pst 422: neuro disorders and rehabilitation: stroke
TRANSCRIPT

PST 422: NEUROLOGICAL
DISORDERS AND
REHABILITATION: STROKE
Instructors:
Prof MOB Olaogun
Dr. F. Adepoju

Recommended texts
• Bobath B. Adult Hemiplegia: Evaluation and Treatment (3rd ed.). Oxford: Butterworth-Heinemann, 1990.
• Carr JH, Shepherd RB. Neurological Rehabilitation: Optimizing Motor Performance. Oxford: Butterworth-Heinemann, 1998.
• O' Sullivan SB, Schmitz TJ, eds. Physical Rehabilitation: Assessment and Treatment. Philadelphia: F.A. Davis Company, 2001

• Porter S. Tidy’s Physiotherapy (13th
ed). Oxford: Butterworth-Heinemann,
2003.
• Stokes M. Physical management in
neurological rehabilitation (2nd ed.).
Edinburgh: Elsevier Mosby, 2004.

Introduction
Definition of Neurorehabilitation
Nervous System
Basic units
Divisions
Overall functions
Effects of Abnormal/Underdevelopement
Diseases and Injury/Trauma

Introduction contd
• Rehabilitation
• Procedure in neurorehabilitation
• Team Concept and Composition
• The Role of Pty in1. Health promotion,
2. Prevention,
3. Treatment and
4. Rehabilitation
• Common Lesions of the Nervous System viz:
• Stroke, Parkinson’s Diseases, Cerebral Palsy, Multiple Sclerosis and Traumatic Injuries

Causes of neurological dysfunction
The principal causes of neurological dysfunction
are:
• Trauma (head injury, spinal cord injury)
• Disease of the nervous system (multiple
sclerosis, Parkinson’s disease etc)
• Lesions of the circulatory system (stroke)
• Congenital defects ( e.g. spina bifida)

DEFINITION OF STROKE
• Stroke is defined by the World Health Organization (WHO) as ‘a clinical syndrome characterized by rapidly developing clinical symptoms and/or signs of focal and at times global (applied to patients in deep coma and to those with subarachnoid haemorrhage) loss of cerebral function, with symptoms lasting more than 24 hours or leading to death, with no other apparent cause other than that of vascular origin’ (Hatano, 1976).It has also been defined as a sudden attack of weakness affecting one side of the body’ resulting from an interruption of the flow of blood to the brain by thrombosis, embolus or ruptured aneurysm (WHO Monica, 1988).

Prevalence of Stroke in
Nigeria• Prevalence is 613/100,000 (Ogunniyi et al, 2001).
• Urban Nigeria prevalence is 1.14/1000 (male:
female=1.51:0.69) and lower in urban Nigeria than
in most developed country (Danesi, Okubanjo and Ojini, 2007)
• 3.6% of all medical admission, with case fatality of
45% with majority occurring in 1st week at OAUTHC (Komolafe et al, 2007)
• Mean stroke age of 52 years reported in Abuja (Imam
and Omorunfemi, 2002)

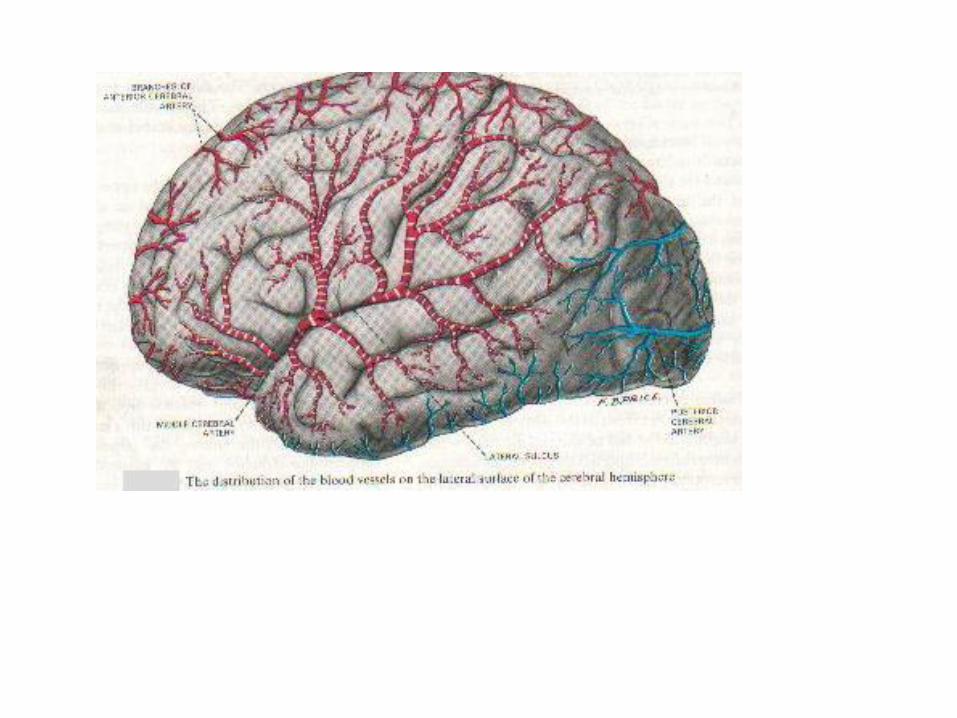
Neuroanatomic and Neurophysiologic Basis of
Stroke
• Cerebral circulation
• Somatotopic map on primary somatosensory cortex
• Risk factors
• Types of stroke
• Implication of types
• Physical manifestation
• Neuroplasticity










Physical Manifestations Include:
• Perceptual,
• Cognitive,
• Sensory,
• Communication (e.g.foreign accent syndrome)
• Motor problems.
•Most common physical consequence is Motor.

• This brain's incredibly adaptive nature,
ability to act and react in ever-changing
ways, also respond to injuries or
diseases -- known as “neuroplasticity.”

Neuroplasticity
• Ability of the brain to
adjust itself functionally, by reorganizing the cortical maps and
reorganize itself by forming new neural connections throughout life.
• This capacity for rewiring of the neuronalsynapses to allow for re-development of entire regions of the brain is present in adults as well as children

By re-developing
• Neuroplasticity allows the neurons in the
brain to compensate for injury and
disease and to adjust their activities in
response to new situations or to changes
in their environment.

• This special characteristic allows the
brain’s estimated 100 billion neurons to
constantly lay down new pathways for
neural communication and to rearrange
existing ones throughout life, thereby
aiding the processes of learning,
memory, and adaptation through
experience.

General clinical features of
neurological conditionsThese are determined partly by the site and severity of the damage. Damage to one part of the CNS usually results in a disruption of function of other parts. Some of the common features are:
1. Movement dysfunction – incoordination, ataxia, involuntary movements, tremor etc
2. Muscle tone disturbance – hypertonia or hypotonia.
3. Pain

4. Sensory disturbances – parasthesia (diminished), anaesthesia (absent), hyperaesthesia (increased), allodynia
5. Cognitive impairments – memory impairment, reduced attention span, reduced motivation
6. Emotional disturbance – depression or euphoria
7. Visual disturbances – hemianopia, diplopia, nystagmus
8. Communication disturbances – e.g. aphasia

Diagnosis of neurological
conditions
• Diagnosis is the determination of the nature or cause of a disease. It involves the evaluation of a patient’s medical history, signs and symptoms and laboratory tests to confirm or establish the presence of the disease. Diagnosis of neurological conditions entails having a good knowledge of the neurological conditions, taking a case history, and

• carrying out appropriate examinations and investigations.
(1) Case History
This is a subjective assessment process aimed at (i) localising where the pathological process is taking place within the nervous system; (ii) identifying the nature of the disease process. This is achieved with the knowledge of the onset, evolution and course of the illness.

(2) Neurological examination
This involves observations and tests to
determine gait, balance, speech defects,
memory impairments, muscle tone,
muscle weakness, co-ordination, reflexes,
sensation, posture etc. The examination
helps to localise the site of the pathology.

(3) Neurological investigations
• These are carried out to confirm a diagnosis or for the purpose of differential diagnosis. Some of these investigations are:-
1. Neuroimaging techniques such as plain radiography of the skull and spinal cord, computed tomography (CT) scanning, magnetic resonance imaging (MRI), positron emission tomography (PET) and angiography.

2. Electrodiagnostic tests such as electro-
encephalography (EEG),
electromyography (EMG), nerve
conduction tests and evoked potentials.
3. Lumbar puncture and examination of
CSF.
4. Muscle biopsy

Assessment of neurological
patients
• Assessment is an integral part of treatment; it is needed to establish the patient’s strengths and difficulties. It includes history-taking and clinical examination.
History taking – This is an interview session during which information is obtained from medical notes, the patient, relatives and carers.

• It involves getting details of the nature of
the problem, pattern of the symptoms,
previous treatments, difficulties with ADL
etc. During the history taking, clues should
be observed on posture, emotion,
cognition, communication and span of
attention.

Clinical examination
• This includes physical and functional
assessments. It enables us to obtain information
on the patient’s difficulties and level of functional
ability. The assessments are carried out in the
context of WHO International Classification of
Functioning (ICF). Emphasis is on body function,
activity and participation rather than on
impairments, disabilities and handicap (ICIDH).

• As far as physiotherapy is concerned,
body functions that need to be assessed
are those that are related to functions of
the:
1. joints (range, contracture),
2. muscles (bulk, strength, tone)
3. movements (balance, coordination)

• 4. sensation (touch, temperature)
• The clinical examination should also
include assessment of activities such as
hand and arm function, observation of gait
and assessment of gait.

Outcome measures
• A wide range of outcome measures are
available for the determination of the
effectiveness of an intervention. They
describe the results or effects of health
interventions by expressing their relative
value or importance in absolute or relative
terms. A good outcome measure should
be valid, reliable and sensitive. Examples
of

• outcome measures frequently used in
clinical setting are Barthel Index, Berg
balance scale, MAS, London Handicap
Scale, Modified Ashworth Scale and 10-
metre walk time test, Forward Upward
Leading Step Test….

Risk factors/Causes of stroke
• Risk factors are traits and lifestyle habits that increase the risk of disease. The most significant risk factor for stroke is hypertension (BP > 160/95). Also, persons who have previously had a stroke are at a markedly increased risk for a recurrent stroke. Generally, risk factors for stroke may be classified into 2 major groups:

Stroke risk factors
• Some stroke risk factors are hereditary. Others are a function of natural processes. Still others result from a person's lifestyle.
• Age; Heredity (family history) and race ;sex (gender); prior stroke, TIA or heart attack; high blood pressure; cigarette smoking; diabetes mellitus; carotid or other artery disease; atrial fibrillation; sickle cell disease; high blood cholesterol; poor diet; physical inactivity and obesity; geographic location; socioeconomic factors; alcohol abuse; drug abuse (AHA, 2007)

Nonmodifiable risk factors
• Age: Stroke can affect people of all ages, including children. However, the incidence of stroke increases with age. Hence, many people with stroke are older (60 or more years old).
• Gender: At each age, stroke is more common in men than women. However, women account for more than half of all stroke deaths.

• Race: Stroke is more common among blacks
than whites. This is partly because blacks have
higher risks of high blood pressure, diabetes and
obesity. Also, blacks have a much higher risk of
death from a stroke than Caucasians do.
• Heredity or family history: The chances of having
a stroke are greater if a close relative (parent,
grandparent, sister or brother) has had a stroke.

Modifiable risk factors
• These include hypertension, previous transient ischaemic attack (TIA), atrial fibrillation, cardiac disease, cardiac surgery, meningitis, cigarette smoking, hyperlipidaemia, diabetes mellitus, sickle cell disease, physical inactivity, obesity, alcohol abuse, drug abuse, and oral contraceptive use.

Stroke prevention
• There is substantial evidence from clinical
trials that a first or recurrent stroke can
often be prevented. A key to stroke
prevention is the control of multiple stroke
risk factors via comprehensive lifestyle
modification and the appropriate use of
pharmacological therapy. Stroke
prevention strategies are:

• Reducing blood pressure
• Lowering blood cholesterol levels
• Eating a diet low in salt and saturated
fats; and rich in fresh fruit, vegetables
and fish oils
• Taking regular exercise
• Avoiding smoking

Clinical Features of stroke
• The signs and symptoms of stroke depend upon
the size and location of the lesion. The specific
clinical features include:
• 1. Paralysis - Usually, there is paralysis of the
muscles on one side of the body, contralateral to
the side of the brain in which the lesion
occurred. This is called hemiplegia. One-sided
weakness is called hemiparesis.

• 2. Loss of sensation - Stroke patients may
have impairments in sensation, on the
hemiplegic side, which rarely disappears.
There is loss of superficial touch and
temperature sensation. Pain is common
e.g. shoulder pain syndrome especially if
there is mismanagement during the initial
stages.

• 3. Motor impairments - At the early stages of stroke there is flaccidity with no voluntary movement. This is later replaced by spasticity, hyperreflexia and mass patterns of movement (synergies). Patients present with paresis or weakness, which does not affect all muscle groups equally. They are unable to

generate levels of force necessary for initiating and controlling movement or for maintaining posture.
• 4. Contractures and deformities - The loss of voluntary movements, loss of flexibility of connective tissue and disuse atrophy generally lead to decreasing range of movement, contracture and deformity.

generate levels of force necessary for initiating and controlling movement or for maintaining posture.
• 4. Contractures and deformities - The loss of voluntary movements, loss of flexibility of connective tissue and disuse atrophy generally lead to decreasing range of movement, contracture and deformity.

• 6. Communication disorders - The speech
centre is located in the cortex of the
dominant hemisphere (typically the left
hemisphere). If the lesion affects this
region, the patient may have speech and
language impairments.

• 7. Loss of coordinated movement -
Damage to a lower part of the brain, the
cerebellum, can affect the body's ability to
coordinate movement, a disability called
ataxia, leading to problems with body
posture, walking, and balance.

Outcome of stroke
• About 20% of stroke patients die within a month,
the prognosis being much better for cerebral
infarction than for intracerebral haemorrhage
(about 10% vs 50% dead). Death is usually due
to the brain lesion itself or indirect
consequences of the brain lesion (pneumonia
and pulmonary embolism) or concurrent cardiac
diseases. After the first month, death can occur
in 10% of the patients

from a further stroke or ischaemic diseases. 30% the patients may make a full recovery while 40% will have a residual neurological deficit. Among the survivors, predictors of final recovery are the initial mild deficit, no cognitive impairment and the patient’s age. Poor prognosis is associated with incontinence and poor premorbid status of the patient.

Pattern of recovery after stroke
• In ischaemic infarct lesions, the full extent
of the initial injury is apparent. The
extensive impairment initially seen in
haemorrhagic stroke is due to localized
inflammation; and the initial recovery in
this type of stroke can be attributed to the
resolution of this inflammation.

• Majority of the patients who do not regain
consciousness within 24 hours after the
CVA may not regain consciousness. For
those who regain consciousness, greatest
recovery may occur in the first 3 months.
Thereafter, potential for improvement may
exist for many months or years.


Management of stroke
• The comprehensive management of
stroke survivors is multidisciplinary in
nature, involving a team of rehabilitation
specialists with a collaborative and
integrated plan of care. It is achieved by
joint efforts of physicians,
physiotherapists, occupational therapists,
speech therapists, nurses, social workers,
psychologists, the patient and the family.

(a) Medical management
This depends on the type of stroke and it is
based on making a correct diagnosis and
knowing the underlying cause of the
lesion. It involves maintenance of vital
functions, treatment of systemic
complications and neurological
deterioration, management of
complications (e.g. pneumonia)

and treatment of comorbid disorders e.g.
cardiac failure and angina.
Also, good nursing care is needed to
ensure that the patient is monitored
regularly, well-positioned, turned regularly,
fed and toileted; and to keep the airway
clear.

(b) Physiotherapy management
• This can be considered to take place in 4 distinct stages:
i. Acute stage
This is the immediate period following the CVA. The aims of treatment are
(a) to improve respiratory function - This is achieved by –
Regular and frequent turning, breathing exercises / percussion and

vibration to the chest and postural
drainage.
• (b) to maintain musculoskeletal
integrity - Passive ROM exercises,
positioning and early systematic
mobilisation. The specific activities
are:

• - all joints should be taken through full-range passive exercises. Particular attention should be paid to the shoulder.
• - The limbs should be placed in correct recovery patterns. Pillow support should be used to put the upper limb in shoulder extension, external rotation and abduction with supination of the forearm and extension of the wrist. The lower

• limb should be in internal rotation of hips, slight flexion of the knee and ankle dorsiflexion.
• - turning over and moving up and down while in bed.
• - weight bearing on affected side e.g. sitting on edge of bed with foot on a stool or floor and arms extended by the side or behind.

ii. Intermediate stage
• This stage commences once the patient is
medically stable and conscious. It may
start within 48 hours after CVA. The aims
are to prevent further deterioration of the
condition and to prepare the patient and
relatives for the tasks ahead. An
assessment is made to obtain an initial
database comprising personal

• details, functional and motor abilities as well as psychological and social details. Early intervention is essential and it has been shown to promote early discharge and ability to walk independently.
• Specific activities include:
• - Reeducation of movement patterns by passive and active mobilization

• of joints.
• - reduction of spasticity with massage and
passive ROM exercises.
• - reeducation of movement
• - functional reeducation e.g. activities of
daily living (ADL).

iii. Discharge and transfer stage
• This is the period immediately prior, to and
following, discharge from formal
rehabilitation. An assessment of residual
disability is made and most of the activities
of the previous stage are continued and
intensified. Necessary modifications
should be made to the patient’s
environment.

iv. Long-term stage
• This is the period following the cessation
of formal regular rehabilitation. Activities
for this stage include regular assessment
of the patient, task-specific treatments and
modification of treatment strategies.

Psychological Stages of the Stroke Survivors
(Kerr’s, 1963)
• CRISIS Sudden onset of incapacitation-Shock
• Therapy Hopeful of full recovery- “I will be well soon”
• Realization* That some deficit may be permanent- “All is lost, No Hope”
• Adjustment** “I will live with this obstacle; part of me (Defence) now- not necessarily a bad thing”
*In 50% of cases, depression sets in with suicidal tendency, inadequacy, dependence and hostilty
**Acceptance varies with cultural background

Common neurological deficits after stroke
Left-Sided Stroke (CVA)
• Right sided paralysis
• Speech Language Deficit
• Slow cautious behaviour
• Hemianopia of the right visual field (homonymous)
• Memory loss in language
• Right sided dysarthria
• Aphasia
• Apraxia
Right-Sided Stroke (CVA)
• Left sided paralysis
• Spatial/perceptual deficits/neglect
• Quick impulsive behaviour
• Hemianopia of the left visual field (homonymous)
• Memory loss in performance
• Left sided dysarthria

Complete the statements
• The principal causes of neurological
dysfunctions are ……
• The possible stages of motor recovery in
stroke survivors are……
• Stages of physiotherapeutic management
include……..
• The psychological stages of stroke
survivors may include……

Write letters that correspond to the right answers in
completing the following
The primary cells of the nervous system are the ?? while
the ?? are the supportive cells. The bulk of the human
brain is formed by the ??. A motor unit consists a ??, ??,
with ?? and ??, while a muscle unit consists of the ??
and the?? innervated. Lesion of the optic tract following
a CVA on a cerebral hemisphere can result in??.
Whereas lesion of the optic nerve may result in ??.
A=Bitemporal Hemianopia; B=Homonymous hemianopia; C=Nerve cell;
D=Nerve fiber; E=Cerebellar Hemispheres; F= Fasciculi supplied;
G=axon; H=muscle fibres innervated; I=Neuroglia; J=Cells;
K=Neurons; L=Cerebrum; M=the branches.