pulmonology conference
DESCRIPTION
Guanzon , Guerrero, Guerzon , Guevarra, Guinto , Gutierrez, Hermoso , Icasas , Ignacio. Pulmonology Conference. General Data. JA 16yo / M Lives in Caloocan City Roman Catholic Single. Chief Complaint: Difficulty of Breathing. (+) productive cough with yellowish sputum - PowerPoint PPT PresentationTRANSCRIPT

PULMONOLOGY CONFERENCEGuanzon, Guerrero, Guerzon, Guevarra, Guinto, Gutierrez, Hermoso, Icasas, Ignacio

General Data
JA 16yo / M Lives in Caloocan City Roman Catholic Single

Chief Complaint:Difficulty of Breathing

1 month PTA
(+) productive cough with yellowish sputum(-) fever, malaise, dyspneaNo consult was done and no medications were taken.
3 weeks PTA
(+) easy fatigability and shortness of breath after walking for 15 meters and after 2 quarters in a basketball game (as compared to before?)(+) fever (Tmax 39.8 C)
Paracetamol 500 mg/tab taken after meals(+) fever in the afternoon and at night(?) night chills, sweating(?) persistence of productive cough(?) known asthmatic?
3 weeks PTA?
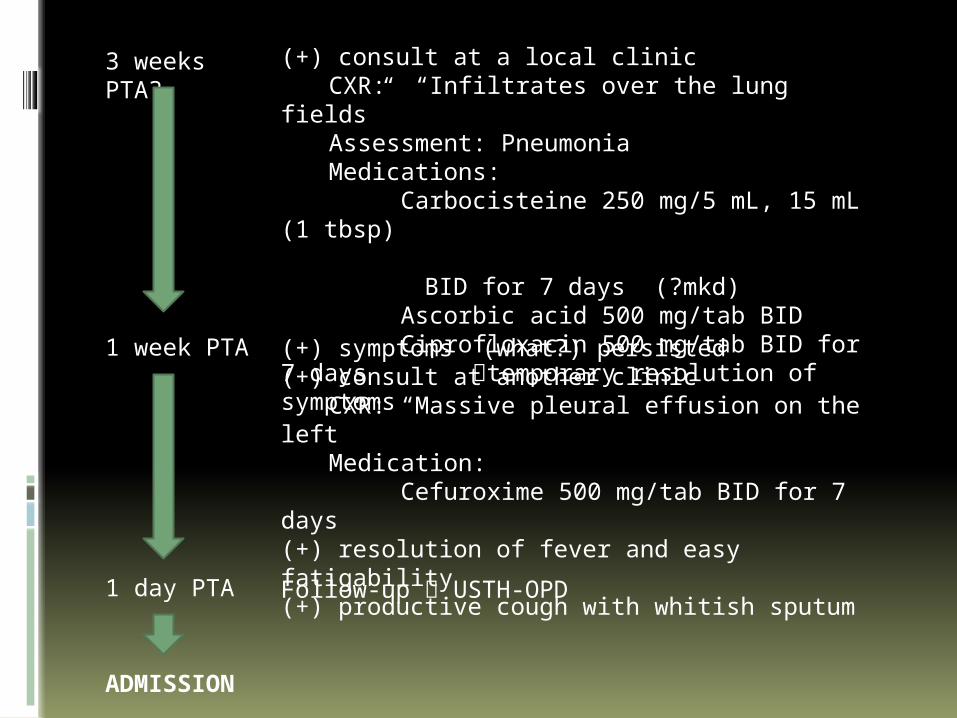
(+) consult at a local clinic CXR: “Infiltrates over the lung fields”Assessment: PneumoniaMedications: Carbocisteine 250 mg/5 mL, 15 mL (1
tbsp) BID for 7 days (?mkd) Ascorbic acid 500 mg/tab BID
Ciprofloxacin 500 mg/tab BID for 7 days temporary resolution of symptoms
1 week PTA (+) symptoms (what?) persisted(+) consult at another clinic
CXR: “Massive pleural effusion on the left”
Medication: Cefuroxime 500 mg/tab BID for 7 days
(+) resolution of fever and easy fatigability(+) productive cough with whitish sputum
1 day PTA Follow-up USTH-OPD
ADMISSION
Review of Systems
No weight gain or weight loss, less activity, good activity
No rash, abnormal pigmentation, hair loss, acne, pruritus
No headache, dizziness, lacrimation, aural discharge, epistaxis, gum bleeding
No orthopnea, cyanosis, fainting spells, chest pain No vomiting, diarrhea, constipation, passage of worms,
abdominal pain, jaundice, food intolerance No dysuria, frequency, urgency No seizures, convulsions, tremors, sleep problems No limitation of motion No pallor, bleeding manifestations, easy bruisability

Personal History H: Patient lives with his mother and father. At home, he
likes to watch cartoons on TV and sleep. Aside from that, he does not do anything else at home. He spends most of his free time outside playing basketball with his friends.
E: Currently in his 3rd year of high school. He prefers to play basketball than go to class or study.
E: Patient eats 3 meals a day and has no preference on the food that he eats.
A: Varsity player of the school’s basketball team; computer games
D: Patient claims that he has never smoke, drink alcohol or took illicit drugs.
S: He had 4 past girlfriends. He claimed that they had never engaged in any sexual activity.
S: Patient claims that he is very contented with his life and would never think of taking his own life.

Past Medical History
(+) Trauma due to fall (1994) – had the wound on his left ear dressed
(-) HPN, (-) DM (-) asthma, allergies

Family History
(+) HPN – paternal and maternal grandfather, father
(+) PTb – maternal grandfather (+) DM – maternal grandfather (+) Thyroid disease - mother (-) Allergies, Asthma (-) Cancer, Kidney disease, Stroke

Family Profile
Name Age Relation Occupation Health
Evangeline 47 Mother Vendor (+) toxic goiter
Nestor 61 Father Retired supervisor
(+) HPN
Nesty John 21 Brother Unemployed Healthy
Ana Carmela 19 Sister Call center agent Healthy
Rose Anne 18 Sister Saleslady Healthy

Socioeconomic & Environmental History
Patient lives with his parents and stays in the same room as them. Their house is a single level cemented bungalow, well ventilated and well lit. Drinking water is obtained from a nearby water refilling station. Garbage is collected everyday by a local garbage collector.
Physical Examination
VS: BP 110/70 HR 76 bpm RR 26/min T 36.4 C Ht: 170 cm Wt: 53 kg Conscious, coherent, ambulatory, not in
cardiorespiratory distress Warm moist skin, not jaundiced, no active dermatoses Pink palpebral conjunctivae, anicteric sclera Nasal septum midline, no nasoaural discharge,
turbinates not congested No tragal tenderness, nonhyperemic EAC AU, TM intact
AUMoist buccal mucosa, nonhyperemic PPW, tonsils enlarged
Supple neck, no palpable cervical lymph nodes
Physical Examination
Asymmetric chest expansion, no retractions, trachea deviated to the right with lagging on the left, decreased vocal and tactile fremiti on the left, dullness on the left infrascapular area (T6 down), decreased breath sounds on the left upper and lower lung fields
Adynamic precordium, AB 5th LICS MCL, no murmurs
Flat abdomen, normoactive bowel sounds, soft, nontender
Pulses full and equal, no edema, no cyanosis

Neurologic Examination
Conscious, coherent, oriented to 3 spheres Pupil size 3-4 mm equally reactive to light; no
ptosis OU No facial asymmetry, (+) corneal reflex, (+) gag
reflex Symmetric palpebral fissures and nasolabial fold MMT 5/5 on all extremities No involuntary movement, no spasticity, no
atrophy No sensory deficits No nuchal rigidity, (-) Brudzinski, (-) Kernig’s

Salient Features

Differential Diagnosis
Pleural Effusion vs. Consolidation vs. Atelectasis, etc. clinically first then via CXR
Degree of Pleural Effusion (Massive, etc?)
Why suspect Pneumonia? Why suspect PTB?

Impression
Massive Pleural Effusion, left probably secondary to Pneumonia vs.
PTB
Pneumonia
Definition Etiologies by age Criteria for Dx Criteria for confinement Ancillary procedures Expected clinical and lab findings Complications Correlate with px

Pulmonary Tuberculosis
Definition Criteria for Dx Categories and Classification Ancillary procedures Expected clinical and lab findings Complications Correlate with px
Pleural Effusion
Definition Light’s criteria Types Complications Management Correlate with px

Pleural Effusion
An abnormal collection of fluid in the pleural space resulting from excess fluid production or decreased absorption.
http://emedicine.medscape.com/article/807375-overview

Clinical Presentation Dyspnea - is the most common symptom at presentation
and generally indicates the presence of a large effusion.
- 50% of patients with malignant pleural effusions
Chest pain - results from pleural irritation
- sharp or stabbing and is exacerbated with deep inspiration.
- raises the likelihood of an exudative etiology such as pleural infection, mesothelioma, or pulmonary infarction.
http://emedicine.medscape.com/article/807375-overview
Normal pleural fluid Clear ultrafiltrate of plasma that originates
from the parietal pleura pH 7.60-7.64 Protein content less than 2% (1-2 g/dL) Fewer than 1000 WBCs per cubic millimeter Glucose content similar to that of plasma Lactate dehydrogenase (LDH) less than 50%
of plasma Sodium, potassium, and calcium
concentration similar to that of the interstitial fluid
http://emedicine.medscape.com/article/807375-overview

Mechanisms in Pleural Effusion Altered permeability of the pleural membranes
(eg, inflammation, malignancy, pulmonary embolus)
Reduction in intravascular oncotic pressure (eg, hypoalbuminemia, cirrhosis)
Increased capillary permeability or vascular disruption (eg, trauma, malignancy, inflammation, infection, pulmonary infarction, drug hypersensitivity, uremia, pancreatitis)
Increased capillary hydrostatic pressure in the systemic and/or pulmonary circulation (eg, congestive heart failure, superior vena cava syndrome) http://emedicine.medscape.com/article/
807375-overview

Mechanisms in Pleural Effusion Reduction of pressure in the pleural
space, preventing full lung expansion (eg, extensive atelectasis, mesothelioma)
Decreased lymphatic drainage or complete blockage, including thoracic duct obstruction or rupture (eg, malignancy, trauma)
Increased peritoneal fluid, with migration across the diaphragm via the lymphatics or structural defect (eg, cirrhosis, peritoneal dialysis)http://emedicine.medscape.com/article/
807375-overview

Mechanisms in Pleural Effusion Movement of fluid from pulmonary
edema across the visceral pleura Persistent increase in pleural fluid
oncotic pressure from an existing pleural effusion, causing further fluid accumulation
http://emedicine.medscape.com/article/807375-overview

Course in the Ward
Brief Discussion of Special Procedures

Management