pseudoaneurysm with left-to-right shunt in a patient with myocardial infarction: evaluation by...
TRANSCRIPT

CASE REPORT
Pseudoaneurysm with left-to-right shunt in a patientwith myocardial infarction: evaluation by three-dimensionalechocardiography
Hirofumi Maeba • Yoko Miyasaka •
Ayako Kotaka • Satoshi Tsujimoto •
Fumio Yuasa • Toshiji Iwasaka
Received: 7 October 2011 / Accepted: 17 January 2012 / Published online: 7 April 2012
� The Japan Society of Ultrasonics in Medicine 2012
Abstract It is often difficult to noninvasively differenti-
ate a post-infarction left ventricular (LV) pseudoaneurysm
from a post-infarction true aneurysm. A 66-year-old
woman with a past history of inferior acute myocardial
infarction was admitted to our hospital because of acute
decompensated heart failure. Two-dimensional transtho-
racic echocardiography showed an aneurysm with a narrow
orifice in the inferoposterior basal area. The pulmonary to
systemic flow ratio (Qp/Qs) was 2.2:1, which corresponded
to moderate left–right shunting. Three-dimensional trans-
esophageal echocardiography (3D-TEE) showed the orifice
in the perforated right ventricular basal area with a color jet
through the orifice from the LV to the right ventricle.
Collectively, based on the 3D-TEE findings, we diagnosed
the case as inferoposterior pseudoaneurysm with a left-to-
right shunt caused by myocardial infarction.
Keywords Pseudoaneurysm � Left-to-right shunt �Three-dimensional transesophageal echocardiography
Introduction
A post-infarction left ventricular (LV) pseudoaneurysm
develops when the ventricular free wall is ruptured and
contained by overlying adherent pericardium. A post-
infarction true aneurysm, in contrast, is caused by scar
formation resulting in the thinning of the myocardium [1]. It
has been reported that a post-infarction LV pseudoaneu-
rysm is a rare complication, accounting for approximately
2% of all LV aneurysm cases [2, 3]. Contrast ventriculog-
raphy, radionuclide ventriculography, and magnetic reso-
nance imaging (MRI) have been used as diagnostic
approaches to distinguish between the two entities. Here,
we report a patient with a post-infarction LV pseudoaneu-
rysm with a left-to-right shunt evaluated by three-dimen-
sional transesophageal echocardiography (3D-TEE).
Case report
A 66-year-old woman with a past history of cerebral
infarction was referred to our coronary care unit (CCU)
because of chest pain. From electrocardiography (ECG)
findings with ST elevation, inferoposterior myocardial
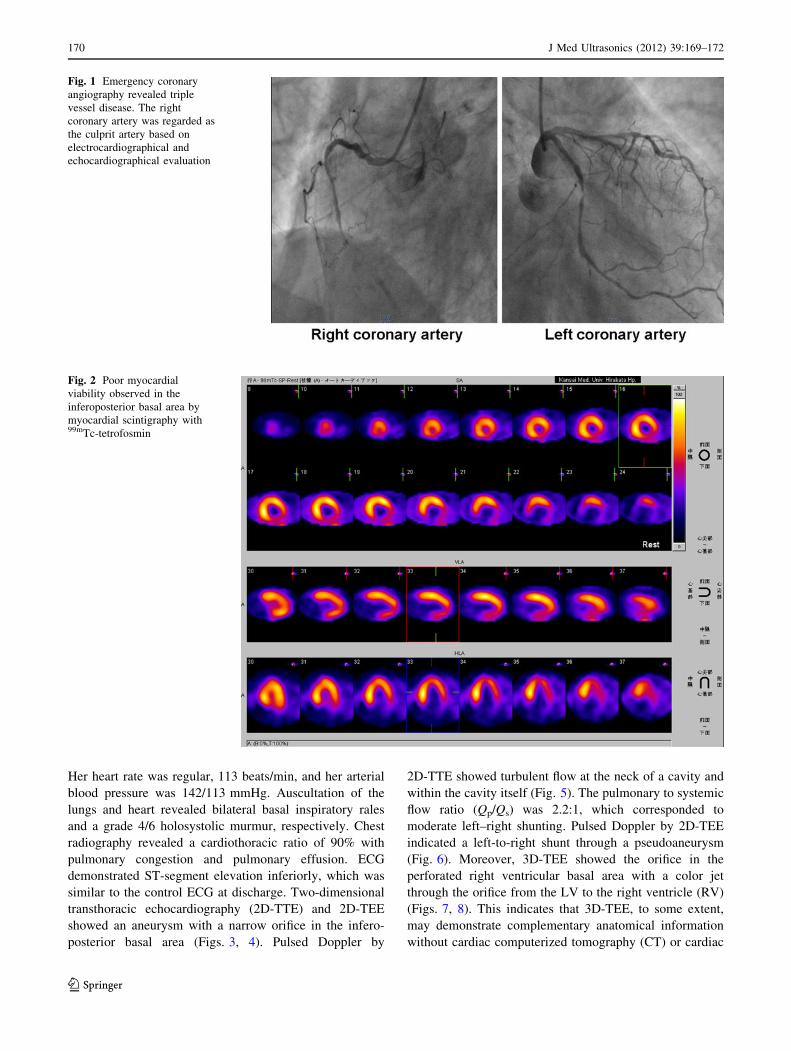
infarction was diagnosed. Emergency coronary angiogra-
phy revealed triple vessel disease (#6: 90%, #3: 100%, #13:
90%) (Fig. 1). The culprit lesion in the right coronary
artery was reperfused with a bare metal stent within 6 h
after onset. The residual stenosis in the left descending
artery and left circumflex artery was reperfused electively
with a drug-eluting stent. Although all coronary artery
branches were reperfused successfully with TIMI 3 flow,
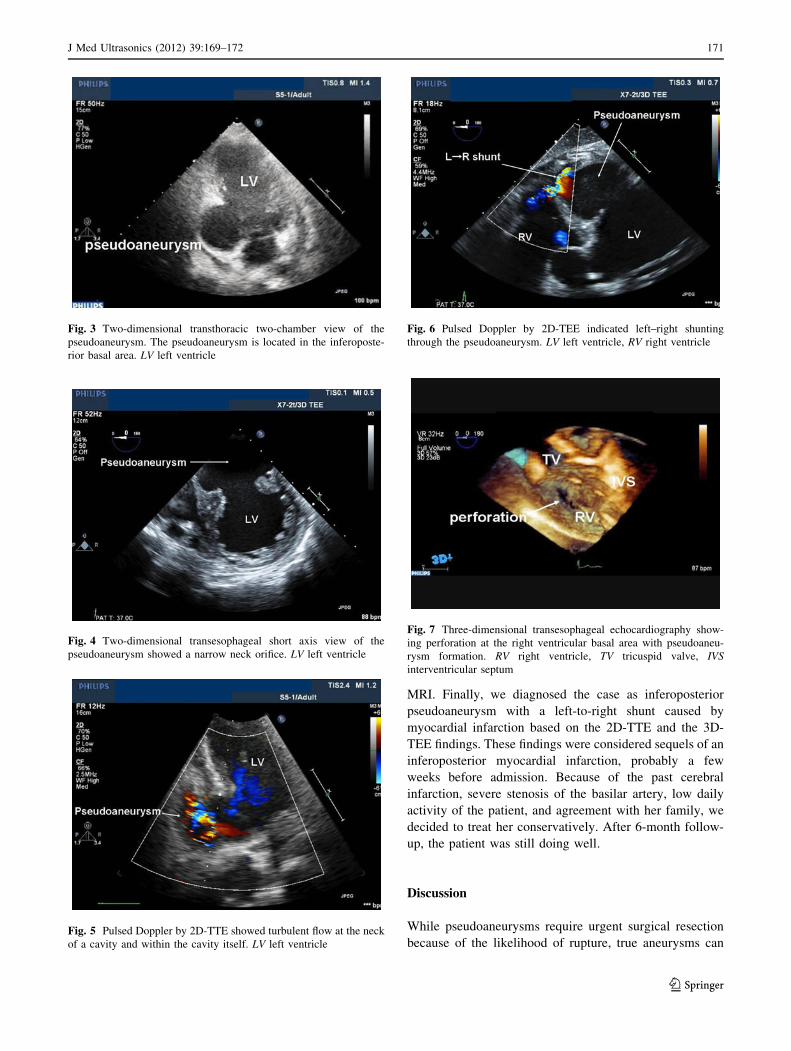
myocardial scintigraphy with 99mTc-tetrofosmin revealed
that myocardial viability in the inferoposterior basal area
was not preserved (Fig. 2). Consequently, she was dis-
charged on the 19th day without cardiac complication.
On the 29th day, she was referred to our CCU again as a
result of progressive dyspnea. Physical examination
revealed peripheral edema of the lower limbs and signs of
raised jugular venous pressure. No abdominal abnormali-
ties were found. Neurological examination revealed
abnormalities because of the previous cerebral infarction.
H. Maeba (&) � Y. Miyasaka � A. Kotaka � S. Tsujimoto �F. Yuasa � T. Iwasaka
Division of Cardiovascular Disease,
Department of Medicine II, Kansai Medical University,
2-3-1 Shinmachi, Hirakata, Osaka 573-1191, Japan
e-mail: [email protected]
123
J Med Ultrasonics (2012) 39:169–172
DOI 10.1007/s10396-012-0355-x
Her heart rate was regular, 113 beats/min, and her arterial
blood pressure was 142/113 mmHg. Auscultation of the
lungs and heart revealed bilateral basal inspiratory rales
and a grade 4/6 holosystolic murmur, respectively. Chest
radiography revealed a cardiothoracic ratio of 90% with
pulmonary congestion and pulmonary effusion. ECG
demonstrated ST-segment elevation inferiorly, which was
similar to the control ECG at discharge. Two-dimensional
transthoracic echocardiography (2D-TTE) and 2D-TEE
showed an aneurysm with a narrow orifice in the infero-
posterior basal area (Figs. 3, 4). Pulsed Doppler by
2D-TTE showed turbulent flow at the neck of a cavity and
within the cavity itself (Fig. 5). The pulmonary to systemic
flow ratio (Qp/Qs) was 2.2:1, which corresponded to
moderate left–right shunting. Pulsed Doppler by 2D-TEE
indicated a left-to-right shunt through a pseudoaneurysm
(Fig. 6). Moreover, 3D-TEE showed the orifice in the
perforated right ventricular basal area with a color jet
through the orifice from the LV to the right ventricle (RV)
(Figs. 7, 8). This indicates that 3D-TEE, to some extent,
may demonstrate complementary anatomical information
without cardiac computerized tomography (CT) or cardiac
Fig. 1 Emergency coronary
angiography revealed triple
vessel disease. The right
coronary artery was regarded as
the culprit artery based on
electrocardiographical and
echocardiographical evaluation
Fig. 2 Poor myocardial
viability observed in the
inferoposterior basal area by
myocardial scintigraphy with99mTc-tetrofosmin
170 J Med Ultrasonics (2012) 39:169–172
123
MRI. Finally, we diagnosed the case as inferoposterior
pseudoaneurysm with a left-to-right shunt caused by
myocardial infarction based on the 2D-TTE and the 3D-
TEE findings. These findings were considered sequels of an
inferoposterior myocardial infarction, probably a few
weeks before admission. Because of the past cerebral
infarction, severe stenosis of the basilar artery, low daily
activity of the patient, and agreement with her family, we
decided to treat her conservatively. After 6-month follow-
up, the patient was still doing well.
Discussion
While pseudoaneurysms require urgent surgical resection
because of the likelihood of rupture, true aneurysms can
Fig. 3 Two-dimensional transthoracic two-chamber view of the
pseudoaneurysm. The pseudoaneurysm is located in the inferoposte-
rior basal area. LV left ventricle
Fig. 4 Two-dimensional transesophageal short axis view of the
pseudoaneurysm showed a narrow neck orifice. LV left ventricle
Fig. 5 Pulsed Doppler by 2D-TTE showed turbulent flow at the neck
of a cavity and within the cavity itself. LV left ventricle
Fig. 6 Pulsed Doppler by 2D-TEE indicated left–right shunting
through the pseudoaneurysm. LV left ventricle, RV right ventricle
Fig. 7 Three-dimensional transesophageal echocardiography show-
ing perforation at the right ventricular basal area with pseudoaneu-
rysm formation. RV right ventricle, TV tricuspid valve, IVSinterventricular septum
J Med Ultrasonics (2012) 39:169–172 171
123

often be managed medically. This stark difference makes
an accurate diagnosis of post-infarction aneurysm essential.
However, there is still no definitive method to diagnose
pseudoaneurysm [1, 2]. A potential feature proposed for
distinguishing pseudoaneurysms from true aneurysms is
location. For instance, an inferior or posterior location is
suggestive of pseudoaneurysm instead of true aneurysm
[1, 2, 4]. Furthermore, a right coronary culprit and an in-
feroposterior basal aneurysm may indicate pseudoaneu-
rysm rather than true aneurysm in the patient.
In multiple reports, a post-infarction aneurysm with a
narrow orifice has been suggestive of a pseudoaneurysm [5,
6], although Yeo et al. [3] reported that a large number of
post-infarction pseudoaneurysms had a wide neck. In the
present case, 2D-TTE and 2D-TEE showed an aneurysm
with a narrow orifice in the inferoposterior basal area;
therefore, we believed that the post-infarction aneurysm
was a pseudoaneurysm. Loperfido et al. [7] reported that
the presence of turbulent flow by pulsed Doppler at the
neck of a cavity or within the cavity itself suggested a
pseudoaneurysm. Accordingly, in the present case, pulsed
Doppler by 2D-TTE and 2D-TEE showed turbulent flow at
the neck of a cavity and within the cavity itself. As a result,
we diagnosed the pseudoaneurysm by the aforesaid echo-
cardiographical features using only 2D-TTE and 2D-TEE.
However, we could not understand the precise anatomical
relationship between the pseudoaneurysm and both ven-
tricles using only these methods. Therefore, we diagnosed
posterior-septal pseudoaneurysm with a left-to-right shunt
caused by inferior acute myocardial infarction using 3D-
TEE. This approach provided sufficient anatomical evalu-
ation of the orifice in the perforated RV and a color jet
through the orifice from the LV to the RV.
The diagnosis of LV pseudoaneurysm was based on
typical morphologic features shown by each imaging
modality, including angiography [8], CT [9], and MRI [10].
There have been a few cases of LV pseudoaneurysm with a
left-to-right shunt reported, but the efficacy of 3D-TEE to
diagnose pseudoaneurysm with a left-to-right shunt has not
been documented yet [11]. As in the present case, it is
useful to perform 3D-TEE to diagnose a pseudoaneurysm
without cardiac CT or cardiac MRI when the patient cannot
abide by our instructions and control their respiration.
Conclusion
We diagnosed LV pseudoaneurysm with a left-to-right
shunt caused by myocardial infarction using 3D-TEE. Our
approach provided sufficient anatomical evaluation. 3D-
TEE might be an efficient tool to diagnose LV pseudoan-
eurysm with a left-to-right shunt after myocardial
infarction.
Conflict of interest There is no financial conflict on the part of any
of the authors.
References
1. Brown SL, Gropler RJ, Harris KM. Distinguishing left ventricular
aneurysm from pseudoaneurysm. Chest. 1997;111:1403–9.
2. Yeo TC, Malouf JF, Oh JK, Seward JB. Clinical profile and
outcome in 52 patients with cardiac pseudoaneurysm. Ann Intern
Med. 1998;128:299–305.
3. Yeo TC, Malouf JF, Reeder GS, Oh JK. Clinical characteristics
and outcome in postinfarction pseudoaneurysm. Am J Cardiol.
1999;84:592–5, A8.
4. Loop FD, Effler DB, Webster JS, Groves LK. Posterior ventric-
ular aneurysms. Etiologic factors and results of surgical treat-
ment. N Engl J Med. 1973;288:237–9.
5. Gatewood RP Jr, Nanda NC. Differentiation of left ventricular
pseudoaneurysm from true aneurysm with two dimensional
echocardiography. Am J Cardiol. 1980;46:869–70.
6. Catherwood E, Mintz GS, Kotler MN, Parry WR, Segal BL. Two-
dimensional echocardiographic recognition of left ventricular
pseudoaneurysm. Circulation. 1980;62:294–303.
7. Loperfido F, Pennestrı̀ F, Mazzari M, Biasucci LM, Vigna C,
Laurenzi F, Manzoli U. Diagnosis of left ventricular pseudoan-
eurysm by pulsed Doppler echocardiography. Am Heart J.
1985;110:1291–3.
8. Spindola-Franco H, Kronacher N. Pseudoaneurysm of the left
ventricle. Radiographic and angiocardiographic diagnosis. Radi-
ology. 1978;127:29–34.
9. Lipiec P, Chrzanowski Ł, Kasprzak JD. Post-myocardial infarc-
tion biventricular pseudoaneurysm with bidirectional shunt.
Heart. 2010;96:483–4.
10. Konen E, Merchant N, Gutierrez C, Provost Y, Mickleborough L,
Paul NS, Butany J. True versus false left ventricular aneurysm:
differentiation with MR imaging-initial experience. Radiology.
2005;236:65–70.
11. Schreurs M, Herregods MC, Bogaert J, Troost E, Budts W.
Pseudoaneurysm of the left ventricle with moderate left-to-right
shunt. Int J Cardiol. 2008;130:11–3.
Fig. 8 Three-dimensional transesophageal echocardiography demon-
strating a color jet through the orifice of the right ventricle indicating
a left-to-right shunt. RV right ventricle, IVS interventricular septum
172 J Med Ultrasonics (2012) 39:169–172
123