pt assigned to cabg is in yellow pt assigned to ptca is in blue diabetics benefited from cabg than...
TRANSCRIPT



• Pt assigned to CABG is in yellow
• Pt assigned to PTCA is in blue
• Diabetics benefited from CABG than from PTCA alone, evidenced by 75% 6year survivability

• By adding a stent to angioplasty, the greatest benefits are seen 100 – 225 days post procedures, decreasing the need for immediate revascularization.


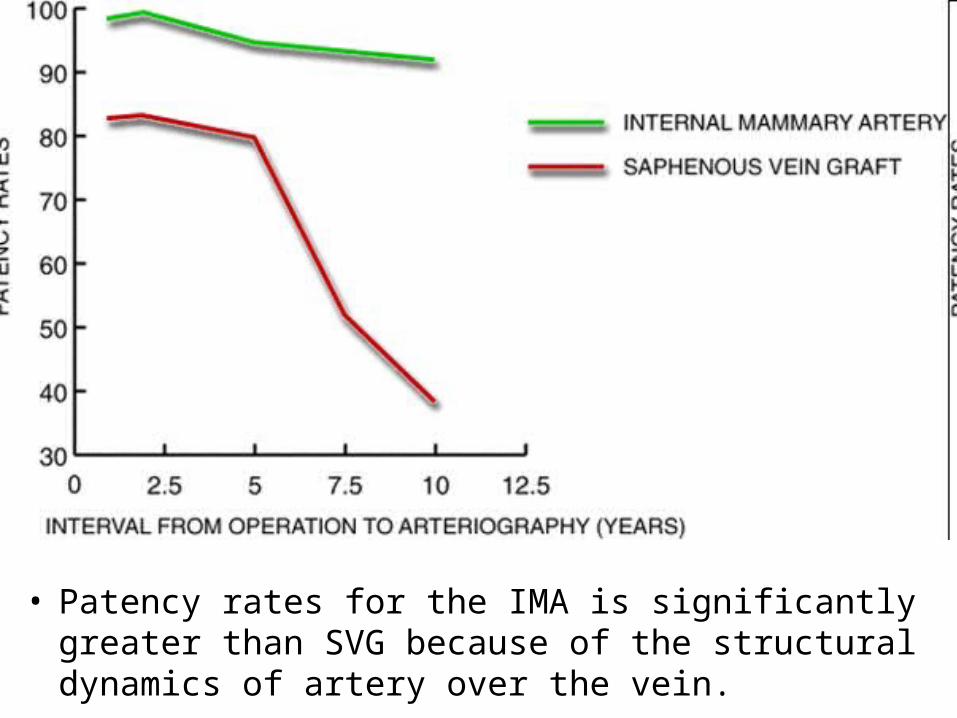
• Patency rates for the IMA is significantly greater than SVG because of the structural dynamics of artery over the vein.

• Angiogram a SVG that is now stenosed producing a non-Q wave MI with frequent bouts of angina in this 80yoa male

Secondary Prevention of CHD
• The secondary prevention of CHD involves management of cardiovascular risk factors in the patient with established CAD. Because the patient with established CAD is at higher risk of future cardiac events than an individual without established disease, secondary prevention has a greater impact on the coronary risk than primary prevention and is more cost effective.








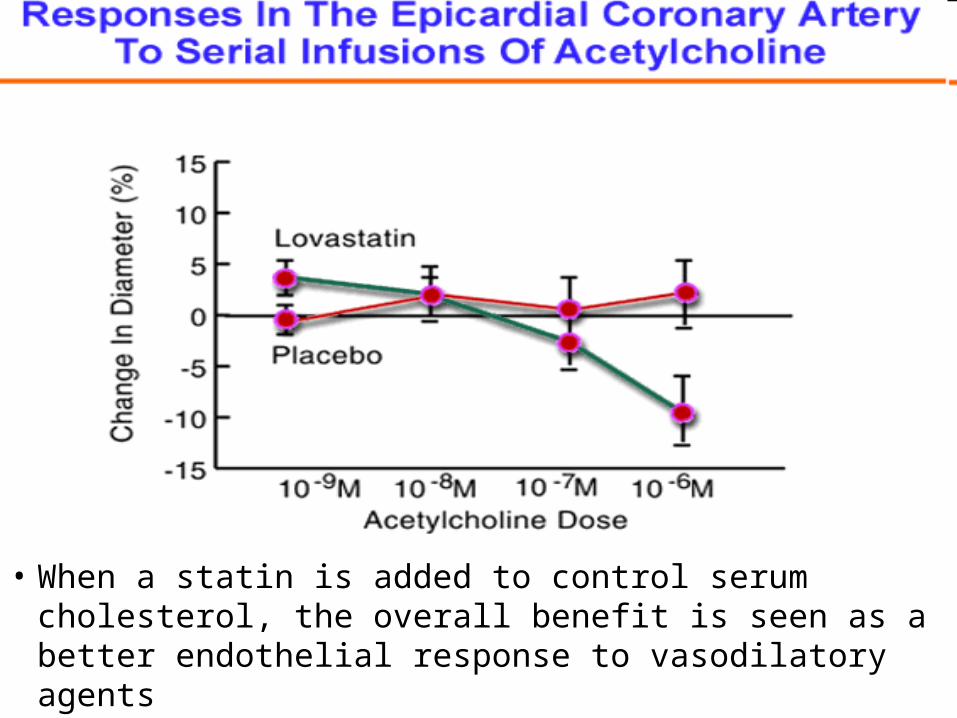
• When a statin is added to control serum cholesterol, the overall benefit is seen as a better endothelial response to vasodilatory agents

Treat by example stop smoking



Unstable Angina and Intermediate Syndrome
• A. Unstable angina represents a constellation of symptoms that usually indicates transient myocardial ischemia. It is an acute dynamic syndrome that is considered intermediate between chronic stable angina and acute MI.
• B. 750,000 hospitalizations annually in the U.S. • C. Progress to acute MI in 15% of cases• D. Mortality in the first year after diagnosis-10%
Cont’d
• E. Up to 57% of patients undergo coronary revascularization within a year of presentation
• F. Unstable angina is defined by its clinical presentation in the absence of electrocardiographic and cardiac enzyme changes diagnostic of a MI.
• G. It has 4 distinct presentations– 1.Rest angina– 2.New onset (usually within 2 months) angina– 3.Crescendo angina(more severe prolonged or frequent)– 4. Post infarction angina

Cont’d
• H. Prinzmetal’s or variant angina can present similarly to unstable angina
Etiology and Pathophysiology
• A. Imbalance in the myocardial oxygen supply demand ratio.
• B. Coronary vasoconstriction and platelet aggregation and/or thrombosis are key elements in this supply imbalance.

Cont’d
• C. Coronary endothelial plaque rupture are independent factors– 1.Anatomic location of lesion-area of high shear stress
more suseptible – 2. Lipid pool size– 3. Amount of infiltrative macrophages within the
plaque– 4. Sympathetic tone– 5. Neurohumoral environment– 6. Impaired fibrinolysis
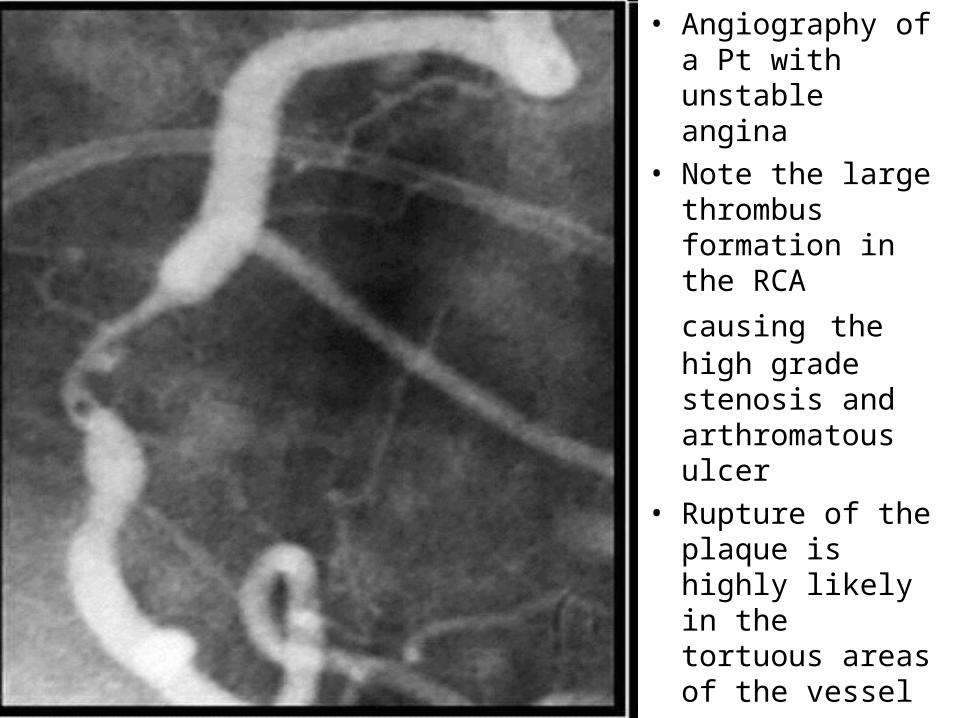
• Angiography of a Pt with unstable angina
• Note the large thrombus formation
in the RCA causing the high grade stenosis and arthromatous ulcer
• Rupture of the plaque is highly likely in the tortuous areas of the vessel

Yes; you need to go back to bio-chem and physiology

Acute Coronary Syndrome
• All acute coronary syndromes up to and including acute MI are now thought to share common pathophysiologic mechanisms.
• Thrombogenic state associated with unstable angina can be detected by various markers of platelet activation and thrombus generation.

Cont’d
• A. Thromboglobulin-secreted in blood during platelet activation
• B. Platelet factor IV-” “
• C. Thromboxane A2-B2
• D. Thrombotic generation by immunoassay
• E. Fibrin D monomers and D-dimers

Acute Coronary Syndrome
• Using thrombolytic agents have not been found to benefit patients with unstable angina, this in contrast to its usefullness in acute MI with ST segment elevation.

Anti-platelet agents• Aspirin inactivates platelets through irreversible
inhibition of the cyclooxygenase pathway.• Ticlopidene, Clopidogrel interferes with membrane
function by inhibiting ADP induced platelet fibrinogen binding and platelet to platelet interaction
• Glycoproteins IIB, IIIA receptor antibodies block platelet receptor IIB3A which is the final common pathway to platelet aggregation
• Heparin forms a complex with anti-thrombin III indirectly inhibiting both thrombin and activated factors in the clotting cascade.
• Heparin does not appreciably affect thrombin bound to tissue or fibrin



Ruptured plaque at 7 to 11 o’clock as well as a large thrombus in the lumen

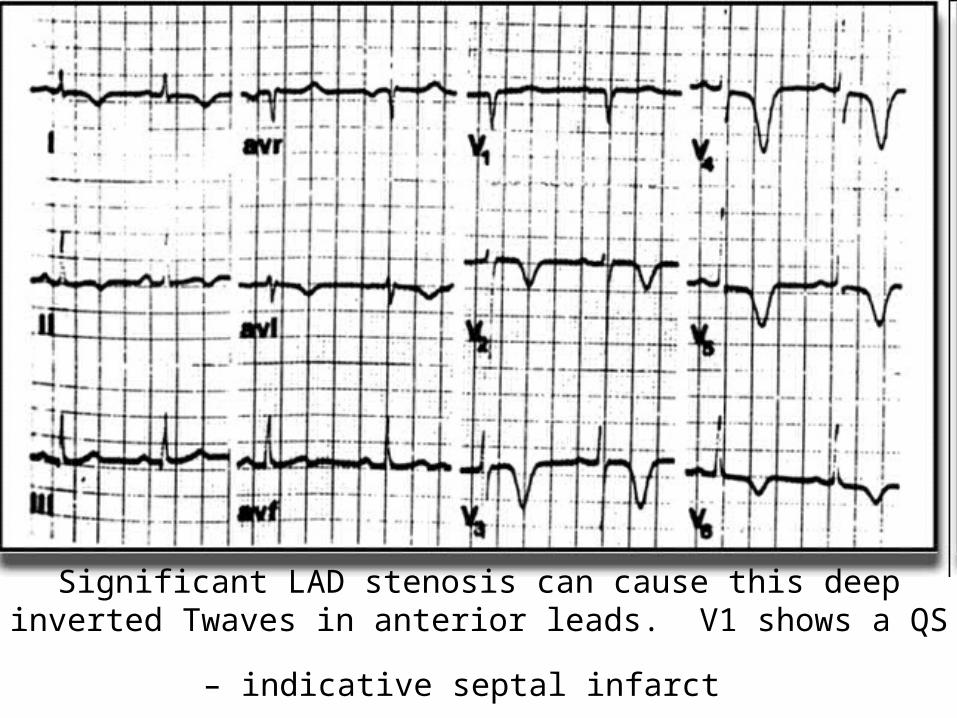
Significant LAD stenosis can cause this deep inverted Twaves in anterior
leads. V1 shows a QS – indicative septal infarct




Variant/Prinzmetal Angina
• Most frequently occurs at a focal site on the coronary artery
• Vasospasm occurs at the site of an atheroma/atherosclerotic plaque or within one cm of atheroma
• Vasospasm can occur in normal coronary vessels in this instant, more frequently involves right coronary artery more than left

Cont’d
• Occurs in younger patients with migraines, Raynaud’s phenomenon and smokers (cocaine one of leading causes of coronary spasm)
• Endothelial disfunction

Clinical Features of Variant Angina
• Younger patients • Rest pain• Women>Men• Pain during night or early morning hours when
awakening• Pain that disappears and recurs without warning• ST elevation with pain, gone when pain free• Sometimes with pain, have arrythmias

Diagnosis and Treatment of Variant Angina
• Ergonovine test during angiogram causes local spasm (causes diffuse luminal narrowing in normal coronary arteries)
• Local spasm can be reversed by nitrates• Ca-channel blocker treatment of
choice(Nifdedipine, Diltiazem, Verapamil)• Cigarette smoking and recreational drug use,
especially cocaine, should be discontinued• Long term prognosis excellent
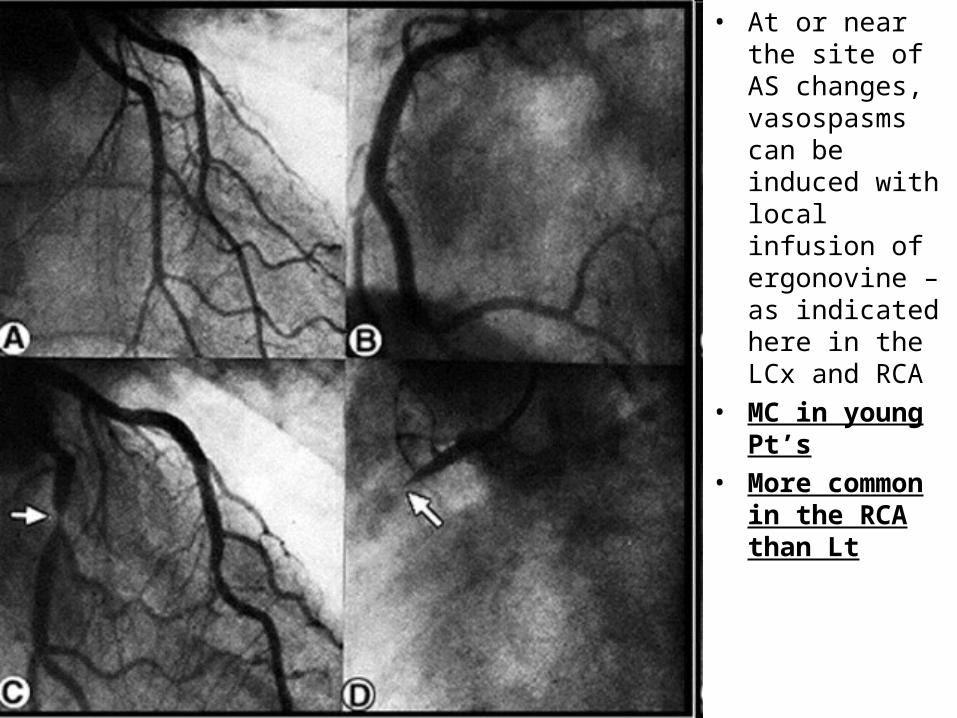
• At or near the site of AS changes, vasospasms can be induced with local infusion of ergonovine – as indicated here in the LCx and RCA
• MC in young Pt’s
• More common in the RCA than Lt



• A.) pt present with acute pain
• B.) 90 min later with out pain
• Where is the Stenosis?
• What leads shows the pathology?
• What leads shows the reciprocal changes?



Syndrome X
• Chest pain in patients with typical extertional angina, positive stress test and normal coronary angiogram
• Microvascular and endothelial dysfunction is present in many patients with syndrome X
• More prevalent in women• Treatment: Ca-channel blockers seem most
effective

Cont’d
• Nitrates and B-blockers not effective in these patients
• Long term survival excellent

Endothelin-l is potent vasoconstrictor. The Factors
to the Lt enhances Endo-1 function while the factor to the
right suppress it





• Both men and women fair the same after the age 60, mainly because women lose the benefits of estrogen

Across the board the Minnesota study shows that women do have a better Px than men


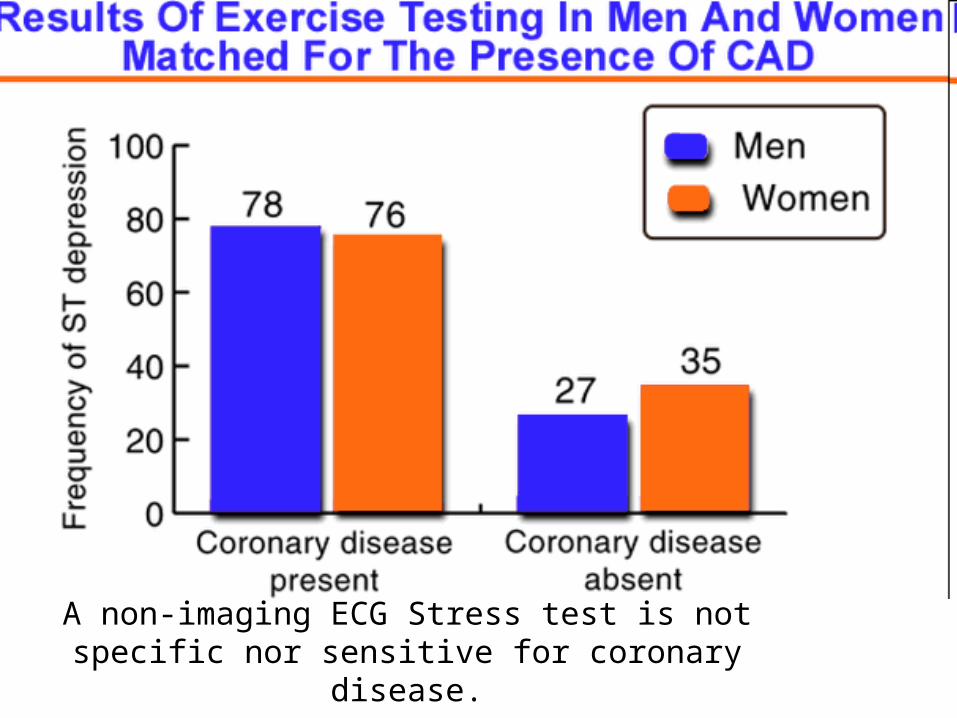
A non-imaging ECG Stress test is not specific nor sensitive for coronary disease.


• False(+) MIBI 2nd to breast attenuation









• Those patients who showed the greatested wall motion abnormality in echocardiogram was those with defensive-hostile response (lowest score)


