffeningoperationandthe
implantation of palatal implants 6 Tongue base suspension 7 Implantable hypoglossal nerve stimulators Respiratory Syncytial Virus (RSV) Prophylaxis bull INITIALRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVfortheinitialRSVseasonmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A ChronicLungDisease(CLD)ofPrematurity 1Infantwasbornatlt32weeks0daysgestationAND 2Infantisle12monthsofageattheonsetofRSVseasonAND 3Infantrequiresgt21oxygenforatleastthefirst28daysafterbirth B Congenital Heart Disease (CHD) 1 Infant is le12monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 17
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
a AcyanoticCHDwhentheinfantisreceivingmedicationtocontrolcongestiveheartfailureandwillrequireacardiacsurgicalprocedureOR
b CyanoticCHDwhenpalivizumabisrecommendedafterconsultationwithapediatriccardiologistOR c Diagnosis of moderate to severe pulmonary hypertension OR 2Childislt24monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing a ChildundergoescardiactransplantationduringtheRSVseasonOR b ChildisreceivingRSVprophylaxisandcontinuestorequireprophylaxisafterasurgicalprocedureinvolving cardiac bypass or at the conclusion of extracorporeal membrane oxygenation C AnatomicPulmonaryAbnormalitiesORNeuromuscularDisorder(egcerebralpalsymusculardystrophy) 1 Infant is le12monthsofageattheonsetofRSVseasonAND 2Infanthasimpairedabilitytoclearsecretionsfromtheupperairway D Cystic Fibrosis 1 Infant is le12monthsofageattheonsetofRSVseasonwithevidenceofCLDandormalnutrition E Immunocompromised Status 1Childislt24monthsofageattheonsetofRSVseasonAND 2Childisprofoundlyimmunocompromised(egduetosolidorgantransplantationhematopoieticstem-cell
transplantation or chemotherapy) F Prematurity without CLD or CHD 1Infantwasbornatlt29weeks0daysgestation(ie28weeks6daysorless)AND 2Infantislt12monthsofageattheonsetofRSVseasonbull SECONDRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVforthepatientrsquossecondyearoftreatmentmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A CLDofPrematurity 1Childwasbornatlt32weeks0daysgestationAND 2Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonAND 3ChildcontinuestorequireatleastONEofthefollowingwithinsix(6)monthsofthestartofthesecondRSV season a SupplementaloxygenOR b ChronicsystemiccorticosteroidtherapyOR c DiuretictherapyOR d Bronchodilator therapy B Cystic Fibrosis 1Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonwithevidenceofCLDandor malnutritionbull AdministrationofRSVProphylaxis A Whentheappropriatecriteriaabovearemetamaximumoffive(5)monthlydosesofpalivizumab(Synagisreg)will
becoveredperRSVseason(definedasNovember1stthroughMarch31st) B Thefirstmonthlydoseofpalivizumab(Synagisreg)willbeapprovedforcoverageofadministrationonorafter
November 1st C Apost-operativedoseofpalivizumab(Synagisreg)willbecoveredforchildrenlt24monthswhoarereceiving
RSVprophylaxisandcontinuetorequireprophylaxisafterasurgicalprocedureinvolvingcardiacbypassorattheconclusion of extracorporeal membrane oxygenation
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 9
bLUE PLUS MEDICAL RECORD DOCUMENTATION REvIEw continuedfrompage8
Tobacco Use Assessment And Counseling
AsampleofmedicalrecordswerereviewedtodeterminetobaccouseamongourBlue Plus members and discussions promoting tobacco cessation during a provider visitin2014Whiletobaccouseappearstoberoutinelyassessedatleastonceduring2014onlyhalfofourmembershavedocumentationofprovidereffortsinaddressingthis health concern
TOTAL MEMbERS
ASSESSED FOR TObACCO USE
TObACCO USE AvERAGE AGE OF TObACCO USERS
DISCUSSION ANDOR Rx ASSISTANCE
MSHO 300 281(93) 24(85) Avg75(67-87)
10(42)
PMAPMNCARE 600 518(86) 164(32) Avg44(20-64)
89(54)
Total 900 799(89) 188(24) Avg49 (20-87)
99(53)
These reviews were completed to encourage providers to open the door to meaningful discussions with their patients on important health issues If you have any questions concerning this article please send an email to the Quality and Health Management department co Sheiladalenbluecrossmncom
Better Care Through Quality Improvement
Every year Blue Cross and Blue Shield of Minnesota (Blue Cross) reviews the care delivered to our subscribers This review determines the goals for the quality program The program currently has many goals to improve health services
Making sure our subscribers receive preventive services and health screenings making sure people with health problems like heart disease receive treatment and improving the customer service experience are just a few of the goals in the program
More detailed information is available about Blue Crossrsquo process and outcomes in meeting quality improvement goals related to subscriber care and service You can see more information about our quality improvement program at bluecrossmncom Enter ldquoquality improvement programrdquo in the search field If you are unable to access the website please contact Eileen Johnson Director | AccreditationampQualityImprovementat(651) 662-4224 to request information about the Quality Improvement Program
QuALITY ImproVemeNT
September 2015 10
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
Medical and behavioral health policies are available for your use and review on the Blue Cross and Blue Shield of Minnesota website at providersbluecrossmncom From this site there are two ways to access medical policy information depending on the patientrsquos Blue Plan membership
For out-of-area Blue Plan patients SelectldquoMedicalPolicyPreCertPreAuthRouterrdquoandclickGoYouwillbetakentothepagewhereyouselecteithermedicalpolicyorpre-certificationpriorauthorizationandenterthepatientrsquosthree-letteralphaprefixasfoundontheirmemberidentificationcardandclickGoOnceyouaccepttherequirementsyouwillberoutedtothepatientrsquoshomeplanwhereyoucanaccessmedicalpolicyorpre-certificationpre-authorizationinformation
For local Blue Cross and Blue Shield of Minnesota plan patients SelectldquoMedicalpolicyrdquo(undertheToolsampResources)readandaccepttheBlueCrossMedicalPolicyStatementandthenselectldquoViewAllActivePoliciesrdquoYouhavenownavigatedtotheBlueCrossandBlueShieldofMinnesotaMedicaland Behavioral Health Policy Manual where there are several selections to assist with your inquiry
The ldquoWhatrsquos Newrdquo section identifies our latest new or revised policies approved by Blue Crossrsquo Medical and Behavioral Health Policy Committee at least 50 days ago These policies are now effective and providers should begin following thesepoliciesimmediatelyThesepoliciesalsoappearintheldquoActivePolicyrdquosectionoftheMedicalandBehavioralHealthPolicy Manual
The ldquoUpcoming Policiesrdquo section lists new or revised policies approved by the Blue Cross Medical and Behavioral Health Policy Committee and are effective 50 days from the date they were posted to the ldquoUpcoming Policiesrdquo section of the Medical and Behavioral Health Policy Manual
TheldquoActivePolicyrdquosectioncontainstheentirelistofpolicieseffectiveatthetimeofyourinquiryPleasenoteDHSPrograms(CoverageGuidelinesforDHSPrograms-MHCPManual)andMedicareContractors(PartAndashNationalGovernmentServices[NGS]PartBndashNationalGovernmentServices[NGS]HomeHealthandHospicendashNationalGovernmentServices[NGS]DurableMedicalEquipmentMedicareAdministrativeContractorndashNationalGovernmentServices[NGS]andTheCentersforMedicareandMedicaidServicesndashCMS)haveseparatesections
TheldquoPre-CertificationPre-Authorizationrdquosectionidentifiesvariousservicesproceduresprescriptiondrugsandmedicaldevicesthatrequirepre-certificationpre-authorizationThefollowingPre-CertificationPre-AuthorizationListsareprovidedforreviewCommercial(includingBlueLinkTPA)MNGovernmentProgramsandMedicarePlansTheselistsarenotexclusive to medical policy services only they encompass other services that are subject to pre-certification pre-authorizationrequirements
If you have additional questions regarding medical or behavioral health policy issues call provider services at (651) 662-5200 or 1-800-262-0820 for assistance
September 2015 11
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
MEDICAL AND bEHAvIORAL HEALTH POLICy ACTIvITy
Policies Effective 072015 Notification Posted 052815
Policies developedNone
Policies revisedPneumatic Compression Devices in the Outpatient or Home Setting
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentoflymphedemaintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet 1 The patient has undergone a four-week trial of conservative therapy which includes a Use of an appropriate compression bandage system or compression garment bExerciseAND c Elevation of the limb AND 2 Thetreatingphysiciandeterminesthatnosignificantimprovementhasoccurredorsignificantsymptomsremain
following the four-week trialbull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (non-programmable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps) OR
2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompressiontreatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentofchronicvenousinsufficiencyofthelowerextremitiesintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet
1 The patient has one or more venous stasis ulcers AND 2 ThepatienthasundergoneatrialofconservativetherapyforaminimumofsixmonthswhichincludesALLofthe
following a The use of an appropriate compression bandage system or compression garment bAppropriatedressingsforthewound c Exercise and d Elevation of the limb AND 3 Thetreatingphysiciandeterminesthatthevenousstasisulcerhasfailedtoheal
September 2015 12
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
bull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (nonprogrammable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
OR 2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompression
treatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingmaybeconsideredMEDICALLYNECESSARYinpatientswhohaveundergoneasurgicalprocedurewhenBOTH1and2aremet
1 Patient meets one or more of the following a Major surgery (eg total hip arthroplasty total knee arthroplasty hip fracture repair open abdominal or open
pelvic procedure OR b Patient is at moderate to severe risk of VTE Examples include i Patient is not able to walk unassisted or is bedridden ii Agegreaterthan60yearsanesthesiaatleast2hoursandbedrestatleast4daysduringcurrentepisodeofcare iii Inpatientstayofmorethan2daysduringcurrentepisodeofcare iv Central venous access during current episode of care v Sepsis during current episode of care viActivecancerorcancertreatment vii Significant comorbidity such as recent myocardial infarction congestive heart failure cerebrovascular disease
moderate to severe chronic obstructive pulmonary disease moderate to severe liver disease moderate to severe chronic kidney disease
viiiPregnancy or post-partum state (lt 1 month) ix Hypercoagulable state (eg Factor V Leiden antithrombin III deficiency protein C or S deficiency
antiphospholipidsyndromedysfibrinolysisprothrombin20210defect) x Prior VTE AND 2Thepatienthasacontraindicationtopharmacologicanticoagulantssuchasbeingathigh-riskforbleedingRisk
factors for bleeding include a Bleeding disorder such as hemophilia bActiveliverdisease c Severe renal failure d Previous major bleed (and previous bleeding risk similar to current risk) e Concomitant antiplatelet agent f History of or difficult-to-control surgical bleeding during the current operative procedure extensive surgical
dissection and revision surgery bull Outpatientorhomeuseofpneumaticcompressiondevicesforpost-surgicalVTEprophylaxisisconsideredNOTMEDICALLYNECESSARYforpatientswhohaveundergoneasurgicalprocedurewithalowriskforVTEandwhohaveno additional risk factors for VTE Examples of lower risk surgical procedures include but are not limited to laparoscopic cholecystectomy appendectomy transurethral prostatectomy and inguinal herniorrhaphy
September 2015 13
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingisconsideredINVESTIGATIVEforallotherindications including but not limited to treatment of arterial insufficiency (e g peripheral arterial disease) and restless legs syndrome due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Angioplasty andor Stenting for Intracranial Aneurysms and Atherosclerosis
bull IntracranialstentplacementmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranial aneurysms for patients when surgical treatment is not feasible and standard endovascular techniques do not allowforcompleteisolationoftheaneurysmegwide-neckaneurysm(4mmormore)orsack-to-neckratiolessthan21
bull IntracranialflowdivertingstentswithFDAapprovalforthetreatmentofintracranialaneurysmsmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranialaneurysmsthatarelargeorgiantwide-necked(aneurysmsizeof10mmormoreandaneckdiameterof4mmormore)intheinternalcarotidarteryfrom the petrous to the superior hypophyseal segments and which are not amenable to surgical treatment or standard endovascular therapy
bull IntracranialstentplacementisconsideredINVESTIGATIVEinthetreatmentofintracranialaneurysmsexceptasnotedabove due to the lack of clinical evidence demonstrating its impact on improved health outcomes
bull PercutaneoustransluminalangioplastywithorwithoutstentingisconsideredINVESTIGATIVEforthetreatmentofintracranial atherosclerosis due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Surgical Treatment of Femoroacetabular Impingement
bull OpenorarthroscopictreatmentoffemoroacetabularimpingementmaybeconsideredMEDICALLYNECESSARYwhenALLofthefollowingconditionsaremet
AAge Patientisskeletallymaturewithdocumentedclosureofgrowthplates(eg15yearsorolder) B Symptoms 1 Moderate-to-severe hip pain that is worsened by flexion activities (eg squatting or prolonged sitting) and which
significantlylimitsactivitiesAND 2Painwhichisunresponsiveorrecursafteratrialofconservativetherapylastingatleast3months(including
activitymodificationsrestrictionofathleticpursuitsandavoidanceofsymptomaticmotion)AND 3Positiveimpingementsignispresentonclinicalexamination(painelicitedwith90degreesofflexionandinternal
rotation and adduction of the femur) C Imaging 1Imagingstudies(egx-raysMRI)confirmthediagnosisofacamorpincer-typeFAIExamplesofmorphology
indicativeofFAIinclude a pistol-grip deformity
b femoralhead-neckoffsetwithanalphaanglegreaterthan50degrees c a positive wall sign d acetabular retroversion (overcoverage with crossover sign) e coxa profunda or protrusion f damage of the acetabular rim AND 2Noevidenceofadvancedosteoarthritis(definedasTonnisgradeIIorIIIorjointspaceoflessthan2mm)AND 3Noevidenceofsevere(modifiedOuterbridgegradeIV)chondraldamagebull Surgicaltreatmentoffemoroacetabularimpingement(FAI)isconsideredINVESTIGATIVEinallothersituations
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 14
Policies inactivatedTobacco Cessation Treatments
Policies Effective 081715 Notification Posted 062515
Policies developedNone
Policies revisedTreatment of Obstructive Sleep Apnea and Snoring in Adults bull Medical Management
A IntraoralAppliances Intraoral appliances (eg mandibular advancingpositioning devices or tongue-retaining devices) may be considered
MEDICALLYNECESSARYwhenALLofthefollowingcriteriaaremet 1PatienthasbeendiagnosedwithOSAdefinedby a AnAHIorRDIof15orgreatereventsperhour OR bAnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms i Excessive daytime sleepiness ii Documented hypertension iii Ischemic heart disease iv History of stroke AND 2Thereisabsenceoftemporomandibulardysfunctionorperiodontaldisease AND 3ThedeviceisprescribedafteradiagnosisofOSAhasbeenestablishedbyaphysicianwhoiseitheradiplomate
oftheAmericanBoardofSleepMedicinearecognizedsubspecialtyoftheAmericanBoardofMedicalSpecialties(ABMS)oranactivestaffmemberofasleepcenterorlaboratoryaccreditedbytheAmericanAcademyofSleepMedicine(AASM)orTheJointCommission
AND 4 The device is custom-fitted by qualified dental personnel under the direction of a Doctor of Dental Surgery (DDS)
or Doctor of Dental Medicine (DMD) B ContinuousPositiveAirwayPressure(CPAP) Continuouspositiveairwaypressure(CPAP)maybeconsideredMEDICALLYNECESSARYinpatientswith
confirmedOSAwith 1AnAHIorRDIof15eventsperhourorgreater OR 2AnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms a Excessive daytime sleepiness b Documented hypertension c Ischemic heart disease d History of stroke
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 15
C Bi-levelPositiveAirwayPressure(BiPAP) BiPAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPAND 2HavefailedapriortrialofCPAPOR 3ForwhomBiPAPisfoundtobemoreeffectivethanCPAPinthesleeplaboratory D Auto-AdjustingPAP(APAP) APAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPaboveAND 2HaveacontraindicationtoCPAPhavefailedapriortrialofCPAPORareundergoingatrialofAPAPtotitrate CPAP AND 3Havenoevidencebyhistoryorphysicalexaminationofthefollowingconditions a Central sleep apnea b Congestive heart failure c Chronic pulmonary disease such as chronic obstructive pulmonary disease d Pulmonary hypertension e Obesityhypoventilationsyndromeorotherconditionwhichmaycausenocturnalarterialoxyhemoglobin desaturationbull Surgical Management A Uvulopalatopharyngoplasty(UPPP) UPPPmaybeconsideredMEDICALLYNECESSARYwhenallthefollowingcriteriaaremet 1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a BMI less than 40 AND bAtrialoforalappliancetherapyhasfailedorthepatientisnotacandidateforanoralappliance AND c PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hoursper nightforthree(3)monthsofPAPusage B Maxillofacial Procedures Maxillofacial surgical procedures such as inferior sagittal mandibular osteotomy and genioglossal advancement
withorwithouthyoidmyotomyandsuspensionormandibular-maxillaryadvancement(MMA)maybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a Objectiveevidenceofhypopharyngealobstructiondocumentedbyeitherfiberopticexaminationor cephalometric radiographs AND
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 16
b PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hourspernightforthree(3)monthsofPAPusage
bull Treatment of Snoring TreatmentofsnoringisconsideredNOTMEDICALLYNECESSARYbecausesimplesnoringintheabsenceof
documented obstructive sleep apnea is not considered a medical condition Therefore all procedures for the sole or adjunctivetreatmentofsnoringareconsideredNOTMEDICALLYNECESSARYincludingbutnotlimitedto
A Uvulopalatopharyngoplasty(UPPP) B Uvulectomy C Laser-assisteduvulopalatoplasty(LAUP) D Radiofrequencyvolumetricreductionofthepalataltissues E Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues F Palatal stiffening procedures including but not limited to cautery-assisted palatal stiffening operation and the
implantation of palatal implants G Tongue base suspensionbull Investigative Indications ThefollowingtreatmentsareconsideredINVESTIGATIVEduetoalackofevidencedemonstratingimprovedhealth outcomes AUPPPforanyconditionotherthanobstructivesleepapneaorsnoring B ExpiratoryPositiveAirwayPressure(EPAP)includingtheProventregdevice C OralpressuretherapydevicesincludingbutnotlimitedtotheWinxTMsystem D Atrialpacing EAllothersurgicalproceduresforthesoleoradjunctivetreatmentofobstructivesleepapneaupperairwayresistance
syndrome including but not limited to 1 Uvulectomy 2Laser-assisteduvulopalatoplasty(LAUP) 3Radiofrequencyvolumetricreductionofthepalataltissues 4Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues 5Palatalstiffeningproceduresincludingbutnotlimitedtocautery-assistedpalatalstiffeningoperationandthe
implantation of palatal implants 6 Tongue base suspension 7 Implantable hypoglossal nerve stimulators Respiratory Syncytial Virus (RSV) Prophylaxis bull INITIALRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVfortheinitialRSVseasonmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A ChronicLungDisease(CLD)ofPrematurity 1Infantwasbornatlt32weeks0daysgestationAND 2Infantisle12monthsofageattheonsetofRSVseasonAND 3Infantrequiresgt21oxygenforatleastthefirst28daysafterbirth B Congenital Heart Disease (CHD) 1 Infant is le12monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 17
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
a AcyanoticCHDwhentheinfantisreceivingmedicationtocontrolcongestiveheartfailureandwillrequireacardiacsurgicalprocedureOR
b CyanoticCHDwhenpalivizumabisrecommendedafterconsultationwithapediatriccardiologistOR c Diagnosis of moderate to severe pulmonary hypertension OR 2Childislt24monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing a ChildundergoescardiactransplantationduringtheRSVseasonOR b ChildisreceivingRSVprophylaxisandcontinuestorequireprophylaxisafterasurgicalprocedureinvolving cardiac bypass or at the conclusion of extracorporeal membrane oxygenation C AnatomicPulmonaryAbnormalitiesORNeuromuscularDisorder(egcerebralpalsymusculardystrophy) 1 Infant is le12monthsofageattheonsetofRSVseasonAND 2Infanthasimpairedabilitytoclearsecretionsfromtheupperairway D Cystic Fibrosis 1 Infant is le12monthsofageattheonsetofRSVseasonwithevidenceofCLDandormalnutrition E Immunocompromised Status 1Childislt24monthsofageattheonsetofRSVseasonAND 2Childisprofoundlyimmunocompromised(egduetosolidorgantransplantationhematopoieticstem-cell
transplantation or chemotherapy) F Prematurity without CLD or CHD 1Infantwasbornatlt29weeks0daysgestation(ie28weeks6daysorless)AND 2Infantislt12monthsofageattheonsetofRSVseasonbull SECONDRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVforthepatientrsquossecondyearoftreatmentmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A CLDofPrematurity 1Childwasbornatlt32weeks0daysgestationAND 2Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonAND 3ChildcontinuestorequireatleastONEofthefollowingwithinsix(6)monthsofthestartofthesecondRSV season a SupplementaloxygenOR b ChronicsystemiccorticosteroidtherapyOR c DiuretictherapyOR d Bronchodilator therapy B Cystic Fibrosis 1Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonwithevidenceofCLDandor malnutritionbull AdministrationofRSVProphylaxis A Whentheappropriatecriteriaabovearemetamaximumoffive(5)monthlydosesofpalivizumab(Synagisreg)will
becoveredperRSVseason(definedasNovember1stthroughMarch31st) B Thefirstmonthlydoseofpalivizumab(Synagisreg)willbeapprovedforcoverageofadministrationonorafter
November 1st C Apost-operativedoseofpalivizumab(Synagisreg)willbecoveredforchildrenlt24monthswhoarereceiving
RSVprophylaxisandcontinuetorequireprophylaxisafterasurgicalprocedureinvolvingcardiacbypassorattheconclusion of extracorporeal membrane oxygenation
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 10
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
Medical and behavioral health policies are available for your use and review on the Blue Cross and Blue Shield of Minnesota website at providersbluecrossmncom From this site there are two ways to access medical policy information depending on the patientrsquos Blue Plan membership
For out-of-area Blue Plan patients SelectldquoMedicalPolicyPreCertPreAuthRouterrdquoandclickGoYouwillbetakentothepagewhereyouselecteithermedicalpolicyorpre-certificationpriorauthorizationandenterthepatientrsquosthree-letteralphaprefixasfoundontheirmemberidentificationcardandclickGoOnceyouaccepttherequirementsyouwillberoutedtothepatientrsquoshomeplanwhereyoucanaccessmedicalpolicyorpre-certificationpre-authorizationinformation
For local Blue Cross and Blue Shield of Minnesota plan patients SelectldquoMedicalpolicyrdquo(undertheToolsampResources)readandaccepttheBlueCrossMedicalPolicyStatementandthenselectldquoViewAllActivePoliciesrdquoYouhavenownavigatedtotheBlueCrossandBlueShieldofMinnesotaMedicaland Behavioral Health Policy Manual where there are several selections to assist with your inquiry
The ldquoWhatrsquos Newrdquo section identifies our latest new or revised policies approved by Blue Crossrsquo Medical and Behavioral Health Policy Committee at least 50 days ago These policies are now effective and providers should begin following thesepoliciesimmediatelyThesepoliciesalsoappearintheldquoActivePolicyrdquosectionoftheMedicalandBehavioralHealthPolicy Manual
The ldquoUpcoming Policiesrdquo section lists new or revised policies approved by the Blue Cross Medical and Behavioral Health Policy Committee and are effective 50 days from the date they were posted to the ldquoUpcoming Policiesrdquo section of the Medical and Behavioral Health Policy Manual
TheldquoActivePolicyrdquosectioncontainstheentirelistofpolicieseffectiveatthetimeofyourinquiryPleasenoteDHSPrograms(CoverageGuidelinesforDHSPrograms-MHCPManual)andMedicareContractors(PartAndashNationalGovernmentServices[NGS]PartBndashNationalGovernmentServices[NGS]HomeHealthandHospicendashNationalGovernmentServices[NGS]DurableMedicalEquipmentMedicareAdministrativeContractorndashNationalGovernmentServices[NGS]andTheCentersforMedicareandMedicaidServicesndashCMS)haveseparatesections
TheldquoPre-CertificationPre-Authorizationrdquosectionidentifiesvariousservicesproceduresprescriptiondrugsandmedicaldevicesthatrequirepre-certificationpre-authorizationThefollowingPre-CertificationPre-AuthorizationListsareprovidedforreviewCommercial(includingBlueLinkTPA)MNGovernmentProgramsandMedicarePlansTheselistsarenotexclusive to medical policy services only they encompass other services that are subject to pre-certification pre-authorizationrequirements
If you have additional questions regarding medical or behavioral health policy issues call provider services at (651) 662-5200 or 1-800-262-0820 for assistance
September 2015 11
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
MEDICAL AND bEHAvIORAL HEALTH POLICy ACTIvITy
Policies Effective 072015 Notification Posted 052815
Policies developedNone
Policies revisedPneumatic Compression Devices in the Outpatient or Home Setting
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentoflymphedemaintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet 1 The patient has undergone a four-week trial of conservative therapy which includes a Use of an appropriate compression bandage system or compression garment bExerciseAND c Elevation of the limb AND 2 Thetreatingphysiciandeterminesthatnosignificantimprovementhasoccurredorsignificantsymptomsremain
following the four-week trialbull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (non-programmable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps) OR
2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompressiontreatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentofchronicvenousinsufficiencyofthelowerextremitiesintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet
1 The patient has one or more venous stasis ulcers AND 2 ThepatienthasundergoneatrialofconservativetherapyforaminimumofsixmonthswhichincludesALLofthe
following a The use of an appropriate compression bandage system or compression garment bAppropriatedressingsforthewound c Exercise and d Elevation of the limb AND 3 Thetreatingphysiciandeterminesthatthevenousstasisulcerhasfailedtoheal
September 2015 12
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
bull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (nonprogrammable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
OR 2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompression
treatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingmaybeconsideredMEDICALLYNECESSARYinpatientswhohaveundergoneasurgicalprocedurewhenBOTH1and2aremet
1 Patient meets one or more of the following a Major surgery (eg total hip arthroplasty total knee arthroplasty hip fracture repair open abdominal or open
pelvic procedure OR b Patient is at moderate to severe risk of VTE Examples include i Patient is not able to walk unassisted or is bedridden ii Agegreaterthan60yearsanesthesiaatleast2hoursandbedrestatleast4daysduringcurrentepisodeofcare iii Inpatientstayofmorethan2daysduringcurrentepisodeofcare iv Central venous access during current episode of care v Sepsis during current episode of care viActivecancerorcancertreatment vii Significant comorbidity such as recent myocardial infarction congestive heart failure cerebrovascular disease
moderate to severe chronic obstructive pulmonary disease moderate to severe liver disease moderate to severe chronic kidney disease
viiiPregnancy or post-partum state (lt 1 month) ix Hypercoagulable state (eg Factor V Leiden antithrombin III deficiency protein C or S deficiency
antiphospholipidsyndromedysfibrinolysisprothrombin20210defect) x Prior VTE AND 2Thepatienthasacontraindicationtopharmacologicanticoagulantssuchasbeingathigh-riskforbleedingRisk
factors for bleeding include a Bleeding disorder such as hemophilia bActiveliverdisease c Severe renal failure d Previous major bleed (and previous bleeding risk similar to current risk) e Concomitant antiplatelet agent f History of or difficult-to-control surgical bleeding during the current operative procedure extensive surgical
dissection and revision surgery bull Outpatientorhomeuseofpneumaticcompressiondevicesforpost-surgicalVTEprophylaxisisconsideredNOTMEDICALLYNECESSARYforpatientswhohaveundergoneasurgicalprocedurewithalowriskforVTEandwhohaveno additional risk factors for VTE Examples of lower risk surgical procedures include but are not limited to laparoscopic cholecystectomy appendectomy transurethral prostatectomy and inguinal herniorrhaphy
September 2015 13
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingisconsideredINVESTIGATIVEforallotherindications including but not limited to treatment of arterial insufficiency (e g peripheral arterial disease) and restless legs syndrome due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Angioplasty andor Stenting for Intracranial Aneurysms and Atherosclerosis
bull IntracranialstentplacementmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranial aneurysms for patients when surgical treatment is not feasible and standard endovascular techniques do not allowforcompleteisolationoftheaneurysmegwide-neckaneurysm(4mmormore)orsack-to-neckratiolessthan21
bull IntracranialflowdivertingstentswithFDAapprovalforthetreatmentofintracranialaneurysmsmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranialaneurysmsthatarelargeorgiantwide-necked(aneurysmsizeof10mmormoreandaneckdiameterof4mmormore)intheinternalcarotidarteryfrom the petrous to the superior hypophyseal segments and which are not amenable to surgical treatment or standard endovascular therapy
bull IntracranialstentplacementisconsideredINVESTIGATIVEinthetreatmentofintracranialaneurysmsexceptasnotedabove due to the lack of clinical evidence demonstrating its impact on improved health outcomes
bull PercutaneoustransluminalangioplastywithorwithoutstentingisconsideredINVESTIGATIVEforthetreatmentofintracranial atherosclerosis due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Surgical Treatment of Femoroacetabular Impingement
bull OpenorarthroscopictreatmentoffemoroacetabularimpingementmaybeconsideredMEDICALLYNECESSARYwhenALLofthefollowingconditionsaremet
AAge Patientisskeletallymaturewithdocumentedclosureofgrowthplates(eg15yearsorolder) B Symptoms 1 Moderate-to-severe hip pain that is worsened by flexion activities (eg squatting or prolonged sitting) and which
significantlylimitsactivitiesAND 2Painwhichisunresponsiveorrecursafteratrialofconservativetherapylastingatleast3months(including
activitymodificationsrestrictionofathleticpursuitsandavoidanceofsymptomaticmotion)AND 3Positiveimpingementsignispresentonclinicalexamination(painelicitedwith90degreesofflexionandinternal
rotation and adduction of the femur) C Imaging 1Imagingstudies(egx-raysMRI)confirmthediagnosisofacamorpincer-typeFAIExamplesofmorphology
indicativeofFAIinclude a pistol-grip deformity
b femoralhead-neckoffsetwithanalphaanglegreaterthan50degrees c a positive wall sign d acetabular retroversion (overcoverage with crossover sign) e coxa profunda or protrusion f damage of the acetabular rim AND 2Noevidenceofadvancedosteoarthritis(definedasTonnisgradeIIorIIIorjointspaceoflessthan2mm)AND 3Noevidenceofsevere(modifiedOuterbridgegradeIV)chondraldamagebull Surgicaltreatmentoffemoroacetabularimpingement(FAI)isconsideredINVESTIGATIVEinallothersituations
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 14
Policies inactivatedTobacco Cessation Treatments
Policies Effective 081715 Notification Posted 062515
Policies developedNone
Policies revisedTreatment of Obstructive Sleep Apnea and Snoring in Adults bull Medical Management
A IntraoralAppliances Intraoral appliances (eg mandibular advancingpositioning devices or tongue-retaining devices) may be considered
MEDICALLYNECESSARYwhenALLofthefollowingcriteriaaremet 1PatienthasbeendiagnosedwithOSAdefinedby a AnAHIorRDIof15orgreatereventsperhour OR bAnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms i Excessive daytime sleepiness ii Documented hypertension iii Ischemic heart disease iv History of stroke AND 2Thereisabsenceoftemporomandibulardysfunctionorperiodontaldisease AND 3ThedeviceisprescribedafteradiagnosisofOSAhasbeenestablishedbyaphysicianwhoiseitheradiplomate
oftheAmericanBoardofSleepMedicinearecognizedsubspecialtyoftheAmericanBoardofMedicalSpecialties(ABMS)oranactivestaffmemberofasleepcenterorlaboratoryaccreditedbytheAmericanAcademyofSleepMedicine(AASM)orTheJointCommission
AND 4 The device is custom-fitted by qualified dental personnel under the direction of a Doctor of Dental Surgery (DDS)
or Doctor of Dental Medicine (DMD) B ContinuousPositiveAirwayPressure(CPAP) Continuouspositiveairwaypressure(CPAP)maybeconsideredMEDICALLYNECESSARYinpatientswith
confirmedOSAwith 1AnAHIorRDIof15eventsperhourorgreater OR 2AnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms a Excessive daytime sleepiness b Documented hypertension c Ischemic heart disease d History of stroke
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 15
C Bi-levelPositiveAirwayPressure(BiPAP) BiPAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPAND 2HavefailedapriortrialofCPAPOR 3ForwhomBiPAPisfoundtobemoreeffectivethanCPAPinthesleeplaboratory D Auto-AdjustingPAP(APAP) APAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPaboveAND 2HaveacontraindicationtoCPAPhavefailedapriortrialofCPAPORareundergoingatrialofAPAPtotitrate CPAP AND 3Havenoevidencebyhistoryorphysicalexaminationofthefollowingconditions a Central sleep apnea b Congestive heart failure c Chronic pulmonary disease such as chronic obstructive pulmonary disease d Pulmonary hypertension e Obesityhypoventilationsyndromeorotherconditionwhichmaycausenocturnalarterialoxyhemoglobin desaturationbull Surgical Management A Uvulopalatopharyngoplasty(UPPP) UPPPmaybeconsideredMEDICALLYNECESSARYwhenallthefollowingcriteriaaremet 1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a BMI less than 40 AND bAtrialoforalappliancetherapyhasfailedorthepatientisnotacandidateforanoralappliance AND c PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hoursper nightforthree(3)monthsofPAPusage B Maxillofacial Procedures Maxillofacial surgical procedures such as inferior sagittal mandibular osteotomy and genioglossal advancement
withorwithouthyoidmyotomyandsuspensionormandibular-maxillaryadvancement(MMA)maybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a Objectiveevidenceofhypopharyngealobstructiondocumentedbyeitherfiberopticexaminationor cephalometric radiographs AND
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 16
b PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hourspernightforthree(3)monthsofPAPusage
bull Treatment of Snoring TreatmentofsnoringisconsideredNOTMEDICALLYNECESSARYbecausesimplesnoringintheabsenceof
documented obstructive sleep apnea is not considered a medical condition Therefore all procedures for the sole or adjunctivetreatmentofsnoringareconsideredNOTMEDICALLYNECESSARYincludingbutnotlimitedto
A Uvulopalatopharyngoplasty(UPPP) B Uvulectomy C Laser-assisteduvulopalatoplasty(LAUP) D Radiofrequencyvolumetricreductionofthepalataltissues E Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues F Palatal stiffening procedures including but not limited to cautery-assisted palatal stiffening operation and the
implantation of palatal implants G Tongue base suspensionbull Investigative Indications ThefollowingtreatmentsareconsideredINVESTIGATIVEduetoalackofevidencedemonstratingimprovedhealth outcomes AUPPPforanyconditionotherthanobstructivesleepapneaorsnoring B ExpiratoryPositiveAirwayPressure(EPAP)includingtheProventregdevice C OralpressuretherapydevicesincludingbutnotlimitedtotheWinxTMsystem D Atrialpacing EAllothersurgicalproceduresforthesoleoradjunctivetreatmentofobstructivesleepapneaupperairwayresistance
syndrome including but not limited to 1 Uvulectomy 2Laser-assisteduvulopalatoplasty(LAUP) 3Radiofrequencyvolumetricreductionofthepalataltissues 4Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues 5Palatalstiffeningproceduresincludingbutnotlimitedtocautery-assistedpalatalstiffeningoperationandthe
implantation of palatal implants 6 Tongue base suspension 7 Implantable hypoglossal nerve stimulators Respiratory Syncytial Virus (RSV) Prophylaxis bull INITIALRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVfortheinitialRSVseasonmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A ChronicLungDisease(CLD)ofPrematurity 1Infantwasbornatlt32weeks0daysgestationAND 2Infantisle12monthsofageattheonsetofRSVseasonAND 3Infantrequiresgt21oxygenforatleastthefirst28daysafterbirth B Congenital Heart Disease (CHD) 1 Infant is le12monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 17
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
a AcyanoticCHDwhentheinfantisreceivingmedicationtocontrolcongestiveheartfailureandwillrequireacardiacsurgicalprocedureOR
b CyanoticCHDwhenpalivizumabisrecommendedafterconsultationwithapediatriccardiologistOR c Diagnosis of moderate to severe pulmonary hypertension OR 2Childislt24monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing a ChildundergoescardiactransplantationduringtheRSVseasonOR b ChildisreceivingRSVprophylaxisandcontinuestorequireprophylaxisafterasurgicalprocedureinvolving cardiac bypass or at the conclusion of extracorporeal membrane oxygenation C AnatomicPulmonaryAbnormalitiesORNeuromuscularDisorder(egcerebralpalsymusculardystrophy) 1 Infant is le12monthsofageattheonsetofRSVseasonAND 2Infanthasimpairedabilitytoclearsecretionsfromtheupperairway D Cystic Fibrosis 1 Infant is le12monthsofageattheonsetofRSVseasonwithevidenceofCLDandormalnutrition E Immunocompromised Status 1Childislt24monthsofageattheonsetofRSVseasonAND 2Childisprofoundlyimmunocompromised(egduetosolidorgantransplantationhematopoieticstem-cell
transplantation or chemotherapy) F Prematurity without CLD or CHD 1Infantwasbornatlt29weeks0daysgestation(ie28weeks6daysorless)AND 2Infantislt12monthsofageattheonsetofRSVseasonbull SECONDRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVforthepatientrsquossecondyearoftreatmentmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A CLDofPrematurity 1Childwasbornatlt32weeks0daysgestationAND 2Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonAND 3ChildcontinuestorequireatleastONEofthefollowingwithinsix(6)monthsofthestartofthesecondRSV season a SupplementaloxygenOR b ChronicsystemiccorticosteroidtherapyOR c DiuretictherapyOR d Bronchodilator therapy B Cystic Fibrosis 1Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonwithevidenceofCLDandor malnutritionbull AdministrationofRSVProphylaxis A Whentheappropriatecriteriaabovearemetamaximumoffive(5)monthlydosesofpalivizumab(Synagisreg)will
becoveredperRSVseason(definedasNovember1stthroughMarch31st) B Thefirstmonthlydoseofpalivizumab(Synagisreg)willbeapprovedforcoverageofadministrationonorafter
November 1st C Apost-operativedoseofpalivizumab(Synagisreg)willbecoveredforchildrenlt24monthswhoarereceiving
RSVprophylaxisandcontinuetorequireprophylaxisafterasurgicalprocedureinvolvingcardiacbypassorattheconclusion of extracorporeal membrane oxygenation
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 11
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
MEDICAL AND bEHAvIORAL HEALTH POLICy ACTIvITy
Policies Effective 072015 Notification Posted 052815
Policies developedNone
Policies revisedPneumatic Compression Devices in the Outpatient or Home Setting
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentoflymphedemaintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet 1 The patient has undergone a four-week trial of conservative therapy which includes a Use of an appropriate compression bandage system or compression garment bExerciseAND c Elevation of the limb AND 2 Thetreatingphysiciandeterminesthatnosignificantimprovementhasoccurredorsignificantsymptomsremain
following the four-week trialbull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (non-programmable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps) OR
2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompressiontreatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull The use of segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmablepumps)maybeconsideredMEDICALLYNECESSARYforthetreatmentofchronicvenousinsufficiencyofthelowerextremitiesintheoutpatientorhomesettingwhenALLofthefollowingcriteriaaremet
1 The patient has one or more venous stasis ulcers AND 2 ThepatienthasundergoneatrialofconservativetherapyforaminimumofsixmonthswhichincludesALLofthe
following a The use of an appropriate compression bandage system or compression garment bAppropriatedressingsforthewound c Exercise and d Elevation of the limb AND 3 Thetreatingphysiciandeterminesthatthevenousstasisulcerhasfailedtoheal
September 2015 12
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
bull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (nonprogrammable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
OR 2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompression
treatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingmaybeconsideredMEDICALLYNECESSARYinpatientswhohaveundergoneasurgicalprocedurewhenBOTH1and2aremet
1 Patient meets one or more of the following a Major surgery (eg total hip arthroplasty total knee arthroplasty hip fracture repair open abdominal or open
pelvic procedure OR b Patient is at moderate to severe risk of VTE Examples include i Patient is not able to walk unassisted or is bedridden ii Agegreaterthan60yearsanesthesiaatleast2hoursandbedrestatleast4daysduringcurrentepisodeofcare iii Inpatientstayofmorethan2daysduringcurrentepisodeofcare iv Central venous access during current episode of care v Sepsis during current episode of care viActivecancerorcancertreatment vii Significant comorbidity such as recent myocardial infarction congestive heart failure cerebrovascular disease
moderate to severe chronic obstructive pulmonary disease moderate to severe liver disease moderate to severe chronic kidney disease
viiiPregnancy or post-partum state (lt 1 month) ix Hypercoagulable state (eg Factor V Leiden antithrombin III deficiency protein C or S deficiency
antiphospholipidsyndromedysfibrinolysisprothrombin20210defect) x Prior VTE AND 2Thepatienthasacontraindicationtopharmacologicanticoagulantssuchasbeingathigh-riskforbleedingRisk
factors for bleeding include a Bleeding disorder such as hemophilia bActiveliverdisease c Severe renal failure d Previous major bleed (and previous bleeding risk similar to current risk) e Concomitant antiplatelet agent f History of or difficult-to-control surgical bleeding during the current operative procedure extensive surgical
dissection and revision surgery bull Outpatientorhomeuseofpneumaticcompressiondevicesforpost-surgicalVTEprophylaxisisconsideredNOTMEDICALLYNECESSARYforpatientswhohaveundergoneasurgicalprocedurewithalowriskforVTEandwhohaveno additional risk factors for VTE Examples of lower risk surgical procedures include but are not limited to laparoscopic cholecystectomy appendectomy transurethral prostatectomy and inguinal herniorrhaphy
September 2015 13
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingisconsideredINVESTIGATIVEforallotherindications including but not limited to treatment of arterial insufficiency (e g peripheral arterial disease) and restless legs syndrome due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Angioplasty andor Stenting for Intracranial Aneurysms and Atherosclerosis
bull IntracranialstentplacementmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranial aneurysms for patients when surgical treatment is not feasible and standard endovascular techniques do not allowforcompleteisolationoftheaneurysmegwide-neckaneurysm(4mmormore)orsack-to-neckratiolessthan21
bull IntracranialflowdivertingstentswithFDAapprovalforthetreatmentofintracranialaneurysmsmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranialaneurysmsthatarelargeorgiantwide-necked(aneurysmsizeof10mmormoreandaneckdiameterof4mmormore)intheinternalcarotidarteryfrom the petrous to the superior hypophyseal segments and which are not amenable to surgical treatment or standard endovascular therapy
bull IntracranialstentplacementisconsideredINVESTIGATIVEinthetreatmentofintracranialaneurysmsexceptasnotedabove due to the lack of clinical evidence demonstrating its impact on improved health outcomes
bull PercutaneoustransluminalangioplastywithorwithoutstentingisconsideredINVESTIGATIVEforthetreatmentofintracranial atherosclerosis due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Surgical Treatment of Femoroacetabular Impingement
bull OpenorarthroscopictreatmentoffemoroacetabularimpingementmaybeconsideredMEDICALLYNECESSARYwhenALLofthefollowingconditionsaremet
AAge Patientisskeletallymaturewithdocumentedclosureofgrowthplates(eg15yearsorolder) B Symptoms 1 Moderate-to-severe hip pain that is worsened by flexion activities (eg squatting or prolonged sitting) and which
significantlylimitsactivitiesAND 2Painwhichisunresponsiveorrecursafteratrialofconservativetherapylastingatleast3months(including
activitymodificationsrestrictionofathleticpursuitsandavoidanceofsymptomaticmotion)AND 3Positiveimpingementsignispresentonclinicalexamination(painelicitedwith90degreesofflexionandinternal
rotation and adduction of the femur) C Imaging 1Imagingstudies(egx-raysMRI)confirmthediagnosisofacamorpincer-typeFAIExamplesofmorphology
indicativeofFAIinclude a pistol-grip deformity
b femoralhead-neckoffsetwithanalphaanglegreaterthan50degrees c a positive wall sign d acetabular retroversion (overcoverage with crossover sign) e coxa profunda or protrusion f damage of the acetabular rim AND 2Noevidenceofadvancedosteoarthritis(definedasTonnisgradeIIorIIIorjointspaceoflessthan2mm)AND 3Noevidenceofsevere(modifiedOuterbridgegradeIV)chondraldamagebull Surgicaltreatmentoffemoroacetabularimpingement(FAI)isconsideredINVESTIGATIVEinallothersituations
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 14
Policies inactivatedTobacco Cessation Treatments
Policies Effective 081715 Notification Posted 062515
Policies developedNone
Policies revisedTreatment of Obstructive Sleep Apnea and Snoring in Adults bull Medical Management
A IntraoralAppliances Intraoral appliances (eg mandibular advancingpositioning devices or tongue-retaining devices) may be considered
MEDICALLYNECESSARYwhenALLofthefollowingcriteriaaremet 1PatienthasbeendiagnosedwithOSAdefinedby a AnAHIorRDIof15orgreatereventsperhour OR bAnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms i Excessive daytime sleepiness ii Documented hypertension iii Ischemic heart disease iv History of stroke AND 2Thereisabsenceoftemporomandibulardysfunctionorperiodontaldisease AND 3ThedeviceisprescribedafteradiagnosisofOSAhasbeenestablishedbyaphysicianwhoiseitheradiplomate
oftheAmericanBoardofSleepMedicinearecognizedsubspecialtyoftheAmericanBoardofMedicalSpecialties(ABMS)oranactivestaffmemberofasleepcenterorlaboratoryaccreditedbytheAmericanAcademyofSleepMedicine(AASM)orTheJointCommission
AND 4 The device is custom-fitted by qualified dental personnel under the direction of a Doctor of Dental Surgery (DDS)
or Doctor of Dental Medicine (DMD) B ContinuousPositiveAirwayPressure(CPAP) Continuouspositiveairwaypressure(CPAP)maybeconsideredMEDICALLYNECESSARYinpatientswith
confirmedOSAwith 1AnAHIorRDIof15eventsperhourorgreater OR 2AnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms a Excessive daytime sleepiness b Documented hypertension c Ischemic heart disease d History of stroke
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 15
C Bi-levelPositiveAirwayPressure(BiPAP) BiPAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPAND 2HavefailedapriortrialofCPAPOR 3ForwhomBiPAPisfoundtobemoreeffectivethanCPAPinthesleeplaboratory D Auto-AdjustingPAP(APAP) APAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPaboveAND 2HaveacontraindicationtoCPAPhavefailedapriortrialofCPAPORareundergoingatrialofAPAPtotitrate CPAP AND 3Havenoevidencebyhistoryorphysicalexaminationofthefollowingconditions a Central sleep apnea b Congestive heart failure c Chronic pulmonary disease such as chronic obstructive pulmonary disease d Pulmonary hypertension e Obesityhypoventilationsyndromeorotherconditionwhichmaycausenocturnalarterialoxyhemoglobin desaturationbull Surgical Management A Uvulopalatopharyngoplasty(UPPP) UPPPmaybeconsideredMEDICALLYNECESSARYwhenallthefollowingcriteriaaremet 1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a BMI less than 40 AND bAtrialoforalappliancetherapyhasfailedorthepatientisnotacandidateforanoralappliance AND c PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hoursper nightforthree(3)monthsofPAPusage B Maxillofacial Procedures Maxillofacial surgical procedures such as inferior sagittal mandibular osteotomy and genioglossal advancement
withorwithouthyoidmyotomyandsuspensionormandibular-maxillaryadvancement(MMA)maybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a Objectiveevidenceofhypopharyngealobstructiondocumentedbyeitherfiberopticexaminationor cephalometric radiographs AND
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 16
b PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hourspernightforthree(3)monthsofPAPusage
bull Treatment of Snoring TreatmentofsnoringisconsideredNOTMEDICALLYNECESSARYbecausesimplesnoringintheabsenceof
documented obstructive sleep apnea is not considered a medical condition Therefore all procedures for the sole or adjunctivetreatmentofsnoringareconsideredNOTMEDICALLYNECESSARYincludingbutnotlimitedto
A Uvulopalatopharyngoplasty(UPPP) B Uvulectomy C Laser-assisteduvulopalatoplasty(LAUP) D Radiofrequencyvolumetricreductionofthepalataltissues E Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues F Palatal stiffening procedures including but not limited to cautery-assisted palatal stiffening operation and the
implantation of palatal implants G Tongue base suspensionbull Investigative Indications ThefollowingtreatmentsareconsideredINVESTIGATIVEduetoalackofevidencedemonstratingimprovedhealth outcomes AUPPPforanyconditionotherthanobstructivesleepapneaorsnoring B ExpiratoryPositiveAirwayPressure(EPAP)includingtheProventregdevice C OralpressuretherapydevicesincludingbutnotlimitedtotheWinxTMsystem D Atrialpacing EAllothersurgicalproceduresforthesoleoradjunctivetreatmentofobstructivesleepapneaupperairwayresistance
syndrome including but not limited to 1 Uvulectomy 2Laser-assisteduvulopalatoplasty(LAUP) 3Radiofrequencyvolumetricreductionofthepalataltissues 4Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues 5Palatalstiffeningproceduresincludingbutnotlimitedtocautery-assistedpalatalstiffeningoperationandthe
implantation of palatal implants 6 Tongue base suspension 7 Implantable hypoglossal nerve stimulators Respiratory Syncytial Virus (RSV) Prophylaxis bull INITIALRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVfortheinitialRSVseasonmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A ChronicLungDisease(CLD)ofPrematurity 1Infantwasbornatlt32weeks0daysgestationAND 2Infantisle12monthsofageattheonsetofRSVseasonAND 3Infantrequiresgt21oxygenforatleastthefirst28daysafterbirth B Congenital Heart Disease (CHD) 1 Infant is le12monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 17
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
a AcyanoticCHDwhentheinfantisreceivingmedicationtocontrolcongestiveheartfailureandwillrequireacardiacsurgicalprocedureOR
b CyanoticCHDwhenpalivizumabisrecommendedafterconsultationwithapediatriccardiologistOR c Diagnosis of moderate to severe pulmonary hypertension OR 2Childislt24monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing a ChildundergoescardiactransplantationduringtheRSVseasonOR b ChildisreceivingRSVprophylaxisandcontinuestorequireprophylaxisafterasurgicalprocedureinvolving cardiac bypass or at the conclusion of extracorporeal membrane oxygenation C AnatomicPulmonaryAbnormalitiesORNeuromuscularDisorder(egcerebralpalsymusculardystrophy) 1 Infant is le12monthsofageattheonsetofRSVseasonAND 2Infanthasimpairedabilitytoclearsecretionsfromtheupperairway D Cystic Fibrosis 1 Infant is le12monthsofageattheonsetofRSVseasonwithevidenceofCLDandormalnutrition E Immunocompromised Status 1Childislt24monthsofageattheonsetofRSVseasonAND 2Childisprofoundlyimmunocompromised(egduetosolidorgantransplantationhematopoieticstem-cell
transplantation or chemotherapy) F Prematurity without CLD or CHD 1Infantwasbornatlt29weeks0daysgestation(ie28weeks6daysorless)AND 2Infantislt12monthsofageattheonsetofRSVseasonbull SECONDRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVforthepatientrsquossecondyearoftreatmentmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A CLDofPrematurity 1Childwasbornatlt32weeks0daysgestationAND 2Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonAND 3ChildcontinuestorequireatleastONEofthefollowingwithinsix(6)monthsofthestartofthesecondRSV season a SupplementaloxygenOR b ChronicsystemiccorticosteroidtherapyOR c DiuretictherapyOR d Bronchodilator therapy B Cystic Fibrosis 1Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonwithevidenceofCLDandor malnutritionbull AdministrationofRSVProphylaxis A Whentheappropriatecriteriaabovearemetamaximumoffive(5)monthlydosesofpalivizumab(Synagisreg)will
becoveredperRSVseason(definedasNovember1stthroughMarch31st) B Thefirstmonthlydoseofpalivizumab(Synagisreg)willbeapprovedforcoverageofadministrationonorafter
November 1st C Apost-operativedoseofpalivizumab(Synagisreg)willbecoveredforchildrenlt24monthswhoarereceiving
RSVprophylaxisandcontinuetorequireprophylaxisafterasurgicalprocedureinvolvingcardiacbypassorattheconclusion of extracorporeal membrane oxygenation
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 12
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
bull The use of segmented pneumatic compression therapy devices with calibrated gradient pressure (programmable pumps)maybeconsideredMEDICALLYNECESSARYintheoutpatientorhomesettingwhenthepatientmeetscriteria for a device without calibrated gradient pressure (nonprogrammable pumps) and either of the following criteria are met
1 The patientrsquos medical condition has failed to respond to therapy using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
OR 2Theindividualhasuniquecharacteristics(egsignificantscarring)thatpreventsatisfactorypneumaticcompression
treatment using segmented or non-segmented pneumatic compression devices without calibrated gradient pressure (non-programmable pumps)
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingmaybeconsideredMEDICALLYNECESSARYinpatientswhohaveundergoneasurgicalprocedurewhenBOTH1and2aremet
1 Patient meets one or more of the following a Major surgery (eg total hip arthroplasty total knee arthroplasty hip fracture repair open abdominal or open
pelvic procedure OR b Patient is at moderate to severe risk of VTE Examples include i Patient is not able to walk unassisted or is bedridden ii Agegreaterthan60yearsanesthesiaatleast2hoursandbedrestatleast4daysduringcurrentepisodeofcare iii Inpatientstayofmorethan2daysduringcurrentepisodeofcare iv Central venous access during current episode of care v Sepsis during current episode of care viActivecancerorcancertreatment vii Significant comorbidity such as recent myocardial infarction congestive heart failure cerebrovascular disease
moderate to severe chronic obstructive pulmonary disease moderate to severe liver disease moderate to severe chronic kidney disease
viiiPregnancy or post-partum state (lt 1 month) ix Hypercoagulable state (eg Factor V Leiden antithrombin III deficiency protein C or S deficiency
antiphospholipidsyndromedysfibrinolysisprothrombin20210defect) x Prior VTE AND 2Thepatienthasacontraindicationtopharmacologicanticoagulantssuchasbeingathigh-riskforbleedingRisk
factors for bleeding include a Bleeding disorder such as hemophilia bActiveliverdisease c Severe renal failure d Previous major bleed (and previous bleeding risk similar to current risk) e Concomitant antiplatelet agent f History of or difficult-to-control surgical bleeding during the current operative procedure extensive surgical
dissection and revision surgery bull Outpatientorhomeuseofpneumaticcompressiondevicesforpost-surgicalVTEprophylaxisisconsideredNOTMEDICALLYNECESSARYforpatientswhohaveundergoneasurgicalprocedurewithalowriskforVTEandwhohaveno additional risk factors for VTE Examples of lower risk surgical procedures include but are not limited to laparoscopic cholecystectomy appendectomy transurethral prostatectomy and inguinal herniorrhaphy
September 2015 13
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingisconsideredINVESTIGATIVEforallotherindications including but not limited to treatment of arterial insufficiency (e g peripheral arterial disease) and restless legs syndrome due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Angioplasty andor Stenting for Intracranial Aneurysms and Atherosclerosis
bull IntracranialstentplacementmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranial aneurysms for patients when surgical treatment is not feasible and standard endovascular techniques do not allowforcompleteisolationoftheaneurysmegwide-neckaneurysm(4mmormore)orsack-to-neckratiolessthan21
bull IntracranialflowdivertingstentswithFDAapprovalforthetreatmentofintracranialaneurysmsmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranialaneurysmsthatarelargeorgiantwide-necked(aneurysmsizeof10mmormoreandaneckdiameterof4mmormore)intheinternalcarotidarteryfrom the petrous to the superior hypophyseal segments and which are not amenable to surgical treatment or standard endovascular therapy
bull IntracranialstentplacementisconsideredINVESTIGATIVEinthetreatmentofintracranialaneurysmsexceptasnotedabove due to the lack of clinical evidence demonstrating its impact on improved health outcomes
bull PercutaneoustransluminalangioplastywithorwithoutstentingisconsideredINVESTIGATIVEforthetreatmentofintracranial atherosclerosis due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Surgical Treatment of Femoroacetabular Impingement
bull OpenorarthroscopictreatmentoffemoroacetabularimpingementmaybeconsideredMEDICALLYNECESSARYwhenALLofthefollowingconditionsaremet
AAge Patientisskeletallymaturewithdocumentedclosureofgrowthplates(eg15yearsorolder) B Symptoms 1 Moderate-to-severe hip pain that is worsened by flexion activities (eg squatting or prolonged sitting) and which
significantlylimitsactivitiesAND 2Painwhichisunresponsiveorrecursafteratrialofconservativetherapylastingatleast3months(including
activitymodificationsrestrictionofathleticpursuitsandavoidanceofsymptomaticmotion)AND 3Positiveimpingementsignispresentonclinicalexamination(painelicitedwith90degreesofflexionandinternal
rotation and adduction of the femur) C Imaging 1Imagingstudies(egx-raysMRI)confirmthediagnosisofacamorpincer-typeFAIExamplesofmorphology
indicativeofFAIinclude a pistol-grip deformity
b femoralhead-neckoffsetwithanalphaanglegreaterthan50degrees c a positive wall sign d acetabular retroversion (overcoverage with crossover sign) e coxa profunda or protrusion f damage of the acetabular rim AND 2Noevidenceofadvancedosteoarthritis(definedasTonnisgradeIIorIIIorjointspaceoflessthan2mm)AND 3Noevidenceofsevere(modifiedOuterbridgegradeIV)chondraldamagebull Surgicaltreatmentoffemoroacetabularimpingement(FAI)isconsideredINVESTIGATIVEinallothersituations
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 14
Policies inactivatedTobacco Cessation Treatments
Policies Effective 081715 Notification Posted 062515
Policies developedNone
Policies revisedTreatment of Obstructive Sleep Apnea and Snoring in Adults bull Medical Management
A IntraoralAppliances Intraoral appliances (eg mandibular advancingpositioning devices or tongue-retaining devices) may be considered
MEDICALLYNECESSARYwhenALLofthefollowingcriteriaaremet 1PatienthasbeendiagnosedwithOSAdefinedby a AnAHIorRDIof15orgreatereventsperhour OR bAnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms i Excessive daytime sleepiness ii Documented hypertension iii Ischemic heart disease iv History of stroke AND 2Thereisabsenceoftemporomandibulardysfunctionorperiodontaldisease AND 3ThedeviceisprescribedafteradiagnosisofOSAhasbeenestablishedbyaphysicianwhoiseitheradiplomate
oftheAmericanBoardofSleepMedicinearecognizedsubspecialtyoftheAmericanBoardofMedicalSpecialties(ABMS)oranactivestaffmemberofasleepcenterorlaboratoryaccreditedbytheAmericanAcademyofSleepMedicine(AASM)orTheJointCommission
AND 4 The device is custom-fitted by qualified dental personnel under the direction of a Doctor of Dental Surgery (DDS)
or Doctor of Dental Medicine (DMD) B ContinuousPositiveAirwayPressure(CPAP) Continuouspositiveairwaypressure(CPAP)maybeconsideredMEDICALLYNECESSARYinpatientswith
confirmedOSAwith 1AnAHIorRDIof15eventsperhourorgreater OR 2AnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms a Excessive daytime sleepiness b Documented hypertension c Ischemic heart disease d History of stroke
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 15
C Bi-levelPositiveAirwayPressure(BiPAP) BiPAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPAND 2HavefailedapriortrialofCPAPOR 3ForwhomBiPAPisfoundtobemoreeffectivethanCPAPinthesleeplaboratory D Auto-AdjustingPAP(APAP) APAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPaboveAND 2HaveacontraindicationtoCPAPhavefailedapriortrialofCPAPORareundergoingatrialofAPAPtotitrate CPAP AND 3Havenoevidencebyhistoryorphysicalexaminationofthefollowingconditions a Central sleep apnea b Congestive heart failure c Chronic pulmonary disease such as chronic obstructive pulmonary disease d Pulmonary hypertension e Obesityhypoventilationsyndromeorotherconditionwhichmaycausenocturnalarterialoxyhemoglobin desaturationbull Surgical Management A Uvulopalatopharyngoplasty(UPPP) UPPPmaybeconsideredMEDICALLYNECESSARYwhenallthefollowingcriteriaaremet 1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a BMI less than 40 AND bAtrialoforalappliancetherapyhasfailedorthepatientisnotacandidateforanoralappliance AND c PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hoursper nightforthree(3)monthsofPAPusage B Maxillofacial Procedures Maxillofacial surgical procedures such as inferior sagittal mandibular osteotomy and genioglossal advancement
withorwithouthyoidmyotomyandsuspensionormandibular-maxillaryadvancement(MMA)maybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a Objectiveevidenceofhypopharyngealobstructiondocumentedbyeitherfiberopticexaminationor cephalometric radiographs AND
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 16
b PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hourspernightforthree(3)monthsofPAPusage
bull Treatment of Snoring TreatmentofsnoringisconsideredNOTMEDICALLYNECESSARYbecausesimplesnoringintheabsenceof
documented obstructive sleep apnea is not considered a medical condition Therefore all procedures for the sole or adjunctivetreatmentofsnoringareconsideredNOTMEDICALLYNECESSARYincludingbutnotlimitedto
A Uvulopalatopharyngoplasty(UPPP) B Uvulectomy C Laser-assisteduvulopalatoplasty(LAUP) D Radiofrequencyvolumetricreductionofthepalataltissues E Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues F Palatal stiffening procedures including but not limited to cautery-assisted palatal stiffening operation and the
implantation of palatal implants G Tongue base suspensionbull Investigative Indications ThefollowingtreatmentsareconsideredINVESTIGATIVEduetoalackofevidencedemonstratingimprovedhealth outcomes AUPPPforanyconditionotherthanobstructivesleepapneaorsnoring B ExpiratoryPositiveAirwayPressure(EPAP)includingtheProventregdevice C OralpressuretherapydevicesincludingbutnotlimitedtotheWinxTMsystem D Atrialpacing EAllothersurgicalproceduresforthesoleoradjunctivetreatmentofobstructivesleepapneaupperairwayresistance
syndrome including but not limited to 1 Uvulectomy 2Laser-assisteduvulopalatoplasty(LAUP) 3Radiofrequencyvolumetricreductionofthepalataltissues 4Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues 5Palatalstiffeningproceduresincludingbutnotlimitedtocautery-assistedpalatalstiffeningoperationandthe
implantation of palatal implants 6 Tongue base suspension 7 Implantable hypoglossal nerve stimulators Respiratory Syncytial Virus (RSV) Prophylaxis bull INITIALRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVfortheinitialRSVseasonmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A ChronicLungDisease(CLD)ofPrematurity 1Infantwasbornatlt32weeks0daysgestationAND 2Infantisle12monthsofageattheonsetofRSVseasonAND 3Infantrequiresgt21oxygenforatleastthefirst28daysafterbirth B Congenital Heart Disease (CHD) 1 Infant is le12monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 17
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
a AcyanoticCHDwhentheinfantisreceivingmedicationtocontrolcongestiveheartfailureandwillrequireacardiacsurgicalprocedureOR
b CyanoticCHDwhenpalivizumabisrecommendedafterconsultationwithapediatriccardiologistOR c Diagnosis of moderate to severe pulmonary hypertension OR 2Childislt24monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing a ChildundergoescardiactransplantationduringtheRSVseasonOR b ChildisreceivingRSVprophylaxisandcontinuestorequireprophylaxisafterasurgicalprocedureinvolving cardiac bypass or at the conclusion of extracorporeal membrane oxygenation C AnatomicPulmonaryAbnormalitiesORNeuromuscularDisorder(egcerebralpalsymusculardystrophy) 1 Infant is le12monthsofageattheonsetofRSVseasonAND 2Infanthasimpairedabilitytoclearsecretionsfromtheupperairway D Cystic Fibrosis 1 Infant is le12monthsofageattheonsetofRSVseasonwithevidenceofCLDandormalnutrition E Immunocompromised Status 1Childislt24monthsofageattheonsetofRSVseasonAND 2Childisprofoundlyimmunocompromised(egduetosolidorgantransplantationhematopoieticstem-cell
transplantation or chemotherapy) F Prematurity without CLD or CHD 1Infantwasbornatlt29weeks0daysgestation(ie28weeks6daysorless)AND 2Infantislt12monthsofageattheonsetofRSVseasonbull SECONDRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVforthepatientrsquossecondyearoftreatmentmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A CLDofPrematurity 1Childwasbornatlt32weeks0daysgestationAND 2Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonAND 3ChildcontinuestorequireatleastONEofthefollowingwithinsix(6)monthsofthestartofthesecondRSV season a SupplementaloxygenOR b ChronicsystemiccorticosteroidtherapyOR c DiuretictherapyOR d Bronchodilator therapy B Cystic Fibrosis 1Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonwithevidenceofCLDandor malnutritionbull AdministrationofRSVProphylaxis A Whentheappropriatecriteriaabovearemetamaximumoffive(5)monthlydosesofpalivizumab(Synagisreg)will
becoveredperRSVseason(definedasNovember1stthroughMarch31st) B Thefirstmonthlydoseofpalivizumab(Synagisreg)willbeapprovedforcoverageofadministrationonorafter
November 1st C Apost-operativedoseofpalivizumab(Synagisreg)willbecoveredforchildrenlt24monthswhoarereceiving
RSVprophylaxisandcontinuetorequireprophylaxisafterasurgicalprocedureinvolvingcardiacbypassorattheconclusion of extracorporeal membrane oxygenation
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 13
bull TheuseofpneumaticcompressiondevicesintheoutpatientorhomesettingisconsideredINVESTIGATIVEforallotherindications including but not limited to treatment of arterial insufficiency (e g peripheral arterial disease) and restless legs syndrome due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Angioplasty andor Stenting for Intracranial Aneurysms and Atherosclerosis
bull IntracranialstentplacementmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranial aneurysms for patients when surgical treatment is not feasible and standard endovascular techniques do not allowforcompleteisolationoftheaneurysmegwide-neckaneurysm(4mmormore)orsack-to-neckratiolessthan21
bull IntracranialflowdivertingstentswithFDAapprovalforthetreatmentofintracranialaneurysmsmaybeconsideredMEDICALLYNECESSARYaspartoftheendovasculartreatmentofintracranialaneurysmsthatarelargeorgiantwide-necked(aneurysmsizeof10mmormoreandaneckdiameterof4mmormore)intheinternalcarotidarteryfrom the petrous to the superior hypophyseal segments and which are not amenable to surgical treatment or standard endovascular therapy
bull IntracranialstentplacementisconsideredINVESTIGATIVEinthetreatmentofintracranialaneurysmsexceptasnotedabove due to the lack of clinical evidence demonstrating its impact on improved health outcomes
bull PercutaneoustransluminalangioplastywithorwithoutstentingisconsideredINVESTIGATIVEforthetreatmentofintracranial atherosclerosis due to the lack of clinical evidence demonstrating its impact on improved health outcomes
Surgical Treatment of Femoroacetabular Impingement
bull OpenorarthroscopictreatmentoffemoroacetabularimpingementmaybeconsideredMEDICALLYNECESSARYwhenALLofthefollowingconditionsaremet
AAge Patientisskeletallymaturewithdocumentedclosureofgrowthplates(eg15yearsorolder) B Symptoms 1 Moderate-to-severe hip pain that is worsened by flexion activities (eg squatting or prolonged sitting) and which
significantlylimitsactivitiesAND 2Painwhichisunresponsiveorrecursafteratrialofconservativetherapylastingatleast3months(including
activitymodificationsrestrictionofathleticpursuitsandavoidanceofsymptomaticmotion)AND 3Positiveimpingementsignispresentonclinicalexamination(painelicitedwith90degreesofflexionandinternal
rotation and adduction of the femur) C Imaging 1Imagingstudies(egx-raysMRI)confirmthediagnosisofacamorpincer-typeFAIExamplesofmorphology
indicativeofFAIinclude a pistol-grip deformity
b femoralhead-neckoffsetwithanalphaanglegreaterthan50degrees c a positive wall sign d acetabular retroversion (overcoverage with crossover sign) e coxa profunda or protrusion f damage of the acetabular rim AND 2Noevidenceofadvancedosteoarthritis(definedasTonnisgradeIIorIIIorjointspaceoflessthan2mm)AND 3Noevidenceofsevere(modifiedOuterbridgegradeIV)chondraldamagebull Surgicaltreatmentoffemoroacetabularimpingement(FAI)isconsideredINVESTIGATIVEinallothersituations
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 14
Policies inactivatedTobacco Cessation Treatments
Policies Effective 081715 Notification Posted 062515
Policies developedNone
Policies revisedTreatment of Obstructive Sleep Apnea and Snoring in Adults bull Medical Management
A IntraoralAppliances Intraoral appliances (eg mandibular advancingpositioning devices or tongue-retaining devices) may be considered
MEDICALLYNECESSARYwhenALLofthefollowingcriteriaaremet 1PatienthasbeendiagnosedwithOSAdefinedby a AnAHIorRDIof15orgreatereventsperhour OR bAnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms i Excessive daytime sleepiness ii Documented hypertension iii Ischemic heart disease iv History of stroke AND 2Thereisabsenceoftemporomandibulardysfunctionorperiodontaldisease AND 3ThedeviceisprescribedafteradiagnosisofOSAhasbeenestablishedbyaphysicianwhoiseitheradiplomate
oftheAmericanBoardofSleepMedicinearecognizedsubspecialtyoftheAmericanBoardofMedicalSpecialties(ABMS)oranactivestaffmemberofasleepcenterorlaboratoryaccreditedbytheAmericanAcademyofSleepMedicine(AASM)orTheJointCommission
AND 4 The device is custom-fitted by qualified dental personnel under the direction of a Doctor of Dental Surgery (DDS)
or Doctor of Dental Medicine (DMD) B ContinuousPositiveAirwayPressure(CPAP) Continuouspositiveairwaypressure(CPAP)maybeconsideredMEDICALLYNECESSARYinpatientswith
confirmedOSAwith 1AnAHIorRDIof15eventsperhourorgreater OR 2AnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms a Excessive daytime sleepiness b Documented hypertension c Ischemic heart disease d History of stroke
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 15
C Bi-levelPositiveAirwayPressure(BiPAP) BiPAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPAND 2HavefailedapriortrialofCPAPOR 3ForwhomBiPAPisfoundtobemoreeffectivethanCPAPinthesleeplaboratory D Auto-AdjustingPAP(APAP) APAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPaboveAND 2HaveacontraindicationtoCPAPhavefailedapriortrialofCPAPORareundergoingatrialofAPAPtotitrate CPAP AND 3Havenoevidencebyhistoryorphysicalexaminationofthefollowingconditions a Central sleep apnea b Congestive heart failure c Chronic pulmonary disease such as chronic obstructive pulmonary disease d Pulmonary hypertension e Obesityhypoventilationsyndromeorotherconditionwhichmaycausenocturnalarterialoxyhemoglobin desaturationbull Surgical Management A Uvulopalatopharyngoplasty(UPPP) UPPPmaybeconsideredMEDICALLYNECESSARYwhenallthefollowingcriteriaaremet 1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a BMI less than 40 AND bAtrialoforalappliancetherapyhasfailedorthepatientisnotacandidateforanoralappliance AND c PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hoursper nightforthree(3)monthsofPAPusage B Maxillofacial Procedures Maxillofacial surgical procedures such as inferior sagittal mandibular osteotomy and genioglossal advancement
withorwithouthyoidmyotomyandsuspensionormandibular-maxillaryadvancement(MMA)maybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a Objectiveevidenceofhypopharyngealobstructiondocumentedbyeitherfiberopticexaminationor cephalometric radiographs AND
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 16
b PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hourspernightforthree(3)monthsofPAPusage
bull Treatment of Snoring TreatmentofsnoringisconsideredNOTMEDICALLYNECESSARYbecausesimplesnoringintheabsenceof
documented obstructive sleep apnea is not considered a medical condition Therefore all procedures for the sole or adjunctivetreatmentofsnoringareconsideredNOTMEDICALLYNECESSARYincludingbutnotlimitedto
A Uvulopalatopharyngoplasty(UPPP) B Uvulectomy C Laser-assisteduvulopalatoplasty(LAUP) D Radiofrequencyvolumetricreductionofthepalataltissues E Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues F Palatal stiffening procedures including but not limited to cautery-assisted palatal stiffening operation and the
implantation of palatal implants G Tongue base suspensionbull Investigative Indications ThefollowingtreatmentsareconsideredINVESTIGATIVEduetoalackofevidencedemonstratingimprovedhealth outcomes AUPPPforanyconditionotherthanobstructivesleepapneaorsnoring B ExpiratoryPositiveAirwayPressure(EPAP)includingtheProventregdevice C OralpressuretherapydevicesincludingbutnotlimitedtotheWinxTMsystem D Atrialpacing EAllothersurgicalproceduresforthesoleoradjunctivetreatmentofobstructivesleepapneaupperairwayresistance
syndrome including but not limited to 1 Uvulectomy 2Laser-assisteduvulopalatoplasty(LAUP) 3Radiofrequencyvolumetricreductionofthepalataltissues 4Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues 5Palatalstiffeningproceduresincludingbutnotlimitedtocautery-assistedpalatalstiffeningoperationandthe
implantation of palatal implants 6 Tongue base suspension 7 Implantable hypoglossal nerve stimulators Respiratory Syncytial Virus (RSV) Prophylaxis bull INITIALRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVfortheinitialRSVseasonmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A ChronicLungDisease(CLD)ofPrematurity 1Infantwasbornatlt32weeks0daysgestationAND 2Infantisle12monthsofageattheonsetofRSVseasonAND 3Infantrequiresgt21oxygenforatleastthefirst28daysafterbirth B Congenital Heart Disease (CHD) 1 Infant is le12monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 17
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
a AcyanoticCHDwhentheinfantisreceivingmedicationtocontrolcongestiveheartfailureandwillrequireacardiacsurgicalprocedureOR
b CyanoticCHDwhenpalivizumabisrecommendedafterconsultationwithapediatriccardiologistOR c Diagnosis of moderate to severe pulmonary hypertension OR 2Childislt24monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing a ChildundergoescardiactransplantationduringtheRSVseasonOR b ChildisreceivingRSVprophylaxisandcontinuestorequireprophylaxisafterasurgicalprocedureinvolving cardiac bypass or at the conclusion of extracorporeal membrane oxygenation C AnatomicPulmonaryAbnormalitiesORNeuromuscularDisorder(egcerebralpalsymusculardystrophy) 1 Infant is le12monthsofageattheonsetofRSVseasonAND 2Infanthasimpairedabilitytoclearsecretionsfromtheupperairway D Cystic Fibrosis 1 Infant is le12monthsofageattheonsetofRSVseasonwithevidenceofCLDandormalnutrition E Immunocompromised Status 1Childislt24monthsofageattheonsetofRSVseasonAND 2Childisprofoundlyimmunocompromised(egduetosolidorgantransplantationhematopoieticstem-cell
transplantation or chemotherapy) F Prematurity without CLD or CHD 1Infantwasbornatlt29weeks0daysgestation(ie28weeks6daysorless)AND 2Infantislt12monthsofageattheonsetofRSVseasonbull SECONDRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVforthepatientrsquossecondyearoftreatmentmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A CLDofPrematurity 1Childwasbornatlt32weeks0daysgestationAND 2Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonAND 3ChildcontinuestorequireatleastONEofthefollowingwithinsix(6)monthsofthestartofthesecondRSV season a SupplementaloxygenOR b ChronicsystemiccorticosteroidtherapyOR c DiuretictherapyOR d Bronchodilator therapy B Cystic Fibrosis 1Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonwithevidenceofCLDandor malnutritionbull AdministrationofRSVProphylaxis A Whentheappropriatecriteriaabovearemetamaximumoffive(5)monthlydosesofpalivizumab(Synagisreg)will
becoveredperRSVseason(definedasNovember1stthroughMarch31st) B Thefirstmonthlydoseofpalivizumab(Synagisreg)willbeapprovedforcoverageofadministrationonorafter
November 1st C Apost-operativedoseofpalivizumab(Synagisreg)willbecoveredforchildrenlt24monthswhoarereceiving
RSVprophylaxisandcontinuetorequireprophylaxisafterasurgicalprocedureinvolvingcardiacbypassorattheconclusion of extracorporeal membrane oxygenation
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 14
Policies inactivatedTobacco Cessation Treatments
Policies Effective 081715 Notification Posted 062515
Policies developedNone
Policies revisedTreatment of Obstructive Sleep Apnea and Snoring in Adults bull Medical Management
A IntraoralAppliances Intraoral appliances (eg mandibular advancingpositioning devices or tongue-retaining devices) may be considered
MEDICALLYNECESSARYwhenALLofthefollowingcriteriaaremet 1PatienthasbeendiagnosedwithOSAdefinedby a AnAHIorRDIof15orgreatereventsperhour OR bAnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms i Excessive daytime sleepiness ii Documented hypertension iii Ischemic heart disease iv History of stroke AND 2Thereisabsenceoftemporomandibulardysfunctionorperiodontaldisease AND 3ThedeviceisprescribedafteradiagnosisofOSAhasbeenestablishedbyaphysicianwhoiseitheradiplomate
oftheAmericanBoardofSleepMedicinearecognizedsubspecialtyoftheAmericanBoardofMedicalSpecialties(ABMS)oranactivestaffmemberofasleepcenterorlaboratoryaccreditedbytheAmericanAcademyofSleepMedicine(AASM)orTheJointCommission
AND 4 The device is custom-fitted by qualified dental personnel under the direction of a Doctor of Dental Surgery (DDS)
or Doctor of Dental Medicine (DMD) B ContinuousPositiveAirwayPressure(CPAP) Continuouspositiveairwaypressure(CPAP)maybeconsideredMEDICALLYNECESSARYinpatientswith
confirmedOSAwith 1AnAHIorRDIof15eventsperhourorgreater OR 2AnAHIorRDIbetween5and14eventsperhourwithanyofthefollowingassociatedsymptoms a Excessive daytime sleepiness b Documented hypertension c Ischemic heart disease d History of stroke
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 15
C Bi-levelPositiveAirwayPressure(BiPAP) BiPAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPAND 2HavefailedapriortrialofCPAPOR 3ForwhomBiPAPisfoundtobemoreeffectivethanCPAPinthesleeplaboratory D Auto-AdjustingPAP(APAP) APAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPaboveAND 2HaveacontraindicationtoCPAPhavefailedapriortrialofCPAPORareundergoingatrialofAPAPtotitrate CPAP AND 3Havenoevidencebyhistoryorphysicalexaminationofthefollowingconditions a Central sleep apnea b Congestive heart failure c Chronic pulmonary disease such as chronic obstructive pulmonary disease d Pulmonary hypertension e Obesityhypoventilationsyndromeorotherconditionwhichmaycausenocturnalarterialoxyhemoglobin desaturationbull Surgical Management A Uvulopalatopharyngoplasty(UPPP) UPPPmaybeconsideredMEDICALLYNECESSARYwhenallthefollowingcriteriaaremet 1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a BMI less than 40 AND bAtrialoforalappliancetherapyhasfailedorthepatientisnotacandidateforanoralappliance AND c PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hoursper nightforthree(3)monthsofPAPusage B Maxillofacial Procedures Maxillofacial surgical procedures such as inferior sagittal mandibular osteotomy and genioglossal advancement
withorwithouthyoidmyotomyandsuspensionormandibular-maxillaryadvancement(MMA)maybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a Objectiveevidenceofhypopharyngealobstructiondocumentedbyeitherfiberopticexaminationor cephalometric radiographs AND
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 16
b PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hourspernightforthree(3)monthsofPAPusage
bull Treatment of Snoring TreatmentofsnoringisconsideredNOTMEDICALLYNECESSARYbecausesimplesnoringintheabsenceof
documented obstructive sleep apnea is not considered a medical condition Therefore all procedures for the sole or adjunctivetreatmentofsnoringareconsideredNOTMEDICALLYNECESSARYincludingbutnotlimitedto
A Uvulopalatopharyngoplasty(UPPP) B Uvulectomy C Laser-assisteduvulopalatoplasty(LAUP) D Radiofrequencyvolumetricreductionofthepalataltissues E Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues F Palatal stiffening procedures including but not limited to cautery-assisted palatal stiffening operation and the
implantation of palatal implants G Tongue base suspensionbull Investigative Indications ThefollowingtreatmentsareconsideredINVESTIGATIVEduetoalackofevidencedemonstratingimprovedhealth outcomes AUPPPforanyconditionotherthanobstructivesleepapneaorsnoring B ExpiratoryPositiveAirwayPressure(EPAP)includingtheProventregdevice C OralpressuretherapydevicesincludingbutnotlimitedtotheWinxTMsystem D Atrialpacing EAllothersurgicalproceduresforthesoleoradjunctivetreatmentofobstructivesleepapneaupperairwayresistance
syndrome including but not limited to 1 Uvulectomy 2Laser-assisteduvulopalatoplasty(LAUP) 3Radiofrequencyvolumetricreductionofthepalataltissues 4Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues 5Palatalstiffeningproceduresincludingbutnotlimitedtocautery-assistedpalatalstiffeningoperationandthe
implantation of palatal implants 6 Tongue base suspension 7 Implantable hypoglossal nerve stimulators Respiratory Syncytial Virus (RSV) Prophylaxis bull INITIALRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVfortheinitialRSVseasonmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A ChronicLungDisease(CLD)ofPrematurity 1Infantwasbornatlt32weeks0daysgestationAND 2Infantisle12monthsofageattheonsetofRSVseasonAND 3Infantrequiresgt21oxygenforatleastthefirst28daysafterbirth B Congenital Heart Disease (CHD) 1 Infant is le12monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 17
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
a AcyanoticCHDwhentheinfantisreceivingmedicationtocontrolcongestiveheartfailureandwillrequireacardiacsurgicalprocedureOR
b CyanoticCHDwhenpalivizumabisrecommendedafterconsultationwithapediatriccardiologistOR c Diagnosis of moderate to severe pulmonary hypertension OR 2Childislt24monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing a ChildundergoescardiactransplantationduringtheRSVseasonOR b ChildisreceivingRSVprophylaxisandcontinuestorequireprophylaxisafterasurgicalprocedureinvolving cardiac bypass or at the conclusion of extracorporeal membrane oxygenation C AnatomicPulmonaryAbnormalitiesORNeuromuscularDisorder(egcerebralpalsymusculardystrophy) 1 Infant is le12monthsofageattheonsetofRSVseasonAND 2Infanthasimpairedabilitytoclearsecretionsfromtheupperairway D Cystic Fibrosis 1 Infant is le12monthsofageattheonsetofRSVseasonwithevidenceofCLDandormalnutrition E Immunocompromised Status 1Childislt24monthsofageattheonsetofRSVseasonAND 2Childisprofoundlyimmunocompromised(egduetosolidorgantransplantationhematopoieticstem-cell
transplantation or chemotherapy) F Prematurity without CLD or CHD 1Infantwasbornatlt29weeks0daysgestation(ie28weeks6daysorless)AND 2Infantislt12monthsofageattheonsetofRSVseasonbull SECONDRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVforthepatientrsquossecondyearoftreatmentmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A CLDofPrematurity 1Childwasbornatlt32weeks0daysgestationAND 2Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonAND 3ChildcontinuestorequireatleastONEofthefollowingwithinsix(6)monthsofthestartofthesecondRSV season a SupplementaloxygenOR b ChronicsystemiccorticosteroidtherapyOR c DiuretictherapyOR d Bronchodilator therapy B Cystic Fibrosis 1Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonwithevidenceofCLDandor malnutritionbull AdministrationofRSVProphylaxis A Whentheappropriatecriteriaabovearemetamaximumoffive(5)monthlydosesofpalivizumab(Synagisreg)will
becoveredperRSVseason(definedasNovember1stthroughMarch31st) B Thefirstmonthlydoseofpalivizumab(Synagisreg)willbeapprovedforcoverageofadministrationonorafter
November 1st C Apost-operativedoseofpalivizumab(Synagisreg)willbecoveredforchildrenlt24monthswhoarereceiving
RSVprophylaxisandcontinuetorequireprophylaxisafterasurgicalprocedureinvolvingcardiacbypassorattheconclusion of extracorporeal membrane oxygenation
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 15
C Bi-levelPositiveAirwayPressure(BiPAP) BiPAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPAND 2HavefailedapriortrialofCPAPOR 3ForwhomBiPAPisfoundtobemoreeffectivethanCPAPinthesleeplaboratory D Auto-AdjustingPAP(APAP) APAPmaybeconsideredMEDICALLYNECESSARYinpatientswho 1MeetthecriteriaforCPAPaboveAND 2HaveacontraindicationtoCPAPhavefailedapriortrialofCPAPORareundergoingatrialofAPAPtotitrate CPAP AND 3Havenoevidencebyhistoryorphysicalexaminationofthefollowingconditions a Central sleep apnea b Congestive heart failure c Chronic pulmonary disease such as chronic obstructive pulmonary disease d Pulmonary hypertension e Obesityhypoventilationsyndromeorotherconditionwhichmaycausenocturnalarterialoxyhemoglobin desaturationbull Surgical Management A Uvulopalatopharyngoplasty(UPPP) UPPPmaybeconsideredMEDICALLYNECESSARYwhenallthefollowingcriteriaaremet 1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a BMI less than 40 AND bAtrialoforalappliancetherapyhasfailedorthepatientisnotacandidateforanoralappliance AND c PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hoursper nightforthree(3)monthsofPAPusage B Maxillofacial Procedures Maxillofacial surgical procedures such as inferior sagittal mandibular osteotomy and genioglossal advancement
withorwithouthyoidmyotomyandsuspensionormandibular-maxillaryadvancement(MMA)maybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
1PresenceofsignificantunexplainedcorpulmonaleorcardiacarrhythmiaresultingfromdocumentedOSA OR 2AnAHIorRDIof15eventsperhourorgreateroranAHIorRDIbetween5and14withdocumented
hypertension ischemic heart disease or history of stroke AND a Objectiveevidenceofhypopharyngealobstructiondocumentedbyeitherfiberopticexaminationor cephalometric radiographs AND
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 16
b PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hourspernightforthree(3)monthsofPAPusage
bull Treatment of Snoring TreatmentofsnoringisconsideredNOTMEDICALLYNECESSARYbecausesimplesnoringintheabsenceof
documented obstructive sleep apnea is not considered a medical condition Therefore all procedures for the sole or adjunctivetreatmentofsnoringareconsideredNOTMEDICALLYNECESSARYincludingbutnotlimitedto
A Uvulopalatopharyngoplasty(UPPP) B Uvulectomy C Laser-assisteduvulopalatoplasty(LAUP) D Radiofrequencyvolumetricreductionofthepalataltissues E Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues F Palatal stiffening procedures including but not limited to cautery-assisted palatal stiffening operation and the
implantation of palatal implants G Tongue base suspensionbull Investigative Indications ThefollowingtreatmentsareconsideredINVESTIGATIVEduetoalackofevidencedemonstratingimprovedhealth outcomes AUPPPforanyconditionotherthanobstructivesleepapneaorsnoring B ExpiratoryPositiveAirwayPressure(EPAP)includingtheProventregdevice C OralpressuretherapydevicesincludingbutnotlimitedtotheWinxTMsystem D Atrialpacing EAllothersurgicalproceduresforthesoleoradjunctivetreatmentofobstructivesleepapneaupperairwayresistance
syndrome including but not limited to 1 Uvulectomy 2Laser-assisteduvulopalatoplasty(LAUP) 3Radiofrequencyvolumetricreductionofthepalataltissues 4Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues 5Palatalstiffeningproceduresincludingbutnotlimitedtocautery-assistedpalatalstiffeningoperationandthe
implantation of palatal implants 6 Tongue base suspension 7 Implantable hypoglossal nerve stimulators Respiratory Syncytial Virus (RSV) Prophylaxis bull INITIALRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVfortheinitialRSVseasonmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A ChronicLungDisease(CLD)ofPrematurity 1Infantwasbornatlt32weeks0daysgestationAND 2Infantisle12monthsofageattheonsetofRSVseasonAND 3Infantrequiresgt21oxygenforatleastthefirst28daysafterbirth B Congenital Heart Disease (CHD) 1 Infant is le12monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 17
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
a AcyanoticCHDwhentheinfantisreceivingmedicationtocontrolcongestiveheartfailureandwillrequireacardiacsurgicalprocedureOR
b CyanoticCHDwhenpalivizumabisrecommendedafterconsultationwithapediatriccardiologistOR c Diagnosis of moderate to severe pulmonary hypertension OR 2Childislt24monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing a ChildundergoescardiactransplantationduringtheRSVseasonOR b ChildisreceivingRSVprophylaxisandcontinuestorequireprophylaxisafterasurgicalprocedureinvolving cardiac bypass or at the conclusion of extracorporeal membrane oxygenation C AnatomicPulmonaryAbnormalitiesORNeuromuscularDisorder(egcerebralpalsymusculardystrophy) 1 Infant is le12monthsofageattheonsetofRSVseasonAND 2Infanthasimpairedabilitytoclearsecretionsfromtheupperairway D Cystic Fibrosis 1 Infant is le12monthsofageattheonsetofRSVseasonwithevidenceofCLDandormalnutrition E Immunocompromised Status 1Childislt24monthsofageattheonsetofRSVseasonAND 2Childisprofoundlyimmunocompromised(egduetosolidorgantransplantationhematopoieticstem-cell
transplantation or chemotherapy) F Prematurity without CLD or CHD 1Infantwasbornatlt29weeks0daysgestation(ie28weeks6daysorless)AND 2Infantislt12monthsofageattheonsetofRSVseasonbull SECONDRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVforthepatientrsquossecondyearoftreatmentmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A CLDofPrematurity 1Childwasbornatlt32weeks0daysgestationAND 2Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonAND 3ChildcontinuestorequireatleastONEofthefollowingwithinsix(6)monthsofthestartofthesecondRSV season a SupplementaloxygenOR b ChronicsystemiccorticosteroidtherapyOR c DiuretictherapyOR d Bronchodilator therapy B Cystic Fibrosis 1Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonwithevidenceofCLDandor malnutritionbull AdministrationofRSVProphylaxis A Whentheappropriatecriteriaabovearemetamaximumoffive(5)monthlydosesofpalivizumab(Synagisreg)will
becoveredperRSVseason(definedasNovember1stthroughMarch31st) B Thefirstmonthlydoseofpalivizumab(Synagisreg)willbeapprovedforcoverageofadministrationonorafter
November 1st C Apost-operativedoseofpalivizumab(Synagisreg)willbecoveredforchildrenlt24monthswhoarereceiving
RSVprophylaxisandcontinuetorequireprophylaxisafterasurgicalprocedureinvolvingcardiacbypassorattheconclusion of extracorporeal membrane oxygenation
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 16
b PatienthasnotrespondedtoordoesnottolerateCPAPBiPAPorAPAPfollowingaminimumof4hourspernightforthree(3)monthsofPAPusage
bull Treatment of Snoring TreatmentofsnoringisconsideredNOTMEDICALLYNECESSARYbecausesimplesnoringintheabsenceof
documented obstructive sleep apnea is not considered a medical condition Therefore all procedures for the sole or adjunctivetreatmentofsnoringareconsideredNOTMEDICALLYNECESSARYincludingbutnotlimitedto
A Uvulopalatopharyngoplasty(UPPP) B Uvulectomy C Laser-assisteduvulopalatoplasty(LAUP) D Radiofrequencyvolumetricreductionofthepalataltissues E Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues F Palatal stiffening procedures including but not limited to cautery-assisted palatal stiffening operation and the
implantation of palatal implants G Tongue base suspensionbull Investigative Indications ThefollowingtreatmentsareconsideredINVESTIGATIVEduetoalackofevidencedemonstratingimprovedhealth outcomes AUPPPforanyconditionotherthanobstructivesleepapneaorsnoring B ExpiratoryPositiveAirwayPressure(EPAP)includingtheProventregdevice C OralpressuretherapydevicesincludingbutnotlimitedtotheWinxTMsystem D Atrialpacing EAllothersurgicalproceduresforthesoleoradjunctivetreatmentofobstructivesleepapneaupperairwayresistance
syndrome including but not limited to 1 Uvulectomy 2Laser-assisteduvulopalatoplasty(LAUP) 3Radiofrequencyvolumetricreductionofthepalataltissues 4Radiofrequencyvolumetrictissuereductionofthetonguewithorwithoutradiofrequencyreductionofthepalatal
tissues 5Palatalstiffeningproceduresincludingbutnotlimitedtocautery-assistedpalatalstiffeningoperationandthe
implantation of palatal implants 6 Tongue base suspension 7 Implantable hypoglossal nerve stimulators Respiratory Syncytial Virus (RSV) Prophylaxis bull INITIALRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVfortheinitialRSVseasonmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A ChronicLungDisease(CLD)ofPrematurity 1Infantwasbornatlt32weeks0daysgestationAND 2Infantisle12monthsofageattheonsetofRSVseasonAND 3Infantrequiresgt21oxygenforatleastthefirst28daysafterbirth B Congenital Heart Disease (CHD) 1 Infant is le12monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 17
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
a AcyanoticCHDwhentheinfantisreceivingmedicationtocontrolcongestiveheartfailureandwillrequireacardiacsurgicalprocedureOR
b CyanoticCHDwhenpalivizumabisrecommendedafterconsultationwithapediatriccardiologistOR c Diagnosis of moderate to severe pulmonary hypertension OR 2Childislt24monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing a ChildundergoescardiactransplantationduringtheRSVseasonOR b ChildisreceivingRSVprophylaxisandcontinuestorequireprophylaxisafterasurgicalprocedureinvolving cardiac bypass or at the conclusion of extracorporeal membrane oxygenation C AnatomicPulmonaryAbnormalitiesORNeuromuscularDisorder(egcerebralpalsymusculardystrophy) 1 Infant is le12monthsofageattheonsetofRSVseasonAND 2Infanthasimpairedabilitytoclearsecretionsfromtheupperairway D Cystic Fibrosis 1 Infant is le12monthsofageattheonsetofRSVseasonwithevidenceofCLDandormalnutrition E Immunocompromised Status 1Childislt24monthsofageattheonsetofRSVseasonAND 2Childisprofoundlyimmunocompromised(egduetosolidorgantransplantationhematopoieticstem-cell
transplantation or chemotherapy) F Prematurity without CLD or CHD 1Infantwasbornatlt29weeks0daysgestation(ie28weeks6daysorless)AND 2Infantislt12monthsofageattheonsetofRSVseasonbull SECONDRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVforthepatientrsquossecondyearoftreatmentmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A CLDofPrematurity 1Childwasbornatlt32weeks0daysgestationAND 2Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonAND 3ChildcontinuestorequireatleastONEofthefollowingwithinsix(6)monthsofthestartofthesecondRSV season a SupplementaloxygenOR b ChronicsystemiccorticosteroidtherapyOR c DiuretictherapyOR d Bronchodilator therapy B Cystic Fibrosis 1Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonwithevidenceofCLDandor malnutritionbull AdministrationofRSVProphylaxis A Whentheappropriatecriteriaabovearemetamaximumoffive(5)monthlydosesofpalivizumab(Synagisreg)will
becoveredperRSVseason(definedasNovember1stthroughMarch31st) B Thefirstmonthlydoseofpalivizumab(Synagisreg)willbeapprovedforcoverageofadministrationonorafter
November 1st C Apost-operativedoseofpalivizumab(Synagisreg)willbecoveredforchildrenlt24monthswhoarereceiving
RSVprophylaxisandcontinuetorequireprophylaxisafterasurgicalprocedureinvolvingcardiacbypassorattheconclusion of extracorporeal membrane oxygenation
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 17
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
a AcyanoticCHDwhentheinfantisreceivingmedicationtocontrolcongestiveheartfailureandwillrequireacardiacsurgicalprocedureOR
b CyanoticCHDwhenpalivizumabisrecommendedafterconsultationwithapediatriccardiologistOR c Diagnosis of moderate to severe pulmonary hypertension OR 2Childislt24monthsofageattheonsetofRSVseasonANDmeetsONEofthefollowing a ChildundergoescardiactransplantationduringtheRSVseasonOR b ChildisreceivingRSVprophylaxisandcontinuestorequireprophylaxisafterasurgicalprocedureinvolving cardiac bypass or at the conclusion of extracorporeal membrane oxygenation C AnatomicPulmonaryAbnormalitiesORNeuromuscularDisorder(egcerebralpalsymusculardystrophy) 1 Infant is le12monthsofageattheonsetofRSVseasonAND 2Infanthasimpairedabilitytoclearsecretionsfromtheupperairway D Cystic Fibrosis 1 Infant is le12monthsofageattheonsetofRSVseasonwithevidenceofCLDandormalnutrition E Immunocompromised Status 1Childislt24monthsofageattheonsetofRSVseasonAND 2Childisprofoundlyimmunocompromised(egduetosolidorgantransplantationhematopoieticstem-cell
transplantation or chemotherapy) F Prematurity without CLD or CHD 1Infantwasbornatlt29weeks0daysgestation(ie28weeks6daysorless)AND 2Infantislt12monthsofageattheonsetofRSVseasonbull SECONDRSVSEASON Theuseofimmuneprophylaxis(egpalivizumab[Synagis])forRSVforthepatientrsquossecondyearoftreatmentmaybeconsideredMEDICALLYNECESSARYwhenthefollowingcriteriaaremet
A CLDofPrematurity 1Childwasbornatlt32weeks0daysgestationAND 2Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonAND 3ChildcontinuestorequireatleastONEofthefollowingwithinsix(6)monthsofthestartofthesecondRSV season a SupplementaloxygenOR b ChronicsystemiccorticosteroidtherapyOR c DiuretictherapyOR d Bronchodilator therapy B Cystic Fibrosis 1Childis12monthstolt24monthsofageattheonsetofthesecondRSVseasonwithevidenceofCLDandor malnutritionbull AdministrationofRSVProphylaxis A Whentheappropriatecriteriaabovearemetamaximumoffive(5)monthlydosesofpalivizumab(Synagisreg)will
becoveredperRSVseason(definedasNovember1stthroughMarch31st) B Thefirstmonthlydoseofpalivizumab(Synagisreg)willbeapprovedforcoverageofadministrationonorafter
November 1st C Apost-operativedoseofpalivizumab(Synagisreg)willbecoveredforchildrenlt24monthswhoarereceiving
RSVprophylaxisandcontinuetorequireprophylaxisafterasurgicalprocedureinvolvingcardiacbypassorattheconclusion of extracorporeal membrane oxygenation
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring
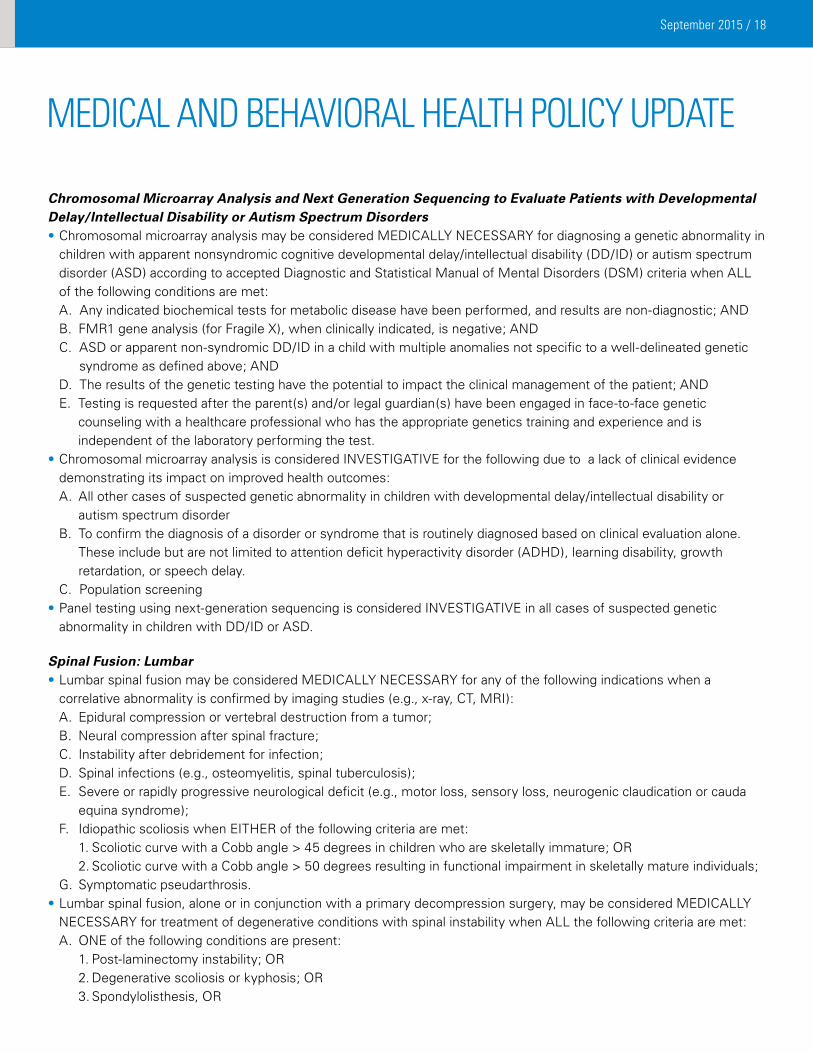
September 2015 18
Chromosomal Microarray Analysis and Next Generation Sequencing to Evaluate Patients with Developmental DelayIntellectual Disability or Autism Spectrum Disorders bullChromosomalmicroarrayanalysismaybeconsideredMEDICALLYNECESSARYfordiagnosingageneticabnormalityin
children with apparent nonsyndromic cognitive developmental delayintellectual disability (DDID) or autism spectrum disorder(ASD)accordingtoacceptedDiagnosticandStatisticalManualofMentalDisorders(DSM)criteriawhenALLof the following conditions are met
AAnyindicatedbiochemicaltestsformetabolicdiseasehavebeenperformedandresultsarenon-diagnosticAND BFMR1geneanalysis(forFragileX)whenclinicallyindicatedisnegativeAND CASDorapparentnon-syndromicDDIDinachildwithmultipleanomaliesnotspecifictoawell-delineatedgenetic
syndromeasdefinedaboveAND DTheresultsofthegenetictestinghavethepotentialtoimpacttheclinicalmanagementofthepatientAND E Testing is requested after the parent(s) andor legal guardian(s) have been engaged in face-to-face genetic
counseling with a healthcare professional who has the appropriate genetics training and experience and is independent of the laboratory performing the test
bullChromosomalmicroarrayanalysisisconsideredINVESTIGATIVEforthefollowingduetoalackofclinicalevidencedemonstrating its impact on improved health outcomes
A Allothercasesofsuspectedgeneticabnormalityinchildrenwithdevelopmentaldelayintellectualdisabilityorautism spectrum disorder
B To confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone Theseincludebutarenotlimitedtoattentiondeficithyperactivitydisorder(ADHD)learningdisabilitygrowthretardation or speech delay
C Population screeningbullPaneltestingusingnext-generationsequencingisconsideredINVESTIGATIVEinallcasesofsuspectedgeneticabnormalityinchildrenwithDDIDorASD
Spinal Fusion Lumbar bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforanyofthefollowingindicationswhenacorrelativeabnormalityisconfirmedbyimagingstudies(egx-rayCTMRI)
A Epiduralcompressionorvertebraldestructionfromatumor B Neural compression after spinal fracture C Instability after debridement for infection D Spinal infections (eg osteomyelitis spinal tuberculosis) E Severe or rapidly progressive neurological deficit (eg motor loss sensory loss neurogenic claudication or cauda
equina syndrome) F IdiopathicscoliosiswhenEITHERofthefollowingcriteriaaremet 1ScolioticcurvewithaCobbanglegt45degreesinchildrenwhoareskeletallyimmatureOR 2ScolioticcurvewithaCobbanglegt50degreesresultinginfunctionalimpairmentinskeletallymatureindividuals G Symptomatic pseudarthrosisbullLumbarspinalfusionaloneorinconjunctionwithaprimarydecompressionsurgerymaybeconsideredMEDICALLYNECESSARYfortreatmentofdegenerativeconditionswithspinalinstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1Post-laminectomyinstabilityOR 2DegenerativescoliosisorkyphosisOR 3SpondylolisthesisOR
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 19
4 Spinal stenosis with spondylolisthesis AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egx-rayCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalinstability(gt
3mmoftranslationandor10degreesormoreofangulationofonevertebracomparedtotheadjacentvertebrainaspinal motion segment)
bullLumbarspinalfusioninconjunctionwithadecompressionsurgerymaybeconsideredMEDICALLYNECESSARYinthetreatmentofcertaindegenerativeconditionswithoutexistinginstabilitywhenALLthefollowingcriteriaaremet
A ONEofthefollowingconditionsarepresent 1SpinalstenosisOR 2RecurrentspinalstenosisatthesamesegmentOR 3Recurrentdischerniationwithfailedlaminectomy AND B Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyfor3monthsIntensive
conservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing 1Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section) AND 2Aminimumoftwosessionsperweekoverthe3-monthperiodAND 3FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy AND 4Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources of back pain AND C Diagnosticimaging(egCTMRI)obtainedwithintheprevious12monthsdemonstratesspinalcordornerveroot
compression
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 20
bullLumbarspinalfusionmaybeconsideredMEDICALLYNECESSARYforchronic(presentforatleast6ndash12months)discogenicbackpainwithoutinstabilitywhenALLthefollowingcriteriaaremet
A Documentedunremittingpainanddisabilityrefractorytointensiveconservativetherapyforatleast3months Intensiveconservativetherapymusthaveoccurredwithintheprevious12monthsANDmustincludeALLofthefollowing
1Anti-inflammatorymedicationandanalgesicsunlesscontraindicatedAND 2TherapeuticinjectionsAND 3Anactiveorganizedandprogressivestrengthandflexibilityprogram NOTEIfapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningpainanddisability
the case will be reviewed on an individual basis by an internal physician reviewer (See Documentation Submission section)
AND 4Aminimumoftwosessionsperweekoverthe3-monthperiodAND 5FunctionalassessmentasmeasuredbytheOswestryDisabilityIndex(ODI)demonstratingONEofthe
following a Lessthan30improvementintheODIscorebetweenthefirstandlastphysicaltherapysessionOR b ContinuedODIscoreofgreaterthanorequalto40attheconclusionofphysicaltherapy 6Aneducationalcomponentthatdealswithpatientexpectationsandperceptionsaswellastheanatomicsources
of back pain AND B Absenceofuntreatedunderlyingcontributorymentalhealthconditionsorpsychosocialissuesincludingbutnot
limited to depression or drug or alcohol abuse AND C Diagnosticimaging(egMRICT)obtainedwithintheprevious12monthsdemonstratesdegenerativediscdisease
limitedto1ndash2disclevelsbull Documentation supporting the medical necessity criteria described in the policy must be included in the prior authorizationInadditionthefollowingdocumentationmustalsobesubmitted
1 Written report from a radiologist describing findings from spinal diagnostic imaging studies 2 Intensiveconservativetherapy bull DocumentationfromthephysicaltherapistmustincludeOswestryDisabilityIndex(ODI)scores bull Ifapatientisunabletocompletephysicaltherapy(PT)duetoprogressivelyworseningsymptomsofpainand
disability the case will be reviewed on an individual basis by an internal physician reviewer Documentation must be submitted from the physical therapist describing the patientrsquos inability to complete PT
3 Forpatientswithchronicdiscogenicbackpainwithoutinstability(policysectionIV)documentationregardingthe absence of untreated underlying contributory mental health conditions or psychosocial issues including but not limited to depression or drug or alcohol abuse must be submitted by the patientrsquos primary care physician or a Mental Health Professional The Mental Health Professional must meet the Minnesota Department of Human ServicesqualificationsassetforthinMinnStatsect245462subd18(2013)andMinnStatsect2454871subd27(2013)
medICAL ANd BeHAVIorAL HeALTH poLICY updATe
September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 21
Policies inactivatedNone There was no Medical and behavioral Health Policy Activity for July 2015
Policies reviewed with no changes in May 2015 and June 2015
Acupuncture
Artificial Intervertebral Disc Cervical Spine
Belimumab
Cardiovascular Disease Risk Assessment and Management Laboratory Evaluation of Non-Traditional Lipid and
Nonlipid Biomarkers
Cellular Immunotherapy for Prostate Cancer
Chelation Therapy
Computerized Dynamic Posturography
Continuous and Intermittent Glucose Monitoring of Interstitial Fluid
Cytochrome P450 Genotyping
Digital Breast Tomosynthesis
Electrocardiographic (ECG) Body Surface Mapping
Endoscopic Radiofrequency Ablation or Cryoablation for Barrettrsquos Esophagus
Epidermal Growth-Factor Receptor (EGFR) Analysis for Non-small Cell Lung Cancer
HP Acthar Gel (Repository Corticotropin)
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
Hematopoietic Stem-Cell Transplantation for Primary Amyloidosis
Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia
Image-Guided Minimally Invasive Lumbar Decompression for Spinal Stenosis
Liposuction
Lung Cancer Screening Using Computed Tomography (CT)
Mastopexy
Microprocessor-Controlled Prosthesis for the Lower Limb
Myoelectric Prosthesis for the Upper Limb
Organ Transplantation
Percutaneous and Endoscopic Techniques for Disc Decompression
September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring

September 2015 22
Medical and Behavioral Health Policy Update
NetworkManagementR317 POBox64560 StPaulMN55164-0560
Provider Press is posted on our website quarterly for business office staff of multi-specialty clinics physicians public health agencies DME providers chiropractors podiatrists physical therapists occupational therapists optometrists and behavioral health professionalsproviders Direct inquiries to
NetworkManagementR317Editor Holly BatchelderPOBox64560StPaulMN55164-0560(651)662-2014tollfree1-800-382-2000ext22014
AdvisorsFaithBauerCPCCPC-HCPC-PJeannieHarpCPCJanineUtechtCPCCPC-HCPC-PCPMAandKarenKiemeleMPH
Information in Provider Press is a general outline Provider and member contracts determine benefits
CPT-4codesnotedareAMAcopyrighted
0915
Peripheral Nerve Stimulation of the Trunk or Limbs for Treatment of Pain
Rhinomanometry and AcousticOptical Rhinometry
Sleep Studies Polysomnograms in Children and Adolescents
Spinal Unloading Devices Patient-Operated
Stem-Cell Therapy for Peripheral Arterial Disease
Subcutaneous Hormone Pellets
Surgical Interruption of Pelvic Nerve Pathways for Primary and Secondary Dysmenorrhea
Systems Pathology Testing for Predicting Risk of Recurrence in Prostate Cancer
Urine Drug Testing for Substance Abuse Treatment and Chronic Pain Management
Wireless Gastric Motility Monitoring