public private partnerships for healthcare delivery...
TRANSCRIPT
1
Public Private Partnerships for Healthcare Delivery in India: Assessing Efficiency for
Appropriate Health Policies
Bharti Birla, Udita Taneja
University School of Management Studies, GGS Indraprastha University Delhi, India
Healthcare delivery is a major concern for India and other developing na-tions. A number of Public Private Partnerships (PPPs) have entered the arena of healthcare delivery. These partnerships are based on different models. The efficiency of such partnerships needs to be assessed as it will help formulate policies that can contribute in enhancing the role of such partnerships in meeting the health goals of the country. There are several factors that govern the efficiency of such partnerships. The present study aims to identify the factors that are considered important while assessing the efficiency of healthcare delivery units based on PPPs, and to rank these factors.
1. Introduction
In the last two decades, there has been a growing concern over the performance of the healthcare delivery system in India. In the year 2006, a mere 0.9% of the GDP was allocated to public health. Peters et al. state that India‘s health system is being forced to adapt to changing health conditions, new technologies, transformations in society and evolving roles for government and the private sectors (Peters; et al., 2003). In recent years, the Indian government has formulated a number of innovative policies and plans to address the issue of under-performance, especially in terms of healthcare delivery. The Indian government has also introduced a number of reforms across different sectors, such as healthcare financing, health insurance, continuing medical education, and health information systems. Yet, the public healthcare deliv-ery system is unable to deliver and meet the health goals of India.
The Government of India (GOI) Report of the National Commission on Macroeco-nomics and Health (2005), states that the principal challenge for India is building a sustainable healthcare system. Selective, fragmented strategies and lack of re-sources have made the health system unaccountable, disconnected to public health goals, inadequately equipped to address people's growing expectations and inability to provide financial risk protection to the poor. According to the Organisation for Eco-nomic Co-operation and Development (OECD) Report (2004), adequate and effec-tive delivery of public services is also central to achieving the Millennium Develop-ment Goals (MDGs). The Planning Commission of the Government of India (GOI) has constituted a Working Group on PPPs to improve healthcare delivery for the Eleventh Five-Year Plan (2007-2012) under the Chairmanship of the Secretary, De-partment of Health & Family Welfare, GOI. According to the draft report prepared by
2
the Group, the share of private players in healthcare delivery has grown tremen-dously. The GOI‘s Report (2006-7) by The Task Force on Medical Education for the National Rural Health Mission, states that the private sector provides 58% of the hospitals, 29% of the beds in the hospitals and 81% of the doctors. Nearly 78% of the rural and 81% of the urban population is provided medical treatment by private healthcare players. Also, according to the National Sample Survey Organisation (NSSO) 60th Report (2004), use of public healthcare is lowest in the rural areas of states of Bihar and Uttar Pradesh. This reliance on the private sector for healthcare delivery is highest in Bihar (89% in urban and 95% in rural areas). Approximately 77% of OPD cases in rural areas and 80% in urban areas are being serviced by the private sector in the country. Bhat suggests that one must look at other options for healthcare delivery because there are no regulations to monitor the cost and quality of the private players. Apart from these negative consequences of the private sector growth, the cost of private healthcare cannot be afforded by most people from the lower strata of society and those who do use private services do so at an exorbitant cost. Bhat further comments that the cost of health care, access and quality problems will worsen with the growth of the private sector. The public policy response to check some of the undesirable consequences of this growth is critical and should focus on strengthening the existing institutional mechanisms to protect patients, developing and implementing an appropriate regulatory framework, and strengthening the public health care delivery system (Bhat, 1999).
Apart from the private players, many civil society organizations have also entered the arena of healthcare delivery. The Indian government is encouraging Public Private Partnerships (PPPs), and is also acknowledging their role and contribution in meeting the health goals of the country. Promotion of these PPPs is also important to lessen the burden on the government in terms of providing the outreach as well as to allevi-ate the funding constraints. Under the 10th Five Year Plan (2002-2007), initiatives have been taken to define the role of the government, private and voluntary organiza-tions in meeting the growing needs for healthcare services and meeting the goals of National Health Programmes. The mid-term appraisal of the 10th Five Year Plan also advocates partnerships subject to suitability at the primary, secondary and tertiary levels. The contemporary National Health Policy of India, formulated in the year 2002, and the ambitious National Rural Health Mission (NRHM) formulated for the period 2005-2012, takes into consideration the important role played by private play-ers and civil society organizations in meeting the health goals of the country. At the national level for India, the MDGs have been integrated into the 10th and 11th Five Year Plans as well as form an integral part of the National Rural Health Mission (NRHM). The National Health Policy of India envisaged the participation of the pri-vate sector in primary, secondary and tertiary care and recommended suitable legis-lation for regulating minimum infrastructure and quality standards in clinical estab-lishments and medical institutions. The GOI, Ministry of Health and Family Welfare, has evolved guidelines for PPPs in different National Health Programmes like Re-vised National Tuberculosis Control Programme (RNTCP), National Blindness Con-trol Programme (NBCP), National Leprosy Eradication Programme (NLEP), and Re-productive and Child Health (RCH). Under the Reproductive and Child Health Programme Phase II (2005-2009), several initiatives have been proposed to strengthen social-franchising initiatives. As per the GOI Planning Commission‘s Draft Report of Working Group on PPPs, the NHRM as well as the National Health Policy envisage a definite role of PPPs in delivering healthcare services to both urban and
3
rural India. Most importantly, NRHM proposes to support the development and effec-tive implementation of regulating mechanisms for the private health sector to ensure equity, transparency and accountability in achieving public health goals.
The recommendations of the GOI Planning Commission‘s Working Group on PPPs, stresses the importance of formulating policies that promote the growth of PPPs in India. The recommendations also call for developing a framework that can monitor and evaluate the performance of the healthcare systems including the PPPs. There has been growing acceptance of PPPs in achieving healthcare goals. The United Nations Economic And Social Council (2005) report states that the fear of privatizing the healthcare services has been, to an extent, mitigated by the PPPs because of the potential advantages these partnerships offer, such as efficiency, outreach, sustain-ability, and quality of services. Best practices and good examples of PPPs have initi-ated a change in government policies. Over the years, the roles of government, pri-vate sector and civil society organizations (CSO) have become more clearly defined and PPPs have become more popular. Vinod et al. describe that partnerships be-tween the state and private institutions, the state and civil society organizations as well as between civil society and for-profit (private) health institutions are growing. The mechanism of such partnerships varies from unit to unit and is not mutually ex-clusive. These mechanisms are social marketing, social franchising and contracting. (Vinod; et al., 2004)
PPPs for healthcare exist at three levels. The first level is for basic research which generally happens in collaboration with universities and research institutes. The sec-ond level of partnerships happens at the level of drug development. This activity is largely in collaboration with pharmaceutical and biotechnology companies engaged in drug development and production. The third level of partnerships is at the level of actual healthcare delivery. Here the state or private healthcare units collaborate with each other to provide delivery systems for access to healthcare services. The Indian healthcare sector is three-tiered – Primary, Secondary and Tertiary. The government, non-profit, charitable, corporate hospitals, and private clinics are key providers of healthcare delivery. Currently most players work in isolation from one another in terms of providing a continuum of care to patients. According to the GOI‘s Planning Commission‘s Task Force on Public Private Partnerships (2007), this network is cur-rently insufficient to provide adequate healthcare services to the Indian population.
Keeping in mind the health goals of the country, it is necessary to not only analyze the performance of the healthcare sector, but also study the various models that have contributed to the growth of this sector in India. This study seeks to analyze the performance of one such model, i.e. the PPPs in the provision of healthcare services in India. It is important to find out how PPPs can help in moving towards the health goals of the country, as well as calculate the efficiency of PPPs in delivering health-care services.
Assessing the efficiency of different models of PPPs will be useful in formulating the monitoring and evaluation schemes and policies of government, international and national donor agencies, as well as the private players. Encouraging business play-ers to enter into efficient forms of healthcare delivery, PPPs would help alleviate pov-erty as a World Bank Report (2002) has pointed out that a single major illness can bring a family to below the poverty line in India.

4
It is important to analyze the factors which can contribute to the efficiency of PPPs engaged in healthcare delivery. It will also be useful to assess which mechanism of partnership is most effective in a given situation. Most studies available describe the factors that are essential for efficient working of a healthcare unit. The relative impor-tance of these factors has, however, not been assessed.
The report of the Australian Steering committee for the Review of Common-wealth/State Service Provision (1997), defines the efficiency of a healthcare unit as the degree to which the observed use of resources to produce outputs of a given quality matches the optimal use of resources to produce outputs of a given quality. According to Worthington, there can be three main measures of the efficiency of healthcare units. These are technical efficiency, allocative efficiency and productive efficiency. Technical efficiency, as the name suggests, pertains to the use of produc-tive resources in the most technologically efficient manner, i.e. getting maximum possible output from a given set of inputs. Allocative efficiency on the other hand measures the ability of the organization to select different efficient combination of inputs to produce the maximum possible outputs (Worthington, 1999). Farrell and Worthington, state that technical and allocative efficiency taken together determine the degree of productive efficiency (also called economic efficiency) (Farrell,1957; Worthington, 2004). Worthington points out that an organization is said to have achieved total productive efficiency (economic efficiency) if its resources are used completely allocatively and technically efficiently. Conversely, if the either allocative or technical inefficiency is present, then the organisation will be operating at less than total economic efficiency (Worthington, 2004).
A number of studies have been conducted worldwide, and a few in India, to calculate the efficiency of healthcare units. In these studies a number of input and output fac-tors have been considered while calculating the efficiency of the unit. Many health-care studies in India and abroad have defined different input factors, such as number of doctors, number of nurses/paramedical staff, cost of supplies, and cost of high-cost technical machinery. Some of the outputs selected are number of regular ad-missions, number of surgeries, case mix categories, and number of discharges. Apart from these quantifiable factors, Kooreman states that efficiency is also a measure of some hard to quantify factors, such as improved health status or im-proved quality of life (Kooreman, 1994).
The objective of this study is twofold. The first objective is to determine the factors that are considered important while assessing the efficiency of healthcare delivery units based on PPPs, and the second is to rank these factors.
2. Methods
A literature survey was done to identify various input and output factors used in dif-ferent studies for measuring the efficiency of healthcare units. For the literature sur-vey different databases such as Medline, Pubmed, Indian Medlars Center, Niscair and online versions of journals on healthcare and health policy were searched. Titles and abstracts of journals were also searched using Google Scholar. Proceedings of past conferences related to the topic, were also accessed. In addition, the websites of World Health Organization (WHO), The World Bank, Ministry of Health and Family
5
Welfare, GOI, Planning Commission, GOI, National Rural Health Mission (NHRM), GOI and other relevant GOI portals were searched to gain access to reports, policies, white papers, recommendations and proceedings of conferences. Different keywords were selected, such as efficiency, input, output, data envelopment analysis, public private partnership/mix, healthcare delivery. It was found that different studies had used different factors.
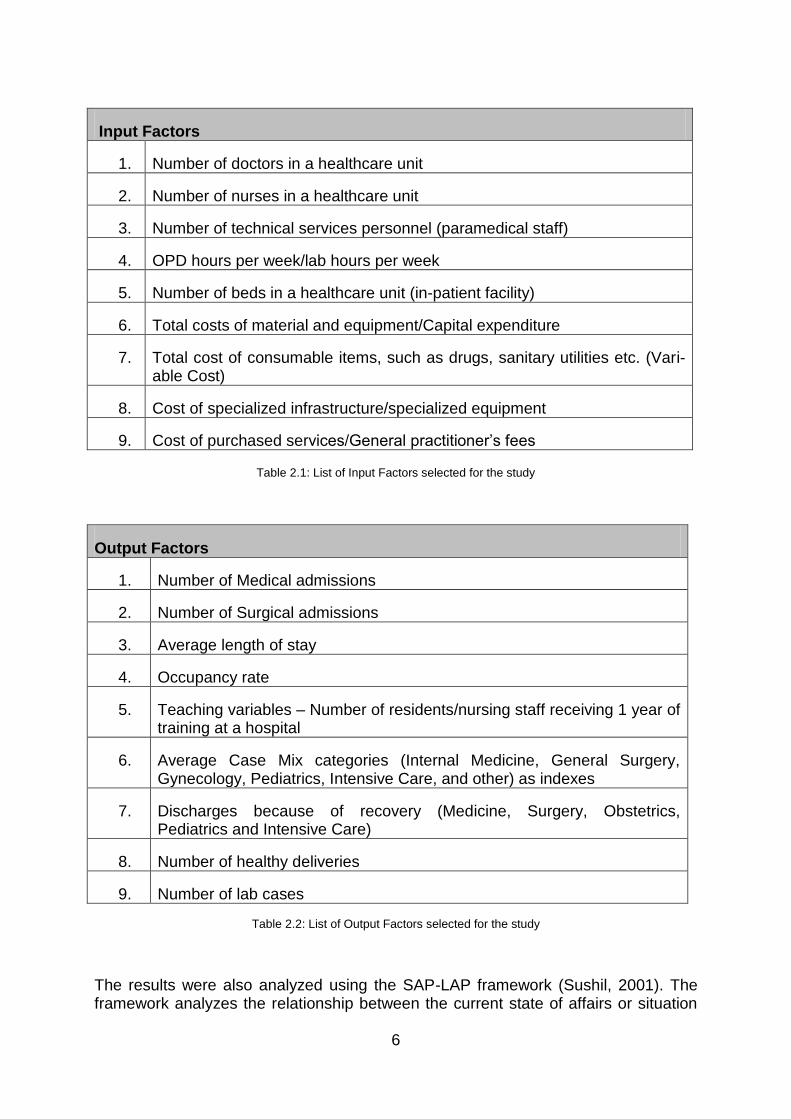
Based on this literature survey, key factors were identified. A pilot questionnaire was developed based on the factors identified. These were tested amongst a group of healthcare professionals. Based on this and on initial interviews with some of the healthcare professionals, 9 input factors (Table 2.1) and 9 output factors (Table 2.2) were selected, which could contribute to the efficiency of a PPP based healthcare delivery unit. The explanatory variables, such as accessibility of the unit, distance to the nearest hospital, impact on overall health of the community, level of community participation, which are largely qualitative in nature, have not been considered in this study.
A cross-sectional exploratory study was then conducted to rank these factors using a survey instrument. Data were collected using a self-administered questionnaire. A five-point Likert scale (anchored at 5 = strongly agree, 4 = agree, 3 = does not mat-ter, 2 = disagree and 1 = strongly disagree) was used to rank the factors. The higher the numerical value of a factor, the higher its importance in contributing towards the efficiency of a healthcare delivery unit. The score for a particular input or output was obtained by summing the scores for all respondents for that factor.
Respondents were also encouraged to suggest additional factors which they thought might be important in assessing the efficiency or could contribute to the efficiency of the health care delivery systems.
Questionnaires were emailed or hand-delivered to various stakeholders in healthcare delivery and planning. The sample size consisted of 85 respondents including healthcare professionals/social workers in civil society organizations, policy mak-ers/influencers, corporate social responsibility wings of business houses providing healthcare services, government officials, and doctors from both government and private practice. The geographical scope included mainly the National Capital Region of Delhi and a few responses from other States in India.
An MS Excel sheet was programmed to analyze the results obtained. Responses received for each selected input and output factor were assigned values, as stated above. Cumulative scores for each factor were calculated. The factors were then ar-ranged in decreasing order of the cumulative scores obtained. The responses re-ceived were also analyzed to see if respondents engaged in community outreach, doctors and researchers differed in ranking these factors.
6
Input Factors
1. Number of doctors in a healthcare unit
2. Number of nurses in a healthcare unit
3. Number of technical services personnel (paramedical staff)
4. OPD hours per week/lab hours per week
5. Number of beds in a healthcare unit (in-patient facility)
6. Total costs of material and equipment/Capital expenditure
7. Total cost of consumable items, such as drugs, sanitary utilities etc. (Vari-able Cost)
8. Cost of specialized infrastructure/specialized equipment
9. Cost of purchased services/General practitioner‘s fees
Table 2.1: List of Input Factors selected for the study
Output Factors
1. Number of Medical admissions
2. Number of Surgical admissions
3. Average length of stay
4. Occupancy rate
5. Teaching variables – Number of residents/nursing staff receiving 1 year of training at a hospital
6. Average Case Mix categories (Internal Medicine, General Surgery, Gynecology, Pediatrics, Intensive Care, and other) as indexes
7. Discharges because of recovery (Medicine, Surgery, Obstetrics, Pediatrics and Intensive Care)
8. Number of healthy deliveries
9. Number of lab cases
Table 2.2: List of Output Factors selected for the study
The results were also analyzed using the SAP-LAP framework (Sushil, 2001). The framework analyzes the relationship between the current state of affairs or situation
7
analysis (S), the stakeholders or the actors (A) and the processes (P). According to Sushil, the more the freedom the actors have, the more adaptive and flexible the processes, and the better the change. This is because the actors need to perform within the given situation by following certain processes. The more freedom the ac-tors have, the more flexible will be the processes. This will help in dealing with the changing situations and bring about a more positive outcome. The synthesis and in-teraction between the different components of Situation-Actor-Process (SAP) leads to several learnings (L), which can lead to further actions (A) and depending upon the effectiveness of the actions, there can be enhanced expected performance (P). This improved performance can, in-turn, affect the situation, actors and processes at dif-ferent levels (Sushil, 2001).
3. Results
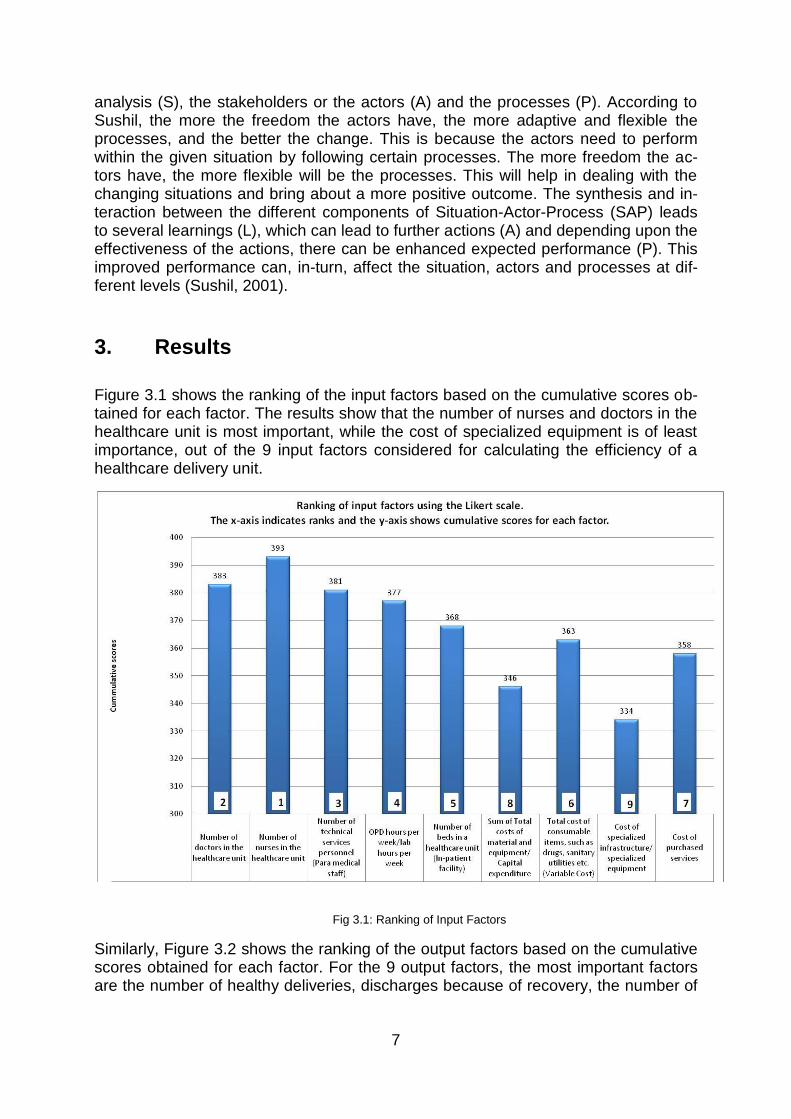
Figure 3.1 shows the ranking of the input factors based on the cumulative scores ob-tained for each factor. The results show that the number of nurses and doctors in the healthcare unit is most important, while the cost of specialized equipment is of least importance, out of the 9 input factors considered for calculating the efficiency of a healthcare delivery unit.
Fig 3.1: Ranking of Input Factors
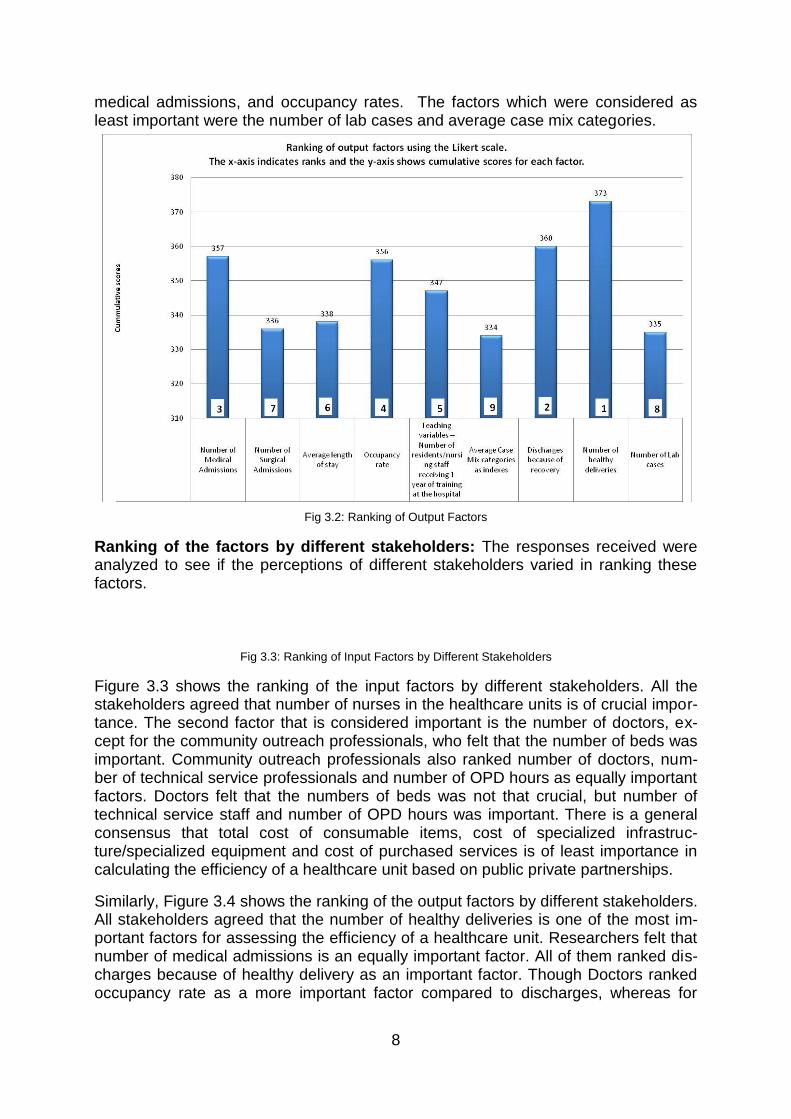
Similarly, Figure 3.2 shows the ranking of the output factors based on the cumulative scores obtained for each factor. For the 9 output factors, the most important factors are the number of healthy deliveries, discharges because of recovery, the number of
8
medical admissions, and occupancy rates. The factors which were considered as least important were the number of lab cases and average case mix categories.
Fig 3.2: Ranking of Output Factors
Ranking of the factors by different stakeholders: The responses received were analyzed to see if the perceptions of different stakeholders varied in ranking these factors.
Fig 3.3: Ranking of Input Factors by Different Stakeholders
Figure 3.3 shows the ranking of the input factors by different stakeholders. All the stakeholders agreed that number of nurses in the healthcare units is of crucial impor-tance. The second factor that is considered important is the number of doctors, ex-cept for the community outreach professionals, who felt that the number of beds was important. Community outreach professionals also ranked number of doctors, num-ber of technical service professionals and number of OPD hours as equally important factors. Doctors felt that the numbers of beds was not that crucial, but number of technical service staff and number of OPD hours was important. There is a general consensus that total cost of consumable items, cost of specialized infrastruc-ture/specialized equipment and cost of purchased services is of least importance in calculating the efficiency of a healthcare unit based on public private partnerships.
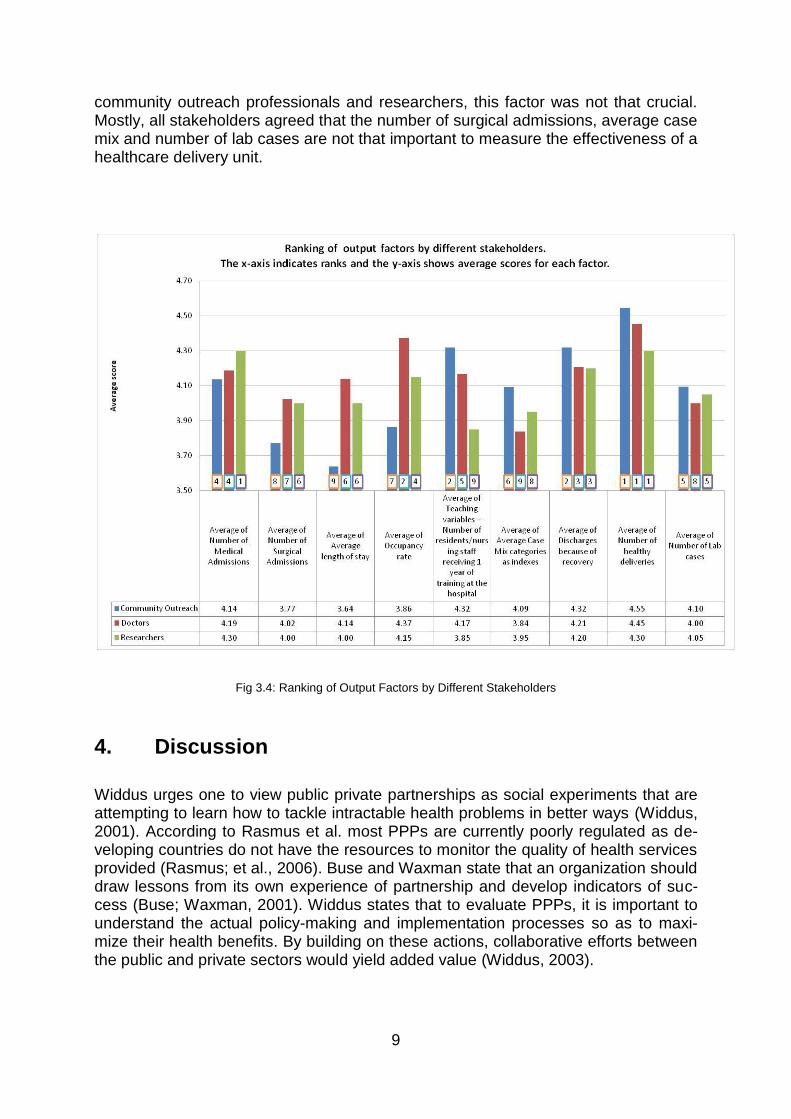
Similarly, Figure 3.4 shows the ranking of the output factors by different stakeholders. All stakeholders agreed that the number of healthy deliveries is one of the most im-portant factors for assessing the efficiency of a healthcare unit. Researchers felt that number of medical admissions is an equally important factor. All of them ranked dis-charges because of healthy delivery as an important factor. Though Doctors ranked occupancy rate as a more important factor compared to discharges, whereas for
9
community outreach professionals and researchers, this factor was not that crucial. Mostly, all stakeholders agreed that the number of surgical admissions, average case mix and number of lab cases are not that important to measure the effectiveness of a healthcare delivery unit.
Fig 3.4: Ranking of Output Factors by Different Stakeholders
4. Discussion
Widdus urges one to view public private partnerships as social experiments that are attempting to learn how to tackle intractable health problems in better ways (Widdus, 2001). According to Rasmus et al. most PPPs are currently poorly regulated as de-veloping countries do not have the resources to monitor the quality of health services provided (Rasmus; et al., 2006). Buse and Waxman state that an organization should draw lessons from its own experience of partnership and develop indicators of suc-cess (Buse; Waxman, 2001). Widdus states that to evaluate PPPs, it is important to understand the actual policy-making and implementation processes so as to maxi-mize their health benefits. By building on these actions, collaborative efforts between the public and private sectors would yield added value (Widdus, 2003).

10
According to a report by the Australian Steering Committee for the Review of Com-monwealth/State Service Provision (1997), such evaluations are important as gov-ernments can use performance measures to stimulate policy development, facilitate improved performance and accountability, promote competition among similar pro-viders operating under similar environments, analyze relationships between various agencies, and in allocating funds.
The ranking obtained in this study shows that in terms of input, the strength of human staff including the number of medical doctors, nurses and paramedical staff present at the healthcare unit are the most important factors for efficient functioning. A World Bank Report (2004) analyzes that even when resources are available, there are at least four reasons why many governments have failed to reach the poor through pub-lic channels. One of the reasons is that although resources are allocated for services that are meant to benefit the poor, such as primary healthcare, the funds often do not reach the frontline service providers or the intended beneficiaries. It could be be-cause traditional approaches tend to focus more on inputs, such as equipment, mate-rials and salaries, regardless of varying local needs. According to a recent study, it is estimated that in India, country-wide absenteeism rates among doctors in the public health sector are 43% (Chaudhury; et al., 2004).
In terms of output factors, number of healthy deliveries, discharges because of re-covery, the number of medical admissions, and occupancy rates are important fac-tors. In several studies, including a study by Shugarman et al. higher occupancy rates are generally associated with low healthcare costs. In terms of policy making, it becomes crucial to focus on the high ranking factors to make the PPPs work at the optimal level (Shugarman; et al., 2007). Osei et al. state that productivity growth, technical progress, and efficiency change of fixed health facilities consumes the ma-jority of the recurrent and development budgets. There is a need for conducting re-search to establish baseline technical and scale efficiencies which can be used as a guiding parameter against which the efficiencies can be compared (Osei; et al., 2007). This information could be used to devise strategies and methods to reduce inefficiencies in health care delivery by making the necessary policy changes. This baseline data can also be used in monitoring the efficiency effects of future policy changes.
The results obtained from the survey were analyzed using the SAP-LAP model for change. The PPPs bring with them a paradigm shift in the way health care goals are being addressed. The existing arrangement needs to change to a new synergistic framework for supporting the vast and varied healthcare needs of the country.
4.1. Situational Analysis
The current healthcare infrastructure is incapable of meeting the health goals of the country. There is a need to develop an alternate supportive system, which can augment and fulfil the un-met health needs of the people in India. This supplementary system is in the form of Public Private Partnerships, which targets the population currently under-served or denied quality healthcare, be-cause of the limited reach and scope of the public health services.
11
The Indian healthcare sector, structured in three tiers (primary, secondary and tertiary), is characterized by the presence of several distinct systems of healthcare delivery such as the government, not-for-profit/charity/faith based organizations, corporate hospitals, and private clinics. Currently, all players work in isolation from one another in terms of providing a continuum of care to patients.
The principal challenge for India is to build a sustainable health system which should be accountable and capable of fulfilling the needs of the public. Selec-tive, fragmented strategies and lack of resources make the current health sys-tem, ill equipped to address people's growing expectations and fails to provide financial risk protection to the poor.
The Government of India has been encouraging public private partnerships in the area of healthcare delivery. The Indian government has introduced a num-ber of reforms across different sectors, such as healthcare financing, health insurance, continuing medical education, and health information systems. Yet, the public healthcare delivery system is unable to deliver and meet the health goals of India.
4.2. Main Actors
Government of India
Healthcare providers – public and private healthcare providers including the Government, not-for-profit/charity/faith based organizations, corporate hospi-tals, and private clinics.
Patients, healthcare seekers, other indirect consumers/stakeholders of health-care services, such as relatives and friends of the patients.
A coalition of the private healthcare providers, civil society organizations and Government of India in form of Public Private Partnerships.
The PPPs model aims at bringing quality and affordable healthcare, which enlarges the reach and expands the services offered by public healthcare in-stitutions across the country. All actors involved in the Public Private Partner-ships work towards meeting the health needs of the country. The objectives, the motivation and factors that provide impetus for such work performed may be different for a For-Profit organization versus a Public Institute or a Not-for-Profit sector organization.
4.3. Public Private Partnerships‟ Healthcare Delivery Processes
The Government of India is increasingly looking to the private sector for assis-tance in meeting the national health goals.
12
Public Private Partnerships bridge the gap between the Government, policy-makers, healthcare needs, and the range of public-funded services on the one side, and private/civil society providers of technical expertise on the other side.
The Public Private Partnerships are being promoted to encompass diverse concepts and models that focus on health systems modernization or providing technical expertise, scaling up operations, enhancing outreach, or initiating varied health system strengthening reforms.
These partnerships strive to create a collaborative framework between differ-ent stakeholders. Apart from addressing the public health issues, these syner-gistic partnerships also provide opportunities for both public and For-Profit or-ganizations to also meet their individual goals.
There are broad guidelines available from the Government, as well as Interna-tional bodies for the formation of these partnerships. But there are no guide-lines or established frameworks defined for measuring the efficiency of these partnerships.
Public Private Partnership does not necessarily imply the use of private fi-nance. Publicly financed health authorities can contract with private or non-profit organizations to provide health care services. The key question is whether these partnerships are able to meet the goal of providing affordable and quality healthcare with the amount of resources or inputs available.
There are numerous input and output factors that can influence the efficiency of these partnerships. Out of these factors which are crucial and important for maintaining a good efficiency level is not known.
4.4. Key Learning Issues
In today‘s context, PPPs are contributing in most sectors of development, be it education, health, or telecommunications. This new trend has several advan-tages over the conventional setups as the expertise of the government and in-dustry is brought together.
From this study it is evident that the presence of healthcare delivery providers is the most crucial input for better functioning of a healthcare unit.
In terms of input factors, the number of healthcare professionals (nurses, doc-tors and paramedical staff), rather than the cost of specialized high-end equipment, are important in calculating the efficiency of a healthcare delivery unit.
In terms of output factors, the number of healthy deliveries and discharges be-cause of recovery are important, both of which are indicative of the health status of the population. The occupancy rate is also a crucial factor, as the higher the occupancy rate, the higher will be the profits, thus enhancing the economic viability of the healthcare unit.
13
The ranking of factors is important to determine the key factors, which if im-proved, can help achieve higher efficiency of a healthcare unit based on a PPP model.
4.5. Suggested Actions
Public Private Partnerships should be taken as innovative joint alliances which function on the joint parameters of risks and rewards with appropriate re-source allocation to meet the needs of public health delivery. It is important to clearly define the input and output factors that ultimately affect the expected outcomes of the venture.
A strategic framework of healthcare delivery through these partnerships needs to be developed. This framework should take into account the varied health needs of the country and the health determinants that can influence and gov-ern the performance of the healthcare delivery system
The key system components or potential areas where partnerships can en-hance the whole system‘s outcomes need to be identified. Once these factors are identified, they can be used to develop Public Private Partnership models that are efficient and provide cost-effective quality health services. These can then be integrated in a comprehensive framework for delivery of healthcare services.
PPPs constitute an area that brings together public and private players to ad-dress common challenges. With the constraints in public healthcare funding versus the health investment needs, the performance improvements versus cost effectiveness; one has to seek an appropriate balance between the healthcare needs of the country and the interests of the private players.
4.6. Expected Performance
By analyzing the factors required for effectiveness of these partnerships, de-ciding upon the radical changes required and then initiating these essential and far-reaching changes will enhance the effectiveness of the Public Private Partnerships. This process can begin by focusing on crucial factors that can enhance the effectiveness, increasing the reach and reducing costs, and en-hancing positive health outcomes.
Once a framework is developed for healthcare delivery through a partnership mechanism, the focus should shift from risks and rewards to a more compre-hensive reason for starting new PPP initiatives. These PPPs should not only provide a means to meet the development agenda, but also be a sustainable and mutually advantageous collaborative arrangement.
This holistic approach through Public Private Partnerships will help develop health care delivery mechanisms that have inclusive strategies to improve the quality of care as well as ensure the sustainability of these partnerships.
14
5. Suggested Road Map
As is evident from above, Public Private Partnerships are emerging as a novel ap-proach for extending the reach and scope of the healthcare delivery systems throughout the world. The government is extending support to the civil society and the civil society and the government is being supported by private companies and corporate entities. This is creating synergistic collaborations with the private sector extending support in terms of finances, technical and managerial expertise for en-hancing healthcare delivery.
A PPP is a collaborative arrangement with give-and-take relationship between two or more parties, with shared goals, defined stakes, and expected outcomes. These con-figurations may define their own structures, processes, set of deliverables, and per-formance indicators. All this needs to be achieved through a set of pre-defined re-sources. With the given set of resources (money, manpower, technology), these partnerships need to bring out the best. Therefore, identification of the factors that improve the efficiency of healthcare delivery via PPPs will be very useful.
6. Conclusion
In this study, we have identified 9 input and 9 output factors that can be considered in calculating the efficiency of a healthcare unit based on PPPs. Ranking of factors has been done based on an exploratory study. This study shows that the input factors important in calculating the efficiency of a healthcare delivery unit are not just the cost of high-end equipment, or the case-mix categories, but rather the number of healthcare professionals (nurses, doctors, and paramedical staff). Similarly, in terms of output, the most important factors are the number of healthy deliveries and dis-charges because of recovery rather than the number of lab cases and average case mix categories, which are of least importance.
The ranking of factors is important to determine the key factors, which if improved, can help achieve higher efficiency of a healthcare unit. In today‘s context, PPPs are contributing in most sectors of development, be it education, health, or telecommuni-cations. This new trend has several advantages over the conventional setups as the expertise of the government and industry is brought together.
As the results of the study show, the presence of healthcare delivery providers is the most crucial input for better functioning of a healthcare unit. In terms of output, the number of healthy deliveries, and discharges because of recovery, both of which are indicative of the health status of the population, are important. Except for doctors, the other two stakeholders did not rank the occupancy rate, which can actually impact the economic viability of a healthcare unit, amongst the top-three output factors. The doctors, however, thought that occupancy rate is the second most crucial output fac-tor to be considered while calculating the efficiency of a healthcare unit based on PPPs.
PPPs are also emerging as a novel approach for extending the reach and scope of the healthcare delivery systems throughout the world. The SAP-LAP analysis clearly
15
shows that PPPs can become one of the most useful models for making quality healthcare services reach the vast majority of people, who are currently denied the basic health services because of the constraints of the existing healthcare delivery structure. The government is extending support to the civil society, and the civil soci-ety and the government is being supported by private companies and corporate houses. This is creating synergistic collaborations with the private sector extending support in terms of finances as well as technical and managerial support for enhanc-ing healthcare delivery services.
7. References
Bhat; R. (1999): Characteristics of private medical practice in India: a provider per-spective. Health Policy and Planning 14, pp. 26-37.
Buse, K.; Waxman, A. (2001): Public–private health partnerships: a strategy for WHO. Bulletin of the World Health Organization 79, pp. 748–754.
Farrell, MJ. (1957): The measurement of productive efficiency. Journal of the Royal Statistical Society 120(3), pp.253-290.
Government of India. (2002): 10th Five Year Plan (2002-2007). Planning Commis-sion of India, available at http://planningcommission.nic.in/plans/planrel /fiveyr/10th/default.htm, last accessed on September 14, 2008.
Government of India. (2005): Report Of The National Commission On Macroeconom-ics And Health, National Commission On Macroeconomics And Health. Min-istry Of Health & Family Welfare, available at http://www.who.int/macro health/action/Report of the National Commission.pdf.
Government of India. (2005): Ministry of Health and Family Welfare, The 10th Five Year Plan, Mission Document - National Rural Health Mission (2005-2012). Available at mohfw.nic.in/NRHM/Documents/ NRHM%20Mission%20 Docu-ment.pdf, last accessed on January 22, 2009.
Government of India. (2007): Report of the working group on public private partner-ship to improve healthcare delivery for the eleventh five-year plan (2007-2012). Planning Commission of India, available at planningcommis-sion.nic.in/aboutus/committee/wrkgrp11/wg11_heasys.doc, last accessed November 30, 2008.
Government of India. (2007): Report On Recommendation Of Task Force On Public Private Partnership For The 11th Plan. Planning Commission of India, avail-able at http://www.planningcommission.nic.in, last accessed on December 2008.
Government of India. (2008): Ministry of Health and Family Welfare website, avail-able at http://www.mohfw.nic.in, last accessed on December 6, 2008.
Government of India. (2008): Report of The Task Force on Medical Education for the National Rural Health Mission, Ministry of Health and Family Welfare avail-
16
able at http://www.mohfw.nic.in/NRHM/Documents/Task_Group_Medical _Education.pdf, last accessed on September 12, 2008.
Kermer, M.; Chaudhury, N; et al. (2004): Teacher and healthcare provider absentee-ism: a multi-country study. The World Bank, available at http://publications.worldbank.org/, last accessed on February 2007.
Kooreman, P. (1984): Nursing home care in the Netherlands: a nonparametric effi-ciency analysis. Journal of Health Economics 13:93, pp. 301-316.
Malmborg, R.; Mann, G.; Thomson, R.; Squire, BS. (2006): Can public-private col-laboration promote tuberculosis case detection amongst the poor and vulner-able? Bulletin of the World Health Organization 84, pp. 752-758.
National Sample Survey Organization (NSSO) 60th Report. (2004): Report No. 507: Morbidity, Health Care and the Condition of the Aged, Jan - June, 2004, available at http://www.mospi.gov.in/mospi_nsso_rept_pubn.htm, last ac-cessed on November 28, 2008.
Organisation for Economic Co-operation and Development. ( 2004): A Global Plan to Achieve the MDGs, Draft report for discussion at the OECD-DAC High-level Consultation on the UN Millennium Project, 8-9 July, 2004. Available at www.norad.no/default.asp?FILE=items/3036/108/Fiscal%20Sustainability%20Feb.doc, last accessed on January 22, 2009.
Osei, D.; d'Almeida, S.; et al. (2005): Technical efficiency of public district hospitals and health centres in Ghana: a pilot study. Cost Effectiveness and Resource Allocation 3, pp. 9.
Peters, DH.; Rao, KS.; Fryatt, R. (2003): Lumping and splitting: the health policy agenda in India. Health Policy and Planning 18(3), pp. 249–260.
Shugarman, LR.; Nicosia N.; Schuster, CR. (2007): Comparing For-Profit and Not-for Profit Health Care Providers: A Review of the Literature. RAND WR-476-MEDPAC, Rand Health. available at http://www.rand.org/pubs/working_ pa-pers /2007/RAND_WR476.pdf, last accessed on November 8, 2008.
Steering Committee for the Review of Commonwealth/State Service Provision. (1997): Data Envelopment Analysis: A technique for measuring the efficiency of government service delivery. AGPS, Canberra, Australia.
Sushil. (2001): SAP-LAP Framework. Global Journal of Flexible Systems Manage-ment 2 (1), pp. 51-55.
The World Bank. (2002): India: Raising the Sights - Better Health Systems for India‘s Poor: Findings, Analysis, and Options, Health, Nutrition, and Population Se-ries. Available at http://publications.worldbank.org/, last accessed on January 2009.
The World Bank. (2004): World Development Report 2004: Making Services Work for Poor People. Available at http://publications.worldbank.org/ ecom-merce/catalog/, last accessed on January 22, 2009.
17
United Nations Economic and Social Council. (2005): Public-Private Partnerships (PPPs) For Service Delivery: Water Supply and Sanitation. Third meeting of the Committee on Human Development and Civil Society, 4-6 May, Addis Ababa, Ethiopia. Available at www.uneca.org/chdcs/chdcs3/ ppps_chdcs_3.pdf, last accessed on January 22, 2009.
Vinod, B.; Annigeri; et al. (2004): Assessment of Public Private Partnership Opportu-nities in India. Poptech Project, USAID. Available at pdf.usaid.gov/pdf_docs/PNADC694.pdf, last accessed on January 22, 2009.
Widdus, R. (2001): Public–private partnerships for health: their main targets, their diversity, and their future directions. Bulletin of the World Health Organization 79, pp. 713–72.
Widdus, R. (2003): Public–private partnerships for health require thoughtful evalua-tion. Bulletin of the World Health Organization 81 (4), pp. 235.
Worthington, AC. (1999): An Empirical Survey Of Frontier Efficiency Measurement Techniques In Healthcare Services. School of Economics and Finance Dis-cussion Papers and Working Papers Series 067, School of Economics and Finance, Queensland University of Technology. Available at http://www.bus.qut.edu.au/faculty/schools/economics/documents/discussionPapers/1999/Worthington_67.pdf, last accessed on November 8, 2008.
Worthington, AC. (2004): Frontier Efficiency Measurement in Healthcare: A Review of Empirical Techniques and Selected Applications. Medical Care Research and Review 61(2), pp. 1-36.
Authors‘ addresses Bharti Birla Research Scholar, University School of Management Studies GGS Indraprastha University, Delhi, India Kashmiri Gate, Delhi 110403, India E-mail: [email protected] Udita Taneja, Ph.D. Associate Professor, University School of Management Studies GGS Indraprastha University, Delhi, India Kashmiri Gate, Delhi 110403, India E-mail: [email protected]