pulmonary arterial hypertension in pediatric opd and icu
TRANSCRIPT
Pulmonary arterial hypertensionwhen to suspect and how to assess
Dr Neeraj AggarwalPediatric Cardiologist
Department of Pediatric Cardiac Sciences Sir Ganga Ram Hospital
Case 1
• 3 year old child • FTT ,lethargy , early tiredness, NYHA dyspnoea class
2-3• Not able to play with peers• 2 episodes of near-syncope• Hepatomegaly and mild distress• Single loud S2 –palpable• Saturations 91 %• F/H –not significant
DD
• Congenital Heart disease - obstructive lesions
• Chronic disorders –Anaemia,Malnutrition
• Chronic lung disease
• PAH ?
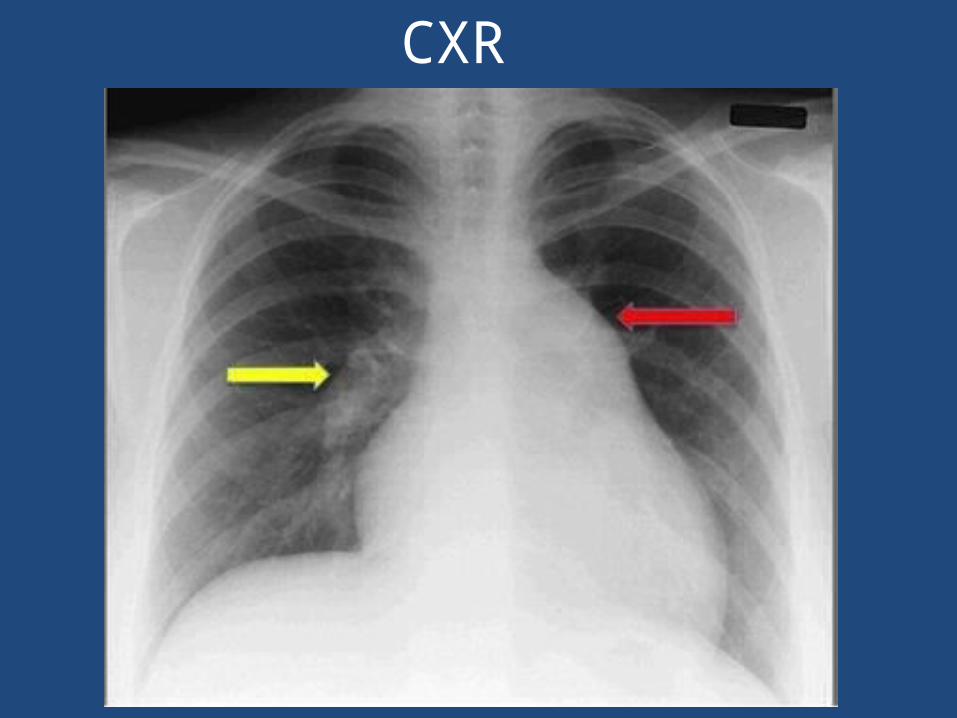
CXR
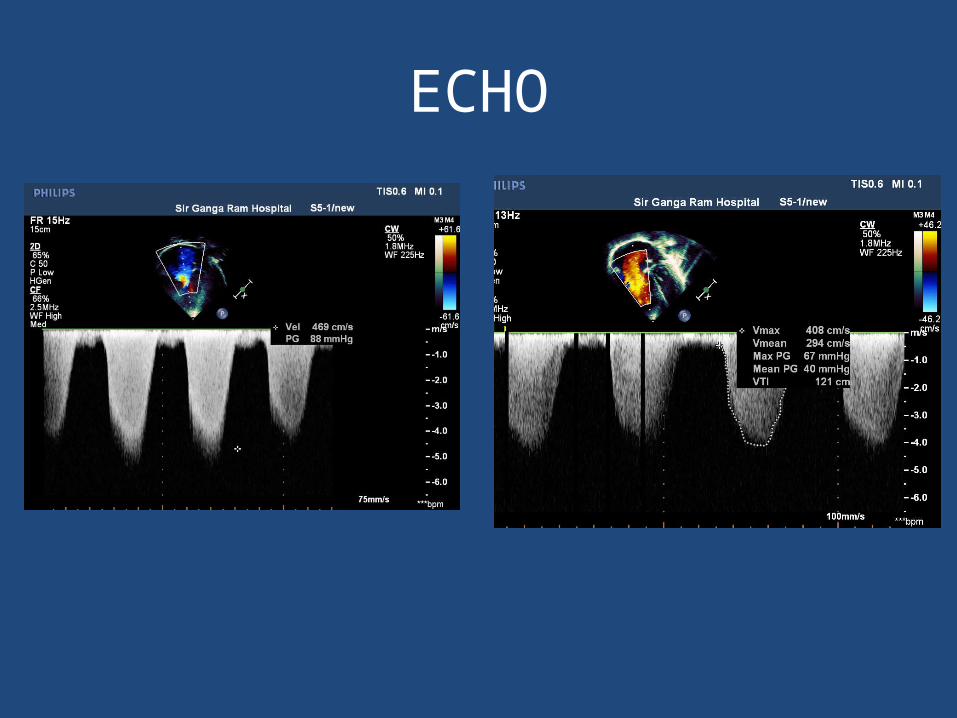
ECHO
• Severe PAH ,TR moderate (PG 80 mmhg)
• Dilated RA RV
• RV mild dysfunction
• No pericardial effusion
Case 2
• 4 yr old male • History of LRTI - admitted outside• Left pleural effusion, resp distress, bilateral chest
pain • Septic markers positive , received IV antibiotics
for 7 days but not better • Echo for associated pericardial effusion - severe
PAH• CT showed multiple small emboli on both sides
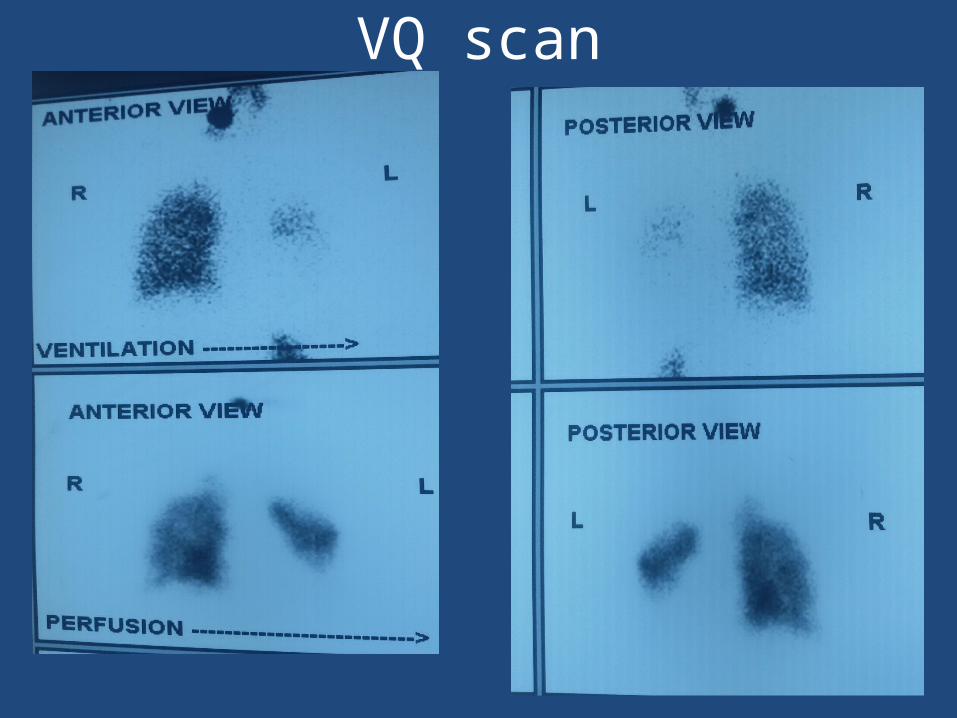
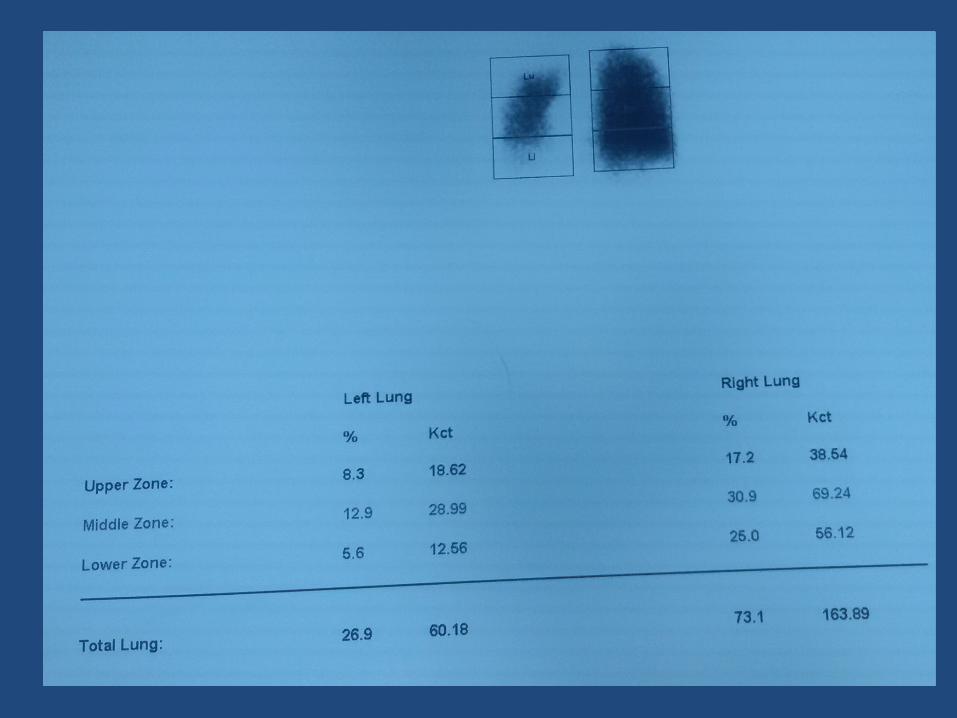
VQ scan
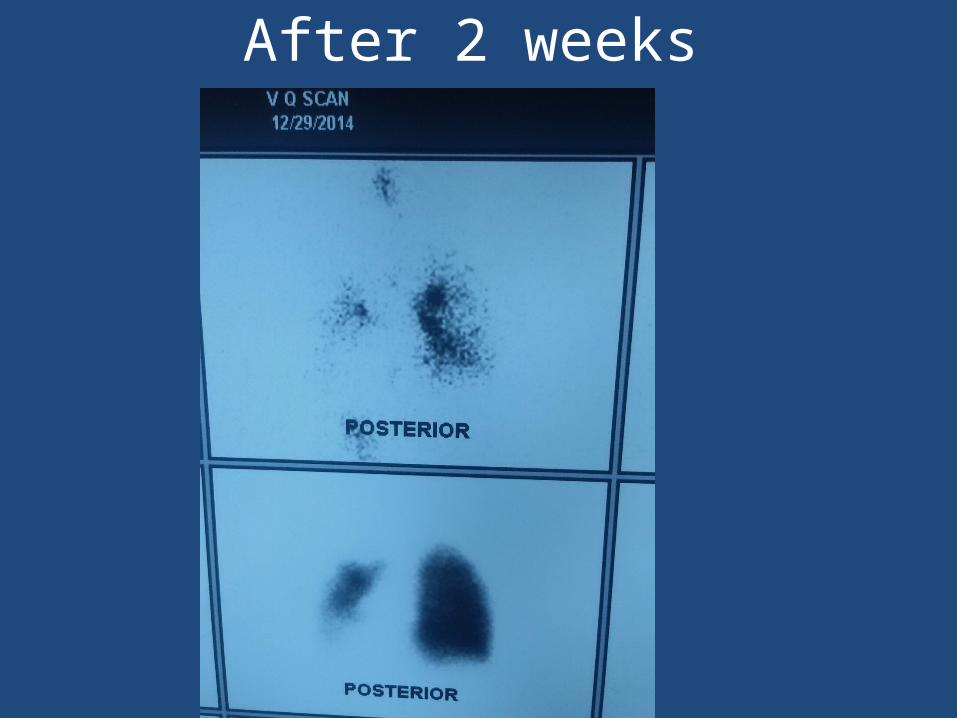
After 2 weeks

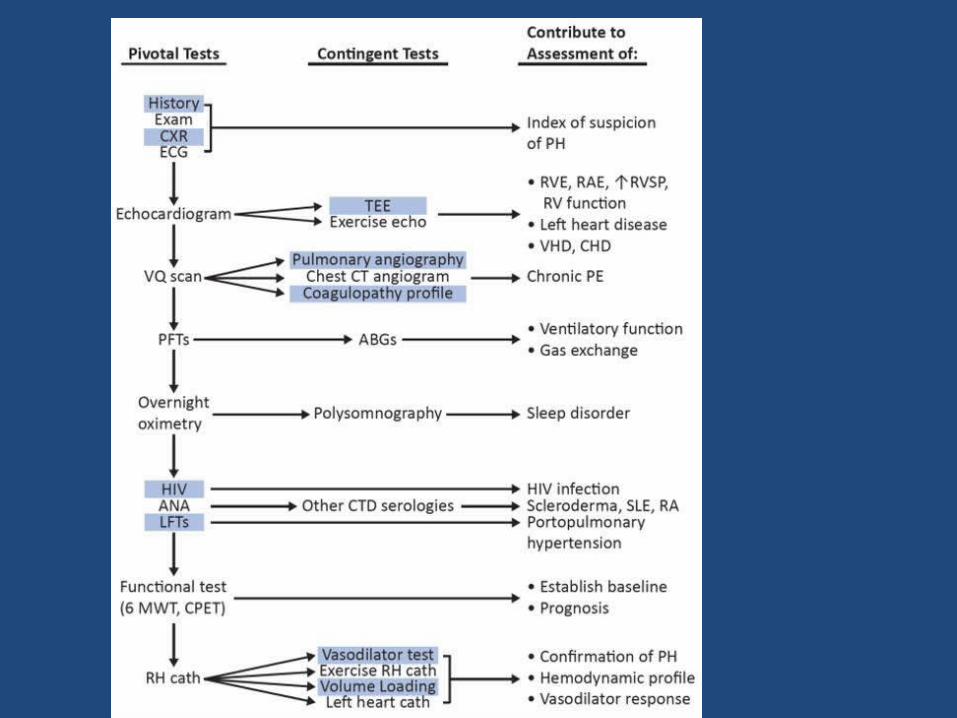
Badesch D et al. J Am Coll Cardiol. 2009;54:S55-S66.McLaughlin VV et al. J Am Coll Cardiol. 2009;53:1573-1619.
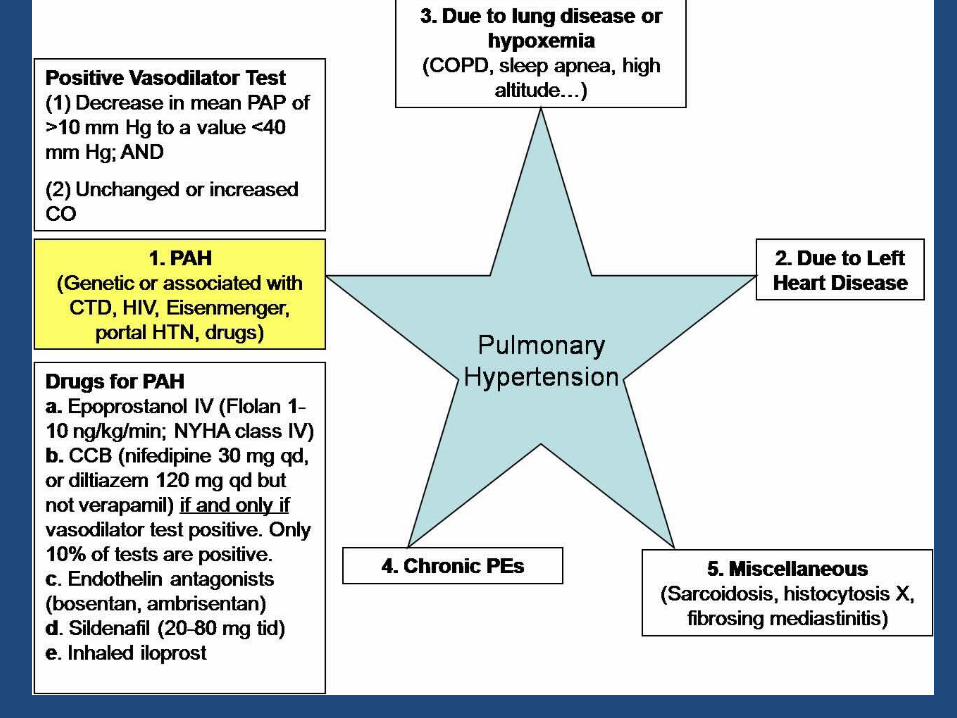
Hemodynamic Definition of PH/PAH
PH
PAH Mean PAP ≥25 mm Hg +PCWP/LVEDP ≤15 mm Hg (absence of LV dysfucntion)
Mean PAP ≥25 mm Hg
AHA includes PVR >3 Wood Units


3. PH Owing to Lung Diseases and/or Hypoxia•COPD ,ILD•Other pulmonary diseases with mixed rest. and obst. pattern•Sleep-disordered breathing•Alveolar hypoventilation disorders•Chronic exposure to high altitude•Developmental abnormalities
4. Chronic Thrombo embolic pulmonary hypertension
5. PH With Unclear Multifactorial Mechanisms Hematologic disorders (Myeloproliferaive disorders, splenectomy)•Systemic disorders -Sarcoidosis,histiocytosis,lymphangio-leiomyomatosis, Thyroid disorders, Renal failure/ dialysis, fibrosing mediastinitis,)

When to Suspect and Screen for PAH• Family history
– 6% - 12% prevalence of positive family history
• Connective tissue disease– Scleroderma: 8%- 30%– Raynaud phenomenon : up to 20% - 25% – SLE: 4% - 14%– Rheumatoid arthritis up to 21%
• Congenital Heart Disease– Reversal of left-to-right shunt– VSD ,PDA, AP window, Atrial Septal Defect
When to Suspect and Screen for PAH
• Portal hypertension -Nearly 10% have PAH
• Deep venous thrombosis/history of pulmonary embolism
– Up to 3-4% of survivors
• Appetite suppressant or stimulant use
• HIV ---- 0.5% pts
• Hemolytic anaemia

When to Suspect and Screen for PAH
• PAST HISTORY OF RHD—Mitral stenosis
• Poorly controlled HT –Look for LV diastolic dysfunction
• Snoring at night –sleep apnoea

How to suspect
• Non specific symptoms• I am a difficult case of asthma• I was fat
Non specific complaints
• Dyspnoea• Syncope • Dizziness• Fatigue • Oedema• Angina

Infants and young
• Takes frequent naps• Poor appetite• Growth restriction• Hesitant and un adventurous• Not interacting with family• Undue fatigue while playing with kids• Dressing /toilet –undue fatigue /syncope• Regression of newly learned activities
SIGNS
• Loud P2• RV lift• Murmur of TR• Signs of CHF

ECG-RAD RVH RAE RBBB


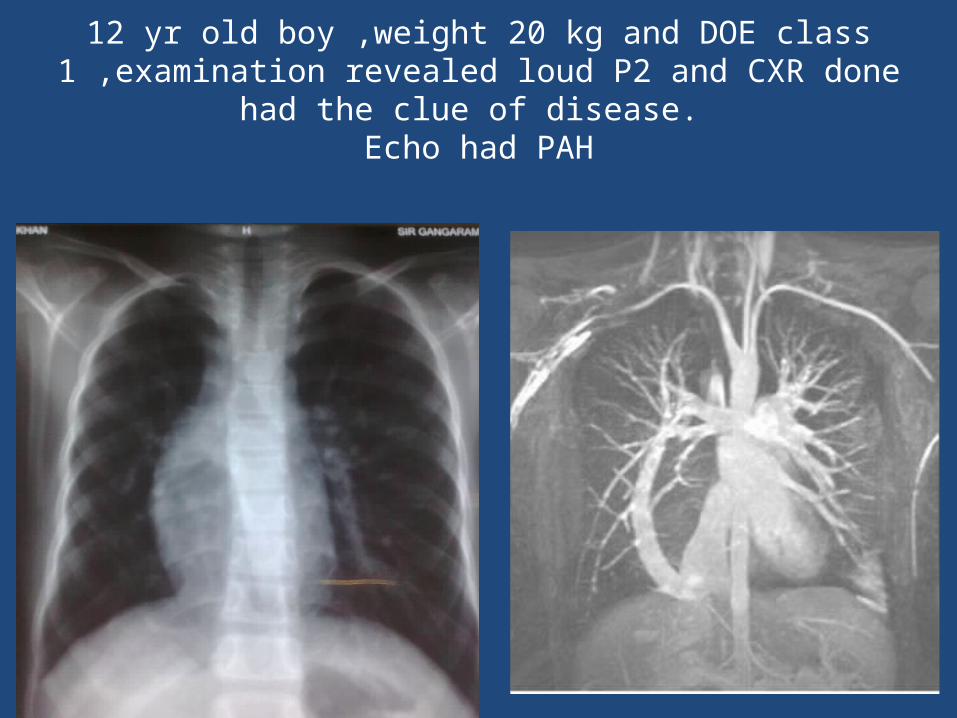
12 yr old boy ,weight 20 kg and DOE class 1 ,examination revealed loud P2 and CXR done had the clue of disease.
Echo had PAH

Patient evaluation
ECHO• RV size and RVH• TR,PR,IVS movement to left side• Reduced RVOT acceleration time• IVC dilatation,not collapsing with respiration
and flow reversal• Dilated pulmonary arteries• Left sided lesions –LA size dilataion• Pulm veno-occlusive disease,shunts

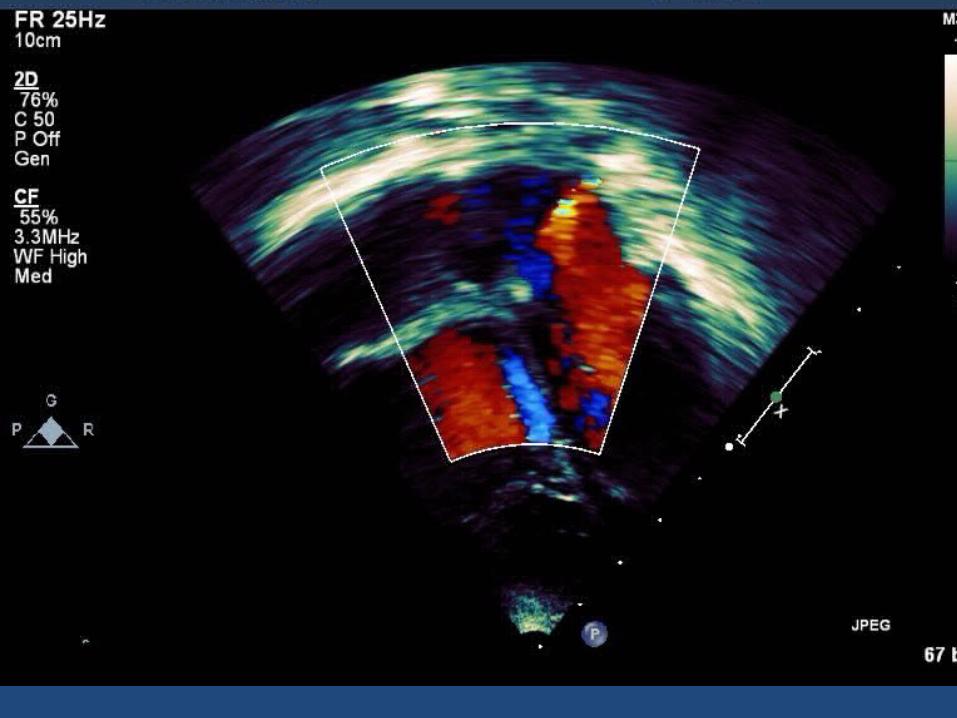
ECHO
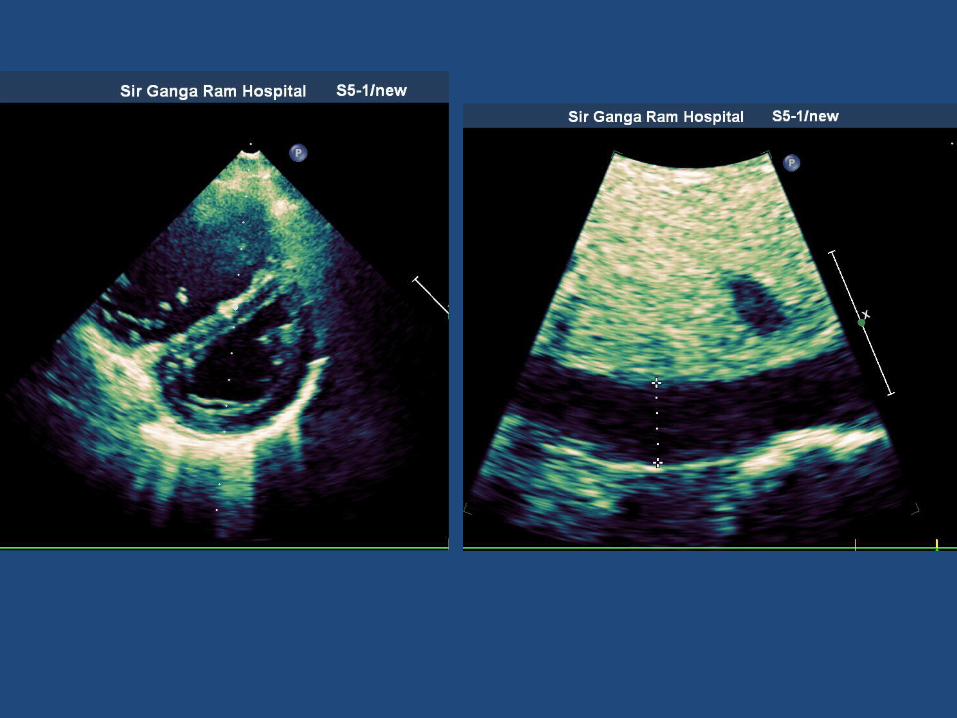
ECHO
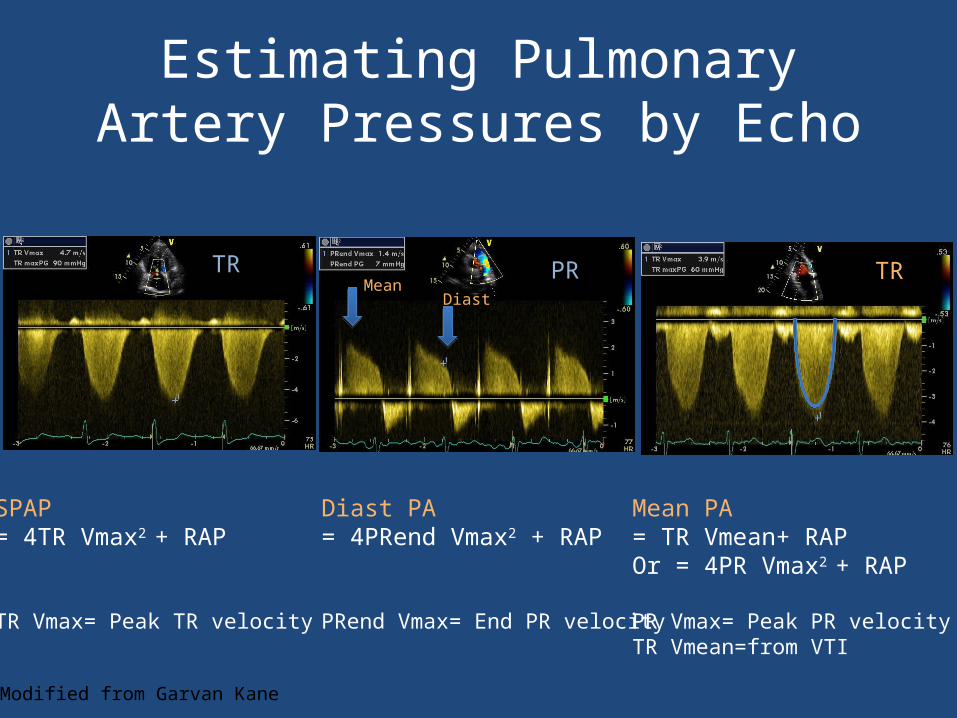
Estimating Pulmonary Artery Pressures by Echo
SPAP= 4TR Vmax2 + RAP
TR Vmax= Peak TR velocity
Diast PA= 4PRend Vmax2 + RAP
PRend Vmax= End PR velocity
TR TRPRMean
Diast
2*
Mean PA= TR Vmean+ RAPOr = 4PR Vmax2 + RAP
PR Vmax= Peak PR velocityTR Vmean=from VTI
Modified from Garvan Kane
TR
limitations of echo
• Experience
• Images can be limited
• The RV, the chamber of highest concern in PAH, is the least emphasized on the “standard” echocardiography exam
• TR jet may be absent in some patients, thus precluding PASP assessment
• May overestimate or underestimate actual pulmonary arterial pressure
• Can estimate LVEDP (PCWP) or CO but may prove impractical

Missed shunts as PAH


Cath
• ACCURACY
• CALCULATION OF PVR
• LEFT SIDED FILLING PRESSURES BY WEDGE


Therapeutic interventions3 pathways

Aim of treatment
• Dilate and reverse the abnormal remodeling of the pulmonary vascular bed and to restore endothelial function
• by acting on the prostacyclin, endothelin and NO pathways
Prostacyclin pathway
• Potent vasodilator in both the pulmonary and systemic circulations
• Anti-proliferative properties • IV prostacyclin (epoprostenol) infusion• Treatment of choice for severely ill patients
Nitric oxide pathway
• Nitric oxide is a potent pulmonary vasodilator, inhibitor of platelet activation and vascular
smooth muscle cell proliferation.
• The effects of NO are mediated via cGMP in vascular smooth muscle cells regulated by phosphodiesterases
• Sildenafil is a PDE-5 inhibitor• Tadafil –long acting
Endothelin pathway
• Endothelin-1 one of the most potent vasoconstrictors and smooth-muscle cell
mitogens• Endothelin receptor antagonists (ERAs) • Selective ERA-Sitaxsentan and Ambrisentan
(less hepatotoxic)• Nonselective-for the ETA and ETB receptors,
(Bosentan)-monthly SGOT/SGPT, quarterly Hb
Management
• NYHA class 1,2 (either of )Sildenafil,
bosentan, Ambrisentan
• NYHA class 3 combination of sildenafil ,
bosentan ,ambrisentan , (iv epoprostenol in
some cases)
• NYHA class 4 iV epoprostenol +others •
Management
• Supportive –controlled diuresis, digoxin, oxygen (Target sats >90)
• Avoid exertion, pregnancy, high altitudes
• Combination therapy
• Inadequate response –Atrial septostomy, lung transplant
COMPLICATIONS OF PULMONARY VASODILATORS
• PAH due to lv dysfunction—pulmonary
oedema
• Severe interstitial fibrosis /emphysema—
worsen V/Q mismatch
• Chronic Thromboembolism – delay Treatment

Evaluation in a PH substrate Family history (gene mutation proved) Annual ECHO
Systemic sclerosis Annual ECHO
Sickle cell /thal intermedia Annual echo
HIV If s/s of PAH- echo
Portal HT If liver transplant /symptoms - ECHO
Prior appetite suppressant use Echo If s/s present
CHD ECHO regularly
Recent acute pulm embolism V/Q scan after 3 months