psychiatric disorders in childhood and adolescence
DESCRIPTION
PSYCHIATRIC DISORDERS IN CHILDHOOD AND ADOLESCENCE. Robert L. Hendren, D.O. Professor of Psychiatry and Pediatrics UMDNJ-RWJMS. Developmental Model of Psychopathology. 2 4-5 6-7 12 14 21. 6. MOS. 0. Eating Disorder Identity Disorder. - PowerPoint PPT PresentationTRANSCRIPT
PSYCHIATRIC DISORDERS PSYCHIATRIC DISORDERS IN CHILDHOOD AND IN CHILDHOOD AND
ADOLESCENCEADOLESCENCERobert L. Hendren, D.O.
Professor of Psychiatry and Pediatrics
UMDNJ-RWJMS
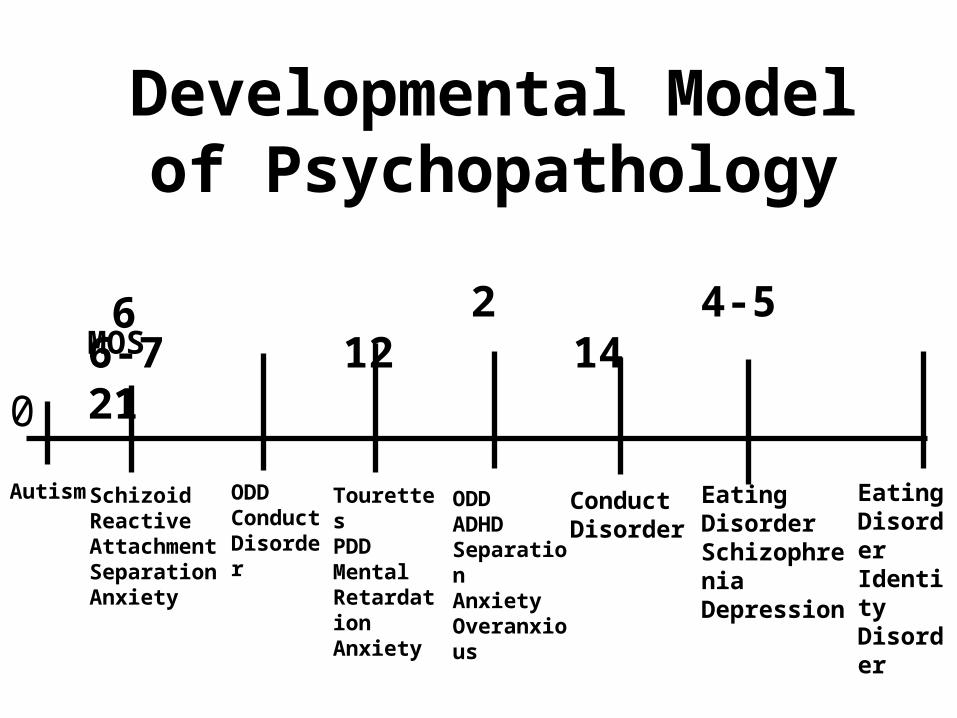
Developmental Model of Psychopathology
2 4-5 6-7 12 14 21
0
Autism SchizoidReactiveAttachmentSeparationAnxiety
ODDConductDisorder
TourettesPDDMentalRetardationAnxiety
ODDADHDSeparationAnxietyOveranxious
ConductDisorder
EatingDisorderSchizophreniaDepression
EatingDisorderIdentityDisorder
6MOS

Mental Retardation Retardation
• Mild (50-55 to 70)• Moderate (35-40 to 50-55)• Severe (20-25 to 35-40)• Profound (<20-25)
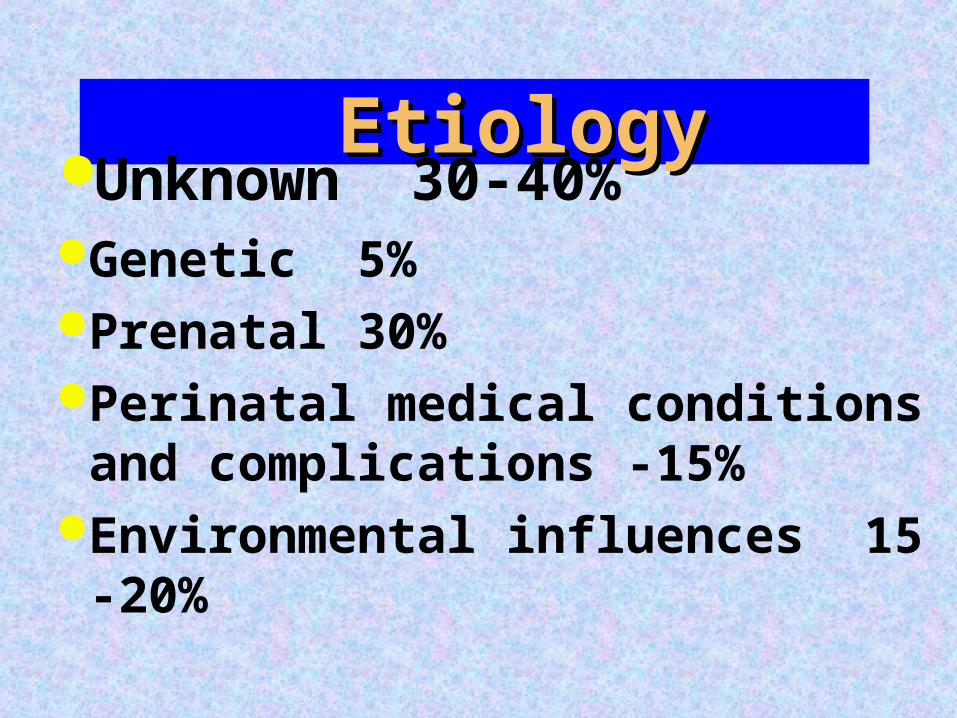
Etiology Etiology Unknown 30-40%Genetic 5%Prenatal 30%Perinatal medical conditions
and complications -15%Environmental influences 15 -
20%

Learning, Motor Skills, Communication Disorders
Reading disorder 7-9% Mathematics disorder Disorder of Written Expression 2-8% Developmental Coordination Disorder 6% Expressive Language Disorder 3-10% Mixed Receptive - Expressive Language Disorder 3-
10% Phonological Disorder 5-10% Stuttering
Autistic DisorderAutistic Disorder
•Reciprocal interaction•Communication•Stereotypes•Brain changes

Pervasive Developmental Pervasive Developmental DisordersDisorders
Asperger’s DisorderRett’s DisorderChildhood Disintegrative
DisorderPDD NOS

Elimination DisordersElimination Disorders Encopresis Enuresis

Concept of Impulse Control Disorder
Common etiology
Diagnostic overlapCo-morbidity
Attention Deficit Hyperactivity Attention Deficit Hyperactivity DisorderDisorder
Over vs. under diagnosis controversy
Subtypes include inattentive, impulsive/hyperactive and combined
Similar life cycle except hyperactivity and co-morbidity

ADHD PrevalenceADHD Prevalence
•3 - 5% school-aged children•Boys more than girls, but may be under-diagnosed in girls

ADHD Biologic EtiologyADHD Biologic EtiologyGenetic riskPrenatal stress and toxinsFrontal lobe, basal ganglia and RAS implicatedNorepinepherine - inattentionSerotonin - impulsivity

ADHD Psychosocial ADHD Psychosocial EtiologyEtiology
Poor social relatednessPeer/Authority rejectionGoodness of fit

ADHD AssessmentADHD Assessment
Context and developmentLife cycle issuesFamily issuesRule out medical causes

Rating Scales - ADHDRating Scales - ADHD
ConnorsAcTERSContinuous PerformanceWender Utah Rating Scale for
retrospective diagnosis

Alternative DiagnosesSchizophreniaPTSDBipolar Disorder

ADHD Co-morbidityADHD Co-morbidity
DepressionTics and TourettesConduct DisorderSubstance Use DisorderLearning Disability

ADHD OutcomeADHD Outcome
Normal 15%Continued Problems 50%Significant pathology 25%Substance abuse

Conduct DisorderConduct DisorderRepetitive persistent pattern of
violation
Childhood vs. adolescent onset9% males; 2% femalesCo-morbidity

CD - Biologic EtiologyCD - Biologic Etiology
Temperament
GeneticsSerotonin
•Developmental instability

CD - Psychosocial CD - Psychosocial EtiologyEtiology
•Cognitive factors•Family factors•Peer group•SES•Culture

“You left your goddam car in the driveway again!”

Oppositional Defiant Oppositional Defiant DisorderDisorder
Recurrent pattern greater than 6 months
Evident by age 8Non-aggressive grow out
Substance Use DisorderSubstance Use DisorderPrevalence
Co-morbidity
Type I/Type II