pulmonary rehabilitation for chronic obstructive pulmonary ... · pulmonary rehabilitation for...
TRANSCRIPT

Supporting Informed Decisions
Pulmonary Rehabilitation for ChronicObstructive Pulmonary Disease: Clinical,Economic, and Budget Impact Analysis
t e c h n o l o g y r e p o r t
Canadian Agency forDrugs and Technologies
in Health
Agence canadienne des médicaments et des technologies de la santé
HTAIssue 126
March 2010
H0482_COVER_for print_20th.ai 1 3/24/2010 1:28:17 PM
Until April 2006, the Canadian Agency for Drugs and Technologies in Health (CADTH) was known as the Canadian Coordinating Office for Health Technology Assessment (CCOHTA).
Cite as: Hailey D, Jacobs P, Stickland M, Chuck A, Marciniuk DD, Mayers I, Mierzwinsky-Urban M. Pulmonary Rehabilitation for Chronic Obstructive Pulmonary Disease: Clinical, Economic, and Budget Impact Analysis [Technology report number 126]. Ottawa: Canadian Agency for Drugs and Technologies in Health; 2010. Production of this report is made possible by financial contributions from Health Canada and the governments of Alberta, British Columbia, Manitoba, New Brunswick, Newfoundland and Labrador, Northwest Territories, Nova Scotia, Nunavut, Prince Edward Island, Saskatchewan, and Yukon. The Canadian Agency for Drugs and Technologies in Health takes sole responsibility for the final form and content of this report. The views expressed herein do not necessarily represent the views of Health Canada or any provincial or territorial government. Reproduction of this document for non-commercial purposes is permitted provided appropriate credit is given to CADTH. CADTH is funded by Canadian federal, provincial, and territorial governments. Legal Deposit – 2010 National Library of Canada ISBN: 978-1-926680-38-5 (print) ISBN: 978-1-926680-39-2 (online) H0482 – March 2010 PUBLICATIONS MAIL AGREEMENT NO. 40026386 RETURN UNDELIVERABLE CANADIAN ADDRESSES TO CANADIAN AGENCY FOR DRUGS AND TECHNOLOGIES IN HEALTH 600-865 CARLING AVENUE OTTAWA ON K1S 5S8
Publications can be requested from:
CADTH 600-865 Carling Avenue
Ottawa ON Canada K1S 5S8 Tel. (613) 226-2553 Fax (613) 226-5392
Email: [email protected]
or downloaded from CADTH’s website: http://www.cadth.ca
Canadian Agency for Drugs and Technologies in Health
Pulmonary Rehabilitation for Chronic Obstructive Pulmonary Disease: Clinical, Economic, and Budget Impact Analysis
David Hailey, MSc PhD Grad RIC1 Philip Jacobs, DPhil2
Michael Stickland, PhD2 Anderson Chuck, MPH PhD2
Darcy D. Marciniuk, MD, FRCP(C), FCCP3 Irvin Mayers, MD, FRCPC2
Monika Mierzwinski-Urban, MLIS4
March 2010
1 Institute of Health Economics, Edmonton, Alberta 2 University of Alberta, Edmonton, Alberta 3 University of Saskatchewan, Saskatoon, Saskatchewan 4 Canadian Agency for Drugs and Technology in Health, Ottawa, Ontario
PR for COPD: Clinical, Economic, and Budget Impact Analysis i
Reviewers
External Reviewers
These individuals kindly provided comments on this report.
Paul Hernandez, MDCM FRCPC Associate Professor of Medicine, Dalhousie University Halifax, Nova Scotia
Michelle McIsaac, MA Health Economist, University of Melbourne Victoria (Parkville), Australia
W. Darlene Reid, BMR(PT) PhD Professor, Department of Physical Therapy, University of British Columbia Vancouver, British Columbia
Ron Goeree, MA Associate Professor, Clinical Epidemiology & Biostatistics, McMaster University Director, PATH Research Institute, St. Joseph’s Healthcare Hamilton Hamilton, Ontario
Nick Barrowman, PhD Senior Scientist, Children’s Hospital of Eastern Ontario Clinical Research Institute Ottawa, Ontario
CADTH Peer Review Group Reviewers
Robert Dales, MD MSc FRCPC Professor of Medicine, University of Ottawa The Ottawa Hospital Ottawa, Ontario
Chris Skedgel, MDE Research Health Economist, Department of Medicine Dalhousie University Halifax, Nova Scotia
This report is a review of existing public literature, studies, materials, and other information and documentation (collectively the “source documentation”),which are available to CADTH. The accuracy of the contents of the source documentation on which this report is based is not warranted, assured, or represented in any way by CADTH and CADTH does not assume responsibility for the quality, propriety, inaccuracies, or reasonableness of any statements, information, or conclusions contained in the source documentation. CADTH takes sole responsibility for the final form and content of this report. The statements and conclusions in this report are those of CADTH and not of its Panel members or reviewers. Authorship
David Hailey coordinated the project, steered the preparation of the protocol, and integrated the components of the study. He led and drafted the clinical review, contributed to the economic analysis, and coordinated the response to reviewers’ comments.
PR for COPD: Clinical, Economic, and Budget Impact Analysis ii
Philip Jacobs developed the study plan, was responsible for the review of economic literature, steered development and use of the economic model, and drafted the economic analysis and budget impact sections. Michael Stickland participated in the clinical review, including study selection, data extraction, and quality assessment. He provided advice on the economic review and aspects of the economic analysis. Anderson Chuck contributed to the review of economic studies, developed the economic analysis model and budget impact analytic framework, and contributed to the drafting of the economic analysis and budget impact sections. Darcy Marciniuk contributed to the preparation of clinical sections of the report, including provision of advice on practice guidelines, and contributed to the economic analysis. Irvin Mayers contributed to the development and preparation of the clinical review and provided clinical input to the economic model. Monica Mierzwinski-Urban prepared the literature search strategy, performed literature searches, wrote the methods section on literature searching, and verified references. Acknowledgment
The authors acknowledge the contribution of Sarah McGill for providing referencing support and a quality check of the references in the final version of the report. Conflicts of Interest Dr. Paul Hernandez is the Medical Director of the Pulmonary Rehabilitation Program at the Capital District Health Authority. He is also a member of the COPD and Pulmonary Rehabilitation Committee with the Canadian Thoracic Society. Dr. Michael Stickland received a speaker’s honorarium from GlaxoSmithKline Inc.

PR for COPD: Clinical, Economic, and Budget Impact Analysis iii
PR for COPD: Clinical, Economic, and Budget Impact Analysis iv
EXECUTIVE SUMMARY
The Issue
Chronic obstructive pulmonary disease (COPD) causes disability and impaired quality of life. In 2006, more than 10% of all hospitalizations in Canada were due to COPD. Pulmonary rehabilitation (PR) can be used to assist in the management of COPD. In Canada, there is poor access to PR because of limited program capacity. Policy-makers and health care providers need advice to help with decision-making about the future establishment and use of PR programs. Information on the cost-effectiveness, budget impact, and operational needs of PR programs and the impact of program elements on clinical outcomes would be helpful for decision-makers. Objectives
The objectives of this assessment were to evaluate the effect of PR programs for COPD on clinical and economic outcomes, and to assess their health services impact. The research questions were: What is the clinical effectiveness of PR and pharmacotherapy (together) compared with
pharmacotherapy alone for adults with COPD? What is the effectiveness of specific elements of PR programs for adults with COPD? What is the cost-effectiveness of PR and pharmacotherapy compared with pharmacological
therapy alone in adults with COPD? What is the health services impact of implementing PR for adults with COPD in Canada? What are the recommendations for the use of PR in current COPD clinical practice guidelines
that are relevant to the Canadian context? Methods
Literature searches were conducted to obtain clinical and economic data using bibliographic databases and grey literature sources. Systematic reviews of clinical and economic literature were undertaken. Recommendations and judgments on evidence were extracted from relevant clinical practice guidelines. A cost-effectiveness analysis was undertaken to compare the costs and health outcomes of usual care (pharmacotherapy) to the costs and health outcomes of usual care plus PR. PR consisted of three sessions per week at 2.5 hours per session over six weeks. A health system perspective was taken. In the budget impact analysis, COPD prevalence data were used to estimate the number of patients recommended to receive PR. The desired capacity for PR in each year is estimated as current capacity plus the number of additional persons served each year. The budget impact of the additional services was estimated by multiplying the unit cost of PR by the additional persons served per year. A time horizon of ten years was used.
PR for COPD: Clinical, Economic, and Budget Impact Analysis v
Clinical Effectiveness of Pulmonary Rehabilitation
The studies that are included in this review showed that, when compared with the usual care (pharmacotherapy) of patients with stable COPD, PR plus usual care is effective in the short term (up to three months), as indicated by improvement in exercise capacity, health-related quality of life (HRQL), and mental health. In some studies, however, the improvements in outcomes were below the minimal clinically important differences. Some longer-term studies found that the benefits from the use of PR disappeared in 12 months or less. Others found that the benefits were sustained for two to three years. Reductions in health care utilization, as indicated by the number of hospital admissions or the length of stay, were reported in studies of variable quality. The findings suggested that patients with COPD can benefit from the use of PR regardless of age, sex, and disease severity. Home-based PR programs provided similar benefits to those obtained from hospital outpatient PR programs. The appropriate duration and content of PR programs is unclear. Information on comparisons of PR with other treatments and on the effectiveness of components of PR programs was limited. Four clinical practice guidelines were identified as being relevant to Canada. Common themes included support for the use of PR for patients with COPD who have dyspnea and reduced exercise capacity, and the inclusion of education as a component of PR. Economic Analysis
If the duration of efficacy of PR is 18 months, the incremental cost-effectiveness ratio of usual care plus PR compared with usual care is $27,924 per additional quality-adjusted life-year (QALY) gained. Health Services Impact
If it is assumed that only the moderate and severe cases need PR, then 1,505 additional persons would be served annually in Canada over a ten-year period for an added annual cost of $1.8 million. If 25% of persons with COPD need PR, this cost would rise to $33.9 million annually for 100% uptake or $19 million if 67% of those who are in need used the services. If all persons with COPD needed PR, the additional annual cost would be $168 million. Conclusions
The use of PR improves short-term exercise capacity, HRQL, and mental health outcomes for patients with COPD. More work is needed to confirm the factors that contribute to the successful long-term management of COPD after PR. There is limited information on the effectiveness of specific elements of PR programs. There are issues relating to patient characteristics and the operation of PR and maintenance programs that require consideration by those who establish or implement these services.
The cost-effectiveness of PR will depend on the duration of benefits. If the duration of the efficacy of PR is18 months, the incremental cost-effectiveness ratio or ICER of usual care plus PR compared with usual care is $27,924 per additional QALY gained. In the most likely scenario from the budget impact analysis, an additional 15,900 persons per year would need PR, and an additional budget of $19 million would be required annually.
PR for COPD: Clinical, Economic, and Budget Impact Analysis vi
TABLE OF CONTENTS
EXECUTIVE SUMMARY ............................................................................................................. iv ACRONYMS AND ABBREVIATIONS ......................................................................................viii 1 INTRODUCTION...................................................................................................................1
1.1 Background and Setting in Canada...............................................................................1 1.2 Overview of Technology................................................................................................2
2 ISSUE ...................................................................................................................................3 3 OBJECTIVES .......................................................................................................................3 4 CLINICAL REVIEW ..............................................................................................................4
4.1 Methods.........................................................................................................................4 4.1.1 Literature searches..........................................................................................4 4.1.2 Selection criteria ..............................................................................................5 4.1.3 Selection method.............................................................................................5 4.1.4 Data extraction strategy...................................................................................5 4.1.5 Strategy for validity assessment......................................................................6 4.1.6 Data analysis methods ....................................................................................6
4.2 Results ..........................................................................................................................7 4.2.1 Quantity of research available .........................................................................7 4.2.2 Study characteristics .......................................................................................7 4.2.3 Clinical practice guidelines ............................................................................22 4.2.4 Data analyses and synthesis.........................................................................22 4.2.5 Elements of PR programs .............................................................................25
5 ECONOMIC ANALYSIS .....................................................................................................26
5.1 Review of Economic Studies: Methods .......................................................................26 5.1.1 Literature searches........................................................................................26 5.1.2 Selection criteria ............................................................................................26 5.1.3 Selection method...........................................................................................26 5.1.4 Data extraction strategy.................................................................................27 5.1.5 Strategy for quality assessment ....................................................................27 5.1.6 Data analysis methods ..................................................................................27
5.2 Review of Economic Studies: Results.........................................................................28 5.2.1 Results of search strategy .............................................................................28 5.2.2 Review of pulmonary rehabilitation versus no rehabilitation..........................28 5.2.3 Summary of results........................................................................................31
5.3 Primary Economic Evaluation: Methods......................................................................32 5.3.1 Type of economic evaluation.........................................................................32 5.3.2 Target population...........................................................................................32 5.3.3 Comparators..................................................................................................32 5.3.4 Perspective....................................................................................................32 5.3.5 Effectiveness .................................................................................................32 5.3.6 Time horizon..................................................................................................33 5.3.7 Modelling .......................................................................................................33 5.3.8 Valuing outcomes ..........................................................................................35
PR for COPD: Clinical, Economic, and Budget Impact Analysis vii
5.3.9 Resource use and costs ................................................................................35 5.3.10 Discount rate .................................................................................................36 5.3.11 Variability and uncertainty .............................................................................36
5.4 Primary Economic Evaluation: Results .......................................................................39 5.4.1 Analysis and results.......................................................................................39
6 HEALTH SERVICES IMPACT............................................................................................42
6.1 Population Impact........................................................................................................42 6.2 Budget Impact .............................................................................................................42
6.2.1 Method...........................................................................................................42 6.3 Planning, Implementation, Utilization, and Legal or Regulatory Considerations........46 6.4 Ethical Considerations.................................................................................................46
6.4.1 Efficiency versus equity .................................................................................46 6.4.2 Process or procedural issues ........................................................................47
7 DISCUSSION......................................................................................................................47
7.1 Summary of Results ....................................................................................................47 7.2 Strengths and Weaknesses of This Assessment ........................................................49 7.3 Generalizability of Findings .........................................................................................50 7.4 Knowledge Gaps.........................................................................................................50
8 CONCLUSIONS..................................................................................................................51 9 REFERENCES....................................................................................................................52 APPENDIX 1: Literature Search Strategy APPENDIX 2: Clinical Studies Data Collection Form APPENDIX 3: Quality Assessment Instrument for Clinical Studies APPENDIX 4: Quality Assessment Form for RCTs APPENDIX 5: Tables for Clinical Review APPENDIX 6: Material from Clinical Practice Guidelines APPENDIX 7: Economic Studies Data Extraction Form APPENDIX 8: Economic Studies that Compared PR to No Rehabilitation APPENDIX 9: Budget Impact Analysis Model Results APPENDIX 10: Excluded Publications
PR for COPD: Clinical, Economic, and Budget Impact Analysis viii
ACRONYMS AND ABBREVIATIONS
ACCP American College of Chest Physicians
AACPR American Association of Cardiovascular and Pulmonary Rehabilitation
ADL activities of daily living
BODE BODE index for COPD (Body mass index, airflow Obstruction, Dyspnea, Exercise Capacity)
BPQ Breathing Problems Questionnaire
CAO chronic airflow obstruction
CET cycle endurance test
COPD chronic obstructive pulmonary disease
COPM Canadian Occupational Performance Measure
CRQ Chronic Respiratory Disease Questionnaire
CTS Canadian Thoracic Society
ESWT Endurance Shuttle Walk Test
FEV1 forced expiratory volume in one second
FFM functionally active fat-free mass
GOLD Global Initiative for Chronic Obstructive Lung Disease
HADS Hospital Anxiety and Depression Scale
HRQL health-related quality of life
HTA Health Technology Assessment
ICER incremental cost-effectiveness ratio
IMT INSPIRATory muscle training
ISWT incremental shuttle walking test
ITT maximal incremental treadmill test
LABA long-acting beta agonist
LVRS lung volume reduction surgery
Maugeri RFQ Maugeri Foundation Respiratory Failure Questionnaire (MRF-28)
MCID minimal clinically important difference
MET metabolic equivalent task
MRF-28 Maugeri Foundation Respiratory Failure Questionnaire
NETT National Emphysema Treatment Trial
NIPPV non-invasive positive pressure ventilation
PR for COPD: Clinical, Economic, and Budget Impact Analysis ix
NNT number needed to treat
NRCT non-randomized controlled trial
NSD no significant difference
PEFR peak expiratory flow rate
PFSDQ-M Modified Pulmonary Functional Status and Dyspnea Questionnaire
PR pulmonary rehabilitation
QALY quality-adjusted life-year
QLI quality of life index
QWB Quality of Well-Being Scale
RCT randomized controlled trial
SF-36 Short Form (36) Health Survey
SGRQ St. George’s Respiratory Questionnaire
SOBQ San Diego Shortness of Breath Questionnaire
STAI State-Trait Anxiety Inventory
TDI Transition Dyspnea Index
3MWD three-minute walk distance
6MRT six-minute ring test
6MWD six-minute walk distance
6MWT six-minute walk test
PR for COPD: Clinical, Economic, and Budget Impact Analysis 1
1 INTRODUCTION
1.1 Background and Setting in Canada
Chronic obstructive pulmonary disease (COPD) is a condition that is characterized by airflow obstruction. The airflow obstruction is usually progressive, not fully reversible, and does not change over months. COPD is predominantly caused by smoking. The airflow obstruction is due to a combination of airway and parenchymal damage as the result of chronic inflammation that differs from that seen in asthma. COPD is associated with symptoms, disability, and impaired quality of life, all of which may respond to pharmacological and other therapies. In some cases, these therapies have limited or no impact on the airflow obstruction.1,2 Of adults over the age of 34 years who were surveyed in the Canadian Community Health Survey of 2005, 4.4% reported that they had been diagnosed with COPD by a health professional.1 The results from Austria indicate that the prevalence of COPD may be underestimated by at least 50% in individuals 40 years of age and over when self-reported physician-diagnosed COPD is used as a measure.1 Consequently, these figures may under-represent the actual prevalence of COPD.1 For adults over the age of 65 years — the largest hospitalized group in Canada — over 10% of all hospitalizations in 2006 were due to COPD. In 2004, COPD was the cause of 4% of all deaths in Canada.1 The goals of COPD management are to prevent disease progression, reduce frequency and severity of exacerbations, alleviate breathlessness and other respiratory symptoms, improve exercise tolerance and daily activity, treat exacerbations and other complications, improve health status, and reduce mortality.2 The means to achieve these goals is the optimized use of pharmacologic and non-pharmacologic interventions. Both are effective and have independent benefits for the patient.2 An option for optimizing the non-pharmacologic management for many patients with COPD is pulmonary rehabilitation (PR).2 The American Thoracic Society and the European Respiratory Society have defined PR as “an evidence-based, multidisciplinary, and comprehensive intervention for patients with chronic respiratory diseases who are symptomatic and often have decreased daily life activities. Integrated into the individualized treatment of the patient, pulmonary rehabilitation is designed to reduce symptoms, optimize functional status, increase participation, and reduce health-care costs through stabilizing or reversing systemic manifestations of the disease. Comprehensive pulmonary rehabilitation programs include patient assessment, exercise training, education, and psychosocial support.”3 The 2007 Canadian Thoracic Society (CTS) guidelines outlined a comprehensive approach to the chronic management of COPD, starting with inhaled bronchodilators. Other therapies may include inhaled corticosteroids, inspired oxygen, and surgery.2 The use of PR has been shown to improve functional exercise capacity and quality of life, while reducing acute exacerbations and hospitalizations.4 The use of PR with concomitant pharmacotherapy has been shown to be a more effective therapeutic strategy for improving health outcomes in COPD compared with traditional pharmacological management with inhaled bronchodilators,4,5 and has emerged as a recommended standard of care for patients with chronic lung disease.4
PR for COPD: Clinical, Economic, and Budget Impact Analysis 2
In Canada, there is poor access to PR for COPD because of limited program capacity. It was determined in a 2005 survey that 1.2% of the COPD population in Canada had access to PR. In 2005, eight provinces indicated they had programs.6 The number of patients eligible for PR may increase as the population ages. There is also an increasing number of younger patients with COPD (from smoking and from talc lung) and an increasing number of female patients. There is no specific programming for younger patients, who may have different needs compared with those in older age groups. A Canadian study that compared the direct costs for patients with COPD before and after they enrolled in a rehabilitation program in Alberta indicated that the implementation of PR programs in Canada would cost between C$220 million and C$307 million annually. The overall savings in direct health care costs could be up to C$172 million per year. The impact on productivity costs would be minimal, because most patients with severe COPD are older individuals who are not in the work force.7
1.2 Overview of Technology
The American College of Chest Physicians (ACCP) and the American Association of Cardiovascular and Pulmonary Rehabilitation (AACPR)4 note that the American Thoracic Society and European Respiratory Society’s joint definition of PR focuses on three features of successful rehabilitation: Multidisciplinary: PR programs integrate expertise from health care disciplines into a
comprehensive and cohesive program that is tailored to each patient’s needs. Individual: Patients with disabling lung disease require individual needs assessment,
individual attention, and a program that is designed to meet realistic individual goals. Attention to physical and social function: PR pays attention to psychological, emotional,
and social problems, and to physical disability; and helps to optimize medical therapy to improve lung function and exercise tolerance.
The ACCP/AACPR state that, in current practice, PR typically includes exercise training, education, instruction in respiratory and chest physiotherapy techniques, and psychosocial support. For the ACCP/AACPR guidelines, comprehensive PR was defined as an intervention that includes one or more of these components beyond exercise training, which is considered to be an essential and mandatory component.4 The main goal of PR is the restoration of the patient to the highest possible level of independent functioning. This goal is accomplished by helping patients become more physically active and learn more about COPD, treatment options, and how to cope. Patients are encouraged to become involved in providing their own health care, become more independent in daily activities, and become less dependent on health professionals and expensive medical resources. Instead of focusing on reversing the disease, rehabilitation is used to reduce symptoms and to reduce disability.4 Pulmonary rehabilitation programs require a health professional who has the expertise to conduct an exercise program and who is trained in cardiopulmonary resuscitation. A multidisciplinary team of health professionals may be involved in the educational component of the program.8 The components of a program include:8
PR for COPD: Clinical, Economic, and Budget Impact Analysis 3
Patient assessment (obtain medical history; assess smoking, nutritional status, exercise capacity, quality of life, breathlessness, and patient’s goals)
Patient exercise training (design an exercise program; determine appropriate exercise, including intensity, duration, and frequency)
Patient education (hold educational sessions on the role and correct use of medications; breathing techniques; managing breathlessness; physical exercise; nutrition; healthy eating; lung diseases; coping with chronic lung disease; and management of depression, anxiety, and panic attacks)
Program evaluation (evaluate the effectiveness of the program based on patient outcomes — for example, exercise capacity, quality of life, breathlessness; obtain patient feedback; communicate with patient’s physician)
Maintenance (if possible, continue to provide one supervised session a week for maintenance, encourage patients to undertake a home exercise program).
The approaches taken vary between programs. All programs provide aerobic exercise and education sessions, but some exclude strength training or psychosocial and behavioural interventions. There may also be differences in the content and presentation of educational sessions. The numbers and length of sessions differ, and there is variation in the use of home exercise between sessions and the support that is offered during maintenance after the completion of PR. Patients who participate in PR programs also have concomitant pharmacotherapy that is generally equivalent to that provided in usual care for the management of COPD.
2 ISSUE
COPD causes disability and impaired quality of life. The use of PR can assist in the management of COPD. In Canada, there is poor access to PR because of limited program capacity. Policy- makers and health care providers need advice to help with decision-making about the future establishment and use of PR programs. Information on the effectiveness, cost-effectiveness, budget impact, and operational needs of PR programs and the impact of specific program elements on clinical outcomes would be helpful for decision-makers. Policy-makers have commented positively on the usefulness of guidelines, such as those from the CTS, as a source of advice.
3 OBJECTIVES
The objectives of this health technology assessment were to evaluate the effect of PR programs for COPD on clinical and economic outcomes, and to assess the health services impact. The research questions were: 1. What is the clinical effectiveness of PR and pharmacotherapy (together) compared with
pharmacotherapy alone for adults with COPD? 2. What is the effectiveness of elements of PR programs for adults with COPD?
PR for COPD: Clinical, Economic, and Budget Impact Analysis 4
3. What is the cost-effectiveness of PR and pharmacotherapy compared with pharmacological therapy alone in adults with COPD?
4. What is the health services impact of implementing PR for adults with COPD in Canada? 5. What are the recommendations for PR in current COPD clinical practice guidelines that are
relevant to the Canadian context?
4 CLINICAL REVIEW
A protocol for the clinical review was written before the research was started and followed throughout the review process.
4.1 Methods
4.1.1 Literature searches The search strategies that were developed by the information specialist [MM], with input from other members of the project team, underwent an internal peer review by another CADTH information specialist. There were no language restrictions. The following bibliographic databases were searched through the Ovid interface: MEDLINE, Medline In-Process & Other Non-Indexed Citations, Embase, BIOSIS Previews, and CINAHL. Parallel searches were conducted in PubMed, The Cochrane Library, and the Health Economic Evaluations Database (HEED). The search strategy comprised controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were chronic obstructive pulmonary disease and pulmonary rehabilitation or exercise therapy. Methodological filters were applied to limit retrieval to randomized controlled trials (RCTs), observational studies, health technology assessments (HTAs), systematic reviews, practice guidelines, and economic studies. The detailed search strategies appear in Appendix 1. The search was restricted to articles that were published from 1998 onwards. Ovid AutoAlerts were set up to send monthly updates with new literature. Updates were performed on HEED, PubMed, and Cochrane Library databases. Grey literature (literature that is not commercially published) was identified by searching the websites of HTA and related agencies, professional associations, relevant conference proceedings, and other specialized databases. Google and other Internet search engines were used to search for web-based information. These searches were supplemented by hand searching the bibliographies and abstracts of key papers and conference proceedings, and through contacts with appropriate experts and agencies. A final grey literature update occurred during the writing of the report.
PR for COPD: Clinical, Economic, and Budget Impact Analysis 5
4.1.2 Selection criteria
a) Inclusion criteria Comparative studies that included the use of PR programs for adults with COPD and that
reported outcomes in terms of morbidity or mortality, health-related quality of life (HRQL), exercise capacity, other patient-centered end points such as shortness of breath or activity limitation, and health-care utilization. The studies could include the use of PR in any setting. The comparators included pharmacological therapy and other approaches to the management of COPD.
Non–comparative studies that included the long-term follow-up of patients after PR, and reported outcomes in terms of morbidity, mortality, HRQL, exercise capacity, or use of health services.
Comparative studies that considered the efficacy or effectiveness of components of PR programs.
Studies that addressed differences in the efficacy or effectiveness of PR based on subgroups, patient characteristics, or provision of rehabilitation.
HTAs and systematic reviews that considered the use of PR programs for adults with COPD.
Clinical practice guidelines for the management of COPD that were judged to be relevant to the Canadian context.
b) Exclusion criteria Studies on the use of PR programs only for conditions other than COPD. Case reports, implementation studies, chart reviews, focus groups, and interviews. Narrative reviews, correspondence, and commentaries. Duplicate publications of the same study. 4.1.3 Selection method
Two reviewers (DH and MS) independently applied the selection criteria to the titles and abstracts that were found during the literature search. Full-text articles were obtained for abstracts that met the selection criteria and those for which decisions could not be reached. Full-text articles were included if they met the selection criteria. Any discrepancies were resolved by consensus. The clinical practice guidelines that are relevant to the Canadian context were selected by three of the authors (DM, IM, MS), based on their clinical experience with PR in Canada. 4.1.4 Data extraction strategy
Two reviewers (DH, MS) independently extracted data from the selected publications using a data abstraction form that was created before the research was started (Appendix 2). Any disagreements were resolved by consensus. The extracted information included the study design, setting, and duration; patient numbers and characteristics; components of the PR program and reported measures of efficacy; clinical outcomes related to HRQL; exercise capacity; hospital stay; exacerbations; and treatment-related adverse effects.
PR for COPD: Clinical, Economic, and Budget Impact Analysis 6
Non-English language papers that were judged to be of appropriate quality based on the abstracts and contents were translated. Information was extracted from the abstracts of other relevant non-English language papers. 4.1.5 Strategy for validity assessment
The quality of the selected studies was evaluated independently by two reviewers (DH and MS), taking into account study design and study performance and linking both to judgments on study reliability9 (Appendix 3). Any disagreements were resolved by consensus. Based on the quality scores, each study was assigned to one of five categories: High quality (high degree of confidence in study findings) Good quality (some uncertainty in the study findings) Fair quality (some limitations that should be considered in the implementation of the study
findings) Poor to fair quality (substantial limitations in the study findings, which should be used
cautiously) Poor quality (study findings have unacceptable uncertainty). The quality of selected RCTs was also assessed using the Jadad Scale10 (Appendix 4). Quality assessment was not attempted for not-translated, non–English language papers or abstracts.
4.1.6 Data analysis methods
Exercise capacity and HRQL were the primary indicators of efficacy and effectiveness. Mental health, use of health services, numbers of acute exacerbations, and mortality were also considered when relevant data were reported. The selected studies that evaluated PR programs varied in components, duration, and patient populations. Also, various methods were used to assess changes in exercise capacity, HRQL, and other outcomes of PR. Because of this lack of homogeneity across studies, the pooling of results was considered to be unrealistic. A series of qualitative reviews were prepared by two reviewers (DH and MS) to summarize the relevant information that could be used to answer the research questions of this HTA. For each selected study, the outcomes of interest were discussed, and any discrepancies were resolved by consensus. Between-group differences in outcomes were interpreted as the means and corresponding 95% confidence intervals, if such information was included in a publication. If a publication excluded such details, other measures of between-group comparisons were used; for example, P values and associated conclusions of statistical significance. The clinical significance of reported point estimates of differences in outcome was judged with reference to minimal clinically important differences (MCIDs) that were determined for tests and measurement scales. MCIDs were defined as follows:
PR for COPD: Clinical, Economic, and Budget Impact Analysis 7
a) Exercise tolerance measures Six-minute walk test (6MWT), 54 metres11 Incremental shuttle walking test (ISWT), 47.5 metres12 Endurance shuttle walk test (ESWT), 85 seconds13 Maximal incremental treadmill test, 10 Watts14 cycle endurance test (CET), 100 seconds.15 b) Quality of life measures Chronic Respiratory Disease Questionnaire (CRQ), 0.5 points for each domain16 St. George’s Respiratory Questionnaire (SGRQ), 4 points17 Short Form (36) Health Survey (SF-36), 5 points for composite scores18 Quality of Well-Being Scale (QWB), 0.03 units.19
c) Mental health measures Beck Depression Inventory, 5 points20 Hospital Anxiety and Depression Scale (HADS), 1.5 points.21 The effect sizes were estimated as Cohen’s d, using difference of the means for intervention and control groups divided by the pooled standard deviations, and classified according to Cohen’s definition of “small, d = 0.2; medium, d = 0.5; and large, d = 0.8.”22
4.2 Results
4.2.1 Quantity of research available
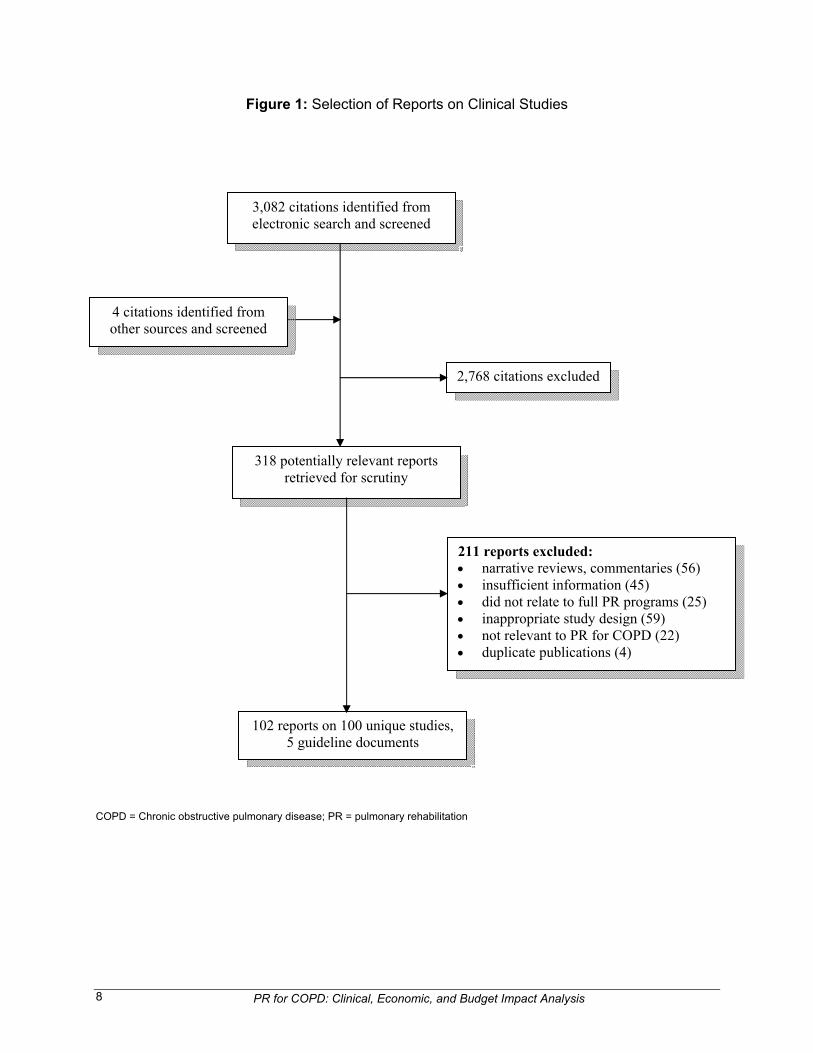
The report selection process is shown in Figure 1. The literature search identified 3,082 citations, and 318 articles were retrieved after preliminary screening. From these, 102 papers on 100 unique studies and five practice guideline documents were selected for inclusion in the review. The most common reasons for excluding citations were use only of narrative reviews or commentaries, failure to deal with full PR programs (those that included education and, in some cases, other components in addition to exercise training), inappropriate study design (for example, small case series), insufficient information, and non-relevance to PR for COPD. 4.2.2 Study characteristics
a) Overview of pulmonary rehabilitation programs and studies Pulmonary rehabilitation and its evaluation is complex. The studies that are included in this HTA reflected the variation in the components of PR programs and the method of implementation. Patients: There was variation between studies in the severity of COPD among the patients who were recruited. The selection criteria in many studies excluded patients with comorbidities (for example, heart disease, malignancy, bone and joint disease). Setting: PR programs were offered in inpatient, outpatient, and home-based settings, and in combinations of these settings.
PR for COPD: Clinical, Economic, and Budget Impact Analysis 8
Figure 1: Selection of Reports on Clinical Studies
COPD = Chronic obstructive pulmonary disease; PR = pulmonary rehabilitation
3,082 citations identified from electronic search and screened
318 potentially relevant reports retrieved for scrutiny
211 reports excluded: narrative reviews, commentaries (56) insufficient information (45) did not relate to full PR programs (25) inappropriate study design (59) not relevant to PR for COPD (22) duplicate publications (4)
2,768 citations excluded
102 reports on 100 unique studies, 5 guideline documents
4 citations identified from other sources and screened
PR for COPD: Clinical, Economic, and Budget Impact Analysis 9
Program components: All PR programs included aerobic exercise and education, and some excluded strength training, or nutritional and psychosocial interventions. Duration of PR: The numbers and duration of sessions varied between programs. The number of sessions ranged from 11 to 96, and the number of weeks from three to 52. Follow-up time: In those studies where data were collected after the end of the PR program, the follow-up lasted from one to 60 months. Study design and performance: Though many studies in the review were of good quality, not all were RCTs. In some studies, not all aspects (patient selection, description of the interventions, specification and analysis of study data, patient disposition [enrollment, adherence, attrition, and loss to follow-up], and outcomes reported) were adequately covered. Many studies had small numbers of patients and limited power. Measures of PR outcome: A variety of methods were used in the studies to measure changes in exercise tolerance and HRQL, thereby complicating the comparison of results across studies. The methods that were used for exercise tolerance included the 6MWT, ISWT, ESWT, and CET. Those that were used to measure HRQL included the SGRQ, CRQ, QWB, and SF-36. Reporting of study results: Most of the papers reviewed reported study outcomes in terms of the statistical significance of changes from baseline (the baseline in some studies was the beginning of the PR program and in other studies it was the end of the PR program). A minority of papers included confidence intervals in the presentation of results. Clinical significance of study results: Many of the reviewed studies did not discuss the clinical significance of findings. A comparison of between-group differences in outcomes to relevant MCIDs has been made in this report. Mean changes in outcomes that are below the MCIDs indicate that the PR program was not clinically effective for a large proportion of the study participants. There are other, less easily described influences on the effectiveness of PR programs. Coultas and McKinley commented that because of the complexity of starting and sustaining behaviour change, the variation in outcomes between PR programs may be influenced by patient factors, and by the attitudes and skills of team members. Little is known about the influence of patient or team characteristics on outcomes.23 Additional details about the studies appear in Appendix 5, Tables A1 to A15. b) Efficacy and effectiveness of pulmonary rehabilitation Most of the evidence on the efficacy and effectiveness of PR and pharmacotherapy was obtained from studies in which the outcomes of patients in PR programs were compared with those of patients who received usual care (typically pharmacological treatment alone). For longer-term outcomes, the comparisons of PR approaches and observational studies were also considered. In the two following sections, which present the studies that reported outcomes in terms of exercise capacity and HRQL, the change in outcome in comparative studies refers to the

PR for COPD: Clinical, Economic, and Budget Impact Analysis 10
between-groups difference in the mean change in outcome from baseline unless otherwise specified. Exercise capacity and health-related quality of life Short term outcomes: This section on short-term outcomes includes studies with outcomes of three months or less, which in many cases cover those measures that are obtained at the end of a PR program. The studies that reported short-term outcomes of PR programs (up to three months from the start of PR) ― including setting, program components, study design, quality ranking, and outcomes of interest ― appear in Appendix 5, Table A1. PR after admission for exacerbation: In a high-quality study, Man et al.24 assessed the effects of early PR (rehabilitation shortly after discharge) for patients who had been admitted to hospital because of acute exacerbations. The use of PR led to statistically and clinically significant improvements in exercise capacity and health status at three months (ISWT median difference 60 metres, SGRQ −12.7 [−5.0, −20.4]). This study was considered in an earlier review that included studies using exercise only in rehabilitation and suggested that the use of PR is effective for patients with COPD after acute exacerbation.25 In a good-quality study, Eaton et al.26 found no difference between groups in change in exercise capacity or in HRQL as measured using the CRQ scale. Those who completed the PR program, however, had statistically significantly higher scores in the physical component of the SF-36 quality of life questionnaire than the usual care group. In a retrospective cohort study, Clini et al.27 considered the effectiveness of early inpatient PR after admission with acute exacerbation. After a four-week PR program, there was clinically significant improvement in exercise capacity and HRQL across all grades in the Medical Research Council (MRC) dyspnea scale . For all patients, the mean change in the six-minute walk distance (6MWD) was 65.3 metres [63.2, 67.5], with 56% reaching the MCID. The proportion of patients reaching 350 metres was higher in the most severe MRC grades. The mean change in SGRQ score was −5.9 [−6.45, −5.34] and higher than MCID for all MRC grades. Studies on patients with stable COPD: Twelve studies included patients with serious but stable COPD in different settings, and in PR programs of varying length and structure. Seven were of high or good quality,28-34 four of fair quality,35-38 and one of poor to fair quality.39 All twelve studies found short-term improvement in exercise capacity. The mean change in exercise capacity was greater than the MCID in four studies. Karapolat et al.28 found that benefits tended to deteriorate during the first month after outpatient PR. The mean values of the change in 6MWD were 107 metres at eight weeks and 58 metres at 12 weeks. In a study on outpatient PR, Griffiths et al.34 found a mean change in ISWT results of 76 metres at eight weeks. In a study on home PR, Oh36 found a change in 6MWD of 68 metres after 8 weeks. Riario-Sforza et al.39 reported that, at the end of a six-week outpatient PR program, 64% of participating patients (Global Initiative for Chronic Obstructive Lung Disease [GOLD] stages I to IV) had an increase in 6MWD of at least 54 m (the MCID) compared with 13% in a usual care control group. The number needed to treat (NNT) in the overall intervention group was 2. The same NNT was obtained for patients at GOLD stages II, III, and IV, and it was 8 for those at stage I. Six studies had mean changes in 6MWD that were less than the MCID: Boxall et al.,31 35 metres (home PR with housebound patients, 12 weeks); Barakat et al.,29 38 metres (outpatient, 14
PR for COPD: Clinical, Economic, and Budget Impact Analysis 11
weeks); Singh et al.,32 47 metres (home PR, four weeks); Theander et al.,30 24 metres (outpatient, 12 weeks); Na et al.,35 14 metres (home, 12 weeks); and Skumlien et al.,37 19 metres (inpatient, four weeks). The change in exercise capacity was also below MCID in Regiane Resqueti et al.’s38 study, which used the three-minute walk distance or 3MWT (16 metres, home PR, nine weeks). Elçi et al.33 (outpatient and home, 12 weeks) found an increase in 6MWD values between 1 and 3 months (24 metres), but the relationship to MCID is unclear because the baseline value was not reported. Ten of eleven studies found improvements in HRQL. In eight of the 10 studies, the changes in mean HRQL scores were greater than the MCID. Boxall et al.,31 Barakat et al.,29 Karapolat et al.,28 Na et al.,35 and Skumlien et al.,37 used the SGRQ; Singh et al.,32 and Oh,36 the CRQ; and Griffiths et al.,34 both instruments. Barakat et al.29 also reported a decrease in the risk of death as measured using the BODE index: body mass, airflow obstruction, dyspnea, exercise capacity. The changes in CRQ scores in Regiane Resqueti et al.’s study38 were below the MCID. Theander et al.30 could not detect a statistically significant difference in fatigue (using the Canadian Occupational Performance Measure and the Fatigue Impact Scale) or health status between the PR and usual care groups (SGRQ and SF-36). Elçi et al.33 found an improvement in SGRQ and SF-36 scores between 1 and 3 months but did not report baseline values. Overall, these results are generally consistent with those included for earlier studies that were considered by Lacasse et al.5
Studies reported in non-English language papers: In an RCT, Jang and Jung (Korea)40 considered outpatient PR for eight weeks, with one session per week that included exercise training, education, and counselling. The program was reported by the authors to be effective in improving self-efficacy, dyspnea, exercise endurance, and HRQL (Quality of Life Index Pulmonary Version III) in patients with COPD, with statistically significant improvements in each of these measures. Ciric et al. (Serbia)41 found that a 21-day PR program improved exercise tolerance and dyspnea when compared with medical therapy alone for patients with mild, severe, and very severe COPD. The mean changes in 6MWD were greater than the MCID for the groups with mild and very severe disease. In a randomized trial, Ringbaek et al. (Denmark)42 reported on an eight-week PR program for patients with moderate COPD and found “insignificant improvement in well-being” and an increase of 29 metres in a walk test. Longer-term outcomes after PR: This section includes studies that obtained longer-term outcomes, some related to the use of maintenance programs after the end of PR. Studies that reported longer-term outcomes after PR appear in Appendix 5, Table A2. All involved home-based programs, most of which occurred after or in association with outpatient or inpatient PR. For longer-term outcomes, a key factor may be the type and intensity of maintenance strategy that is adopted after the completion of PR. The following studies include comparisons of PR and usual care, and of maintenance programs and usual care after the completion of PR. In a high-quality study, van Wetering et al.43 found that PR plus long-term (20 months) maintenance was effective in patients with COPD, exercise impairment, and less advanced airflow obstruction. After 24 months, the intervention group had improved changes in SGRQ score and cycle endurance test (CET) time compared with baseline. No improvement in 6MWD
PR for COPD: Clinical, Economic, and Budget Impact Analysis 12
was noted. The mean change in CET remained above the MCID at 20 months follow-up. The mean change in SGRQ score was greater than the MCID at four months and lower than the MCID at later follow-up. Regiane Resqueti et al.38 found that patients with severe or very severe COPD (GOLD III or IV) maintained an increase in exercise capacity at six months, although the mean between-group differences were below the MCID. Between-group differences were below the MCIDs for all domains of the CRQ. In high-quality studies, Engström et al.44 and Güell et al.45 reported longer-term outcomes after extended PR interventions. Engström et al.44 found that lasting effects on physical fitness were achieved with an outpatient program over 12 months, although changes in the mean values for 6MWD remained below the MCID. No effects were shown on HRQL, as measured using the SGRQ. Güell et al.45 considered the outcomes of a six-month PR program plus a further six months of weekly supervised breathing exercises. The benefits in exercise capacity that were achieved persisted for 18 months, with changes in the mean values for 6MWD above the MCID. There were clinically significant increases at six months for the PR group in all domains of the CRQ, with differences from controls continuing at 18 months follow-up. The values of all domains of the CRQ were greater than the relevant MCIDs. In the follow-up to post-PR findings, Na et al.35 found that the short-term change in exercise tolerance was not maintained at one year after the end of PR. In a good-quality study on a six-week outpatient PR program, Finnerty et al. found that benefits were maintained at 24 weeks.46 The difference in 6MWD scores was above the MCID at follow- up (67 metres [−1.6, 135.6]). The difference in SGRQ scores was above the MCID at follow-up (−7.1 [−14.7, 0.54]). In a good-quality study, Griffiths et al.34 found that, after a six-week PR program, the differences in mean scores of the SGRQ and CRQ remained higher than the MCIDs at 12 months. The values of exercise capacity, measured using the ISWT, were lower than the MCID at 12 months. In a good-quality study on the use of a home PR program for patients with very severe COPD who were on long-term oxygen treatment, Fernandez et al.47 found that the difference in 6MWD total scores was above the MCID after 12 months (66 metres). They47 also found that the difference in SGRQ total score was above the MCID after 12 months (−12.2). In a prospective cohort study with long-term follow-up, Cote and Celli48 reported mortality and BODE index scores for two years after PR, and hospitalization details for one year before and after PR (116 participants in the PR group and 130 participants in the usual care group). The study quality was rated as poor to fair. There were 13 deaths (eight respiratory-related) in the PR group and 66 deaths (57 respiratory-related) in the usual care group (Kaplan-Meier log rank analysis P < 0.0001). Cote and Celli defined a one-unit change in the BODE index as being clinically significant. After rehabilitation (three months from baseline), 83 (71%) participants in the PR group had an improvement of more than one unit, 29 (25%) participants had an improvement of two units, 25 participants (21.6%) had no change, and 8 participants (6.9%) had a worse index score. The PR group had an initial improvement in the BODE index of 19% (three
PR for COPD: Clinical, Economic, and Budget Impact Analysis 13
months), which returned to baseline after one year and remained stable at two years. The usual care group had a decline in the BODE index of 4% after one year and 18% at two years (P < 0.001 between groups for all time points). These findings were described by the authors as indicating the beneficial effects of PR and subsequent maintenance exercise. In a German-language paper, Göhl et al.49 reported findings from a small RCT of a PR intervention over 12 months. There were statistically significant improvements from baseline for SGRQ total and SF-36 composite scores for the PR group, but not for the controls. The difference in 6MWD from baseline for the PR group was 79 metres (P = 0.003), with no statistically significant difference for the controls, indicating that the change in exercise capacity was above the MCID. Studies on maintenance after PR: du Moulin et al.50 concluded that home-based exercise training was as effective as maintenance in patients with moderate COPD, with benefits in exercise tolerance and HRQL at six months. The differences in changes to mean 6MWD between intervention and control groups after the end of PR were 20 metres at three months and 46 metres at six months (statistically significant). Changes during PR were not reported so that the relationship of the overall change in exercise tolerance to the MCID is uncertain. A similar pattern was found for mean CRQ total scores (differences of 0.4 at three months and 0.7 at six months).
Moullec et al.51 found that an approach that linked home exercise with self-help association programs (patient-run support groups) produced benefits in exercise capacity and HRQL at six months that were maintained at 12 months after the start of the program. At the end of a four-week PR program, the mean changes of 6MWD were below the MCID, and those for the SGRQ were greater than the MCID. After six months of the maintenance program, the intervention group had higher values for 6MWD than controls (difference 74.2 m, 95% CI [37.7 to 110.5]). The intervention group also had higher scores in the SGRQ domains of symptoms difference of −6.7 [−16.2 , 2.7]), activities (difference −20.2 [−33.4, −7.1]), and impacts (difference −17.0 [−28.1, −5.8]). These differences were maintained at 12-month follow-up (6MWD difference 75.8 [32.0 ,11.6], SGRQ symptoms difference −18.5 [−30.9, −6.2], SGRQ activities difference −27.0 [−40.0, −14.0], SGRQ impacts difference −32.4 [−42.0, −22.8]). All differences were above the MCIDs.
Steele et al.52 evaluated the effectiveness of a post-PR exercise adherence intervention for a home exercise program. The experimental group received weekly telephone calls, a home visit, and a pedometer for self-monitoring. At the end of PR, the mean increase in 6MWD for all participants was 45 metres (below the MCID). After 20 weeks post-PR, 6MWD had decreased by 10.7 metres in the intervention group and by 35.4 metres among controls (P = 0.023). At 52 weeks, the differences from post-PR values were −21 metres and −39.6 metres, respectively. There were no differences between the groups in HRQL. The authors concluded that there was no long-term benefit from using the intervention in a sedentary group of patients with chronic lung disease (85% had COPD).
Ries et al.53 evaluated a 12-month maintenance program after PR. The intervention included weekly telephone contacts and monthly supervised reinforcement sessions. During the intervention, exercise tolerance (maximum treadmill workload and 6MWD) and overall health
PR for COPD: Clinical, Economic, and Budget Impact Analysis 14
status ratings were better maintained in the experimental group than among patients who had standard care. There were no between-group differences for self-efficacy or generic and disease-specific HRQL. By 24 months, there were no statistically significant group differences, and patients returned to levels that were close to pre-rehabilitation measures. Ries et al. concluded that the program produced modest improvements in the maintenance of benefits after PR. Other studies reporting longer-term outcomes after PR: Other studies that reported longer-term outcomes after PR appear in Appendix 5, Table A3. Romagnoli et al.54 compared the outcomes of patients who participated in three PR programs over 12 months with those who participated in two programs. They found that there were improvements in 6MWD and SGRQ scores after the end of each PR program. The changes in mean values for each program were below the MCIDs, and the benefits were partially lost between programs. When compared with baseline, the mean values of 6MWD were above the MCID at the end of the second and third PR programs, and those of SGRQ scores were above the MCID at the start of the third program. Verrill et al.55 compared outcomes after 12 weeks and 24 weeks of PR in seven outpatient programs. They found that physical performance continued to improve with up to 24 weeks of PR (6MWD above the MCID). HRQL and dyspnea improved after 12 weeks, and the improvement was maintained at 24 weeks. Two observational studies from Norway indicated that there were benefits after lengthy PR and maintenance.56,57 After a home PR program that lasted 12 months, improvements in HRQL were maintained to two years, with a mean total SGRQ score above the MCID at one year and below it at two years. The exercise capacity did not change from baseline, and it did not deteriorate over two years.56 In the second study,56,57 a one-year PR program was followed by a further year of regular exercise sessions. Participants improved HRQL and exercise tolerance in the first year, with no further clinically relevant improvement in the second year. This status was maintained three years after the end of the program. The mean values of the 6MWD and SGRQ total score remained above the MCIDs. At two years, the mean difference in 6MWD from baseline was 86 metres (63, 109), and the mean difference of total SGRQ score from baseline was −11.1 (−13.9, −8.4). Self-reported data indicated that participants continued to exercise regularly during the three years after the program.
c) Mental health outcomes Ten studies reported mental health outcomes, usually in the short-term, and measured using several instruments (Appendix 5, Table A4). Six studies compared PR with usual care and showed a benefit from using rehabilitation.26,33,58-61 In good-quality studies, Paz Diaz et al.58 and Elçi et al.33 found improvement in anxiety and depression in the PR groups, although Elçi did not report separate scores for the two conditions. In Paz Diaz et al.’s study, the between-group difference in the Beck Depression Inventory was above the MCID. Eaton et al.26 and Kayahan et al.59 found improvements in anxiety and no improvements in scores for depression, compared with usual care. The mean change in score using the HADS in Eaton’s study was below the MCID. In a study of poor to fair quality, Kozora et al.60 found a decline in depressive symptoms (below the MCID for the Beck Depression Inventory) and did not measure anxiety. Güell et al.61 found improvements in all components of the Millon Behavioral Health Inventory and suggested
PR for COPD: Clinical, Economic, and Budget Impact Analysis 15
that the use of PR may decrease psychosocial morbidity even without a psychological intervention. Three studies62-64 compared PR groups using different approaches (different numbers of supervised and home sessions,63 with or without progressive muscle relaxation,64 or in a cold climate versus a warm climate).62 A reduction in scores of anxiety and depression were noted. Two studies reported longer-term outcomes. Both groups in Haugen and Stavem’s62 study had HADS scores of depression below baseline and less than the MCID, at eight-month follow-up. One group was also below the baseline score in anxiety and above the MCID. O’Neill et al.63 found that the differences from baseline in anxiety and depression declined from six weeks to six months after PR, consistent with trends in exercise capacity and HRQL (Table A13). All changes in scores were below the MCID. Both groups in Lolak et al.’s64 study had mean changes in HADS scores for anxiety and depression that were greater than the MCID, but the between- group differences did not exceed the MCIDs. De Godoy et al.65 found improvements in anxiety and depression in patients whose PR programs included psychotherapy. d) Effect of pulmonary rehabilitation on chronic obstructive pulmonary disease
exacerbations Few reports of studies evaluating PR included details about exacerbations in the reported outcomes. Güell et al.45 and Cote and Celli48 found there were statistically significantly fewer exacerbations in the PR groups than among patients who received usual care (Appendix 5, Table A5). In the other studies (Appendix 5, Table A5), there were fewer exacerbations in a group receiving PR plus tiotropium compared with PR alone,66 exacerbations were less frequent in a warm climate than a cool climate62 and there was no difference between groups receiving outpatient or home PR.67 In an RCT, van Wetering et al.43 found there was no difference between intervention and usual care groups during four months of PR and 20 months’ maintenance. e) Effects on health care utilization Studies that included health-care utilization — mostly in terms of hospitalization of patients with COPD — appear in Appendix 5, Table A6. In good-quality studies, Eaton et al.26 and Man et al.24 considered patients who had been hospitalized with exacerbations. There were trends to lower rates of COPD-related re-admission among patients who received PR. Man et al. reported a statistically significant decrease in the number of emergency visits per patient (0.10 versus 0.43, P = 0.01). In a high-quality study, Güell et al.45 found lower admission rates over the two years after PR among patients who had participated in the program compared with those who received usual care (0.6 versus 1.3). The difference did not reach statistical significance. Griffiths et al.34 found lower mean admission rates and length of stay for patients who had participated in a PR program (respiratory-related admissions 1.4 versus 1.9, P = 0.044, hospital days 9.4 versus 18.1, P = 0.048). The six other studies48,51,56,57,68,69 that reported hospitalization after PR and usual care used before-after approaches, with data for 12 months before PR being compared with those after the end of rehabilitation. All but one of these found statistically significant reductions in the number
PR for COPD: Clinical, Economic, and Budget Impact Analysis 16
of hospital admissions or number of hospital days after PR. One study was of good quality51, four were of poor to fair quality,48,56,57,68 one was of poor69 quality, and some used self-reported data.51,69 Golmohammadi et al.7 did another before-after analysis of an outpatient program that provided education, counselling, and rehabilitation. Utilization for a comparison group of non-attendees with COPD was also used. The program saved $33 in utilization. Ambrosino et al.66 reported fewer hospitalizations in a PR plus tiotropium group than in a PR only group, but the group sizes were small. Wittmann et al. found a greater decrease in hospital admissions among patients who had a training intervention plus PR than among those who had PR alone (0.13 versus 0.21 over 12 months, P < 0.001).70 In a comparison of outpatient and home PR, Maltais et al.67 found there was no difference in the number of admissions (0.45 and 0.42 per patient). Romagnoli et al.54 found no statistically significant difference in the number of admissions among patients who had participated in two or three PR programs. f) PR and other treatments Pharmacological therapy: Three studies reported comparisons of PR and tiotropium with PR alone (Appendix 5, Table A7). In a high-quality study, Ambrosino et al.66 found that the addition of tiotropium to PR did not improve 6MWT performance compared with PR alone. There were no differences between groups in HRQL as measured using the SGRQ. The mean changes in 6MWD and SGRQ scores for both groups were below the MCIDs, except the SGRQ score for the tiotropium group at the end of PR. There was a statistically significant improvement in perceived dyspnea in the tiotropium group at the end of PR, but not at follow-up. Casaburi et al.71 found that tiotropium plus exercise training increased exercise endurance of a constant work rate treadmill task when compared with exercise training alone (difference at end of PR: 5.35 minutes [0.69, 10.00]; difference at end of 12-week follow-up: 6.60 minutes [1.15, 12.02]). The differences in SGRQ scores for the two groups were 3.86 at end of PR and 4.43 at follow-up, the latter being above the MCID. It appears that the rehabilitation that was used in this study consisted only of exercise training, instead of PR. A sub-study found that the use of tiotropium enhanced the efficacy of exercise training as measured by self-reported participation on physical activity, although the response rate was low.72 A lower quality study73 found that six weeks of PR gave no additional benefits to patients who were already taking tiotropium. Airway therapies: Duiverman et al. (Appendix 5, Table A8) compared the use of non-invasive positive pressure ventilation (NIPPV) with PR to PR alone.74 They suggest that NIPPV augments the benefits of PR in patients with chronic hypercapnic failure by reducing dyspnea and the work of breathing. While the NIPPV group improved in the fatigue domain of the CRQ compared with the group receiving PR alone, there were no statistically significant differences between groups in the CRQ total. There was no difference between groups in changes in 6MWD, which were below the MCID. In a poor to fair quality prospective study on inpatients with severe COPD (GOLD IV), Köhnlein et al.75 found that those using NIPPV plus PR had better exercise tolerance and HRQL than those using PR alone. The difference in 6MWD changes between the groups was statistically
PR for COPD: Clinical, Economic, and Budget Impact Analysis 17
significant, with the mean value of the intervention group exceeding the MCID (82 metres versus 50 metres, effect sizes 0.89 and 0.52). There were also statistically significant differences between groups in changes to the mental health component of the SF-36 (NIPPV group difference 13.9, effect size 0.73 versus PR group difference 8.0, effect size 0.44). In a high-quality study, Eves et al.76 compared the use of PR, while patients were breathing a mixture of helium and oxygen (60%, 40%), with the use of PR alone. Patients without hypoxemia and with COPD who breathed this mixture during a PR program had increased intensity and duration of exercise, which resulted in greater improvements in constant load exercise time and HRQL (change in exercise time 9.6 versus 4.4 minutes, P = 0.047, change in SGRQ score −7.6 versus −3.6, P = 0.049). Oxygen therapy is an effective intervention to reduce dyspnea in COPD. The addition of supplemental oxygen to maintain arterial oxygenation during exercise, which is standard care in rehabilitation, differs from the addition of oxygen to reduce dyspnea for patients who are not hypoxemic. A previous review concluded that the use of supplemental oxygen during physical exercise in non-hypoxemic patients does not provide a clinically relevant benefit.77 Surgical procedures: Two studies considered PR and lung volume reduction surgery (LVRS) (Appendix 5, Table A9). Pompeo et al.78 found that there were short-term improvements in subjective dyspnea, inspiratory muscle strength, and exercise capacity after either treatment. The improvements after PR were smaller and less stable than those after LVRS (change in 6MWD at six months 31 metres versus 93 metres). The LVRS group had more late complications in hospital than those who had PR (19 versus 4), but fewer long-term complications (3 versus 9). Mercer et al.79 had similar findings. PR plus bilateral LVRS gave greater improvement than PR alone in dyspnea with exercise, exercise tolerance, and subjective functional state at six months after surgery in patients with severe COPD (change in 6MWD at six months 29 metres versus 193 metres). There was one surgery-related death. Neuromuscular electrical stimulation in PR: In a small, fair quality RCT, Vivodtzev et al.80 compared PR plus electrical stimulation with PR alone in severely disabled patients with low BMI (Appendix 5, Table A10). PR plus electrical stimulation produced greater improvement in overall HRQL and in dyspnea during the performance of daily tasks than PR alone (change in Maugeri Foundation Respiratory Failure Questionnaire [MRF–28] scores –15% versus zero, P = 0.035 and −1.7 versus −0.2, P = 0.05). There was also improvement in 6MWD (greater than MCID in the intervention group), although the difference between groups was not statistically significant. The authors suggest that clinical interest in electrostimulaton is directed towards disabled patients who are unable to perform usual exercise regularly. g) PR context and operation There were studies that addressed other aspects of PR relevant to the operation of programs, including patient characteristics and program settings. Patient characteristics: Several studies considered issues related to patients who are candidates for PR. These studies appear in Appendix 5, Table A11.
PR for COPD: Clinical, Economic, and Budget Impact Analysis 18
Age profile: Baltzan et al.81 found that an inpatient PR program benefited patients with COPD who were 80 years of age or older. There was no statistically significant difference in hospital stay (28.7 days [21.9, 24.3] versus 32.2 days [27.1, 37.3], P = 0.35) or in days spent in rehabilitation, compared with a younger age group. The values of 6MWD, two-minute stair test, and Global functional score improved for both groups. The mean difference in 6MWD was above the MCID for the younger group and below it for the 80-and-over group. In a study of poor to fair quality, Fabre et al.82 found that older (more than 65 years) and younger (65 years or less) patients with COPD benefited from training at maximal workload, although peak power was statistically significantly higher in the younger age group. The mean differences were above the MCID in both groups. In a Japanese language paper on a before-after study, Ando et al.83 found similar improvements in exercise capacity for older (77 years) and younger (70 years) groups after PR, although a Kaplan-Meier analysis indicated poorer outcomes in the older group over the next three years. Disease severity: Riario-Sforza et al.84 found that patients with COPD and a history of acute exacerbations had less favourable PR outcomes than those without a history of acute exacerbations (mean 6MWD difference 31 metres versus 58 metres, P = 0.028). Two fair-quality studies reported that patients of all MRC dyspnea grades had similar benefits from PR, including statistically and clinically significant improvement in exercise capacity (mean differences in ISWT were above MCID for all grades).85,86 In a study of poor to fair quality, Garrod et al.87 reported benefits for patients with different MRC grades, including those with mild COPD. They found that only mild- and moderate-grade patients had clinically significant improvements on the 6MWD and SGRQ, as judged by the mean scores being greater than the MCIDs. The proportions of patients with a 6MWD greater than 54 metres (the MCID) were 81% for grades 1 and 2, 59% for grades 3 and 4, and 46% for grade 5. The corresponding proportions for those with an SGRQ of more than 4 units were 50%, 50%, and 39% respectively. Carone et al.88 observed similar outcomes after PR for patients with or without chronic respiratory failure, suggesting that PR is suitable for more severe patients with COPD (change in 6MWD 48 metres for both groups, change in SGRQ scores −8.3 versus −11.1, P > 0.05). Two poor-quality studies found that patients with severe ventilatory limitations can improve exercise tolerance with PR,89 and that the most physically impaired patients obtained the greatest benefit.90 Adherence to rehabilitation: In a comparison of patients with COPD having medical treatment and those receiving LVRS,91 surgical patients and those with more than 20% forced expiratory volume in one second (FEV1) and higher education were more likely to complete PR (attendance at 10 or more sessions 73.3% versus 85.4%, P < 0.0001). Patients with depression or anxiety symptoms, and those at greater distance from a PR program, were less likely to complete the program. Heppner et al.92 found that regular walking post-PR was associated with a slower decline in HRQL and walking self-efficacy. There was no effect on the decline in exercise tolerance.
PR for COPD: Clinical, Economic, and Budget Impact Analysis 19
Previous treatment with PR: In a good-quality study, Ries et al.93 found that patients with no previous PR benefited more than those who had received previous PR (change in 6MWD 101.7 metres versus 60.7 metres, P < 0.01, change in SGRQ scores −5.1 versus −2.6, P = 0.01). Gender: In fair-quality studies, Haave et al.94 and Lizak et al.85 found that PR had similar effects for women and men. Skumlien37 found that men improved 6MWD statistically significantly compared with women (women difference −8 metres [−36, 21], P =0.58; men difference 33 metres [13, 53], P = 0.003). Six men and one woman improved 6MWD by more than the associated MCID. The reasons for the poor performance in the 6MWT are unclear. Twelve of 18 men and five of 15 women had a change in SGRQ that was greater than the associated MCID (P = 0.08). Comparisons of settings for PR: Appendix 5, Table A12 shows studies that compared the performance of PR programs in different settings. Two high-quality studies indicated that outpatient and home-based PR programs can give similar benefits to patients with COPD.67,95 Another high-quality study found that there was no difference in outcomes between patients who were treated in a cold climate (Norway) and those treated in a warm climate (Spain).62 Duration of PR: Four studies compared outcomes from different numbers or types of PR sessions (Appendix 5, Table A13). O’Neill et al.63 found no difference in the effectiveness of two PR approaches with differing numbers of supervised outpatient and home sessions. Some changes resulting from the use of PR were maintained at two months (difference between groups in ISWT 3.9 metres, ESWT 131 seconds, CRQ total 9.2) and then were mostly dissipated by six months (ISWT 0.6 metres, ESWT 87 seconds, CRQ total 6.7). Both groups achieved at least 80% adherence to home exercises over a six-week period, as indicated by diary records. In a study of fair quality, Sewell et al.96 found that a shortened four-week supervised PR program plus three weeks unsupervised rehabilitation at home gave similar results in a seven-week program at the comparable time point of seven weeks and at six months follow-up. This followed an earlier study97 that found greater benefits from the seven-week program compared with a four-week program without subsequent home PR. An observational study98 of poor to fair quality found that 10 weeks of PR produced limited clinical benefits compared with those after 20 weeks PR among outpatients with mild to moderate chronic airways obstruction. Eighteen of the 25 participants had COPD. Verrill et al.55 compared outcomes after 12 weeks and 24 weeks of PR, and found that physical performance continued to improve up to 24 weeks. HRQL and dyspnea improved after 12 weeks, and improvement was maintained at 24 weeks. Approaches to exercise training: The following studies addressed approaches to exercise training that might be relevant to PR programs (Appendix 5, Table A14). Carrieri-Kohlman et al.99 compared outcomes from different numbers of supervised exercise sessions and from unsupervised home exercise. The use of a greater number of supervised training sessions (24) improved exercise performance more than the use of four supervised sessions and the use of no supervision. At 12 months, the changes from baseline in the endurance
PR for COPD: Clinical, Economic, and Budget Impact Analysis 20
treadmill test were 8.1 minutes (3.2, 13.0) compared with 1.9 minutes (−2.8, 6.5), and 1.1 minutes (−3.9, 6.1) for the no-supervision and four supervised session groups, respectively. There was no statistically significant difference in the 6MWT between groups, and the changes were below the MCID. At four, eight, and 12 months, all groups improved their mean CRQ dyspnea subscale scores above the MCID. There was no statistically significant difference between groups for any CRQ subscale at 12 months. Sewell et al.100 found that general exercise training was as effective as individually targeted training in PR. There was no additional benefit with a more complex goal-directed, individually targeted rehabilitation approach that included exercises based on the individual’s daily activities. Puhan et al.101 compared the outcomes of high-intensity continuous exercise with interval exercise (high-intensity alternating with low-intensity exercise). They found no statistically significant difference between groups in HRQL, exercise capacity, or muscular strength. They concluded that interval exercise is no less effective than high-intensity continuous exercise and is better tolerated (fewer breaks and better adherence to protocol). In a good-quality study, Mador et al.102 found that interval training was well-tolerated but showed no advantages over continuous training in exercise tolerance or HRQL. Varga et al.103 found that continuous and interval training had similar effects in patients with COPD, and claimed that both were superior to a self-managed program according to the results of an incremental exercise test. The study seemed to be in the context of an “exercise only” program instead of full PR. In an observational study, Hsieh et al.104 compared the outcomes of patients who completed or did not complete a program that included high-intensity training. Both groups had similar improvements in 6MWD. Only those who completed the high-intensity exercise in PR improved maximal exercise capacity. Magadle et al.105 considered the effects of adding INSPIRATory muscle training (IMT) to exercise training. They found that, after six months of IMT, there was a small, statistically significant improvement in SGRQ in the intervention group. They concluded that IMT provides additional benefits to those undergoing an exercise program and is worthwhile, even if patients have undertaken a previous exercise program. There was no difference in exercise capacity or FEV1, and some data are not presented. IMT was undertaken after patients had started exercise training, and the program involved exercise training alone without other components of PR (such as education). h) Specific elements of PR programs Studies on PR and education or counselling: Education is an integral component of PR.4 The studies that considered the effectiveness of education or counselling during PR appear in Appendix 5, Table A15. In a high-quality study, Wittmann et al.70 looked at the effect of structured group behaviour training followed by the development of individualized action plans for patients. Patients who received these additional components of patient education in an inpatient PR program had clinically significant changes in HRQL (group changes in total SGRQ score −2.7 versus +0.4, P < 0.01).They also had improvements in hospital stay. The absence of change in SGRQ scores for the control group (PR program only) seems surprising in view of the drop in questionnaire scores after PR.

PR for COPD: Clinical, Economic, and Budget Impact Analysis 21
De Blok et al.106 used a pedometer with exercise counselling as an addition to a PR program. When compared with PR alone, there was an increase in the number of steps per day after nine weeks of rehabilitation (1,787 versus 1,220 over seven days, including rehabilitation) and in exercise capacity (20.8 metres versus 5.8 metres for the 2MWT) but the differences between groups did not reach statistical significance. In a study of an outpatient PR centre, Norweg et al.107 found that patients who had activity-specific training combined with exercise had statistically significantly greater changes in HRQL scores than those who received exercise training plus a lecture series (CRQ total score mean difference 3.56, P = 0.03). There was no statistically significant difference between these groups and an exercise training group in either exercise tolerance or self efficacy. In a study of poor to fair quality, Scherer et al.108 found that patients receiving 12 weeks of PR with exercise and education had a statistically significant change in mean score for self-efficacy at six months from baseline. The mean score at six months for patients who had education and non–supervised exercise at home was not statistically significantly different from the baseline value. More information on the efficacy of educational interventions, outside the context of PR, is provided by Coultas et al.109 In groups of patients with COPD, neither of two nurse-assisted home care training approaches was effective in improving HRQL or health care utilization. PR and nutritional intervention: Weight loss is associated with decreased exercise capacity, decreased health status, decreased mortality, and increased morbidity among patients with moderate to severe COPD.110 Advice on appropriate diet formed part of the educational component of many PR programs. A few studies considered specific dietary interventions. Three studies assessed the influence of creatine supplements on PR (Appendix 5, Table A16).111-
113 None of the studies found that creatine supplements improved exercise performance relative to the control group. Fuld et al. found that there was a clinically significant improvement in HRQL in the intervention group compared with the control group(change in SGRQ total scores −7.7 [−14.9, −0.5]).111 This difference was associated with a worsening of the activity domain for the PR group only, which the authors described as “surprising.” Slinde et al.114 found that an intervention involving detailed advice and follow-up by a dietician over a 12-month period was successful in maintaining or positively modifying body weight. In an earlier systematic review, Puhan et al.77 identified two RCTs that assessed the value of nutritional supplements in rehabilitation for COPD. Neither study showed benefits from the interventions. Puhan et al. concluded that the evidence for nutritional and other supplemental interventions was too weak to recommend or discourage their use in clinical practice. The findings from this clinical review are consistent with that position. Psychotherapy in PR: De Godoy et al.65 compared the outcomes of patients who had PR that included a psychotherapy component with those whose rehabilitation excluded such an
PR for COPD: Clinical, Economic, and Budget Impact Analysis 22
intervention. The results showed that patients participating in PR with psychotherapy had clinically significantly better outcomes after 12 weeks, as measured using the Beck Anxiety and Depression Inventories, distance walked-weight product, and the SGRQ (Appendix 5, Table A4). In the groups who received psychotherapy, the mean changes in scores for the Beck Anxiety and Depression Inventories and for SGRQ total scores were above the MCIDs. The group who did not have psychotherapy had a worse outcome on the Beck Depression Inventory (mean change in score was plus two points). The authors concluded that psychotherapy with PR reduces anxiety and depression, and assists patients in coping with disease-related limitations by reducing behavioural symptoms, and through influencing exercise capacity and HRQL. Strength training in PR: The studies that considered the effects of including strength training in PR appear in Appendix 5, Table A17. Phillips et al.115 found that the inclusion of resistance training led to statistically significant increases in strength when compared with PR alone, but there was no difference in exercise capacity. These authors commented that their single-set resistance training protocol produced improvements comparable to those in studies that used multi-set resistance training. Alexander et al.116 found no statistically significant difference between groups in exercise capacity or muscle strength when strength training was added to PR. Costi et al.117 found that adding unsupported upper extremity exercise training to PR improved functional exercise capacity in patients with COPD. The authors note that it is difficult to explain the large difference in 6MWD between the groups (74.4 metres versus 24.2 metres) with only the intervention group reaching the MCID. 4.2.3 Clinical practice guidelines
Of the 24 practice guidelines that were identified in the literature search, four were considered to be relevant to the Canadian context. These documents were prepared by the CTS,2,118 ACCP, and the AACPR,4 the US Department of Veterans Affairs and Department of Defense (VA/DoD),119 and GOLD.120 The development of the selected guidelines followed processes that included comprehensive reviews of relevant literature, evaluation of evidence by content experts, and formulation of recommendations by expert committees, taking account of the feedback that was received. The guidelines provide information on the strength of evidence in support of aspects of PR. The CTS, ACCP/AACPR, and VA/DoD guidelines give recommendations and indicate the strength of the recommendations. The GOLD document lists the benefits associated with PR and links these to the strength of available evidence. The VA/DoD guideline includes judgments on the net effect of the interventions. Common themes include support for the use of PR by patients with COPD who have dyspnea and reduced capacity, and inclusion of education as a component of PR. The recommendations and statements in these guidelines appear in Appendix 6. 4.2.4 Data analyses and synthesis
a) Effectiveness of PR Studies that are included in this review show that, when compared with usual care (pharmacotherapy) of patients with stable COPD, PR and pharmacotherapy provides benefits in the short term (up to three months). In all 12 of the selected studies 28-39, there was improvement in exercise capacity. Ten of 11 studies found improvements in HRQL, with mean changes being
PR for COPD: Clinical, Economic, and Budget Impact Analysis 23
greater than the MCID in eight studies. The mean values for changes in exercise capacity were less than the MCID in seven of 11 studies. These findings are consistent with those in earlier reviews showing improvements in HRQL.4,5 Seven studies were rated as being of good quality,28-34 four of fair quality,35-38 and one of poor to fair quality.39 Two studies (of high and good quality, respectively)24,26 examining the effects of PR in patients who had been admitted to hospital because of acute exacerbations reported contrary findings. One found clinically significant improvements in exercise capacity and health status at three months; the other found no difference between groups in these measures. A retrospective cohort study27 found clinically significant improvement in exercise capacity and HRQL across all MRC grades. The longer-term comparisons of PR and usual care gave mixed results. A fair-quality, non-randomized study35 found the disappearance of benefits over time. One high-quality44 and one fair-quality study38 found that the improvements in exercise capacity were maintained over 12 and six months but with mean values below the MCIDs. Three high- or good-quality studies found benefits in exercise capacity and HRQL at six months or more, with mean values above the associated MCIDs. In one of these studies, the benefits in exercise capacity and HRQL were sustained for 18 months after the end of the PR program.45 A high-quality study found that the improvement in cycle endurance time (above MCID) was maintained, and HRQL scores remained greater than those of controls at 20 months post-PR, although PR had no effect on 6MWD.43 A good-quality study found improvements in HRQL measures, but not in exercise capacity, and remained above the MCID at 12 months.34 Four high- or good-quality studies compared maintenance programs and usual care following the end of PR.50-53 Two of these studies found that home-based exercise training was effective as maintenance, with benefits being maintained at six months50 and at 12 months51 after the end of PR. The other two studies found more limited benefits from maintenance. A 12-month program produced modest improvements in the maintenance of benefits, with no differences from usual care at 24 months.53 In the other study, the limited improvement at six months had disappeared by 12 months.52 A good-quality study, which compared the outcomes of patients who participated in two or three PR programs over 12 months, found statistically significant improvements after the end of each PR program, with benefits being totally or partially lost between programs.54 Two observational studies found benefits after lengthy PR and maintenance programs.56,57 Benefits were maintained to two years in the first study and to three years after the end of the program in the second study. Such findings suggest that the benefits of PR can be maintained in the long term, depending on patient adherence and availability of lengthy rehabilitation and maintenance programs. COPD is characterized by increased incidences of depression and anxiety. Through the typical group setting and interaction with health-care professionals, basic PR programs provide social support to patients. Therefore, PR is likely to improve psychosocial outcomes in patients. Six comparisons of PR and usual care (four rated as high or good quality) reported improved mental health outcomes up to three months following PR.26,33,58-61
PR for COPD: Clinical, Economic, and Budget Impact Analysis 24
A reduction in scores for anxiety and depression were noted in four studies that compared PR using different approaches or in different settings.62-65 In one of these studies, the scores remained above baseline at eight months.62 In another, the differences from baseline in anxiety and depression declined from six weeks to six months following PR.63 COPD is a burden to health care, because patients who are poorly managed often experience exacerbations of their lung condition, present at emergency rooms, and are hospitalized for several days receiving treatment. A goal of PR is to help patients learn how to self-manage their disease. Therefore, PR as a component of chronic COPD management2 would help reduce COPD-related health care utilization. The indications of reduction in health care utilization, including hospital admissions and length of stay, were included in ten studies24,26,34,45,48,51,56,57,68,69 that compared PR with usual care. In four high- or good-quality studies, there was lower utilization by groups who had PR.24,26,34,45 The differences from comparison groups were statistically significant in one of these.34 Another good-quality study found a reduction in the number of admissions in two types of PR programs but did not provide a statistical comparison between them.67 Four studies found reductions in hospital utilization over periods of 12 months. Three of these studies were of poor to fair or poor quality, and all used before-after designs. The combined findings indicate that improvements in health outcomes are observed immediately after PR. The benefits of PR may not be maintained in the months or years after PR. This indicates that PR can be effective at improving patient health, and that better maintenance programs help transition patients from the typically clinic-based PR program back into the community. PR and other treatments Several studies examined the effectiveness of adjunct airway therapies in combination with PR. These included an evaluation of the use of tiotropium in addition to PR. When bronchodilation is maximized, patients would have reduced dyspnea and could exercise at higher intensities during PR.66,71,73 It was unclear from these studies whether or not the inclusion of tiotropium in PR programs offered statistically significant additional benefit. Studies on the use of NIPPV with PR had contrasting results. A good-quality study found that this approach offered no advantages over the use of PR.74 In a poor- to fair-quality study,75 those using NIPPV plus PR had better exercise tolerance and HRQL than patients who only used PR. Replacing nitrogen with helium in the air that patients breathe reduces the work of breathing, allowing patients to exercise at higher intensities during PR. A high-quality study found statistically significant benefits for patients who used a mixture of helium and oxygen during PR.76 This approach merits further investigation. Two studies (high and good quality) found that lung volume reduction surgery gave greater improvement than PR alone.78,79 A small study with severely disabled patients found PR plus electrical stimulation produced greater improvement in HRQL and 6MWD than PR alone.80
PR for COPD: Clinical, Economic, and Budget Impact Analysis 25
PR context and operation Patients: Fourteen studies addressed PR in terms of patient characteristics. Three studies (fair quality, poor to fair quality, and not assessed) found that PR programs benefited patients who were 80 years or older, 65 years or older, and 77 years old.81-83 A fair-quality study found that patients with COPD and a history of acute exacerbations had less favourable PR outcomes than those without.39 Six other studies that considered disease severity (two fair quality,85,86 four poor to fair or poor quality87-90) reported the benefits of PR among patients with all grades of dyspnea. Fair- and good-quality studies from the National Emphysema Treastment Trial (NETT) found that surgical patients and those with more than 20% predicted FEV1 and higher education were more likely to complete PR, and that those with no previous PR benefited more than those who had used previous PR.91,93 Two fair-quality studies reported that PR had similar effects in women and men.85,94 Another fair quality investigation found that men improved their walking distance statistically significantly compared with women.37 Combined, these studies suggest that patients with COPD can benefit from the use of PR, regardless of age, disease severity, and sex. Settings: Two high-quality studies found home-based PR programs provided similar benefits to patients compared with hospital outpatient PR programs.67,95 Patients with COPD often list transportation issues as a limitation to PR participation. Therefore, home-based PR programs would eliminate this barrier to PR participation, while increasing the system’s capacity to deliver PR. Environmental conditions could affect patient participation and the outcomes derived from PR. A high-quality study found there was no difference in outcomes between patients treated in a cold climate and those treated in a warm climate.62 Duration of PR: The appropriate duration and content of PR programs are unclear based on the studies that were included in this review. One study found that a shortened (four-week) PR program plus three weeks of home rehabilitation gave similar results to those of a seven-week program.96 Two studies reported increased benefits at 20 and 24 weeks compared with those at 10 and 12 weeks.63,98 Approaches to exercise training: The use of 24 supervised training sessions improved dyspnea and exercise performance more than two other exercise approaches with less supervision.99 General exercise training is as effective as individually targeted training.100 Three studies found that high-intensity continuous exercise and interval exercise gave similar results for exercise capacity and HRQL.25,102,103 The addition of IMT to exercise training did not produce statistically significant additional benefit (fair-quality study).105 Combined, these studies indicate that more supervision is beneficial, while individually prescribed exercise training or high- intensity training does not seem to be of added benefit. 4.2.5 Elements of PR programs
Little information was obtained from the reviewed studies on the effectiveness of different components of PR programs. A high-quality study showed benefits to HRQL and hospital stay
PR for COPD: Clinical, Economic, and Budget Impact Analysis 26
from behaviour training and development of individualized action plans for patients.70 Good- quality studies indicated the feasibility but not the efficacy of using a pedometer with exercise counselling,106 and showed that supervised physical activity with controlled breathing in activity training was more effective in improving functional status and HRQL than didactic instruction.107 Three studies (two good-quality111,112 and one fair-quality113) on the influence of creatine supplements found no benefits in exercise performance. One found an improvement in HRQL. A good-quality study found that patients who used PR that included a psychotherapy component had clinically significantly better outcomes at 12 weeks compared with those whose rehabilitation excluded such an intervention. Two small studies that considered the effects of including strength training in PR found that there was no influence on exercise capacity.115,116
5 ECONOMIC ANALYSIS
5.1 Review of Economic Studies: Methods
5.1.1 Literature searches
The literature search strategy was applied for the clinical review and the economic evaluation (Appendix 1). For the review of economic studies, the main search concepts involved specific COPD rehabilitation programs and their impact on mortality, morbidity, and HRQL. We added the descriptors of “cost,” “cost-effectiveness,” “cost benefit,” “cost utility,” “cost consequence,” “cost impact,” “budget impact,” and “economic.” Methodological search filters were applied to limit retrieval to economic studies. 5.1.2 Selection criteria
We used the same selection criteria as were chosen for the clinical review, except that the outcomes of interest were costs and clinical outcomes. a) Inclusion criteria We included all studies that were analyses of comparative interventions and that had an economic component (measured the cost of implementing the technology). b) Exclusion criteria We excluded any study that did not report primary data and that did not contain program costs (but may have included service delivery costs). The approaches that were taken to information and data retrieval strategies were the same as in the clinical review. 5.1.3 Selection method
Two reviewers (PJ, AC) examined the results of the literature search and independently selected potentially relevant articles. First, the reviewers applied the inclusion criteria to the search results to select titles or abstracts that met all criteria. If all criteria were met or if there was uncertainty
PR for COPD: Clinical, Economic, and Budget Impact Analysis 27
or disagreement about an article’s eligibility, the paper was obtained in full text. Second, the reviewers selected the full texts that met all the inclusion criteria. They compared their findings and discussed any differences. Disagreements were resolved through consensus, or a neutral third party (DH) was consulted when needed. 5.1.4 Data extraction strategy
A data extraction form was developed before the research was started (Appendix 7). The data included study ID, country, description of setting, year, perspective, intervention (type of services included: education, counselling, and exercise therapy), hours per session, number of sessions per week, duration of the program, and time horizon. Cost elements included program costs with component breakdown, utilization costs for COPD, cost for each element, method of estimating each cost element, clinical outcome (from clinical review), cost-effectiveness ratio, and quality of study. The study data were extracted by one reviewer (PJ) and verified by a second (AC). Disagreement was resolved through consensus, and a neutral third party (DH) was consulted when needed. 5.1.5 Strategy for quality assessment
Our quality score was based on Drummond and Jefferson’s checklist,121 which we adapted to the current issue of pulmonary rehabilitation. Nine quality-related questions were addressed, and each was assigned a score of 1 (criteria met positively) or 0 (issue inappropriately addressed): Is the perspective clear? Does the study include post-program outcomes? Does the study include post-program services (utilization)? Are all relevant services included? Do the authors present physical measures for services? Do the authors measure the full cost (for example, including all relevant resources and
overhead costs) of the services? Do the authors present unit costs for each service? Is an incremental analysis conducted? Is uncertainty accounted for?
Other quality indicators, such as the use of discounting, were excluded because they were irrelevant in this setting. 5.1.6 Data analysis methods
The design of PR varied between studies, and there was no standard. The outcomes that were used varied and, because program design varied, there was no standard cost measure. As a result, the authors of this report could not develop an integrative analysis. Therefore, we conducted a descriptive analysis.
PR for COPD: Clinical, Economic, and Budget Impact Analysis 28
5.2 Review of Economic Studies: Results
5.2.1 Results of search strategy
From the electronic search we obtained 1,494 citations (Figure 2). We obtained eight citations from other sources, for a total of 1,502 citations. After the screening, we excluded 1,476 citations. Disagreement on 10 citations was resolved by discussion. Of the 26 potential articles that we retrieved, 17 were excluded. The reasons for exclusion were absence of program costs (2), foreign language (2), and irrelevant articles (13). Eight of the nine articles that met our criteria for inclusion were comparisons of PR with no intervention. One was a comparison of inpatient PR with outpatient PR. Of the eight articles that compared PR with no PR, seven focused on outpatient rehabilitation and one on a combination of inpatient and outpatient rehabilitation.
5.2.2 Review of pulmonary rehabilitation versus no rehabilitation Eight papers compared PR to no rehabilitation (Appendix 8). Five studies were published after 2000 and three were published in the late 1990s. In seven papers, the rehabilitation was conducted in an outpatient setting. In one paper, the intervention started in the inpatient setting and then continued in the outpatient setting. a) White et al.122 White et al. conducted a pre-post study of a six-week, 30-hour total PR program. The program included exercise, education, and counselling. The outcomes included distance walked in six minutes and components of the CRQ.123 Costs included program costs, with no utilization of health services. Of 42 persons who began the program, 36 completed it. At six weeks, three of the four CRQ components (dyspnea, emotion, and mastery) increased at a clinically important and statistically significant level. Changes in the fourth component, fatigue, were not clinically significant. The cost of the program was estimated at £400 per person. There was no incremental ratio, and we assigned the study a quality score of 2 out of a maximum of 9 points. b) Scherer and Schieder124 Scherer and Schieder compared a one-year pre-program with up to five years post-program analyses of hospital utilization. The intervention took 54 hours (36 1½ hour interventions) over a 12-week period. The program had three components — education, counselling, and exercise training. There were no health outcomes assessed. The only outcome was a questionnaire, six years after the end of the program, asking how many days the person was hospitalized during one year before the program and each of five years afterwards. The study found that hospitalization was lower in each of the four years after the program; there were difficulties with data in the fifth year. The cost of the program was estimated to be between $1,500 and $2,000. There was no incremental ratio. We rated the study a score of 3 out of 9 because of the lack of measurements.
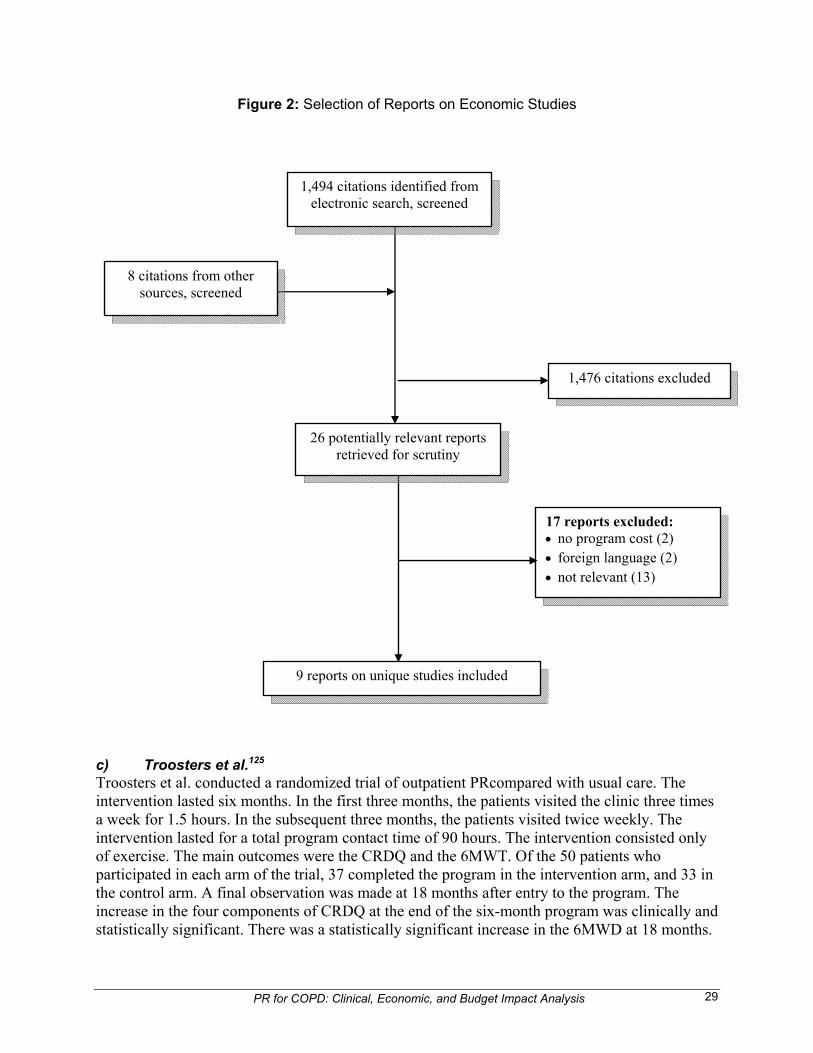
PR for COPD: Clinical, Economic, and Budget Impact Analysis 29
Figure 2: Selection of Reports on Economic Studies
c) Troosters et al.125 Troosters et al. conducted a randomized trial of outpatient PRcompared with usual care. The intervention lasted six months. In the first three months, the patients visited the clinic three times a week for 1.5 hours. In the subsequent three months, the patients visited twice weekly. The intervention lasted for a total program contact time of 90 hours. The intervention consisted only of exercise. The main outcomes were the CRDQ and the 6MWT. Of the 50 patients who participated in each arm of the trial, 37 completed the program in the intervention arm, and 33 in the control arm. A final observation was made at 18 months after entry to the program. The increase in the four components of CRDQ at the end of the six-month program was clinically and statistically significant. There was a statistically significant increase in the 6MWD at 18 months.
1,476 citations excluded
17 reports excluded: no program cost (2) foreign language (2) not relevant (13)
9 reports on unique studies included
1,494 citations identified from electronic search, screened
8 citations from other sources, screened
26 potentially relevant reports retrieved for scrutiny
PR for COPD: Clinical, Economic, and Budget Impact Analysis 30
The cost of the program was US$2,615 per person. Utilization was not measured. We gave the study a quality score of 4 out of 9, because of missing information. d) Jenkins et al.126 Jenkins et al. conducted a baseline post-analysis of an exercise program. The program was held in a clinic, and patients attended twice a week for one hour. The program lasted eight weeks (16 hours in total). Of the 72 patients who were enrolled, 57 completed the program. The outcomes were the CRQ and SF-36, which were measured at the end of the eight-week period. The authors measured program costs but did not measure utilization of health services related to COPD. The program costs excluded overhead costs. In total, the program cost was A$249 per person. The outcomes increased at eight weeks, compared with baseline, and were clinically significant. We rated the study a score of 5 out of 9, because of the lack of follow-up data, incomplete measures of costs, and no comparison group. e) Griffiths et al.127 Griffiths et al. conducted a randomized trial in an outpatient setting that compared PR to usual care. The patients attended three two-hour sessions for six weeks (36 hours). The program included education, counselling, and exercise sessions. Of the 99 patients who were enrolled in the study group, 92 completed the program; and of the 101 in the control group, 88 completed the program. The final observation period was at 12 months. The outcomes were the SF-36, from which quality-adjusted life-years (QALYs) were derived. The study included care related to the patient’s condition, for up to one year. The cost of the intervention included operating costs, overhead costs, and transportation costs. The results indicated that the net difference in QALYs was + 0.03. The cost of the intervention program was £725 (Cdn$1,450), and the cost of health care was £1,671 for the study group and £1,826 for the control group over the observation period. Using probabilistic analysis, 95% of all observations fell below £17,000 per QALY. We assigned a quality score of 9/9 to the study. f) Golmohammadi et al.7 Golmohammadi et al. conducted a before-after analysis of an outpatient program. Participants completed the program in six weeks (three days per week) or eight weeks (two days per week). The sessions lasted 2.5 hours. The program provided education, counselling, and rehabilitation. The program costs included operating and overhead costs. The observation period for outcomes was the duration of the program and for costs it was twelve months. Hospitalization and outpatient services were measured for one year before and one year after the program. Utilization for a comparison group of non-attendees with COPD was also used. The outcomes for the 210 program participants were based on the SGRQ. The program cost per person was $1,092, and the program saved $344 in utilization. We assigned a quality score of 5/9 because of a lack of a comparison group. g) Cecins et al.128 Cecins et al. conducted a before-after analysis of an outpatient program. The program offered education and exercise therapy. The program had two sessions a week for eight weeks. Each session lasted 1.25 hours. The outcomes were measured at baseline and after eight weeks using the CRDQ, and utilization was measured after one year. Program costs included operating and overhead expenses. Of the 256 persons who enrolled in the program, 187 completed the program. The program cost A$292 per person, and overall there were savings of A$397,000. The

PR for COPD: Clinical, Economic, and Budget Impact Analysis 31
outcomes were statistically significant. We assigned a rating score of 7 and noted that an appropriate control sample was missing. h) Goldstein et al.129 Goldstein et al. conducted a combined inpatient-outpatient program for patients with severe COPD. The inpatient program lasted eight weeks (five days per week), and the outpatient portion lasted eight weeks. The program was an RCT with the comparison group being usual care. The program included counselling, education, and exercise therapy. The observation period lasted 24 weeks. The outcomes included walking distance in a given time and CRDQ. The program costs included overhead and operating expenses. The authors excluded utilization for COPD. The results showed that CRQ improved in the study group, with the difference in CRQ mastery being 0.7. The program cost $12,251 per person; the same services that were used by the control group cost $663. The authors provided a cost per unit, with the cost for achieving a clinically significant outcome being $28,893. We assigned this study a quality score of 7, and note that utilization for COPD is missing. i) Clini et al.130 Clini et al. compared inpatient to outpatient pulmonary rehabilitation in patients with chronic airway obstruction (a combination of patients with COPD and with asthma). The inpatient group was offered 11 daily sessions over 19 days, each session lasting three hours. The outpatient group was offered 21 sessions over eight weeks. These sessions also lasted three hours. The intervention in each arm included education, counselling, rehabilitation, and exercise. The observation period was the period of the intervention. The patients were assigned to each arm using randomization. The outcomes included respiratory muscle strength, maximal inspiratory pressure, and expiratory pressure. The program costs included operating costs, overhead costs, and transportation costs of providing the rehabilitation services. The costs of hospital stay were excluded. Health services use was excluded. The outpatient services cost more (€3,677) than inpatient services (€2,720), because there were more outpatient sessions. The outcomes were similar. We assigned a quality score of 6/9. The study did not have any information on post-program utilization and outcomes. 5.2.3 Summary of results
In eight of nine studies, the intervention was on an outpatient basis. These eight studies did not have a common intervention. Rehabilitation or exercise was provided in all of them, patient education was provided in six, and counselling was provided in three. The cost per participant ranged from US$292 to US$2,615. In the full-service group, the cost ranged from US$800 to US$1,450. Therefore, the mean cost was approximately $1,100. There were insufficient data on utilization to make generalizations. The best documented study of health system costs was Griffiths’s127 study, which showed a reduction of approximately 150 GB Pounds Sterling in the intervention group. As a result, it was not possible to provide a numerical cost-effectiveness result. The outcomes were better in the study groups, but the outcome measures were not uniform. Whether the study used CRQ, QALYs, or SGRQ, the outcomes were better during the study period. In the two studies with physical measures, the outcomes improved.
PR for COPD: Clinical, Economic, and Budget Impact Analysis 32
5.3 Primary Economic Evaluation: Methods
5.3.1 Type of economic evaluation
We conducted a cost-utility analysis because the outcomes focussed on changes in HRQL that are affected by COPD exacerbations. Survival is not a key outcome indicator because of the short-term impact of PR. 5.3.2 Target population
The patients with COPD in the economic model were representative of those who had COPD in a national (United States) population consisting of 79% males, 21% females, 87% white, those of an average age of 61 years (standard deviation 7.7), and 97% current or former smokers.131 All persons with COPD, whatever the severity, are included in the analysis, because all are potential candidates for PR use. 5.3.3 Comparators
The cost-utility analysis was used to compare the costs and health outcomes between usual care (pharmacotherapy) and usual care plus pulmonary rehabilitation. Usual care as pharmacotherapy is assumed to be optimal (it is assumed that all persons with COPD get long-acting anti-cholinergics). It is assumed that persons with stage 2 and 3 (GOLD criteria) COPD also get combination therapy (long-acting beta agonists and corticosteroids). PR includes exercise therapy, education, and counselling. The PR program consisted of three sessions per week at 2.5 hours per session over six weeks (total of 45 hours), which is the approximate average based on all programs that reported such data. Pulmonary rehabilitation is given to patients once. Pharmacotherapy is continual COPD care. 5.3.4 Perspective A health system perspective was taken in the analysis. This includes government and private payers. We included all the resources that are used to produce pulmonary rehabilitation, all affected health services, and all pharmaceuticals. For pharmaceuticals, government plans vary by province. We have included all drug costs. Pulmonary rehabilitation is not provided widely in any province. It is not an “insured” service that is federally mandated. Because it is a “health service,” its full cost is included. 5.3.5 Effectiveness
Based on the clinical review, there is evidence that the use of PR reduces the risk of exacerbations compared with usual care. There is no evidence of a differential impact on mortality, and there was little information describing usual care. Nevertheless, a baseline treatment is needed for the comparative analysis. In this analysis, usual care is based on the CTS guidelines of providing for stage 1 COPD and long-acting anti-cholinergics, and CT for stages 2 and 3.
PR for COPD: Clinical, Economic, and Budget Impact Analysis 33
5.3.6 Time horizon
Based on the clinical review, no studies evaluated the efficacy of PR longer than three years. Hence, it is uncertain whether or not the benefits of PR will last that long without a booster. Accordingly, the base case simulation model evaluates PR in one scenario ― an 18-month horizon.34 There is evidence of a one-year program with a home exercise booster having a positive impact at three years.56 This alternative is covered in a sensitivity analysis. 5.3.7 Modelling
All analyses were conducted using Microsoft EXCEL and TreeAge Pro Suite (TreeAge Software Inc; Williamstown, MA). The simulation model is based on an epidemiologic model of the natural progression of COPD (Figure 3). The assumptions and sources appear in Table 1. In the model, patients are divided into three mutually exclusive disease severity categories:132 Stage 1 disease was defined as forced expiratory volume in one second (FEV1) 50.0% or
more of predicted. Stage 2 disease was defined as FEV1 of 35.0% to 49.9% of predicted. Stage 3 disease was defined as FEV1 less than 35.0% of predicted.
It is assumed that at baseline, 93% of the patient population had stage 1 disease, 4% had stage 2 disease, and 3% had stage 3 disease.131 Over time, less severe stages of COPD progress to more severe stages because of declining FEV1. Using estimates of the mean rate of FEV1 reduction for each severity group from the literature, the model simulates the three-month transition probability for a person in stage1 progressing into stage 2 and a person in stage 2 progressing into stage 3. For each three-month cycle, there is a probability of death. All-cause mortality rates for COPD were estimated to be 3.92% in stage 1, 6.16% in stage 2, and 9.24 % in stage 3 disease.133 All-cause mortality was chosen because patients with COPD may die from the complications of COPD and other causes, and the distinction may be unclear. Furthermore, there is an increasing frequency of exacerbations and a possible increased risk of mortality associated with the more severe stages of COPD. COPD exacerbations can be divided into three mutually exclusive categories:134 Mild: Defined as worsening of symptoms requiring routine physician services and the use of
medications or antimicrobials (exacerbation therapy). Moderate: Defined as clinical episodes requiring emergency department services. Severe: Defined as requiring inpatient care (including exacerbation therapy). a) Economic model The economic model is shown in Figure 3. Exacerbations, which are the primary driver of health services utilization costs, negatively affect HRQL. For each comparator, all patients are followed over six intervals. During each interval, they face a probability of mild, moderate, or severe exacerbations, depending on the severity of the person’s COPD. They stay in a given cycle, progress to a higher level of severity, or die. Over the 18-month period of the model, each person accrues exacerbations (by severity), health outcomes (QALYs), and health services utilization and costs. The resulting 18-month costs and health outcomes of each comparator are compared with the alternative to estimate the cost-effectiveness analysis.
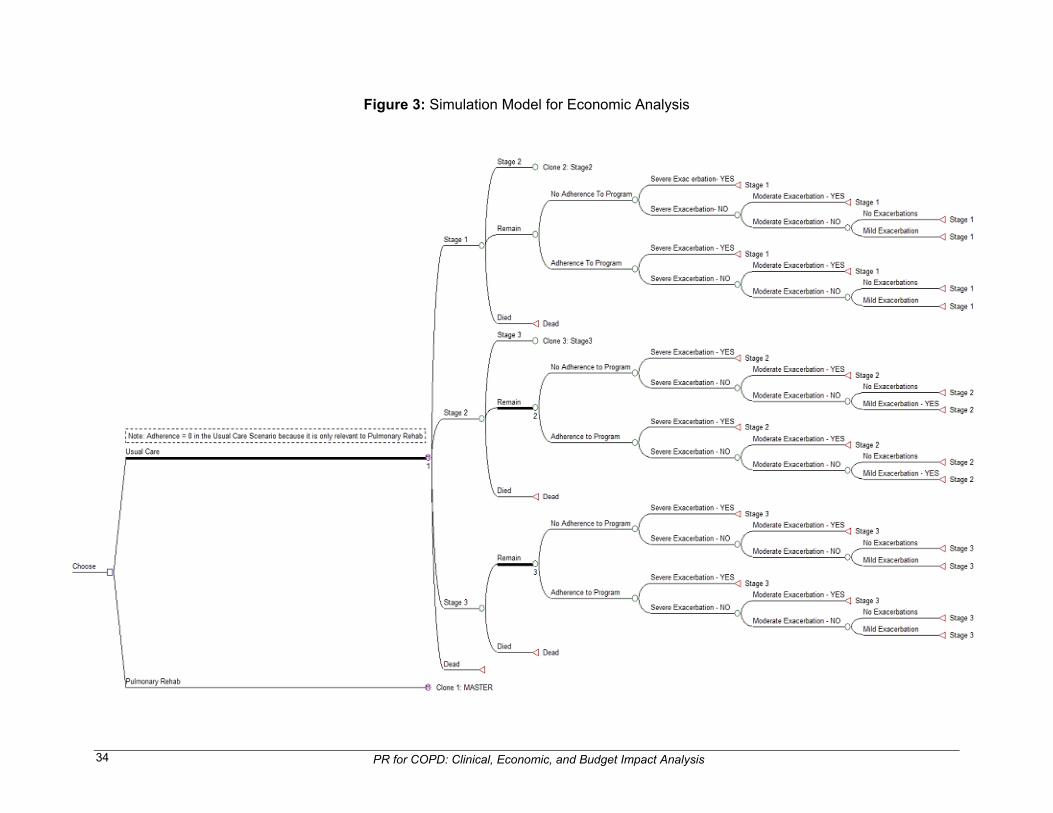
PR for COPD: Clinical, Economic, and Budget Impact Analysis 34
Figure 3: Simulation Model for Economic Analysis
PR for COPD: Clinical, Economic, and Budget Impact Analysis 35
5.3.8 Valuing outcomes
a) Health outcomes HRQL is measured in QALYs. A QALY based on the EQ-5D was obtained for the duration of each of the three stages (Table 1). The EQ-5D provides descriptive health status scores ranging from −0.59 to 1.00.135 A score of 0.0 represents death, and a score of 1.0 represents perfect health. Negative scores represent health states that are considered to be worse than death. The minimally important clinical difference for the EQ-5D is 0.074.135 A QALY weight is applied to each stage of COPD (baseline index of HRQL associated with the stage of COPD). For each exacerbation event, QALYs are reduced by a specific amount, depending on the severity of the exacerbation (Table 1). 5.3.9 Resource use and costs
a) Model inputs Model inputs (for example, probabilities, costs, and outcomes) are derived from the clinical and economic review in this report, published literature, and databases. Canadian data will be used whenever possible. Costs: The cost of care consists of the costs of routine maintenance, exacerbations, pharmacotherapy, and pulmonary rehabilitation (Table 1). Routine maintenance services for persons with COPD were based on those found in Oostenbrink et al.’s136 study. The amount of services for routine maintenance care varied according to severity. The number of exacerbations by level of severity (Table 1) is based on data from recent studies. The services and costs increase with severity. A mild exacerbation leads to a physician visit and use of medications, a moderate one may lead to the use of additional emergency services, and a severe one may lead to the use of additional hospitalization, including ICU care. We used service estimates for Ontario from Mittmann et al.137 for the two higher levels of severity. All others were derived for Alberta (Table 1). The pharmacotherapy costs of alternative treatment regimens were based on recommended doses and 2008 drug prices as listed in the 2008 Alberta Health and Wellness drug plan formulary. The cost of the pulmonary rehabilitation program consisted of the costs of administration (13%), rent (3%), staff, and supplies, based on Golmohammadi’s7 study. All costs were updated to 2008 levels using the General Consumer Price Index, which was obtained from Statistics Canada. b) Criteria for cost-effectiveness The analysis will identify the differences in costs and QALYs between usual care, and usual care and PR. The criteria for concluding that PR is cost effective are (all comparisons are to usual care): If usual care plus PR is more costly and less effective, then usual care plus PR is not cost-
effective. If usual care plus PR is less costly and more effective, then usual care plus PR is cost-
effective.
PR for COPD: Clinical, Economic, and Budget Impact Analysis 36
If usual care plus PR is more costly and more effective, then it is uncertain whether usual care plus PR is cost-effective, because it depends on whether or not decision-makers deem the additional effectiveness to be worth the additional costs. The ICER is the ratio between the differences in costs and in QALYs between usual care
and usual care plus PR. The ICER is compared with a minimally acceptable value (represents a decision-maker’s willingness to pay for an additional unit of improvement) to conclude whether usual care plus PR is cost-effective. A cost per QALY threshold of $ Cdn 50,000 is commonly used as a threshold for determining cost-effectiveness.138 Therefore, usual care plus PR is considered to be cost-effective if its ICER is below a threshold of $50,000 per QALY gained.
5.3.10 Discount rate
All costs were discounted at 5% for the base case, and at 3% and 0% for sensitivity. Given the 18-month time span of the study, the discount rates are of minor importance to the results and are not reported in the sensitivity analysis. 5.3.11 Variability and uncertainty
a) Sensitivity analysis A probabilistic sensitivity analysis was conducted using 100,000 Monte Carlo simulations to generate the distribution of potential costs and effectiveness associated with each treatment. We conducted one-way sensitivity analysis for the following variables: Relative risk from pulmonary rehabilitation: The only estimate for this variable was obtained from Güell et al.45 (0.48). We used probability estimates ranging from a low value of 0.28 to a high value of 0.68. Program cost: We assumed a low value of $250 per person128 and a high value of $5,400130 per person. We also estimated the cost at which the ICER was equal to $50,000. Duration of benefits: There was variation in the estimates of the duration of benefits. The most common measure was twelve months.34,44,49,51 Güell et al.45 reported an impact at 18 months, and Lomundal and Steinsbekk56 reported an effect at three years, although the latter was with a booster. We estimated cost-effectiveness at two years, three years, and the base case, which was for 18 months. Program uptake: In our base case, we assumed a program uptake of 80%. We also estimated the cost-effectiveness with a 60% uptake. Exacerbations: There are differences in the literature on exacerbation rates. We used an alternative set of rates, based on Sin et al.132 This set of numbers had fewer exacerbations overall, with almost all the difference being in the mild and moderate groups. Severe cases had the same number of exacerbations.
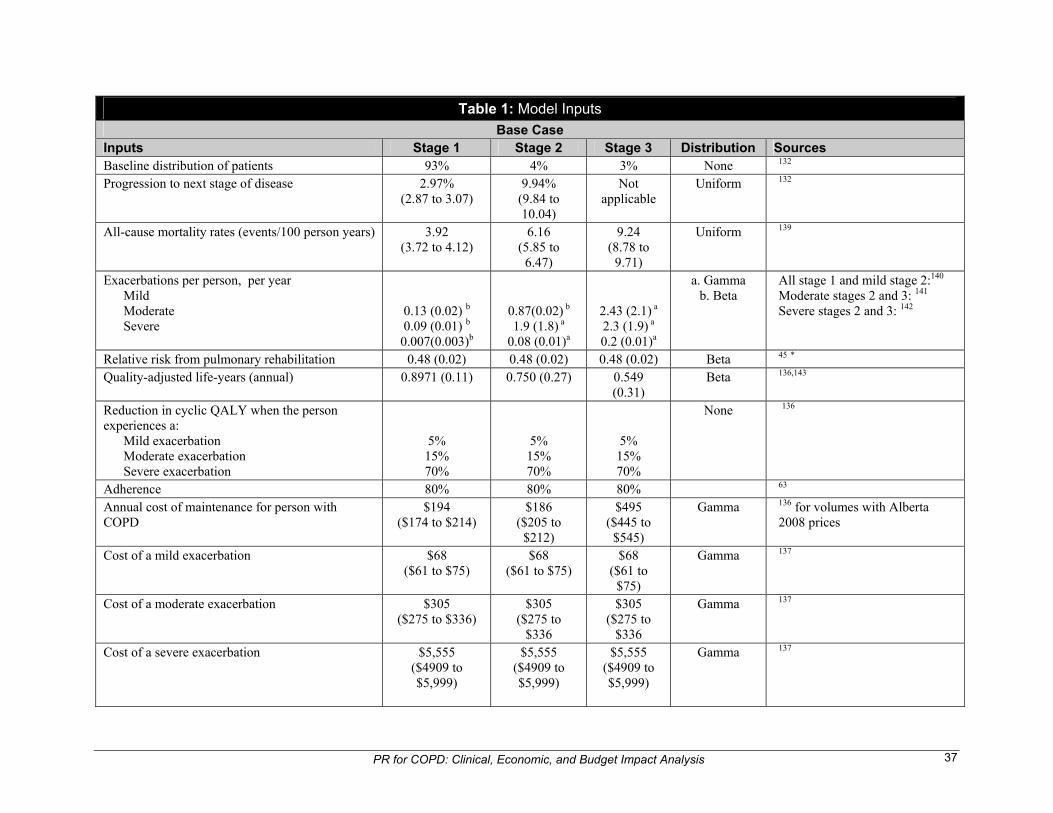
PR for COPD: Clinical, Economic, and Budget Impact Analysis 37
Table 1: Model Inputs
Base Case Inputs Stage 1 Stage 2 Stage 3 Distribution Sources Baseline distribution of patients 93% 4% 3% None 132 Progression to next stage of disease 2.97%
(2.87 to 3.07) 9.94%
(9.84 to 10.04)
Not applicable
Uniform 132
All-cause mortality rates (events/100 person years) 3.92 (3.72 to 4.12)
6.16 (5.85 to
6.47)
9.24 (8.78 to
9.71)
Uniform 139
Exacerbations per person, per year Mild Moderate Severe
0.13 (0.02) b 0.09 (0.01) b 0.007(0.003)b
0.87(0.02) b 1.9 (1.8) a
0.08 (0.01)a
2.43 (2.1) a 2.3 (1.9) a 0.2 (0.01)a
a. Gamma b. Beta
All stage 1 and mild stage 2:140 Moderate stages 2 and 3: 141 Severe stages 2 and 3: 142
Relative risk from pulmonary rehabilitation 0.48 (0.02) 0.48 (0.02) 0.48 (0.02) Beta 45 * Quality-adjusted life-years (annual) 0.8971 (0.11) 0.750 (0.27) 0.549
(0.31) Beta 136,143
Reduction in cyclic QALY when the person experiences a: Mild exacerbation Moderate exacerbation Severe exacerbation
5% 15% 70%
5% 15% 70%
5% 15% 70%
None 136
Adherence 80% 80% 80% 63 Annual cost of maintenance for person with COPD
$194 ($174 to $214)
$186 ($205 to
$212)
$495 ($445 to
$545)
Gamma 136 for volumes with Alberta 2008 prices
Cost of a mild exacerbation $68 ($61 to $75)
$68 ($61 to $75)
$68 ($61 to
$75)
Gamma 137
Cost of a moderate exacerbation $305 ($275 to $336)
$305 ($275 to
$336
$305 ($275 to
$336
Gamma 137
Cost of a severe exacerbation $5,555 ($4909 to $5,999)
$5,555 ($4909 to $5,999)
$5,555 ($4909 to $5,999)
Gamma 137
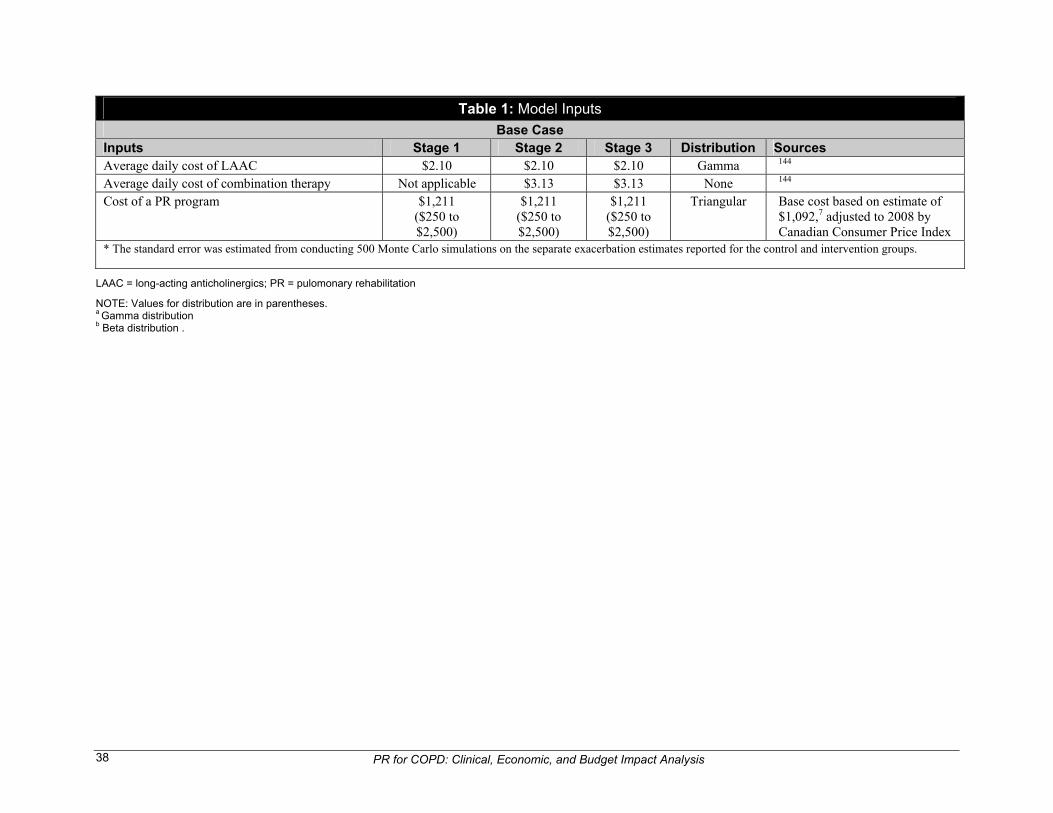
PR for COPD: Clinical, Economic, and Budget Impact Analysis 38
Table 1: Model Inputs
Base Case Inputs Stage 1 Stage 2 Stage 3 Distribution Sources Average daily cost of LAAC $2.10 $2.10 $2.10 Gamma 144 Average daily cost of combination therapy Not applicable $3.13 $3.13 None 144 Cost of a PR program $1,211
($250 to $2,500)
$1,211 ($250 to $2,500)
$1,211 ($250 to $2,500)
Triangular Base cost based on estimate of $1,092,7 adjusted to 2008 by Canadian Consumer Price Index
* The standard error was estimated from conducting 500 Monte Carlo simulations on the separate exacerbation estimates reported for the control and intervention groups.
LAAC = long-acting anticholinergics; PR = pulomonary rehabilitation
NOTE: Values for distribution are in parentheses. a Gamma distribution b Beta distribution .
PR for COPD: Clinical, Economic, and Budget Impact Analysis 39
5.4 Primary Economic Evaluation: Results
5.4.1 Analysis and results
a) Base case In the base model, costs and outcomes are driven by exacerbations. For the entire group of persons with all severity levels and without rehabilitation, the average number of mild exacerbations per year was 0.968. With rehabilitation, the average number of mild exacerbations was 0.624 per year (a difference of 0.344). The average person had 1.456 moderate exacerbations without rehabilitation and 0.904 exacerbations with rehabilitation (a difference of 0.552). The average person had 0.336 severe exacerbations without rehabilitation and 0.236 with rehabilitation (a difference of 0.1). Mild exacerbations only included those for which a physician visit was required. Some mild exacerbations may not have required care, but these are not reported in most studies. In the base-case model, a person with usual care and no rehabilitation had an average of 1.107 QALYs for an 18-month period. A person with rehabilitation had 1.149 QALYs over the 18- month period of the model. A person in “perfect” health would have a QALY of 1.500 during an 18-month period. In the base-case model, the cost per person without rehabilitation (including drugs and other maintenance costs) and costs for treating exacerbations over an 18-month period was $2,025. When rehabilitation is added, the costs increase to $3,209. The increased costs of rehabilitation ($1,211) are offset by a reduction in maintenance costs, so that the net difference is $27. b) Probabilistic results The cost-effectiveness of rehabilitation is calculated as the difference between costs and outcomes ($27,924 per QALY). The probabilistic results appear in Figure 4. The curve is steep, and almost 90% of all observations in the probabilistic analysis fall below $50,000 per QALY, which is an often-used threshold. c) One-way sensitivity analysis The results of the one-way sensitivity analyses appear in Table 2. We varied the key effectiveness variable, the relative risk of exacerbations with PR (base value 0.48) from 0.28 to 0.68. At 0.28, the ICER was almost $50,000. At 0.68, the ICER was $17,550 per QALY. Within a broad range of effectiveness, PR is cost-effective (under a threshold value of $50,000 per QALY). We varied the program costs from $250 to $5,400 per person, which is the range of programs in our literature review. At a program cost of $5,400, the ICER is $120,516 per QALY. PR would not be cost-effective if the program cost was this high. If the program cost were $2,300 per person, the cost per QALY threshold of $50,000 would be reached.
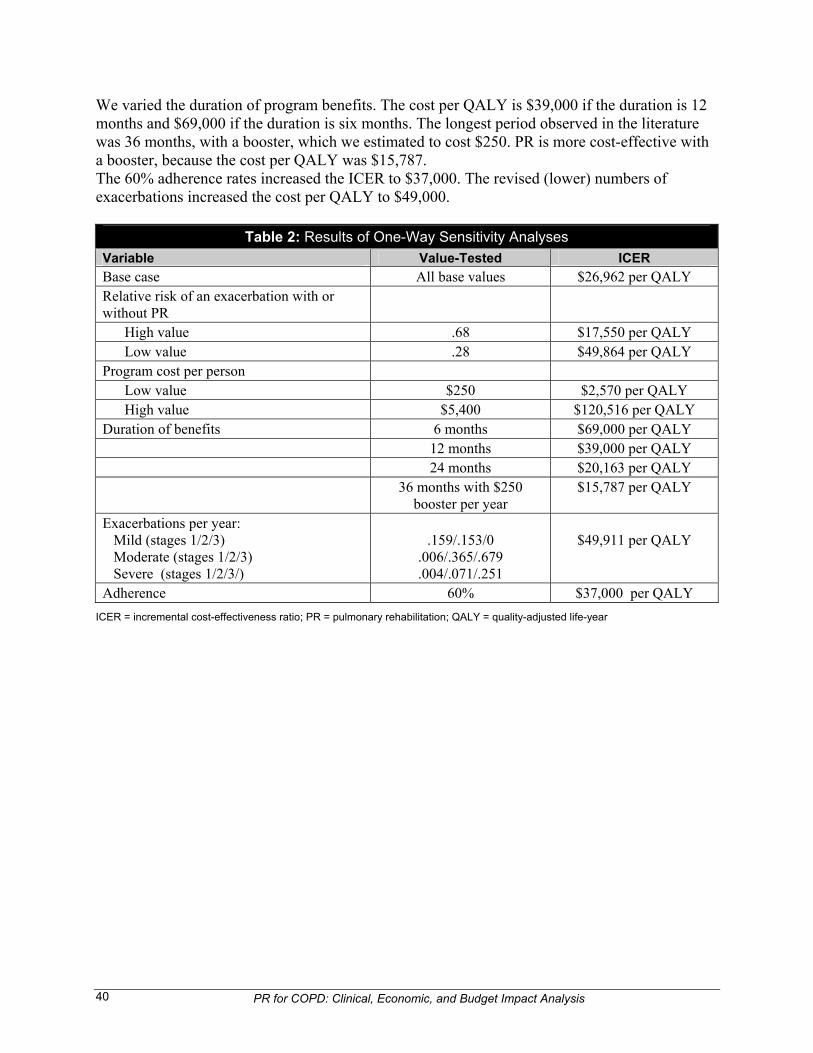
PR for COPD: Clinical, Economic, and Budget Impact Analysis 40
We varied the duration of program benefits. The cost per QALY is $39,000 if the duration is 12 months and $69,000 if the duration is six months. The longest period observed in the literature was 36 months, with a booster, which we estimated to cost $250. PR is more cost-effective with a booster, because the cost per QALY was $15,787. The 60% adherence rates increased the ICER to $37,000. The revised (lower) numbers of exacerbations increased the cost per QALY to $49,000.
Table 2: Results of One-Way Sensitivity Analyses
Variable Value-Tested ICER
Base case All base values $26,962 per QALY Relative risk of an exacerbation with or without PR
High value .68 $17,550 per QALY Low value .28 $49,864 per QALY Program cost per person Low value $250 $2,570 per QALY High value $5,400 $120,516 per QALY Duration of benefits 6 months $69,000 per QALY 12 months $39,000 per QALY 24 months $20,163 per QALY 36 months with $250
booster per year $15,787 per QALY
Exacerbations per year: Mild (stages 1/2/3) Moderate (stages 1/2/3) Severe (stages 1/2/3/)
.159/.153/0
.006/.365/.679
.004/.071/.251
$49,911 per QALY
Adherence 60% $37,000 per QALY
ICER = incremental cost-effectiveness ratio; PR = pulmonary rehabilitation; QALY = quality-adjusted life-year
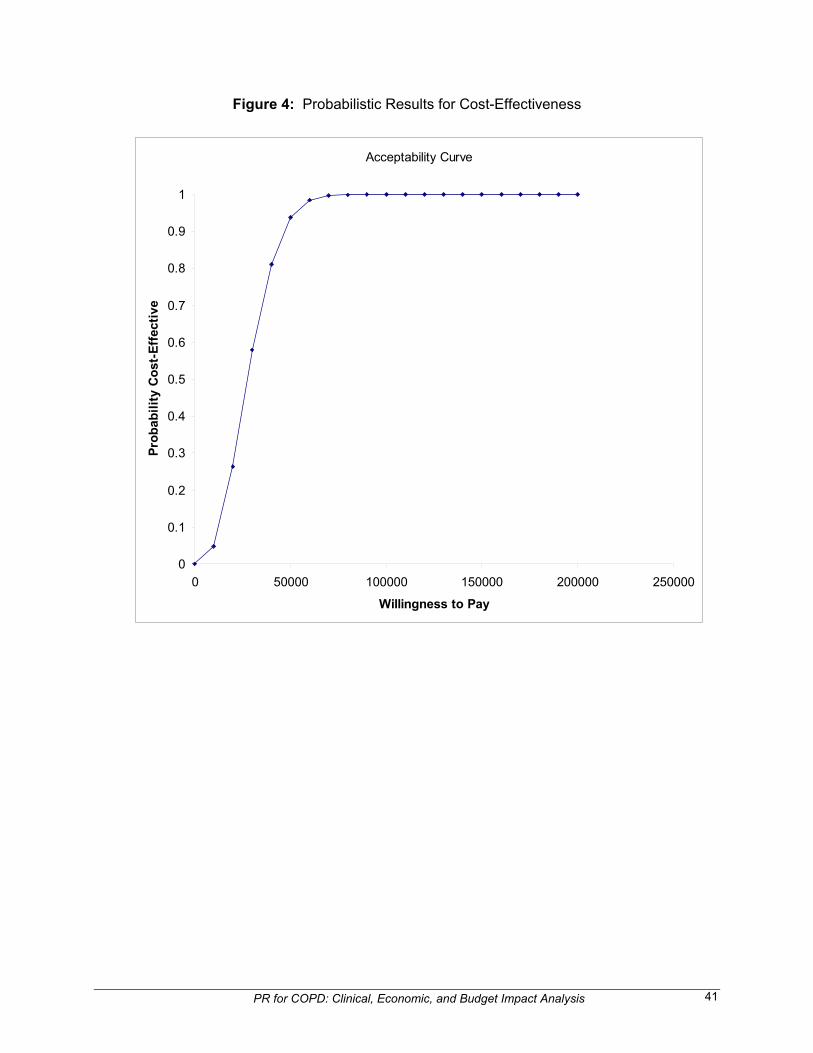
PR for COPD: Clinical, Economic, and Budget Impact Analysis 41
Acceptability Curve
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 50000 100000 150000 200000 250000
Willingness to Pay
Pro
bab
ilit
y C
ost
-Eff
ecti
ve
Figure 4: Probabilistic Results for Cost-Effectiveness
PR for COPD: Clinical, Economic, and Budget Impact Analysis 42
6 HEALTH SERVICES IMPACT
6.1 Population Impact
Few people with COPD receive PR. In 2006, it was reported that approximately 775,000 persons in Canada over the age of 35 years were diagnosed with COPD.145 The estimate for the capacity of all PR programs in 2005 was 8,927 persons,6 which is approximately 1.1% of the COPD population. It is unrealistic to assume that the capacity will meet all the recommended rehabilitation in one year. Therefore, the element of time must be considered in our analysis. Time enters into our budgetary analysis in two ways. First, it takes time to bring additional resources to PR. Health care providers plan for programs and then procure space and equipment. Appropriate personnel, including therapists, are hired from other positions, or they are trained. When a decision is made to increase rehabilitation services, it takes years for the health regions to put the resources into place. Second, because of the large number of persons with COPD who are not served, health regions will probably be unable to serve the entire target population using standard program designs. We can estimate the number of people who will or will not be served over a specified time frame. The budget analysis is then conducted over this period.
6.2 Budget Impact
6.2.1 Method
a) Budget impact model In the budget impact model, the goal is to meet the total need for PR over a selected time frame. We have chosen a time horizon of ten years to bring a more modest amount of resources into use. We begin the model using the Canadian COPD prevalence in 2006 for our baseline estimate. In each of the following ten years, the COPD population is increased by the COPD incidence and reduced according to the COPD mortality rate. Using COPD prevalence data, we estimate the number who are recommended to receive PR (who are in need) using different assumptions. The desired capacity for PR in each year is estimated as current capacity plus the number of additional persons served. We define the latter variable (additional persons receiving PR) so that the cumulative number served equals the total needs of the population by ten years. To estimate the budget impact of the additional services, we multiply the unit cost of PR by the number of additional persons served per year. b) Data COPD prevalence: We obtained an estimate of the population in each province by age group (35 to 44 years, 45 to 54 years, 55 to 64 years, 65 to 74 years, and 75 years or older) for 2008 from Statistics Canada. We obtained the country-wide percentage of persons in each age group who had been diagnosed with COPD from the Public Health Agency of Canada’s chronic disease
PR for COPD: Clinical, Economic, and Budget Impact Analysis 43
website. These data were based on the 2006 Statistics Canada Canadian Community Health Survey. We used the prevalence rate and the Canadian age-specific populations to obtain the number of persons with COPD nationally. COPD incidence: The incidence of COPD was based on a study from Rotterdam, the Netherlands,146 which included persons over the age of 55 years. We used this estimate because Canadian data were unavailable. The incidence was 9.2 per 1,000 person-years. Using the baseline number of persons with COPD in that study (11.6% of the baseline population), we estimated the incidence rate as a percentage of the baseline prevalence, which was 7.9%. COPD mortality: The mortality rate is the overall average Canadian rate of COPD mortality in 2006.145 Need for PR: We used different estimates to obtain the number of persons in each province who are recommended for PR. The guidelines of the National Institute for Health and Clinical Excellence (NICE) in
England suggest that 25% of persons with COPD are moderate or severe, and these persons should be targeted.147 We used these numbers (assuming 100% uptake) in our first estimate of program expansion because Canadian estimates were unavailable. Canadian guidelines are similar to those of NICE.
According to the NICE guidelines, there is an uptake of 67% in the UK. We adjusted the rate obtained in the first estimate by 67% to obtain a second estimate.
According to the CTS guidelines,2 all persons with COPD should receive PR, because early therapy has been shown to be beneficial. Therefore, in our third estimate, we assume that all persons should be offered services.
Using estimates from the United States National Health and Nutrition Examination Survey,132 7 % of persons with COPD have been classified as moderate or severe (FEV1 less than 50%). In a separate estimate, we will assume that only these persons will be provided with rehabilitation.
Cost of PR: We assume that the per person cost of pulmonary rehabilitation is $1,211. This is based on Golmohammadi’s Alberta estimate for an outpatient program in 20047 of $1,092, adjusted to 2008 by 110.9% using the Canadian Consumer Price Index.148 In the Edmonton program, the services included exercise therapy, education, and counselling. The program required persons to attend three times per week at 2.5 hours per session for six weeks (a total of 45 hours). There were 10 persons per class. The costs of this program consisted of administration costs (13%), rent (3%), and the remainder for staff and supplies. All are operating costs that are incurred by the health services or regions. Based on our economic literature review, there is a range of costs in programs. The differences are due to program content, the number of hours, and the size of the group. In our sample of five programs for which data were available (Jenkins et al,126 Troosters et al.,125 Golmohammadi et al.,7 Griffiths et al.,127 and White et al.122), two programs offered only exercise therapy; and three offered exercise therapy, counselling, and education. Total hours ranged from 16126 to 90,125 with the mode between 30 and 40 hours. Class size was between eight and 12 except in the Troosters et al.125 study, which had a staff to patient ratio of 1:1. As a result, there was a range in costs
PR for COPD: Clinical, Economic, and Budget Impact Analysis 44
from $250126 to $2,500.125 The mode was $1,200. Therefore, we used two additional values in sensitivity analyses: $250 per person and $2,500 per person. We estimated the cost of treating the entire target population and the additional cost of meeting their needs. The latter estimate was obtained by deducting the current costs of serving the 8,927 persons, based on the 2005 national capacity estimates.6 c) Results Details of the Canada-wide impact of expanding PR for the COPD population appear in Appendix 9. In Model 1, we use the baseline assumptions with no provision for program expansion; the volume of services remains at the current level (8,927 persons served) for ten years. At the end of that period, 89,000 persons will have been served, and the need for the surviving COPD population will have grown to 371,000 persons. Therefore, there will be approximately 281,000 persons who meet the NICE criteria, but who are unserved. There will be no additional budgetary needs. In Model 2, we assume a need for PR of 25% of persons with COPD (as in the NICE assumptions), with a 100% uptake. At the end of the ten-year period, the need will be for 371,000 persons served. To meet the need, approximately 28,000 additional persons will be served per year. This means an additional budget of $33.9 million annually. If only 67% of those who are in need use the services (Model 3), 15,900 additional places are needed annually. This requires an additional budget of $19 million annually. In Model 4, we make our estimates based on the assumption that all persons with COPD need PR. With this assumption, 139,000 additional persons will be served annually for an additional annual cost of $168 million. In Model 5, we assume that only the moderate and severe cases need PR. This will require that 1,505 additional persons are served annually, for an added cost of $1.8 million. In Table 3, we present a provincial breakdown of the estimated budgetary impact of the different models. The percentage breakdown is based on the distribution of the population who is over 65 years.
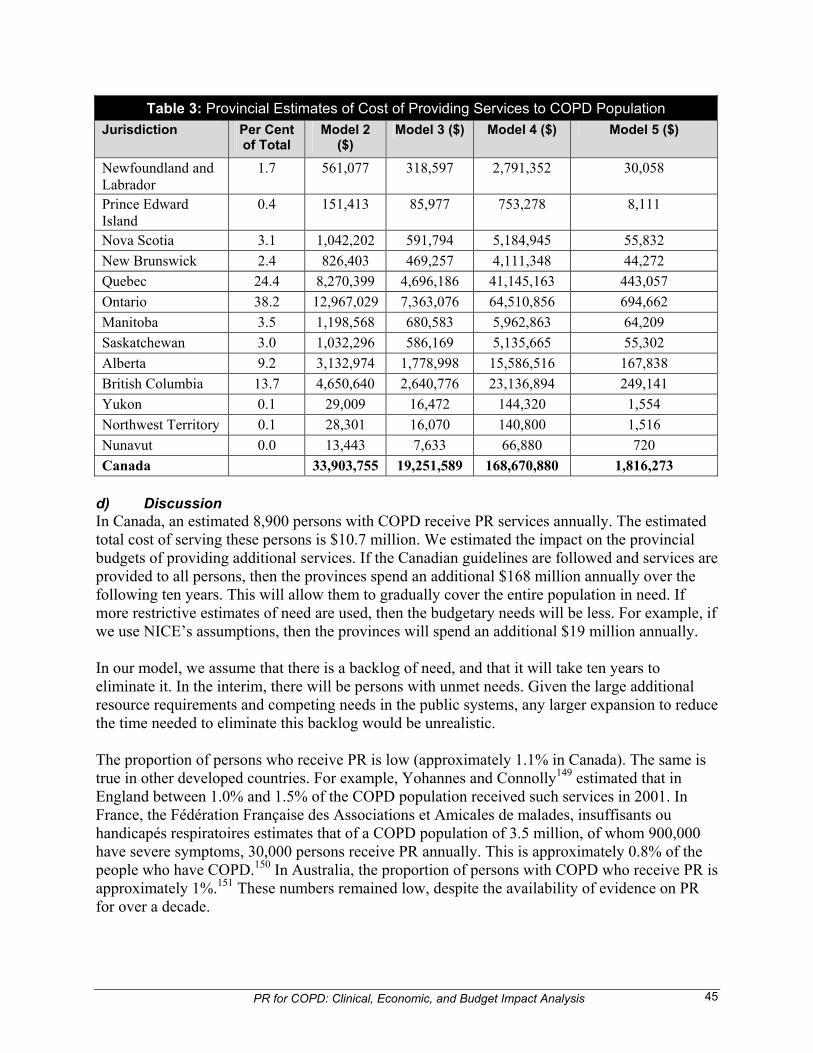
PR for COPD: Clinical, Economic, and Budget Impact Analysis 45
Table 3: Provincial Estimates of Cost of Providing Services to COPD Population
Jurisdiction Per Cent of Total
Model 2 ($)
Model 3 ($) Model 4 ($) Model 5 ($)
Newfoundland and Labrador
1.7 561,077 318,597 2,791,352 30,058
Prince Edward Island
0.4 151,413 85,977 753,278 8,111
Nova Scotia 3.1 1,042,202 591,794 5,184,945 55,832
New Brunswick 2.4 826,403 469,257 4,111,348 44,272
Quebec 24.4 8,270,399 4,696,186 41,145,163 443,057
Ontario 38.2 12,967,029 7,363,076 64,510,856 694,662
Manitoba 3.5 1,198,568 680,583 5,962,863 64,209
Saskatchewan 3.0 1,032,296 586,169 5,135,665 55,302
Alberta 9.2 3,132,974 1,778,998 15,586,516 167,838
British Columbia 13.7 4,650,640 2,640,776 23,136,894 249,141
Yukon 0.1 29,009 16,472 144,320 1,554
Northwest Territory 0.1 28,301 16,070 140,800 1,516
Nunavut 0.0 13,443 7,633 66,880 720
Canada 33,903,755 19,251,589 168,670,880 1,816,273
d) Discussion In Canada, an estimated 8,900 persons with COPD receive PR services annually. The estimated total cost of serving these persons is $10.7 million. We estimated the impact on the provincial budgets of providing additional services. If the Canadian guidelines are followed and services are provided to all persons, then the provinces spend an additional $168 million annually over the following ten years. This will allow them to gradually cover the entire population in need. If more restrictive estimates of need are used, then the budgetary needs will be less. For example, if we use NICE’s assumptions, then the provinces will spend an additional $19 million annually. In our model, we assume that there is a backlog of need, and that it will take ten years to eliminate it. In the interim, there will be persons with unmet needs. Given the large additional resource requirements and competing needs in the public systems, any larger expansion to reduce the time needed to eliminate this backlog would be unrealistic. The proportion of persons who receive PR is low (approximately 1.1% in Canada). The same is true in other developed countries. For example, Yohannes and Connolly149 estimated that in England between 1.0% and 1.5% of the COPD population received such services in 2001. In France, the Fédération Française des Associations et Amicales de malades, insuffisants ou handicapés respiratoires estimates that of a COPD population of 3.5 million, of whom 900,000 have severe symptoms, 30,000 persons receive PR annually. This is approximately 0.8% of the people who have COPD.150 In Australia, the proportion of persons with COPD who receive PR is approximately 1%.151 These numbers remained low, despite the availability of evidence on PR for over a decade.
PR for COPD: Clinical, Economic, and Budget Impact Analysis 46
Given the chronically low level of attention given to PR and the looming high budgetary needs, current budgetary requirements may not be realistic. One alternative would be to focus on less costly models of care. For example, Jenkins et al.126 studied a model of 16 hours in total, with a quarter of the cost of the inexpensive model that we used in the analysis. There is little evidence about the relative efficacy of models with varying levels of resource intensity. The limitations in information used in our analysis may have biased our results. First, commentators stated that COPD is incompletely reported, and that the true incidence is higher than the figures used in our analysis.145 If regions increased surveillance and the number of persons diagnosed, this would increase the need for PR. Second, we did not account for mortality in our estimate of patients served. Although the number would be small (approximately 1% annually), some of those who received PR would die during the period analysed, and the need would be greater than we stated, although this would not affect the order of magnitude of the results. Third, we assumed that the addition appeared in the first year of the program. In fact, it would take years to increase the capacity, and costs would be lower in the earlier years. The time horizon of ten years is an example. Any longer horizon would mean more persons would not be served in the interim. If health regions had a shorter adjustment period, then a greater strain would be placed on the health care system.
6.3 Planning, Implementation, Utilization, and Legal or Regulatory Considerations
Planners would need to consider the elements to be offered in a PR program, the duration of the program, and the nature and availability of subsequent maintenance. The availability of appropriately qualified health professionals would be essential. The economic model used in this assessment indicates that an incremental ICER for PR compared with usual care was $27,924. Information from the clinical review suggests that the duration of PR effectiveness will be relatively short in most programs. Those who plan and operate PR services should consider levels of participation in rehabilitation and maintenance programs. The ACCP/AACPR guideline notes the difficulties in achieving long-term patient participation. A relatively small proportion of patients who are offered a community-based exercise maintenance program will accept it and adhere to it. For example, Cockram et al. reported participation in PR and a subsequent community-based maintenance exercise program.152 Of 467 patients (80% with COPD) who were referred to a PR service, 230 entered PR. Eighty-four of the 172 patients who completed PR chose the maintenance program, and 46 were attending at follow-up.
6.4 Ethical Considerations
6.4.1 Efficiency versus equity
Access to PR services in Canada is limited. Information from studies in the clinical review is consistent with the conclusions of earlier reviews4,5 that PR provides comparable benefit to all

PR for COPD: Clinical, Economic, and Budget Impact Analysis 47
age groups and for all degrees of disease severity. There seems to be no single basis for selecting particular groups of patients for PR.
6.4.2 Process or procedural issues
An issue in the provision of effective PR is the ability to achieve high levels of patient participation and compliance with rehabilitation processes. There is evidence to suggest that higher levels of patient supervision in PR programs are associated with better outcomes. The duration and extent of benefits from the use of PR will be associated with how well patients accept and comply with maintenance programs. The ACCP/AACPR guideline notes that shorter program duration can reduce the cost per patient served and spread limited resources. On the other hand, longer program duration may produce greater gains and improved maintenance of benefits.4 Increasing levels of contact with rehabilitation professionals will have resource implications, but failure to meet these implications will tend to lower the effectiveness of the intervention.
7 DISCUSSION
7.1 Summary of Results
When compared with the usual care of patients with stable COPD, PR provides benefits in the short term (up to three months) as indicated by improvement in exercise capacity, HRQL, and mental health.28-39 The mean values of changes in exercise capacity, however, were less than the MCID in most studies. These findings are consistent with those of earlier reviews showing improvements in HRQL.4,5 Studies on the effects of PR in patients who had been admitted to hospital because of acute exacerbations had contrary findings,24,26,27 so that the effects on exercise capacity and health status are uncertain for such groups. The differences in the definition of what is “ usual care” has been suggested as a reason for the discrepancy between the two studies.26 Studies that considered longer-term outcomes of PR made a less certain picture. The disappearance of benefits over time occurred in a fair-quality non-randomized study.35 One high- quality study44 and one fair-quality study38 found that improvements in exercise capacity were maintained over 12 and six months with mean values below the MCIDs. Five high- or good- quality studies found improvements at six months or more,34,43,45-47 with some benefits being sustained for 18 and 20 months, respectively, in two studies.43,45 Two observational studies found that improvements to 6MWD and HRQL were maintained to two and three years.56,57 Two studies that compared maintenance programs and usual care after the end of PR found that home-based exercise training was effective in maintenance, with benefits being maintained at six months50 and 12 months.51 Two other studies52,53 found limited benefits from maintenance. Ten studies26,33,58-65 that reported mental health outcomes found improvements in anxiety and depression, with scores above the MCIDs in eight studies.
PR for COPD: Clinical, Economic, and Budget Impact Analysis 48
There were indications of reduction in hospital admissions and length of stay after PR. In three of the four better-quality studies, the differences in comparison groups were not statistically significant.24,26,45 It was unclear from reviewed studies whether the inclusion of tiotropium in PR programs offered statistically significant additional benefit.66,71,73 A high-quality study found statistically significant benefits in patients using a mixture of helium and oxygen during PR.76 Two studies comparing PR and LVRS plus PR found that surgery gave greater improvement than PR alone.78,79 The results from several studies suggest that patients with COPD can benefit from the use of PR regardless of patient age,81-83 disease severity,84-86,88 and sex.85,94 More higher-quality studies would be desirable. Home-based PR programs provided similar benefits to patients compared with hospital outpatient PR programs.67,95 The appropriate duration and content of PR programs are unclear based on the studies. Studies on approaches to exercise training indicated that more supervision is beneficial.99 Individually prescribed exercise training or high-intensity training does not seem to be of added benefit.77,100,102 Little information was available on the effectiveness of components of PR programs. A comparative summary of eight of nine studies in the economic review where PR was offered on an outpatient basis7,122,124-129 showed that the mean cost per participant was approximately $1,100. It was not possible to provide a numerical cost-effectiveness. The outcomes were better in the intervention groups, but the outcome measures were not uniform. The primary economic assessment was a cost-effectiveness analysis that compared the costs and health outcomes between usual care (pharmacotherapy) and usual care plus PR in three sessions per week for six weeks. When the duration of efficacy of PR was 18 months, the cost per person of PR was $27 more than usual care (incorporating maintenance costs and utilization from exacerbations) and generated 0.042 additional QALYs. The incremental cost-effectiveness ratio of PR compared with usual care was 27,924 per additional QALY gained. This result is within the acceptability threshold of $50,000, and the results hold up for a variety of changes, except if the cost of PR is high (more than $2,300 per person). The budget impact analysis reflected current levels of demand and PR services in Canada. It was assumed that there is a backlog of need and that it would take ten years to eliminate it. Further expansion of services was unrealistic because of the large additional resource requirements and competing needs in the public health care systems. If it is assumed that only the moderate and severe cases need PR, 1,505 additional persons would be served annually in Canada, for an added cost of $1.8 million. If 25% of persons with COPD needed PR, this would rise to $33.9 million annually for 100% uptake or $19 million if 67% of those in need had used the services. If all persons with COPD needed PR, the additional annual cost would be $168 million.
PR for COPD: Clinical, Economic, and Budget Impact Analysis 49
7.2 Strengths and Weaknesses of This Assessment
The assessment included a clinical review that considered short-term and longer-term outcomes of PR, efficacy of other treatments and components of PR, and the context and operation of PR programs. The quality of publications was assessed. A cost-effectiveness analysis, which was used to compare the costs and health outcomes of usual care and usual care plus PR, drew mainly from Canadian and US data. The budget impact analysis included several models based on different scenarios for demand, and took account of the availability of PR programs in Canada. Weaknesses in the assessment were mainly linked to limitations in the primary data. The studies that were included in the clinical review related to PR programs that varied in components, duration, and patient populations. The selected studies used several methods to assess the outcomes of PR, which contributed to heterogeneity. Consequently, the derivation of summary statistics was considered to be unrealistic, and a series of qualitative reviews were prepared. Many of the papers presented findings on outcomes with reference to P values and did not give confidence intervals. In the economic review, the variation in PR design and measured outcomes between studies meant that an integrative analysis could not be developed, because there was no standard cost measure. Because there was interest in the more recent literature on PR, the literature search was restricted to publications from 1998 onward, and there was no analysis of earlier material. Points from the earlier literature were considered through the use of systematic reviews. In the clinical review, with one exception, data from non-English language papers were limited to what was available in the abstracts and some of the tables. The appraisal of quality was not possible for these publications. It is considered likely, however, that more information from these studies would have made little difference to the overall findings of this review. Of the 34 papers in the clinical review that were used to assess exercise capacity, HRQL and mental health outcomes, 26 were RCTs, with a mean Jadad score of 2.4. This reflects the absence of double blinding in most of the RCTs. Of the 34 papers, 65% were of high or good quality and 21% of fair quality. Of the 47 papers included in other parts of the clinical review, 37% were of high or good quality and 36% of fair quality. None of the 14 studies that addressed patient characteristics were RCTs. One of the nine studies in the economic review met all nine of the quality criteria, and two others met seven. The studies in the economic review varied in interventions, patients treated, and methods of analysis. There was no “modal” value of costs, and outcome data had to be taken from the clinical review. One study from the clinical review presented adequate results for the number of exacerbations, which was a driving variable. Nevertheless, the results were sensitive to a variety of values of the relative risk of PR on exacerbations. If the true incidence of COPD is higher than that used in the economic analysis, and regions increased surveillance and persons diagnosed, this would increase the demand and need for PR. Some of those who received PR would die during the period analyzed, although this would not affect the order of magnitude of the results. It was assumed that the additional resources appeared in the first year of the program, but it would take several years to increase the capacity, so costs would be lower in the earlier years.
PR for COPD: Clinical, Economic, and Budget Impact Analysis 50
7.3 Generalizability of Findings
The findings of the studies comparing PR with usual care that reported short-term outcomes are consistent with those from earlier work4,5 and can be considered to be generalizable. The findings that outpatient and home-based PR programs can give similar benefits to patients with COPD are probably also generalizable. The generalizability of studies reporting longer-term outcomes is less clear. Sustained benefits from PR have been achieved in some settings but not in others, and more work seems to be needed to confirm factors that contribute to longer-term success. The findings from studies on age profile and disease severity are consistent with previous experience, but generalizability is unclear because of limited study quality. The primary economic evaluation made several assumptions, but the overall findings can be considered to be generalizable. The cost-effectiveness was within the acceptable range and did not vary with key operational variables. Several assumptions are made in the budget impact analysis, but overall findings are generalizable to Canadian jurisdictions.
7.4 Knowledge Gaps
The AACP/AACPR guideline4 notes that more research is needed to clarify the relative impact of the factors that can affect the duration of benefits from short-term PR. These include the maintenance program structure, content, and location; exacerbations of respiratory disease; and complications of other medical comorbidities. More work is needed to evaluate the optimal methods to incorporate short-term rehabilitation strategies into long-term disease management programs for patients with chronic lung disease. Some studies in the clinical review suggest that successful outcomes after PR may be associated with the use of longer programs and maintenance. Longer duration PR programs would provide more stimulus. Therefore, patients would see greater health benefits. Extended programs, however, would be more costly ― with implications for budget impact ― and represent a greater time commitment by patients. There seems to be a need for better information on patient characteristics and the optimum structure and operation of PR programs. The approaches vary between programs. Limited information was obtained in the clinical review on the efficacy of individual components of PR. The same can be said for the economic review. Given the lack of longer-term data on outcomes, we need information on the decay of benefits and the possible need for boosters. While the short- term benefits of PR are established, the extent of these benefits may be unclear because many studies excluded patients with comorbidities and those who had recent exacerbations. There was little information from the clinical review on the efficacy and effectiveness of adjunct therapies for PR. The evidence of benefit from adjunct therapies would need to be compelling for them to be adopted in routine use. While such therapies might maximize health outcomes for patients who received PR, they would present additional costs to those of standard PR programs. As basic PR programs typically provide clinically significant improvements in HRQL and exercise capacity, it is likely a better use of resources to increase PR capacity across Canada, instead of working to maximize gains in the small patient group who are already receiving PR.

PR for COPD: Clinical, Economic, and Budget Impact Analysis 51
8 CONCLUSIONS
This assessment confirms findings from earlier work that PR is effective in improving short-term exercise capacity, HRQL, and mental health outcomes for patients with stable COPD. The use of PR may also be associated with reductions in hospitalization, but better-quality studies are needed. There is evidence that, in some settings, the benefits of PR can be sustained in the longer term, but at other centres the benefits decline over six to 18 months after the completion of rehabilitation. More work is needed to confirm the factors that contribute to the successful long- term management of COPD after PR. There is limited information on the effectiveness of elements of PR programs. Issues that relate to patient characteristics and the operation of PR and maintenance programs need to be considered by those who establish and provide these services. If the duration of effectiveness of PR is 18 months, as in some of the studies from the clinical literature, the ICER of usual care plus PR compared with usual care is $27,924 per additional QALY gained. This is within the range of acceptability according to current thresholds, and the results are not highly sensitive to variations in the values of the model variables. The estimates of additional costs of PR services in Canada ranged from $1.8 million to $168 million annually. In the most likely scenario, corresponding to 25% of persons with COPD needing PR and a 67% uptake, another $19 million would be needed annually.
PR for COPD: Clinical, Economic, and Budget Impact Analysis 52
9 REFERENCES 1. Public Health Agency of Canada. Life and breath: respiratory disease in Canada. Ottawa: The Agency;
2009. Available: http://www.phac-aspc.gc.ca/publicat/2007/lbrdc-vsmrc/intro-eng.php#13 (accessed 2009 Sep 14).
2. O'Donnell DE, Aaron S, Bourbeau J, Hernandez P, Marciniuk DD, Balter M, et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease - 2007 update. Can Respir J 2007;14(Suppl B):5B-32B.
3. Nici L, Donner C, Wouters E, ZuWallack R, Ambrosino N, Bourbeau J, et al. American Thoracic Society/European Respiratory Society statement on pulmonary rehabilitation. Am J Respir Crit Care Med 2006;173(12):1390-413. Available: http://ajrccm.atsjournals.org/cgi/reprint/173/12/1390?maxtoshow=&HITS=10&hits=10&RESULTFORMAT=&fulltext=society&searchid=1&FIRSTINDEX=0&volume=173&issue=12&resourcetype=HWCIT (accessed 2009 Feb 27).
4. Ries AL, Bauldoff GS, Carlin BW, Casaburi R, Emery CF, Mahler DA, et al. Pulmonary rehabilitation: joint ACCP/AACVPR evidence-based clinical practice guidelines. Chest 2007;131(5 Suppl):4S-42S. Available: http://www.chestjournal.org/cgi/reprint/131/5_suppl/4S (accessed 2009 Sep 30).
5. Lacasse Y, Goldstein R, Lasserson TJ, Martin S. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2006;(4):CD003793.
6. Brooks D, Hill K, Goldstein R. Pulmonary rehabilitation in 2006: what works, what doesn't and what is presently being done in Canada. Can Respir J 2007;14(Suppl A):9A-10A.
7. Golmohammadi K, Jacobs P, Sin DD. Economic evaluation of a community-based pulmonary rehabilitation program for chronic obstructive pulmonary disease. Lung 2004;182(3):187-96.
8. Australian Lung Foundation, Australian Physiotherapy Association. Pulmonary rehabilitation toolkit. Lutwyche (AU): The Foundation; 2006. Available: http://www.pulmonaryrehab.com.au/welcome.asp (accessed 2009 Sep 18).
9. Hailey D, Ohinmaa A, Roine R. Study quality and evidence of benefit in recent assessments of telemedicine. J Telemed Telecare 2004;10(6):318-24.
10. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 1996;17(1):1-12.
11. Redelmeier DA, Bayoumi AM, Goldstein RS, Guyatt GH. Interpreting small differences in functional status: the Six Minute Walk test in chronic lung disease patients. Am J Respir Crit Care Med 1997;155(4):1278-82.
12. Singh SJ, Jones PW, Evans R, Morgan MD. Minimum clinically important improvement for the incremental shuttle walking test. Thorax 2008;63(9):775-7.
13. Brouillard C, Pepin V, Milot J, Lacasse Y, Maltais F. Endurance shuttle walking test: responsiveness to salmeterol in COPD. Eur Respir J 2008;31(3):579-84. Available: http://erj.ersjournals.com/cgi/reprint/31/3/579 (accessed 2009 Nov 5).
14. Sutherland ER, Make BJ. Maximum exercise as an outcome in COPD: minimal clinically important difference. COPD 2005;2(1):137-41.
15. Laviolette L, Bourbeau J, Bernard S, Lacasse Y, Pepin V, Breton MJ, et al. Assessing the impact of pulmonary rehabilitation on functional status in COPD. Thorax 2008;63(2):115-21.
16. Chauvin A, Rupley L, Meyers K, Johnson K, Eason J. Outcomes in Cardiopulmonary Physical Therapy: Chronic Respiratory Disease Questionnaire. Cardiopulm Phys Ther J 2008;19(2):61-7. Available: http://www.cpptjournal.org/cppt/members/fulltext/2008/june/june-article6.pdf (accessed 2009 Nov 5).
17. Jones PW. Interpreting thresholds for a clinically significant change in health status in asthma and COPD. Eur Respir J 2002;19(3):398-404. Available: http://erj.ersjournals.com/cgi/reprint/19/3/398 (accessed 2009 Nov 5).

PR for COPD: Clinical, Economic, and Budget Impact Analysis 53
18. Hays RD, Morales LS. The RAND-36 measure of health-related quality of life. Ann Med 2001;33(5):350-7.
19. Kaplan RM. The minimally clinically important difference in generic utility-based measures. COPD 2005;2(1):91-7.
20. Hiroe T, Kojima M, Yamamoto I, Nojima S, Kinoshita Y, Hashimoto N, et al. Gradations of clinical severity and sensitivity to change assessed with the Beck Depression Inventory-II in Japanese patients with depression. Psychiatry Res 2005;135(3):229-35.
21. Puhan MA, Frey M, Buchi S, Schunemann HJ. The minimal important difference of the hospital anxiety and depression scale in patients with chronic obstructive pulmonary disease. Health Qual Life Outcomes 2008;6:46. Available: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2459149/ (accessed 2010 Mar 3).
22. Cohen J. A power primer. Psychol Bull 1992;112(1):155-9.
23. Coultas D, McKinley J. Update on pulmonary rehabilitation for COPD. Clin Pulm Med 2009;16(4):183-8.
24. Man WD, Polkey MI, Donaldson N, Gray BJ, Moxham J. Community pulmonary rehabilitation after hospitalisation for acute exacerbations of chronic obstructive pulmonary disease: randomised controlled study. BMJ 2004;329(7476):1209. Available: http://www.pubmedcentral.nih.gov/picrender.fcgi?artid=529363&blobtype=pdf (accessed 2009 Feb 13).
25. Puhan M, Scharplatz M, Troosters T, Walters EH, Steurer J. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2009;(1):1-32.
26. Eaton T, Young P, Fergusson W, Moodie L, Zeng I, O'Kane F, et al. Does early pulmonary rehabilitation reduce acute health-care utilization in COPD patients admitted with an exacerbation? A randomized controlled study. Respirology 2009;14(2):230-8.
27. Clini EM, Crisafulli E, Costi S, Rossi G, Lorenzi C, Fabbri LM, et al. Effects of early inpatient rehabilitation after acute exacerbation of COPD. Respir Med 2009;103(10):1526-31.
28. Karapolat H, Atasever A, Atamaz F, Kirazli Y, Elmas F, Erdinç E. Do the benefits gained using a short-term pulmonary rehabilitation program remain in COPD patients after participation? Lung 2007;185(4):221-5.
29. Barakat S, Michele G, George P, Nicole V, Guy A. Outpatient pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis 2008;3(1):155-62. Available: http://www.dovepress.com/outpatient-pulmonary-rehabilitation-in-patients-with-chronic-obstructi-peer-reviewed-article (accessed 2009 Sep 30).
30. Theander K, Jakobsson P, Jorgensen N, Unosson M. Effects of pulmonary rehabilitation on fatigue, functional status and health perceptions in patients with chronic obstructive pulmonary disease: a randomized controlled trial. Clin Rehabil 2009;23(2):125-36.
31. Boxall AM, Barclay L, Sayers A, Caplan GA. Managing chronic obstructive pulmonary disease in the community: a randomized controlled trial of home-based pulmonary rehabilitation for elderly housebound patients. J Cardiopulm Rehabil 2005;25(6):378-85.
32. Singh V, Khandelwal DC, Khandelwal R, Abusaria S. Pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. Indian J Chest Dis Allied Sci 2003;45(1):13-7.
33. Elçi A, Börekçi S, Ovayolu N, Elbek O. The efficacy and applicability of a pulmonary rehabilitation programme for patients with COPD in a secondary-care community hospital. Respirology 2008;13(5):703-7.
34. Griffiths TL, Burr ML, Campbell IA, Lewis-Jenkins V, Mullins J, Shiels K, et al. Results at 1 year of outpatient multidisciplinary pulmonary rehabilitation: a randomised controlled trial. Lancet 2000;355(9201):362-8.
35. Na JO, Kim DS, Yoon SH, Jegal YJ, Kim WS, Kim ES, et al. A simple and easy home-based pulmonary rehabilitation programme for patients with chronic lung diseases. Monaldi Arch Chest Dis 2005;63(1):30-6.
36. Oh EG. The effects of home-based pulmonary rehabilitation in patients with chronic lung disease. Int J Nurs Stud 2003;40(8):873-9.

PR for COPD: Clinical, Economic, and Budget Impact Analysis 54
37. Skumlien S, Skogedal EA, Bjørtuft O, Ryg MS. Four weeks' intensive rehabilitation generates significant health effects in COPD patients. Chron Respir Dis 2007;4(1):5-13.
38. Regiane Resqueti V, Gorostiza A, Galdiz JB, López de Santa María E, Clara PC, Güell Rous R. Benefits of a home-based pulmonary rehabilitation program for patients with severe chronic obstructive pulmonary disease. Arch Bronconeumol 2007;43(11):599-604. Available: http://external.doyma.es/pdf/260/260v43n11a13112222pdf001.pdf (accessed 2009 Apr 17).
39. Riario-Sforza GG, Incorvaia C, Paterniti F, Pessina L, Caligiuri R, Pravettoni C, et al. Effects of pulmonary rehabilitation on exercise capacity in patients with COPD: a number needed to treat study. Int J Chron Obstruct Pulmon Dis 2009;4(2):315-9.
40. Jang HJ, Jung YK. The effects of self-efficacy promoting pulmonary rehabilitation program in out-patients with chronic obstructive pulmonary disease [in Korean]. Tuberc Respir Dis 2006;61(6):533-46.
41. Ciric Z, Stankovic I, Rancic M, Pejcic T, Radovic M. Pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. Vojnosanit Pregl 2008;65(7):533-8.
42. Ringbaek TJ, Brondum E, Hemmingsen L, Lybeck K, Nielsen D, Andersen C, et al. Rehabilitering af patienter med kronisk obstruktiv lungesygdom: er troening to gange ugentlig tilstroekkeligt? [Rehabilitation of patients with chronic obstructive lung disease. Are two exercise sessions per week sufficient?] [in Danish]. Ugeskr Laeger 2000;162(4):498-501. Available: http://www.ugeskriftet.dk/lf/UFL/ufl99_00/1999_2000/ufl2004/v_p/org5.htm (accessed 2009 Feb 12).
43. van Wetering CR, Hoogendoorn M, Mol SM, Rutten-van Möken MP, Schols AM. Short- and long-term efficacy of a community-based COPD management program in less advanced COPD: a randomized controlled trial. Thorax 2009.
44. Engström CP, Persson LO, Larsson S, Sullivan M. Long-term effects of a pulmonary rehabilitation programme in outpatients with chronic obstructive pulmonary disease: a randomized controlled study. Scand J Rehabil Med 1999;31(4):207-13.
45. Güell R, Casan P, Belda J, Sangenis M, Morante F, Guyatt GH, et al. Long-term effects of outpatient rehabilitation of COPD: a randomized trial. Chest 2000;117(4):976-83. Available: http://www.chestjournal.org/content/117/4/976.full.pdf+html (accessed 2009 Feb 13).
46. Finnerty JP, Keeping I, Bullough I, Jones J. The effectiveness of outpatient pulmonary rehabilitation in chronic lung disease: a randomized controlled trial. Chest 2001;119(6):1705-10. Available: http://chestjournal.chestpubs.org/content/119/6/1705.full.pdf+html (accessed 2009 Nov 5).
47. Fernandez AM, Pascual J, Ferrando C, Arnal A, Vergara I, Sevila V. Home-based pulmonary rehabilitation in very severe COPD: Is it safe and useful? J Cardiopulm Rehabil Prev 2009;29(5):325-31.
48. Cote CG, Celli BR. Pulmonary rehabilitation and the BODE index in COPD. Eur Respir J 2005;26(4):630-6. Available: http://erj.ersjournals.com/cgi/reprint/26/4/630 (accessed 2009 Sep 30).
49. Göhl O, Linz H, Schönleben T, Otte B, Weineck J, Worth H. Effekte eines multimodularen ambulanten trainingsprogramms für patienten mit COPD = Benefits of a multimodular outpatient training program for patients with COPD. Pneumologie 2006;60(9):529-36.
50. du Moulin M, Taube K, Wegscheider K, Behnke M, van den Bussche H. Home-based exercise training as maintenance after outpatient pulmonary rehabilitation [Epub ahead of print]. Respiration 2008;77:139-45.
51. Moullec G, Ninot G, Varray A, Desplan J, Hayot M, Prefaut C. An innovative maintenance follow-up program after a first inpatient pulmonary rehabilitation. Respir Med 2008;102(4):556-66.
52. Steele BG, Belza B, Cain KC, Coppersmith J, Lakshminarayan S, Howard J, et al. A randomized clinical trial of an activity and exercise adherence intervention in chronic pulmonary disease. Arch Phys Med Rehabil 2008;89(3):404-12.
53. Ries AL, Kaplan RM, Myers R, Prewitt LM. Maintenance after pulmonary rehabilitation in chronic lung disease: a randomized trial. Am J Respir Crit Care Med 2003;167(6):880-8. Available: http://ajrccm.atsjournals.org/cgi/content/full/167/6/880 (accessed 2010 Jan 13).
PR for COPD: Clinical, Economic, and Budget Impact Analysis 55
54. Romagnoli M, Dell'Orso D, Lorenzi C, Crisafulli E, Costi S, Lugli D, et al. Repeated pulmonary rehabilitation in severe and disabled COPD patients. Respiration 2006;73(6):769-76.
55. Verrill D, Barton C, Beasley W, Lippard WM. The effects of short-term and long-term pulmonary rehabilitation on functional capacity, perceived dyspnea, and quality of life. Chest 2005;128(2):673-83. Available: http://www.chestjournal.org/content/128/2/673.full.pdf+html (accessed 2009 Feb 13).
56. Lomundal BK, Steinsbekk A. Observational studies of a one year self-management program and a two year pulmonary rehabilitation program in patients with COPD. Int J Chron Obstruct Pulmon Dis 2007;2(4):617-24.
57. Steinsbekk A, Lomundal B. Three-year follow-up after a two-year comprehensive pulmonary rehabilitation program. Chron Respir Dis 2009;6(1):5-11.
58. Paz-Diaz H, Montes de Oca M, Lopez JM, Celli BR. Pulmonary rehabilitation improves depression, anxiety, dyspnea and health status in patients with COPD. Am J Phys Med Rehabil 2007;86(1):30-6.
59. Kayahan B, Karapolat H, Atyntoprak E, Atasever A, Öztürk O. Psychological outcomes of an outpatient pulmonary rehabilitation program in patients with chronic obstructive pulmonary disease. Respir Med 2006;100(6):1050-7.
60. Kozora E, Tran ZV, Make B. Neurobehavioral improvement after brief rehabilitation in patients with chronic obstructive pulmonary disease. J Cardiopulm Rehabil 2002;22(6):426-30.
61. Güell R, Resqueti V, Sangenis M, Morante F, Martorell B, Casan P, et al. Impact of pulmonary rehabilitation on psychosocial morbidity in with severe COPD. Chest 2006;129(4):899-904. Available: http://www.chestjournal.org/content/129/4/899.full.pdf+html (accessed 2009 Feb 13).
62. Haugen TS, Stavem K. Rehabilitation in a warm versus a colder climate in chronic obstructive pulmonary disease: a randomized study. J Cardiopulm Rehabil Prev 2007;27(1):50-6.
63. O'Neill B, McKevitt A, Rafferty S, Bradley JM, Johnston D, Bradbury I, et al. A comparison of twice- versus once-weekly supervision during pulmonary rehabilitation in chronic obstructive pulmonary disease. Arch Phys Med Rehabil 2007;88(2):167-72.
64. Lolak S, Connors GL, Sheridan MJ, Wise TN. Effects of progressive muscle relaxation training on anxiety and depression in patients enrolled in an outpatient pulmonary rehabilitation program. Psychother Psychosom 2008;77(2):119-25.
65. De Godoy DV, De Godoy RF, Junior BB, Vaccari PF, Michelli M, Teixeira PJZ, et al. The effect of psychotherapy provided as part of a pulmonary rehabilitation program for the treatment of patients with chronic obstructive pulmonary disease. Jornal Brasileiro de pneumologia 2005;31(6):499-505.
66. Ambrosino N, Foglio K, Balzano G, Paggiaro PL, Lessi P, Kesten S. Tiotropium and exercise training in COPD patients: effects on dyspnea and exercise tolerance. Int J Chron Obstruct Pulmon Dis 2008;3(4):771-80. Available: http://www.pubmedcentral.nih.gov/picrender.fcgi?artid=2650608&blobtype=pdf (accessed 2009 Apr 21).
67. Maltais F, Bourbeau J, Shapiro S, Lacasse Y, Perrault H, Baltzan M, et al. Effects of home-based pulmonary rehabilitation in patients with chronic obstructive pulmonary disease: a randomized trial. Ann Intern Med 2008;149(12):869-78.
68. Raskin J, Spiegler P, McCusker C, ZuWallack R, Bernstein M, Busby J, et al. The effect of pulmonary rehabilitation on healthcare utilization in chronic obstructive pulmonary disease: the northeast pulmonary rehabilitation consortium. J Cardiopulm Rehabil 2006;26(4):231-6.
69. California Pulmonary Rehabilitation Collaborative Group. Effects of pulmonary rehabilitation on dyspnea, quality of life, and healthcare costs in California. J Cardiopulm Rehabil 2004;24(1):52-62 (accessed 2009 Apr 17).
70. Wittmann M, Spohn S, Schultz K, Pfeifer M, Petro W. COPD-schulung im rahmen der stationaren rehabilitation verbessert lebensqualitat und morbiditat [Patient education in COPD during patient rehabilitation improves quality of life and morbidity] [in German]. Pneumologie 2007;61(10):636-43.

PR for COPD: Clinical, Economic, and Budget Impact Analysis 56
71. Casaburi R, Kukafka D, Cooper CB, Witek TJ, Kesten S. Improvement in exercise tolerance with the combination of tiotropium and pulmonary rehabilitation in patients with COPD. Chest 2005;127(3):809-17. Available: http://www.chestjournal.org/content/127/3/809.full.pdf+html (accessed 2009 Feb 13).
72. Kesten S, Casaburi R, Kukafka D, Cooper CB. Improvement in self-reported exercise participation with the combination of tiotropium and rehabilitative exercise training in COPD patients. Int J Chron Obstruct Pulmon Dis 2008;3(1):127-36.
73. Lindsay M, Lee A, Chan K, Poon P, Han LK, Wong WCW, et al. Does pulmonary rehabilitation give additional benefit over tiotropium therapy in primary care management of chronic obstructive pulmonary disease? Randomized controlled clinical trial in Hong Kong Chinese. J Clin Pharm Ther 2005;30(6):567-73.
74. Duiverman ML, Wempe JB, Bladder G, Jansen DF, Kerstjens HA, Zijlstra JG, et al. Nocturnal non-invasive ventilation in addition to rehabilitation in hypercapnic patients with COPD. Thorax 2008;63(12):1052-7.
75. Kohnlein T, Schonheit-Kenn U, Winterkamp S, Welte T, Kenn K. Noninvasive ventilation in pulmonary rehabilitation of COPD patients. Respir Med 2009;103(9):1329-36.
76. Eves ND, Sandmeyer LC, Wong EY, Jones LW, MacDonald GF, Ford GT, et al. Helium-hyperoxia: a novel intervention to improve the benefits of pulmonary rehabilitation for patients with COPD. Chest 2008. Available: http://www.chestjournal.org/content/135/3/609.full.pdf+html (accessed 2009 Apr 17).
77. Puhan MA, Schunemann HJ, Frey M, Bachmann LM. Value of supplemental interventions to enhance the effectiveness of physical exercise during respiratory rehabilitation in COPD patients. A systematic review. Respir Res 2004;5:25. Available: http://www.pubmedcentral.nih.gov/picrender.fcgi?artid=539299&blobtype=pdf (accessed 2009 Feb 12).
78. Pompeo E, Marino M, Nofroni I, Matteucci G, Mineo TC, Iannettoni MD, et al. Reduction pneumoplasty versus respiratory rehabilitation in severe emphysema: a randomized study. Ann Thorac Surg 2000;70(3):948-54. Available: http://ats.ctsnetjournals.org/cgi/reprint/70/3/948 (accessed 2009 Sep 30).
79. Mercer K, Follette D, Breslin E, Allen R, Hoso A, Volz B, et al. Comparison of functional state between bilateral lung volume reduction surgery and pulmonary rehabilitation: a six-month followup study. Int J Surg Investig 1999;1(2):139-47.
80. Vivodtzev I, Pepin JL, Vottero G, Mayer V, Porsin B, Levy P, et al. Improvement in quadriceps strength and dyspnea in daily tasks after 1 month of electrical stimulation in severely deconditioned and malnourished COPD. Chest 2006;129(6):1540-8. Available: http://chestjournal.chestpubs.org/content/129/6/1540.long (accessed 2009 Dec 15).
81. Baltzan MA, Kamel H, Alter A, Rotaple M, Wolkove N. Pulmonary rehabilitation improves functional capacity in patients 80 years of age or older. Can Respir J 2004;11(6):407-13.
82. Fabre C, Grosbois JM, Bart F, Borel B, Mucci P. At identical isowork rates, ageing influences cardiorespiratory adaptations in COPD out-patients. Respir Med 2007;101(11):2305-11.
83. Ando M, Mori A, Esaki H, Shiraki T, Uemura H, Okazawa M, et al. The effects of pulmonary rehabilitation in elderly patients [in Japanese]. Nihon Kokyuki Gakkai Zasshi 2003;41(2):81-8.
84. Riario-Sforza GG, Incorvaia C, Paterniti F, Dugnani N, Fumagalli M. Different outcomes of pulmonary rehabilitation in patients with COPD with or without exacerbations. Monaldi Arch Chest Dis 2005;63(3):129-32.
85. Lizak MK, Singh S, Lubina S, Zembala M. Female and male chronic obstructive pulmonary disease patients with severe dyspnea do not profit less from pulmonary rehabilitation. Pol Arch Med Wewn 2008;118(7-8):413-8.
86. Evans RA, Singh SJ, Collier R, Williams JE, Morgan MD. Pulmonary rehabilitation is successful for COPD irrespective of MRC dyspnoea grade. Respir Med 2009;103(7):1070-5.
87. Garrod R, Marshall J, Barley E, Jones PW. Predictors of success and failure in pulmonary rehabilitation. Eur Respir J 2006;27(4):788-94.

PR for COPD: Clinical, Economic, and Budget Impact Analysis 57
88. Carone M, Patessio A, Ambrosino N, Baiardi P, Balbi B, Balzano G, et al. Efficacy of pulmonary rehabilitation in chronic respiratory failure (CRF) due to chronic obstructive pulmonary disease (COPD): the Maugeri Study. Respir Med 2007;101(12):2447-53.
89. Plankeel JF, McMullen B, MacIntyre NR. Exercise outcomes after pulmonary rehabilitation depend on the initial mechanism of exercise limitation among non-oxygen-dependent COPD patients. Chest 2005;127(1):110-6.
90. Di Meo F, Pedone C, Lubich S, Pizzoli C, Traballesi M, Incalzi RA. Age does not hamper the response to pulmonary rehabilitation of COPD patients. Age Ageing 2008;37(5):530-5.
91. Fan VS, Giardino ND, Blough DK, Kaplan RM, Ramsey SD, Fishman AP, et al. Costs of pulmonary rehabilitation and predictors of adherence in the National Emphysema Treatment Trial. Int J Chron Obstruct Pulmon Dis 2008;5(2):105-16.
92. Heppner PS, Morgan C, Kaplan RM, Ries AL. Regular walking and long-term maintenance of outcomes after pulmonary rehabilitation. J Cardiopulm Rehabil 2006;26(1):44-53.
93. Ries AL, Make BJ, Lee SM, Krasna MJ, Bartels M, Crouch R, et al. The effects of pulmonary rehabilitation in the National Emphysema Treatment Trial. Chest 2005;128(6):3799-809. Available: http://www.chestjournal.org/content/128/6/3799.full.pdf+html (accessed 2009 Sep 30).
94. Haave E, Skumlien S, Hyland ME. Gender considerations in pulmonary rehabilitation. J Mol Signal 2008;28(3):215-9.
95. Güell MR, de Lucas P, Gáldiz JB, Montemayor T, González-Moro JMR, Gorostiza A, et al. Home vs. hospital-based pulmonary rehabilitation for patients with chronic obstructive pulmonary disease: a Spanish multicenter trial. Arch Bronconeumol 2008;44(10):512-8.
96. Sewell L, Singh SJ, Williams JEA, Collier R, Morgan MDL. How long should outpatient pulmonary rehabilitation be? A randomised controlled trial of 4 weeks versus 7 weeks. Thorax 2006;61(9):767-71.
97. Green RH, Singh SJ, Williams J, Morgan MD. A randomised controlled trial of four weeks versus seven weeks of pulmonary rehabilitation in chronic obstructive pulmonary disease. Thorax 2001;56(2):143-5. Available: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1746003 (accessed 2009 Jan 13).
98. Rossi G, Florini F, Romagnoli M, Bellantone T, Lucic S, Lugli D, et al. Length and clinical effectiveness of pulmonary rehabilitation in outpatients with chronic airway obstruction. Chest 2005;127(1):105-9. Available: http://www.chestjournal.org/content/127/1/105.full.pdf+html (accessed 2009 Feb 13).
99. Carrieri-Kohlman V, Nguyen HQ, Donesky-Cuenco D, Demir-Deviren S, Neuhaus J, Stulbarg MS. Impact of brief or extended exercise training on the benefit of a dyspnea self-management program in COPD. J Cardiopulm Rehabil 2005;25(5):275-84.
100. Sewell L, Singh SJ, Williams JEA, Collier R, Morgan MDL. Can individualized rehabilitation improve functional independence in elderly patients with COPD. Chest 2005;128(3):1194-200. Available: http://www.chestjournal.org/content/128/3/1194.full.pdf+html (accessed 2009 Feb 13).
101. Puhan MA, Büsching G, Schünemann HJ, vanOort E, Zaugg C, Frey M. Interval versus continuous high-intensity exercise in chronic obstructive pulmonary disease: a randomized trial. Ann Intern Med 2006;145(11):816-25. Available: http://www.annals.org/cgi/reprint/145/11/816.pdf (accessed 2009 Feb 26).
102. Mador MJ, Krawza M, Alhajhusian A, Khan AI, Shaffer M, Kufel TJ. Interval training versus continuous training in patients with chronic obstructive pulmonary disease. J Cardiopulm Rehabil Prev 2009;29(2):126-32.
103. Varga J, Porszasz J, Boda K, Casaburi R, Somfay A. Supervised high intensity continuous and interval training vs. self-paced training in COPD. Respir Med 2007;101(11):2297-304.
104. Hsieh M-J, Lan C-C, Chen N-H, Huang C-C, Wu Y-K, Cho H-Y, et al. Effects of high-intensity exercise training in a pulmonary rehabilitation programme for patients with chronic obstructive pulmonary disease. Respirology 2007;12(3):381-8.

PR for COPD: Clinical, Economic, and Budget Impact Analysis 58
105. Magadle R, McConnell AK, Beckerman M, Weiner P. Inspiratory muscle training in pulmonary rehabilitation program in COPD patients. Respir Med 2007;101(7):1500-5.
106. De Blok BM, de Greef MH, ten Hacken NH, Sprenger SR, Postema K, Wempe JB. The effects of a lifestyle physical activity counseling program with feedback of a pedometer during pulmonary rehabilitation in patients with COPD: a pilot study. Patient Educ Couns 2006;61(1):48-55.
107. Norweg AM, Whiteson J, Malgady R, Mola A, Rey M. The effectiveness of different combinations of pulmonary rehabilitation program components: a randomized controlled trial. Chest 2005;128(2):663-72. Available: http://www.chestjournal.org/content/128/2/663.full.pdf+html (accessed 2009 Feb 13).
108. Scherer YK, Schmieder LE, Shimmel S. The effects of education alone and in combination with pulmonary rehabilitation on self-efficacy in patients with COPD. Rehabil Nurs 1998;23(2):71-7.
109. Coultas D, Frederick J, Barnett B, Singh G, Wludyka P. A randomized trial of two types of nurse-assisted home care for patients with COPD. Chest 2005;128(4):2017-24. Available: http://www.chestjournal.org/content/128/4/2017.full.pdf+html (accessed 2009 Feb 13).
110. Brug J, Schols A, Mesters I. Dietary change, nutrition education and chronic obstructive pulmonary disease. Patient Educ Couns 2004;52(3):249-57.
111. Fuld JP, Kilduff LP, Neder JA, Pitsiladis Y, Lean MEJ, Ward SA, et al. Creatine supplementation during pulmonary rehabilitation in chronic obstructive pulmonary disease. Thorax 2005;60(7):531-7.
112. Deacon SJ, Vincent EE, Greenhaff PL, Fox J, Steiner MC, Singh SJ, et al. Randomized controlled trial of dietary creatine as an adjunct therapy to physical training in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2008;178(3):233-9.
113. Faager G, Soderlund K, Skold CM, Rundgren S, Tollback A, Jakobsson P. Creatine supplementation and physical training in patients with COPD: a double blind, placebo-controlled study. Int J Chron Obstruct Pulmon Dis 2006;1(4):445-53.
114. Slinde F, Grönberg AM, Engström CR, Rossander-Hulthén L, Larsson S. Individual dietary intervention in patients with COPD during multidisciplinary rehabilitation. Respir Med 2002;96(5):330-6.
115. Phillips WT, Benton MJ, Wagner CL, Riley C. The effect of single set resistance training on strength and functional fitness in pulmonary rehabilitation patients. J Cardiopulm Rehabil 2006;26(5):330-7.
116. Alexander JL, Phillips WT, Wagner CL. The effect of strength training on functional fitness in older patients with chronic lung disease enrolled in pulmonary rehabilitation. Rehabil Nurs 2008;33(3):91-7.
117. Costi S, Crisafulli E, Antoni FD, Beneventi C, Fabbri LM, Clini EM. Effects of unsupported upper extremity exercise training in patients with COPD: a randomized clinical trial. Chest 2009;136(2):387-95.
118. O'Donnell DE, Hernandez P, Kaplan A, Aaron S, Bourbeau J, Marciniuk D, et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease - 2008 update - highlights for primary care. Can Respir J 2008;15(Suppl A):1A-8A. Available: http://www.lung.ca/cts-sct/pdf/COPD-Highlights.pdf (accessed 2009 Apr 17).
119. Management of COPD Working Group. VA/DoD clinical practice guideline for the management of outpatient chronic obstructive pulmonary disease. Washington DC: Department of Veteran Affairs, Department of Defense; 2007. Available: http://www.healthquality.va.gov/copd/copd_20.pdf (accessed 2009 Sep 14).
120. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for diagnosis, management, and prevention of COPD. Gig Harbor (WA): Medical Communication Resources, Inc.; 2008. Available: http://www.goldcopd.com/Guidelineitem.asp?l1=2&l2=1&intId=2003 (accessed 2009 Sep 14).
121. Drummond MF, Jefferson TO, BMJ Economic Evaluation Working Party. Guidelines for authors and peer reviewers of economic submissions to the BMJ. BMJ 1996;313(7052):275-83. Available: http://www.bmj.com/cgi/content/full/313/7052/275 (accessed 2007 Feb 19).
122. White RJ, Rudkin ST, Ashley J, Stevens VA, Burrows S, Pounsford JC, et al. Outpatient pulmonary rehabilitation in severe chronic obstructive pulmonary disease. J R Coll Physicians Lond 1997;31(5):541-5.

PR for COPD: Clinical, Economic, and Budget Impact Analysis 59
123. Guyatt GH, Berman LB, Townsend M, Pugsley SO, Chambers LW. A measure of quality of life for clinical trials in chronic lung disease. Thorax 1987;42(10):773-8.
124. Scherer YK, Schieder LE. Pulmonary rehabilitation: is it cost effective? J N Y State Nurses Assoc 1998;29(3-4):16-20.
125. Troosters T, Gosselink R, Decramer M. Short- and long-term effects of outpatient rehabilitation in patients with chronic obstructive pulmonary disease: a randomized trial. Am J Med 2000;109(3):207-12.
126. Jenkins SC, Cecins NM, Collins GB. Outcomes and direct costs of a pulmonary rehabilitation service. Physiother Theory Pract 2001;17:67-76.
127. Griffiths TL, Phillips CJ, Davies S, Burr ML, Campbell IA. Cost effectiveness of an outpatient multidisciplinary pulmonary rehabilitation programme. Thorax 2001;56(10):779-84.
128. Cecins N, Geelhoed E, Jenkins SC. Reduction in hospitalisation following pulmonary rehabilitation in patients with COPD. Aust Health Rev 2008;32(3):415-22.
129. Goldstein RS, Gort EH, Guyatt GH, Feeny D. Economic analysis of respiratory rehabilitation. Chest 1997;112(2):370-9.
130. Clini E, Foglio K, Bianchi L, Porta R, Vitacca M, Ambrosino N. In-hospital short-term training program for patients with chronic airway obstruction. Chest 2001;120(5):1500-5. Available: http://www.chestjournal.org/content/120/5/1500.full.pdf+html (accessed 2009 Sep 30).
131. Sin DD, Stafinski T, Ng YC, Bell NR, Jacobs P. The impact of chronic obstructive pulmonary disease on work loss in the United States. Am J Respir Crit Care Med 2002;165(5):704-7.
132. Sin DD, Golmohammadi K, Jacobs P. Cost-effectiveness of inhaled corticosteroids for chronic obstructive pulmonary disease according to disease severity. Am J Med 2004;116(5):325-31.
133. Paggiaro PL, Dahle R, Bakran I, Frith L, Hollingworth K, Efthimiou J. Multicentre randomised placebo-controlled trial of inhaled fluticasone propionate in patients with chronic obstructive pulmonary disease. International COPD Study Group. Lancet 1998;351(9105):773-80.
134. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. American Thoracic Society. Am J Respir Crit Care Med 1995;152(5 Pt 2):S77-121.
135. Walters SJ, Brazier JE. Comparison of the minimally important difference for two health state utility measures: EQ-5D and SF-6D. Qual Life Res 2005;14(6):1523-32.
136. Oostenbrink JB, Rutten-van Molken MP, Monz BU, FitzGerald JM. Probabilistic Markov model to assess the cost-effectiveness of bronchodilator therapy in COPD patients in different countries. Value Health 2005;8(1):32-46.
137. Mittmann N, Kuramoto L, Seung SJ, Haddon JM, Bradley-Kennedy C, FitzGerald JM. The cost of moderate and severe COPD exacerbations to the Canadian healthcare system. Respir Med 2008;102(3):413-21.
138. Laupacis A, Feeny D, Detsky AS, Tugwell PX. How attractive does a new technology have to be to warrant adoption and utilization? Tentative guidelines for using clinical and economic evaluations. CMAJ 1992;146(4):473-81.
139. Anthonisen NR, Wright EC, Hodgkin JE. Prognosis in chronic obstructive pulmonary disease. Am Rev Respir Dis 1986;133(1):14-20.
140. de Oca MM, Talamo C, Halbert RJ, Perez-Padilla R, Lopez MV, Muino A, et al. Frequency of self-reported COPD exacerbation and airflow obstruction in five Latin American cities: the Proyecto Latinoamericano de Investigacion en Obstruccion Pulmonar (PLATINO) study. Chest 2009;136(1):71-8.
141. Miravitlles M, Mayordomo C, Artes M, Sanchez-Agudo L, Nicolau F, Segu JL. Treatment of chronic obstructive pulmonary disease and its exacerbations in general practice. EOLO Group. Estudio Observacional de la Limitacion Obstructiva al Flujo aEreo. Respir Med 1999;93(3):173-9.
PR for COPD: Clinical, Economic, and Budget Impact Analysis 60
142. Decramer M, Celli B, Kesten S, Lystig T, Mehra S, Tashkin DP. Effect of tiotropium on outcomes in patients with moderate chronic obstructive pulmonary disease (UPLIFT): a prespecified subgroup analysis of a randomised controlled trial. Lancet 2009;374(9696):1171-8.
143. Borg S, Ericsson A, Wedzicha J, Gulsvik A, Lundback B, Donaldson GC, et al. A computer simulation model of the natural history and economic impact of chronic obstructive pulmonary disease. Value Health 2004;7(2):153-67.
144. Alberta Health and Wellness Drug Benefit List [database online]. Edmonton: Alberta Health and Wellness; 2009. Available: http://www.health.alberta.ca/AHCIP/drug-benefit-list.html (accessed 2009 Sep 21).
145. Public Health Agency of Canada. COPD. In: Life and breath: respiratory disease in Canada. Ottawa: The Agency; 2007. Available: http://www.phac-aspc.gc.ca/publicat/2007/lbrdc-vsmrc/copd-mpoc-eng.php (accessed 2009 Jul 28).
146. van Durme YM, Verhamme KM, Stijnen T, van Rooij FJ, Van Pottelberge GR, Hofman A, et al. Prevalence, incidence, and lifetime risk for the development of COPD in the elderly: the Rotterdam study. Chest 2009;135(2):368-77.
147. National Institute for Clincal Excellence. Assumptions used in estimating a population benchmark. In: Pulmonary rehabilitation service for patients with COPD. London: The Institute; 2009. Available: http://www.nice.org.uk/usingguidance/commissioningguides/pulmonaryrehabilitationserviceforpatientswithcopd/assumptions.jsp (accessed 2009 Jul 27).
148. Statistics Canada. Consumer Price Index, historical summary (1989 to 2008) [database online]. Ottawa: Statistics Canada; 2009. Available: http://www40.statcan.ca/l01/cst01/econ46a-eng.htm (accessed 2009 Sep 30).
149. Yohannes AM, Connolly MJ. Pulmonary rehabilitation programmes in the UK: a national representative survey. Clin Rehabil 2004;18(4):444-9.
150. Fédération Française des Associations et Amicales de Malades, Insuffisants ou Handicapes Respiratoires (FFAAIR). Paris: FFAAIR; 2007. Available: http://www.ffaair.org/index.php (accessed 2009 Sep 29).
151. The Australian Lung Foundation. Pulmonary Rehabilitation. Bowen Hills (AU): The Foundation; 2009. Available: http://www.lungfoundation.com.au/content/view/197/197 (accessed 2009 Jul 23).
152. Cockram J, Cecins N, Jenkins S. Maintaining exercise capacity and quality of life following pulmonary rehabilitation. Respirology 2006;11(1):98-104.
153. Hailey D, Ohinmaa A, Roine R. Published evidence on the success of telecardiology: a mixed record. J Telemed Telecare 2004;10(Suppl 1):36-8.
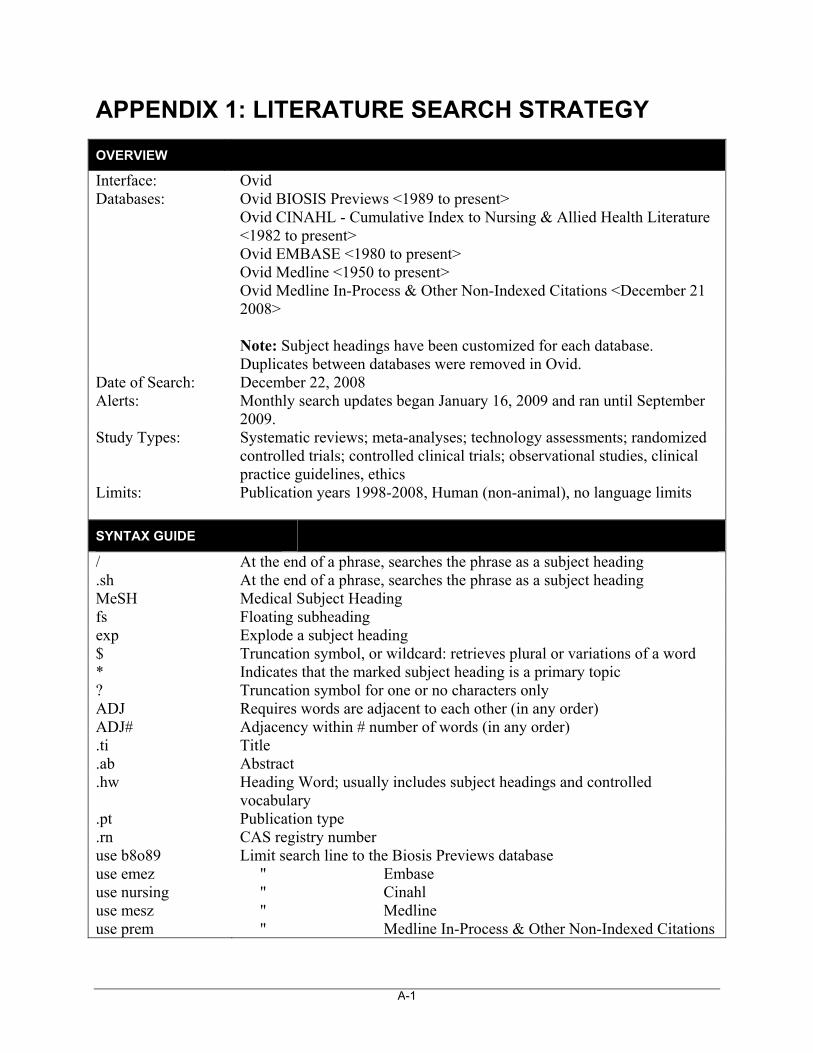
A-1
APPENDIX 1: LITERATURE SEARCH STRATEGY
OVERVIEW
Interface: Ovid Databases: Ovid BIOSIS Previews <1989 to present>
Ovid CINAHL - Cumulative Index to Nursing & Allied Health Literature <1982 to present> Ovid EMBASE <1980 to present> Ovid Medline <1950 to present> Ovid Medline In-Process & Other Non-Indexed Citations <December 21 2008> Note: Subject headings have been customized for each database. Duplicates between databases were removed in Ovid.
Date of Search: December 22, 2008 Alerts: Monthly search updates began January 16, 2009 and ran until September
2009. Study Types: Systematic reviews; meta-analyses; technology assessments; randomized
controlled trials; controlled clinical trials; observational studies, clinical practice guidelines, ethics
Limits: Publication years 1998-2008, Human (non-animal), no language limits
SYNTAX GUIDE
/ At the end of a phrase, searches the phrase as a subject heading .sh At the end of a phrase, searches the phrase as a subject heading MeSH Medical Subject Heading fs Floating subheading exp Explode a subject heading $ Truncation symbol, or wildcard: retrieves plural or variations of a word * Indicates that the marked subject heading is a primary topic ? Truncation symbol for one or no characters only ADJ Requires words are adjacent to each other (in any order) ADJ# Adjacency within # number of words (in any order) .ti Title .ab Abstract .hw Heading Word; usually includes subject headings and controlled
vocabulary .pt Publication type .rn CAS registry number use b8o89 Limit search line to the Biosis Previews database use emez " Embase use nursing " Cinahl use mesz " Medline use prem " Medline In-Process & Other Non-Indexed Citations
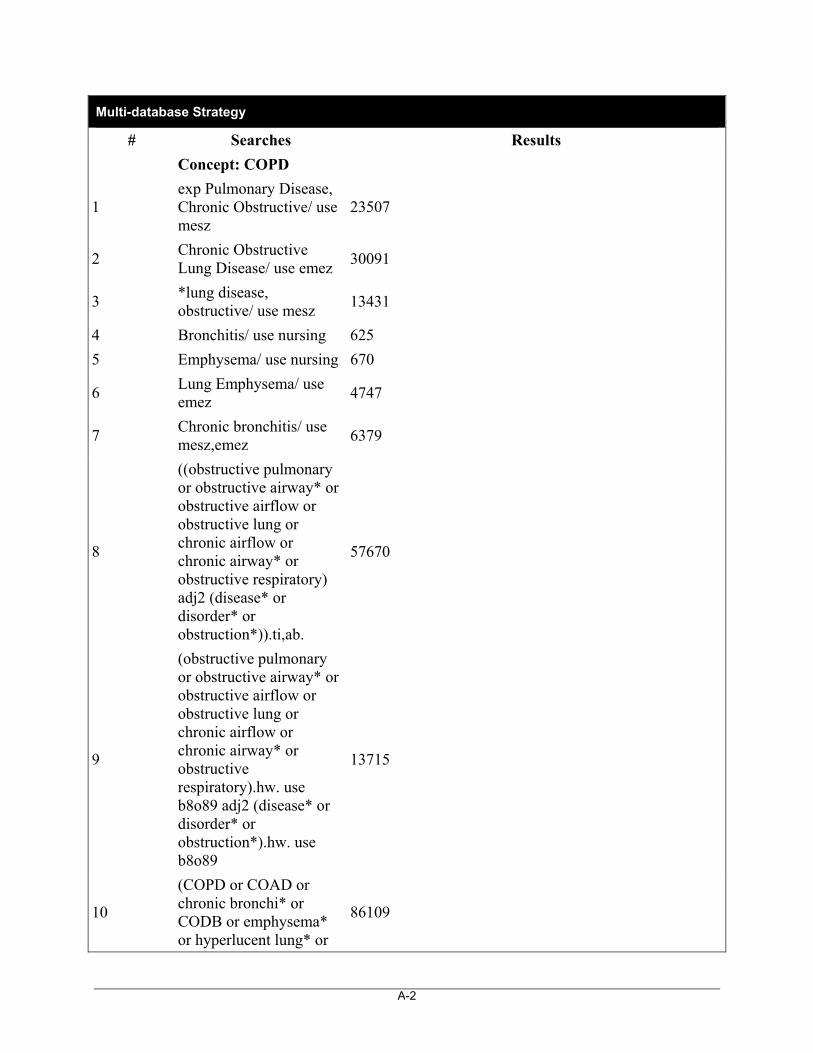
A-2
Multi-database Strategy
# Searches Results
Concept: COPD
1 exp Pulmonary Disease, Chronic Obstructive/ use mesz
23507
2 Chronic Obstructive Lung Disease/ use emez
30091
3 *lung disease, obstructive/ use mesz
13431
4 Bronchitis/ use nursing 625
5 Emphysema/ use nursing 670
6 Lung Emphysema/ use emez
4747
7 Chronic bronchitis/ use mesz,emez
6379
8
((obstructive pulmonary or obstructive airway* or obstructive airflow or obstructive lung or chronic airflow or chronic airway* or obstructive respiratory) adj2 (disease* or disorder* or obstruction*)).ti,ab.
57670
9
(obstructive pulmonary or obstructive airway* or obstructive airflow or obstructive lung or chronic airflow or chronic airway* or obstructive respiratory).hw. use b8o89 adj2 (disease* or disorder* or obstruction*).hw. use b8o89
13715
10
(COPD or COAD or chronic bronchi* or CODB or emphysema* or hyperlucent lung* or
86109
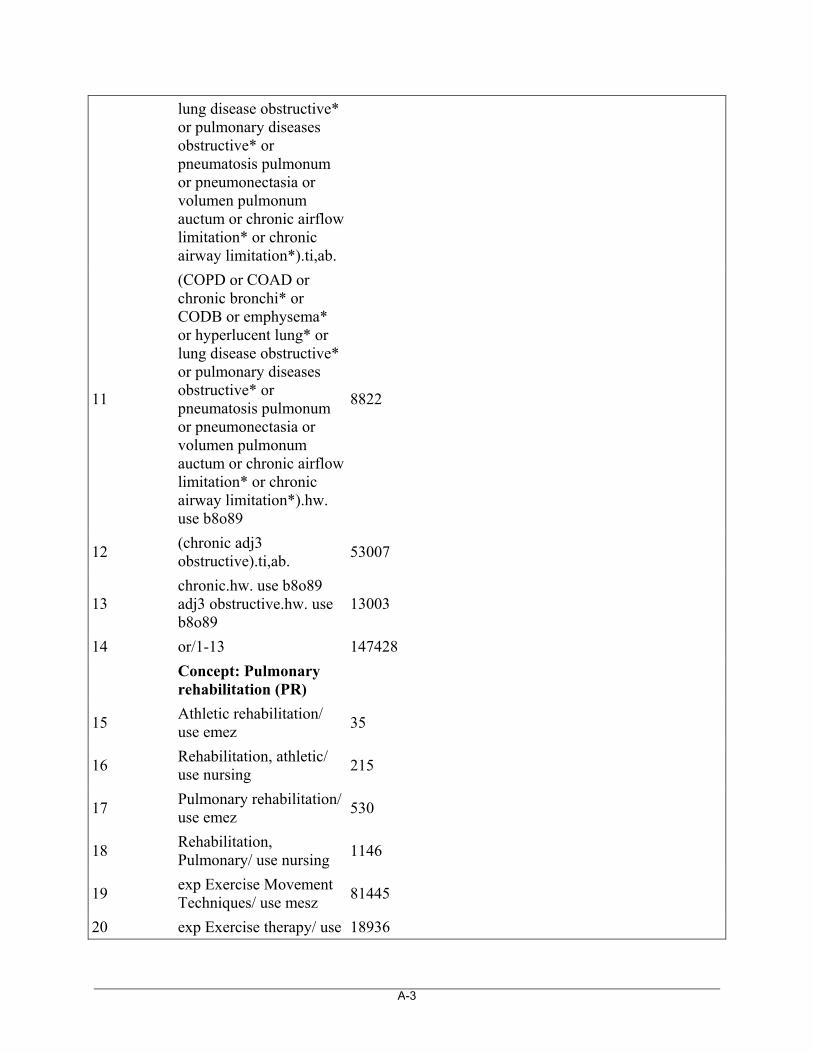
A-3
lung disease obstructive* or pulmonary diseases obstructive* or pneumatosis pulmonum or pneumonectasia or volumen pulmonum auctum or chronic airflow limitation* or chronic airway limitation*).ti,ab.
11
(COPD or COAD or chronic bronchi* or CODB or emphysema* or hyperlucent lung* or lung disease obstructive* or pulmonary diseases obstructive* or pneumatosis pulmonum or pneumonectasia or volumen pulmonum auctum or chronic airflow limitation* or chronic airway limitation*).hw. use b8o89
8822
12 (chronic adj3 obstructive).ti,ab.
53007
13 chronic.hw. use b8o89 adj3 obstructive.hw. use b8o89
13003
14 or/1-13 147428
Concept: Pulmonary rehabilitation (PR)
15 Athletic rehabilitation/ use emez
35
16 Rehabilitation, athletic/ use nursing
215
17 Pulmonary rehabilitation/ use emez
530
18 Rehabilitation, Pulmonary/ use nursing
1146
19 exp Exercise Movement Techniques/ use mesz
81445
20 exp Exercise therapy/ use 18936
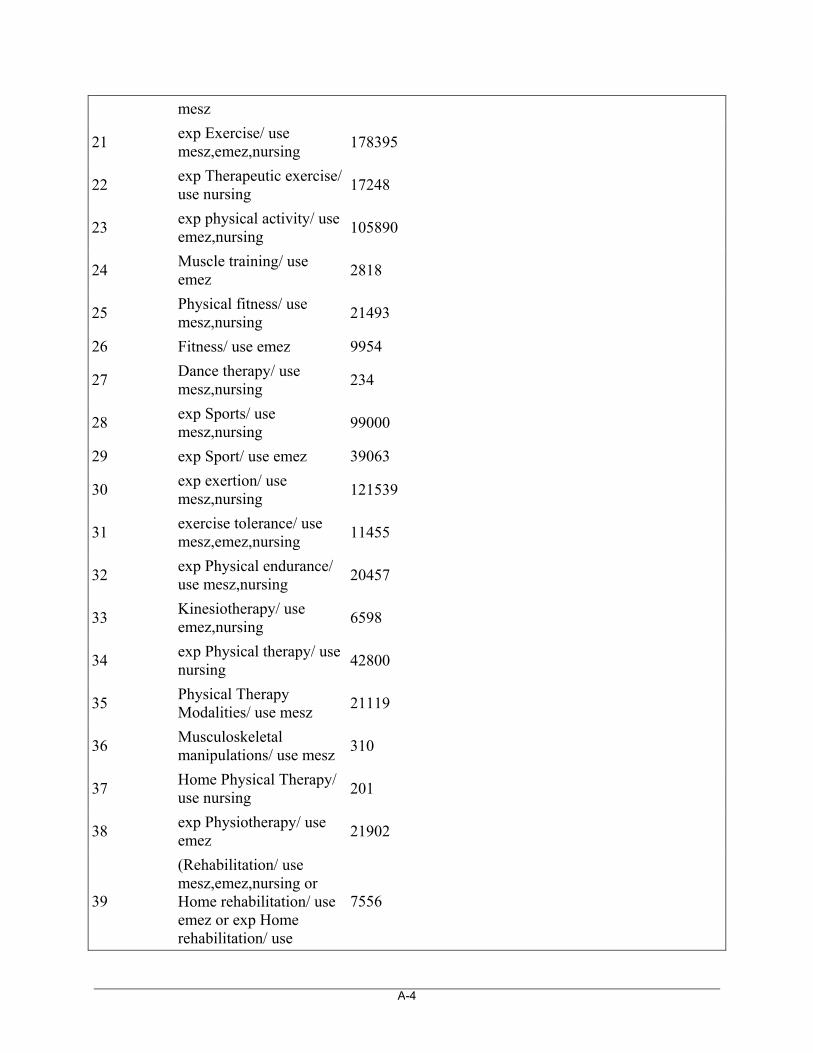
A-4
mesz
21 exp Exercise/ use mesz,emez,nursing
178395
22 exp Therapeutic exercise/ use nursing
17248
23 exp physical activity/ use emez,nursing
105890
24 Muscle training/ use emez
2818
25 Physical fitness/ use mesz,nursing
21493
26 Fitness/ use emez 9954
27 Dance therapy/ use mesz,nursing
234
28 exp Sports/ use mesz,nursing
99000
29 exp Sport/ use emez 39063
30 exp exertion/ use mesz,nursing
121539
31 exercise tolerance/ use mesz,emez,nursing
11455
32 exp Physical endurance/ use mesz,nursing
20457
33 Kinesiotherapy/ use emez,nursing
6598
34 exp Physical therapy/ use nursing
42800
35 Physical Therapy Modalities/ use mesz
21119
36 Musculoskeletal manipulations/ use mesz
310
37 Home Physical Therapy/ use nursing
201
38 exp Physiotherapy/ use emez
21902
39
(Rehabilitation/ use mesz,emez,nursing or Home rehabilitation/ use emez or exp Home rehabilitation/ use
7556
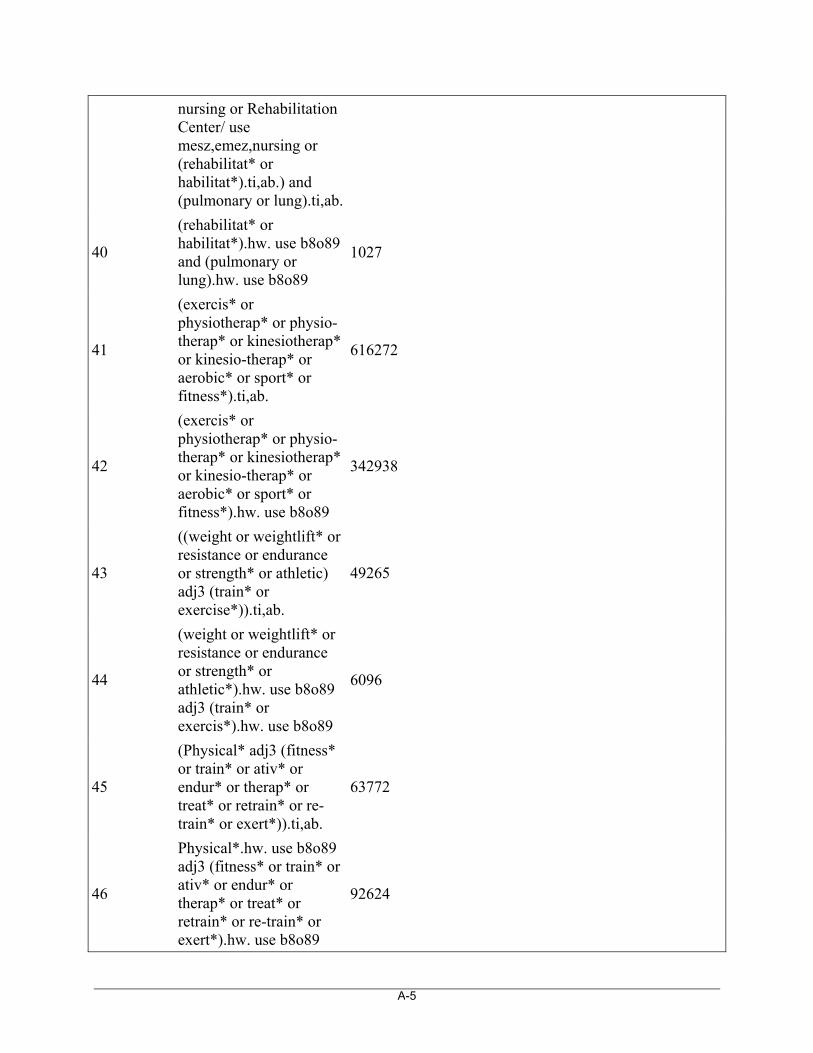
A-5
nursing or Rehabilitation Center/ use mesz,emez,nursing or (rehabilitat* or habilitat*).ti,ab.) and (pulmonary or lung).ti,ab.
40
(rehabilitat* or habilitat*).hw. use b8o89 and (pulmonary or lung).hw. use b8o89
1027
41
(exercis* or physiotherap* or physio-therap* or kinesiotherap* or kinesio-therap* or aerobic* or sport* or fitness*).ti,ab.
616272
42
(exercis* or physiotherap* or physio-therap* or kinesiotherap* or kinesio-therap* or aerobic* or sport* or fitness*).hw. use b8o89
342938
43
((weight or weightlift* or resistance or endurance or strength* or athletic) adj3 (train* or exercise*)).ti,ab.
49265
44
(weight or weightlift* or resistance or endurance or strength* or athletic*).hw. use b8o89 adj3 (train* or exercis*).hw. use b8o89
6096
45
(Physical* adj3 (fitness* or train* or ativ* or endur* or therap* or treat* or retrain* or re-train* or exert*)).ti,ab.
63772
46
Physical*.hw. use b8o89 adj3 (fitness* or train* or ativ* or endur* or therap* or treat* or retrain* or re-train* or exert*).hw. use b8o89
92624
A-6
47
(athletic* or strength* or physical* or exercis* or fitness*).ti,ab. and training/ use emez
11395
48 or/15-47 1194718
Results: COPD & PR
49 14 and 48 16039
Concept: Methodology filter: SRs/MAs/HTAs
50
(MEDLINE or systematic review).tw. or Meta-analysis.pt. or Meta-analysis/ use mesz
115950
51 exp Technology Assessment, Biomedical/ use mesz
7878
52 (Meta analysis or systematic review).ti,ab. use prem
5694
53 review.ti. use prem 15102
54
(Meta Analysis or Systematic Review or Biomedical Technology Assessment).mp. use b8o89
20156
55 (Meta Analysis or Systematic Review).sh. use emez
45829
56 medline.tw. use emez 23041
57 exp Meta Analysis/ use nursing
7250
58 systematic review.pt. use nursing
13184
59
(meta analy* or metaanaly* or met analy* or metanaly* or health technology assessment* or HTA or HTAs or biomedical technology assessment* or bio-medical technology
74349
A-7
assessment*).ti,ab.
60
(meta regression* or metaregression* or mega regression*).ti,ab. use b8o89
445
61
((systematic* adj (literature review* or review* or overview*)) or (methodologic* adj (literature review* or review* or overview*))).ti,ab.
55871
62
((quantitative adj (review* or overview* or synthes*)) or (research adj (integration* or overview*))).ti,ab.
1750
63
((integrative adj2 (review* or overview*)) or (collaborative adj (review* or overview*)) or (pool* adj analy*)).ti,ab.
7181
64 (data synthes* or data extraction* or data abstraction*).ti,ab.
21342
65 (handsearch* or hand search*).ti,ab.
6715
66
(mantel haenszel or peto or der simonian or dersimonian or fixed effect* or latin square*).ti,ab.
21482
67 or/50-66 249522
Concept: Methodology filter: economic (with cost-related QOL)
68 *Economics/ use mesz,emez,nursing,b8o89
12490
69 exp Economic Evaluation/ use emez
101056
70 *Economics, Medical/ 4589
A-8
use mesz
71 *Economics, Pharmaceutical/ use mesz,nursing
1525
72 *Economics, Hospital/ use mesz
5729
73 exp "Costs and Cost Analysis"/ use mesz,nursing
172342
74 exp decision support techniques/ use mesz
57965
75 exp Budgets/ use mesz,nursing
12685
76 exp Models, economic/ use mesz
6231
77 markov chains.sh. use mesz
5268
78 monte carlo method.sh. use mesz,emez
19009
79 uncertainty.sh. use mesz,emez,nursing
4811
80 Quality-Adjusted Life Years/ use mesz
3719
81 Value of life/ use mesz 5091
82 exp Health status indicators/ use mesz,nursing
128044
83 quality of life/ use mesz,emez,nursing
187536
84 exp Health economics/ use emez
227305
85 exp "health care cost"/ use emez
103597
86 Budget/ use emez 7772
87 Socioeconomics/ use emez
31553
88 Decision support system/ use emez
1503
89 quality adjusted life year/ use emez
3971
A-9
90 "Economic Value of Life"/ use nursing
122
91 Health Resource Allocation/ use nursing
3500
92 Economic Aspects of Illness/ use nursing
1937
93
(econom* or cost or costs or costly or costing or costed or price or prices or pricing or priced or discount or discounts or discounted or discounting or expenditure or expenditures or budget* or afford* or pharmacoeconomic* or pharmaco-economic* or financ*).ti,ab.
1011386
94
(cost* adj2 (util* or effective* or efficac* or benefit* or consequence* or analy* or minimi* or saving* or breakdown or lowering or estimate* or variable* or allocation* or control* or illness or sharing or life or lives or affordabl* or instrument* or technolog* or day* or fee or fees or charge or charges)).ti,ab.
209466
95 (decision adj2 (tree* or analy* or model*)).ti,ab.
20568
96
((value or values or valuation) adj2 (money or monetary or life or lives or costs or cost)).ti,ab.
8269
97 (markov* or monte carlo).ti,ab.
54484
98
(sensitivity analys#s or "willingness to pay" or quality adjusted life or disability adjusted
31077
A-10
life).ti,ab.
99
(unit cost? or drug cost? or hospital cost? or health care cost? or medical cost?).ti,ab.
35191
100 (health adj2 (indicator? or status or utilit*)).ti,ab.
71497
101 or/68-100 1702919
Concept: Methodology filter: QOL
102 quality of life/ use mesz,emez,nursing
187536
103
(qol or qoly or qolys or hrqol or qaly or qalys or qale or qales or qald or qtime or daly or euroqol or eq5d or eq-5d or hql or hqol or h-qol or hrqol or hr-qol or hye or hyes).ti,ab.
43295
104 or/102-103 204353
Concept: Methodology filter: Practice Guidelines
105 Guidelines as topic/ use mesz
22233
106 Health Planning Guidelines/ use mesz
2760
107 Practice Guidelines as Topic/ use mesz
48893
108 Clinical Protocols/ use mesz
15022
109
(Guideline or Practice Guideline or Consensus Development Conference).pt. use mesz
23863
110 Standards.fs. use mesz 417839
111 Practice Guideline/ use emez
100506
112 Clinical Practice/ use emez
77772
A-11
113 Clinical Protocols/ use emez
40482
114 Health Care Planning/ use emez
21289
115 Practice guidelines/ use nursing
16133
116 exp Protocols/ use nursing
10660
117 exp consensus development conference/ use mesz
6521
118
(practice guidelines or protocol or critical path or care plan).pt. or standards.pt. use nursing
15613
119 (guideline* or standards or best practice).ti.
116643
120 (guideline* or standards or best practice).hw. use b8o89
17814
121
(expert consensus or consensus statement or consensus conference* or practice parameter* or position statement* or policy statement* or CPG or CPGs).ti,ab.
55054
122
(expert consensus or consensus statement or consensus conference* or practice parameter* or position statement* or policy statement* or CPG or CPGs).hw. use b8o89
7090
123 or/105-122 860524
Concept: Methodology filter: RCTs & CCTs
124
(Randomized Controlled Trial or Controlled Clinical Trial or Clinical Trial).pt.
556959
125 Randomized Controlled 6
A-12
Trials as Topic/ use prem
126 Randomized Controlled Trials as Topic/ use mesz
58509
127 Controlled Clinical Trials as Topic/ use prem
0
128 Controlled Clinical Trials as Topic/ use mesz
3961
129 Clinical Trials as Topic/ use prem
5
130 Clinical Trials as Topic/ use mesz
144891
131 Randomized Controlled Trial/ use emez
163768
132 Randomization/ use emez 26367
133 Controlled Clinical Trial/ use emez
54634
134 Double-Blind Method.sh. use prem
1
135 Double-Blind Method.sh. use mesz
101566
136 Double Blind Procedure.sh. use emez
70768
137 Double-blind Studies.sh. use nursing
12341
138 Single-blind Method.sh. use prem
1
139 Single-blind Method.sh. use mesz
12762
140 Single Blind Procedure.sh. use emez
7858
141 Single-blind Studies.sh. use nursing
3241
142 Placebos/ use mesz 28390
143 placebos/ use prem 0
144 Placebo$/ use emez 121040
145 Placebo$/ use nursing 4855
146 Random Allocation.sh. use prem
5
147 Random Allocation.sh. 63710
A-13
use mesz
148 Random Assignment.sh. use nursing
19971
149 Clinical Trials.sh. use nursing
52817
150
(random$ or sham$ or placebo$ or (singl$ adj (blind$ or dumm$ or mask$)) or (doubl$ adj (blind$ or dumm$ or mask$))).ti,ab,hw.
1768917
151
((tripl$ adj (blind$ or dumm$ or mask$)) or (trebl$ adj (blind$ or dumm$ or mask$))).ti,ab,hw.
576
152 trial.ti. 227141
153 or/124-152 2131988
Concept: Methodology filter: Observational studies
154 Comparative Study/ 1616393
155 Evaluation Studies as Topic/
121342
156 evaluation studies.pt. 113940
157 Comparative Study.pt. 1455392
158 Multicenter Study.pt. 104730
159 multicenter study/ 151319
160
epidemiologic studies/ or case-control studies/ or retrospective studies/ or cohort studies/ or longitudinal studies/ or follow-up studies/ or prospective studies/ or cross-sectional studies/
1783643
161 (Observational adj2 (study or studies or design)).ti,ab.
68111
162 (Population adj3 (study or studies)).ti,ab.
164906
A-14
163 control groups/ 6022
164 ((multicent$ or multi-cent$) adj2 (study or studies)).ti,ab.
65036
165
((case control* or case-control* or case comparison*) adj2 (study or studies or design* or analysis or analyses or trial*)).ti,ab.
120407
166
(cohort adj2 (study or studies or design$ or analysis or analyses)).ti,ab.
137701
167 evaluation studies/ 180163
168
((retrospective* or prospective* or cross-section* or longitudinal* or follow-up) adj2 (study or studies or design$ or analysis or analyses)).ti,ab.
912425
169
((long term or long-term or longterm) adj2 (study or studies or design or analysis or analyses or trial*)).ti,ab.
53237
170 or/154-169 4171013
Concept: Methodology filter: ethics
171 exp Ethics/ use mesz,emez,nursing
225600
172 exp Privacy/ use mesz,emez
10927
173 exp Privacy/ and Confidentiality/ use nursing
8404
174 Computer Security/ use mesz,emez
4404
175 Data Security/ use nursing
2422
A-15
176 exp Jurisprudence/ use mesz,nursing
173418
177 exp Legal aspect/ use emez
232733
178 exp Informatics/es, lj use mesz
134
179 exp Informatics/ei use nursing
198
180 exp Data Collection/es, lj use mesz
5445
181 exp Data Collection/lj, ei use nursing
169
182
Medical Records Systems, Computerized/es, lj use mesz
860
183 Computerized Patient Record/lj, ei use nursing
100
184 (ethic* or moral* or bioethic* or e-ethic*).ti,ab,hw.
251861
185 (privacy or confidential* or security or safe*).ti,ab,hw.
1080074
186 (legal* or liability or law).ti,ab,hw.
332577
187 (informed adj2 (consent or decision making)).ti,ab,hw.
72340
188
((data or information or informatics or records or record or database*) adj3 (disclosure or compromis* or ownership or property or modification* or policy or policies or protect*)).ti,ab.
20088
189 "secondary use of data".ti,ab.
408
190 or/171-189 1837113
A-16
Concept: Methodology filter: humans
191 exp animals/ 22863457
192 exp animal experimentation/
1273853
193 exp models animal/ 791579
194 nonhuman/ 3153714
195 exp vertebrate/ 29990958
196 animal.po. 0
197 or/191-196 32155762
198 exp humans/ 22289186
199 human.po. 0
200 or/198-199 22289186
201 197 not 200 9866576
Results: COPD & PR & (SRs OR RCTs OR observational studies OR ethics) & human filter
202 49 and (67 or 153 or 170 or 190)
5866
203 202 not 201 5808
Results: COPD & PR & (QOL OR Practice Guidelines)
204 49 and (104 or 123) 2562
205 203 or 204 7068
206 limit 205 to yr="1998 - 2009"
5155
207 remove duplicates from 206
3240
Results: COPD & economic filter
208 49 and 101 3336
209 limit 208 to yr="1998 - 2009"
2785
210 remove duplicates from 209
1914
A-17
OTHER DATABASES SEARCHED
Cochrane Library Databases Issue 4 2008
Same MeSH, keywords, limits, and study types used as per Medline search, with appropriate syntax used.
Centre for Reviews and Dissemination Databases (CRD) University of York 2008
Same keywords and date limits used as per Medline search, excluding study types and Human restrictions.
Health Economic Evaluations Database (HEED) http://heed.wiley.com
Syntax adjusted for HEED database
Grey Literature and Hand Searches Date of Search: December 2008 Keywords: Included terms COPD, chronic obstructive pulmonary disease, pulmonary
rehabilitation, exercise Limits: Publication years 1998-present
NOTE: This section lists the main agencies, organizations, and websites searched; it is not a complete list. For a complete list of sources searched, contact CADTH (http://www.cadth.ca). Health Technology Assessment Agencies Alberta Heritage Foundation for Medical Research (AHFMR) http://www.ahfmr.ab.ca Agence d’Evaluation des Technologies et des Modes d’Intervention en Santé (AETMIS). Québec http://www.aetmis.gouv.qc.ca Canadian Agency for Drugs and Technologies in Health (CADTH) http://www.cadth.ca Centre for Evaluation of Medicines. Father Sean O'Sullivan Research Centre, St.Joseph's Healthcare,Hamilton, and McMaster University, Faculty of Health Sciences. Hamilton, Ontario http://www.thecem.net/ Centre for Health Services and Policy Research, University of British Columbia http://www.chspr.ubc.ca/cgi-bin/pub
A-18
Health Quality Council of Alberta (HQCA) http://www.hqca.ca Health Quality Council. Saskatchewan. http://www.hqc.sk.ca/ Institute for Clinical Evaluative Sciences (ICES). Ontario http://www.ices.on.ca/ Institute of Health Economics (IHE). Alberta http://www.ihe.ca/ Manitoba Centre for Health Policy (MCHP) http://www.umanitoba.ca/centres/mchp/ Ontario Ministry of Health and Long Term Care. Health Technology Analyses and Recommendations http://www.health.gov.on.ca/english/providers/program/ohtac/tech/techlist_mn.html The Technology Assessment Unit of the McGill University Health Centre http://www.mcgill.ca/tau/ Therapeutics Initiative. Evidence-Based Drug Therapy. University of British Columbia http://www.ti.ubc.ca Health Technology Assessment International (HTAi) http://www.htai.org International Network for Agencies for Health Technology Assessment (INAHTA) http://www.inahta.org WHO Health Evidence Network http://www.euro.who.int/HEN Australian Safety and Efficacy Register of New Interventional Procedures – Surgical (ASERNIP-S) http://www.surgeons.org/Content/NavigationMenu/Research/ASERNIPS/default.htm Centre for Clinical Effectiveness, Monash University http://www.med.monash.edu.au/healthservices/cce/ Medicare Services Advisory Committee, Department of Health and Aging http://www.msac.gov.au/
A-19
NPS RADAR (National Prescribing Service Ltd.) http://www.npsradar.org.au/site.php?page=1&content=/npsradar%2Fcontent%2Farchive_alpha.html Institute of Technology Assessment (ITA) http://www.oeaw.ac.at/ita/index.htm Federal Kenniscentrum voor de Gezendheidszorg http://www.kenniscentrum.fgov.be Danish Centre for Evaluation and Health Technology Assessment (DCEHTA). National Board of Health http://www.dihta.dk/ DSI Danish Institute for Health Services Research and Development http://www.dsi.dk/frz_about.htm Finnish Office for Health Care Technology and Assessment (FinOHTA). National Research and Development Centre for Welfare and Health http://finohta.stakes.fi/EN/index.htm L’Agence Nationale d’Accréditation et d’Evaluation en Santé (ANAES). Ministere de la Santé, de la Famille, et des Personnes handicappés http://www.anaes.fr/anaes/anaesparametrage.nsf/HomePage?ReadForm Committee for Evaluation and Diffusion of Innovative Technologies (CEDIT) http://cedit.aphp.fr/english/index_present.html German Institute for Medical Documentation and Information (DIMDI). Federal Ministry of Health http://www.dimdi.de/static/de/hta/db/index.htm Health Service Executive http://www.hse.ie/eng/ College voor Zorgverzekeringen/Health Care Insurance Board (CVZ) http://www.cvz.nl Health Council of the Netherlands http://www.gr.nl New Zealand Health Technology Assessment Clearing House for Health Outcomes and Health Technology Assessment (NZHTA) http://nzhta.chmeds.ac.nz/
A-20
Norwegian Centre for Health Technology Assessment (SMM) http://www.kunnskapssenteret.no/ Agencia de Evaluación de Tecnologias Sanitarias (AETS), Instituto de Salud “Carlos III”/ Health Technology Assessment Agency http://www.isciii.es/htdocs/investigacion/Agencia_quees.jsp Basque Office for Health Technology Assessment (OSTEBA). Departemento de Sanidad http://www.osasun.ejgv.euskadi.net/r52-2536/es/ Catalan Agency for Health Technology Assessment and Research (CAHTA) http://www.gencat.net/salut/depsan/units/aatrm/html/en/Du8/index.html CMT - Centre for Medical Technology Assessment http://www.cmt.liu.se/ Swedish Council on Technology Assessment in Health Care (SBU) http://www.sbu.se/ Swiss Network for Health Technology Assessment http://www.snhta.ch/ European Information Network on New and Changing Health Technologies (EUROSCAN). University of Birmingham. National Horizon Scanning Centre http://www.euroscan.bham.ac.uk National Horizon Scanning Centre (NHSC) http://www.pcpoh.bham.ac.uk/publichealth/horizon NIHR Health Technology Assessment Programme / National Coordinating Centre for Health Technology Assessment (NCCHTA). Department of Health R&D Division http://www.hta.ac.uk/ NHS National Institute for Clinical Excellence (NICE) http://www.nice.org.uk NHS Quality Improvement Scotland http://www.nhshealthquality.org University of York NHS Centre for Reviews and Dissemination (NHS CRD) http://www.york.ac.uk/inst/crd The Wessex Institute for Health Research and Development. Succinct and Timely Evaluated Evidence Review (STEER) http://www.wihrd.soton.ac.uk/
A-21
West Midlands Health Technology Assessment Collaboration (WMHTAC) http://www.publichealth.bham.ac.uk/wmhtac/ Agency for Healthcare Research and Quality (AHRQ) http://www.ahrq.gov/ Dept. of Veterans Affairs Research & Development, general publications http://www.research.va.gov/ VA Technology Assessment Program (VATAP) http://www.va.gov/vatap/ ECRI http://www.ecri.org/ Institute for Clinical Systems Improvement http://www.icsi.org/index.asp Technology Evaluation Center (Tec). BlueCross BlueShield Association http://www.bluecares.com/tec/index.html University HealthSystem Consortium (UHC) http://www.uhc.edu/ Health Economic Bases Codecs. CODECS (COnnaissances et Décision en EConomie de la Santé) Collège des Economistes de la Santé/INSERM http://infodoc.inserm.fr/codecs/codecs.nsf Centre for Health Economics and Policy Analysis (CHEPA). Dept. of Clinical Epidemiology and Biostatistics. Faculty of Health Sciences. McMaster University, Canada http://www.chepa.org Health Economics Research Group (HERG). Brunel University, U.K. http://www.brunel.ac.uk/about/acad/herg Health Economics Research Unit (HERU). University of Aberdeen http://www.abdn.ac.uk/heru/ The Hospital for Sick Children (Toronto). PEDE Database http://pede.bioinfo.sickkids.on.ca/pede/index.jsp University of Connecticut. Department of Economics. RePEc database http://ideas.repec.org
A-22
Organizations The American Thoracic Society http://www.thoracic.org/ The European Respiratory Society http://dev.ersnet.org/ The British Thoracic Society http://www.brit-thoracic.org.uk/ American Association of Cardiovascular and Pulmonary Rehabilitation http://www.aacvpr.org/ Canadian Thoracic Society http://www.lung.ca/cts-sct/home-accueil_e.php Canadian Lung Association http://www.lung.ca/home-accueil_e.php Search Engines Google http://www.google.ca/ Yahoo! http://www.yahoo.com
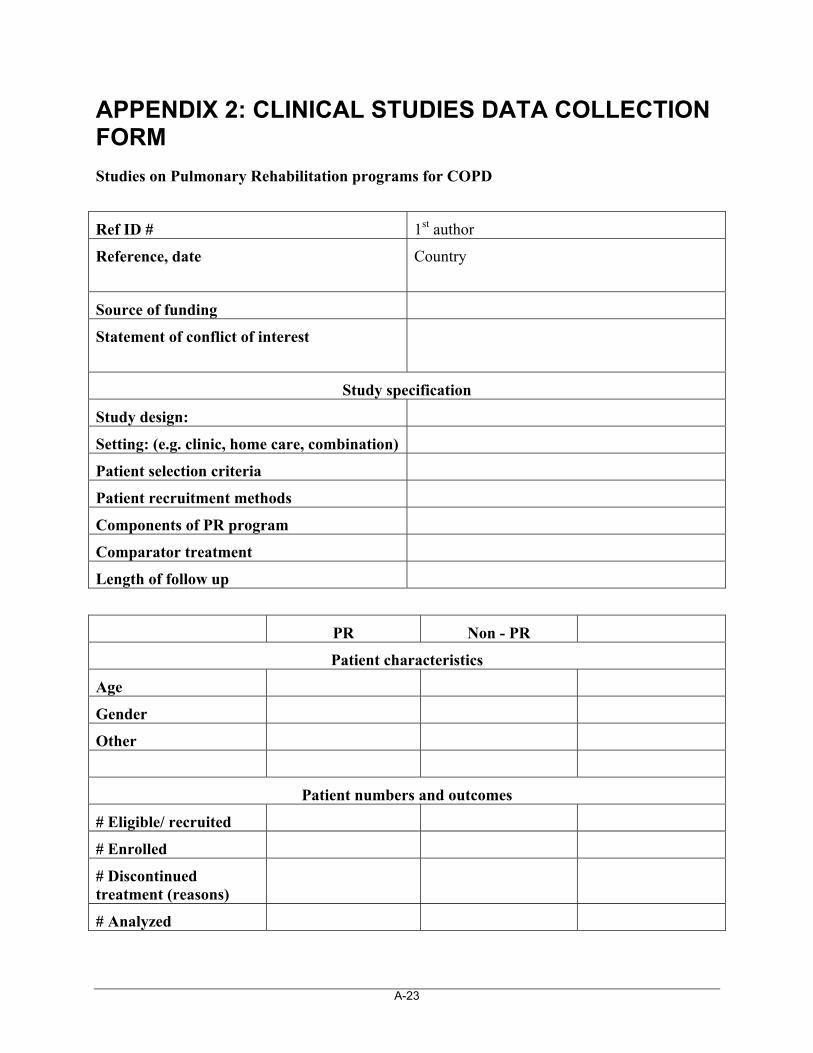
A-23
APPENDIX 2: CLINICAL STUDIES DATA COLLECTION FORM
Studies on Pulmonary Rehabilitation programs for COPD
Ref ID # 1st author
Reference, date
Country
Source of funding
Statement of conflict of interest
Study specification
Study design:
Setting: (e.g. clinic, home care, combination)
Patient selection criteria
Patient recruitment methods
Components of PR program
Comparator treatment
Length of follow up
PR Non - PR
Patient characteristics
Age
Gender
Other
Patient numbers and outcomes
# Eligible/ recruited
# Enrolled
# Discontinued treatment (reasons)
# Analyzed
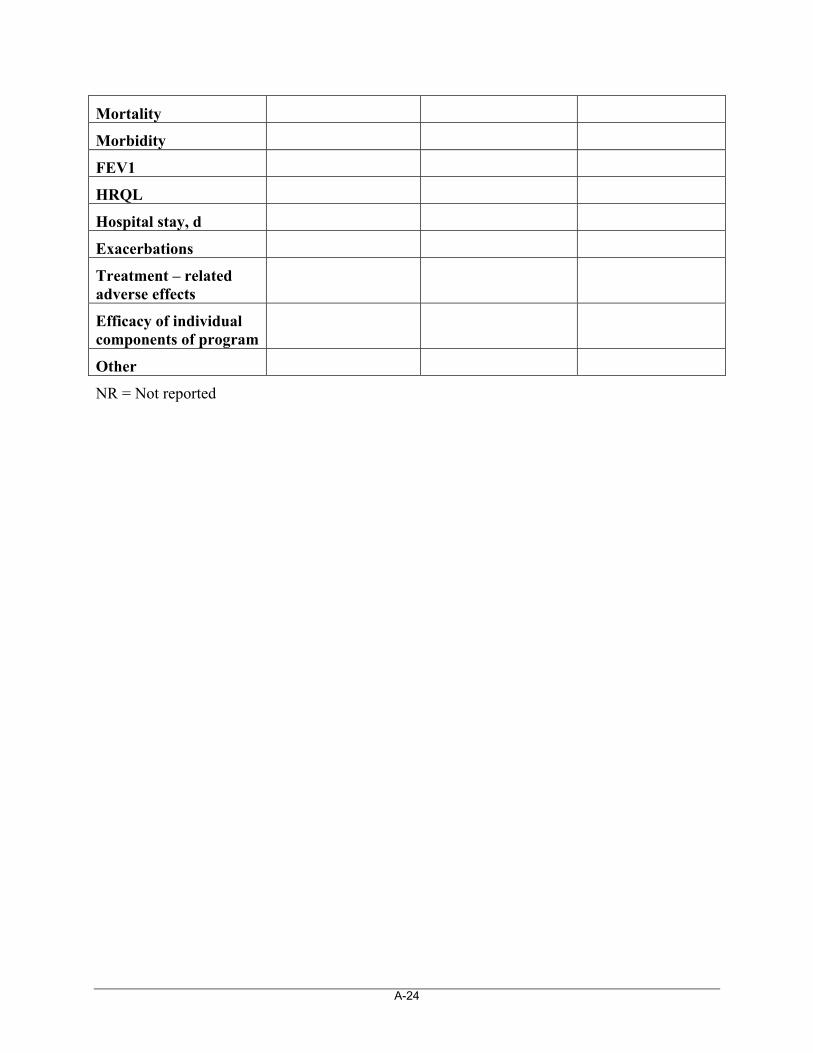
A-24
Mortality
Morbidity
FEV1
HRQL
Hospital stay, d
Exacerbations
Treatment – related adverse effects
Efficacy of individual components of program
Other
NR = Not reported
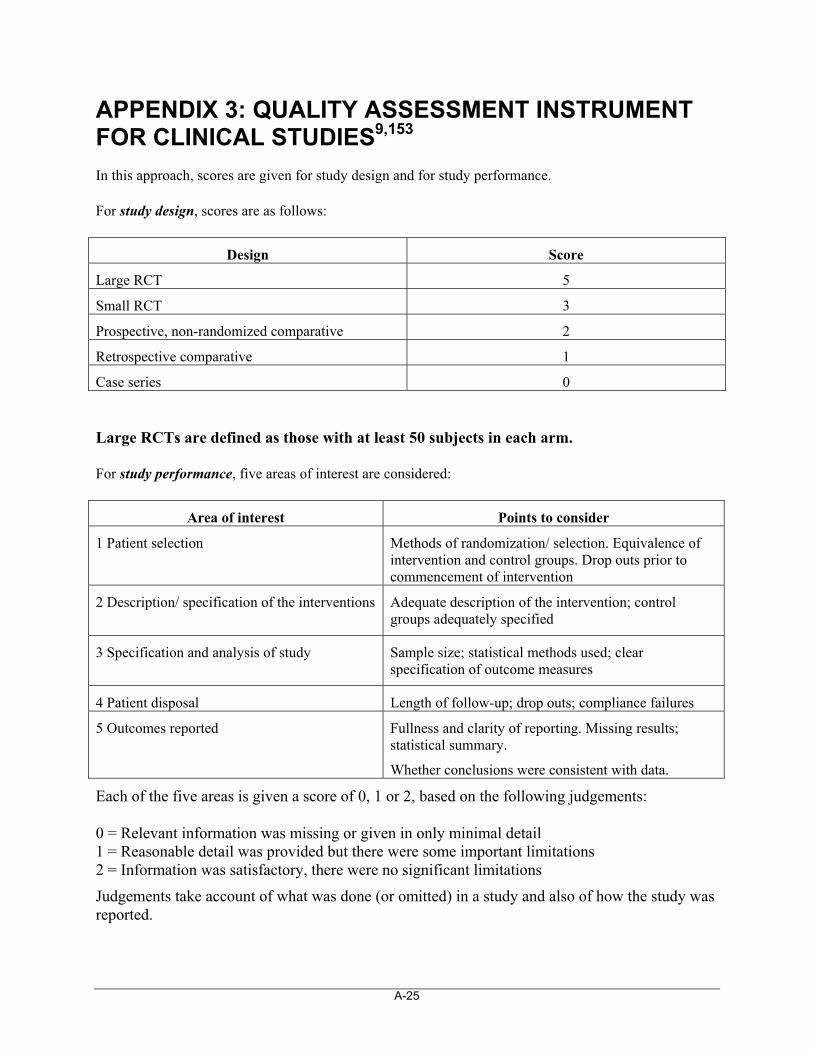
A-25
APPENDIX 3: QUALITY ASSESSMENT INSTRUMENT FOR CLINICAL STUDIES9,153
In this approach, scores are given for study design and for study performance.
For study design, scores are as follows:
Design Score
Large RCT 5
Small RCT 3
Prospective, non-randomized comparative 2
Retrospective comparative 1
Case series 0
Large RCTs are defined as those with at least 50 subjects in each arm.
For study performance, five areas of interest are considered:
Area of interest Points to consider
1 Patient selection Methods of randomization/ selection. Equivalence of intervention and control groups. Drop outs prior to commencement of intervention
2 Description/ specification of the interventions
Adequate description of the intervention; control groups adequately specified
3 Specification and analysis of study
Sample size; statistical methods used; clear specification of outcome measures
4 Patient disposal Length of follow-up; drop outs; compliance failures
5 Outcomes reported Fullness and clarity of reporting. Missing results; statistical summary.
Whether conclusions were consistent with data.
Each of the five areas is given a score of 0, 1 or 2, based on the following judgements:
0 = Relevant information was missing or given in only minimal detail 1 = Reasonable detail was provided but there were some important limitations 2 = Information was satisfactory, there were no significant limitations
Judgements take account of what was done (or omitted) in a study and also of how the study was reported.
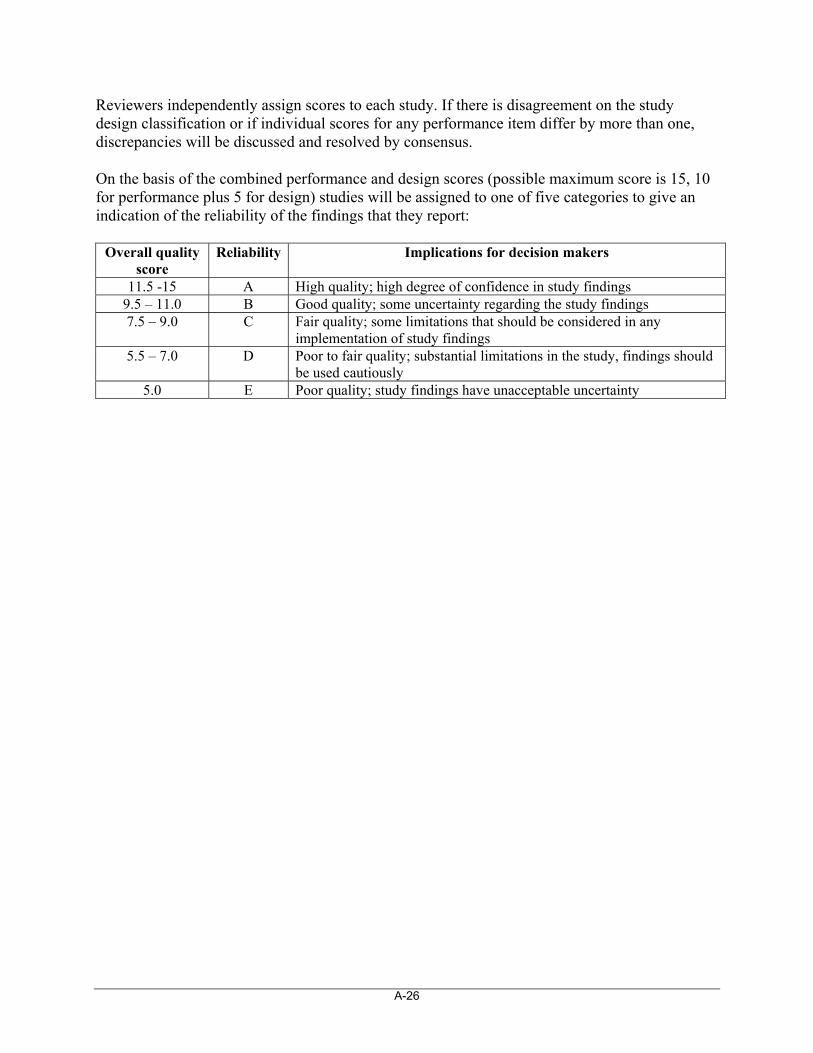
A-26
Reviewers independently assign scores to each study. If there is disagreement on the study design classification or if individual scores for any performance item differ by more than one, discrepancies will be discussed and resolved by consensus.
On the basis of the combined performance and design scores (possible maximum score is 15, 10 for performance plus 5 for design) studies will be assigned to one of five categories to give an indication of the reliability of the findings that they report:
Overall quality score
Reliability Implications for decision makers
11.5 -15 A High quality; high degree of confidence in study findings 9.5 – 11.0 B Good quality; some uncertainty regarding the study findings 7.5 – 9.0 C Fair quality; some limitations that should be considered in any
implementation of study findings 5.5 – 7.0 D Poor to fair quality; substantial limitations in the study, findings should
be used cautiously 5.0 E Poor quality; study findings have unacceptable uncertainty
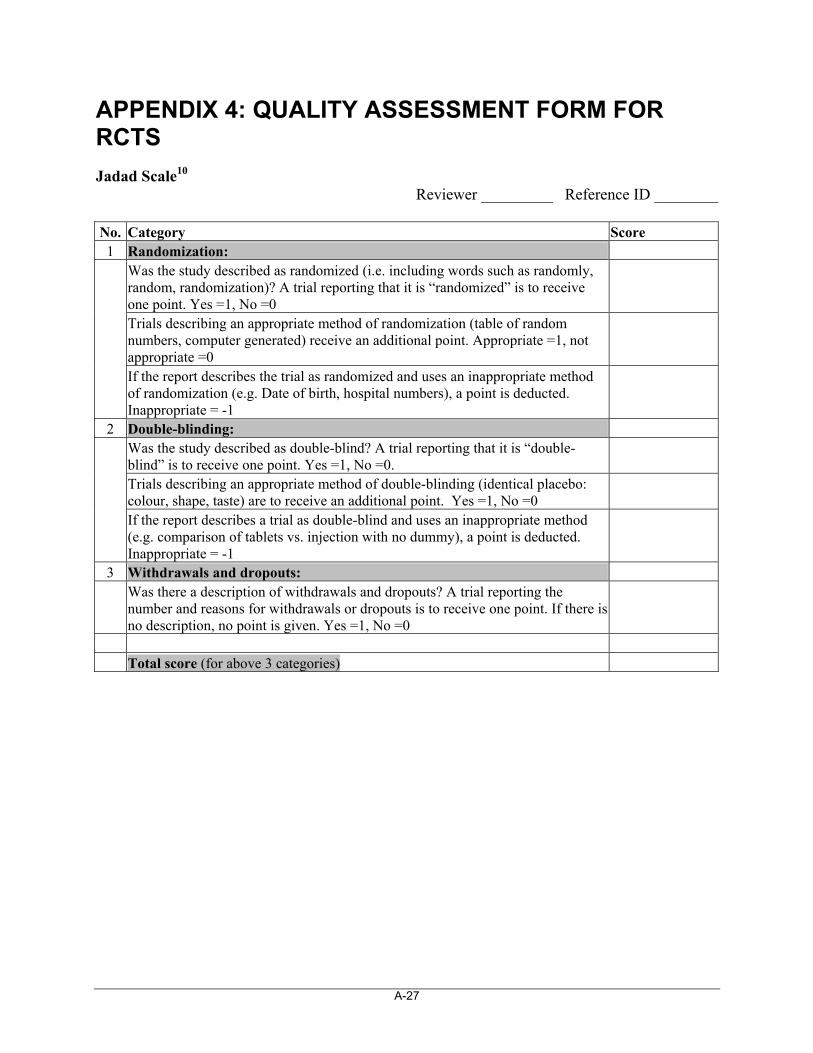
A-27
APPENDIX 4: QUALITY ASSESSMENT FORM FOR RCTS
Jadad Scale10 Reviewer _________ Reference ID ________
No. Category Score 1 Randomization:
Was the study described as randomized (i.e. including words such as randomly, random, randomization)? A trial reporting that it is “randomized” is to receive one point. Yes =1, No =0 Trials describing an appropriate method of randomization (table of random numbers, computer generated) receive an additional point. Appropriate =1, not appropriate =0
If the report describes the trial as randomized and uses an inappropriate method of randomization (e.g. Date of birth, hospital numbers), a point is deducted. Inappropriate = -1
2 Double-blinding: Was the study described as double-blind? A trial reporting that it is “double-blind” is to receive one point. Yes =1, No =0. Trials describing an appropriate method of double-blinding (identical placebo: colour, shape, taste) are to receive an additional point. Yes =1, No =0
If the report describes a trial as double-blind and uses an inappropriate method (e.g. comparison of tablets vs. injection with no dummy), a point is deducted. Inappropriate = -1
3 Withdrawals and dropouts:
Was there a description of withdrawals and dropouts? A trial reporting the number and reasons for withdrawals or dropouts is to receive one point. If there is no description, no point is given. Yes =1, No =0
Total score (for above 3 categories)
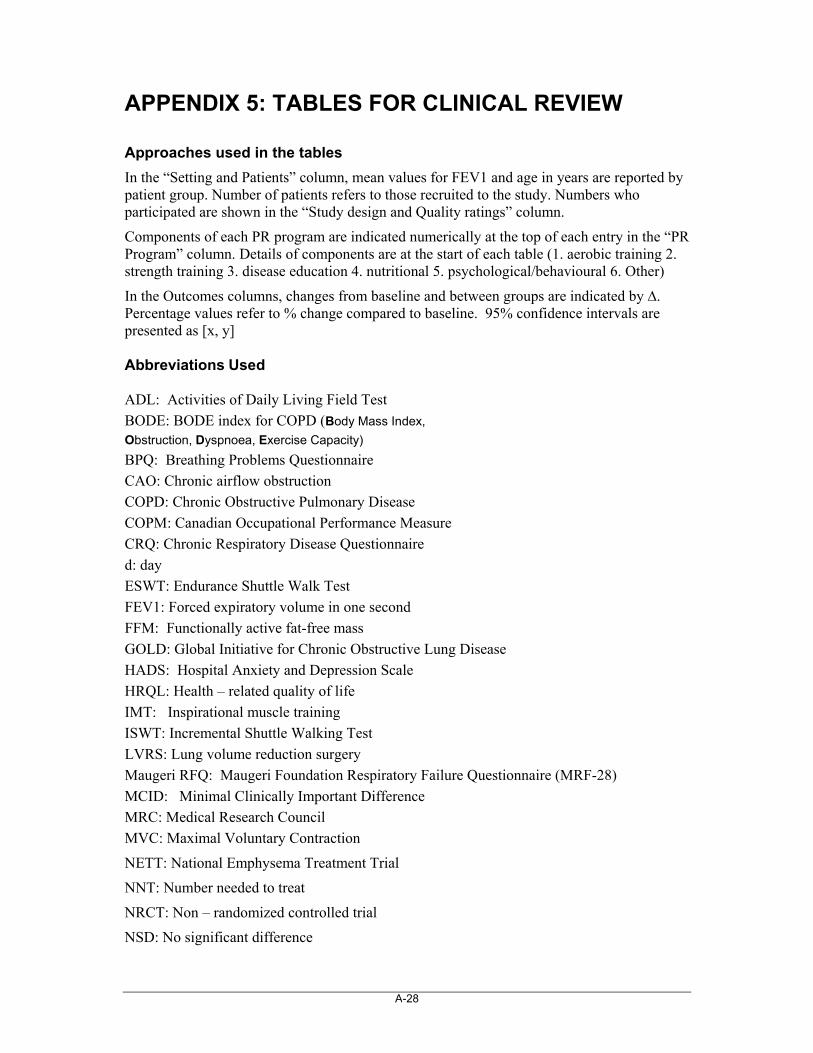
A-28
APPENDIX 5: TABLES FOR CLINICAL REVIEW
Approaches used in the tables
In the “Setting and Patients” column, mean values for FEV1 and age in years are reported by patient group. Number of patients refers to those recruited to the study. Numbers who participated are shown in the “Study design and Quality ratings” column.
Components of each PR program are indicated numerically at the top of each entry in the “PR Program” column. Details of components are at the start of each table (1. aerobic training 2. strength training 3. disease education 4. nutritional 5. psychological/behavioural 6. Other)
In the Outcomes columns, changes from baseline and between groups are indicated by ∆. Percentage values refer to % change compared to baseline. 95% confidence intervals are presented as [x, y] Abbreviations Used ADL: Activities of Daily Living Field Test
BODE: BODE index for COPD (Body Mass Index,
Obstruction, Dyspnoea, Exercise Capacity)
BPQ: Breathing Problems Questionnaire
CAO: Chronic airflow obstruction
COPD: Chronic Obstructive Pulmonary Disease
COPM: Canadian Occupational Performance Measure
CRQ: Chronic Respiratory Disease Questionnaire
d: day
ESWT: Endurance Shuttle Walk Test
FEV1: Forced expiratory volume in one second
FFM: Functionally active fat-free mass
GOLD: Global Initiative for Chronic Obstructive Lung Disease
HADS: Hospital Anxiety and Depression Scale
HRQL: Health – related quality of life
IMT: Inspirational muscle training
ISWT: Incremental Shuttle Walking Test
LVRS: Lung volume reduction surgery
Maugeri RFQ: Maugeri Foundation Respiratory Failure Questionnaire (MRF-28)
MCID: Minimal Clinically Important Difference
MRC: Medical Research Council
MVC: Maximal Voluntary Contraction
NETT: National Emphysema Treatment Trial
NNT: Number needed to treat
NRCT: Non – randomized controlled trial
NSD: No significant difference
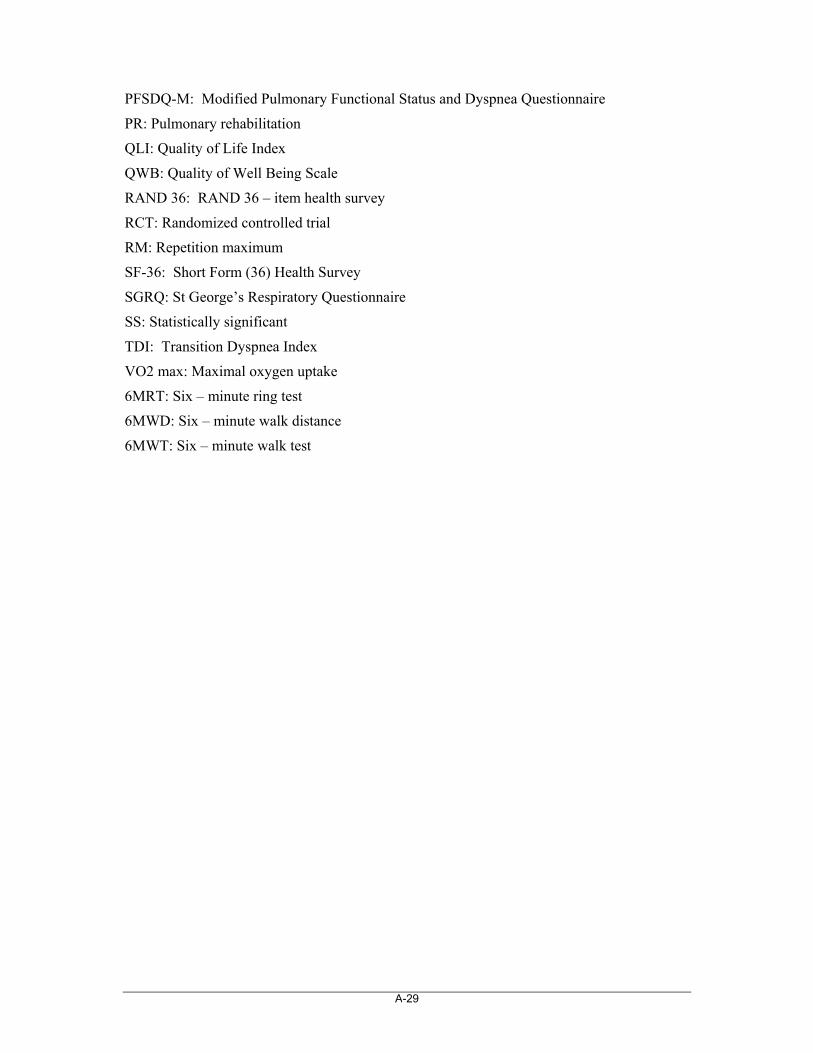
A-29
PFSDQ-M: Modified Pulmonary Functional Status and Dyspnea Questionnaire
PR: Pulmonary rehabilitation
QLI: Quality of Life Index
QWB: Quality of Well Being Scale
RAND 36: RAND 36 – item health survey
RCT: Randomized controlled trial
RM: Repetition maximum
SF-36: Short Form (36) Health Survey
SGRQ: St George’s Respiratory Questionnaire
SS: Statistically significant
TDI: Transition Dyspnea Index
VO2 max: Maximal oxygen uptake
6MRT: Six – minute ring test
6MWD: Six – minute walk distance
6MWT: Six – minute walk test
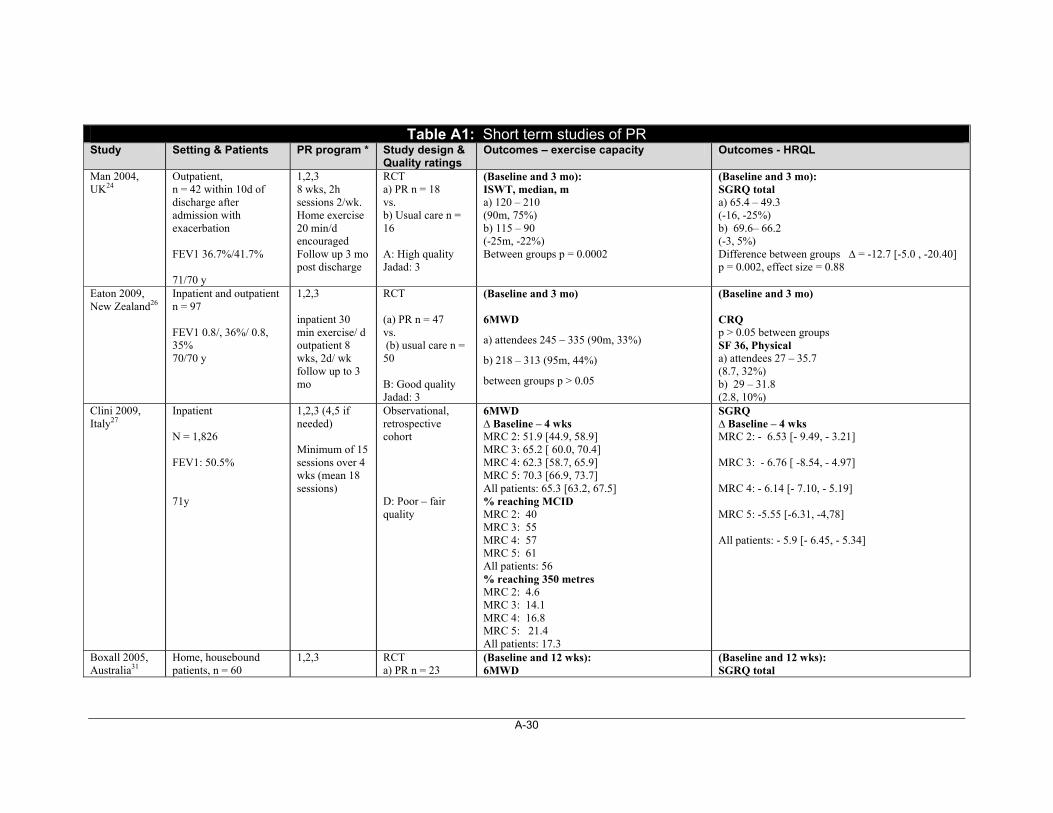
A-30
Table A1: Short term studies of PR Study Setting & Patients PR program * Study design &
Quality ratings Outcomes – exercise capacity Outcomes - HRQL
Man 2004, UK24
Outpatient, n = 42 within 10d of discharge after admission with exacerbation FEV1 36.7%/41.7% 71/70 y
1,2,3 8 wks, 2h sessions 2/wk. Home exercise 20 min/d encouraged Follow up 3 mo post discharge
RCT a) PR n = 18 vs. b) Usual care n = 16 A: High quality Jadad: 3
(Baseline and 3 mo): ISWT, median, m a) 120 – 210 (90m, 75%) b) 115 – 90 (-25m, -22%) Between groups p = 0.0002
(Baseline and 3 mo): SGRQ total a) 65.4 – 49.3 (-16, -25%) b) 69.6– 66.2 (-3, 5%) Difference between groups ∆ = -12.7 [-5.0 , -20.40] p = 0.002, effect size = 0.88
Eaton 2009, New Zealand26
Inpatient and outpatient n = 97 FEV1 0.8/, 36%/ 0.8, 35% 70/70 y
1,2,3 inpatient 30 min exercise/ d outpatient 8 wks, 2d/ wk follow up to 3 mo
RCT (a) PR n = 47 vs. (b) usual care n = 50 B: Good quality Jadad: 3
(Baseline and 3 mo) 6MWD
a) attendees 245 – 335 (90m, 33%)
b) 218 – 313 (95m, 44%)
between groups p > 0.05
(Baseline and 3 mo) CRQ p > 0.05 between groups SF 36, Physical a) attendees 27 – 35.7 (8.7, 32%) b) 29 – 31.8 (2.8, 10%)
Clini 2009, Italy27
Inpatient N = 1,826 FEV1: 50.5% 71y
1,2,3 (4,5 if needed) Minimum of 15 sessions over 4 wks (mean 18 sessions)
Observational, retrospective cohort D: Poor – fair quality
6MWD ∆ Baseline – 4 wks MRC 2: 51.9 [44.9, 58.9] MRC 3: 65.2 [ 60.0, 70.4] MRC 4: 62.3 [58.7, 65.9] MRC 5: 70.3 [66.9, 73.7] All patients: 65.3 [63.2, 67.5] % reaching MCID MRC 2: 40 MRC 3: 55 MRC 4: 57 MRC 5: 61 All patients: 56 % reaching 350 metres MRC 2: 4.6 MRC 3: 14.1 MRC 4: 16.8 MRC 5: 21.4 All patients: 17.3
SGRQ ∆ Baseline – 4 wks MRC 2: - 6.53 [- 9.49, - 3.21] MRC 3: - 6.76 [ -8.54, - 4.97] MRC 4: - 6.14 [- 7.10, - 5.19] MRC 5: -5.55 [-6.31, -4,78] All patients: - 5.9 [- 6.45, - 5.34]
Boxall 2005, Australia31
Home, housebound patients, n = 60
1,2,3
RCT a) PR n = 23
(Baseline and 12 wks): 6MWD
(Baseline and 12 wks): SGRQ total
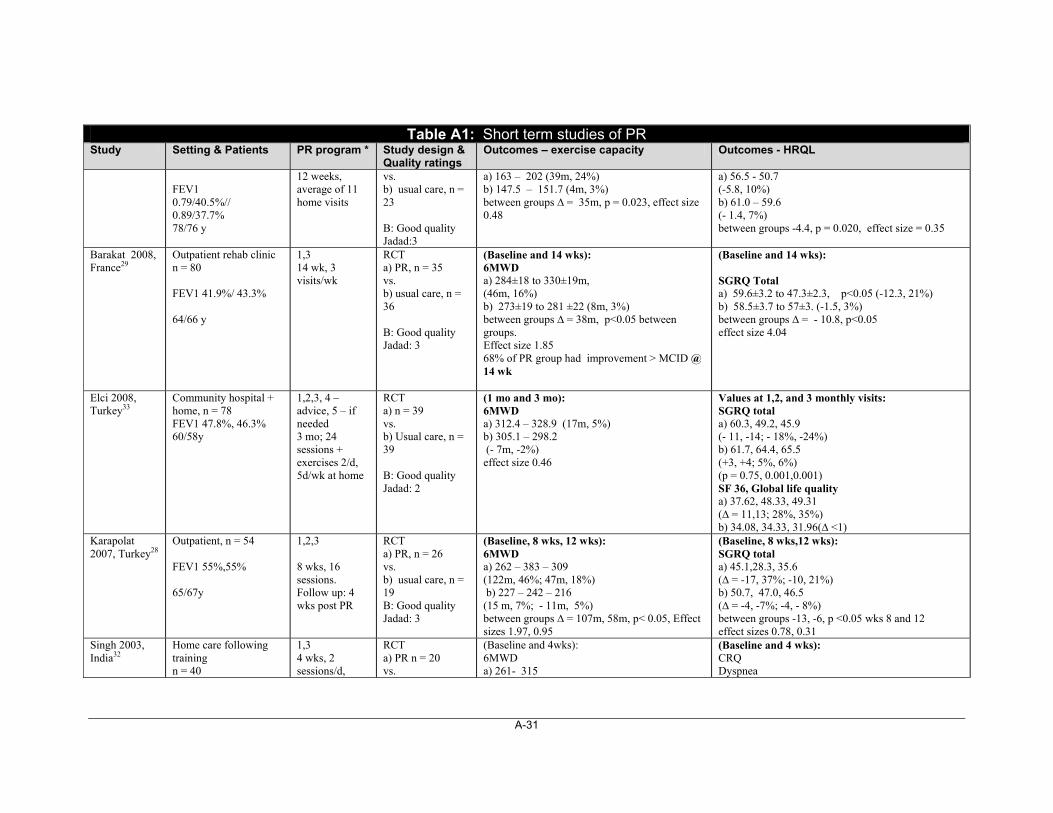
A-31
Table A1: Short term studies of PR Study Setting & Patients PR program * Study design &
Quality ratings Outcomes – exercise capacity Outcomes - HRQL
FEV1 0.79/40.5%// 0.89/37.7% 78/76 y
12 weeks, average of 11 home visits
vs. b) usual care, n = 23 B: Good quality Jadad:3
a) 163 – 202 (39m, 24%) b) 147.5 – 151.7 (4m, 3%) between groups ∆ = 35m, p = 0.023, effect size 0.48
a) 56.5 - 50.7 (-5.8, 10%) b) 61.0 – 59.6 (- 1.4, 7%) between groups -4.4, p = 0.020, effect size = 0.35
Barakat 2008, France29
Outpatient rehab clinic n = 80 FEV1 41.9%/ 43.3% 64/66 y
1,3 14 wk, 3 visits/wk
RCT a) PR, n = 35 vs. b) usual care, n = 36 B: Good quality Jadad: 3
(Baseline and 14 wks): 6MWD a) 284±18 to 330±19m, (46m, 16%) b) 273±19 to 281 ±22 (8m, 3%) between groups ∆ = 38m, p<0.05 between groups. Effect size 1.85 68% of PR group had improvement > MCID @ 14 wk
(Baseline and 14 wks): SGRQ Total a) 59.6±3.2 to 47.3±2.3, p<0.05 (-12.3, 21%) b) 58.5±3.7 to 57±3. (-1.5, 3%) between groups ∆ = - 10.8, p<0.05 effect size 4.04
Elci 2008, Turkey33
Community hospital + home, n = 78 FEV1 47.8%, 46.3% 60/58y
1,2,3, 4 – advice, 5 – if needed 3 mo; 24 sessions + exercises 2/d, 5d/wk at home
RCT a) n = 39 vs. b) Usual care, n = 39 B: Good quality Jadad: 2
(1 mo and 3 mo): 6MWD a) 312.4 – 328.9 (17m, 5%) b) 305.1 – 298.2 (- 7m, -2%) effect size 0.46
Values at 1,2, and 3 monthly visits: SGRQ total a) 60.3, 49.2, 45.9 (- 11, -14; - 18%, -24%) b) 61.7, 64.4, 65.5 (+3, +4; 5%, 6%) (p = 0.75, 0.001,0.001) SF 36, Global life quality a) 37.62, 48.33, 49.31 (∆ = 11,13; 28%, 35%) b) 34.08, 34.33, 31.96(∆ <1)
Karapolat 2007, Turkey28
Outpatient, n = 54 FEV1 55%,55% 65/67y
1,2,3 8 wks, 16 sessions. Follow up: 4 wks post PR
RCT a) PR, n = 26 vs. b) usual care, n = 19 B: Good quality Jadad: 3
(Baseline, 8 wks, 12 wks): 6MWD a) 262 – 383 – 309 (122m, 46%; 47m, 18%) b) 227 – 242 – 216 (15 m, 7%; - 11m, 5%) between groups ∆ = 107m, 58m, p< 0.05, Effect sizes 1.97, 0.95
(Baseline, 8 wks,12 wks): SGRQ total a) 45.1,28.3, 35.6 (∆ = -17, 37%; -10, 21%) b) 50.7, 47.0, 46.5 (∆ = -4, -7%; -4, - 8%) between groups -13, -6, p <0.05 wks 8 and 12 effect sizes 0.78, 0.31
Singh 2003, India32
Home care following training n = 40
1,3 4 wks, 2 sessions/d,
RCT a) PR n = 20 vs.
(Baseline and 4wks): 6MWD a) 261- 315
(Baseline and 4 wks): CRQ Dyspnea
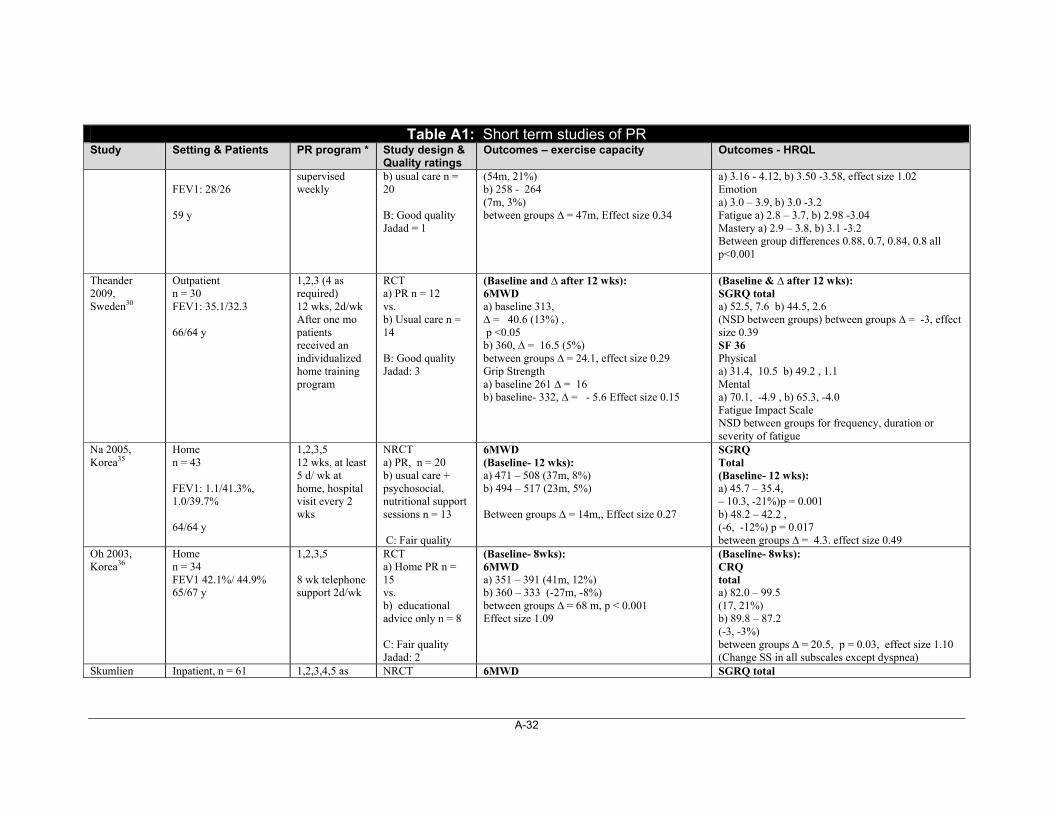
A-32
Table A1: Short term studies of PR Study Setting & Patients PR program * Study design &
Quality ratings Outcomes – exercise capacity Outcomes - HRQL
FEV1: 28/26 59 y
supervised weekly
b) usual care n = 20 B: Good quality Jadad = 1
(54m, 21%) b) 258 - 264 (7m, 3%) between groups ∆ = 47m, Effect size 0.34
a) 3.16 - 4.12, b) 3.50 -3.58, effect size 1.02 Emotion a) 3.0 – 3.9, b) 3.0 -3.2 Fatigue a) 2.8 – 3.7, b) 2.98 -3.04 Mastery a) 2.9 – 3.8, b) 3.1 -3.2 Between group differences 0.88, 0.7, 0.84, 0.8 all p<0.001
Theander 2009, Sweden30
Outpatient n = 30 FEV1: 35.1/32.3 66/64 y
1,2,3 (4 as required) 12 wks, 2d/wk After one mo patients received an individualized home training program
RCT a) PR n = 12 vs. b) Usual care n = 14 B: Good quality Jadad: 3
(Baseline and ∆ after 12 wks): 6MWD a) baseline 313, ∆ = 40.6 (13%) , p <0.05 b) 360, ∆ = 16.5 (5%) between groups ∆ = 24.1, effect size 0.29 Grip Strength a) baseline 261 ∆ = 16 b) baseline- 332, ∆ = - 5.6 Effect size 0.15
(Baseline & ∆ after 12 wks): SGRQ total a) 52.5, 7.6 b) 44.5, 2.6 (NSD between groups) between groups ∆ = -3, effect size 0.39 SF 36 Physical a) 31.4, 10.5 b) 49.2 , 1.1 Mental a) 70.1, -4.9 , b) 65.3, -4.0 Fatigue Impact Scale NSD between groups for frequency, duration or severity of fatigue
Na 2005, Korea35
Home n = 43 FEV1: 1.1/41.3%, 1.0/39.7% 64/64 y
1,2,3,5 12 wks, at least 5 d/ wk at home, hospital visit every 2 wks
NRCT a) PR, n = 20 b) usual care + psychosocial, nutritional support sessions n = 13 C: Fair quality
6MWD (Baseline- 12 wks): a) 471 – 508 (37m, 8%) b) 494 – 517 (23m, 5%) Between groups ∆ = 14m,, Effect size 0.27
SGRQ Total (Baseline- 12 wks): a) 45.7 – 35.4, – 10.3, -21%)p = 0.001 b) 48.2 – 42.2 , (-6, -12%) p = 0.017 between groups ∆ = 4.3. effect size 0.49
Oh 2003, Korea36
Home n = 34 FEV1 42.1%/ 44.9% 65/67 y
1,2,3,5 8 wk telephone support 2d/wk
RCT a) Home PR n = 15 vs. b) educational advice only n = 8 C: Fair quality Jadad: 2
(Baseline- 8wks): 6MWD a) 351 – 391 (41m, 12%) b) 360 – 333 (-27m, -8%) between groups ∆ = 68 m, p < 0.001 Effect size 1.09
(Baseline- 8wks): CRQ total a) 82.0 – 99.5 (17, 21%) b) 89.8 – 87.2 (-3, -3%) between groups ∆ = 20.5, p = 0.03, effect size 1.10 (Change SS in all subscales except dyspnea)
Skumlien Inpatient, n = 61 1,2,3,4,5 as NRCT 6MWD SGRQ total
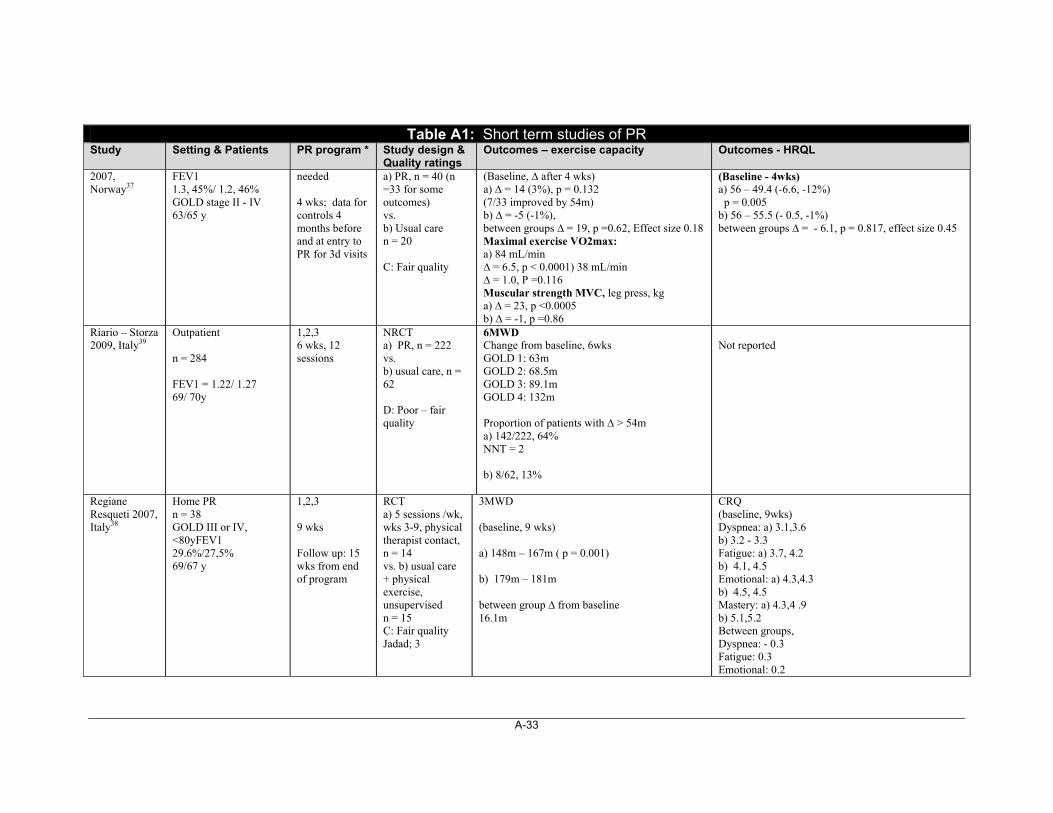
A-33
Table A1: Short term studies of PR Study Setting & Patients PR program * Study design &
Quality ratings Outcomes – exercise capacity Outcomes - HRQL
2007, Norway37
FEV1 1.3, 45%/ 1.2, 46% GOLD stage II - IV 63/65 y
needed 4 wks; data for controls 4 months before and at entry to PR for 3d visits
a) PR, n = 40 (n =33 for some outcomes) vs. b) Usual care n = 20 C: Fair quality
(Baseline, ∆ after 4 wks) a) ∆ = 14 (3%), p = 0.132 (7/33 improved by 54m) b) ∆ = -5 (-1%), between groups ∆ = 19, p =0.62, Effect size 0.18 Maximal exercise VO2max: a) 84 mL/min ∆ = 6.5, p < 0.0001) 38 mL/min ∆ = 1.0, P =0.116 Muscular strength MVC, leg press, kg a) ∆ = 23, p <0.0005 b) ∆ = -1, p =0.86
(Baseline - 4wks) a) 56 – 49.4 (-6.6, -12%) p = 0.005 b) 56 – 55.5 (- 0.5, -1%) between groups ∆ = - 6.1, p = 0.817, effect size 0.45
Riario – Storza 2009, Italy39
Outpatient n = 284 FEV1 = 1.22/ 1.27 69/ 70y
1,2,3 6 wks, 12 sessions
NRCT a) PR, n = 222 vs. b) usual care, n = 62 D: Poor – fair quality
6MWD Change from baseline, 6wks GOLD 1: 63m GOLD 2: 68.5m GOLD 3: 89.1m GOLD 4: 132m Proportion of patients with ∆ > 54m a) 142/222, 64% NNT = 2 b) 8/62, 13%
Not reported
Regiane Resqueti 2007, Italy38
Home PR n = 38 GOLD III or IV, <80yFEV1 29.6%/27,5% 69/67 y
1,2,3 9 wks Follow up: 15 wks from end of program
RCT a) 5 sessions /wk, wks 3-9, physical therapist contact, n = 14 vs. b) usual care + physical exercise, unsupervised n = 15 C: Fair quality Jadad; 3
3MWD (baseline, 9 wks) a) 148m – 167m ( p = 0.001) b) 179m – 181m between group ∆ from baseline 16.1m
CRQ (baseline, 9wks) Dyspnea: a) 3.1,3.6 b) 3.2 - 3.3 Fatigue: a) 3.7, 4.2 b) 4.1, 4.5 Emotional: a) 4.3,4.3 b) 4.5, 4.5 Mastery: a) 4.3,4 .9 b) 5.1,5.2 Between groups, Dyspnea: - 0.3 Fatigue: 0.3 Emotional: 0.2
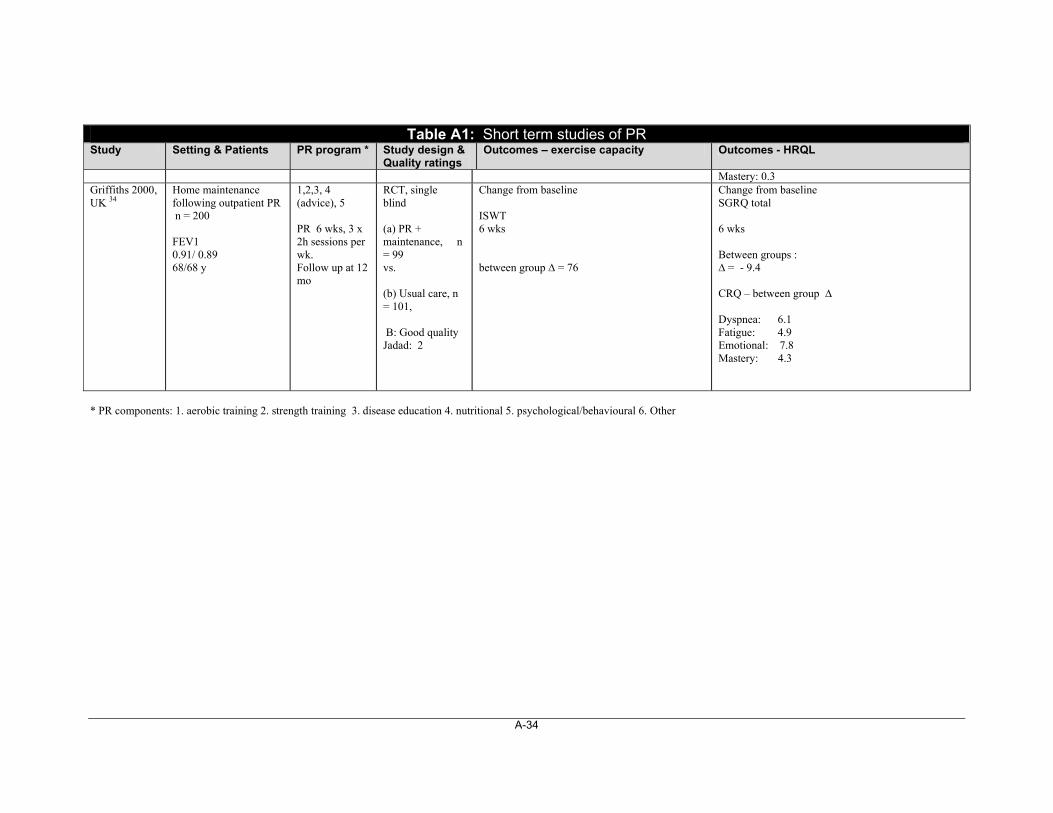
A-34
Table A1: Short term studies of PR Study Setting & Patients PR program * Study design &
Quality ratings Outcomes – exercise capacity Outcomes - HRQL
Mastery: 0.3 Griffiths 2000, UK 34
Home maintenance following outpatient PR n = 200 FEV1 0.91/ 0.89 68/68 y
1,2,3, 4 (advice), 5 PR 6 wks, 3 x 2h sessions per wk. Follow up at 12 mo
RCT, single blind (a) PR + maintenance, n = 99 vs. (b) Usual care, n = 101, B: Good quality Jadad: 2
Change from baseline ISWT 6 wks between group ∆ = 76
Change from baseline SGRQ total 6 wks Between groups : ∆ = - 9.4 CRQ – between group ∆ Dyspnea: 6.1 Fatigue: 4.9 Emotional: 7.8 Mastery: 4.3
* PR components: 1. aerobic training 2. strength training 3. disease education 4. nutritional 5. psychological/behavioural 6. Other
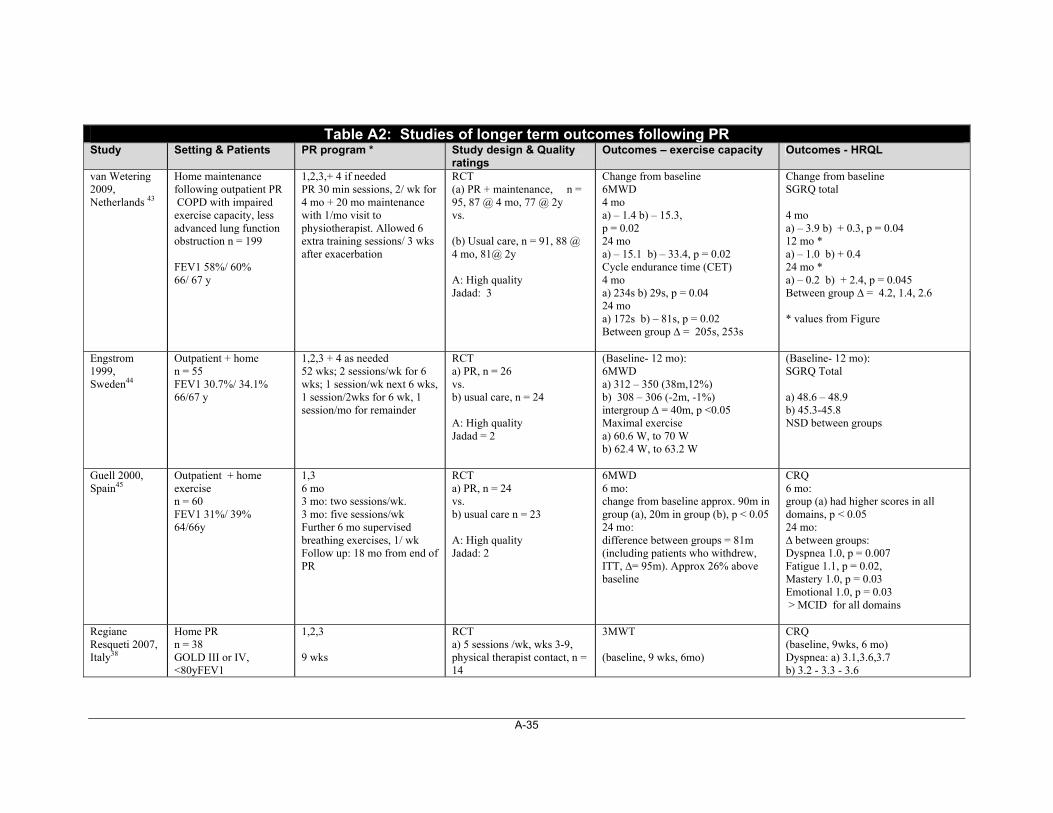
A-35
Table A2: Studies of longer term outcomes following PR Study Setting & Patients PR program * Study design & Quality
ratings Outcomes – exercise capacity
Outcomes - HRQL
van Wetering 2009, Netherlands 43
Home maintenance following outpatient PR COPD with impaired exercise capacity, less advanced lung function obstruction n = 199 FEV1 58%/ 60% 66/ 67 y
1,2,3,+ 4 if needed PR 30 min sessions, 2/ wk for 4 mo + 20 mo maintenance with 1/mo visit to physiotherapist. Allowed 6 extra training sessions/ 3 wks after exacerbation
RCT (a) PR + maintenance, n = 95, 87 @ 4 mo, 77 @ 2y vs. (b) Usual care, n = 91, 88 @ 4 mo, 81@ 2y A: High quality Jadad: 3
Change from baseline 6MWD 4 mo a) – 1.4 b) – 15.3, p = 0.02 24 mo a) – 15.1 b) – 33.4, p = 0.02 Cycle endurance time (CET) 4 mo a) 234s b) 29s, p = 0.04 24 mo a) 172s b) – 81s, p = 0.02 Between group ∆ = 205s, 253s
Change from baseline SGRQ total 4 mo a) – 3.9 b) + 0.3, p = 0.04 12 mo * a) – 1.0 b) + 0.4 24 mo * a) – 0.2 b) + 2.4, p = 0.045 Between group ∆ = 4.2, 1.4, 2.6 * values from Figure
Engstrom 1999, Sweden44
Outpatient + home n = 55 FEV1 30.7%/ 34.1% 66/67 y
1,2,3 + 4 as needed 52 wks; 2 sessions/wk for 6 wks; 1 session/wk next 6 wks, 1 session/2wks for 6 wk, 1 session/mo for remainder
RCT a) PR, n = 26 vs. b) usual care, n = 24 A: High quality Jadad = 2
(Baseline- 12 mo): 6MWD a) 312 – 350 (38m,12%) b) 308 – 306 (-2m, -1%) intergroup ∆ = 40m, p <0.05 Maximal exercise a) 60.6 W, to 70 W b) 62.4 W, to 63.2 W
(Baseline- 12 mo): SGRQ Total a) 48.6 – 48.9 b) 45.3-45.8 NSD between groups
Guell 2000, Spain45
Outpatient + home exercise n = 60 FEV1 31%/ 39% 64/66y
1,3 6 mo 3 mo: two sessions/wk. 3 mo: five sessions/wk Further 6 mo supervised breathing exercises, 1/ wk Follow up: 18 mo from end of PR
RCT a) PR, n = 24 vs. b) usual care n = 23 A: High quality Jadad: 2
6MWD 6 mo: change from baseline approx. 90m in group (a), 20m in group (b), p < 0.05 24 mo: difference between groups = 81m (including patients who withdrew, ITT, ∆= 95m). Approx 26% above baseline
CRQ 6 mo: group (a) had higher scores in all domains, p < 0.05 24 mo: ∆ between groups: Dyspnea 1.0, p = 0.007 Fatigue 1.1, p = 0.02, Mastery 1.0, p = 0.03 Emotional 1.0, p = 0.03 > MCID for all domains
Regiane Resqueti 2007, Italy38
Home PR n = 38 GOLD III or IV, <80yFEV1
1,2,3 9 wks
RCT a) 5 sessions /wk, wks 3-9, physical therapist contact, n = 14
3MWT (baseline, 9 wks, 6mo)
CRQ (baseline, 9wks, 6 mo) Dyspnea: a) 3.1,3.6,3.7 b) 3.2 - 3.3 - 3.6
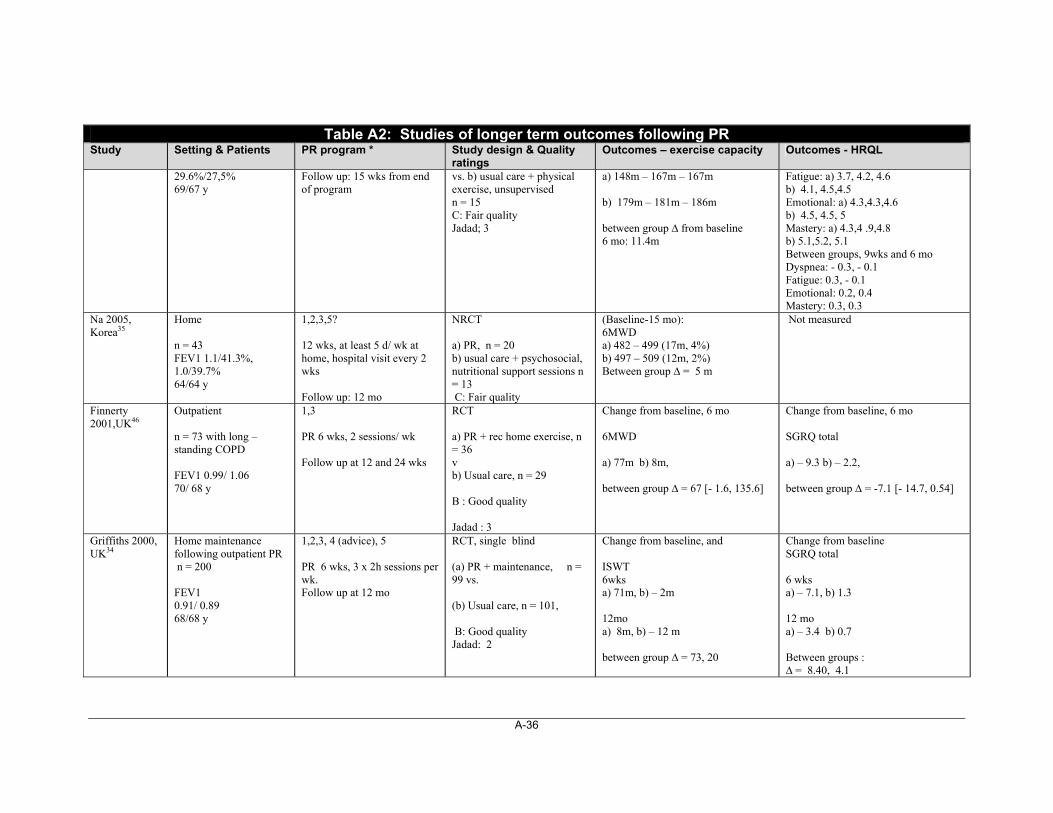
A-36
Table A2: Studies of longer term outcomes following PR Study Setting & Patients PR program * Study design & Quality
ratings Outcomes – exercise capacity
Outcomes - HRQL
29.6%/27,5% 69/67 y
Follow up: 15 wks from end of program
vs. b) usual care + physical exercise, unsupervised n = 15 C: Fair quality Jadad; 3
a) 148m – 167m – 167m b) 179m – 181m – 186m between group ∆ from baseline 6 mo: 11.4m
Fatigue: a) 3.7, 4.2, 4.6 b) 4.1, 4.5,4.5 Emotional: a) 4.3,4.3,4.6 b) 4.5, 4.5, 5 Mastery: a) 4.3,4 .9,4.8 b) 5.1,5.2, 5.1 Between groups, 9wks and 6 mo Dyspnea: - 0.3, - 0.1 Fatigue: 0.3, - 0.1 Emotional: 0.2, 0.4 Mastery: 0.3, 0.3
Na 2005, Korea35
Home n = 43 FEV1 1.1/41.3%, 1.0/39.7% 64/64 y
1,2,3,5? 12 wks, at least 5 d/ wk at home, hospital visit every 2 wks Follow up: 12 mo
NRCT a) PR, n = 20 b) usual care + psychosocial, nutritional support sessions n = 13 C: Fair quality
(Baseline-15 mo): 6MWD a) 482 – 499 (17m, 4%) b) 497 – 509 (12m, 2%) Between group ∆ = 5 m
Not measured
Finnerty 2001,UK46
Outpatient n = 73 with long – standing COPD FEV1 0.99/ 1.06 70/ 68 y
1,3 PR 6 wks, 2 sessions/ wk Follow up at 12 and 24 wks
RCT a) PR + rec home exercise, n = 36 v b) Usual care, n = 29 B : Good quality Jadad : 3
Change from baseline, 6 mo 6MWD a) 77m b) 8m, between group ∆ = 67 [- 1.6, 135.6]
Change from baseline, 6 mo SGRQ total a) – 9.3 b) – 2.2, between group ∆ = -7.1 [- 14.7, 0.54]
Griffiths 2000, UK34
Home maintenance following outpatient PR n = 200 FEV1 0.91/ 0.89 68/68 y
1,2,3, 4 (advice), 5 PR 6 wks, 3 x 2h sessions per wk. Follow up at 12 mo
RCT, single blind (a) PR + maintenance, n = 99 vs. (b) Usual care, n = 101, B: Good quality Jadad: 2
Change from baseline, and ISWT 6wks a) 71m, b) – 2m 12mo a) 8m, b) – 12 m between group ∆ = 73, 20
Change from baseline SGRQ total 6 wks a) – 7.1, b) 1.3 12 mo a) – 3.4 b) 0.7 Between groups : ∆ = 8.40, 4.1
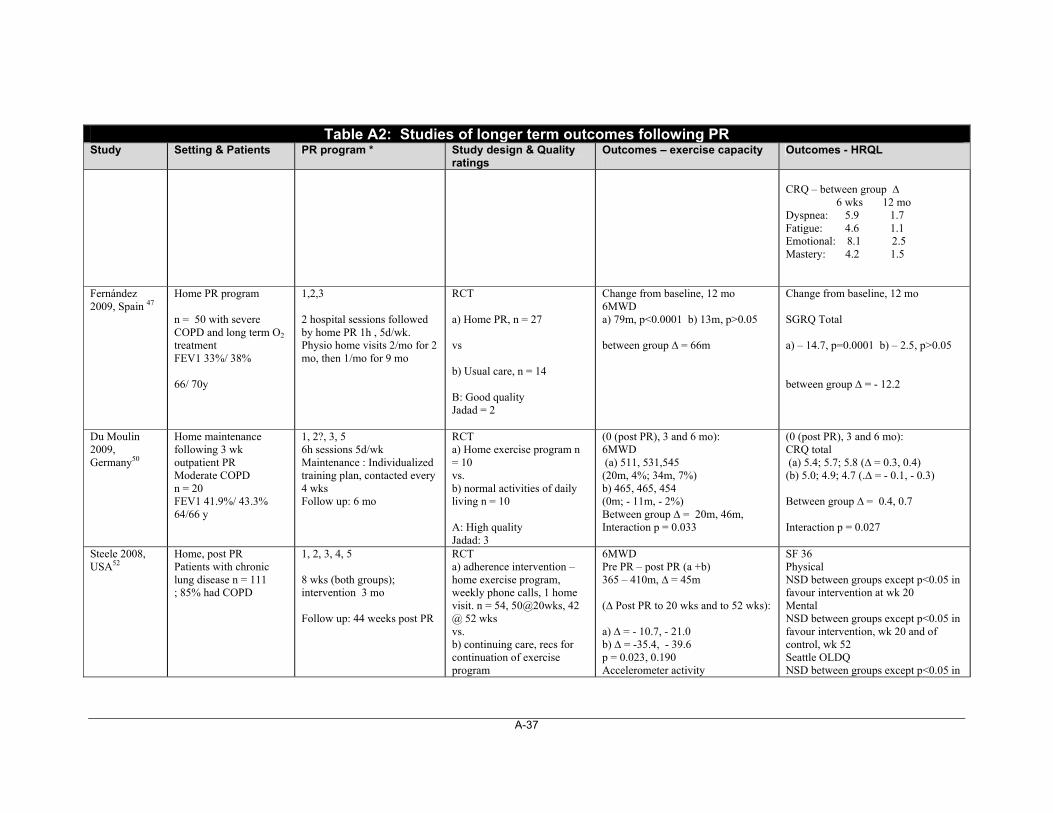
A-37
Table A2: Studies of longer term outcomes following PR Study Setting & Patients PR program * Study design & Quality
ratings Outcomes – exercise capacity
Outcomes - HRQL
CRQ – between group ∆ 6 wks 12 mo Dyspnea: 5.9 1.7 Fatigue: 4.6 1.1 Emotional: 8.1 2.5 Mastery: 4.2 1.5
Fernández 2009, Spain 47
Home PR program n = 50 with severe COPD and long term O2
treatment FEV1 33%/ 38% 66/ 70y
1,2,3 2 hospital sessions followed by home PR 1h , 5d/wk. Physio home visits 2/mo for 2 mo, then 1/mo for 9 mo
RCT a) Home PR, n = 27 vs b) Usual care, n = 14 B: Good quality Jadad = 2
Change from baseline, 12 mo 6MWD a) 79m, p<0.0001 b) 13m, p>0.05 between group ∆ = 66m
Change from baseline, 12 mo SGRQ Total a) – 14.7, p=0.0001 b) – 2.5, p>0.05 between group ∆ = - 12.2
Du Moulin 2009, Germany50
Home maintenance following 3 wk outpatient PR Moderate COPD n = 20 FEV1 41.9%/ 43.3% 64/66 y
1, 2?, 3, 5 6h sessions 5d/wk Maintenance : Individualized training plan, contacted every 4 wks Follow up: 6 mo
RCT a) Home exercise program n = 10 vs. b) normal activities of daily living n = 10 A: High quality Jadad: 3
(0 (post PR), 3 and 6 mo): 6MWD (a) 511, 531,545 (20m, 4%; 34m, 7%) b) 465, 465, 454 (0m; - 11m, - 2%) Between group ∆ = 20m, 46m, Interaction p = 0.033
(0 (post PR), 3 and 6 mo): CRQ total (a) 5.4; 5.7; 5.8 (∆ = 0.3, 0.4) (b) 5.0; 4.9; 4.7 (.∆ = - 0.1, - 0.3) Between group ∆ = 0.4, 0.7 Interaction p = 0.027
Steele 2008, USA52
Home, post PR Patients with chronic lung disease n = 111 ; 85% had COPD
1, 2, 3, 4, 5 8 wks (both groups); intervention 3 mo Follow up: 44 weeks post PR
RCT a) adherence intervention – home exercise program, weekly phone calls, 1 home visit. n = 54, 50@20wks, 42 @ 52 wks vs. b) continuing care, recs for continuation of exercise program
6MWD Pre PR – post PR (a +b) 365 – 410m, ∆ = 45m (∆ Post PR to 20 wks and to 52 wks): a) ∆ = - 10.7, - 21.0 b) ∆ = -35.4, - 39.6 p = 0.023, 0.190 Accelerometer activity
SF 36 Physical NSD between groups except p<0.05 in favour intervention at wk 20 Mental NSD between groups except p<0.05 in favour intervention, wk 20 and of control, wk 52 Seattle OLDQ NSD between groups except p<0.05 in
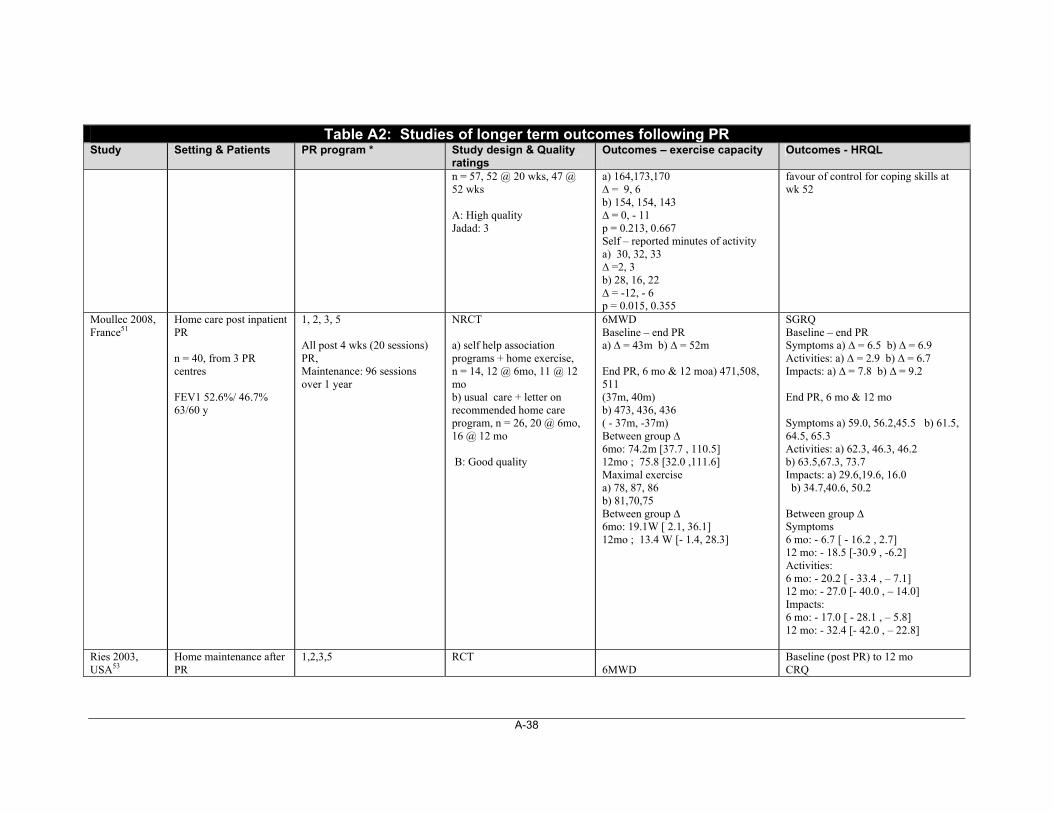
A-38
Table A2: Studies of longer term outcomes following PR Study Setting & Patients PR program * Study design & Quality
ratings Outcomes – exercise capacity
Outcomes - HRQL
n = 57, 52 @ 20 wks, 47 @ 52 wks A: High quality Jadad: 3
a) 164,173,170 ∆ = 9, 6 b) 154, 154, 143 ∆ = 0, - 11 p = 0.213, 0.667 Self – reported minutes of activity a) 30, 32, 33 ∆ =2, 3 b) 28, 16, 22 ∆ = -12, - 6 p = 0.015, 0.355
favour of control for coping skills at wk 52
Moullec 2008, France51
Home care post inpatient PR n = 40, from 3 PR centres FEV1 52.6%/ 46.7% 63/60 y
1, 2, 3, 5 All post 4 wks (20 sessions) PR, Maintenance: 96 sessions over 1 year
NRCT a) self help association programs + home exercise, n = 14, 12 @ 6mo, 11 @ 12 mo b) usual care + letter on recommended home care program, n = 26, 20 @ 6mo, 16 @ 12 mo B: Good quality
6MWD Baseline – end PR a) ∆ = 43m b) ∆ = 52m End PR, 6 mo & 12 moa) 471,508, 511 (37m, 40m) b) 473, 436, 436 ( - 37m, -37m) Between group ∆ 6mo: 74.2m [37.7 , 110.5] 12mo ; 75.8 [32.0 ,111.6] Maximal exercise a) 78, 87, 86 b) 81,70,75 Between group ∆ 6mo: 19.1W [ 2.1, 36.1] 12mo ; 13.4 W [- 1.4, 28.3]
SGRQ Baseline – end PR Symptoms a) ∆ = 6.5 b) ∆ = 6.9 Activities: a) ∆ = 2.9 b) ∆ = 6.7 Impacts: a) ∆ = 7.8 b) ∆ = 9.2 End PR, 6 mo & 12 mo Symptoms a) 59.0, 56.2,45.5 b) 61.5, 64.5, 65.3 Activities: a) 62.3, 46.3, 46.2 b) 63.5,67.3, 73.7 Impacts: a) 29.6,19.6, 16.0 b) 34.7,40.6, 50.2 Between group ∆ Symptoms 6 mo: - 6.7 [ - 16.2 , 2.7] 12 mo: - 18.5 [-30.9 , -6.2] Activities: 6 mo: - 20.2 [ - 33.4 , – 7.1] 12 mo: - 27.0 [- 40.0 , – 14.0] Impacts: 6 mo: - 17.0 [ - 28.1 , – 5.8] 12 mo: - 32.4 [- 42.0 , – 22.8]
Ries 2003, USA53
Home maintenance after PR
1,2,3,5
RCT
6MWD
Baseline (post PR) to 12 mo CRQ
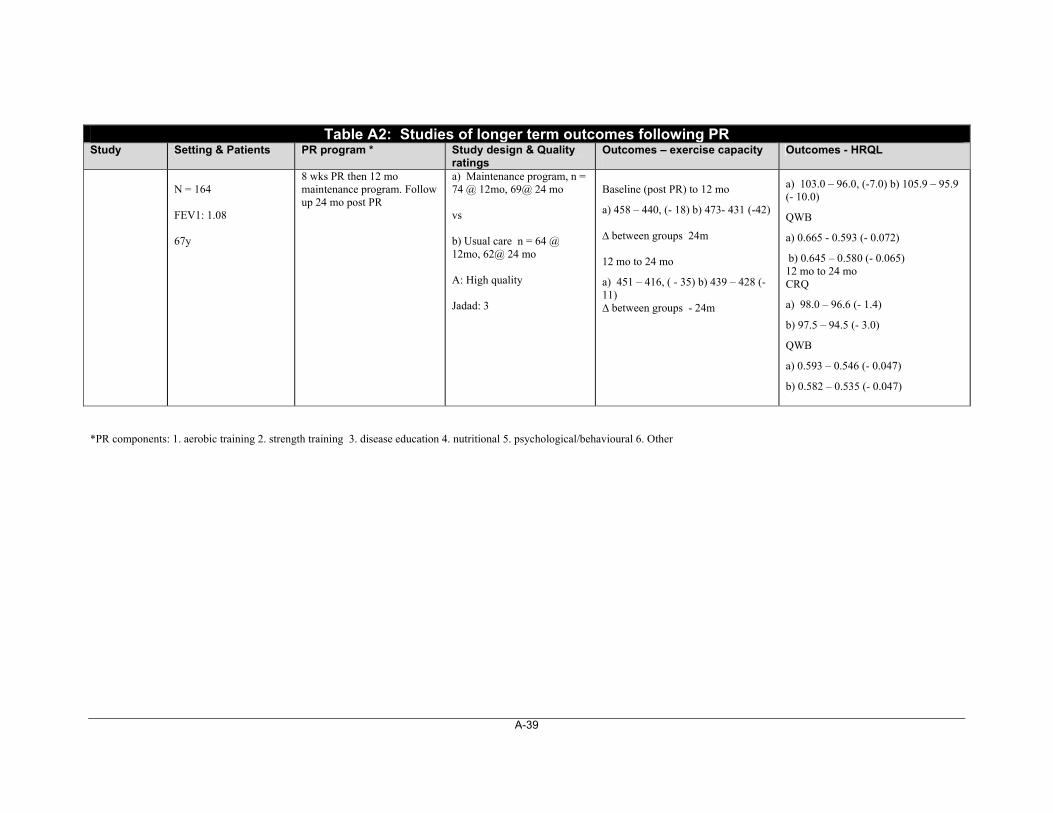
A-39
Table A2: Studies of longer term outcomes following PR Study Setting & Patients PR program * Study design & Quality
ratings Outcomes – exercise capacity
Outcomes - HRQL
N = 164 FEV1: 1.08 67y
8 wks PR then 12 mo maintenance program. Follow up 24 mo post PR
a) Maintenance program, n = 74 @ 12mo, 69@ 24 mo vs b) Usual care n = 64 @ 12mo, 62@ 24 mo A: High quality Jadad: 3
Baseline (post PR) to 12 mo
a) 458 – 440, (- 18) b) 473- 431 (-42) ∆ between groups 24m 12 mo to 24 mo
a) 451 – 416, ( - 35) b) 439 – 428 (-11) ∆ between groups - 24m
a) 103.0 – 96.0, (-7.0) b) 105.9 – 95.9 (- 10.0)
QWB
a) 0.665 - 0.593 (- 0.072)
b) 0.645 – 0.580 (- 0.065) 12 mo to 24 mo CRQ
a) 98.0 – 96.6 (- 1.4)
b) 97.5 – 94.5 (- 3.0)
QWB
a) 0.593 – 0.546 (- 0.047)
b) 0.582 – 0.535 (- 0.047)
*PR components: 1. aerobic training 2. strength training 3. disease education 4. nutritional 5. psychological/behavioural 6. Other
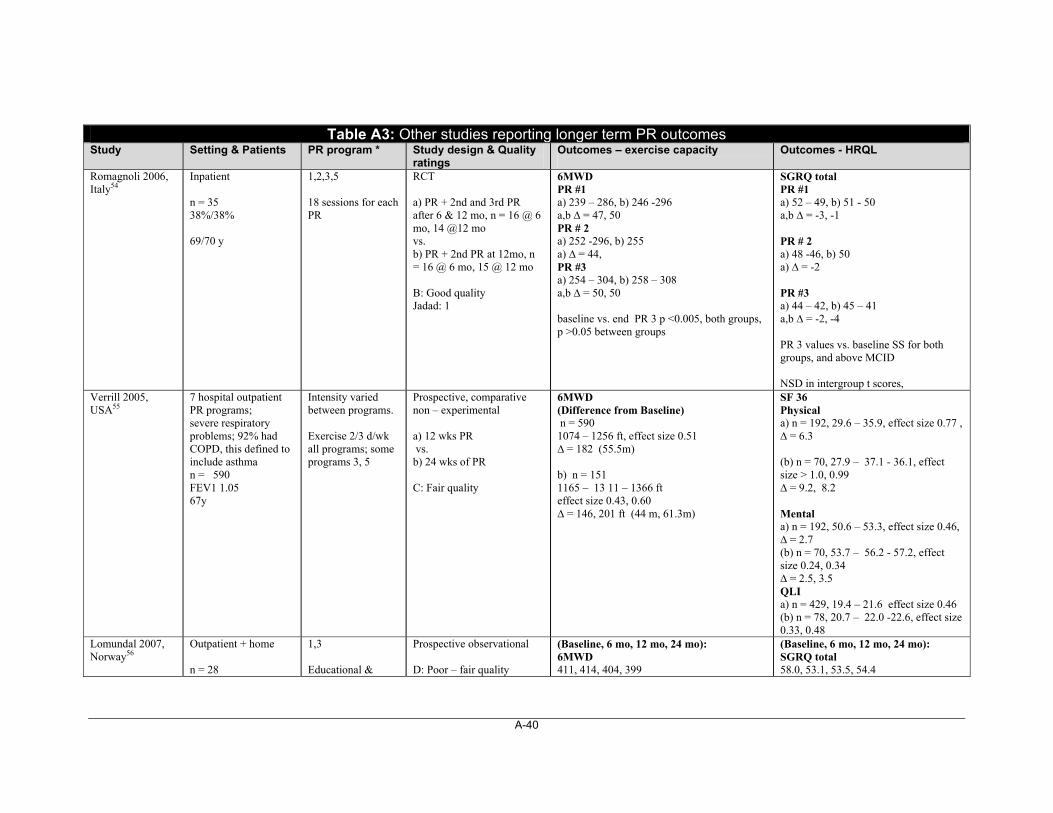
A-40
Table A3: Other studies reporting longer term PR outcomes Study Setting & Patients PR program * Study design & Quality
ratings Outcomes – exercise capacity
Outcomes - HRQL
Romagnoli 2006, Italy54
Inpatient n = 35 38%/38% 69/70 y
1,2,3,5 18 sessions for each PR
RCT a) PR + 2nd and 3rd PR after 6 & 12 mo, n = 16 @ 6 mo, 14 @12 mo vs. b) PR + 2nd PR at 12mo, n = 16 @ 6 mo, 15 @ 12 mo B: Good quality Jadad: 1
6MWD PR #1 a) 239 – 286, b) 246 -296 a,b ∆ = 47, 50 PR # 2 a) 252 -296, b) 255 a) ∆ = 44, PR #3 a) 254 – 304, b) 258 – 308 a,b ∆ = 50, 50 baseline vs. end PR 3 p <0.005, both groups, p >0.05 between groups
SGRQ total PR #1 a) 52 – 49, b) 51 - 50 a,b ∆ = -3, -1 PR # 2 a) 48 -46, b) 50 a) ∆ = -2 PR #3 a) 44 – 42, b) 45 – 41 a,b ∆ = -2, -4 PR 3 values vs. baseline SS for both groups, and above MCID NSD in intergroup t scores,
Verrill 2005, USA55
7 hospital outpatient PR programs; severe respiratory problems; 92% had COPD, this defined to include asthma n = 590 FEV1 1.05 67y
Intensity varied between programs. Exercise 2/3 d/wk all programs; some programs 3, 5
Prospective, comparative non – experimental a) 12 wks PR vs. b) 24 wks of PR C: Fair quality
6MWD (Difference from Baseline) n = 590 1074 – 1256 ft, effect size 0.51 ∆ = 182 (55.5m) b) n = 151 1165 – 13 11 – 1366 ft effect size 0.43, 0.60 ∆ = 146, 201 ft (44 m, 61.3m)
SF 36 Physical a) n = 192, 29.6 – 35.9, effect size 0.77 , ∆ = 6.3 (b) n = 70, 27.9 – 37.1 - 36.1, effect size > 1.0, 0.99 ∆ = 9.2, 8.2 Mental a) n = 192, 50.6 – 53.3, effect size 0.46, ∆ = 2.7 (b) n = 70, 53.7 – 56.2 - 57.2, effect size 0.24, 0.34 ∆ = 2.5, 3.5 QLI a) n = 429, 19.4 – 21.6 effect size 0.46 (b) n = 78, 20.7 – 22.0 -22.6, effect size 0.33, 0.48
Lomundal 2007, Norway56
Outpatient + home n = 28
1,3 Educational &
Prospective observational D: Poor – fair quality
(Baseline, 6 mo, 12 mo, 24 mo): 6MWD 411, 414, 404, 399
(Baseline, 6 mo, 12 mo, 24 mo): SGRQ total 58.0, 53.1, 53.5, 54.4
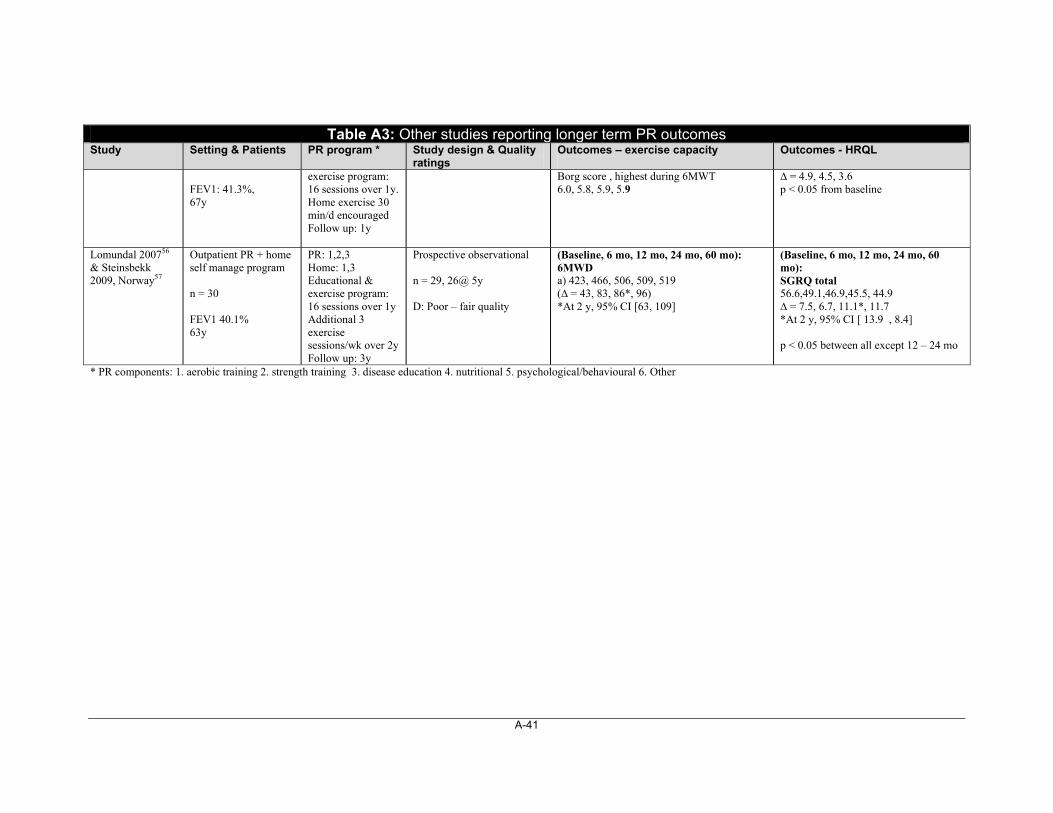
A-41
Table A3: Other studies reporting longer term PR outcomes Study Setting & Patients PR program * Study design & Quality
ratings Outcomes – exercise capacity
Outcomes - HRQL
FEV1: 41.3%, 67y
exercise program: 16 sessions over 1y. Home exercise 30 min/d encouraged Follow up: 1y
Borg score , highest during 6MWT 6.0, 5.8, 5.9, 5.9
∆ = 4.9, 4.5, 3.6 p < 0.05 from baseline
Lomundal 200756 & Steinsbekk 2009, Norway57
Outpatient PR + home self manage program n = 30 FEV1 40.1% 63y
PR: 1,2,3 Home: 1,3 Educational & exercise program: 16 sessions over 1y Additional 3 exercise sessions/wk over 2y Follow up: 3y
Prospective observational n = 29, 26@ 5y D: Poor – fair quality
(Baseline, 6 mo, 12 mo, 24 mo, 60 mo): 6MWD a) 423, 466, 506, 509, 519 (∆ = 43, 83, 86*, 96) *At 2 y, 95% CI [63, 109]
(Baseline, 6 mo, 12 mo, 24 mo, 60 mo): SGRQ total 56.6,49.1,46.9,45.5, 44.9 ∆ = 7.5, 6.7, 11.1*, 11.7 *At 2 y, 95% CI [ 13.9 , 8.4] p < 0.05 between all except 12 – 24 mo
* PR components: 1. aerobic training 2. strength training 3. disease education 4. nutritional 5. psychological/behavioural 6. Other
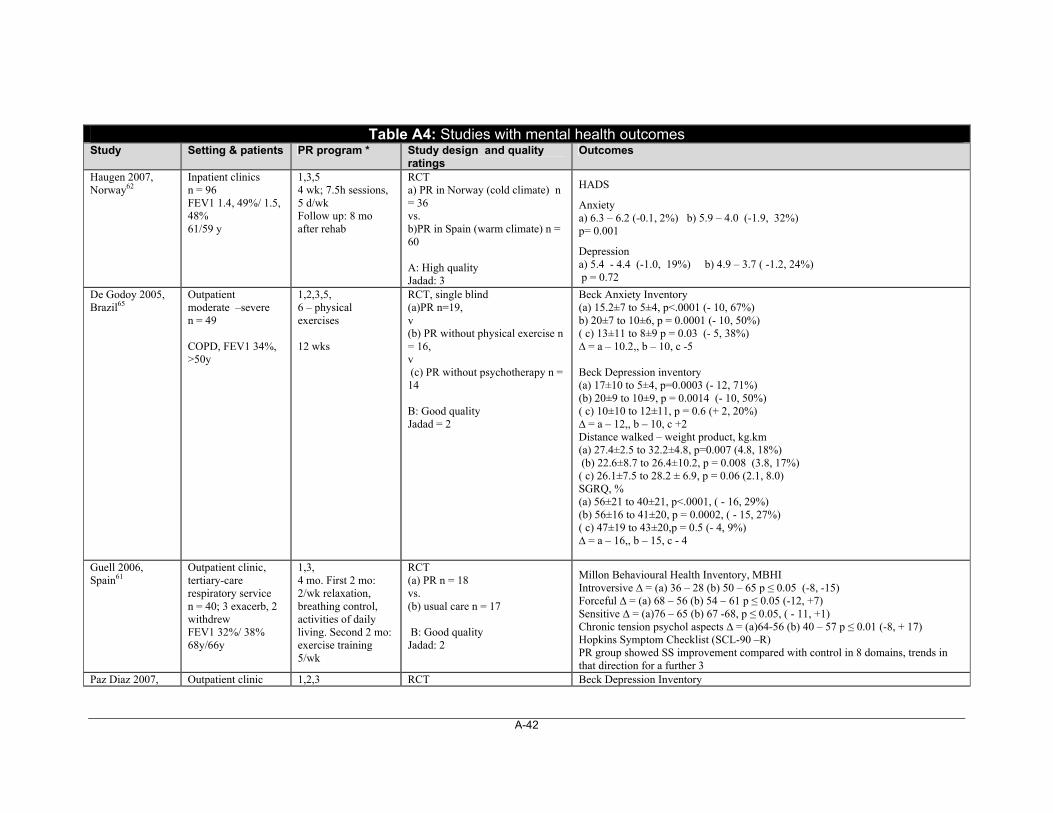
A-42
Table A4: Studies with mental health outcomes Study Setting & patients PR program * Study design and quality
ratings Outcomes
Haugen 2007, Norway62
Inpatient clinics n = 96 FEV1 1.4, 49%/ 1.5, 48% 61/59 y
1,3,5 4 wk; 7.5h sessions, 5 d/wk Follow up: 8 mo after rehab
RCT a) PR in Norway (cold climate) n = 36 vs. b)PR in Spain (warm climate) n = 60 A: High quality Jadad: 3
HADS
Anxiety a) 6.3 – 6.2 (-0.1, 2%) b) 5.9 – 4.0 (-1.9, 32%) p= 0.001
Depression a) 5.4 - 4.4 (-1.0, 19%) b) 4.9 – 3.7 ( -1.2, 24%) p = 0.72
De Godoy 2005, Brazil65
Outpatient moderate –severe n = 49 COPD, FEV1 34%, >50y
1,2,3,5, 6 – physical exercises 12 wks
RCT, single blind (a)PR n=19, v (b) PR without physical exercise n = 16, v (c) PR without psychotherapy n = 14 B: Good quality Jadad = 2
Beck Anxiety Inventory (a) 15.2±7 to 5±4, p<.0001 (- 10, 67%) b) 20±7 to 10±6, p = 0.0001 (- 10, 50%) ( c) 13±11 to 8±9 p = 0.03 (- 5, 38%) ∆ = a – 10.2,, b – 10, c -5 Beck Depression inventory (a) 17±10 to 5±4, p=0.0003 (- 12, 71%) (b) 20±9 to 10±9, p = 0.0014 (- 10, 50%) ( c) 10±10 to 12±11, p = 0.6 (+ 2, 20%) ∆ = a – 12,, b – 10, c +2 Distance walked – weight product, kg.km (a) 27.4±2.5 to 32.2±4.8, p=0.007 (4.8, 18%) (b) 22.6±8.7 to 26.4±10.2, p = 0.008 (3.8, 17%) ( c) 26.1±7.5 to 28.2 ± 6.9, p = 0.06 (2.1, 8.0) SGRQ, % (a) 56±21 to 40±21, p<.0001, ( - 16, 29%) (b) 56±16 to 41±20, p = 0.0002, ( - 15, 27%) ( c) 47±19 to 43±20,p = 0.5 (- 4, 9%) ∆ = a – 16,, b – 15, c - 4
Guell 2006, Spain61
Outpatient clinic, tertiary-care respiratory service n = 40; 3 exacerb, 2 withdrew FEV1 32%/ 38% 68y/66y
1,3, 4 mo. First 2 mo: 2/wk relaxation, breathing control, activities of daily living. Second 2 mo: exercise training 5/wk
RCT (a) PR n = 18 vs. (b) usual care n = 17 B: Good quality Jadad: 2
Millon Behavioural Health Inventory, MBHI Introversive ∆ = (a) 36 – 28 (b) 50 – 65 p ≤ 0.05 (-8, -15) Forceful ∆ = (a) 68 – 56 (b) 54 – 61 p ≤ 0.05 (-12, +7) Sensitive ∆ = (a)76 – 65 (b) 67 -68, p ≤ 0.05, ( - 11, +1) Chronic tension psychol aspects ∆ = (a)64-56 (b) 40 – 57 p ≤ 0.01 (-8, + 17) Hopkins Symptom Checklist (SCL-90 –R) PR group showed SS improvement compared with control in 8 domains, trends in that direction for a further 3
Paz Diaz 2007, Outpatient clinic 1,2,3 RCT Beck Depression Inventory
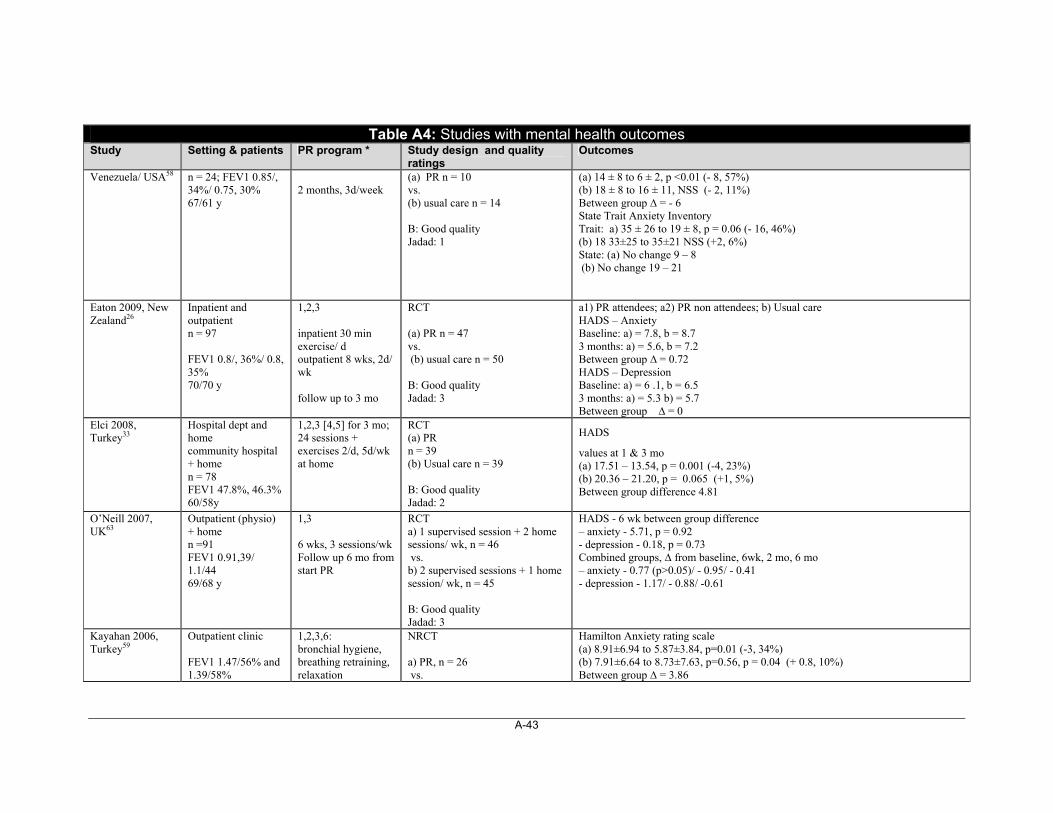
A-43
Table A4: Studies with mental health outcomes Study Setting & patients PR program * Study design and quality
ratings Outcomes
Venezuela/ USA58
n = 24; FEV1 0.85/, 34%/ 0.75, 30% 67/61 y
2 months, 3d/week
(a) PR n = 10 vs. (b) usual care n = 14 B: Good quality Jadad: 1
(a) 14 ± 8 to 6 ± 2, p <0.01 (- 8, 57%) (b) 18 ± 8 to 16 ± 11, NSS (- 2, 11%) Between group ∆ = - 6 State Trait Anxiety Inventory Trait: a) 35 ± 26 to 19 ± 8, p = 0.06 (- 16, 46%) (b) 18 33±25 to 35±21 NSS (+2, 6%) State: (a) No change 9 – 8 (b) No change 19 – 21
Eaton 2009, New Zealand26
Inpatient and outpatient n = 97 FEV1 0.8/, 36%/ 0.8, 35% 70/70 y
1,2,3 inpatient 30 min exercise/ d outpatient 8 wks, 2d/ wk follow up to 3 mo
RCT (a) PR n = 47 vs. (b) usual care n = 50 B: Good quality Jadad: 3
a1) PR attendees; a2) PR non attendees; b) Usual care HADS – Anxiety Baseline: a) = 7.8, b = 8.7 3 months: a) = 5.6, b = 7.2 Between group ∆ = 0.72 HADS – Depression Baseline: a) = 6 .1, b = 6.5 3 months: a) = 5.3 b) = 5.7 Between group ∆ = 0
Elci 2008, Turkey33
Hospital dept and home community hospital + home n = 78 FEV1 47.8%, 46.3% 60/58y
1,2,3 [4,5] for 3 mo; 24 sessions + exercises 2/d, 5d/wk at home
RCT (a) PR n = 39 (b) Usual care n = 39 B: Good quality Jadad: 2
HADS
values at 1 & 3 mo (a) 17.51 – 13.54, p = 0.001 (-4, 23%) (b) 20.36 – 21.20, p = 0.065 (+1, 5%) Between group difference 4.81
O’Neill 2007, UK63
Outpatient (physio) + home n =91 FEV1 0.91,39/ 1.1/44 69/68 y
1,3 6 wks, 3 sessions/wk Follow up 6 mo from start PR
RCT a) 1 supervised session + 2 home sessions/ wk, n = 46 vs. b) 2 supervised sessions + 1 home session/ wk, n = 45 B: Good quality Jadad: 3
HADS - 6 wk between group difference – anxiety - 5.71, p = 0.92 - depression - 0.18, p = 0.73 Combined groups, ∆ from baseline, 6wk, 2 mo, 6 mo – anxiety - 0.77 (p>0.05)/ - 0.95/ - 0.41 - depression - 1.17/ - 0.88/ -0.61
Kayahan 2006, Turkey59
Outpatient clinic FEV1 1.47/56% and 1.39/58%
1,2,3,6: bronchial hygiene, breathing retraining, relaxation
NRCT a) PR, n = 26 vs.
Hamilton Anxiety rating scale (a) 8.91±6.94 to 5.87±3.84, p=0.01 (-3, 34%) (b) 7.91±6.64 to 8.73±7.63, p=0.56, p = 0.04 (+ 0.8, 10%) Between group ∆ = 3.86
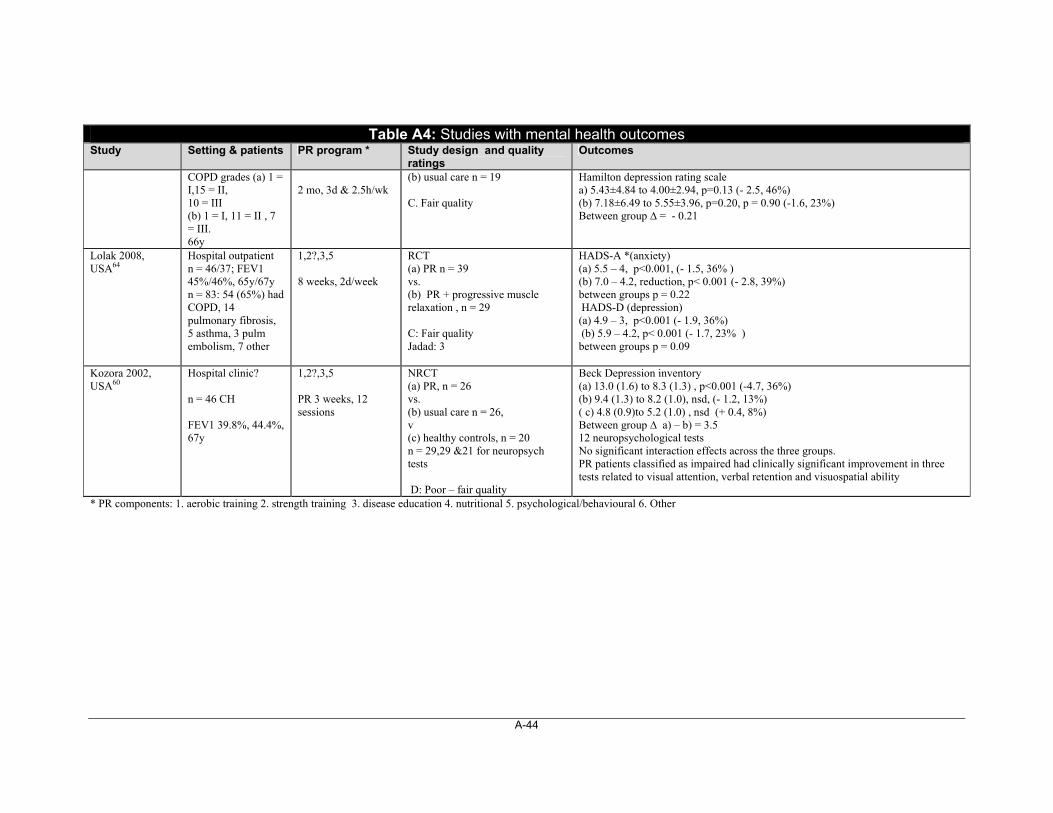
A-44
Table A4: Studies with mental health outcomes Study Setting & patients PR program * Study design and quality
ratings Outcomes
COPD grades (a) 1 = I,15 = II, 10 = III (b) 1 = I, 11 = II , 7 = III. 66y
2 mo, 3d & 2.5h/wk
(b) usual care n = 19 C. Fair quality
Hamilton depression rating scale a) 5.43±4.84 to 4.00±2.94, p=0.13 (- 2.5, 46%) (b) 7.18±6.49 to 5.55±3.96, p=0.20, p = 0.90 (-1.6, 23%) Between group ∆ = - 0.21
Lolak 2008, USA64
Hospital outpatient n = 46/37; FEV1 45%/46%, 65y/67y n = 83: 54 (65%) had COPD, 14 pulmonary fibrosis, 5 asthma, 3 pulm embolism, 7 other
1,2?,3,5 8 weeks, 2d/week
RCT (a) PR n = 39 vs. (b) PR + progressive muscle relaxation , n = 29 C: Fair quality Jadad: 3
HADS-A *(anxiety) (a) 5.5 – 4, p<0.001, (- 1.5, 36% ) (b) 7.0 – 4.2, reduction, p< 0.001 (- 2.8, 39%) between groups p = 0.22 HADS-D (depression) (a) 4.9 – 3, p<0.001 (- 1.9, 36%) (b) 5.9 – 4.2, p< 0.001 (- 1.7, 23% ) between groups p = 0.09
Kozora 2002, USA60
Hospital clinic? n = 46 CH FEV1 39.8%, 44.4%, 67y
1,2?,3,5 PR 3 weeks, 12 sessions
NRCT (a) PR, n = 26 vs. (b) usual care n = 26, v (c) healthy controls, n = 20 n = 29,29 &21 for neuropsych tests D: Poor – fair quality
Beck Depression inventory (a) 13.0 (1.6) to 8.3 (1.3) , p<0.001 (-4.7, 36%) (b) 9.4 (1.3) to 8.2 (1.0), nsd, (- 1.2, 13%) ( c) 4.8 (0.9)to 5.2 (1.0) , nsd (+ 0.4, 8%) Between group ∆ a) – b) = 3.5 12 neuropsychological tests No significant interaction effects across the three groups. PR patients classified as impaired had clinically significant improvement in three tests related to visual attention, verbal retention and visuospatial ability
* PR components: 1. aerobic training 2. strength training 3. disease education 4. nutritional 5. psychological/behavioural 6. Other
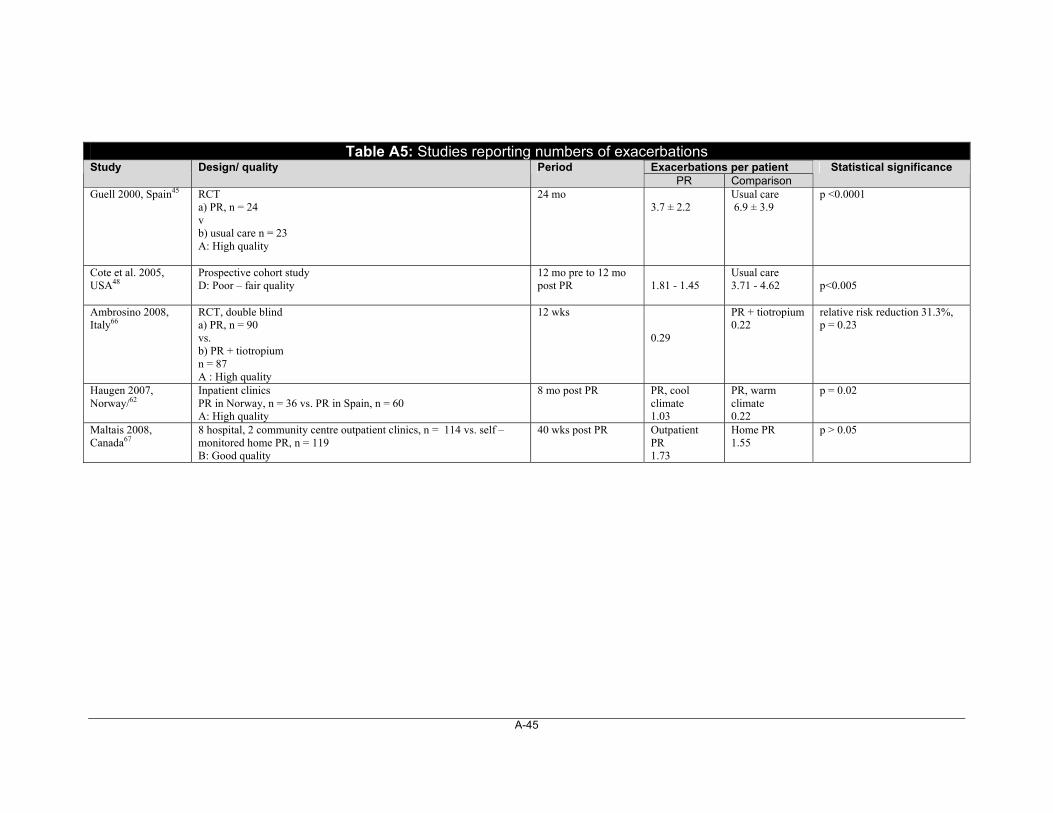
A-45
Table A5: Studies reporting numbers of exacerbations
Exacerbations per patient Study Design/ quality Period PR Comparison
Statistical significance
Guell 2000, Spain45 RCT a) PR, n = 24 v b) usual care n = 23 A: High quality
24 mo 3.7 ± 2.2
Usual care 6.9 ± 3.9
p <0.0001
Cote et al. 2005, USA48
Prospective cohort study D: Poor – fair quality
12 mo pre to 12 mo post PR
1.81 - 1.45
Usual care 3.71 - 4.62
p<0.005
Ambrosino 2008, Italy66
RCT, double blind a) PR, n = 90 vs. b) PR + tiotropium n = 87 A : High quality
12 wks 0.29
PR + tiotropium 0.22
relative risk reduction 31.3%, p = 0.23
Haugen 2007, Norway/62
Inpatient clinics PR in Norway, n = 36 vs. PR in Spain, n = 60 A: High quality
8 mo post PR PR, cool climate 1.03
PR, warm climate 0.22
p = 0.02
Maltais 2008, Canada67
8 hospital, 2 community centre outpatient clinics, n = 114 vs. self – monitored home PR, n = 119 B: Good quality
40 wks post PR Outpatient PR 1.73
Home PR 1.55
p > 0.05

A-46
Table A6: Studies that included hospitalization data Hospital admissions/ patient Hospital days/ patient Study Comparison and data Quality Period PR Non - PR PR Non - PR
Other
Eaton 2009, New Zealand26
PR v usual care, patients admitted with exacerbations. COPD – related readmissions
B: Good 3 mo 0.23 0.32 1.7 4.2 NSD between groups
Man 2004, UK24
Patients admitted with exacerbations. COPD – related readmissions PR v usual care
A: High 3 mo 0.35 0.59 4.8 7.7 p = 0.30, 0.21
Guell 200045 PR v usual care A: High 24 mo 0.6 1.3 p = 0.57 Griffiths 2000, UK 34
PR v usual care B: Good 12 mo Respiratory – related: 1.4 All causes: 1.7
1.9 2.2
Respiratory. – related: 9.4 All causes: 10.4
18.1 20.0
p = 0.044, 0.048 p = 0.021, 0.022
Raskin 2006, USA68
Post PR vs. pre PR, 11 centres All admissions
D: Poor - fair
12 mo Respiratory – related: 0.18 All causes: 0.40
0.35 0.65
Respiratory – related: 2.26 All causes: 1.98
3.24 4.16
p = 0.008, 0.016 p = 0.017, 0.150
Californian PRCG 2004, USA69
Post PR vs. pre PR, 9 centres All admissions, self – reported data
E: Poor 12 mo 3.4 10.0 p < 0.05
Lomundal 2007,56 Steinsbekk 2009,57
Post PR vs. pre PR, maintenance study, admissions due to exacerbations
D: Poor - fair
12- 36 mo
0.3 0.7
1.4 4.3
p < 0.05, > 0.05
Lomundal 200756
Post PR vs. pre PR, self management study, admissions due to exacerbations
D: Poor - fair
24 mo 0.8 0.8 3.8 4.0 p > 0.05, > 0.05
Moullec 2008, France51
Post PR vs. pre PR; PR + self help associations v usual care. Self reported data
B: Good 12 mo Respiratory – related: 3.0 –0.0 All causes: 3.5 – 1.5
2.7 – 6.4 5.6 – 7.9
p < 0.03
Cote 2005, USA48
PR v usual care, Post PR vs. pre PR COPD – related admissions
D: Poor - fair
12 mo 0.49 – 0.26 0.56 – 0.42 1.81 – 1.45 3.71 – 4.62 p <0.005
Ambrosino 200866
PR v PR + tiotropium A: High 3 mo 0.05 0.02
Wittmann 2007, Germany70
PR vs. PR + behaviour training. Pre PR vs. post PR. COPD – related admissions, data from surveys
B: Good 12 mo 0.25 – 0.12 0.31 – 0.10

A-47
Table A7: Comparison of PR and pharmacological therapy
Study Setting & Patients
PR program * Study design & Quality ratings
Outcomes
Ambrosino 2008, Italy66
12 pulmonary units with PR n = 234 FEV1 1.1, 40%/ 1.1/ 43% 67/68 y
1, 3 8 wks (5 wk prior PR) Follow up 12 wks no PR, still treated with drug/placebo
RCT, double blind a) PR, n = 90 vs. b) PR + tiotropium n = 87 A : High quality Jadad : 3
Exercise capacity (6MWD) Baseline, start PR , end PR, follow up; a) 402, 411,444, 440 b) 405, 424,451, 434 ∆ from start PR (a) 33, 29 (b) 27, 10 NSD between groups HRQL _SGRQ total Baseline, start PR, end PR, follow up: (a) 39.1, 37.0, 33.1, 33.1 (b) 39.1, 35.6, 30.9, 31.8 ∆ from start PR (a) - 3.9, -3.9 (b) - 4.7, -3.8, Dyspnea, TDI a) 2.25, b) 3.60 a) 2.1 b) 2.4
Casaburi 2005, USA71
17 sites providing PR n = 108 FEV1 0.94/36.2/ 0.82/32.6 67/66 y
1, 2? 8 wks (following 5 wks run in with drug) Follow up 12 wks
RCT, double blind a) PR, n = 44 vs. b) PR + tiotropium n = 47 A : High quality Jadad : 3
Maximal exercise (treadmill/cycle ergometer),
Endurance time, min-
Baseline -end PR – end follow up
a) 10.5, 16.5,15.8
b) 12.1, 21.9,22.4
Between group ∆
End PR: 5.35 [0.69 , 10.00]
End follow up: 6.60 [1.15 ,12.02]
HRQL _SGRQ total Baseline - end PR – follow up a) ∆ = - 3.41, - 1.63 b) ∆ = - 7.27, - 6.06
Between group ∆
Baseline - end PR: 3.86
End PR - end follow up: 4.43
Lindsay 2005, PRC – Hong Kong73
Outpatient n = 50 FEV1 0.9/0.8 70/70 y
1,3,5 PR 6 wks, 1d/wk (6wk run in prior to PR) Follow up 12 wks (?post PR)
RCT a) PR + tiotropium 18μ/d , n = 25 vs. b) tiotropium only n = 25 D : Poor to fair quality Jadad: 1
Exercise capacity 6MWD baseline - end PR a) ∆ = 22.98 b) ∆ = 30.80 baseline - 3mo a) ∆ = 11.28 b) ∆ = 36.68 HRQL - CRQ baseline - end PR – 3 mo Dyspnea (a) ∆ = 1.18, 0.99 ; (b) ∆ = 1.12, 1.08 Fatigue (a) ∆ = 0.41, 0.51 ; b) ∆ = 0.40, 0.43 Emotion (a) ∆ = 0.38, 0.42 b) ∆ = 0.28, 0.36 Mastery (a) ∆ = 0.34, 0.49 (b) 0.34, 0.41 NSD between groups
* PR components: 1. aerobic training 2. strength training 3. disease education 4. nutritional 5. psychological/behavioural 6. Other
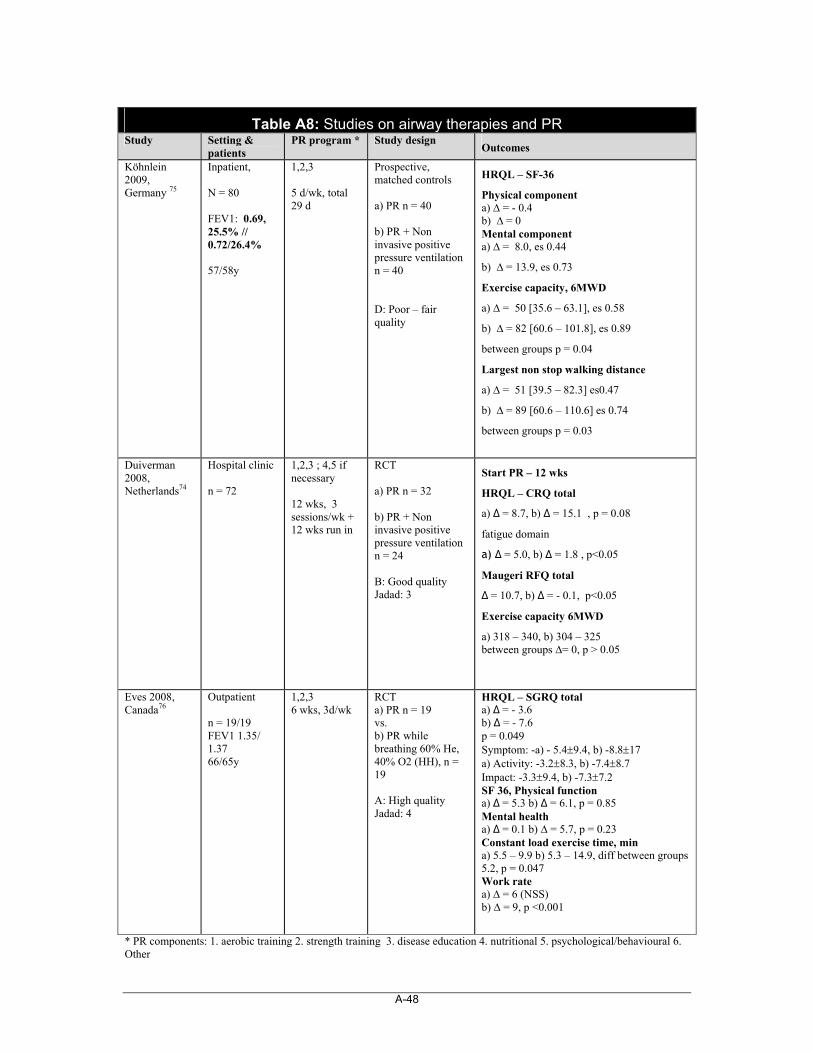
A-48
Table A8: Studies on airway therapies and PR Study Setting &
patients PR program * Study design
Outcomes
Köhnlein 2009, Germany 75
Inpatient, N = 80 FEV1: 0.69, 25.5% // 0.72/26.4% 57/58y
1,2,3 5 d/wk, total 29 d
Prospective, matched controls a) PR n = 40 b) PR + Non invasive positive pressure ventilation n = 40 D: Poor – fair quality
HRQL – SF-36
Physical component a) ∆ = - 0.4 b) ∆ = 0 Mental component a) ∆ = 8.0, es 0.44
b) ∆ = 13.9, es 0.73
Exercise capacity, 6MWD
a) ∆ = 50 [35.6 – 63.1], es 0.58
b) ∆ = 82 [60.6 – 101.8], es 0.89
between groups p = 0.04
Largest non stop walking distance
a) ∆ = 51 [39.5 – 82.3] es0.47
b) ∆ = 89 [60.6 – 110.6] es 0.74
between groups p = 0.03
Duiverman 2008, Netherlands74
Hospital clinic n = 72
1,2,3 ; 4,5 if necessary 12 wks, 3 sessions/wk + 12 wks run in
RCT a) PR n = 32 b) PR + Non invasive positive pressure ventilation n = 24 B: Good quality Jadad: 3
Start PR – 12 wks
HRQL – CRQ total
a) ∆ = 8.7, b) ∆ = 15.1 , p = 0.08
fatigue domain
a) ∆ = 5.0, b) ∆ = 1.8 , p<0.05
Maugeri RFQ total
∆ = 10.7, b) ∆ = - 0.1, p<0.05
Exercise capacity 6MWD
a) 318 – 340, b) 304 – 325 between groups ∆= 0, p > 0.05
Eves 2008, Canada76
Outpatient n = 19/19 FEV1 1.35/ 1.37 66/65y
1,2,3 6 wks, 3d/wk
RCT a) PR n = 19 vs. b) PR while breathing 60% He, 40% O2 (HH), n = 19 A: High quality Jadad: 4
HRQL – SGRQ total a) ∆ = - 3.6 b) ∆ = - 7.6 p = 0.049 Symptom: -a) - 5.49.4, b) -8.817 a) Activity: -3.28.3, b) -7.48.7 Impact: -3.39.4, b) -7.37.2 SF 36, Physical function a) ∆ = 5.3 b) ∆ = 6.1, p = 0.85 Mental health a) ∆ = 0.1 b) ∆ = 5.7, p = 0.23 Constant load exercise time, min a) 5.5 – 9.9 b) 5.3 – 14.9, diff between groups 5.2, p = 0.047 Work rate a) ∆ = 6 (NSS) b) ∆ = 9, p <0.001
* PR components: 1. aerobic training 2. strength training 3. disease education 4. nutritional 5. psychological/behavioural 6. Other
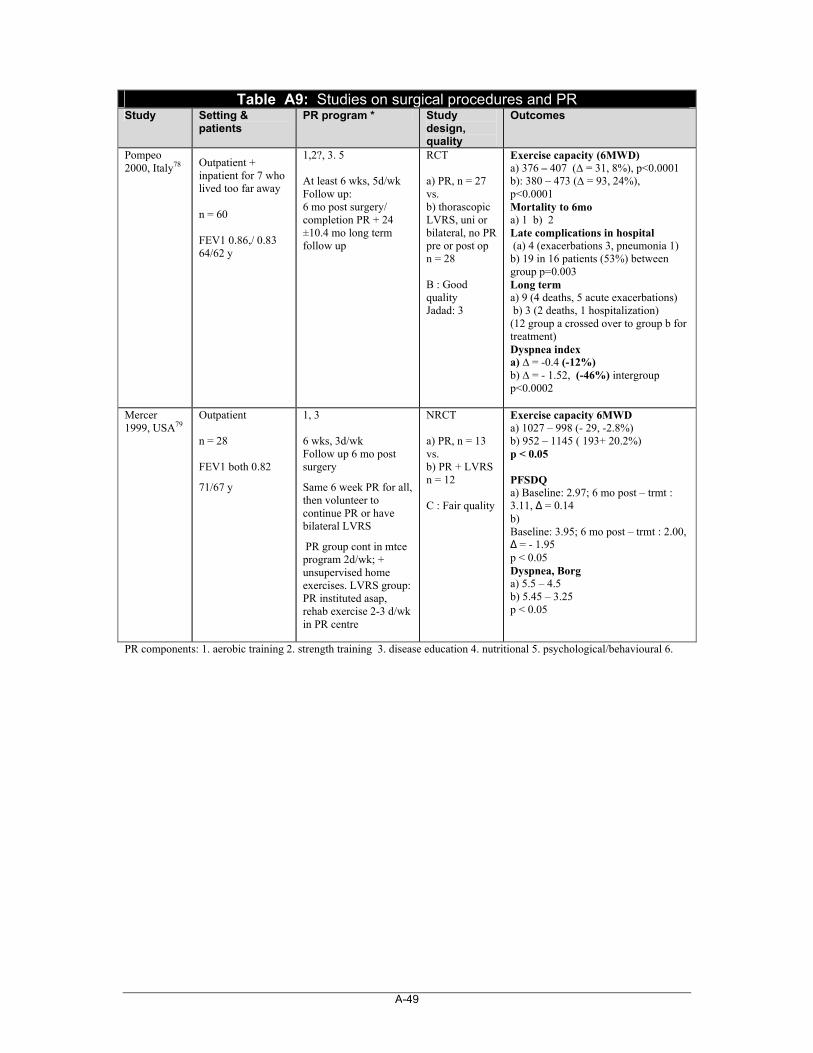
A-49
Table A9: Studies on surgical procedures and PR Study Setting &
patients PR program * Study
design, quality
Outcomes
Pompeo 2000, Italy78 Outpatient +
inpatient for 7 who lived too far away n = 60 FEV1 0.86,/ 0.83 64/62 y
1,2?, 3. 5 At least 6 wks, 5d/wk Follow up: 6 mo post surgery/ completion PR + 24 ±10.4 mo long term follow up
RCT a) PR, n = 27 vs. b) thorascopic LVRS, uni or bilateral, no PR pre or post op n = 28 B : Good quality Jadad: 3
Exercise capacity (6MWD) a) 376 – 407 (∆ = 31, 8%), p<0.0001 b): 380 – 473 (∆ = 93, 24%), p<0.0001 Mortality to 6mo a) 1 b) 2 Late complications in hospital (a) 4 (exacerbations 3, pneumonia 1) b) 19 in 16 patients (53%) between group p=0.003 Long term a) 9 (4 deaths, 5 acute exacerbations) b) 3 (2 deaths, 1 hospitalization) (12 group a crossed over to group b for treatment) Dyspnea index a) ∆ = -0.4 (-12%) b) ∆ = - 1.52, (-46%) intergroup p<0.0002
Mercer 1999, USA79
Outpatient n = 28 FEV1 both 0.82
71/67 y
1, 3 6 wks, 3d/wk Follow up 6 mo post surgery
Same 6 week PR for all, then volunteer to continue PR or have bilateral LVRS
PR group cont in mtce program 2d/wk; + unsupervised home exercises. LVRS group: PR instituted asap, rehab exercise 2-3 d/wk in PR centre
NRCT a) PR, n = 13 vs. b) PR + LVRS n = 12 C : Fair quality
Exercise capacity 6MWD a) 1027 – 998 (- 29, -2.8%) b) 952 – 1145 ( 193+ 20.2%) p < 0.05 PFSDQ a) Baseline: 2.97; 6 mo post – trmt : 3.11, ∆ = 0.14 b) Baseline: 3.95; 6 mo post – trmt : 2.00, ∆ = - 1.95 p < 0.05 Dyspnea, Borg a) 5.5 – 4.5 b) 5.45 – 3.25 p < 0.05
PR components: 1. aerobic training 2. strength training 3. disease education 4. nutritional 5. psychological/behavioural 6.
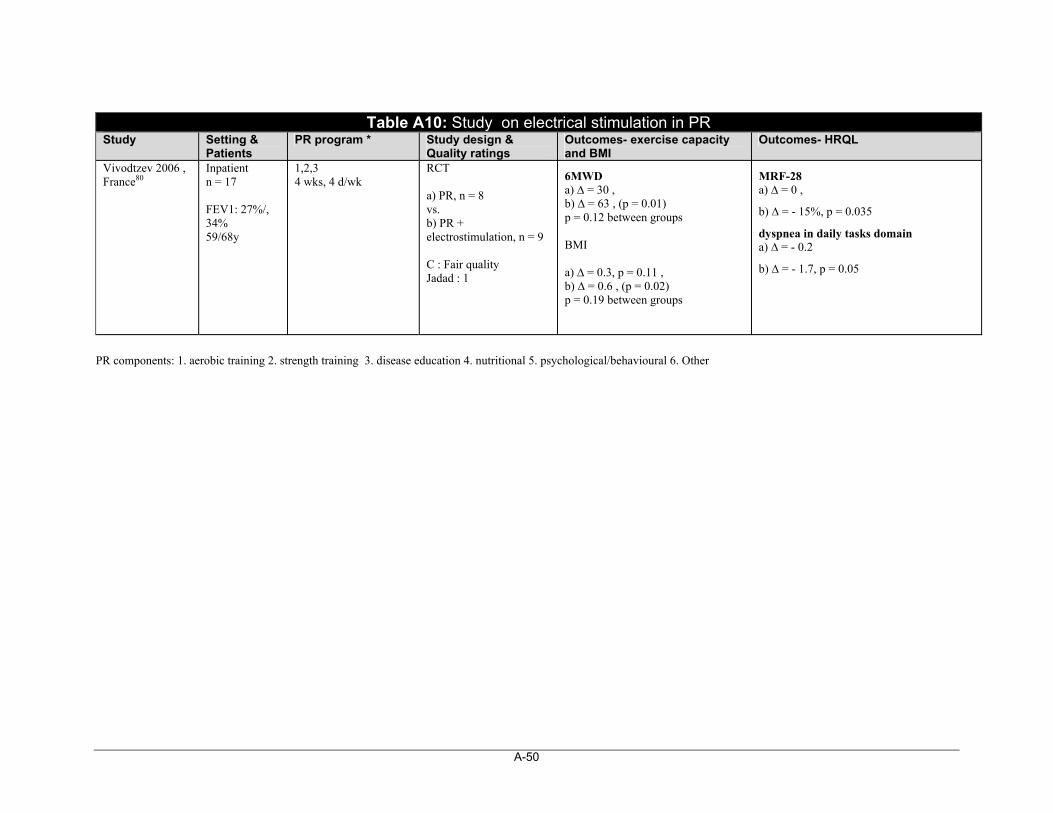
A-50
PR components: 1. aerobic training 2. strength training 3. disease education 4. nutritional 5. psychological/behavioural 6. Other
Table A10: Study on electrical stimulation in PR Study Setting &
Patients PR program * Study design &
Quality ratings Outcomes- exercise capacity and BMI
Outcomes- HRQL
Vivodtzev 2006 , France80
Inpatient n = 17 FEV1: 27%/, 34% 59/68y
1,2,3 4 wks, 4 d/wk
RCT a) PR, n = 8 vs. b) PR + electrostimulation, n = 9 C : Fair quality Jadad : 1
6MWD a) ∆ = 30 , b) ∆ = 63 , (p = 0.01) p = 0.12 between groups BMI a) ∆ = 0.3, p = 0.11 , b) ∆ = 0.6 , (p = 0.02) p = 0.19 between groups
MRF-28 a) ∆ = 0 ,
b) ∆ = - 15%, p = 0.035
dyspnea in daily tasks domain a) ∆ = - 0.2
b) ∆ = - 1.7, p = 0.05
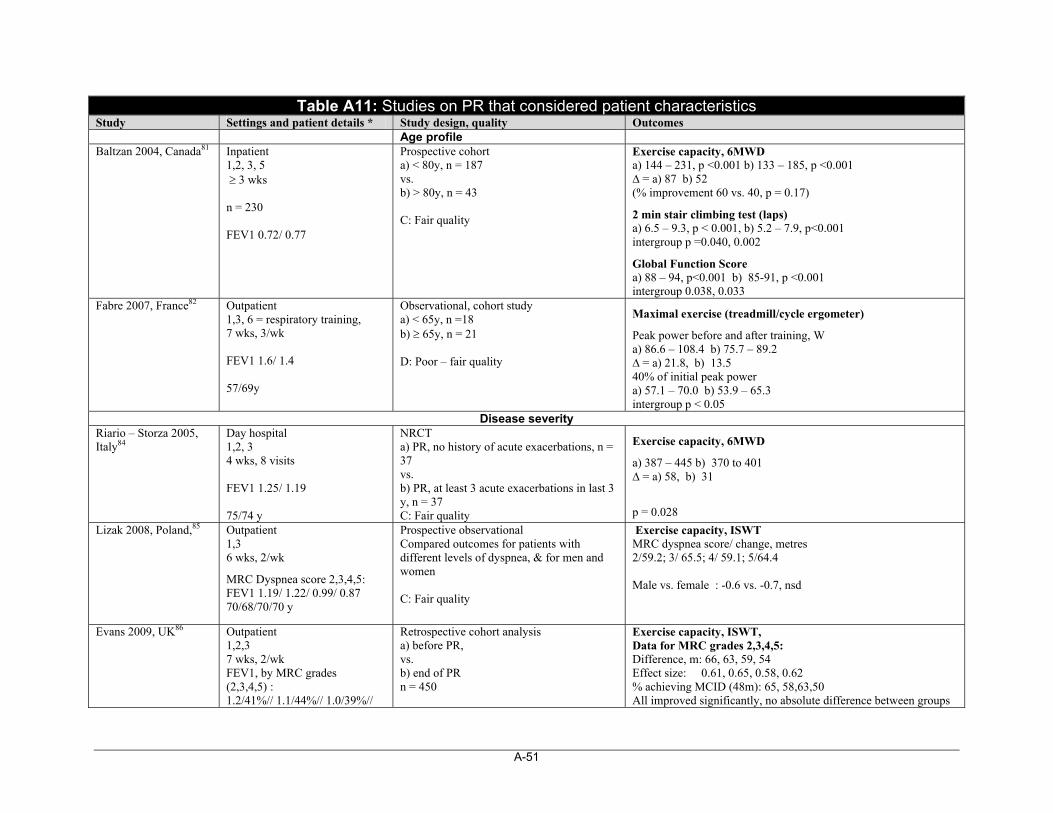
A-51
Table A11: Studies on PR that considered patient characteristics Study Settings and patient details * Study design, quality Outcomes Age profile Baltzan 2004, Canada81 Inpatient
1,2, 3, 5 3 wks n = 230 FEV1 0.72/ 0.77
Prospective cohort a) < 80y, n = 187 vs. b) > 80y, n = 43 C: Fair quality
Exercise capacity, 6MWD a) 144 – 231, p <0.001 b) 133 – 185, p <0.001 ∆ = a) 87 b) 52 (% improvement 60 vs. 40, p = 0.17)
2 min stair climbing test (laps) a) 6.5 – 9.3, p < 0.001, b) 5.2 – 7.9, p<0.001 intergroup p =0.040, 0.002
Global Function Score a) 88 – 94, p<0.001 b) 85-91, p <0.001 intergroup 0.038, 0.033
Fabre 2007, France82 Outpatient 1,3, 6 = respiratory training, 7 wks, 3/wk FEV1 1.6/ 1.4 57/69y
Observational, cohort study a) < 65y, n =18 b) 65y, n = 21 D: Poor – fair quality
Maximal exercise (treadmill/cycle ergometer)
Peak power before and after training, W a) 86.6 – 108.4 b) 75.7 – 89.2 ∆ = a) 21.8, b) 13.5 40% of initial peak power a) 57.1 – 70.0 b) 53.9 – 65.3 intergroup p < 0.05
Disease severity Riario – Storza 2005, Italy84
Day hospital 1,2, 3 4 wks, 8 visits FEV1 1.25/ 1.19 75/74 y
NRCT a) PR, no history of acute exacerbations, n = 37 vs. b) PR, at least 3 acute exacerbations in last 3 y, n = 37 C: Fair quality
Exercise capacity, 6MWD
a) 387 – 445 b) 370 to 401 ∆ = a) 58, b) 31
p = 0.028
Lizak 2008, Poland,85 Outpatient 1,3 6 wks, 2/wk
MRC Dyspnea score 2,3,4,5: FEV1 1.19/ 1.22/ 0.99/ 0.87 70/68/70/70 y
Prospective observational Compared outcomes for patients with different levels of dyspnea, & for men and women C: Fair quality
Exercise capacity, ISWT MRC dyspnea score/ change, metres 2/59.2; 3/ 65.5; 4/ 59.1; 5/64.4 Male vs. female : -0.6 vs. -0.7, nsd
Evans 2009, UK86 Outpatient
1,2,3 7 wks, 2/wk FEV1, by MRC grades (2,3,4,5) : 1.2/41%// 1.1/44%// 1.0/39%//
Retrospective cohort analysis a) before PR, vs. b) end of PR n = 450
Exercise capacity, ISWT, Data for MRC grades 2,3,4,5: Difference, m: 66, 63, 59, 54 Effect size: 0.61, 0.65, 0.58, 0.62 % achieving MCID (48m): 65, 58,63,50 All improved significantly, no absolute difference between groups
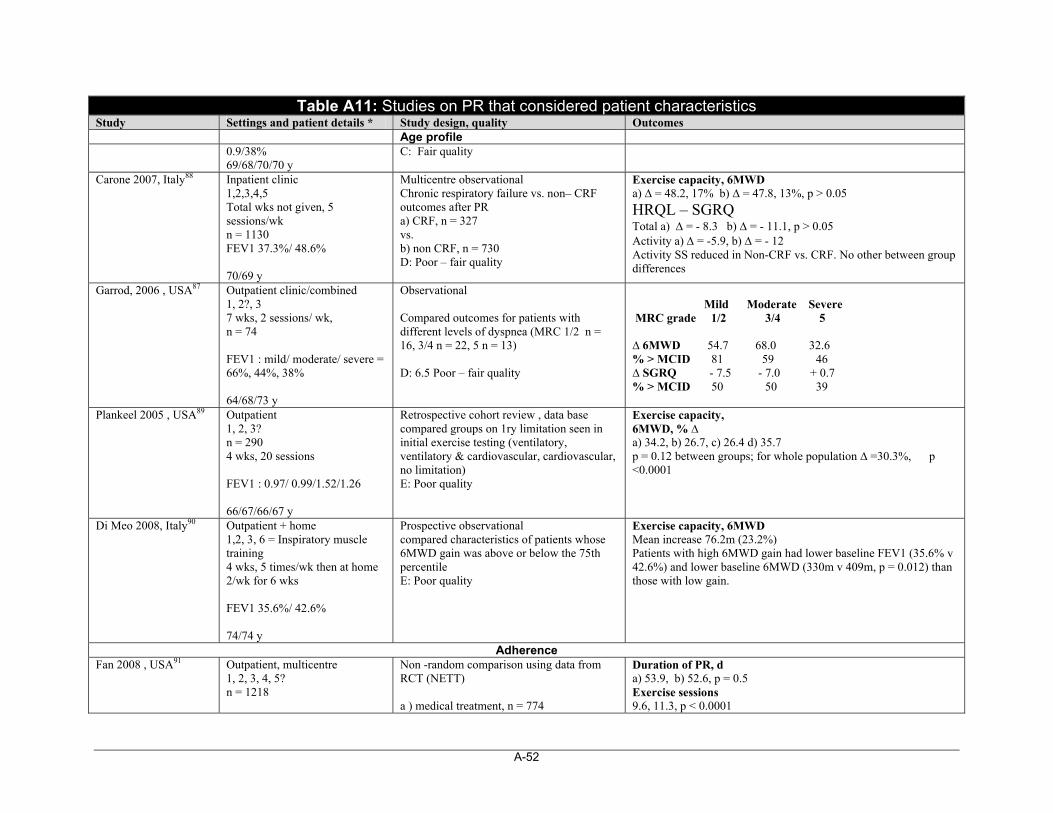
A-52
Table A11: Studies on PR that considered patient characteristics Study Settings and patient details * Study design, quality Outcomes Age profile
0.9/38% 69/68/70/70 y
C: Fair quality
Carone 2007, Italy88 Inpatient clinic 1,2,3,4,5 Total wks not given, 5 sessions/wk n = 1130 FEV1 37.3%/ 48.6% 70/69 y
Multicentre observational Chronic respiratory failure vs. non– CRF outcomes after PR a) CRF, n = 327 vs. b) non CRF, n = 730 D: Poor – fair quality
Exercise capacity, 6MWD a) ∆ = 48.2, 17% b) ∆ = 47.8, 13%, p > 0.05
HRQL – SGRQ Total a) = - 8.3 b) = - 11.1, p > 0.05 Activity a) = -5.9, b) = - 12 Activity SS reduced in Non-CRF vs. CRF. No other between group differences
Garrod, 2006 , USA87 Outpatient clinic/combined 1, 2?, 3 7 wks, 2 sessions/ wk, n = 74 FEV1 : mild/ moderate/ severe = 66%, 44%, 38% 64/68/73 y
Observational Compared outcomes for patients with different levels of dyspnea (MRC 1/2 n = 16, 3/4 n = 22, 5 n = 13) D: 6.5 Poor – fair quality
Mild Moderate Severe MRC grade 1/2 3/4 5 ∆ 6MWD 54.7 68.0 32.6 % > MCID 81 59 46 ∆ SGRQ - 7.5 - 7.0 + 0.7 % > MCID 50 50 39
Plankeel 2005 , USA89 Outpatient 1, 2, 3? n = 290 4 wks, 20 sessions FEV1 : 0.97/ 0.99/1.52/1.26 66/67/66/67 y
Retrospective cohort review , data base compared groups on 1ry limitation seen in initial exercise testing (ventilatory, ventilatory & cardiovascular, cardiovascular, no limitation) E: Poor quality
Exercise capacity, 6MWD, % ∆ a) 34.2, b) 26.7, c) 26.4 d) 35.7 p = 0.12 between groups; for whole population ∆ =30.3%, p <0.0001
Di Meo 2008, Italy90 Outpatient + home 1,2, 3, 6 = Inspiratory muscle training 4 wks, 5 times/wk then at home 2/wk for 6 wks FEV1 35.6%/ 42.6% 74/74 y
Prospective observational compared characteristics of patients whose 6MWD gain was above or below the 75th percentile E: Poor quality
Exercise capacity, 6MWD Mean increase 76.2m (23.2%) Patients with high 6MWD gain had lower baseline FEV1 (35.6% v 42.6%) and lower baseline 6MWD (330m v 409m, p = 0.012) than those with low gain.
Adherence Fan 2008 , USA91 Outpatient, multicentre
1, 2, 3, 4, 5? n = 1218
Non -random comparison using data from RCT (NETT) a ) medical treatment, n = 774
Duration of PR, d a) 53.9, b) 52.6, p = 0.5 Exercise sessions 9.6, 11.3, p < 0.0001
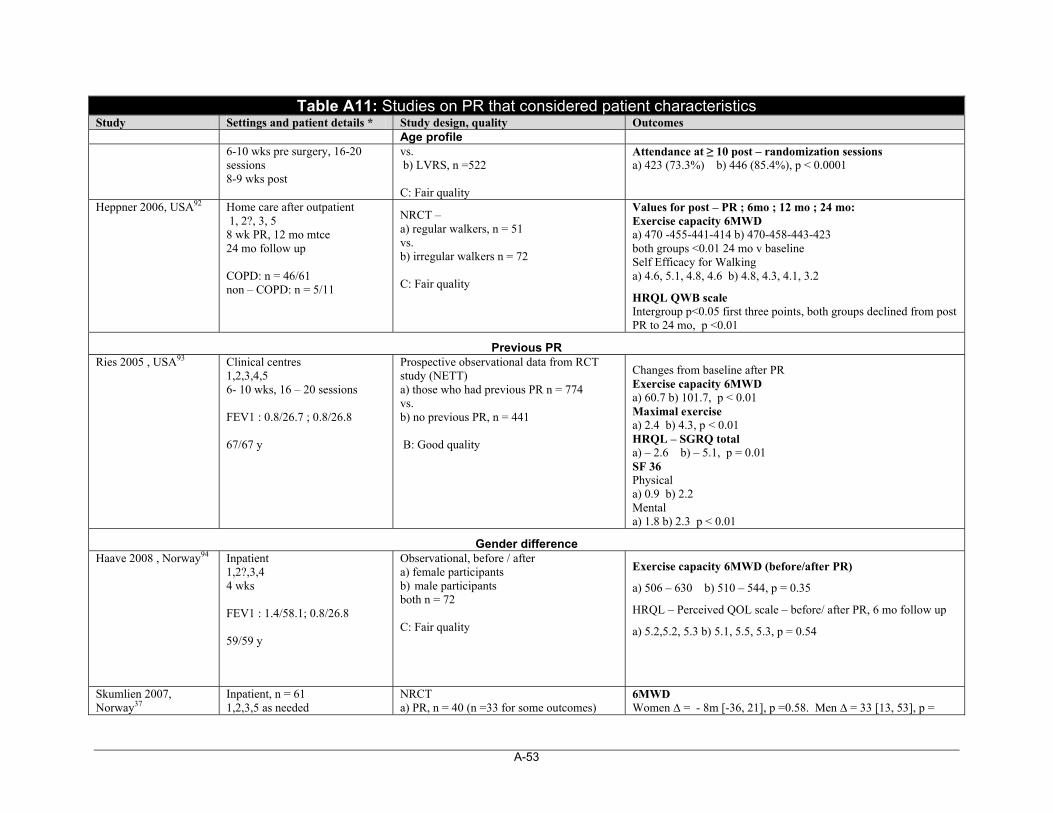
A-53
Table A11: Studies on PR that considered patient characteristics Study Settings and patient details * Study design, quality Outcomes Age profile
6-10 wks pre surgery, 16-20 sessions 8-9 wks post
vs. b) LVRS, n =522 C: Fair quality
Attendance at ≥ 10 post – randomization sessions a) 423 (73.3%) b) 446 (85.4%), p < 0.0001
Heppner 2006, USA92 Home care after outpatient 1, 2?, 3, 5 8 wk PR, 12 mo mtce 24 mo follow up COPD: n = 46/61 non – COPD: n = 5/11
NRCT – a) regular walkers, n = 51 vs. b) irregular walkers n = 72 C: Fair quality
Values for post – PR ; 6mo ; 12 mo ; 24 mo: Exercise capacity 6MWD a) 470 -455-441-414 b) 470-458-443-423 both groups <0.01 24 mo v baseline Self Efficacy for Walking a) 4.6, 5.1, 4.8, 4.6 b) 4.8, 4.3, 4.1, 3.2
HRQL QWB scale Intergroup p<0.05 first three points, both groups declined from post PR to 24 mo, p <0.01
Previous PR Ries 2005 , USA93 Clinical centres
1,2,3,4,5 6- 10 wks, 16 – 20 sessions FEV1 : 0.8/26.7 ; 0.8/26.8 67/67 y
Prospective observational data from RCT study (NETT) a) those who had previous PR n = 774 vs. b) no previous PR, n = 441 B: Good quality
Changes from baseline after PR Exercise capacity 6MWD a) 60.7 b) 101.7, p < 0.01 Maximal exercise a) 2.4 b) 4.3, p < 0.01 HRQL – SGRQ total a) – 2.6 b) – 5.1, p = 0.01 SF 36 Physical a) 0.9 b) 2.2 Mental a) 1.8 b) 2.3 p < 0.01
Gender difference Haave 2008 , Norway94 Inpatient
1,2?,3,4 4 wks FEV1 : 1.4/58.1; 0.8/26.8 59/59 y
Observational, before / after a) female participants b) male participants both n = 72 C: Fair quality
Exercise capacity 6MWD (before/after PR)
a) 506 – 630 b) 510 – 544, p = 0.35
HRQL – Perceived QOL scale – before/ after PR, 6 mo follow up
a) 5.2,5.2, 5.3 b) 5.1, 5.5, 5.3, p = 0.54
Skumlien 2007, Norway37
Inpatient, n = 61 1,2,3,5 as needed
NRCT a) PR, n = 40 (n =33 for some outcomes)
6MWD Women ∆ = - 8m [-36, 21], p =0.58. Men ∆ = 33 [13, 53], p =
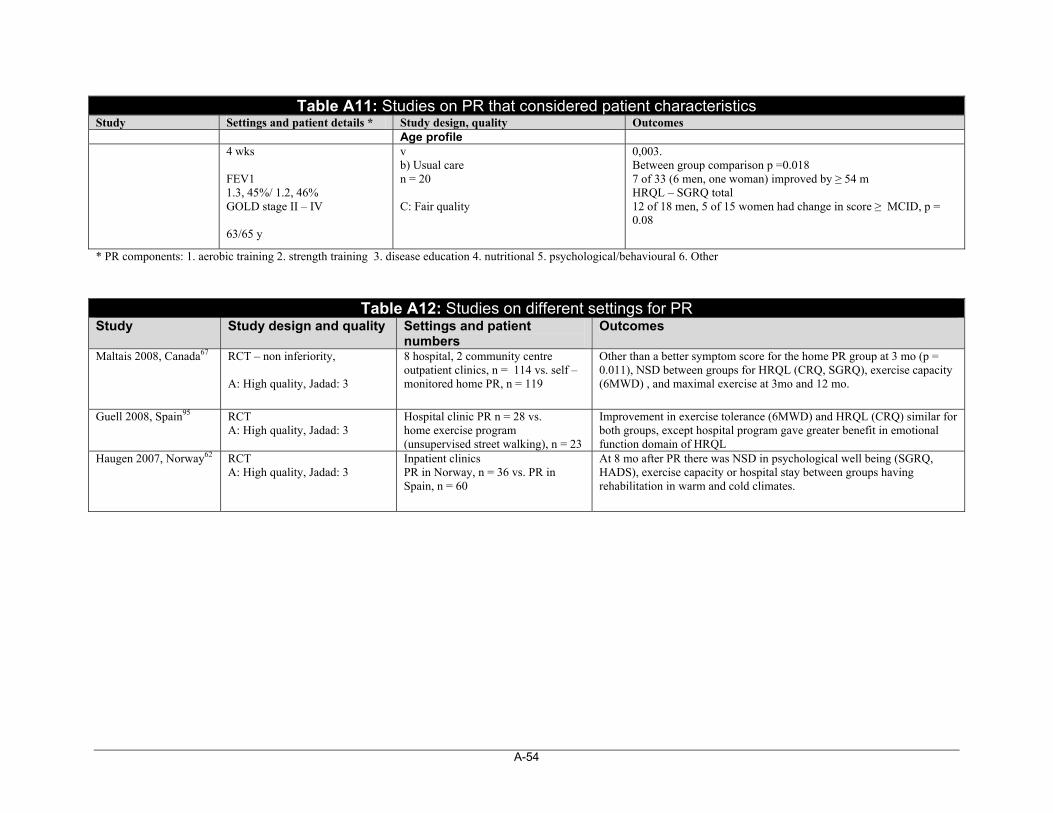
A-54
Table A11: Studies on PR that considered patient characteristics Study Settings and patient details * Study design, quality Outcomes Age profile
4 wks FEV1 1.3, 45%/ 1.2, 46% GOLD stage II – IV 63/65 y
v b) Usual care n = 20 C: Fair quality
0,003. Between group comparison p =0.018 7 of 33 (6 men, one woman) improved by ≥ 54 m HRQL – SGRQ total 12 of 18 men, 5 of 15 women had change in score ≥ MCID, p = 0.08
* PR components: 1. aerobic training 2. strength training 3. disease education 4. nutritional 5. psychological/behavioural 6. Other
Table A12: Studies on different settings for PR Study Study design and quality Settings and patient
numbers Outcomes
Maltais 2008, Canada67 RCT – non inferiority, A: High quality, Jadad: 3
8 hospital, 2 community centre outpatient clinics, n = 114 vs. self – monitored home PR, n = 119
Other than a better symptom score for the home PR group at 3 mo (p = 0.011), NSD between groups for HRQL (CRQ, SGRQ), exercise capacity (6MWD) , and maximal exercise at 3mo and 12 mo.
Guell 2008, Spain95 RCT
A: High quality, Jadad: 3 Hospital clinic PR n = 28 vs. home exercise program (unsupervised street walking), n = 23
Improvement in exercise tolerance (6MWD) and HRQL (CRQ) similar for both groups, except hospital program gave greater benefit in emotional function domain of HRQL
Haugen 2007, Norway62 RCT A: High quality, Jadad: 3
Inpatient clinics PR in Norway, n = 36 vs. PR in Spain, n = 60
At 8 mo after PR there was NSD in psychological well being (SGRQ, HADS), exercise capacity or hospital stay between groups having rehabilitation in warm and cold climates.
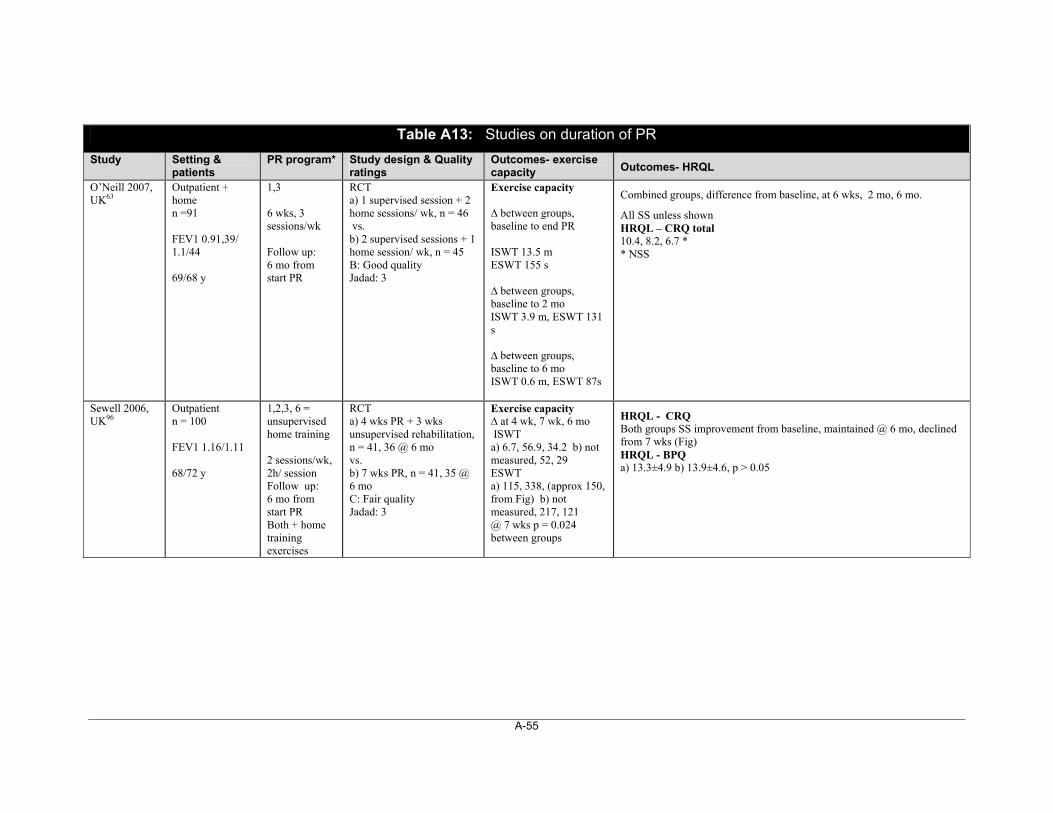
A-55
Table A13: Studies on duration of PR
Study Setting & patients
PR program* Study design & Quality ratings
Outcomes- exercise capacity Outcomes- HRQL
O’Neill 2007, UK63
Outpatient + home n =91 FEV1 0.91,39/ 1.1/44 69/68 y
1,3 6 wks, 3 sessions/wk Follow up: 6 mo from start PR
RCT a) 1 supervised session + 2 home sessions/ wk, n = 46 vs. b) 2 supervised sessions + 1 home session/ wk, n = 45 B: Good quality Jadad: 3
Exercise capacity ∆ between groups, baseline to end PR ISWT 13.5 m ESWT 155 s ∆ between groups, baseline to 2 mo ISWT 3.9 m, ESWT 131 s ∆ between groups, baseline to 6 mo ISWT 0.6 m, ESWT 87s
Combined groups, difference from baseline, at 6 wks, 2 mo, 6 mo.
All SS unless shown HRQL – CRQ total 10.4, 8.2, 6.7 * * NSS
Sewell 2006, UK96
Outpatient n = 100 FEV1 1.16/1.11 68/72 y
1,2,3, 6 = unsupervised home training 2 sessions/wk, 2h/ session Follow up: 6 mo from start PR Both + home training exercises
RCT a) 4 wks PR + 3 wks unsupervised rehabilitation, n = 41, 36 @ 6 mo vs. b) 7 wks PR, n = 41, 35 @ 6 mo C: Fair quality Jadad: 3
Exercise capacity ∆ at 4 wk, 7 wk, 6 mo ISWT a) 6.7, 56.9, 34.2 b) not measured, 52, 29 ESWT a) 115, 338, (approx 150, from Fig) b) not measured, 217, 121 @ 7 wks p = 0.024 between groups
HRQL - CRQ Both groups SS improvement from baseline, maintained @ 6 mo, declined from 7 wks (Fig) HRQL - BPQ a) 13.3±4.9 b) 13.9±4.6, p > 0.05
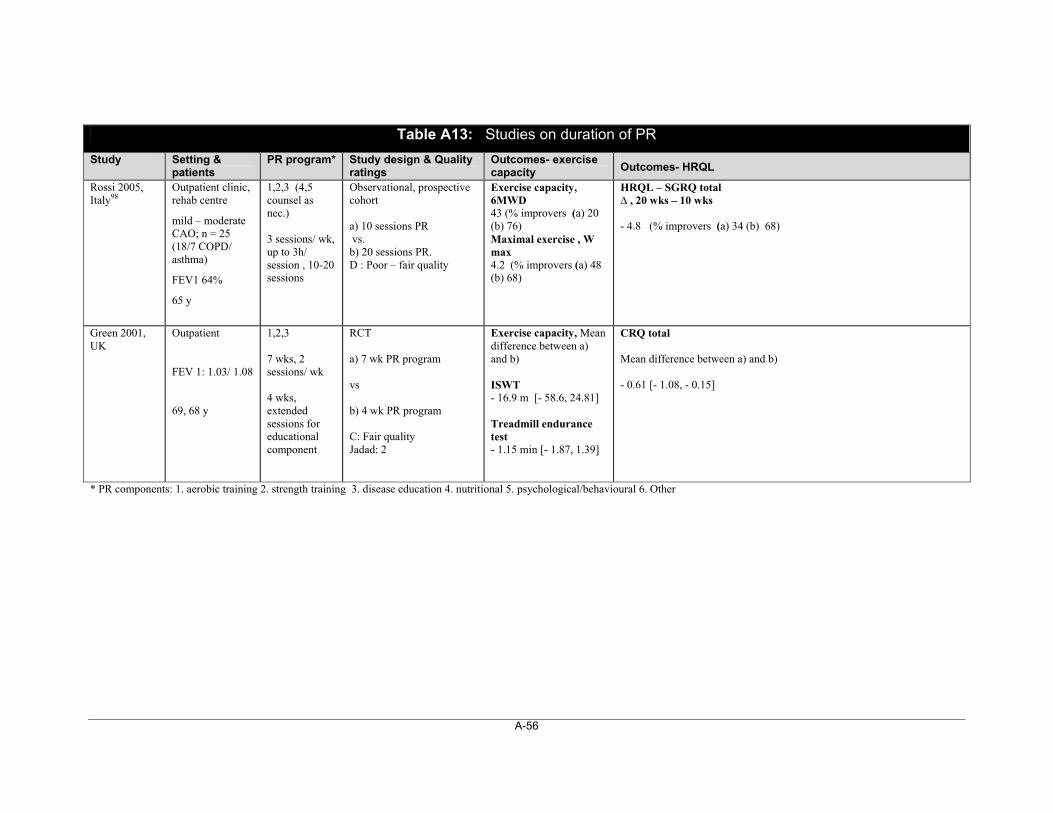
A-56
Table A13: Studies on duration of PR
Study Setting & patients
PR program* Study design & Quality ratings
Outcomes- exercise capacity Outcomes- HRQL
Rossi 2005, Italy98
Outpatient clinic, rehab centre
mild – moderate CAO; n = 25 (18/7 COPD/ asthma)
FEV1 64%
65 y
1,2,3 (4,5 counsel as nec.) 3 sessions/ wk, up to 3h/ session , 10-20 sessions
Observational, prospective cohort a) 10 sessions PR vs. b) 20 sessions PR. D : Poor – fair quality
Exercise capacity, 6MWD 43 (% improvers (a) 20 (b) 76) Maximal exercise , W max 4.2 (% improvers (a) 48 (b) 68)
HRQL – SGRQ total ∆ , 20 wks – 10 wks - 4.8 (% improvers (a) 34 (b) 68)
Green 2001, UK
Outpatient FEV 1: 1.03/ 1.08 69, 68 y
1,2,3 7 wks, 2 sessions/ wk 4 wks, extended sessions for educational component
RCT a) 7 wk PR program vs b) 4 wk PR program C: Fair quality Jadad: 2
Exercise capacity, Mean difference between a) and b) ISWT - 16.9 m [- 58.6, 24.81] Treadmill endurance test - 1.15 min [- 1.87, 1.39]
CRQ total Mean difference between a) and b) - 0.61 [- 1.08, - 0.15]
* PR components: 1. aerobic training 2. strength training 3. disease education 4. nutritional 5. psychological/behavioural 6. Other
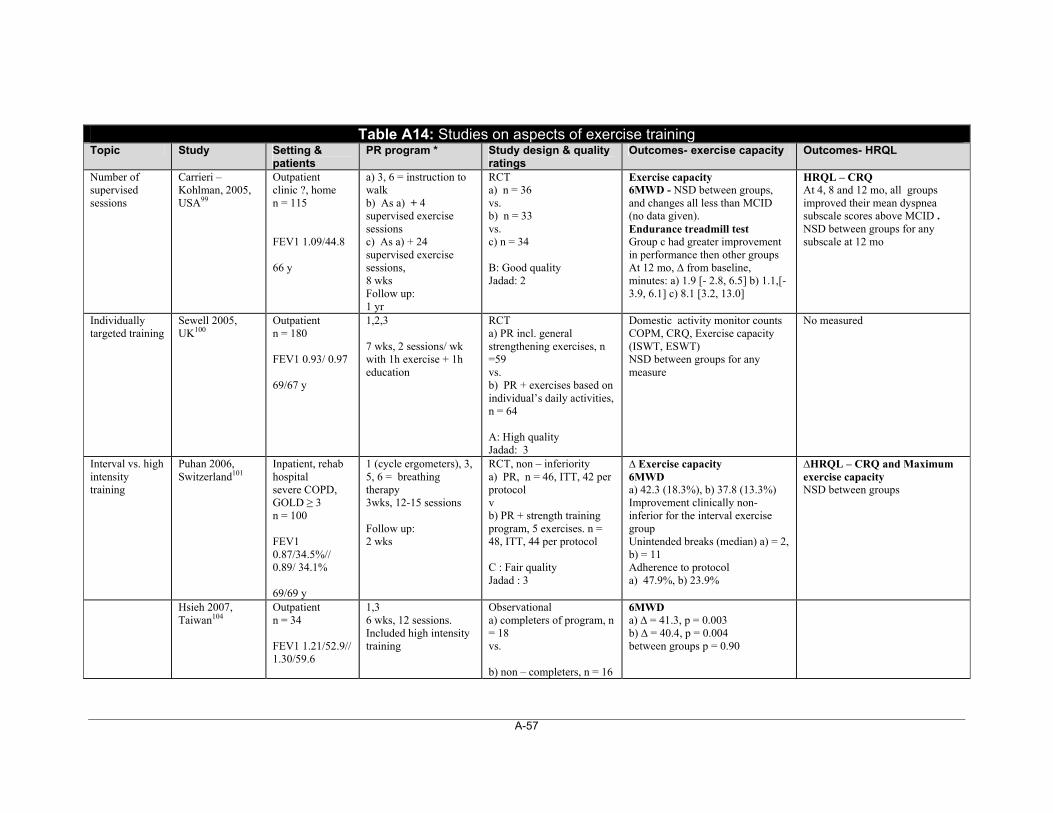
A-57
Table A14: Studies on aspects of exercise training Topic Study Setting &
patients PR program * Study design & quality
ratings Outcomes- exercise capacity Outcomes- HRQL
Number of supervised sessions
Carrieri – Kohlman, 2005, USA99
Outpatient clinic ?, home n = 115 FEV1 1.09/44.8 66 y
a) 3, 6 = instruction to walk b) As a) + 4 supervised exercise sessions c) As a) + 24 supervised exercise sessions, 8 wks Follow up: 1 yr
RCT a) n = 36 vs. b) n = 33 vs. c) n = 34 B: Good quality Jadad: 2
Exercise capacity 6MWD - NSD between groups, and changes all less than MCID (no data given). Endurance treadmill test Group c had greater improvement in performance then other groups At 12 mo, ∆ from baseline, minutes: a) 1.9 [- 2.8, 6.5] b) 1.1,[- 3.9, 6.1] c) 8.1 [3.2, 13.0]
HRQL – CRQ At 4, 8 and 12 mo, all groups improved their mean dyspnea subscale scores above MCID . NSD between groups for any subscale at 12 mo
Individually targeted training
Sewell 2005, UK100
Outpatient n = 180 FEV1 0.93/ 0.97 69/67 y
1,2,3 7 wks, 2 sessions/ wk with 1h exercise + 1h education
RCT a) PR incl. general strengthening exercises, n =59 vs. b) PR + exercises based on individual’s daily activities, n = 64 A: High quality Jadad: 3
Domestic activity monitor counts COPM, CRQ, Exercise capacity (ISWT, ESWT) NSD between groups for any measure
No measured
Interval vs. high intensity training
Puhan 2006, Switzerland101
Inpatient, rehab hospital severe COPD, GOLD ≥ 3 n = 100 FEV1 0.87/34.5%// 0.89/ 34.1% 69/69 y
1 (cycle ergometers), 3, 5, 6 = breathing therapy 3wks, 12-15 sessions Follow up: 2 wks
RCT, non – inferiority a) PR, n = 46, ITT, 42 per protocol v b) PR + strength training program, 5 exercises. n = 48, ITT, 44 per protocol C : Fair quality Jadad : 3
∆ Exercise capacity 6MWD a) 42.3 (18.3%), b) 37.8 (13.3%) Improvement clinically non-inferior for the interval exercise group Unintended breaks (median) a) = 2, b) = 11 Adherence to protocol a) 47.9%, b) 23.9%
∆HRQL – CRQ and Maximum exercise capacity NSD between groups
Hsieh 2007, Taiwan104
Outpatient n = 34 FEV1 1.21/52.9// 1.30/59.6
1,3 6 wks, 12 sessions. Included high intensity training
Observational a) completers of program, n = 18 vs. b) non – completers, n = 16
6MWD a) ∆ = 41.3, p = 0.003 b) ∆ = 40.4, p = 0.004 between groups p = 0.90
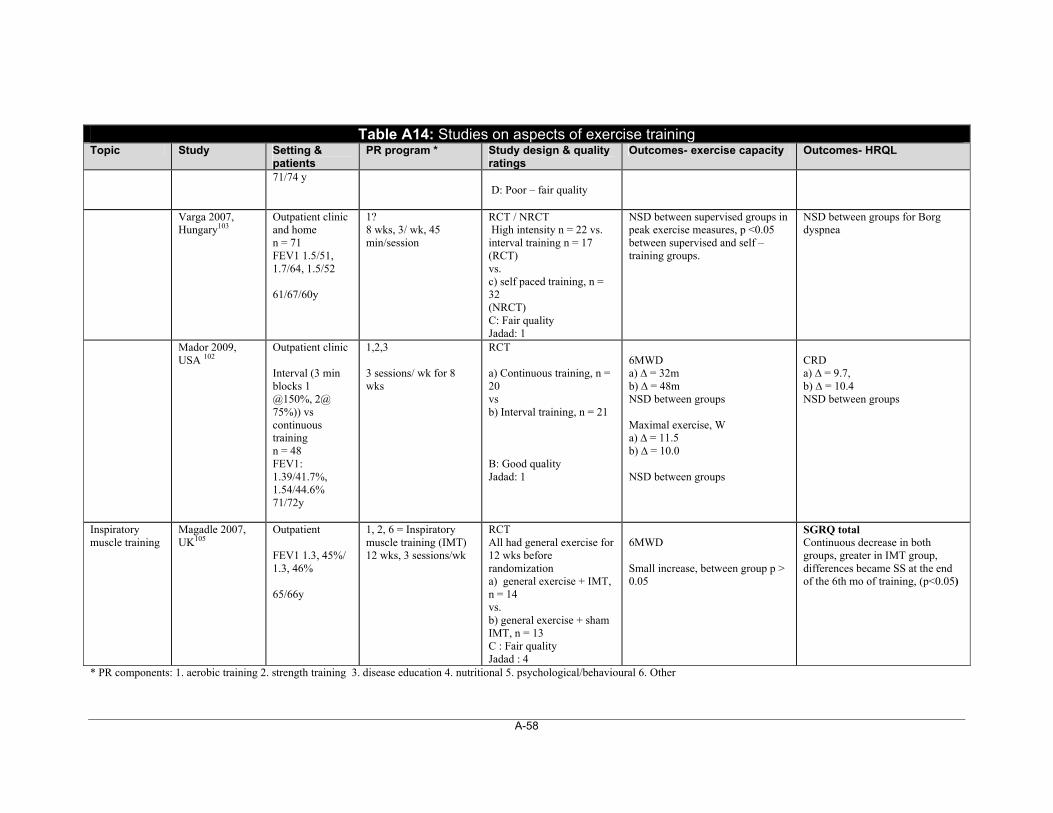
A-58
Table A14: Studies on aspects of exercise training Topic Study Setting &
patients PR program * Study design & quality
ratings Outcomes- exercise capacity Outcomes- HRQL
71/74 y
D: Poor – fair quality
Varga 2007, Hungary103
Outpatient clinic and home n = 71 FEV1 1.5/51, 1.7/64, 1.5/52 61/67/60y
1? 8 wks, 3/ wk, 45 min/session
RCT / NRCT High intensity n = 22 vs. interval training n = 17 (RCT) vs. c) self paced training, n = 32 (NRCT) C: Fair quality Jadad: 1
NSD between supervised groups in peak exercise measures, p <0.05 between supervised and self – training groups.
NSD between groups for Borg dyspnea
Mador 2009, USA 102
Outpatient clinic Interval (3 min blocks 1 @150%, 2@ 75%)) vs continuous training n = 48 FEV1: 1.39/41.7%, 1.54/44.6% 71/72y
1,2,3 3 sessions/ wk for 8 wks
RCT a) Continuous training, n = 20 vs b) Interval training, n = 21 B: Good quality Jadad: 1
6MWD a) ∆ = 32m b) ∆ = 48m NSD between groups Maximal exercise, W a) ∆ = 11.5 b) ∆ = 10.0 NSD between groups
CRD a) ∆ = 9.7, b) ∆ = 10.4 NSD between groups
Inspiratory muscle training
Magadle 2007, UK105
Outpatient FEV1 1.3, 45%/ 1.3, 46% 65/66y
1, 2, 6 = Inspiratory muscle training (IMT) 12 wks, 3 sessions/wk
RCT All had general exercise for 12 wks before randomization a) general exercise + IMT, n = 14 vs. b) general exercise + sham IMT, n = 13 C : Fair quality Jadad : 4
6MWD Small increase, between group p > 0.05
SGRQ total Continuous decrease in both groups, greater in IMT group, differences became SS at the end of the 6th mo of training, (p<0.05)
* PR components: 1. aerobic training 2. strength training 3. disease education 4. nutritional 5. psychological/behavioural 6. Other
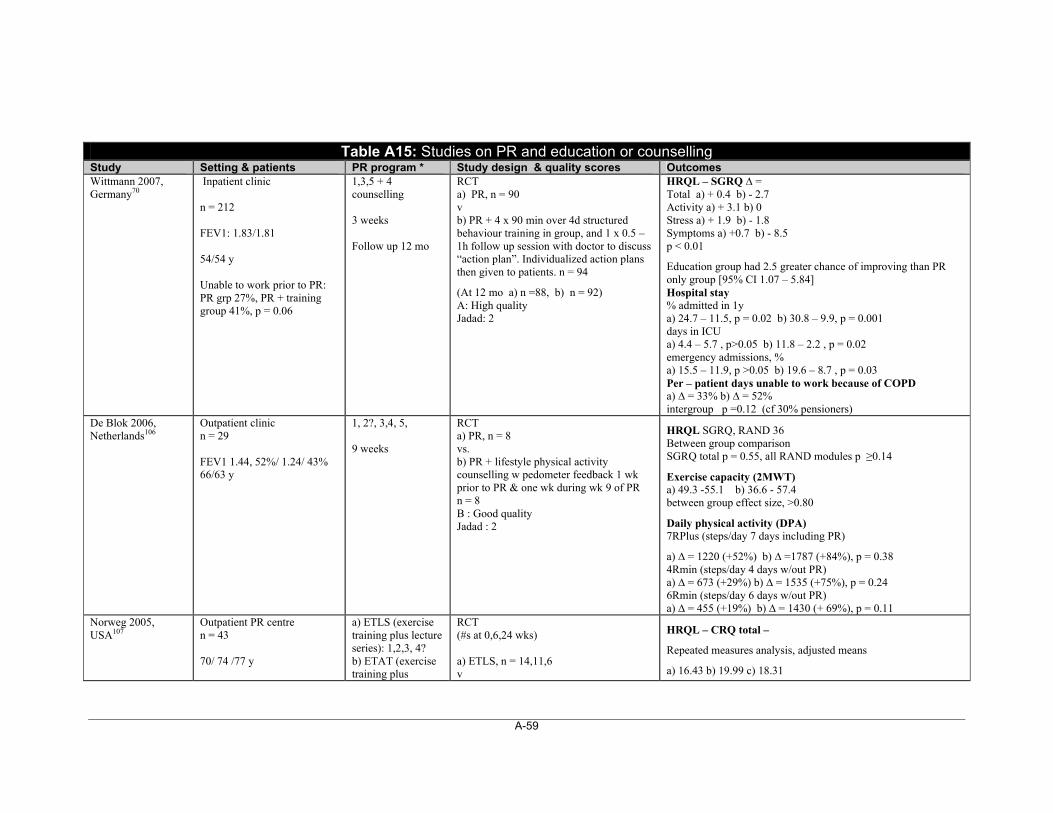
A-59
Table A15: Studies on PR and education or counselling
Study Setting & patients PR program * Study design & quality scores Outcomes Wittmann 2007, Germany70
Inpatient clinic n = 212 FEV1: 1.83/1.81 54/54 y Unable to work prior to PR: PR grp 27%, PR + training group 41%, p = 0.06
1,3,5 + 4 counselling 3 weeks Follow up 12 mo
RCT a) PR, n = 90 v b) PR + 4 x 90 min over 4d structured behaviour training in group, and 1 x 0.5 – 1h follow up session with doctor to discuss “action plan”. Individualized action plans then given to patients. n = 94
(At 12 mo a) n =88, b) n = 92) A: High quality Jadad: 2
HRQL – SGRQ ∆ = Total a) + 0.4 b) - 2.7 Activity a) + 3.1 b) 0 Stress a) + 1.9 b) - 1.8 Symptoms a) +0.7 b) - 8.5 p < 0.01
Education group had 2.5 greater chance of improving than PR only group [95% CI 1.07 – 5.84] Hospital stay % admitted in 1y a) 24.7 – 11.5, p = 0.02 b) 30.8 – 9.9, p = 0.001 days in ICU a) 4.4 – 5.7 , p>0.05 b) 11.8 – 2.2 , p = 0.02 emergency admissions, % a) 15.5 – 11.9, p >0.05 b) 19.6 – 8.7 , p = 0.03 Per – patient days unable to work because of COPD a) ∆ = 33% b) ∆ = 52% intergroup p =0.12 (cf 30% pensioners)
De Blok 2006, Netherlands106
Outpatient clinic n = 29 FEV1 1.44, 52%/ 1.24/ 43% 66/63 y
1, 2?, 3,4, 5, 9 weeks
RCT a) PR, n = 8 vs. b) PR + lifestyle physical activity counselling w pedometer feedback 1 wk prior to PR & one wk during wk 9 of PR n = 8 B : Good quality Jadad : 2
HRQL SGRQ, RAND 36 Between group comparison SGRQ total p = 0.55, all RAND modules p ≥0.14
Exercise capacity (2MWT) a) 49.3 -55.1 b) 36.6 - 57.4 between group effect size, >0.80
Daily physical activity (DPA) 7RPlus (steps/day 7 days including PR)
a) ∆ = 1220 (+52%) b) ∆ =1787 (+84%), p = 0.38 4Rmin (steps/day 4 days w/out PR) a) ∆ = 673 (+29%) b) ∆ = 1535 (+75%), p = 0.24 6Rmin (steps/day 6 days w/out PR) a) ∆ = 455 (+19%) b) ∆ = 1430 (+ 69%), p = 0.11
Norweg 2005, USA107
Outpatient PR centre n = 43 70/ 74 /77 y
a) ETLS (exercise training plus lecture series): 1,2,3, 4? b) ETAT (exercise training plus
RCT (#s at 0,6,24 wks) a) ETLS, n = 14,11,6 v
HRQL – CRQ total –
Repeated measures analysis, adjusted means
a) 16.43 b) 19.99 c) 18.31
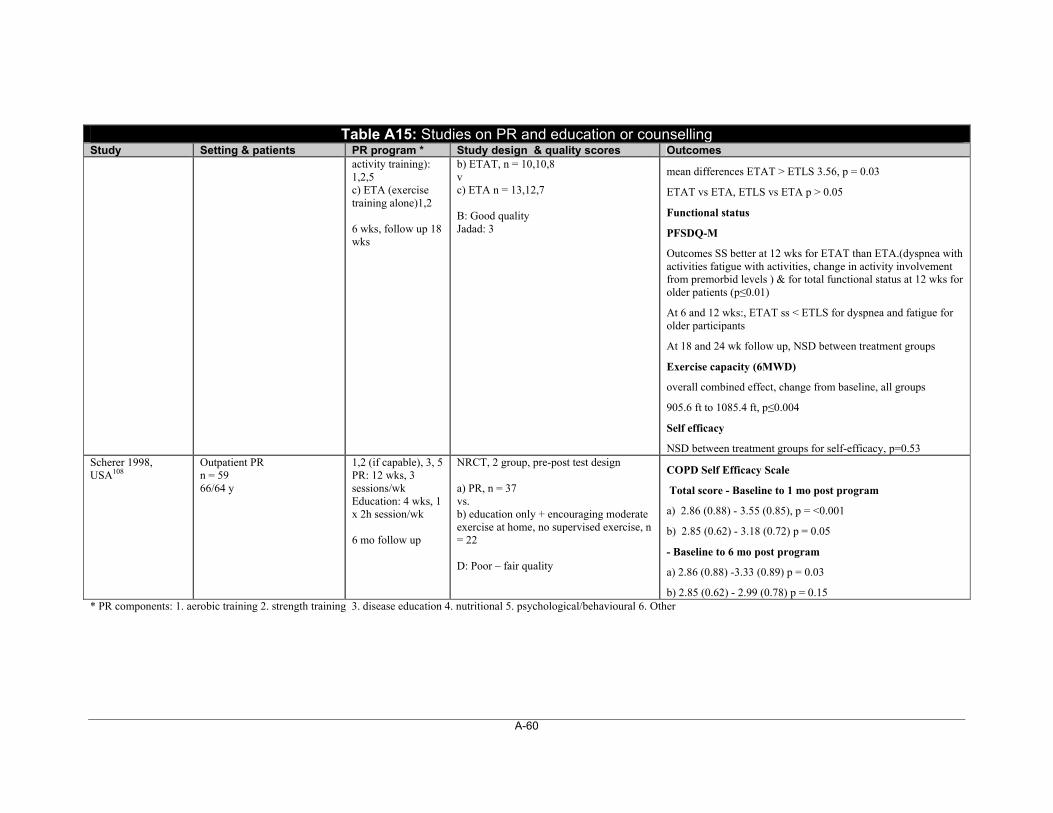
A-60
Table A15: Studies on PR and education or counselling Study Setting & patients PR program * Study design & quality scores Outcomes
activity training): 1,2,5 c) ETA (exercise training alone)1,2 6 wks, follow up 18 wks
b) ETAT, n = 10,10,8 v c) ETA n = 13,12,7 B: Good quality Jadad: 3
mean differences ETAT > ETLS 3.56, p = 0.03
ETAT vs ETA, ETLS vs ETA p > 0.05
Functional status
PFSDQ-M
Outcomes SS better at 12 wks for ETAT than ETA.(dyspnea with activities fatigue with activities, change in activity involvement from premorbid levels ) & for total functional status at 12 wks for older patients (p≤0.01)
At 6 and 12 wks:, ETAT ss < ETLS for dyspnea and fatigue for older participants
At 18 and 24 wk follow up, NSD between treatment groups
Exercise capacity (6MWD)
overall combined effect, change from baseline, all groups
905.6 ft to 1085.4 ft, p≤0.004
Self efficacy
NSD between treatment groups for self-efficacy, p=0.53 Scherer 1998, USA108
Outpatient PR n = 59 66/64 y
1,2 (if capable), 3, 5 PR: 12 wks, 3 sessions/wk Education: 4 wks, 1 x 2h session/wk 6 mo follow up
NRCT, 2 group, pre-post test design a) PR, n = 37 vs. b) education only + encouraging moderate exercise at home, no supervised exercise, n = 22 D: Poor – fair quality
COPD Self Efficacy Scale
Total score - Baseline to 1 mo post program
a) 2.86 (0.88) - 3.55 (0.85), p = <0.001
b) 2.85 (0.62) - 3.18 (0.72) p = 0.05
- Baseline to 6 mo post program
a) 2.86 (0.88) -3.33 (0.89) p = 0.03
b) 2.85 (0.62) - 2.99 (0.78) p = 0.15 * PR components: 1. aerobic training 2. strength training 3. disease education 4. nutritional 5. psychological/behavioural 6. Other
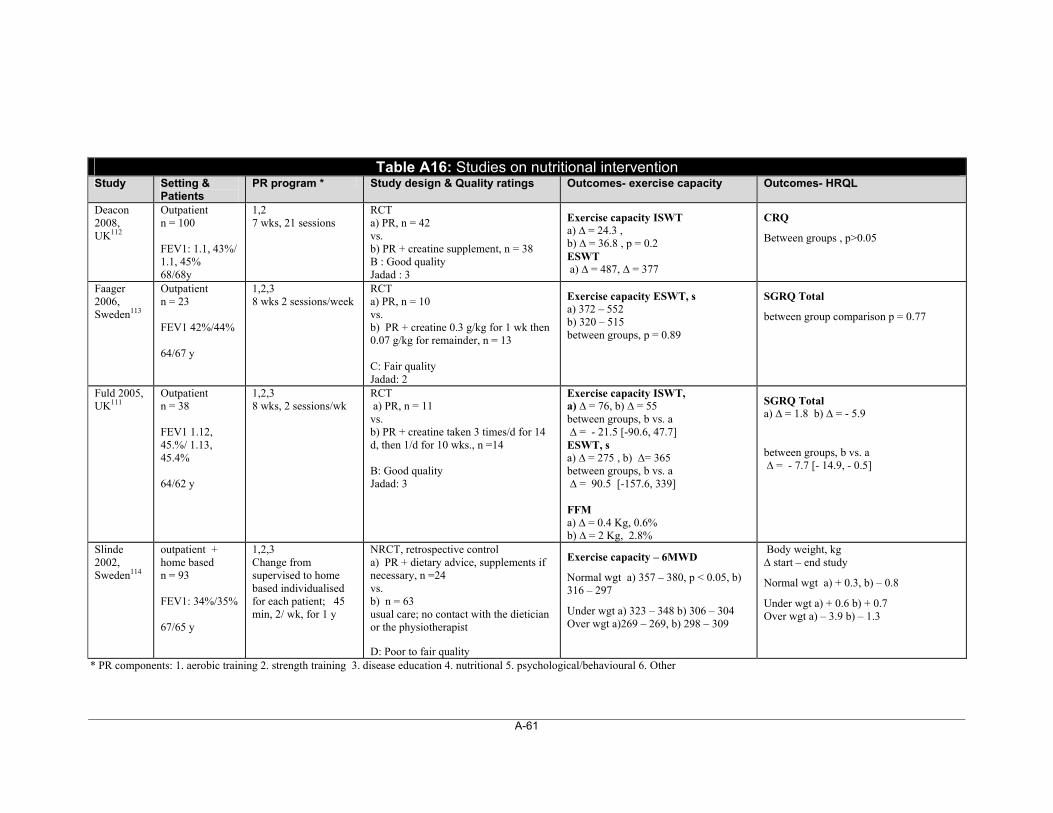
A-61
* PR components: 1. aerobic training 2. strength training 3. disease education 4. nutritional 5. psychological/behavioural 6. Other
Table A16: Studies on nutritional intervention Study Setting &
Patients PR program * Study design & Quality ratings Outcomes- exercise capacity Outcomes- HRQL
Deacon 2008, UK112
Outpatient n = 100 FEV1: 1.1, 43%/ 1.1, 45% 68/68y
1,2 7 wks, 21 sessions
RCT a) PR, n = 42 vs. b) PR + creatine supplement, n = 38 B : Good quality Jadad : 3
Exercise capacity ISWT a) ∆ = 24.3 , b) ∆ = 36.8 , p = 0.2 ESWT a) ∆ = 487, ∆ = 377
CRQ
Between groups , p>0.05
Faager 2006, Sweden113
Outpatient n = 23 FEV1 42%/44% 64/67 y
1,2,3 8 wks 2 sessions/week
RCT a) PR, n = 10 vs. b) PR + creatine 0.3 g/kg for 1 wk then 0.07 g/kg for remainder, n = 13 C: Fair quality Jadad: 2
Exercise capacity ESWT, s a) 372 – 552 b) 320 – 515 between groups, p = 0.89
SGRQ Total
between group comparison p = 0.77
Fuld 2005, UK111
Outpatient n = 38 FEV1 1.12, 45.%/ 1.13, 45.4% 64/62 y
1,2,3 8 wks, 2 sessions/wk
RCT a) PR, n = 11 vs. b) PR + creatine taken 3 times/d for 14 d, then 1/d for 10 wks., n =14 B: Good quality Jadad: 3
Exercise capacity ISWT, a) ∆ = 76, b) ∆ = 55 between groups, b vs. a ∆ = - 21.5 [-90.6, 47.7] ESWT, s a) ∆ = 275 , b) ∆= 365 between groups, b vs. a ∆ = 90.5 [-157.6, 339] FFM a) ∆ = 0.4 Kg, 0.6% b) ∆ = 2 Kg, 2.8%
SGRQ Total a) ∆ = 1.8 b) ∆ = - 5.9 between groups, b vs. a ∆ = - 7.7 [- 14.9, - 0.5]
Slinde 2002, Sweden114
outpatient + home based n = 93 FEV1: 34%/35% 67/65 y
1,2,3 Change from supervised to home based individualised for each patient; 45 min, 2/ wk, for 1 y
NRCT, retrospective control a) PR + dietary advice, supplements if necessary, n =24 vs. b) n = 63 usual care; no contact with the dietician or the physiotherapist D: Poor to fair quality
Exercise capacity – 6MWD
Normal wgt a) 357 – 380, p < 0.05, b) 316 – 297
Under wgt a) 323 – 348 b) 306 – 304 Over wgt a)269 – 269, b) 298 – 309
Body weight, kg ∆ start – end study
Normal wgt a) + 0.3, b) – 0.8
Under wgt a) + 0.6 b) + 0.7 Over wgt a) – 3.9 b) – 1.3
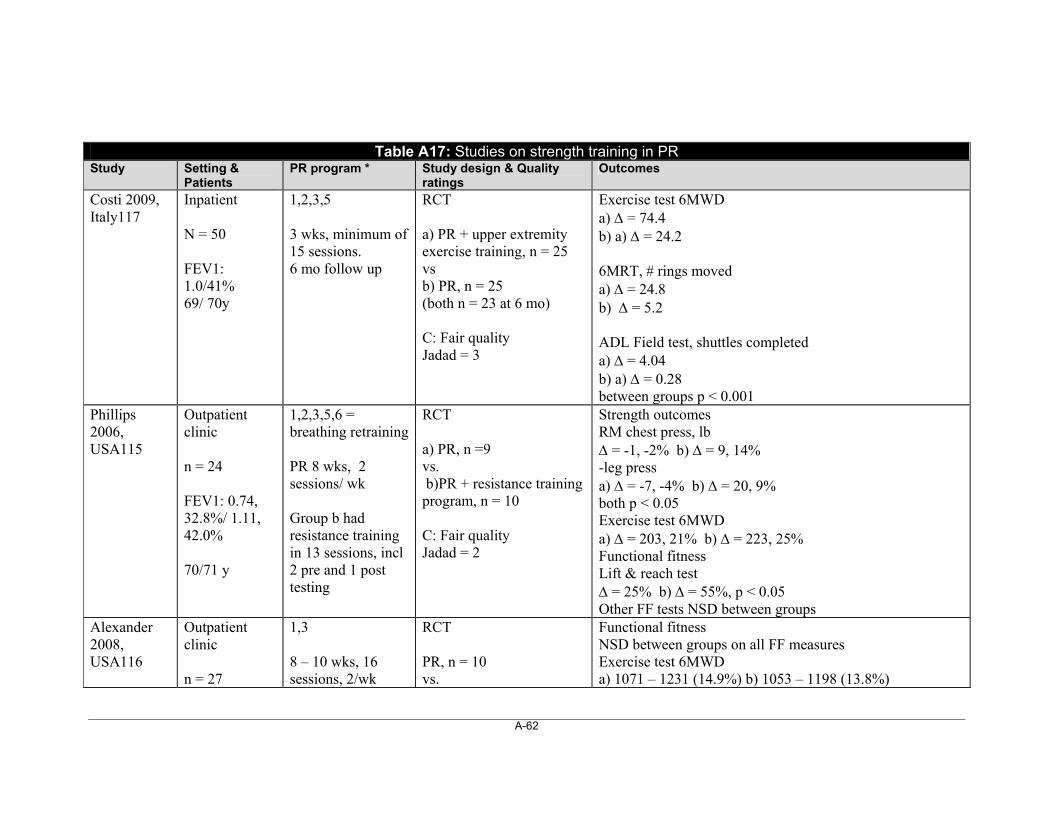
A-62
Table A17: Studies on strength training in PR
Study Setting & Patients
PR program * Study design & Quality ratings
Outcomes
Costi 2009, Italy117
Inpatient N = 50 FEV1: 1.0/41% 69/ 70y
1,2,3,5 3 wks, minimum of 15 sessions. 6 mo follow up
RCT a) PR + upper extremity exercise training, n = 25 vs b) PR, n = 25 (both n = 23 at 6 mo) C: Fair quality Jadad = 3
Exercise test 6MWD a) = 74.4 b) a) = 24.2 6MRT, # rings moved a) = 24.8 b) = 5.2 ADL Field test, shuttles completed a) = 4.04 b) a) = 0.28 between groups p < 0.001
Phillips 2006, USA115
Outpatient clinic n = 24 FEV1: 0.74, 32.8%/ 1.11, 42.0% 70/71 y
1,2,3,5,6 = breathing retraining PR 8 wks, 2 sessions/ wk Group b had resistance training in 13 sessions, incl 2 pre and 1 post testing
RCT a) PR, n =9 vs. b)PR + resistance training program, n = 10 C: Fair quality Jadad = 2
Strength outcomes RM chest press, lb = -1, -2% b) = 9, 14% -leg press a) = -7, -4% b) = 20, 9% both p < 0.05 Exercise test 6MWD a) = 203, 21% b) = 223, 25% Functional fitness Lift & reach test = 25% b) = 55%, p < 0.05 Other FF tests NSD between groups
Alexander 2008, USA116
Outpatient clinic n = 27
1,3 8 – 10 wks, 16 sessions, 2/wk
RCT PR, n = 10 vs.
Functional fitness NSD between groups on all FF measures Exercise test 6MWD a) 1071 – 1231 (14.9%) b) 1053 – 1198 (13.8%)
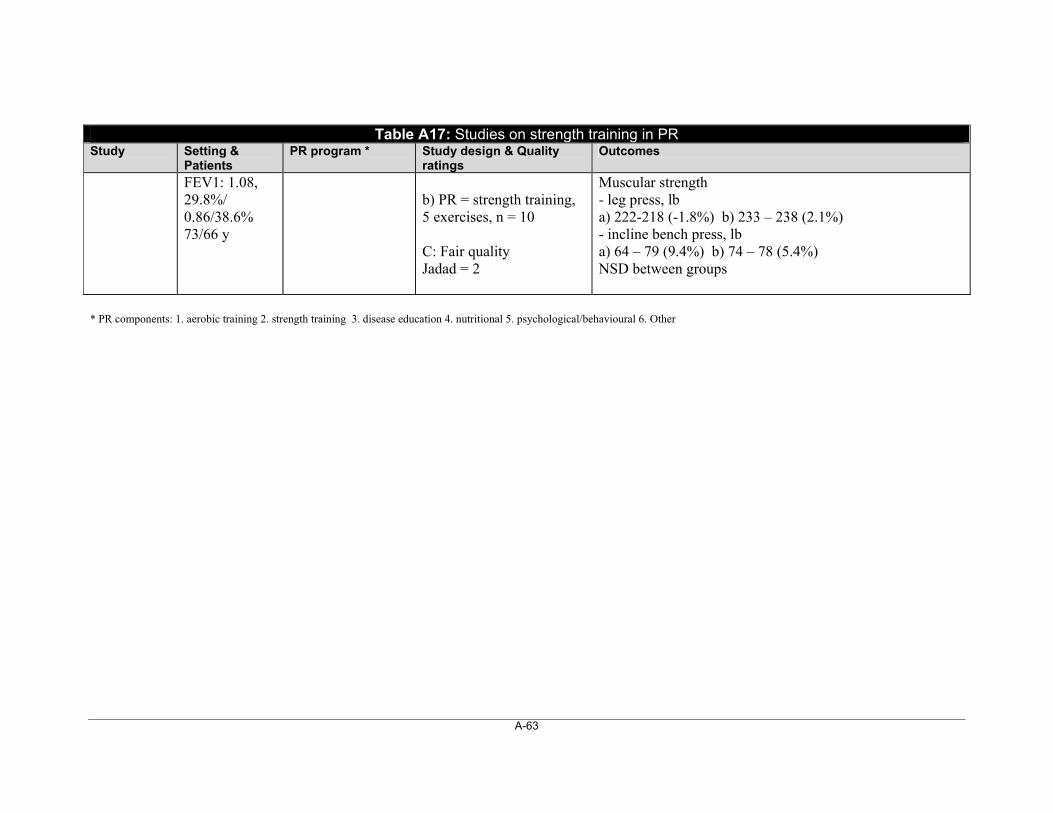
A-63
Table A17: Studies on strength training in PR Study Setting &
Patients PR program * Study design & Quality
ratings Outcomes
FEV1: 1.08, 29.8%/ 0.86/38.6% 73/66 y
b) PR = strength training, 5 exercises, n = 10 C: Fair quality Jadad = 2
Muscular strength - leg press, lb a) 222-218 (-1.8%) b) 233 – 238 (2.1%) - incline bench press, lb a) 64 – 79 (9.4%) b) 74 – 78 (5.4%) NSD between groups
* PR components: 1. aerobic training 2. strength training 3. disease education 4. nutritional 5. psychological/behavioural 6. Other
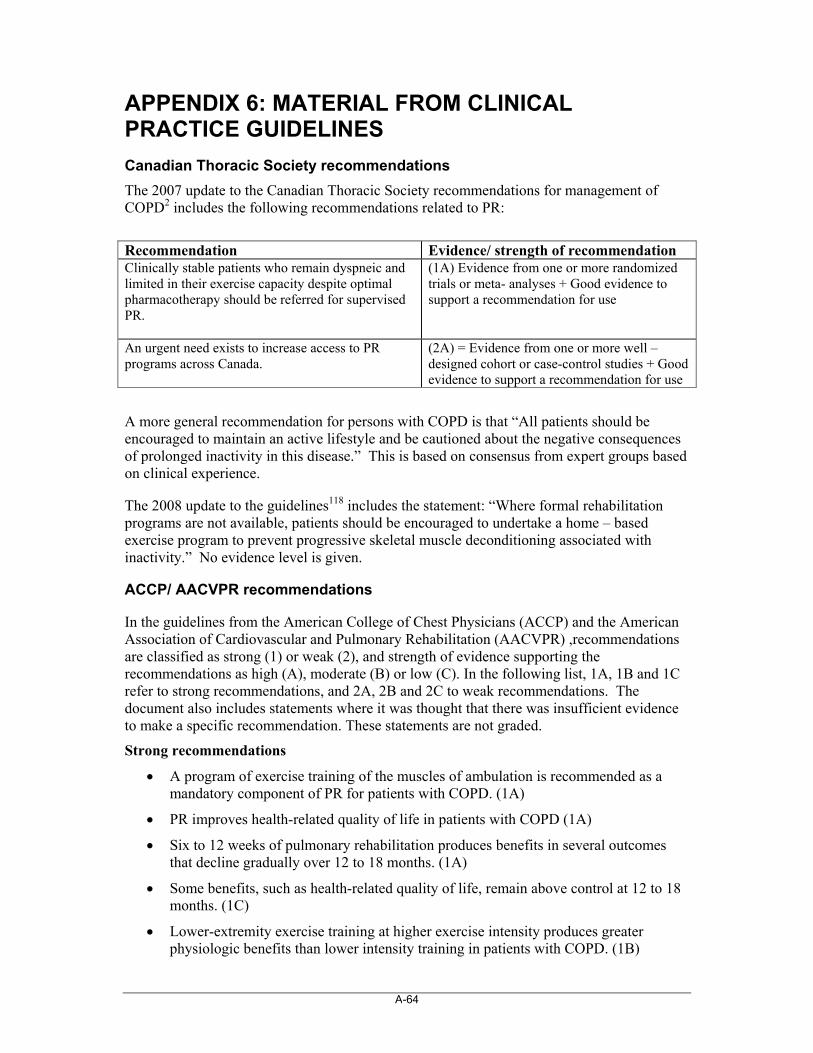
A-64
APPENDIX 6: MATERIAL FROM CLINICAL PRACTICE GUIDELINES
Canadian Thoracic Society recommendations
The 2007 update to the Canadian Thoracic Society recommendations for management of COPD2 includes the following recommendations related to PR:
Recommendation Evidence/ strength of recommendation Clinically stable patients who remain dyspneic and limited in their exercise capacity despite optimal pharmacotherapy should be referred for supervised PR.
(1A) Evidence from one or more randomized trials or meta- analyses + Good evidence to support a recommendation for use
An urgent need exists to increase access to PR programs across Canada.
(2A) = Evidence from one or more well – designed cohort or case-control studies + Good evidence to support a recommendation for use
A more general recommendation for persons with COPD is that “All patients should be encouraged to maintain an active lifestyle and be cautioned about the negative consequences of prolonged inactivity in this disease.” This is based on consensus from expert groups based on clinical experience.
The 2008 update to the guidelines118 includes the statement: “Where formal rehabilitation programs are not available, patients should be encouraged to undertake a home – based exercise program to prevent progressive skeletal muscle deconditioning associated with inactivity.” No evidence level is given.
ACCP/ AACVPR recommendations
In the guidelines from the American College of Chest Physicians (ACCP) and the American Association of Cardiovascular and Pulmonary Rehabilitation (AACVPR) ,recommendations are classified as strong (1) or weak (2), and strength of evidence supporting the recommendations as high (A), moderate (B) or low (C). In the following list, 1A, 1B and 1C refer to strong recommendations, and 2A, 2B and 2C to weak recommendations. The document also includes statements where it was thought that there was insufficient evidence to make a specific recommendation. These statements are not graded.
Strong recommendations
A program of exercise training of the muscles of ambulation is recommended as a mandatory component of PR for patients with COPD. (1A)
PR improves health-related quality of life in patients with COPD (1A)
Six to 12 weeks of pulmonary rehabilitation produces benefits in several outcomes that decline gradually over 12 to 18 months. (1A)
Some benefits, such as health-related quality of life, remain above control at 12 to 18 months. (1C)
Lower-extremity exercise training at higher exercise intensity produces greater physiologic benefits than lower intensity training in patients with COPD. (1B)

A-65
Both low- and high intensity exercise training produce clinical benefits for patients with COPD. (1A)
Addition of a strength training component to a program of pulmonary rehabilitation increases muscle strength and muscle mass. (1A)
Unsupported endurance training of the upper extremities is beneficial in patients with COPD and should be included in PR programs. (1A)
The scientific evidence does not support the routine use of inspiratory muscle training as an essential component of PR. (1B)
Education should be an integral component of PR. Education should include information on collaborative self-management and prevention and treatment of exacerbations. (1B)
Supplemental oxygen should be used during rehabilitative exercise training in patients with severe exercise-induced hypoxemia. (1C)
Weak recommendations
PR reduces the number of hospital days and other measures of health-care utilization in patients with COPD. (2B)
PR is cost-effective in patients with COPD (2C)
There are psychosocial benefits from comprehensive PR programs in patients with COPD. (2B)
Longer PR programs (12 weeks) produce greater sustained benefits than shorter programs. (2B)
Maintenance strategies following PR have a modest effect on long-term outcomes. (2C)
Current scientific evidence does not support the routine use of anabolic agents in PR for patients with COPD. (2C)
There is minimal evidence to support the benefits of psychosocial interventions as a single therapeutic modality. (2C)
Administering supplemental oxygen during high-intensity exercise programs in patients without exercise-induced hypoxemia may improve gains in exercise endurance. (2C)
As an adjunct to exercise training in selected patients with severe COPD, non-invasive ventilation produces modest additional improvements in exercise performance. (2B)
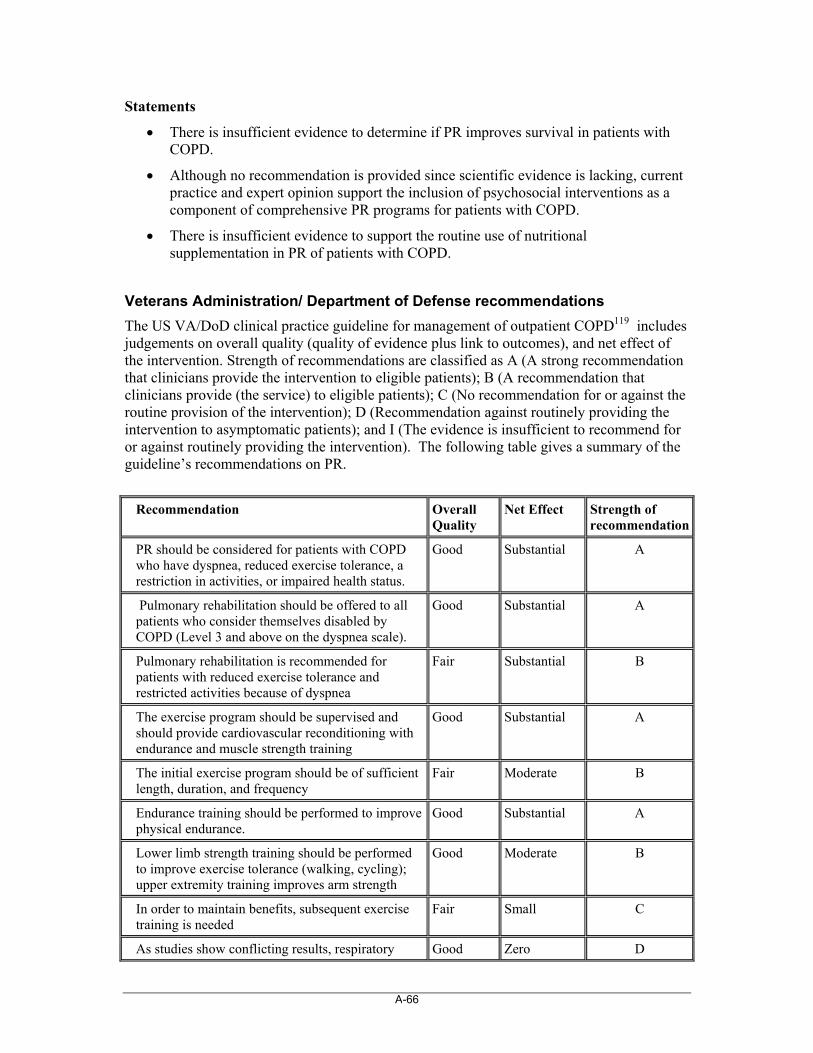
A-66
Statements
There is insufficient evidence to determine if PR improves survival in patients with COPD.
Although no recommendation is provided since scientific evidence is lacking, current practice and expert opinion support the inclusion of psychosocial interventions as a component of comprehensive PR programs for patients with COPD.
There is insufficient evidence to support the routine use of nutritional supplementation in PR of patients with COPD.
Veterans Administration/ Department of Defense recommendations
The US VA/DoD clinical practice guideline for management of outpatient COPD119 includes judgements on overall quality (quality of evidence plus link to outcomes), and net effect of the intervention. Strength of recommendations are classified as A (A strong recommendation that clinicians provide the intervention to eligible patients); B (A recommendation that clinicians provide (the service) to eligible patients); C (No recommendation for or against the routine provision of the intervention); D (Recommendation against routinely providing the intervention to asymptomatic patients); and I (The evidence is insufficient to recommend for or against routinely providing the intervention). The following table gives a summary of the guideline’s recommendations on PR.
Recommendation Overall Quality
Net Effect Strength of recommendation
PR should be considered for patients with COPD who have dyspnea, reduced exercise tolerance, a restriction in activities, or impaired health status.
Good Substantial A
Pulmonary rehabilitation should be offered to all patients who consider themselves disabled by COPD (Level 3 and above on the dyspnea scale).
Good Substantial A
Pulmonary rehabilitation is recommended for patients with reduced exercise tolerance and restricted activities because of dyspnea
Fair Substantial B
The exercise program should be supervised and should provide cardiovascular reconditioning with endurance and muscle strength training
Good Substantial A
The initial exercise program should be of sufficient length, duration, and frequency
Fair Moderate B
Endurance training should be performed to improve physical endurance.
Good Substantial A
Lower limb strength training should be performed to improve exercise tolerance (walking, cycling); upper extremity training improves arm strength
Good Moderate B
In order to maintain benefits, subsequent exercise training is needed
Fair Small C
As studies show conflicting results, respiratory Good Zero D
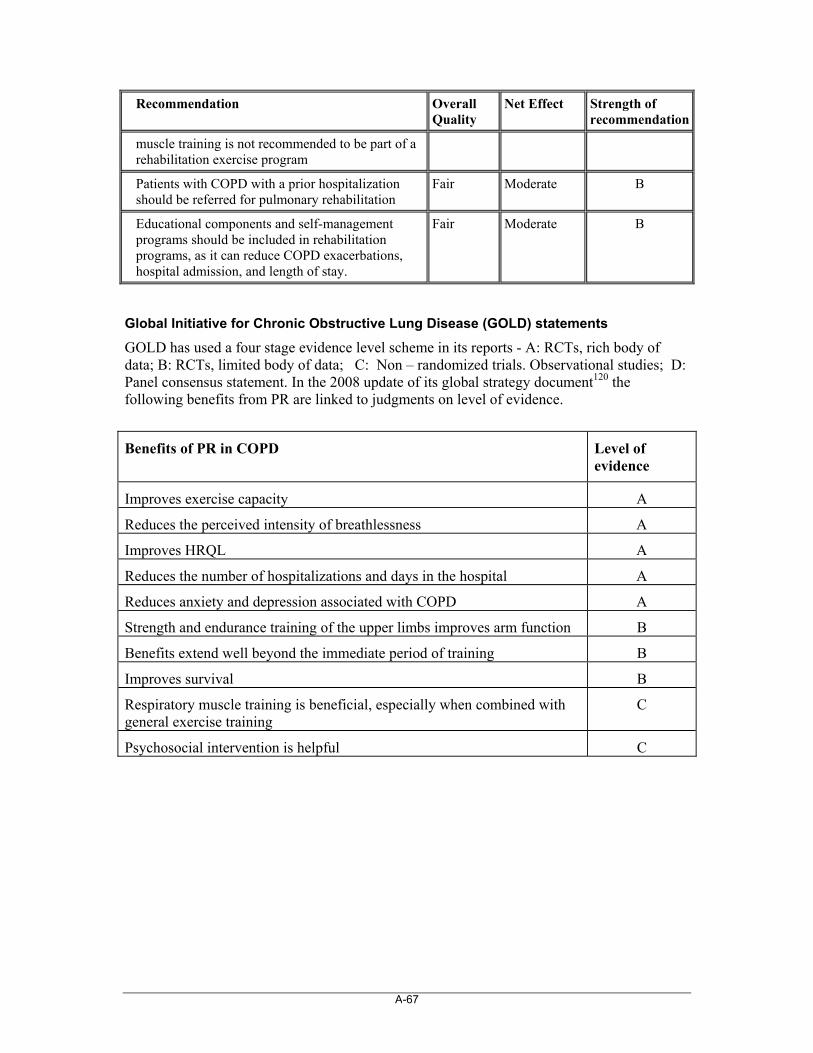
A-67
Recommendation Overall Quality
Net Effect Strength of recommendation
muscle training is not recommended to be part of a rehabilitation exercise program
Patients with COPD with a prior hospitalization should be referred for pulmonary rehabilitation
Fair Moderate B
Educational components and self-management programs should be included in rehabilitation programs, as it can reduce COPD exacerbations, hospital admission, and length of stay.
Fair Moderate B
Global Initiative for Chronic Obstructive Lung Disease (GOLD) statements
GOLD has used a four stage evidence level scheme in its reports - A: RCTs, rich body of data; B: RCTs, limited body of data; C: Non – randomized trials. Observational studies; D: Panel consensus statement. In the 2008 update of its global strategy document120 the following benefits from PR are linked to judgments on level of evidence.
Benefits of PR in COPD
Level of evidence
Improves exercise capacity A
Reduces the perceived intensity of breathlessness A
Improves HRQL A
Reduces the number of hospitalizations and days in the hospital A
Reduces anxiety and depression associated with COPD A
Strength and endurance training of the upper limbs improves arm function B
Benefits extend well beyond the immediate period of training B
Improves survival B
Respiratory muscle training is beneficial, especially when combined with general exercise training
C
Psychosocial intervention is helpful C

A-68
These points are informed in the text by the following additional statements:
Benefits of PR in COPD
Level of evidence
COPD patients in all stages of disease appear to benefit from exercise training programs, improving with respect to both exercise tolerance and symptoms of dyspnea and fatigue
A
Benefit does wane after a rehabilitation program ends, but if exercise training is maintained at home the patient’s health status remains above pre- rehabilitation levels.
B
There is no consensus on whether repeated rehabilitation courses enable patients to sustain benefits gained through the initial course
N/A
Educational and exercise training components are usually conducted in groups, normally with 6 – 8 individuals per class
D
Benefits have been seen in patients with a wide range of disability, although those who are chair-bound appear unlikely to respond even to home visiting programs
A
Stratification by breathlessness using the MRC questionnaire may be helpful in selecting patients most likely to benefit. Those with MRC Grade 5 dyspnea may not benefit
B
Some data indicate that continuing smokers are less likely to complete PR programs than non-smokers.
B
Use of a simple wheeled walking aid seems to improve walking distance and reduces breathlessness in severely disabled COPD patients.
C
The minimum length of an effective rehabilitation program is 6 weeks; the longer the program continues, the more effective the results.
B
A study from the UK provided evidence that an intensive, multidisciplinary rehabilitation program was cost – effective and decreased the use of health services.
B
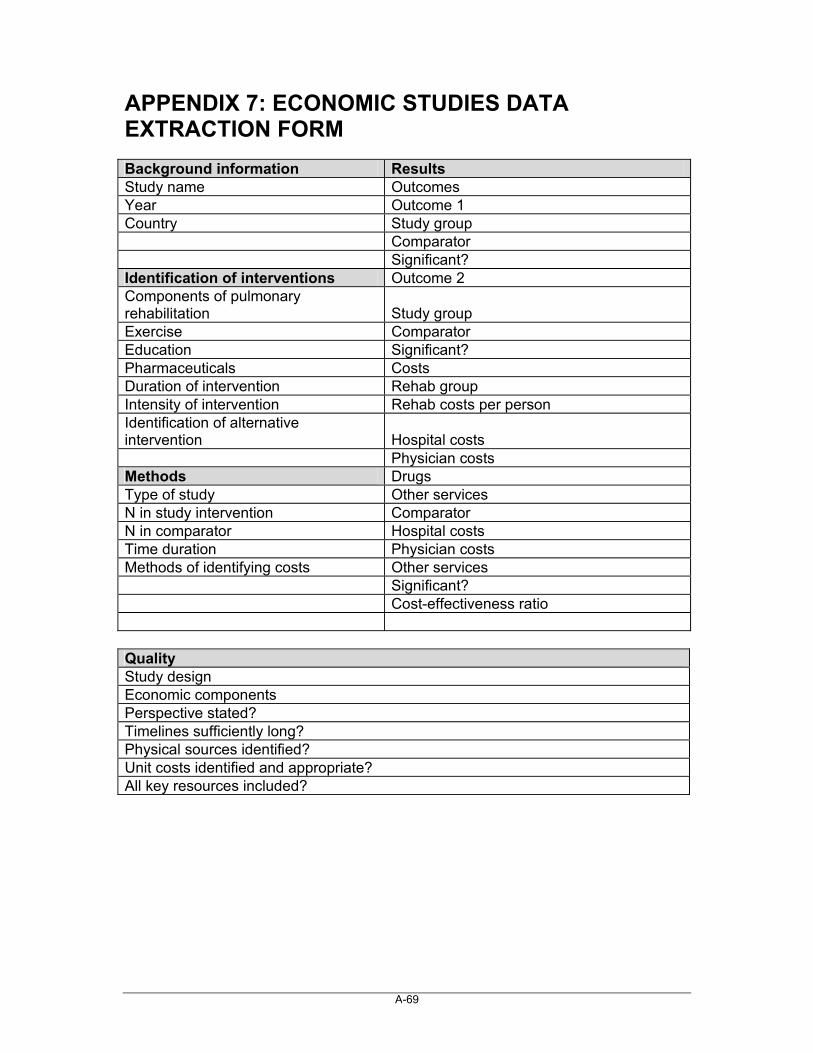
A-69
APPENDIX 7: ECONOMIC STUDIES DATA EXTRACTION FORM Background information Results Study name Outcomes Year Outcome 1 Country Study group Comparator Significant? Identification of interventions Outcome 2 Components of pulmonary rehabilitation Study group Exercise Comparator Education Significant? Pharmaceuticals Costs Duration of intervention Rehab group Intensity of intervention Rehab costs per person Identification of alternative intervention Hospital costs Physician costs Methods Drugs Type of study Other services N in study intervention Comparator N in comparator Hospital costs Time duration Physician costs Methods of identifying costs Other services Significant? Cost-effectiveness ratio Quality Study design Economic components Perspective stated? Timelines sufficiently long? Physical sources identified? Unit costs identified and appropriate? All key resources included?
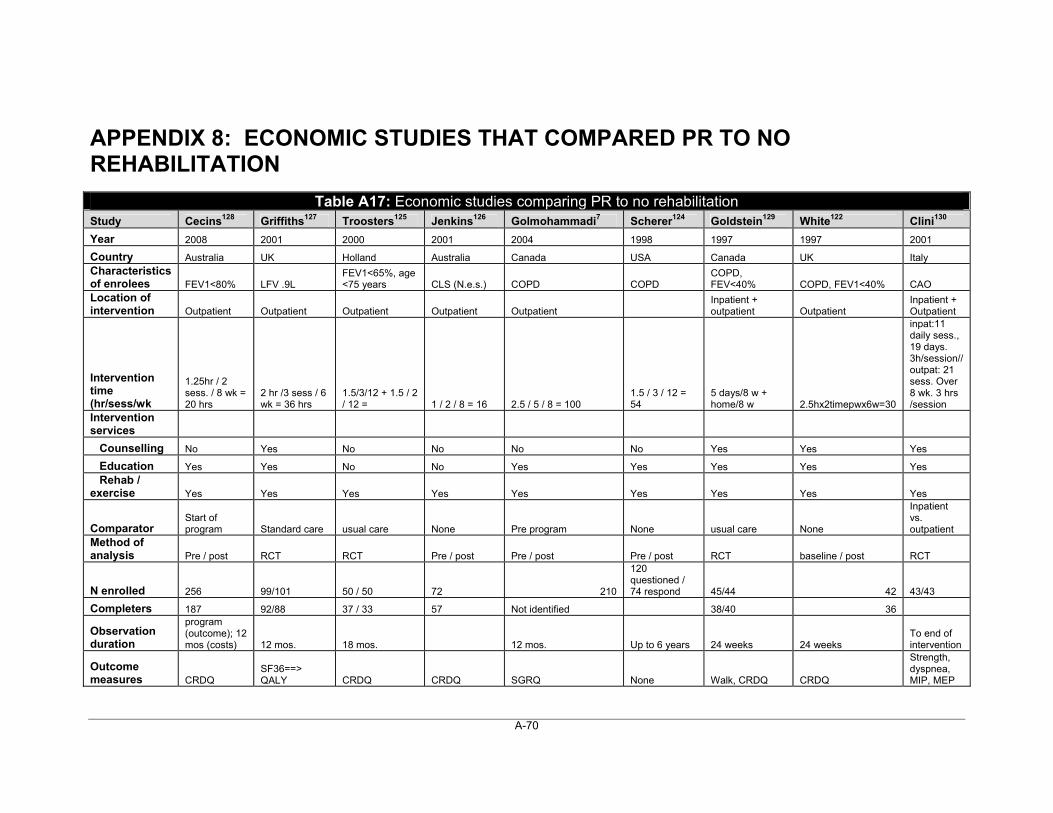
A-70
APPENDIX 8: ECONOMIC STUDIES THAT COMPARED PR TO NO REHABILITATION
Table A17: Economic studies comparing PR to no rehabilitation Study Cecins128 Griffiths127 Troosters125 Jenkins126 Golmohammadi7 Scherer124 Goldstein129 White122 Clini130
Year 2008 2001 2000 2001 2004 1998 1997 1997 2001
Country Australia UK Holland Australia Canada USA Canada UK Italy Characteristics of enrolees FEV1<80% LFV .9L
FEV1<65%, age <75 years CLS (N.e.s.) COPD COPD
COPD, FEV<40% COPD, FEV1<40% CAO
Location of intervention Outpatient Outpatient Outpatient Outpatient Outpatient
Inpatient + outpatient Outpatient
Inpatient + Outpatient
Intervention time (hr/sess/wk
1.25hr / 2 sess. / 8 wk = 20 hrs
2 hr /3 sess / 6 wk = 36 hrs
1.5/3/12 + 1.5 / 2 / 12 = 1 / 2 / 8 = 16 2.5 / 5 / 8 = 100
1.5 / 3 / 12 = 54
5 days/8 w + home/8 w 2.5hx2timepwx6w=30
inpat:11 daily sess., 19 days. 3h/session// outpat: 21 sess. Over 8 wk. 3 hrs /session
Intervention services
Counselling No Yes No No No No Yes Yes Yes
Education Yes Yes No No Yes Yes Yes Yes Yes Rehab / exercise Yes Yes Yes Yes Yes Yes Yes Yes Yes
Comparator Start of program Standard care usual care None Pre program None usual care None
Inpatient vs. outpatient
Method of analysis Pre / post RCT RCT Pre / post Pre / post Pre / post RCT baseline / post RCT
N enrolled 256 99/101 50 / 50 72 210
120 questioned / 74 respond 45/44 42 43/43
Completers 187 92/88 37 / 33 57 Not identified 38/40 36
Observation duration
program (outcome); 12 mos (costs) 12 mos. 18 mos. 12 mos. Up to 6 years 24 weeks 24 weeks
To end of intervention
Outcome measures CRDQ
SF36==> QALY CRDQ CRDQ SGRQ None Walk, CRDQ CRDQ
Strength, dyspnea, MIP, MEP
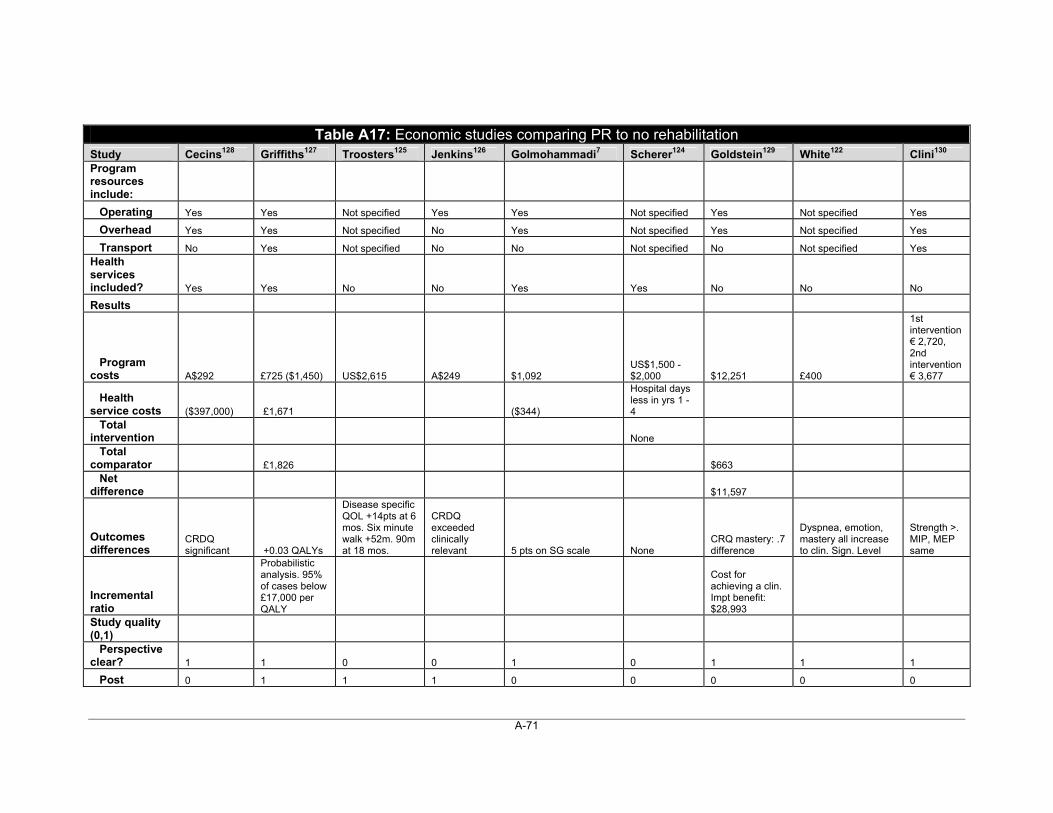
A-71
Table A17: Economic studies comparing PR to no rehabilitation Study Cecins128 Griffiths127 Troosters125 Jenkins126 Golmohammadi7 Scherer124 Goldstein129 White122 Clini130 Program resources include:
Operating Yes Yes Not specified Yes Yes Not specified Yes Not specified Yes
Overhead Yes Yes Not specified No Yes Not specified Yes Not specified Yes
Transport No Yes Not specified No No Not specified No Not specified Yes Health services included? Yes Yes No No Yes Yes No No No
Results
Program costs A$292 £725 ($1,450) US$2,615 A$249 $1,092
US$1,500 - $2,000 $12,251 £400
1st intervention € 2,720, 2nd intervention € 3,677
Health service costs ($397,000) £1,671 ($344)
Hospital days less in yrs 1 - 4
Total intervention None Total comparator £1,826 $663 Net difference $11,597
Outcomes differences
CRDQ significant +0.03 QALYs
Disease specific QOL +14pts at 6 mos. Six minute walk +52m. 90m at 18 mos.
CRDQ exceeded clinically relevant 5 pts on SG scale None
CRQ mastery: .7 difference
Dyspnea, emotion, mastery all increase to clin. Sign. Level
Strength >. MIP, MEP same
Incremental ratio
Probabilistic analysis. 95% of cases below £17,000 per QALY
Cost for achieving a clin. Impt benefit: $28,993
Study quality (0,1) Perspective clear? 1 1 0 0 1 0 1 1 1
Post 0 1 1 1 0 0 0 0 0
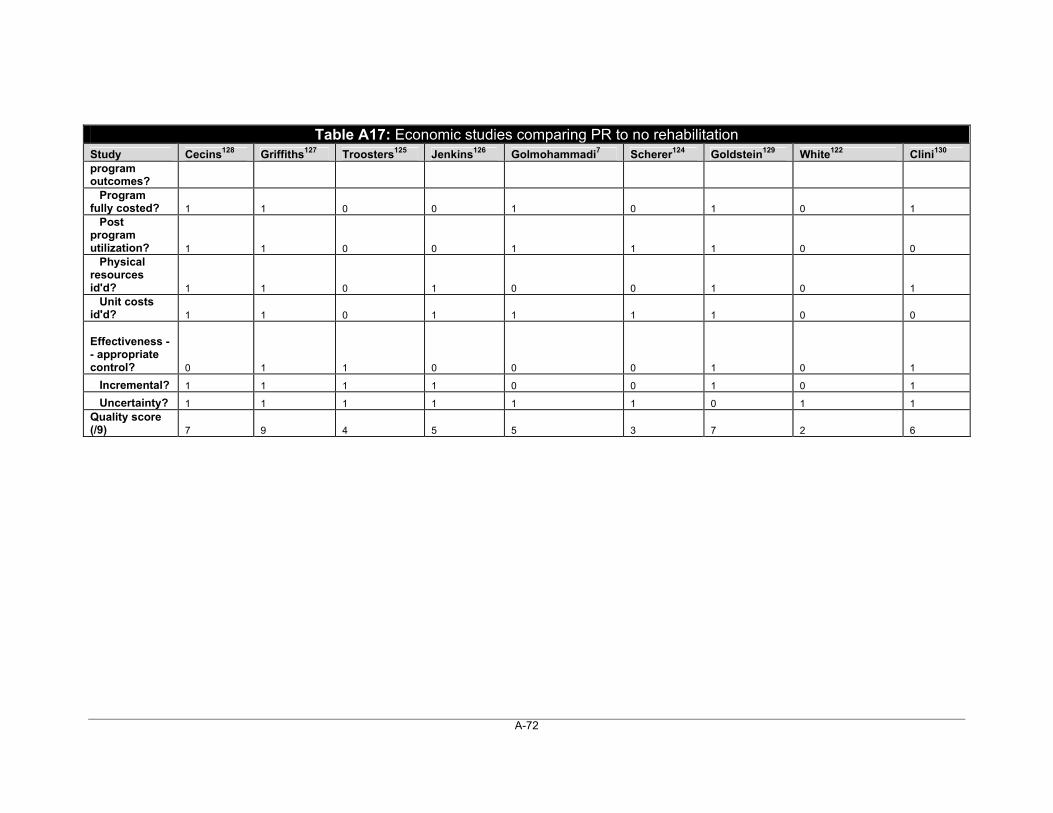
A-72
Table A17: Economic studies comparing PR to no rehabilitation Study Cecins128 Griffiths127 Troosters125 Jenkins126 Golmohammadi7 Scherer124 Goldstein129 White122 Clini130 program outcomes? Program fully costed? 1 1 0 0 1 0 1 0 1 Post program utilization? 1 1 0 0 1 1 1 0 0 Physical resources id'd? 1 1 0 1 0 0 1 0 1 Unit costs id'd? 1 1 0 1 1 1 1 0 0 Effectiveness -- appropriate control? 0 1 1 0 0 0 1 0 1
Incremental? 1 1 1 1 0 0 1 0 1
Uncertainty? 1 1 1 1 1 1 0 1 1 Quality score (/9) 7 9 4 5 5 3 7 2 6
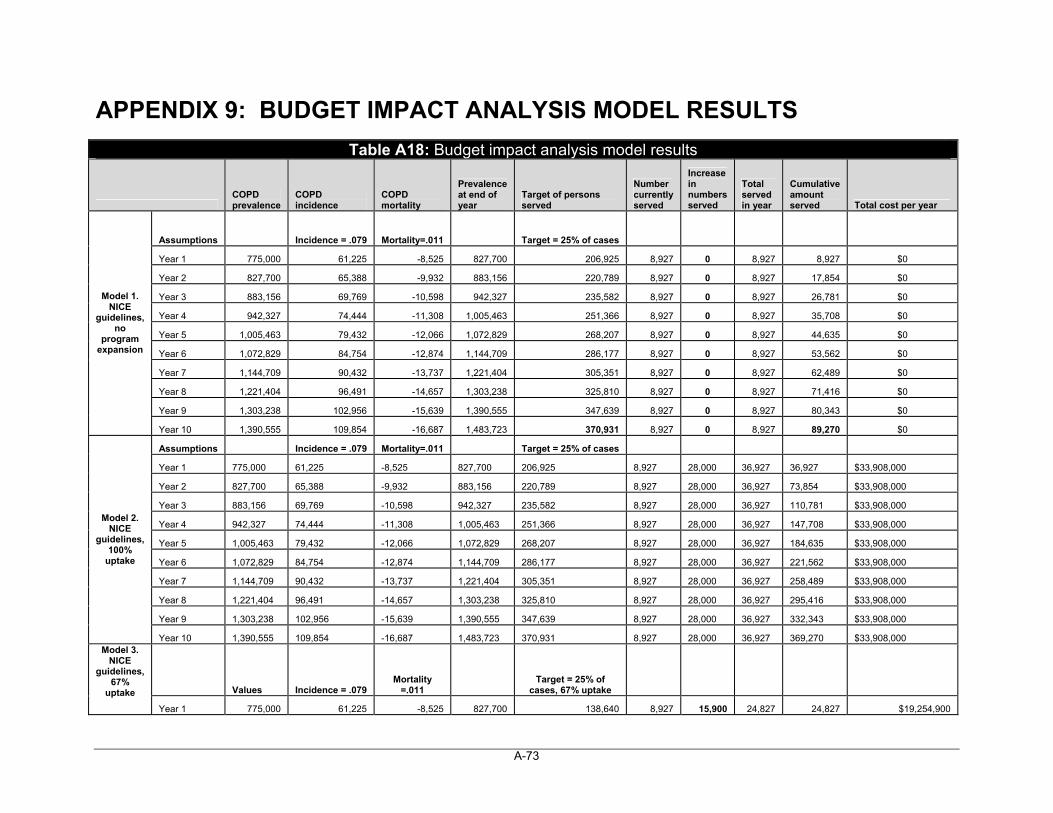
A-73
APPENDIX 9: BUDGET IMPACT ANALYSIS MODEL RESULTS
Table A18: Budget impact analysis model results
COPD prevalence
COPD incidence
COPD mortality
Prevalence at end of year
Target of persons served
Number currently served
Increase in numbers served
Total served in year
Cumulative amount served Total cost per year
Assumptions Incidence = .079 Mortality=.011 Target = 25% of cases
Year 1 775,000 61,225 -8,525 827,700 206,925 8,927 0 8,927 8,927 $0
Year 2 827,700 65,388 -9,932 883,156 220,789 8,927 0 8,927 17,854 $0
Year 3 883,156 69,769 -10,598 942,327 235,582 8,927 0 8,927 26,781 $0
Year 4 942,327 74,444 -11,308 1,005,463 251,366 8,927 0 8,927 35,708 $0
Year 5 1,005,463 79,432 -12,066 1,072,829 268,207 8,927 0 8,927 44,635 $0
Year 6 1,072,829 84,754 -12,874 1,144,709 286,177 8,927 0 8,927 53,562 $0
Year 7 1,144,709 90,432 -13,737 1,221,404 305,351 8,927 0 8,927 62,489 $0
Year 8 1,221,404 96,491 -14,657 1,303,238 325,810 8,927 0 8,927 71,416 $0
Year 9 1,303,238 102,956 -15,639 1,390,555 347,639 8,927 0 8,927 80,343 $0
Model 1. NICE
guidelines, no
program expansion
Year 10 1,390,555 109,854 -16,687 1,483,723 370,931 8,927 0 8,927 89,270 $0
Assumptions Incidence = .079 Mortality=.011 Target = 25% of cases
Year 1 775,000 61,225 -8,525 827,700 206,925 8,927 28,000 36,927 36,927 $33,908,000
Year 2 827,700 65,388 -9,932 883,156 220,789 8,927 28,000 36,927 73,854 $33,908,000
Year 3 883,156 69,769 -10,598 942,327 235,582 8,927 28,000 36,927 110,781 $33,908,000
Year 4 942,327 74,444 -11,308 1,005,463 251,366 8,927 28,000 36,927 147,708 $33,908,000
Year 5 1,005,463 79,432 -12,066 1,072,829 268,207 8,927 28,000 36,927 184,635 $33,908,000
Year 6 1,072,829 84,754 -12,874 1,144,709 286,177 8,927 28,000 36,927 221,562 $33,908,000
Year 7 1,144,709 90,432 -13,737 1,221,404 305,351 8,927 28,000 36,927 258,489 $33,908,000
Year 8 1,221,404 96,491 -14,657 1,303,238 325,810 8,927 28,000 36,927 295,416 $33,908,000
Year 9 1,303,238 102,956 -15,639 1,390,555 347,639 8,927 28,000 36,927 332,343 $33,908,000
Model 2. NICE
guidelines, 100%
uptake
Year 10 1,390,555 109,854 -16,687 1,483,723 370,931 8,927 28,000 36,927 369,270 $33,908,000
Values Incidence = .079 Mortality
=.011 Target = 25% of
cases, 67% uptake
Model 3. NICE
guidelines, 67%
uptake
Year 1 775,000 61,225 -8,525 827,700 138,640 8,927 15,900 24,827 24,827 $19,254,900
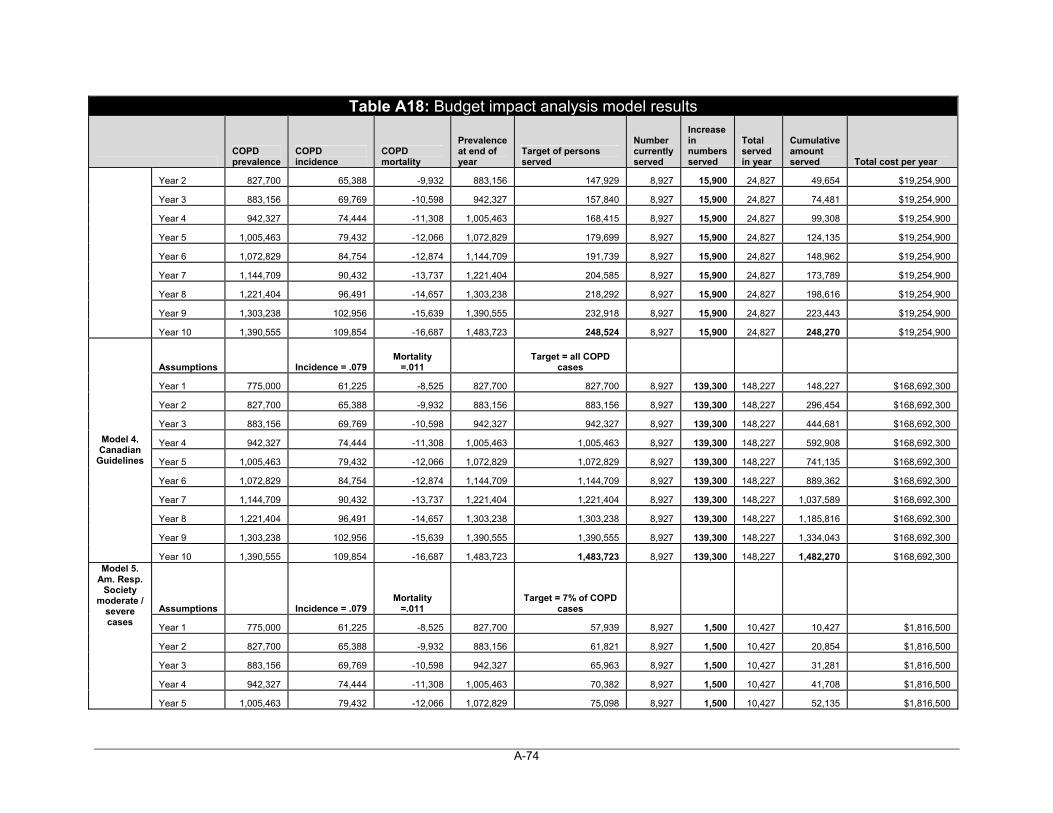
A-74
Table A18: Budget impact analysis model results
COPD prevalence
COPD incidence
COPD mortality
Prevalence at end of year
Target of persons served
Number currently served
Increase in numbers served
Total served in year
Cumulative amount served Total cost per year
Year 2 827,700 65,388 -9,932 883,156 147,929 8,927 15,900 24,827 49,654 $19,254,900
Year 3 883,156 69,769 -10,598 942,327 157,840 8,927 15,900 24,827 74,481 $19,254,900
Year 4 942,327 74,444 -11,308 1,005,463 168,415 8,927 15,900 24,827 99,308 $19,254,900
Year 5 1,005,463 79,432 -12,066 1,072,829 179,699 8,927 15,900 24,827 124,135 $19,254,900
Year 6 1,072,829 84,754 -12,874 1,144,709 191,739 8,927 15,900 24,827 148,962 $19,254,900
Year 7 1,144,709 90,432 -13,737 1,221,404 204,585 8,927 15,900 24,827 173,789 $19,254,900
Year 8 1,221,404 96,491 -14,657 1,303,238 218,292 8,927 15,900 24,827 198,616 $19,254,900
Year 9 1,303,238 102,956 -15,639 1,390,555 232,918 8,927 15,900 24,827 223,443 $19,254,900
Year 10 1,390,555 109,854 -16,687 1,483,723 248,524 8,927 15,900 24,827 248,270 $19,254,900
Assumptions Incidence = .079 Mortality
=.011 Target = all COPD
cases
Year 1 775,000 61,225 -8,525 827,700 827,700 8,927 139,300 148,227 148,227 $168,692,300
Year 2 827,700 65,388 -9,932 883,156 883,156 8,927 139,300 148,227 296,454 $168,692,300
Year 3 883,156 69,769 -10,598 942,327 942,327 8,927 139,300 148,227 444,681 $168,692,300
Year 4 942,327 74,444 -11,308 1,005,463 1,005,463 8,927 139,300 148,227 592,908 $168,692,300
Year 5 1,005,463 79,432 -12,066 1,072,829 1,072,829 8,927 139,300 148,227 741,135 $168,692,300
Year 6 1,072,829 84,754 -12,874 1,144,709 1,144,709 8,927 139,300 148,227 889,362 $168,692,300
Year 7 1,144,709 90,432 -13,737 1,221,404 1,221,404 8,927 139,300 148,227 1,037,589 $168,692,300
Year 8 1,221,404 96,491 -14,657 1,303,238 1,303,238 8,927 139,300 148,227 1,185,816 $168,692,300
Year 9 1,303,238 102,956 -15,639 1,390,555 1,390,555 8,927 139,300 148,227 1,334,043 $168,692,300
Model 4. Canadian
Guidelines
Year 10 1,390,555 109,854 -16,687 1,483,723 1,483,723 8,927 139,300 148,227 1,482,270 $168,692,300
Assumptions Incidence = .079 Mortality
=.011 Target = 7% of COPD
cases
Year 1 775,000 61,225 -8,525 827,700 57,939 8,927 1,500 10,427 10,427 $1,816,500
Year 2 827,700 65,388 -9,932 883,156 61,821 8,927 1,500 10,427 20,854 $1,816,500
Year 3 883,156 69,769 -10,598 942,327 65,963 8,927 1,500 10,427 31,281 $1,816,500
Year 4 942,327 74,444 -11,308 1,005,463 70,382 8,927 1,500 10,427 41,708 $1,816,500
Model 5. Am. Resp.
Society moderate /
severe cases
Year 5 1,005,463 79,432 -12,066 1,072,829 75,098 8,927 1,500 10,427 52,135 $1,816,500
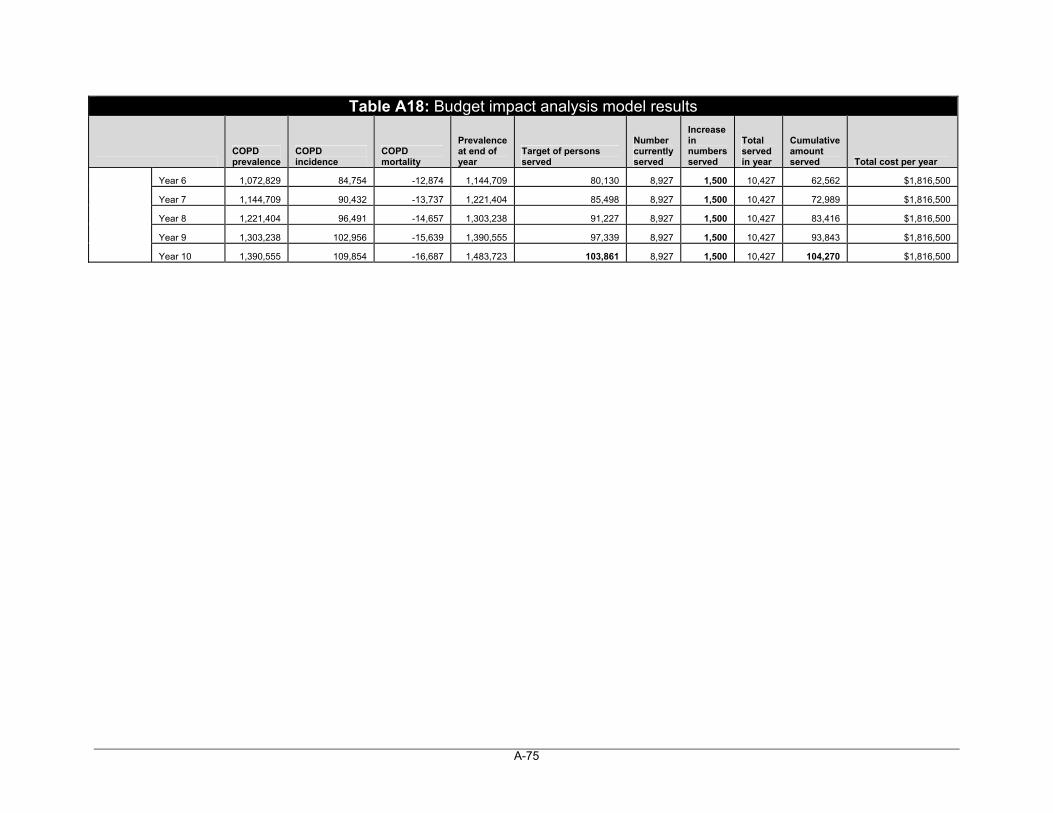
A-75
Table A18: Budget impact analysis model results
COPD prevalence
COPD incidence
COPD mortality
Prevalence at end of year
Target of persons served
Number currently served
Increase in numbers served
Total served in year
Cumulative amount served Total cost per year
Year 6 1,072,829 84,754 -12,874 1,144,709 80,130 8,927 1,500 10,427 62,562 $1,816,500
Year 7 1,144,709 90,432 -13,737 1,221,404 85,498 8,927 1,500 10,427 72,989 $1,816,500
Year 8 1,221,404 96,491 -14,657 1,303,238 91,227 8,927 1,500 10,427 83,416 $1,816,500
Year 9 1,303,238 102,956 -15,639 1,390,555 97,339 8,927 1,500 10,427 93,843 $1,816,500
Year 10 1,390,555 109,854 -16,687 1,483,723 103,861 8,927 1,500 10,427 104,270 $1,816,500
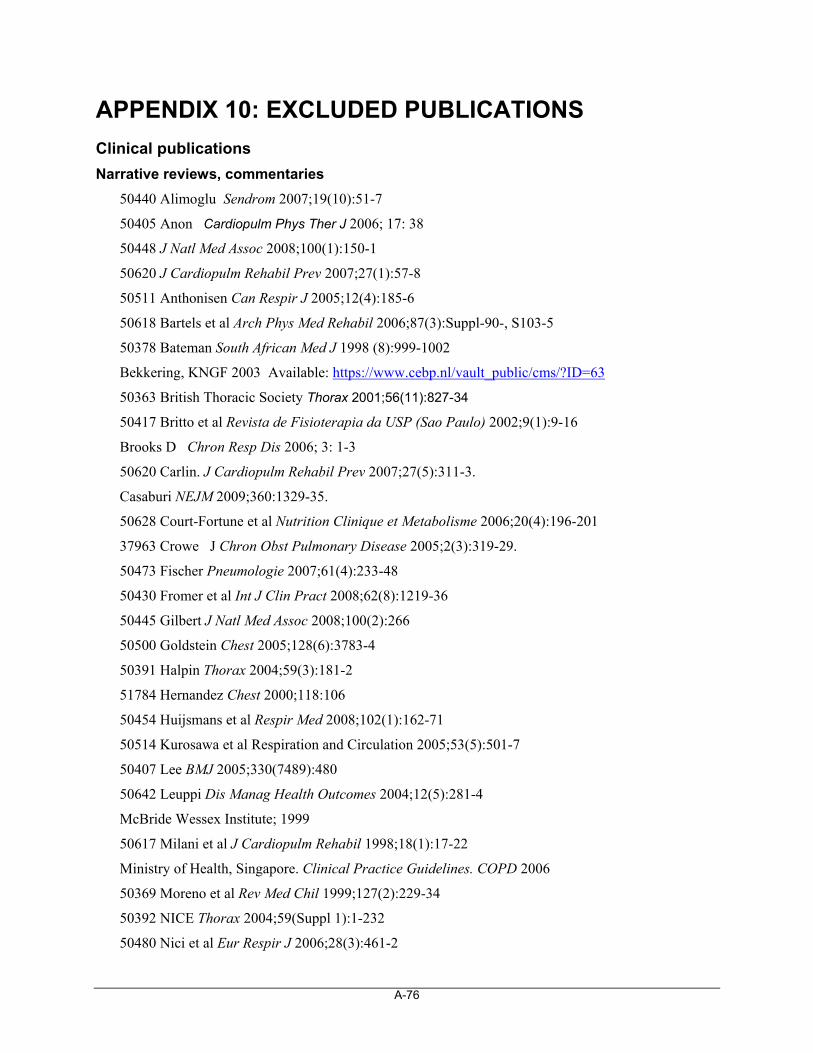
A-76
APPENDIX 10: EXCLUDED PUBLICATIONS
Clinical publications
Narrative reviews, commentaries
50440 Alimoglu Sendrom 2007;19(10):51-7
50405 Anon Cardiopulm Phys Ther J 2006; 17: 38
50448 J Natl Med Assoc 2008;100(1):150-1
50620 J Cardiopulm Rehabil Prev 2007;27(1):57-8
50511 Anthonisen Can Respir J 2005;12(4):185-6
50618 Bartels et al Arch Phys Med Rehabil 2006;87(3):Suppl-90-, S103-5
50378 Bateman South African Med J 1998 (8):999-1002
Bekkering, KNGF 2003 Available: https://www.cebp.nl/vault_public/cms/?ID=63
50363 British Thoracic Society Thorax 2001;56(11):827-34
50417 Britto et al Revista de Fisioterapia da USP (Sao Paulo) 2002;9(1):9-16
Brooks D Chron Resp Dis 2006; 3: 1-3
50620 Carlin. J Cardiopulm Rehabil Prev 2007;27(5):311-3.
Casaburi NEJM 2009;360:1329-35.
50628 Court-Fortune et al Nutrition Clinique et Metabolisme 2006;20(4):196-201
37963 Crowe J Chron Obst Pulmonary Disease 2005;2(3):319-29.
50473 Fischer Pneumologie 2007;61(4):233-48
50430 Fromer et al Int J Clin Pract 2008;62(8):1219-36
50445 Gilbert J Natl Med Assoc 2008;100(2):266
50500 Goldstein Chest 2005;128(6):3783-4
50391 Halpin Thorax 2004;59(3):181-2
51784 Hernandez Chest 2000;118:106
50454 Huijsmans et al Respir Med 2008;102(1):162-71
50514 Kurosawa et al Respiration and Circulation 2005;53(5):501-7
50407 Lee BMJ 2005;330(7489):480
50642 Leuppi Dis Manag Health Outcomes 2004;12(5):281-4
McBride Wessex Institute; 1999
50617 Milani et al J Cardiopulm Rehabil 1998;18(1):17-22
Ministry of Health, Singapore. Clinical Practice Guidelines. COPD 2006
50369 Moreno et al Rev Med Chil 1999;127(2):229-34
50392 NICE Thorax 2004;59(Suppl 1):1-232
50480 Nici et al Eur Respir J 2006;28(3):461-2
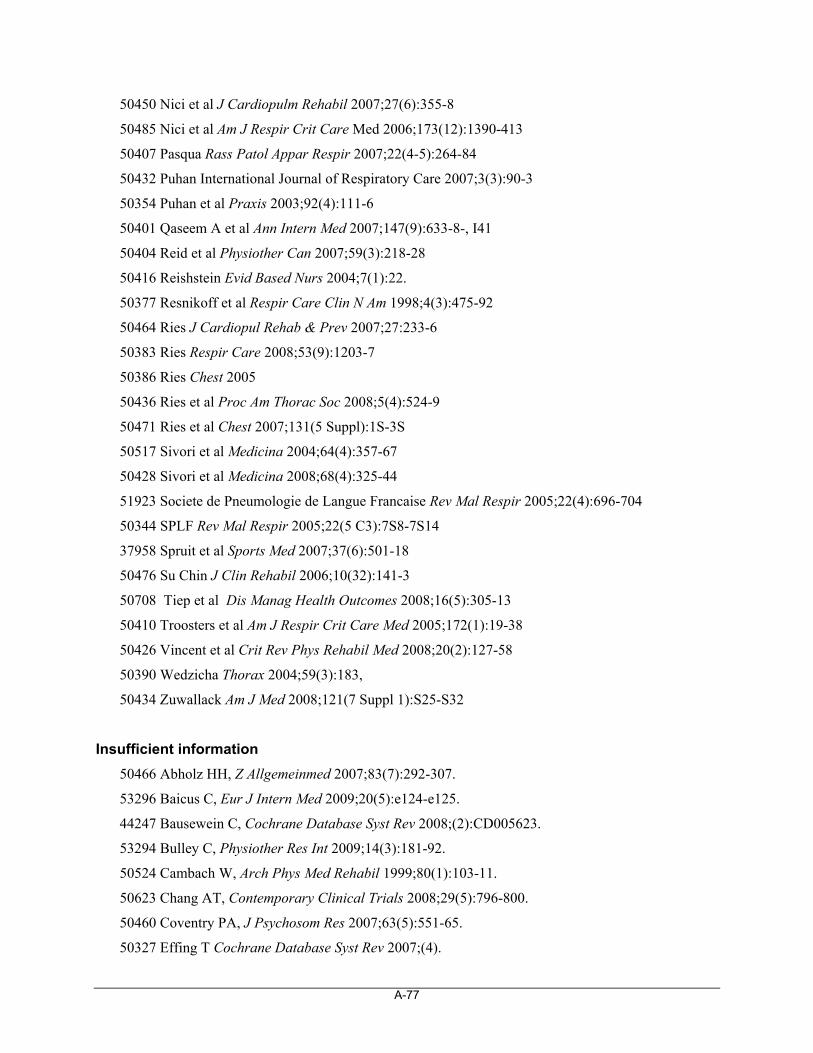
A-77
50450 Nici et al J Cardiopulm Rehabil 2007;27(6):355-8
50485 Nici et al Am J Respir Crit Care Med 2006;173(12):1390-413
50407 Pasqua Rass Patol Appar Respir 2007;22(4-5):264-84
50432 Puhan International Journal of Respiratory Care 2007;3(3):90-3
50354 Puhan et al Praxis 2003;92(4):111-6
50401 Qaseem A et al Ann Intern Med 2007;147(9):633-8-, I41
50404 Reid et al Physiother Can 2007;59(3):218-28
50416 Reishstein Evid Based Nurs 2004;7(1):22.
50377 Resnikoff et al Respir Care Clin N Am 1998;4(3):475-92
50464 Ries J Cardiopul Rehab & Prev 2007;27:233-6
50383 Ries Respir Care 2008;53(9):1203-7
50386 Ries Chest 2005
50436 Ries et al Proc Am Thorac Soc 2008;5(4):524-9
50471 Ries et al Chest 2007;131(5 Suppl):1S-3S
50517 Sivori et al Medicina 2004;64(4):357-67
50428 Sivori et al Medicina 2008;68(4):325-44
51923 Societe de Pneumologie de Langue Francaise Rev Mal Respir 2005;22(4):696-704
50344 SPLF Rev Mal Respir 2005;22(5 C3):7S8-7S14
37958 Spruit et al Sports Med 2007;37(6):501-18
50476 Su Chin J Clin Rehabil 2006;10(32):141-3
50708 Tiep et al Dis Manag Health Outcomes 2008;16(5):305-13
50410 Troosters et al Am J Respir Crit Care Med 2005;172(1):19-38
50426 Vincent et al Crit Rev Phys Rehabil Med 2008;20(2):127-58
50390 Wedzicha Thorax 2004;59(3):183,
50434 Zuwallack Am J Med 2008;121(7 Suppl 1):S25-S32
Insufficient information
50466 Abholz HH, Z Allgemeinmed 2007;83(7):292-307.
53296 Baicus C, Eur J Intern Med 2009;20(5):e124-e125.
44247 Bausewein C, Cochrane Database Syst Rev 2008;(2):CD005623.
53294 Bulley C, Physiother Res Int 2009;14(3):181-92.
50524 Cambach W, Arch Phys Med Rehabil 1999;80(1):103-11.
50623 Chang AT, Contemporary Clinical Trials 2008;29(5):796-800.
50460 Coventry PA, J Psychosom Res 2007;63(5):551-65.
50327 Effing T Cochrane Database Syst Rev 2007;(4).
A-78
53234 Fischer MJ Respir Med 2009;103(10):1564-71.
50403 Gallucci MA. (Teachers College, Columbia University).
50641 Garrod R Cochrane Database of Systematic Reviews 2008 Issue 1. 2008. CD006906.
50475 Gomez A, Aten Primaria 2006;38(4):230-3.
51785 Guyatt GH, J Clin Epidemiol 1999;52(3):187-92.
HAS 2007 Available: http://www.hassante.fr/portail/upload/docs/application/pdf/rapport_reentrainement_a_lexercice_s
50402 Hassanein 2006 Case Western Reserve University
ICSI Jan 2009 Available: http://www.icsi.org/chronic_obstructive_pulmonary_disease/chronic_obstructive_pulmonary_disease_2286.html
50639 Ilnitskii AN. Ter Arkh 2003;75(3):50-3. 50357?
53295 Kagaya H, Tohoku J Exp Med 2009;218(3):215-9. Available: http://www.jstage.jst.go.jp/article/tjem/218/3/215/_pdf
50372 Lewczuk J, Pneumonol Alergol Pol 1998;66(9-10):464-7.
50374 Lewczuk J Pol Arch Med Wewn 1998;100(4):331-6.
50521 Liu Chin J Clin Rehabil 2002;6(21):3170-1.
51924 Lopez Varela MV, Arch Bronconeumol 2006;42(9):434-9.
50408 McCarroll ML. (The Ohio State University).
53298 Menadue C, Cochrane Database Syst Rev 2009;(2).
50330 Milenkovic B, Srp Arh Celok Lek 2007;135(7-8):419-24.
NIHR 2008 Available: http://www.hta.ac.uk/project/1316.asp?SearchText=chronic+bronchitis%2FCOPD&PjtId=1316&PjtTypeWebsite=HTA-STD
37961 Nonoyama ML, Cochrane Database Syst Rev 2007;(2):CD005372. Ref ID:
50335 Oh H, J Clin Nurs 2007;16(1):3-15.
50384 Oh HS. Taehan Kanho Hakhoe Chi 2003;33(6):743-52.
50395 Ong KC, Annals Academy of Medicine Singapore 2001;30(1):15-21.
50420 Peters ML. State University of New York at Albany.
50359 Piszko Pneumonol Alergol Pol 2002;70(11-12):566-72.
50351 Piszko Pol Arch Med Wewn 2004;111(1):57-62.
50348 Puhan MA, Respir Res 2005;6:54. Available: http://www.pubmedcentral.nih.gov/picrender.fcgi?artid=1164434&blobtype=pdf
Registered Nurses' Association of Ontario March 2005 Available: http://www.rnao.org/Page.asp?PageID=924&ContentID=807
50637 Romagnoli M, Eur Respir J 2005;26(Suppl 49).
50399 Salman GF, JGIM 1999;14(Suppl 2):68.
A-79
50531 Salman GF, J Gen Intern Med 2003;18:213-21.
50385 Subramanaim V, Chest 2007;132(4 Suppl S):536S.
50313 Titova ON, Vopr Kurortol Fizioter Lech Fiz Kult 2008;(4):17-20.
50396 Tregonning M, Thorax 2000;55(Supplement 3):A7.
50493 Varga J, Orv Hetil 2005;146(44):2249-55.
WHO 2001 Available: http://www.who.int/respiratory/publications/WHO_MNC_CRA_02.1.pdf
50149 Wijkstra PJ, Monaldi Arch Chest Dis 2000;55(2):130-4.
50423 Zhang ZQ, Chinese Critical Care Medicine 2008;20(10):607-10.
Did not relate to full PR programs
50412 Alexander JL Arizona State University
53077 Allan et al Respir Care 2009;54(9):1175-82
50365 Carrieri-Kohlman et al Nurs Res 2001;50(3):136-46.
50361 Cegla et al Pneumologie 2002;56(7):418-24
Garrod R, Chartered Soc of Physiotherapists E05 March 2003 Available: http://www.csp.org.uk
50499 Chen et al Chin J Clin Rehabil 2005;9(43):17-9
53233 Dourado Braz J Med Biol Res 2009;42(3):263-71
50609 Franssen et al Chest 2004;125(6):2021-8
50483 Garcia-Aymerich et al Thorax 2006;61(9):772-8
50398 Lum et al J Am Geriatr Soc 1999;47(9):S105
50508 Murphy et al Respir Med 2005;99(10):1297-302
NZHTA 1998 Available: http://nzhta.chmeds.ac.nz/publications/nzhta2.pdf
50443 O'Brien et al J Cardiopulm Rehabil Prev 2008;28(2):128-41
50615 O'Donnell et al Am J Respir Crit Care Med 1998;157(5 Pt 1):1489-97
37987 Puhan Thorax 2005;60(5):367-75
50526 Shioya et al Eur Respir J 2007;30(Suppl 51):188s
50373 Sivori et al Medicina (B Aires) 1998;58(6):717-27
50449 Skumlien et al Respir Med 2008;102(3):422-9
50406 Smidt et al Ned Tijdschr Fysiother 2005;115(4):86-95
50424 van Wetering Int J Chron Obstruct Pulmon Dis 2008;3(3):443-51.
50634 Vogiatzis et al Chest 2005;128(6):3838-45
50604 Vogiatzis et al Thorax 2007;62(11):950-6
50621 Wadell et al Adv Physiother 2005;7(2):51-9
2956 Weiner et al Chest 2000;118(3):672-8
50414 Whitsel 1998, Syracuse University
A-80
Inappropriate study design
50341 Alexopoulos et al Am J Geriatr Psychiatry 2006;14(5):466-75
50371 Ando et al Nihon Kokyuki Gakkai Zasshi 1999;37(9):680-7
50418 Arena et al Cardiopulm Phys Ther J 2003;14(3):3-6
50490 Arnold et al Patient Educ Couns 2006;61(1):99-108
50520 Barakat International Journal of COPD 2007;2(4):585-91
50636 Belza et al J Cardiopulm Rehabil Prev 2005;25(2):107-14
50478 Biscione et al Eur Respir J 2006;27(6):1320-1
50367 Buchi et al Schweiz Med Wochenschr 2000;130(5):135-42
50468 Carr et al Chest 2007;132(1):127-34
53334 Carr J Cardiopulm Rehabil Prev 2009;29(5):318-24
50319 Cecins et al Aust Health Rev 2008;32(3):415-22
50329 Drozdowski et al Pneumonol Alergol Pol 2007;75(2):147-52
51779 Duren-Winfield et al West J Nurs Res 2000;22(4):460-74
50415 Faager et al Nordisk Fysioterapi 1999;3(4):146-52
50630 Ferreira et al J Cardiopulm Rehabil Prev 2006;26(1):54-60
50463 Foglio et al Respir Med 2007;101(9):1961-70
50427 Garcia-Aymerich et al Ann Epidemiol 2008;18(10):775-83
50608 Garrod et al Physiother Res Int 2004;9(3):111-20
50619 Geddes et al Cardiopulm Phys Ther J 2007;18(4):3-13
50456 Georgiadou et al Eur Respir J 2007;29(2):284-91
50387 Hillerdal Chest 2005;128;3489-3499
50316 Haave et al Chron Respir Dis 2008; 5(2):69-73
50453 Haave Int J COPD 2007;2(3):355-9
53231 Hassenein J Mol Signal 2009;29(4):255-60.
50518 Holland et al J Cardiopulm Rehabil Prev 2004;24(6):422-7
50376 Inoue et al Nihon Kokyuki Gakkai Zasshi 1998;36(9):756-62
50488 Koppers et al Chest 2006;129(4):886-92
50336 Kubo Asia Pac J Clin Nutr 2006;15(4):551-5.
50515 Lange et al Ugeskr Laeger 2005;167(3):274-9
50447 Laviolette et al Thorax 2008;63(2):115-21
50498 Leleu et al Rev Pneumol Clin 2005;61(6):359-64
50616 Leuppi et al Dtsch Med Wochenschr 1998;123(7):174-8
50364 Lisboa et al Rev Med Chil 2001;129(4):359-66
50626 Lotshaw et al J Cardiopulm Rehabil Prev 2007;27(4):247-51
A-81
50612 Mador Chest 2005;128(3):1216-24
50422 Mann et al Can J Respir Ther 1998;34(4):123-7
50366 Miyahara et al Acta Med Okayama 2000;54(4):179-84
50419 Mok et al Asian J Nursing Stud 2003;6(2):58-64
50519 Ngaage et al Heart Lung 2004;33(6):381-9
50431 Ninot et al Disabil Rehabil 2007;29(22):1671-8
50503 Nishiyama et al Qual Life Res 2005;14(10):2315-21
50395 Ong Annals Academy of Medicine Singapore 2001;30(1):15-21, January, 2001
50347 Pande et al Indian J Chest Dis Allied Sci 2005;47(3):217-9
50352 Panton et al Eur J Appl Physiol 2004;91(4):443-9
50625 Pitta et al Chest 2008;134(2):273-80
50644 Rae et al Prim Care Respir J 2008; 17
50497 Riario-Sforza et al Rass Patol Appar Respir 2005;20(6):284-90
50315 Ringbaek et al Chron Respir Dis 2008;5(2):75-80.
50333 Ringbaek et al Ugeskr Laeger 2007;169(17):1572-6
50613 Rajendran et al Indian Heart J 1998;50(5):531-4
50353 Schaanning Tidsskr Nor Lægeforen 2000;120(5):551-5
50375 Scherer et al J N Y State Nurses Assoc 1998;29(3-4):16-20
50340 Schultz et al Dtsch Med Wochenschr 2006;131(33):1793-8
50643 Solanes et al Respir Med 2008;
50506 Trappenburg et al Arch Phys Med Rehabil 2005;86(9):1788-92
50370 Vogiatzis et al Chest 1999;116(5):1200-7
51771 Von Leupoldt Lung 2008;186(6):387-91
50492 Zhao et al Chinese Journal of Rehabilitation Medicine 2006;21(2):127-31
50631 Zuwallack et al Chron Respir Dis 2006;3(1):11-8
Not relevant to PR for COPD
42046 Adams Drug Benefit Trends 2006; 259 - 265
AHRQ 2001 Available: http://www.ahrq.gov/clinic/epcsums/copdsum.htm
50388 Baggott Chest 2004;126(4 Suppl S):739S, OCT
32813 Chumillas et al Arch Phys Med Rehabil 1998;79(1):5-9
50611 Clini et al Thorax 2001;56(7):519-23
50504 Coultas et al Chest 2005;128(4):2017-24
50458 Garrod et al Respir Med 2007;101(12):2429-36
50633 Harpa et al Respir Med 2006;100(1):130-9
A-82
Health Council of the Netherlands 2003 Available: http://www.gezondheidsraad.nl/nl/adviezen/oefentherapie
50516 Hendriksen et al Ugeskr Laeger 2005;167(3):269-72
50389 Kujala Scand J Med Sci Sports 2004;14(6):339-45
50640 Lenz et al Dtsch Z Sportmed 2001;52(7/8):S16
50635 Mercken et al Am J Respir Crit Care Med 2005;172(8):994-1001
50331 Montgomery et al Prev Chronic Dis 2007;4(3):A62, 2007
50413 Migliore. New York University 2003
50421 Muth. Union Institute, 2001.
50610 Ortega et al Am J Respir Crit Care Med 2002;166(5):669-74
50462 O'Shea et al Chron Respir Dis 2007;4(3):135-42
50438 Peytremann-Bridevaux et al Am J Med 2008;121(5):433-43
SBU 2000. Available: http://www.sbu.se/en/Published/Yellow/Treating-asthma-and-COPD/
50527 Sugawara et al Eur Respir J 2007;30(Suppl 51):514s
50409 Wang et al Chinese Nursing Research 2004;18(9B):1608-9
Duplicates or support material related to selected publications
50530 Lacasse Y Lancet 1996;348:1115-9.
50323 Lacasse Y Eur Medicophys 2007;43(4):475-85.
Sillen Chest 2009;136(1):44-61
49112 Wilt et al Ann Intern Med 2007;147(9):639-53
Economic publications
31498 Ashworth Cochrane Database Syst Rev 2005;(1):CD004017
50153 Barandun Schweiz Rundsch Med Prax 1997;86:1979-83
50144 California Pulmonary Rehabilitation Collaborative Group. J Cardiopulm Rehabil 2004;24(1):52-62
51779 Duren-Winfield West J Nurs Res 2000;22(4):460-74
50632 Eaton Respirology 2009;14(2):230-8.
50147 Fan Int J Chron Obstruct Pulmon Dis 2008;5(2):105-16
53169 Goldstein Chest 1997;112(2):370-9
53465 Haggerty Chest 1991;100: 607-12.
50146 Hanaoka Respirology 2008;13(6):919-22
50145 Hessel Pneumologie 2000;54(7):289-95
51858 Motegi Nihon Kokyuki Gakkai Zasshi 2006;44(11):787-94
A-83
50151 Parker Respir Care 1998;43(3):177-82
51291 Roselle Respir Care 1982;27(10):1194-9
50379 Scherer Rehabil Nurs 1998;23(2):71-7
53461 Strijbos Chest 1996;109(2):366-72
51860 Troosters Am J Med 2000;109(3):207-12
50149 Wijkstra Monaldi Arch Chest Dis 2000;55(2):130-4