pulmonary complications in a child with aml children’s hospital & research center oakland...
TRANSCRIPT
Pulmonary complications in a
child with AML
CHILDREN’S HOSPITAL & RESEARCH CENTER OAKLAND
Hazel Villa, MD

Background•LC,11 y/o girl
•AMLM1 at 20 months old
•1st transplant (BMT) at 2 y/o–HLA-matched sibling donor
•Recurrent cutaneous disease at 3 y/o
• 2nd transplant peripheral stem cell at 3 y/o-same sibling donor

Background
First transplant: BMT 1.Induction chemotherapy: Idarubicin, Ara-C,
Etoposide, 6-thioguanine, dexamethasone
2. Preparation for transplant: myeloablation with : Busulfan, CyclophosphamideCytoxan
3. Prophylaxis for GVHD: Methotrexate

Background
2nd transplant : peripheral stem cell transplant ( She had cutaneous relapse)
1.Preparation for SCT: total body irradiation chemotherapy with: Etoposide, cyclophosphamide
2.GVHD prevention with Methotrexate

Background
10/2003-1/2004 (5 months post SCT)
Chronic GVHD!!!
•Oral lesionsbudesonide topical•Crackles- chest CT: mosaic perfusion
•Flovent 44 2 puffs BID•Cyclosporine

2-4 years after 2nd transplant ( Patient is 4-6 years of age)
•Asymptomatic
• PFT FVC 94 pre FEV1 68 post FEV1 74 FEV1/FVC 62 TLC 142 RV 259 DLCO- normal
Flovent BID /Albuterol MDI prn


What do you see?

Disease Progression
7 years post 2nd transplant ( patient was 10 y/o)
•Admitted from the ED for respiratory distress•Treated for community acquired pneumonia

% predicted


Patient was re-admitted
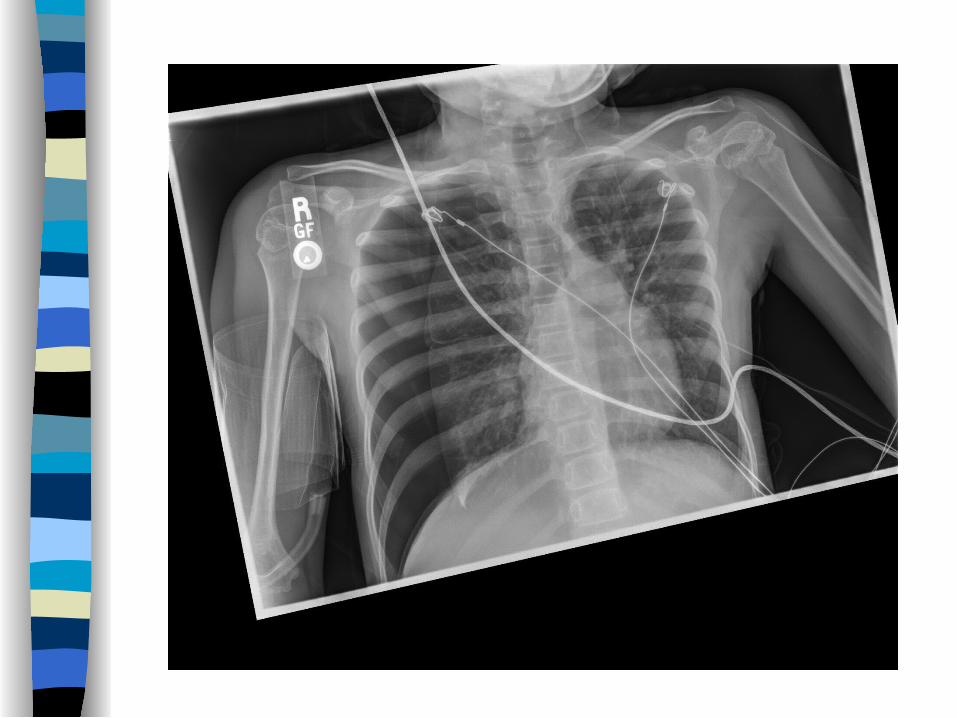
* CXR –increased infiltrates on the right* Chest CT :

What do you think of the CT?

* Flexible bronchoscopy: normal anatomy
* BAL: AFB result was pending, NURF
• Treatment intensified
* Plan to start azithromycin for BO, if TB negative

•BAL : Mycobacterium kansasii
•Quantiferon Gold –negative•INH, RIF, EMB* Airway clearance therapy was continued



What is your next step?

?
BOS or BOOP/COP
INFECTIONBOS/BOOP PROGRESSION
REMOVE THE CYST OR NOT

Patient came back…
Pulmonary Plan:
* Agree with immunosuppression if (-) pneumothorax, (-) chest tube
* Resection of the enlarging cyst. (Blebectomy preferred, pt has low lung reserve)
* NO pleurodesis for recurrent pneumothorax, if lung transplant is an option
* Favor Azithromycin (BOS/ NTB) Prednisone (BOS/Immunosuppresion)

Course: * Underwent blebectomy- lung tissue sent for histopathology* No recurrence of pneumothorax post-blebectomy* Started on cyclosporine and prednisone* Now 4-drug treatment for M. kansasii (+ Azithromycin)
Outpatient follow up: 10/4/10* Pt doing well.* Started on cyclosporine and prednisone per Heme- Oncology

•No evidence of recurrent AML•Areas of obliterated bronchioles show mature collagenous fibrosis•No interstitial scarring in most of the damaged airways. •No features of cryptogenic organizing pneumonia (COP).
Histopathological Report
ORGANIZING FIBRINOUS PLEURITISCONSISTENT WITH PNEUMOTHORAX
OBLITERATIVE BRONCHIOLITIS CONSISTENT WITH PULMONARY GRAFT VERSUS HOST DISEASE

Any other thoughts?

Thank youvery much!!!