psoriasis: is the impairment to a patient’s life cumulative?medf.nsu.ru/files/Влияние...
TRANSCRIPT

DOI: 10.1111/j.1468-3083.2010.03705.x JEADV
CPD PAPER
Psoriasis: is the impairment to a patient’s life cumulative?
AB Kimball,†,* U Gieler,ffi D Linder,§ F Sampogna,– RB Warren,** M Augustin†† † ffi Department of Dermatology, Harvard Medical School, Boston, MA, USA Department of Psychosomatic Medicine and Psychotherapy, Justus-Liebig-University Giessen, Giessen, Germany §Dermatology University Clinic, Padua, Italy –Istituto Dermopatico dell’Immacolata IDI-IRCCS, Rome, Italy **Dermatological Sciences, the University of Manchester, Manchester Academic Health Sciences Centre, Salford Royal Foundation Trust, Manchester, UK ††CVderm – German Center for Health Services Research in Dermatology, University Clinics of Hamburg, Hamburg, Germany *Correspondence: Dr AB Kimball. E-mail: [email protected]
Abstract Psoriasis is associated with significant physical and psychological burden affecting all facets of a patient’s life – relationships, social activities, work and emotional wellbeing. The cumulative effect of this disability may be self- perpetuating social disconnection and failure to achieve a ‘full life potential’ in some patients. Health-related quality of life studies have quantified the burden of psoriasis providing predominantly cross-sectional data and point-in-time images of patients’ lives rather than assessing the possible cumulative disability over a patient’s lifetime. However, social and economic outcomes indicate there are likely negative impacts that accumulate over time. To capture the cumulative effect of psoriasis and its associated co-morbidities and stigma over a patient’s life course, we propose the concept of ‘Cumulative Life Course Impairment’ (CLCI). CLCI results from an interaction between (A) the burden of stigmatization, and physical and psychological co-morbidities and (B) coping strategies and external factors. Several key aspects of the
CLCI concept are supported by data similar to that used in health-related quality of life assessments. Future research should focus on (i) establishing key components of CLCI and determining the mechanisms of impairment through longitudinal or retrospective case–control studies, and (ii) assessing factors that put patients at increased risk of developing CLCI. In the future, this concept may lead to a better understanding of the overall impact of psoriasis, help identify more vulnerable patients, and facilitate more appropriate treatment decisions or earlier referrals. To our knowledge, this is a first attempt to apply and develop concepts from ‘Life Course Epidemiology’ to psoriasis research. Received: 29 January 2010; Accepted: 23 March 2010
Keywords coping strategies, Cumulative Life Course Impairment, physical co-morbidities, psoriasis, psychological co-morbidi- ties, stigma
Conflict of interest None declared.
Funding sources The research and development of this manuscript was supported by funding from Abbott Laboratories.
Introduction Psoriasis is a chronic, inflammatory, immune-mediated, skin dis- ease, affecting approximately 1–3% of the population worldwide.1 The pathophysiology of psoriasis is complex, involving compo- nents of the innate and adaptive immune systems, genetics and the environment. This interplay of factors results in an increase in antigen presentation, and the activation of T-helper cell type 1 (TH1) and the more recently identified T-helper cell type 17 (TH17), resulting in what we recognize as typical cutaneous pla-
ques of psoriasis.2,3 As a systemic inflammatory disease,4 psoriasis is associated with several serious physical co-morbidities, includ- ing psoriatic arthritis, cardiovascular disease, metabolic syndrome (ischaemic heart disease, hypertension, non-alcoholic fatty liver disease, diabetes and obesity), Crohn’s disease and other immune- related conditions (Table 1).5–16 Although psoriasis may initially occur at any time throughout a person’s life, onset can often occur early in childhood, and may be associated with co-morbidities at a young age.17,18 It is commonly
JEADV 2010, 24, 989–1004 ª 2010 The Authors Journal compilation ª 2010 European Academy of Dermatology and Venereology

990 Kimball et al.
Table 1 Co-morbidities in patients with psoriasis
Physical co-morbidities Psoriatic arthritis5,7,8 Crohn’s disease†5,7 Coronary heart disease6,11 Stroke6,16 Metabolic syndrome (ischaemic heart disease, hypertension, non-alcoholic fatty liver disease, diabetes and obesity)†9,10,12–15
Psychological co-morbidities Depression20,36,37,43,77 Anxiety43,44 Suicide ideation43,78 Alexithymia79
†Psoriasis is associated with pleiotropic susceptibility loci identified in type II diabetes and Crohn’s disease.80
associated with chronic inflammatory processes and concomitant diseases. Physical co-morbidities, such as psoriatic arthritis, Cro- hn’s disease and metabolic syndrome (Table 1), are associated with the presence of psoriasis and occur more frequently in psori- atic patients than in the general population, with subsequent effects on morbidity and mortality.25 The relationship between psoriasis and co-morbidities is linked to the underlying chronic inflammatory nature of psoriasis itself,4 whereby increased levels of proinflammatory factors central to psoriasis pathogenesis inter- act with molecular mechanisms involved in other conditions (e.g. the dysregulation of metabolic function).26 Both independently and through the inflammatory process, physical co-morbidities add to the cumulative impairment over a patient’s lifetime poten- tially contributing to the worsening of psoriasis and enhancing, as a consequence, poor psychological and social outcomes.
Stigma recognized that the stigma associated with visible skin lesions, cre- ates a strong psychological burden affecting multiple facets of a patient’s life including relationships, social activities, work and emotional wellbeing.19,20 Furthermore, difficulties in coping with life circumstances and key life events may worsen the psychologi- cal, social and physical effects of psoriasis. Thus, patients with poorly managed psoriasis may follow a different or diminished life course compared with what they might have expected had they not had the condition. Several health-related quality-of-life (HRQoL) studies have quantified the burden of psoriasis on a patient’s life, producing cross-sectional data in the domains of physical, psychological, social and economic functioning.21–24 However, the cross-sectional data gained in HRQoL surveys typi- cally provide point-in-time snapshot perspectives or short-term responses to therapy and do not assess possible additive and ⁄ or cumulative physical, psychological and social damage over time. Thus, there are gaps in our understanding of the various factors that interact to cause long-term impairment. In this article, we propose a new term, ‘Cumulative Life Course Impairment’ (CLCI), intended to capture the overall effect of pso- riasis over a patient’s life course, considering the associated clinical and psychological implications that result in an altered or impaired life potential. CLCI will be defined on the basis of the currently available evidence that psoriasis has a cumulative impact on a patient’s life course, which is not detected by the measure of HRQoL at a specific time point. The concept of CLCI presented in this article, along with the currently available evidence to support it, is the result of a steering committee of international experts in the fields of dermatology, psychology and psychometric medicine.
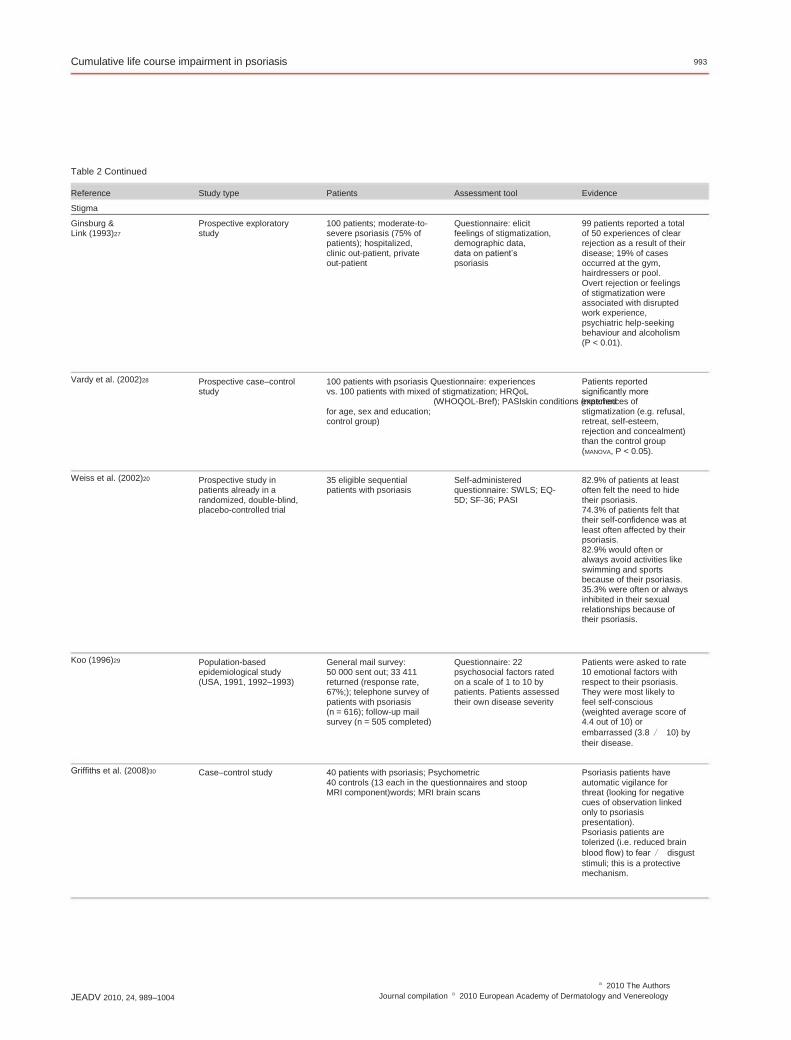
Stigmatization in psoriasis has been reported in prospective cross- sectional surveys or case–control studies, the majority of which have employed validated questionnaires for data collection (Table 2).20,27–31 Results from these studies show that, because of the visibility of psoriatic lesions, patients with psoriasis commonly experience social stigmatization and overt public rejection, such as being asked to leave public places.27 It has been reported that these experiences are more common with psoriasis than with other skin conditions.28 These rejection experiences not only lead to feelings of being stigmatized, but also result in greater sensitivity to the attitudes of others and further anticipation of rejection,27 which is also more evident in psoriasis than in other dermatological disor- ders.32,33 Recent data have shown that patients with psoriasis have an automatic vigilance for threat.30 Either overt rejection or feelings of stigmatization can have a profound effect on self-confidence, self-image and sense of wellbe- ing.20 Feelings of embarrassment, shame or lack of self-confidence can result in avoidance of public places or situations where skin is exposed, thus reducing social and even employment opportunities and inhibiting relationships with others.20,34 In particular, sexual relationships can be impaired, and problems can exist even after large improvements in, or complete clearance of, disease.35 Overall, these data provide good evidence for both real and per- ceived stigmatization in patients with psoriasis, and suggest that this can alter patients’ self-perception, self-confidence and thus behaviour. The long-term impact of these feelings or avoidance behaviours has yet to be explored; however, it is plausible that it may contribute to an impairment of a patient’s life course.
Psychological co-morbidities The evidence
Physical co-morbidities The physical aspects of psoriasis, such as symptoms, especially itching, caused by the disease, are important components of the disease burden on a patient’s life. Moreover, psoriasis is often
Data evaluating the effects of psoriasis on mental wellbeing have been generated in prospective, cross-sectional, epidemiological phone or internet surveys, prospective clinical surveys, and large (n = 581–5687) retrospective studies (Table 2).12,20,36–42 Patient records and questionnaires, many of which are well recognized
JEADV 2010, 24, 989–1004 ª 2010 The Authors Journal compilation ª 2010 European Academy of Dermatology and Venereology

Cumulative life course impairment in psoriasis 991
Table 2 Evidence for Cumulative Life Course Impairment
Reference
Finlay & Coles (1995)58
Study type
Survey of patients admitted for in-patient care (1992–1993)
Patients
369 patients with severe psoriasis
Assessment tool
Questionnaire: 6 questions on history; 15 questions comprising PDI; question comparing skin disease to other conditions; 4 questions to determine value placed on skin condition
Evidence
Of 150 patients currently working, 59.3% had lost a mean of 26 days from work during the preceding year because of their psoriasis. Of the 180 patients not working, 33.9% attributed this to their psoriasis.
Participants had missed 6.6% (±15.4%) of their working time within the past 4 weeks because of health problems. Mean productivity loss because of presenteeism of 7.6% (±9.1%).
3–5% of patients reported that psoriasis prevented them from getting a job.
1.3% of 79 patients not working, were out of work because of their psoriasis. 3.9% of respondents changed their job because of their psoriasis 24.3% of patients had a reduction in their earning capacity because of their psoriasis. 4.4% had gone into early retirement because of their psoriasis. Moderate-to-severe psoriasis resulted in a mean annual productivity loss of € 1310. 57 patients (31.0%) reported inactive periods resulting from sick leave because of their psoriasis, the average duration of which was 46.4 days (range: 1–90 days). The mean number of sick leave days was 14.1 days.
Social and economic outcomes
Schmitt & Ford (2006)59
Cross-sectional study of adults recruited via the internet (2005, USA)
WLQ; DLQI; SAPASI201 patients aged ‡18 years with self-reported psoriasis
Krueger et al. (2001)19 Mail survey followed by a telephone survey of patients with severe psoriasis (1998)
Sohn et al. (2006)61 Retrospective analysis of cost- of-illness study
502 patients with severe psoriasis
4-page self-administered questionnaire (reflects patients perceptions and experiences)
Assessment of direct and indirect costs; PASI; PBSA; PGA; SF-36 (German); DLQI (German)
184 out-patients
JEADV 2010, 24, 989–1004 ª 2010 The Authors Journal compilation ª 2010 European Academy of Dermatology and Venereology

992 Kimball et al.
Table 2 Continued
Reference Horn et al. (2007) 60
Study type Six surveys of NPF database (2003–2005)
Patients Assessment tool Evidence Probability of low income (<$30 000) was significantly greater among patients with severe disease than those with mild disease (P = 0.0002). Patients with severe disease had lower probability of working full time than patients with mild psoriasis (ns). Significantly more patients with severe psoriasis (17%) vs. mild (6%) disease reported that psoriasis was the reason for not working (P = 0.01).
The ratio of divorced ⁄ married in patients with psoriasis was 1335 ⁄ 12 619 (10.6%), n = 22 828. The negative impact on relationships was similar to that in other chronic conditions.
35.5–71.3% of patients (depending on the questionnaire used) reported having sexual problems related to their psoriasis.
70% of respondents stated that the treatment of their relative or partner resulted in them having to spend extra time on housework. 57% described psychological pressures (anxiety, being upset and being worried about the patient’s future). 55% described social disruption attributable to lack of social confidence either because of embarrassment or because of the time required for care duties. 44% described limitations to holiday plans, sport and leisure activities, and evenings out. 37% described limitations on their daily activities such as shopping, work and time spent with other family members. 37% felt that their close relationships had deteriorated.
601 patients with psoriasis Information was obtained who responded to income on household income, employment status, reasonquestions for not working, and negative effect of psoriasis on the job
Frangos & Kimball (2008)62
Survey of the RPDR 22 828 patients with psoriasis
Assessed divorced ⁄ marriage ratio
Sampogna et al. (2007)35
Prospective study in a dermatological hospital (2000–2002)
936 patients with psoriasis Questionnaires and items concerning sexual life: Skindex-29 item 29; DLQI item 9; IPSO item 6; PASI; SAPASI; GHQ-12
63 relatives and partners of patients with psoriasis
Qualitative interviews or postal questions; PASI; DLQI; PDI
Eghlileb et al. (2007)63
Postal and interview survey
JEADV 2010, 24, 989–1004 ª 2010 The Authors Journal compilation ª 2010 European Academy of Dermatology and Venereology
Cumulative life course impairment in psoriasis 993
Table 2 Continued
Reference Stigma Ginsburg & Link (1993)27
Prospective exploratory study
100 patients; moderate-to- severe psoriasis (75% of patients); hospitalized, clinic out-patient, private out-patient
Questionnaire: elicit feelings of stigmatization, demographic data, data on patient’s psoriasis
99 patients reported a total of 50 experiences of clear rejection as a result of their disease; 19% of cases occurred at the gym, hairdressers or pool. Overt rejection or feelings of stigmatization were associated with disrupted work experience, psychiatric help-seeking behaviour and alcoholism (P < 0.01).
Patients reported significantly more experiences of stigmatization (e.g. refusal, retreat, self-esteem, rejection and concealment) than the control group (MANOVA, P < 0.05).
82.9% of patients at least often felt the need to hide their psoriasis. 74.3% of patients felt that their self-confidence was at least often affected by their psoriasis. 82.9% would often or always avoid activities like swimming and sports because of their psoriasis. 35.3% were often or always inhibited in their sexual relationships because of their psoriasis.
Patients were asked to rate 10 emotional factors with respect to their psoriasis. They were most likely to feel self-conscious (weighted average score of 4.4 out of 10) or embarrassed (3.8 ⁄ 10) by their disease.
Psoriasis patients have automatic vigilance for threat (looking for negative cues of observation linked only to psoriasis presentation). Psoriasis patients are tolerized (i.e. reduced brain blood flow) to fear ⁄ disgust stimuli; this is a protective mechanism.
Study type Patients Assessment tool Evidence
Vardy et al. (2002)28 Prospective case–control study
100 patients with psoriasis Questionnaire: experiences vs. 100 patients with mixed of stigmatization; HRQoL (WHOQOL-Bref); PASIskin conditions (matched for age, sex and education; control group)
Weiss et al. (2002)20 Prospective study in patients already in a randomized, double-blind, placebo-controlled trial
35 eligible sequential patients with psoriasis
Self-administered questionnaire: SWLS; EQ- 5D; SF-36; PASI
Koo (1996)29 Population-based epidemiological study (USA, 1991, 1992–1993)
General mail survey: 50 000 sent out; 33 411 returned (response rate, 67%;); telephone survey of patients with psoriasis (n = 616); follow-up mail survey (n = 505 completed)
Questionnaire: 22 psychosocial factors rated on a scale of 1 to 10 by patients. Patients assessed their own disease severity
Griffiths et al. (2008)30 Case–control study 40 patients with psoriasis; Psychometric 40 controls (13 each in the questionnaires and stoop MRI component)words; MRI brain scans
JEADV 2010, 24, 989–1004 ª 2010 The Authors Journal compilation ª 2010 European Academy of Dermatology and Venereology

994 Kimball et al.
Table 2 Continued
Reference Schmid-Ott et al. (2005)31
Study type 1-year prospective follow-up
Patients 347 patients with psoriasis
Assessment tool PASI, SPASI, QES
Evidence Improvement in skin condition did not correlate with feeling less stigmatized in women over 1 year, suggesting a considerable influence of other psychological variables such as coping skills
Psychological co-morbidity Lynde et al. (2009)36 500 patients withNationwide telephone
moderate-to-severesurvey (SKIN, 2007, Canada); 5093 households psoriasis contacted
17% of psoriasis patientsQuestions modelled after those of the 2001 National reported having depression. Psoriasis Foundation’s Benchmark Survey on Psoriasis and Psoriatic Arthritis
Skindex 16; DLQI; Self-reported disease severity;
Self-administered questionnaire: SWLS; EQ-5D; SF-36; PASI
CRSD; self-rated indices of psoriasis severity
30% of psoriasis patients reported having depression. 22% of psoriasis patients reported having anxiety.
8 patients (22.9%) stated that they had been previously diagnosed with depression.
9.7% of patients reported a wish to be dead. 5.5% reported active suicidal ideation. Death wish and suicidal ideation were associated with higher depression scores (P < 0.0001) and higher patient self-ratings of psoriasis severity (P < 0.05).
Over one-quarter of the psoriatic patients were heavy drinkers. 25 patients with psoriasis (19%) drank more than 50 units ⁄ week; five showed features of dependency.
1918 deaths were observed in contrast to the 1211 deaths expected on the basis of the national mortality rates. Excess mortality was high for all causes of death directly related to alcohol; the SMR for men was 4.46 (95% CI, 3.60–5.45); for women, 5.60 (95% CI, 2.98–8.65).
Waters et al. (2009)37 Internet survey (Psoriasis1006 self-identified Patient Study Project, 2008) psoriasis patients
Weiss et al. (2002)20 Prospective study in patients already in a randomized, double-blind, placebo-controlled trial
35 eligible sequential patients with psoriasis
Gupta & Schork (1993)38 217 patients withSurvey of consecutive psoriasispatients attending Dept. Dermatology, University of Michigan
Higgins et al. (1993)39 Survey (Kings College Hospital)
130 patients with psoriasis Information on smoking history and drinkingControl groups (222 patients attending general habits obtained skin clinic; 42 patients with atopic eczema)
Poikolainen et al. (1999)40
Retrospective survey of patient records (1973–1984)
3132 men and 2555 women admitted to inpatient treatment with psoriasis as the principal diagnosis
Deaths were identified and underlying causes determined based on official death certificates coded according to the Finnish modification of the International Classification of Diseases, Eighth Revision and Ninth Revision and obtained from Statistics Finland
Sommer et al. (2006)12 Retrospective cohort study (Germany)
581 hospitalized patients with chronic plaque psoriasis
Data recorded on patient’s Increased alcohol chartsconsumption was seen twice as frequently in patients with moderate-to- severe psoriasis than in hospital-based controls.
JEADV 2010, 24, 989–1004 ª 2010 The Authors Journal compilation ª 2010 European Academy of Dermatology and Venereology

Cumulative life course impairment in psoriasis 995
Table 2 Continued
Reference Kirby et al. (2008) 41
Study type Prospective study of patients attending a psoriasis specialty outpatient clinic
Patients 95 patients with psoriasis
Assessment tool PDI, HADS, PSWQ, HSS, MAST
Evidence 17–30% of patients had difficulties with alcohol. 13% and 18% of patients believed they had a current or past drinking problem, respectively. There was a correlation between levels of anxiety ⁄ depression and weekly alcohol consumption (r = 0.29, P < 0.01 and r = 0.24, P = 0.03, respectively). Patients who believed that they had an alcohol problem had higher levels of anxiety (P = 0.03), depression (P < 0.01) and psoriasis-associated disability (P = 0.04).
Prevalence of psoriasis was 15%. Tobin et al. (2009)81 Survey of consecutive patients for hepatology outpatient clinics
Prospective study of patients attending outpatient clinics
100 patients with proven alcoholic liver disease
Questionnaire assessing history of psoriasis; full skin examination and PASI where relevant
GHQ-12 Sampogna et al. (2004)42
Patients with skin conditions including 936 patients with psoriasis
General mail survey: 50 000 sent out; 33 411 returned (response rate, 67%); telephone survey of patients with psoriasis (n = 616); follow-up mail survey (n = 505 completed)
72 patients with psoriasis
48% of patients had probable depression or anxiety.
Coping Koo (1996)29 Population-based
epidemiological study (USA, 1991, 1992–1993)
Questionnaire: 22 psychosocial factors rated on a scale of 1 to 10 by patients; Patients assessed their own disease severity
Patients commonly felt helpless because of their disease (weighted score of 3.9 out of 10).
Fortune et al. (2004)82
Prospective study evaluating patients before and after PUVA therapy
PDI; PLSI; HADS; PSWQ; Illness Perception Questionnaire; COPE; PASI
Medical management of disease significantly reduced disease- related disability (mean difference ± SEM: 8.01 ± 1.05, P = 0.01) and stress (mean difference ± SEM: 4.47 ± 0.92, P = 0.015).
The personality trait neuroticism was associated with the following coping strategies: an increased use of hostile reaction, escapist fantasy, self-blame, sedation, withdrawal, wishful thinking, passivity and indecisiveness (P < 0.05 to P < 0.001). Extraversion was associated with rational action, positive thinking, substitution and restraint (P < 0.05 to P < 0.001). Open individuals use humour and closed individuals use faith when dealing with stress (P < 0.01 to P < 0.001).
McCrae & Costa (2006)68
Two studies in a community sample
Adults without psoriasis (n = 255 and 151)
Study 1: Checklist of life events Study 2: Questionnaire: coping with harm and loss; coping with threat; coping with challenge
JEADV 2010, 24, 989–1004 ª 2010 The Authors Journal compilation ª 2010 European Academy of Dermatology and Venereology

996 Kimball et al.
Table 2 Continued
Reference Hill & Kennedy (2002) 73
Study type Patients Assessment tool PDI; PLSI; HADS; COPE scale
Evidence Maladaptive coping strategies (venting emotions and mental disengagement) were significantly associated with subjective disability and psychological distress, accounting for a greater proportion of variance than age, gender or duration of disease.
89 people withCross-sectional postal psoriasissurvey of hospital outpatients and patients in a support group
Scharloo et al. (2000)69 Longitudinal study (two measures one year apart)
69 patients with psoriasis
Initial higher levels ofMedical perceptions perceived control andquestionnaire; SF-20; HADS; Utrecht Coping List; curability of illness, and more perceived symptomsBody Surface Scores were associated with greater future utilization of outpatient services. Higher initial use of coping characterized by the expression of emotions was associated with a lower number of different prescribed therapies. Initial high scores on the perception that the disease has disabling consequences were associated with more negative perceived health 1 year later. High scores on passive coping were associated with worse physical functioning at 12 months. There was strong correlation between passive coping and avoidant coping (r = 0.54, P < 0.001).
PASI, questionnaires (perceptions of how well patient was dealing with their illness, life quality, sense of coherence, and critical life events)
Patients with a low sense of cohesion suffered their first relapse 3.5 months after therapy, whereas patients with a high sense of cohesion had a first relapse after 10 months.
Kupfer et al. (2003)70 Ward-based rehabilitation study and follow-up postal questionnaires
72 patients
COPE, coping orientation of problem experience; CRSD, Carroll rating scale for depression; DLQI, Dermatology Life Quality Index; EQ-5D, Euro-QoL 5D; GHQ-12, General Health Questionnaire 12; HADS, Hospital Anxiety Depression Scale; HRQoL, health-related quality of life; HSS, health screening survey revised; IPSO, Impact of Psoriasis on Quality of Life Questionnaire; MANOVA, multivariate analysis of variance; MAST, Michigan alcohol screening test; MRI, magnetic resonance imaging; NPF, National Psoriasis Foundation; ns, not significant; PASI, Psoriasis Assessment Severity Index; PBSA, psoriatic body surface area; PDI, Psoriasis Disability Index; PGA, physician’s global assessment; PLSI, Psoriasis Life Stress Inventory; PSWQ, Penn State Worry Questionnaire; PUVA, psoralen plus ultraviolet A; QES, Questionnaire on experience with skin complaints; RPDR, Research Patient Database Registry; SAPASI, self-administered PASI; SEM, standard error of the mean; SF-36, Medical Outcomes Study Short Form 36; SMR, standardized mortality ratio; SWLS, satisfaction with life scale; WHOQOL-Bref, World health Organisation Quality of Life; WLQ, Work Limitations Questionnaire.
and have been previously validated, were used in data collection. Results show that patients with psoriasis have increased rates of depression, which occurs in up to 30% of patients irrespective of disease severity,20,36,37 anxiety, reported in over one-third of patients,43,44 and suicide ideation, evident in up to 10% of patients.38 Furthermore, the incidence of both depression and
anxiety increase with increasing disease severity, with, for example, almost half of those with moderate-to-severe disease reporting depression related to their psoriasis.20,36,37 Furthermore, there is increasing evidence that the inflammatory processes may be directly linked to some psychological conditions, such as major depression, with patients exhibiting increased
JEADV 2010, 24, 989–1004 ª 2010 The Authors Journal compilation ª 2010 European Academy of Dermatology and Venereology

Cumulative life course impairment in psoriasis 997
peripheral blood inflammatory biomarkers, which are known to access the brain and interact with pathophysiological pathways involved in depression.45 Conversely, increased psychological dis- tress may trigger or further aggravate the manifestation of psoria- sis through disturbances in the dynamic equilibrium established between the nervous, endocrine and immune systems.46–50 Recent work has shown that acute experimental social stress is associated with a reduction in frequency of epidermal Langerhans cells, which is accompanied by altered expression of cutaneous neuro- peptides, supporting the concept of a connection between the brain and the skin (brain-skin axis).48 Psychological distress in patients with psoriasis may also lead to behavioural changes, such as increased social phobia, alcoholism and non-adherence to treatment,51 some of which may further exacerbate skin disease or even increase the risk of death.40 In par- ticular, there is good evidence for a higher incidence of alcoholism in patients with psoriasis than in the general public, which is known to increase in relation to the severity of disease.12,39,40,52 Problems with alcohol have been further correlated with the pres- ence of anxiety and depression in psoriatic patients.41 This may be a result of emotional reactions, whereby patients with psoriasis seem to have a lower anger reaction than healthy controls.53 In summary, we have good evidence for a high prevalence of psychological co-morbidities in patients with psoriasis. Neverthe- less, there are no longitudinal data tracking the long-term impact of these co-morbidities.
Life course epidemiology: Cumulative Life Course Impairment and modulating factors
For decades, Life Course Research has been predominantly a sub- ject of studies for sociology and related fields.54 Nevertheless, recently the study of health and health impairment over the life course has appeared as an emerging topic54 and articles on life course epidemiology, especially with regard to chronic diseases, are increasingly being published.55,56 To the authors’ best knowl- edge, however, no specific research has been performed on life course of psoriasis patients. As we have shown, we have evidence, predominantly from cross-sectional studies, indicating that patients with psoriasis are vulnerable to stigmatization and are at increased risk for psycho- logical co-morbidities. However, without longitudinal data we currently cannot empirically demonstrate the cumulative impair- ment associated with these factors over a patient’s lifetime. How- ever, patient cases, such as the personal experience of Ray Jobling having lived with psoriasis for 50 years, provide some information about the long-term effects of disease.57 In addition, evidence of social and economic outcomes is sug- gestive of a cumulative negative impact over time. Economically, patients with psoriasis can have difficulties gaining and retaining paid employment or working to their full potential, which may limit their lifetime earning potential19,58–61 and can result in socie- tal cost associated with productivity loss.61 In one study in the
United States, data from the National Psoriasis Foundation data- base demonstrated that the probability of a low income (<US$30 000) was significantly greater among patients with severe disease than among those with mild psoriasis (P = 0.0002).60 However, the effects of psoriasis on income may vary from coun- try-to-country. It must also be conceded that low income may lead to behaviours (such as unhealthy alimentary habits and poor com- pliance) that further exacerbate disease and poor socioeconomic outcomes. In addition, at the social level, psoriasis affects close relationships causing psychological pressures and disrupting family social activities, potentially resulting in higher divorce rates.62,63 The negative impact of psoriasis on relationships is similar to that of other chronic conditions,62 with relatives of patients reporting social disruption (55%), limitations to holiday plans and leisure activities (44%), and deterioration of close relationships (37%).63 We propose the concept of CLCI to indicate the cumulative life-long effects of physical co-morbidities, stigma and psychologi- cal co-morbidities, and the economic and social consequences, which have the potential to place each psoriasis patient at risk of not living their life to their full potential. It is important to recog- nize at risk patients and to assess or measure their risk of a dam- aged life course (although more work is required to define these measures). The core components of CLCI are summarized in Table 3. CLCI is the result of stigmatization, and physical and psy- chological co-morbidities, together with coping strategies and external factors, such as social support, that appear to have a potential moderating effect. In patients with ineffective coping strategies and limited social support even a small burden may be overwhelming, resulting in significant impairment. This effect may be less exaggerated in patients with highly effective coping strategies and strong social support networks, even if the burden of severity is large. The interaction of key interpersonal aspects in CLCI, such as coping strategies in relation to physical co-morbidi- ties, stigmatization and psychological co-morbidities is schemati- cally represented in Fig. 1. Support for the role of coping as one of the key moderating components in CLCI can be found in the literature for chronic ill- ness, which suggests that outcomes are influenced by patients’ individual coping styles (i.e. how they confront their illness)64,65 along with their beliefs about: (i) the labels and symptoms describing their illness (identity); (ii) aetiology (causes); (iii) the effects and outcome of illness (consequences); (iv) the duration of disease (timelines); and (v) how they can control or recover from illness (controllability ⁄ cure).64–67 This effect is further influenced by a person’s personality.68 In patients with psoriasis, Scharloo et al. demonstrated that coping strategies and illness perceptions accounted for the observed variance in health outcomes, with patients with higher levels of perceived control and curability of illness and greater expression of emotion having better health out- comes over the course of a year than those engaging in passive and avoidant coping behaviours (Table 2).69 In addition, in a 1-year follow-up study, Kupfer et al. demonstrated that the time
JEADV 2010, 24, 989–1004 ª 2010 The Authors Journal compilation ª 2010 European Academy of Dermatology and Venereology

998 Kimball et al.
Table 3 Core components of Cumulative Life Course Impairment
Physical co-morbidities
Psoriatic arthritis
Cardiovascular disease
Metabolic syndrome (ischaemic heart disease, hypertension, diabetes, obesity)
Crohn’s disease
Other immune-related conditions
Stigma
Skin damage (perception) Overt public rejection Other rejecting behaviours
Psychological co-morbidities Anxiety
Social phobia
Depression
Social support
Family
Friends
Colleagues
Coping
Maladaptive coping (continued avoidance) Limited activity (skin damage) Mental disengagement
Self-image
Body image Self-confidence
Suicide ideation
Alexithymia Addiction (smoking, alcohol)
Patient support groups
Healthcare professionals
Denial Minimization Sense of coherence Helplessness Family factors
Less vulnerable to CLCI More vulnerable to CLCI
Psychological co-morbidities
Stigma
Coping Physicalco-morbidities co- morbidities
Psychological Co pin
g Stigma
Physical co-morbidities
Personality Personality
Figure 1 Interaction of key intrapersonal components that make patients more or less vulnerable to Cumulative Life Course Impairment.
to relapse despite treatment was longer in psoriasis patients who had a high sense of coherence than in those with a low sense of cohesion.70 Furthermore, cognitive-behavioural therapy in addi- tion to standard treatment has been shown to modify patient’s perceptions of illness and reduce psychological distress, thereby improving disease severity.71,72 Further evidence that maladaptive coping strategies can increase distress and disability was presented by Hill & Kennedy, who examined the role of coping strategies in 89 patients with psoriasis in a cross-sectional postal survey. They found that maladaptive coping strategies, in particular venting emotions and mental disengagement, were significantly associated with subjective disability and psychological distress, accounting for a greater proportion of the variance than age, gender or duration of disease (Table 2).73 However, coping strategies that work in the short term may be counterproductive over the long term.68 For example, avoidance of certain social situations may alleviate immediate distress and
anxiety but if continued can result in social disconnection. Avoid- ance can also lead to decreased adherence to therapy allowing psoriasis severity to worsen.30 Moreover, throughout a person’s lifetime, the cumulative demands that psoriasis places on that individual may potentially exhaust their coping mechanisms, resulting in significant impairment. Thus, how a patient copes with psoriasis at any time point, along with their social environment, are likely key factors in deter- mining outcomes. The interaction between the various compo- nents will change throughout an individual’s life putting a person more or less at risk of cumulative impairment. Thus, at some time points a patient may perform well (e.g. at year 10 on Fig. 2), whereas at others s ⁄ he may be performing poorly (e.g. at year 6 on Fig. 2). To accurately assess a patient’s long-term or cumulative impairment we must assess each of the key contributors, e.g. the nature of their stigmatization and physical and psychological co- morbidities, along with the impact of their coping strategies and
JEADV 2010, 24, 989–1004 ª 2010 The Authors Journal compilation ª 2010 European Academy of Dermatology and Venereology

Cumulative life course impairment in psoriasis 999
140 Physical co-morbidity
120
100
CLCI score
Psychological co-morbidity Stigma Total CLCI score
Point at which person is at risk of CLCI
80
60
40
20
1 2 3 4 5 Years
6 7 8 9 10
Figure 2 Hypothetical impairment over a patient’s life course.
external factors (e.g. support networks), over time (represented by the bars on Fig. 2). The overall effect on a patients’ life course is cumulative and might be visualized by an accumulation of the yearly impact of each of these components (as shown by the line in Fig. 2). Thus, even at a timepoint when an individual is per- forming well (according to individual component measures), putting them at less risk of CLCI at that point, she ⁄ he may still have significant life course impairment as a result of the cumula- tive impact of past events.
Discussion Currently available assessments of the impact of psoriasis on patients are designed to provide a point-in-time measure [e.g. last week for Dermatology Life Quality Index (DLQI)]. There is inter- est in developing a concept and a tool that may help physicians understand the impact over a longer period of time and to iden- tify features of patients particularly at risk of developing CLCI (provided of course that such features exist). The assessment of a patient’s CLCI would require a prospective longitudinal assess- ment in newly diagnosed patients, together with a retrospective historical record of disease, psychological state, and key life events. Several key aspects of the CLCI concept are currently supported by data that have been used to support the argument for reduced HRQoL in patients with psoriasis (Table 2). These data are largely from retrospective cross-sectional studies, that vary considerably in terms of study design, patient numbers investigated (n = 35 to approximately n = 23 000), and data collection methods (non- validated vs. validated generic or disease-specific instruments). Although there is well-established support for key components of CLCI, such as stigmatization, and physical and psychological co- morbidities, longitudinal data supporting the existence and cumu- lative nature of psoriasis-originated life course impairment, includ- ing the ongoing interaction between components, are not currently
available. A systematic review of the literature with predetermined inclusion and exclusion criteria is required to critically evaluate the available data and determine the precise data gaps that currently exist. We suggest that there is probably also a need to develop and validate a new assessment tool (such as a ‘course of life’ question- naire for psoriasis patients), most likely starting from existing tools, to meaningfully assess CLCI. Analogous research has been per- formed and published for vitiligo, cancer and atopic dermatitis using a validated ‘course of life’ questionnaire, in which achieve- ment of developmental milestones is assessed retrospectively.74 Future research into CLCI should be focused on establishing key components of CLCI and determining the mechanisms of impairment through longitudinal studies or retrospective case– control studies, along with the development of tools to assess fac- tors that put patients more at risk of developing CLCI. As a first step, we need to identify individuals whose life has been impaired and understand the key contributors to this impairment. Once this has been established, we can begin to assess patients effectively for cumulative life impairment and its key components, which might include, for example, prolonged periods of stigmatization or reduced coping ability. A mathematical modelling approach, analogous to the one used to describe the concept of allostatic load as a cumulative biological risk,75 may be worth considering. Research can here be performed in two ways. (1) One may con- sider the cumulative psychological and physical ‘load’ derived from the ongoing chronic inflammatory disease and attempt to infer the risk for a ‘crippled’ life course. (2) It may be interesting to investigate whether ongoing ‘stress’ and other psychological and possibly metabolic burdens accumulated over time may not facilitate the onset of psoriasis. Indeed, at least for another inflam- matory disease – adult onset arthritis – a cumulative effect of stress factors leading to a cumulative ‘allostatic load’ seems to influence the risk of contracting the disease later in life.76
JEADV 2010, 24, 989–1004 ª 2010 The Authors Journal compilation ª 2010 European Academy of Dermatology and Venereology

1000 Kimball et al.
In conclusion, the model of CLCI strives to incorporate the multifactorial dimensions of psoriasis into a comprehensive model to describe the cumulative disease-related impairment experienced by patients throughout their lifetime. This model could support physicians in better understanding the true impact of psoriasis, potentially help the identification of key patients who may be more vulnerable to this impact, and allow physicians to make more appropriate treatment decisions earlier in the course of dis- ease and potentially prevent the progression of CLCI. Although the key components of the concept are supported by cross- sectional data, further longitudinal research is required to prove how CLCI occurs and how this might be reduced with appropriate interventions.
Acknowledgements The concept presented in this review was derived from discus- sions held during meetings of the CLCI Steering Committee, which was comprised of the following international experts: Dr Lucia Tomas Aragones, Dr Jose Manuel Carrascosa, Prof. John de Korte, Dr Marta Ferran, Dr Fukuchi, Prof. Gregor Jemec, Marita Kosmadaki, Ms Susan Maguire, Prof. Mamitaro ˜Ohtsuki, Ms Liz Parrish, Dr Javier Pedraz Munoz, Dr Franco- ise Poot, Ms Sandra Ros, Dr Jacek Szepietowski, Prof. Anna Zalewska-Janowska. We thank Susan Cheer, PhD, who pro- vided writing assistance on this manuscript. Financial support for writing assistance was supplied by Abbott Laboratories.
JEADV 2010, 24, 989–1004 ª 2010 The Authors Journal compilation ª 2010 European Academy of Dermatology and Venereology

Cumulative life course impairment in psoriasis 1001
References 1 Greaves MW, Weinstein GD. Treatment of psoriasis. N Engl J Med 1995; 332: 581–588. 2 Griffiths CE, Barker JN. Pathogenesis and clinical features of psoriasis. Lancet 2007; 370: 263–271. 3 Lowes MA, Kikuchi T, Fuentes-Duculan J et al. Psoriasis vulgaris lesions contain discrete populations of Th1 and Th17 T cells. J Invest Dermatol 2008; 128: 1207–1211. 4 Alexandroff AB, Pauriah M, Camp RDR et al. More than skin deep: atherosclerosis as a systemic manifestation of psoriasis. Br J Dermatol 2009; 161: 1–7. 5 Kimball AB, Gladman D, Gelfand JM et al. National Psoriasis Foundation clinical consensus on psoriasis comorbidities and recommendations for screening. J Am Acad Dermatol 2008; 58: 1031–1042. 6 Kimball AB, Guerin A, Mulani P, Gupta S. The risk of coronary heart disease and stroke among psoriasis patients. JAAD 2009; 60(Suppl.): AB179. 7 Najarian DJ, Gottlieb AB. Connections between psoriasis and Crohn’s disease. J Am Acad Dermatol 2003; 48: 805–821. ¨¨8 Reich K, Kruger K, Mossner R, Augustin M. Epidemiology and clinical pattern of psoriatic arthritis in Germany: a prospective interdisciplinary epidemiological study of 1511 patients with plaque-type psoriasis. Br J Dermatol 2009; 160: 1040–1047. 9 Cohen AD, Sherf M, Vidavsky L et al. Association between psoriasis and the metabolic syndrome. Dermatology 2008; 216: 152–155. 10 Qureshi AA, Choi HK, Setty AR et al. Psoriasis and the risk of diabetes and hypertension: a prospective study of US female nurses. Arch Der- matol 2009; 145: 379–382. 11 Gelfand JM, Neimann AL, Shin DB et al. Risk of myocardial infarction in patients with psoriasis. JAMA 2006; 296: 1735–1741. 12 Sommer DM, Jenisch S, Suchan M et al. Increased prevalence of the metabolic syndrome in patients with moderate to severe psoriasis. Arch Dermatol Res 2006; 298: 321–328. 13 Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB, Gelfand JM. Prevalence of cardiovascular risk factors in patients with psoriasis. J Am Acad Dermatol 2006; 55: 829–835. 14 Gisondi P, Tessari G, Conti A et al. Prevalence of metabolic syndrome in patients with psoriasis: a hospital-based case–control study. Br J Der- matol 2007; 156: 68–73. 15 Gisondi P, Targher G, Zoppini G, Girolomoni G. Non-alcoholic fatty liver disease in patients with chronic plaque psoriasis. J Hepatol 2009; 51: 758–764. 16 Prodanovich S, Kirsner RS, Kravetz JD et al. Association of psoriasis with coronary artery, cerebrovascular, and peripheral vascular diseases and mortality. Arch Dermatol 2009; 145: 700–703. 17 Benoit S, Hamm H. Childhood psoriasis. Clin Dermatol 2007; 25: 555– 562. 18 Augustin M, Glaeske G, Radtke MA, Christophers E, Reich K, Schafer I. Epidemiology and comorbidity of psoriasis in children. Br J Dermatol 2010; 162: 633–636. 19 Krueger G, Koo J, Lebwohl M et al. The impact of psoriasis on quality of life. Arch Dermatol 2001; 137: 280–284. 20 Weiss SC, Kimball AB, Liewehr DJ et al. Quantifying the harmful effect of psoriasis on health-related quality of life. JAAD 2002; 47: 512–518. 21 Kimball AB, Jacobson C, Weiss S et al. The psychosocial burden of psoriasis. Am J Clin Dermatol 2005; 6: 383–392. ¨22 Augustin M, Kruger K, Radtke MA et al. Disease severity, quality of life and healthcare in plaque-type psoriasis: a multicentre, cross-sectional study in Germany. Dermatology 2008; 216: 366–372. 23 Misery L, Thomas L, Jullien D et al. Comparative study of stress and quality of life in outpatients consulting for different dermatoses in 5 aca- demic departments of dermatology. Eur J Dermatol 2008; 18: 412–415. 24 Zachariae R, Zachariae C, Ibsen H et al. Dermatology life quality index: data from Danish inpatients and outpatients. Acta Derm Venereol 2000; 80: 272–276.
25 Gulliver W. Long-term prognosis in patients with psoriasis. Br J Dermatol 2008; 159(Suppl. 2): 2–9. 26 Gottlieb AB, Chao C, Dann F. Psoriasis comorbidities. J Dermatolog Treat 2008; 19: 5–21. 27 Ginsburg IH, Link BG. Psychological consequences of rejection and stigma feelings in psoriasis patients. Int J Dermatol 1993; 32: 587–591. 28 Vardy D, Besser A, Amir M et al. Experiences of stigmatization play a role in mediating the impact of disease severity on quality of life in psoriasis patients. Br J Dermatol 2002; 147: 736–742. 29 Koo J. Population-based epidermatologic study of psoriasis with emphasis on quality of life assessment. Dermatol Clin 1996; 14: 485– 496. 30 Kleyn CE, McKie S, Ross AR et al. Diminished neural and cognitive responses to facial expressions of disgust in patients with psoriasis: a functional magnetic resonance imaging study. J Invest Dermatol 2009; 129: 2613–2619. ¨¨31 Schmid-Ott G, Kunsebeck H-W, Jager B et al. Significance of the stig- matization experience of psoriasis patients: a 1-year follow-up of the ill- ness and its psychosocial consequences in men and women. Acta Derm Venereol 2005; 85: 27–32. 32 Schmid-Ott G, Kuensebeck H-W, Jaeger B et al. Validity study for the stigmatization experience in atopic dermatitis and psoriatic patients. Acta Derm Venereol 1999; 79: 443–447. 33 Schmid-Ott G, Burchard R, Niederauer HH et al. Stigmatization and quality of life of patients with psoriasis and atopi dermatitis [Stigmati- ¨sierung und Lebensqualitat bei Patienten mit Psoriasis und Neuroderm- itis.] Der Hautarzt 2003; 54: 852–857. (paper in German). 34 Fox FE, Rumsey N, Morris N. ‘‘Ur skin is the thing that everyone sees and you can’t change it!’’: exploring the appearance-related concerns of young people with psoriasis. Dev Neurorehabil 2007; 10: 133–141. 35 Sampogna F, Gisondi P, Tabolli S et al. Impairment of sexual life in patients with psoriasis. Dermatology 2007; 214: 144–150. 36 Lynde C, Guenther L, Poulin Y. The burden of psoriasis and psoriatic arthritis in Canada: insights from the psoriasis knowledge in Canada (SKIN) survey. JAAD 2009; 60(Suppl.): AB165. 37 Waters HC, Carter CT, Piech CT et al. The impact of psoriasis on psychological functioning and quality of life. JAAD 2009; 60(Suppl.): AB183. 38 Gupta MA, Schork N. Suicidal ideation in psoriasis. Int J Dermatol 1993; 32: 188–190. 39 Higgins EM, Peters TJ, du Vivier AWP. Smoking, drinking and psoria- sis. Br J Dermatol 1993; 129: 749–750. 40 Poikolainen K, Karvonen J, Pukkala E. Excess mortality related to alcohol and smoking among hospital-treated patients with psoriasis. Arch Dermatol 1999; 35: 1490–1493. 41 Kirby B, Richards HL, Mason DL et al. Alcohol consumption and psy- chological distress in patients with psoriasis. Br J Dermatol 2008; 158: 138–140. 42 Sampogna F, Picardi A, Chren M-M et al. Association between poorer quality of life and psychiatric morbidity in patients with different dermatological conditions. Psychosom Med 2004; 66: 620–624. 43 Gupta MA, Gupta AK. Psychiatric and psychological co-morbidity in patients with dermatologic disorders: epidemiology and management. Am J Clin Dermatol 2003; 4: 833–842. 44 Langley RGB, Krueger GG, Griffiths CEM. Psoriasis: epidemiology, clinical features, and quality of life. Ann Rheum Dis 2005; 64(Suppl. 2): ii18–ii23. 45 Miller AH, Maletic V, Raison CL. Inflammation and its discontents: the role of cytokines in the pathophysiology of major depression. Biol Psychiatry 2009; 65: 732–741. 46 Arck P, Paus R. From the brain-skin connection: the neuroendocrine- immune misalliance of stress and itch. Neuroimmunomodulation 2006; 13: 347–356. 47 Saraceno R, Kleyn CE, Terenghi G, Griffiths CEM. The role of neuro- peptides in psoriasis. Br J Dermatol 2006; 155: 876–882.
JEADV 2010, 24, 989–1004 ª 2010 The Authors Journal compilation ª 2010 European Academy of Dermatology and Venereology

1002 Kimball et al.
48 Kleyn CE, Schneider L, Saraceno R et al. The effects of acute social stress on epidermal langerhans’ cell frequency and expression of cutane- ous neuropeptides. J Invest Dermatol 2008; 128: 1273–1279. ¨49 Schmid-Ott G, Jacobs R, Jager B et al. Stress induced endocrine and immunological changes in psoriasis patients and healthy controls. Psychother Psychosom 1998; 67: 37–42. 50 Schmid-Ott G, Jaeger B, Adamek C et al. Levels of circulating CD8(+) T lymphocytes, natural killer cells, and eosinophils increase upon acute psychosocial stress in patients with atopy dermatitis. J Allergy Clin Immunol 2001; 107: 171–177. 51 Schaaf H, Eipp C, Deubner R et al. [Psychosocial aspects of coping with tinnitus and psoriasis patients. A comparative study of suicidal tenden- cies, anxiety and depression.] HNO 2009; 57: 57–63. (article in German) 52 Chaput J-C, Poynard T, Naveau S et al. Psoriasis, alcohol, and liver disease. Br Med J 1985; 291: 25. 53 Niemeier V, Fritz J, Kupfer J, Gieler U. Aggressive verbal behaviour as a function of experimentally induced anger in persons with psoriasis. Eur J Dermatol 1999; 9: 555–558. 54 Mayer CU. New directions in life course research. Annu Rev Sociol 2009; 35: 413–433. 55 Ben-Shlomo Y, Kuh D. A life course approach to chronic disease epide- miology: conceptual models, empirical challenges and interdisciplinary perspectives. Int J Epidemiol 2002; 31: 285–293. 56 Lynch J, Smith GD. A life course approach to chronic disease epidemi- ology. Annu Rev Public Health 2005; 26: 1–35. 57 Jobling R. Psoriasis. Br Med J 2007; 334: 953–954. 58 Finlay AY, Coles ECl. The effect of severe psoriasis on the quality of life of 369 patients. Br J Dermatol 1995; 132: 236–244. 59 Schmitt JM, Ford DE. Work limitations and productivity loss are asso- ciated with health-related quality of life but not with clinical severity in patients with psoriasis. Dermatology 2006; 213: 102–110. 60 Horn EJ, Fox KM, Patel V et al. Association of patient-reported psoriasis severity with income and employment. JAAD 2007; 57: 963– 971. 61 Sohn S, Schoeffski O, Prinz J et al. Cost of moderate to severe plaque psoriasis in Germany: a multicenter cost-of-illness study. Dermatology 2006; 212: 137–144. 62 Frangos JE, Kimball AB. Divorce ⁄ marriage ratio in patients with psoria- sis compared to patients with other chronic medical conditions. J Invest Dermatol 2008; 128(Suppl. 1): S87. 63 Eghlileb AM, Davies EEG, Finlay AY. Psoriasis has a major secondary impact on the lives of family members and partners. Br J Dermatol 2007; 156: 1245–1250. 64 Scharloo M, Kaptein AA, Weinman J et al. Illness perceptions, coping and functioning in patients with rheumatoid arthritis, chronic obstruc- tive pulmonary disease and psoriasis. J Psychosom Res 1998; 44: 573– 585. 65 Scharloo M, Kaptein AA, Weinman JA et al. Predicting functional status in patients with rheumatoid arthritis. J Rheumatol 1999; 26: 1686–1693. 66 Hampson SE, Glasgow RE, Zeiss AM. Personal models of osteoarthritis and their relation to self-management activities and quality of life. J Behav Med 1994; 17: 143–158.
67 Petrie KJ, Weinman J, Sharpe N, Buckley J. Role of patients’ view of their illness in predicting return to work and functioning after myocardial infarction: longitudinal study. Br Med J 1996; 312: 1191–1194. 68 McCrae R, Costa PT. Personality, coping, and coping effectiveness in an adult sample. J Pers 2006; 54: 385–404. 69 Scharloo M, Kaptein AA, Weinman J et al. Patients’ illness perceptions and coping as predictors of functional status in psoriasis: a 1-year follow-up. Br J Dermatol 2000; 142: 899–907. 70 Kupfer J, Niemeier V, Brosig B et al. Sense of coherence among psoria- tics as a predictor of symptom-free time following dermatological inpa- tient therapy. Dermatol Psychosom 2003; 4: 200–206. 71 Fortune DG, Richards HL, Kirby B et al. A cognitive-behavioural symp- tom management programme as an adjunct in psoriasis therapy. Br J Dermatol 2002; 146: 458–465. 72 Fortune DG, Richards HL, Griffiths CEM et al. Targeting cognitive- behaviour therapy to patients’ implicit model of psoriasis: results from a patient preference controlled trial. Br J Clin Psychol 2004; 43: 65–83. 73 Hill L, Kennedy P. The role of coping strategies in mediating subjective disability in people who have psoriasis. Psychol Health Med 2002; 7: 261–269. 74 Brenninkmeijer EEA, Legieres CM, Sillevis Smitt JH et al. The course of life of patients with childhood atopic dermatitis. Pediatr Dermatol 2009; 26: 14–22. 75 Seeman TE, McEwen BS, Rowe JW, Singer BH. Allostatic load as a marker of cumulative biological risk: MacArthur studies of successful aging. Proc Natl Acad Sci USA 2001; 98: 4770–4775. 76 Von Korff M, Alonso J, Ormel J et al. Childhood psychosocial stressors and adult onset arthritis: broad spectrum risk factors and allostatic load. Pain 2009; 143: 76–83. 77 Esposito M, Saraceno R, Giunta A et al. An Italian study on psoriasis and depression. Dermatology 2006; 212: 123–127. 78 Gupta MA, Gupta AK. Depression and suicidal ideation in dermatology patients with acne, alopecia areata, atopic dermatitis and psoriasis. Br J Dermatol 1998; 139: 846–850. 79 Fortune DG, Richards HL, Griffiths CE, Main CJ. Psychological stress, distress and disability in patients with psoriasis: consensus and variation in the contribution of illness perceptions, coping and alexithymia. Br J Clin Psychol 2002; 41: 157–174. 80 Wolf N, Quaranta M, Prescott NJ et al. Psoriasis is associated with pleiotropic susceptibility loci identified in type II diabetes and Crohn disease. J Med Genet 2008; 45: 114–116. 81 Tobin AM, Higgins EM, Norris S, Kirby B. Prevalence of psoriasis in patients with alcoholic liver disease. Clin Exp Dermatol 2009; 34: 698– 701. 82 Fortune DG, Richards HL, Kirby B et al. Epidemiology and health services research successful treatment of psoriasis improves psoriasis- specific but not more general aspects of patients’ well-being. Br J Dermatol 2004; 151: 1219–1226.
JEADV 2010, 24, 989–1004 ª 2010 The Authors Journal compilation ª 2010 European Academy of Dermatology and Venereology

Cumulative life course impairment in psoriasis 1003
Information on authors
Alexa Boer Kimball, MD, MPH, is an Associate Professor at Harvard Medical School, and Vice Chair of the Department of Dermatology and Director of the Clinical Unit for Research Trials in Skin, Massachusetts General Hospital. She is well recognized for her work on psoriasis, physician workforce economics and out- comes research, which is widely published in peer reviewed journals.
Uwe Gieler, MD, is a Professor and Chair of Psychosomatic Medicine and Psychotherapy at the Justus- Liebig-University of Giessen, Germany. He is also Chair of the Consultation-Liaison Service at the Clinic of Psychosomatic Medicine and Psychotherapy in Germany, and Chair of the Atopic Dermatitis Educa- ¨tion Academy, Hessen-Thuringen, among other appointments. His interests are in the fields of psycho- dermatology, including the effects of psoriasis.
Dennis Linder, MD, MSc, studied Mathematics at the Swiss Federal Institute of Technology and Medi- cine at the Innsbruck Medical University where he received specialist training in Dermatology. He lec- tures at the University of Padua Medical School. He has contributed chapters to dermatological textbooks and has authored several articles for peer-reviewed dermatology journals. He is Vice-President of the International Society of Biopsychosocial Medicine, Secretary General of the European Society for Dermatology and Psychiatry (ESDaP), and Secretary General of the Italian Society for Psychosomatic Dermatology.
Francesca Sampogna, PhD, obtained a Masters degree in Genetic Epidemiology at the University Paris ¨Sud of Paris; and a PhD in Oral Public Health at the University of Malmo, Sweden. She has been work- ing for 10 years in dermatoepidemiology, with a particular interest in psoriasis. Her main areas of inter- est are: quality of life, psychosocial and psychosomatic aspects of disease, methodology in outcomes research, patient satisfaction and the patient-provider relationship.
JEADV 2010, 24, 989–1004 ª 2010 The Authors Journal compilation ª 2010 European Academy of Dermatology and Venereology

1004 Kimball et al.
Richard Warren, MD, is a Clinical Senior Lecturer and Honorary Consultant Dermatologist in Manches- ter, UK. He graduated from Liverpool University with a first class honours degree in Pharmacology and gained his Medical degree, with honours, one year later. His work in Dermatology has focussed on phar- macogenetics (forming the basis of his PhD thesis), the genetic susceptibility of psoriasis, biological ther- apies and their use in psoriasis and, more recently, co-morbidities of psoriasis.
Matthias Augustin, MD, is Professor for Health Economics and Quality of Life Research and Head of the Outpatient Clinic for Chronic Wounds, Department of Dermatology, University Clinics of Hamburg, Germany. He is also Director of the Institute for Health Services Research in Dermatology and Nursing and Chair of the Center for Dermatological Research. His research interests are in the field of health economics and outcomes research and dermatology, on which he has published more than 200 articles.
JEADV 2010, 24, 989–1004 ª 2010 The Authors Journal compilation ª 2010 European Academy of Dermatology and Venereology