public intervention in health care. folland et al chapters 18 and 19
TRANSCRIPT
Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Public intervention in health care.Folland et al Chapters 18 and 19
Chris AuldEconomics 317
March 14, 2012
Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Stuff in the textbook we’re skipping.
Chapter 16: Health care labor markets and professionaltraining.Chapter 17. The pharmaceutical industry.

Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Economic efficiency, markets, and market failure.
I Why do governments intervene in health care markets?Should governments intervene in health care markets?
I When do markets do well and when do they do poorly?

Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
The notion of economic efficiency.
I Recall positive analysis attempts to discover the waythe world works. Normative analysis tells us what weought to do.
I e.g. “Rent controls will reduce the supply of housing” isa positive statement. ”...therefore, we ought notimpose price controls” is a normative statement.
I Most economic analysis is positive. Here, we will moreformally explore some of the normative reasons forgovernment intervention.
Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Efficiency
I Recall we refer to a situation as Pareto efficient if thereis no way to make anyone better off without making atleast one person worse off.
I This is a “no money left on the ground” type argument:we do not have to make interpersonal comparisons todefine such states.
I the First fundamental theorem of welfareeconomics states that if markets are competitive, thenthe market equilibrium is Pareteo efficient.

Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Redistribution.
I The Second fundamental theorem of welfareeconomics says that any Pareto efficient outcome canbe achieved as a competitive equilibrium given anappropriate endowment.
I Loosely: the First Theorem says markets will not leavemoney lying on the sidewalk—all gains from trade willbe exhausted. But we could reach one of infinitedifferent equilibria depending on where we start. TheSecond Theorem says that in principle we can deal withmatters of social justice through redistribution programsand otherwise leave the market alone.
I (graph: utility possibility frontier)

Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Welfare theorems cont.
I This is a powerful result since it suggests we can pursuepolicies which increase efficiency ignoring thedistributive aspects.
I Example: a new technology increases production butputs some workers out of jobs. So long as, in principle,the winners could compensate the losers and still beahead, government should not attempt to quash thetechnology.
I Example: one way to try to help the poor would be tosubsidize the goods the poor tend to consume. Thewelfare theorems imply that that is a poor way to try toredistribute: if different people face different prices theoutcome will not be efficient, so we are leaving moneyon the sidewalk. Better to just transfer income to thepoor and let the market find prices.

Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
welfare theorems cont.
I A problem with this argument is that we cannotcostlessly shuffle endowments around (“no lump sumtaxes.”) It costs the government more than a dollar toraise one dollar in tax revenue.
I There is, then, usually a tradeoff between equity andefficiency: if we try to redistribute the pie moreequitably, we will make the pie smaller.
Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
The welfare theorems in a health context.
I We have strong reasons to believe that the conditionsunder which the welfare theorems hold are wildlyviolated in health settings. The two most importantfailures are:
1. Information problems (uncertainty and asymmetricinformation) are prevalent in health care, as we haveseen.
2. Externalities are common, e.g., communicable disease.
Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
The second best.
I Difficult result: suppose we consider an idealized worldin which the two welfare theorems hold. We then gointo one of the many markets in the economy andintroduce some distortion, for example, firms in thismarket generate pollution, a negative externality.
I Now consider any other market in this economy.Suppose we correct a problem in this market. Giventhat the other market is distorted, it is generally nottrue that this “correction” will improve welfare.

Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Second best cont.
I Example: we break up an auto workers union which hadbeen holding wages artificially high. This lowers themarginal costs of the firm, which produces morepollution while making more cars.
I Upshot: we cannot assume that a policy which makes agiven situation look more like a competitive market willimprove welfare overall. We need to try to take thewhole system into account.
Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Rationales for social health insurance
I We have seen that insurance markets will sometimeswork very badly due to information problems.
I Those problems may be enough to justify large scaleintervention in health care.
I It may also be the case that there are external effects ofhealth care consumption.
I e.g., suppose relatively wealthy people simply get a“warm glow” when the poor consume health care:
I Since the poor do not take the “warm glow” intoaccount when choosing health care, there will be toolittle health care provided.
I (graph—positive externalities in health care)
Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
A note on “extra-welfarism”
I The preceding discussion is conventional neoclassicaleconomic theory, which presumes that social outcomescan always be reduced to the behavior of individuals(which is not to say that individual behaviors cannotcombine to produce emergent phenomena at the sociallevel), and that individuals are the best judges of theirown welfare.
I Some health economists and other analysts reject thispresumption. They argue that social outcomes cannotbe understood in terms of individual behavior, and/orthat people are irrational and are not the best judges oftheir own welare.
I This is an “extra-welfarist” argument.
Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
“Need” for health care.
I Some people argue that government should provide theamount of health care people “need.”
I But what do we mean by “need”? Need cannot bedetermined by physiology alone. beginenumerate
I Does it mean MB=0? MB=MC? Some minimum levelof health care?
I We should change health care patterns when costschange.
I There will generally be many different ways of achievinga given health goal. Which way do we select?
Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Equity in health care delivery.
I We can define and measure health or health careinequality in much the same way we define incomeinequality.
I (graph–health inequality index)
Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
CMAJ • January 17, 2006 • 174(2) | 182
Research
-0.04
-0.02
0.00
0.02
0.04
0.06
0.08
0.10
0.12
0.14
Pro-rich
Pro-poor
All doctor visits GP visits Specialist visits
Hor
izon
tal in
equit
y in
dic
es f
or d
octo
r vi
sit
pro
bab
ilit
y
US
Denm
ark
Belgi
um
Switz
erland UK
Austra
liaSp
ain
Greec
e
Hunga
ry
Austria
Fran
ce
Germ
any
Nethe
rland
s
Ireland Ita
ly
Norway
Cana
da
Swed
en
Portug
al
Finl
and
Mexico
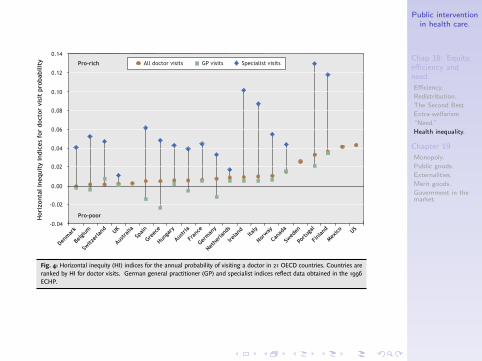
Fig. 4: Horizontal inequity (HI) indices for the annual probability of visiting a doctor in 21 OECD countries. Countries areranked by HI for doctor visits. German general practitioner (GP) and specialist indices reflect data obtained in the 1996ECHP.
–0.10
–0.05
0.00
0.05
0.10
0.15
0.20
0.25Pro-rich
Pro-poor
All doctor visits GP visits Specialist visits
Hor
izon
tal in
equit
y in
dice
s fo
r num
ber
of
doct
or v
isit
s
UK
Ireland
Belgi
um
Nethe
rland
s
Spain
Switz
erland
Hunga
ryIta
ly
Denm
ark
Cana
da
Greec
e
Norway
Germ
any
Fran
ce
Austria
Swed
en US
Portug
al
Finl
and
Fig. 5: Horizontal inequity (HI) indices for the annual mean number of visits to a doctor in 19 OECD countries. Countriesare ranked by HI index for doctor visits. German general practitioner (GP) and specialist indices reflect data obtained in the1996 ECHP.

Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Chapter 19: Government intervention in healthcare markets.
I This chapter provides and overview and summary of themain rationales for government intervention in healthcare.
I This builds on our previous discussion, and in mostcases rehashes material from Econ 103.
I Recall: (1) governments spend tremendous amounts ofmoney producing or financing health care delivery and(2) health care is heavily regulated. Why? Shouldgovernments be this deeply involved?
Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Problem 1: Monopoly power.
I Recall: A monopoly is thought to be inefficient becausethe monopolist produces too little. Does not have to beliterally one seller; most forms of oligopoly also involvedeadweight loss.
I In health care, we observe powerful monopolisticorganization even in our, and the U.S.’s, heavilyregulated and socially financed systems:
I physician “unions” (AMA, CMA)I health care providers are licensed, which is a barrier to
entryI many pharmaceutical products are patented, which is a
government-mandated monopolyI large insurers (e.g. Blue Cross) may have monopoly
power.
Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Problem 2: Public goods.
I Recall: a public good is a good which is not excludable(cannot stop someone from consuming it if they refuseto pay) and non-rival (your consumption has no effecton my consumption).
I (Note that a public good is NOT a good provided bythe government, although it may be the case that suchgoods do wind up under government provision.)
I Such goods will not be provided in efficient quantity bythe market.
Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Public goods cont.
I Health care is not a public good: it is rival (e.g., if youuse a physician’s time, there is less of her time left forme) and excludable (you can be stopped fromconsuming health care).

Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Public goods cont.
I But some aspects of health care could be consideredpublic goods:
I Some types of information could be considered publicgoods or nearly so. When you learn something it doesnot prevent me from learning that thing, and it mightbe costly to prevent others from learning that thing.Private markets may then provide too little information.Government can fund research or directly provideinformation (e.g., health effects of smoking).
I Redistribution has public good aspects. Suppose allwealthier people feel happier when the poor have accessto health care. Then ‘the poor having access to healthcare’ is like a public good and will be underprovided bya free market. Possible that everyone will be better off ifthe well off are taxed to provide health care for the poor.

Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Problem 3: Externalities.
I Recall an externality occurs when A takes an actionwhich involuntarily affects B but A neither compensatesnor is compensated by B.
I This is NOT NOT NOT the correct definition:Nature pollinates all of the flowering plants, itis nature that decays material, returns it tothe earth. It creates soil, participates in thenitrogen cycle, the carbon cycle, and thewater cycle. All of these are economicallyvaluable services performed by nature buteconomists called them externalities, by whichthey mean that they are not in the economicequation. – David Suzuki
Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Externalities cont.
I In health, possibly the most important class ofexternalities arise from communicable disease.
I Any action you take which increases the probability youcatch a communicable disease is a negative externalityon me.
I Vaccination is an important example: if you fail to getvaccinated, you increase the probability I get sick. Themarket will provide too few vaccinations. (graph)
I Other behaviors which affect disease transmissionsimilarly have external effects. e.g., optimally, peoplewould use more condoms and have fewer sexualpartners than they do, because anything you do whichincreases the probability you catch a STD induces anegative externality.
Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Merit goods.
I A merit good is (for our purposes) a good which isunderconsumed because people don’t know what’s bestfor them and would be better off if they chose toconsume more.
I This is paternalistic. We are claiming that someonewould be better if with A rather than B even if theperson chooses B over A.
Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Merit goods cont.
I e.g., we are more willing to provide food to the homelessthan cash to the homeless, because we (we?) don’tthink the homeless would spend cash in the right way.
I e.g., government provides subsidies to the fine arts andnot to Justin Bieber.
I e.g., certain types of irrational behaviors create“internalities” and people may be better off if thegovernment paternalistically alters their behavior (“Ican’t stop smoking by myself, thank you for raisingtobacco taxes.”)

Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Merit goods cont.
I We can explain, albeit perhaps not condone, manypolicies as responses to perceived merit goods.
I e.g., Drug prohibition and heavy tobacco and alcoholregulation may in part be a response to the idea thatpeople cannot by themselves make the right decisionswith respect to the consumption of alcohol and otherdrugs.
Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Forms of government intervention.
I Taxes and subsidies. Pigouvian taxes/subsidies cancorrect externalities and other problems.
I Public provision of health care and/or health insurance.
I Transfer programs.
I Regulation.

Public interventionin health care.
Chap 18: Equity,efficiency andneed.
Efficiency.
Redistribution.
The Second Best
Extra-welfarism
“Need.”
Health inequality.
Chapter 19
Monopoly.
Public goods.
Externalities.
Merit goods.
Government in themarket.
Government failure.
I A lot of economic theory looks something like: ‘Wehave decided that the private market will provide Q=10,but that the efficient level is Q=15. If the governmentdoes something or other just right, like impose a tax oft=1.34, then we will get to the efficient level. So thegovernment should intervene.’
I This would only follow if we had good reason to believethat if the government does intervene, it will intervenein just the right way.
I But we rarely have reason to believe that governmentwill do everything just right.
I Therefore, we should at least consider what we expectgovernment to actually do if it intervenes rather thanprescribing intervention whenever we see a marketfailure.