quale profilassi e quale terapia nei soggetti portatori di...
TRANSCRIPT
Quale profilassi e quale terapia
nei soggetti portatori di trombofilia
Bari, 9 aprile 2016
Maurizio Margaglione
Genetica Medica
Università di Foggia
• Emostasi
• Trombosi
• Trombofilia
• Test (genetici)
• Consulenza (genetica)
Profilassi, terapia e trombofilia
• Emostasi
• Trombosi
• Trombofilia
• Test (genetici)
• Consulenza (genetica)
Profilassi, terapia e trombofilia

Trombofilia: semantica
• Presenza di una tendenza familiare ad alta
penetranza al tromboembolismo
Tendenza al tromboembolismo geneticamente determinato. (Lane DA et al, Thromb Haemost 1996;76:651-662.)
Trombofilia ereditaria
• Presenza di un difetto protrombotico
• Entrambi i casi
• Emostasi
• Trombosi
• Trombofilia
• Test (genetici)
• Consulenza (genetica)
Profilassi, terapia e trombofilia
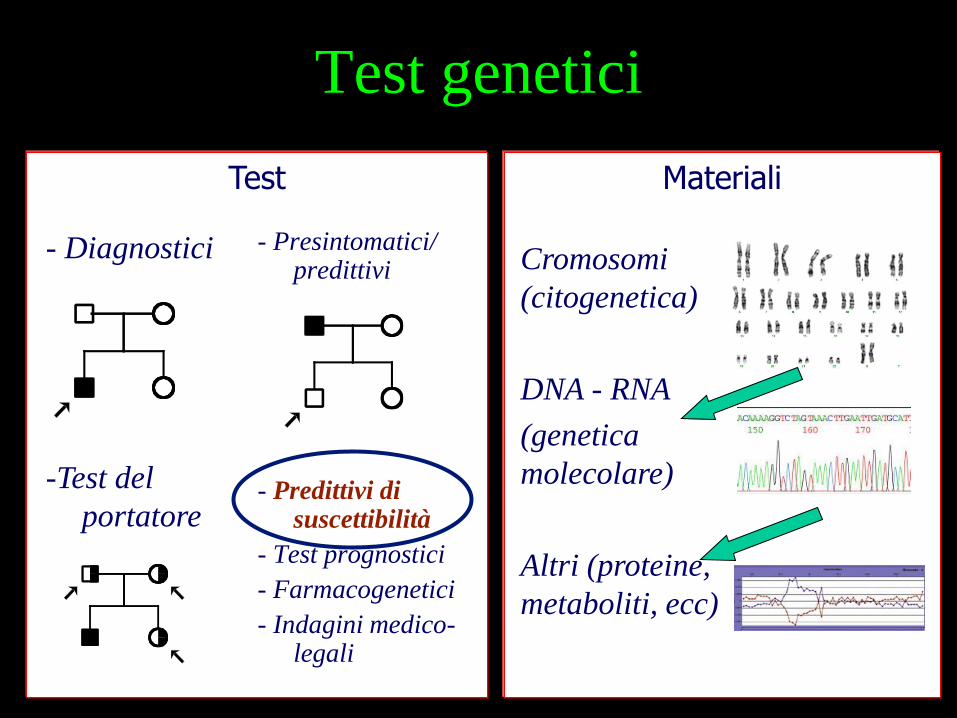
Materiali Test
- Diagnostici
-Test del
portatore
Test genetici
- Presintomatici/ predittivi
- Predittivi di suscettibilità
- Test prognostici
- Farmacogenetici
- Indagini medico-legali
Cromosomi
(citogenetica)
DNA - RNA
(genetica
molecolare)
Altri (proteine,
metaboliti, ecc)
TEST DI SUSCETTIBILITA’

Who has a genetic risk?
TROMBOSI
EMORRAGIA
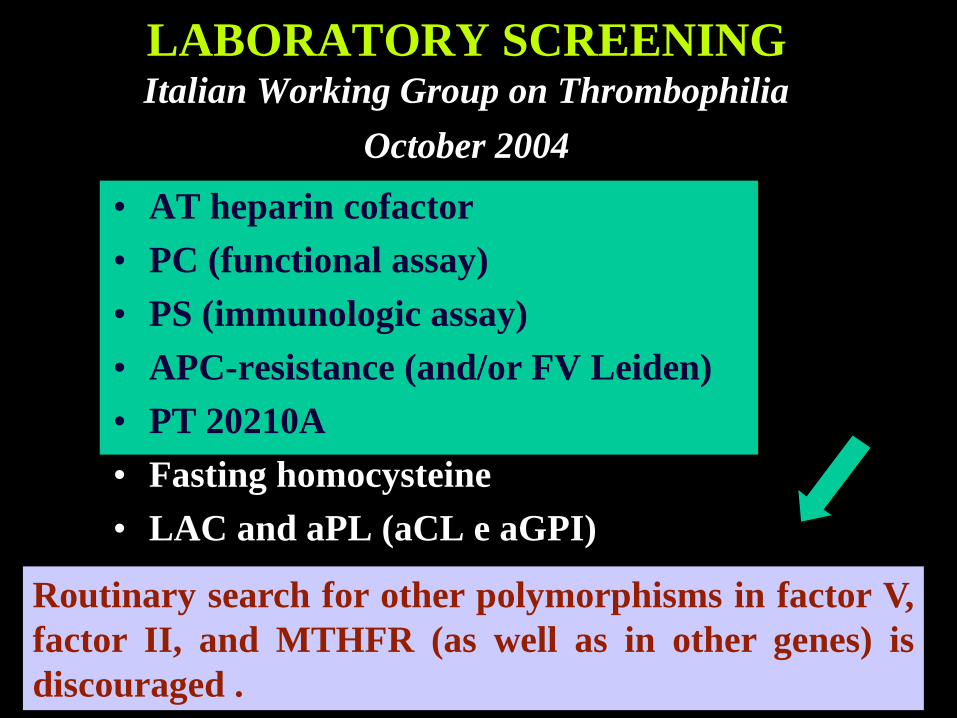
LABORATORY SCREENING Italian Working Group on Thrombophilia
October 2004
• AT heparin cofactor
• PC (functional assay)
• PS (immunologic assay)
• APC-resistance (and/or FV Leiden)
• PT 20210A
• Fasting homocysteine
• LAC and aPL (aCL e aGPI)
Routinary search for other polymorphisms in factor V,
factor II, and MTHFR (as well as in other genes) is
discouraged .
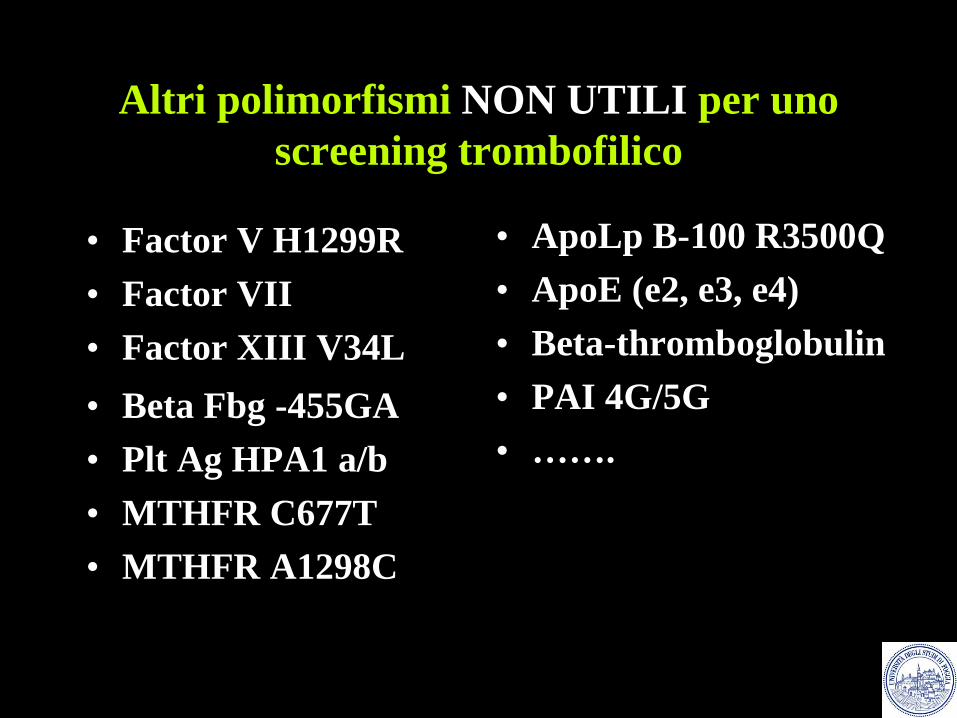
Altri polimorfismi NON UTILI per uno
screening trombofilico
• Factor V H1299R
• Factor VII
• Factor XIII V34L
• Beta Fbg -455GA
• Plt Ag HPA1 a/b
• MTHFR C677T
• MTHFR A1298C
• ApoLp B-100 R3500Q
• ApoE (e2, e3, e4)
• Beta-thromboglobulin
• PAI 4G/5G
• …….
• Emostasi
• Trombosi
• Trombofilia
• Test (genetici)
• Consulenza (genetica)
Profilassi, terapia e trombofilia
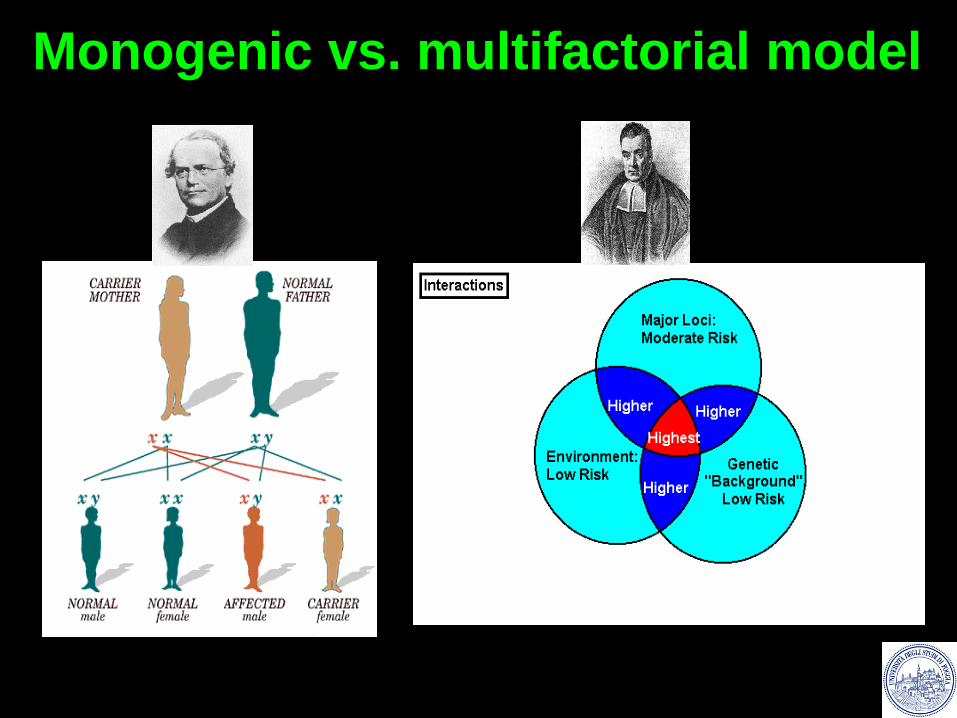
Monogenic vs. multifactorial model
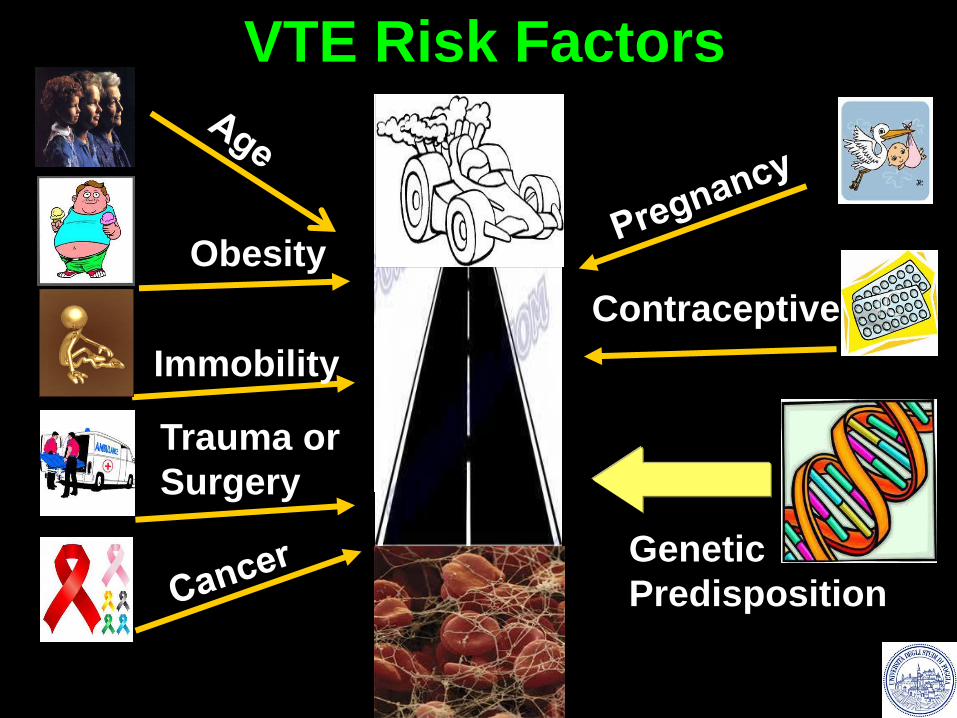
Obesity
Contraceptives
Immobility
Trauma or
Surgery
VTE Risk Factors
Genetic
Predisposition
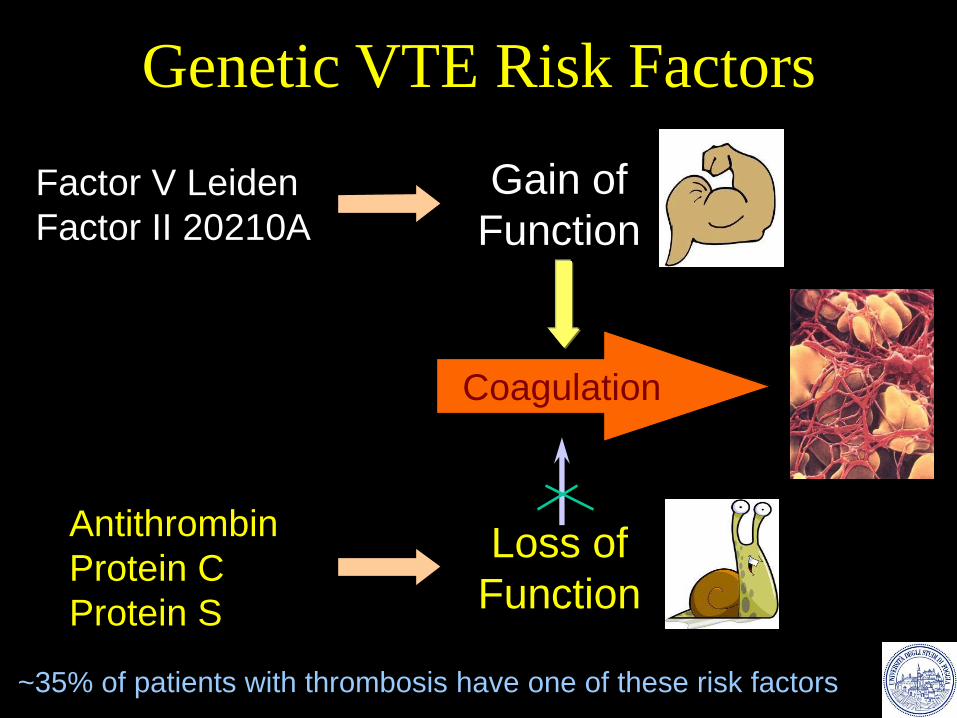
Genetic VTE Risk Factors
Coagulation
Factor V Leiden
Factor II 20210A
Antithrombin
Protein C
Protein S
Gain of
Function
Loss of
Function
~35% of patients with thrombosis have one of these risk factors
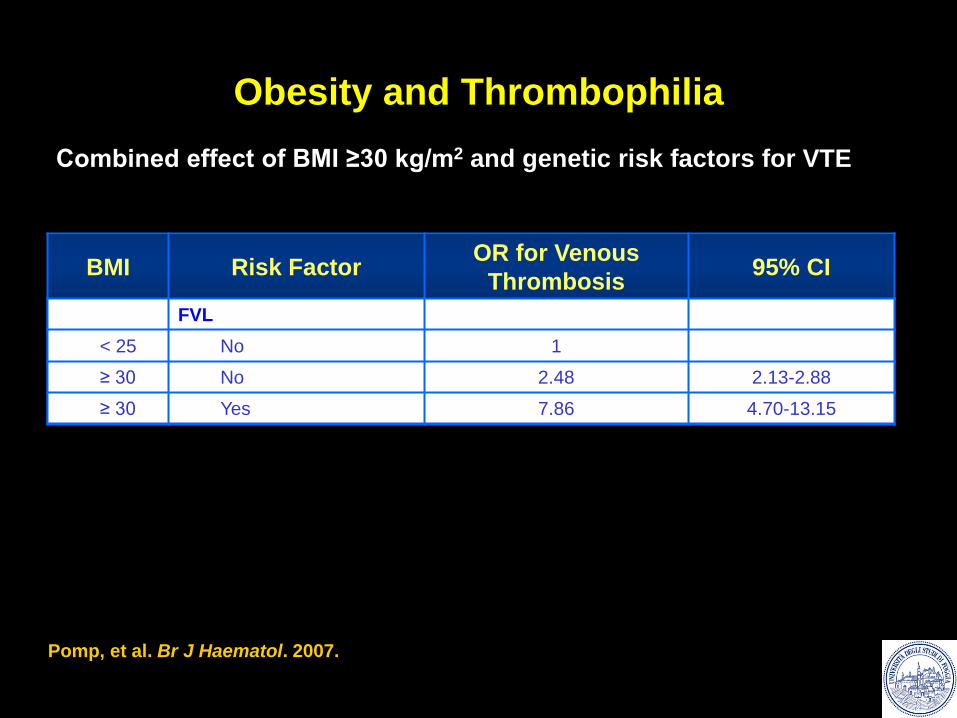
Obesity and Thrombophilia
BMI Risk Factor OR for Venous
Thrombosis 95% CI
OC use
< 25 No 1
≥ 30 No 3.04 1.66-5.57
≥ 30 Yes 23.78 13.35-42.34
Combined effect of BMI ≥30 kg/m2 and genetic risk factors for VTE
FVL
< 25 No 1
≥ 30 No 2.48 2.13-2.88
≥ 30 Yes 7.86 4.70-13.15
Pomp, et al. Br J Haematol. 2007.
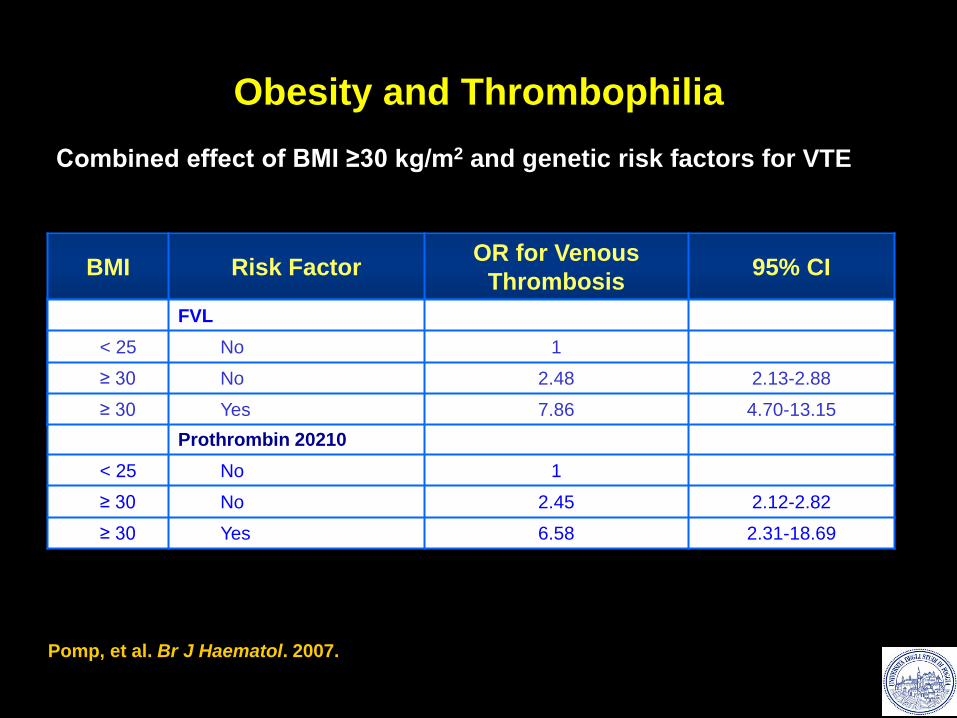
Pomp, et al. Br J Haematol. 2007.
Obesity and Thrombophilia
BMI Risk Factor OR for Venous
Thrombosis 95% CI
OC use
< 25 No 1
≥ 30 No 3.04 1.66-5.57
≥ 30 Yes 23.78 13.35-42.34
Combined effect of BMI ≥30 kg/m2 and genetic risk factors for VTE
Prothrombin 20210
< 25 No 1
≥ 30 No 2.45 2.12-2.82
≥ 30 Yes 6.58 2.31-18.69
FVL
< 25 No 1
≥ 30 No 2.48 2.13-2.88
≥ 30 Yes 7.86 4.70-13.15
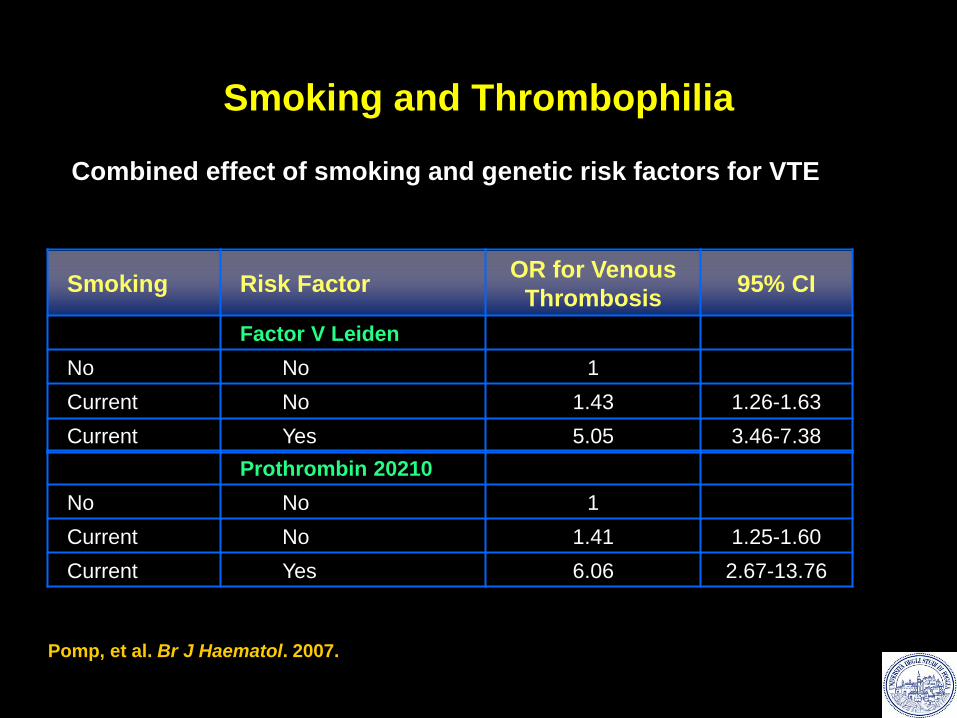
Smoking and Thrombophilia
Smoking Risk Factor OR for Venous
Thrombosis 95% CI
Factor V Leiden
No No 1
Current No 1.43 1.26-1.63
Current Yes 5.05 3.46-7.38
Combined effect of smoking and genetic risk factors for VTE
Prothrombin 20210
No No 1
Current No 1.41 1.25-1.60
Current Yes 6.06 2.67-13.76
Pomp, et al. Br J Haematol. 2007.
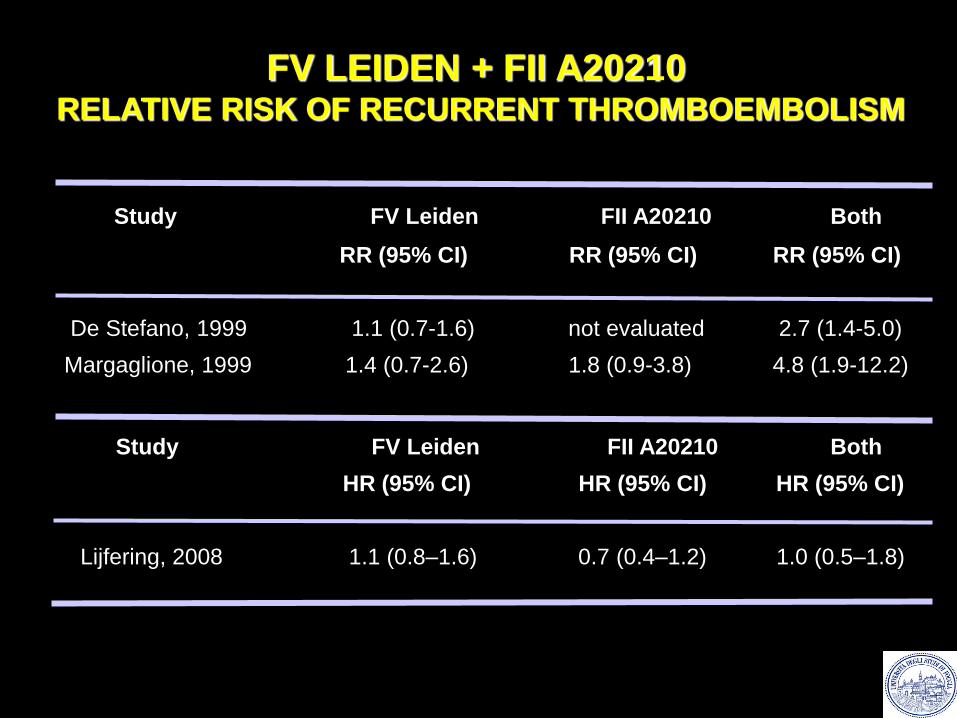
FV LEIDEN + FII A20210
RELATIVE RISK OF RECURRENT THROMBOEMBOLISM
Study FV Leiden FII A20210 Both
RR (95% CI) RR (95% CI) RR (95% CI)
De Stefano, 1999 1.1 (0.7-1.6) not evaluated 2.7 (1.4-5.0)
Margaglione, 1999 1.4 (0.7-2.6) 1.8 (0.9-3.8) 4.8 (1.9-12.2)
Study FV Leiden FII A20210 Both
HR (95% CI) HR (95% CI) HR (95% CI)
Lijfering, 2008 1.1 (0.8–1.6) 0.7 (0.4–1.2) 1.0 (0.5–1.8)
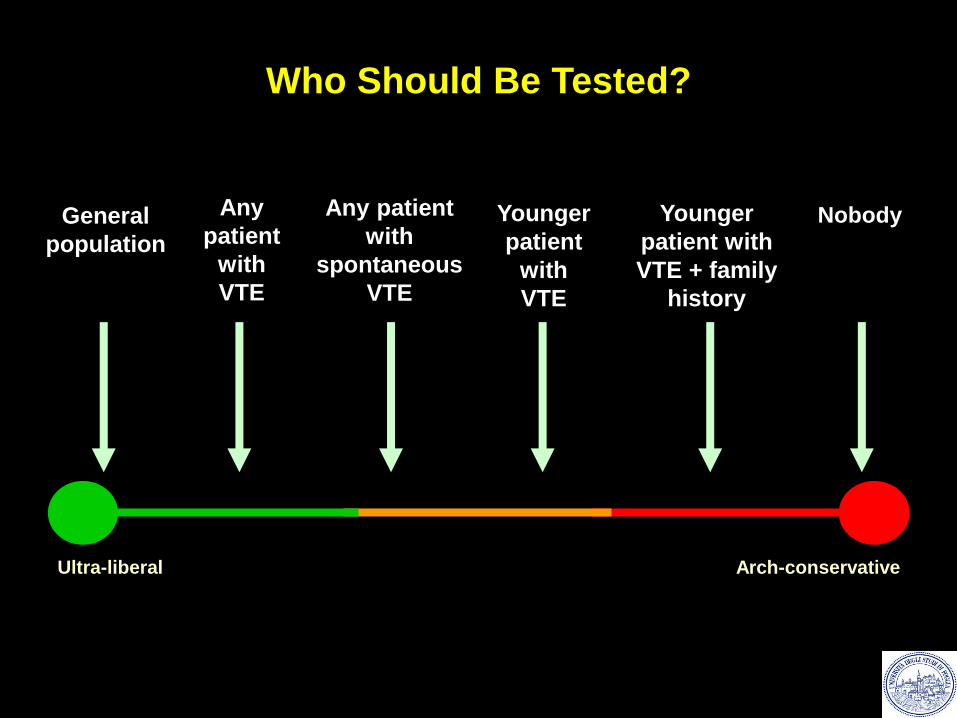
Any patient
with
spontaneous
VTE
Younger
patient with
VTE + family
history
Any
patient
with
VTE
General
population
Younger
patient
with
VTE
Arch-conservative Ultra-liberal
Nobody
Who Should Be Tested?
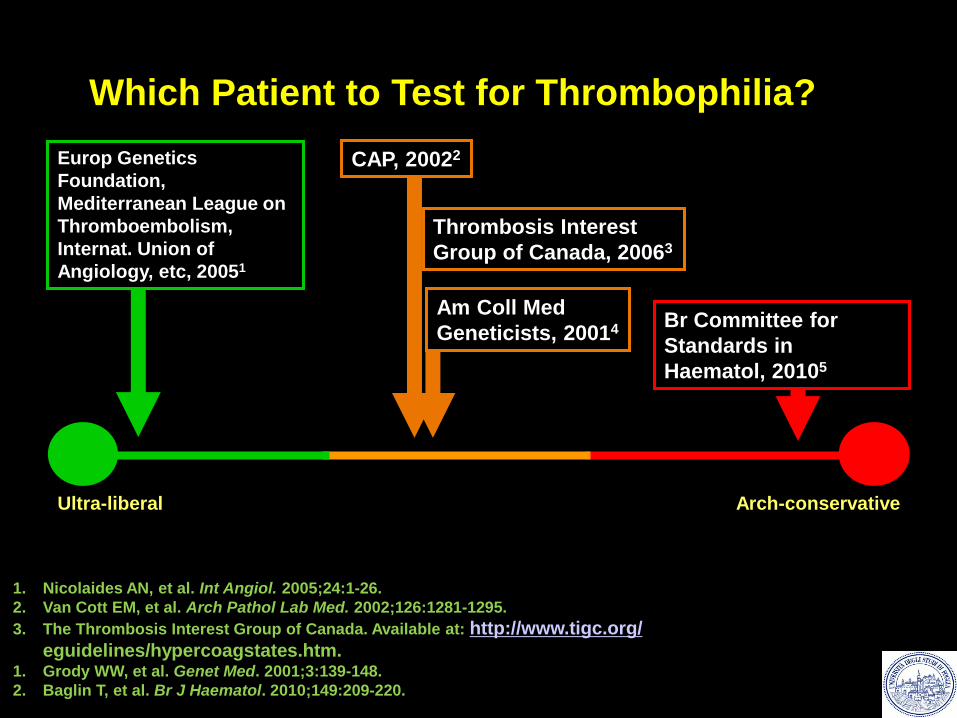
1. Nicolaides AN, et al. Int Angiol. 2005;24:1-26.
2. Van Cott EM, et al. Arch Pathol Lab Med. 2002;126:1281-1295.
3. The Thrombosis Interest Group of Canada. Available at: http://www.tigc.org/
eguidelines/hypercoagstates.htm. 1. Grody WW, et al. Genet Med. 2001;3:139-148.
2. Baglin T, et al. Br J Haematol. 2010;149:209-220.
Am Coll Med
Geneticists, 20014 Br Committee for
Standards in
Haematol, 20105
Europ Genetics
Foundation,
Mediterranean League on
Thromboembolism,
Internat. Union of
Angiology, etc, 20051
Which Patient to Test for Thrombophilia?
CAP, 20022
Arch-conservative Ultra-liberal
Thrombosis Interest
Group of Canada, 20063
“ In this real-world setting, testing for
inherited thrombophilia is frequently at
odds with the recommendations of the
CAP consensus conference. There is a
need for wider dissemination of concise
thrombophilia testing guidelines.”
Jackson et al. BMC Clinical Pathology 2008;8:3
Testing for hereditary thrombophilia: a retrospective
analysis of testing referred to a national laboratory
Consulenza genetica e test genetici
Eventuali problematiche
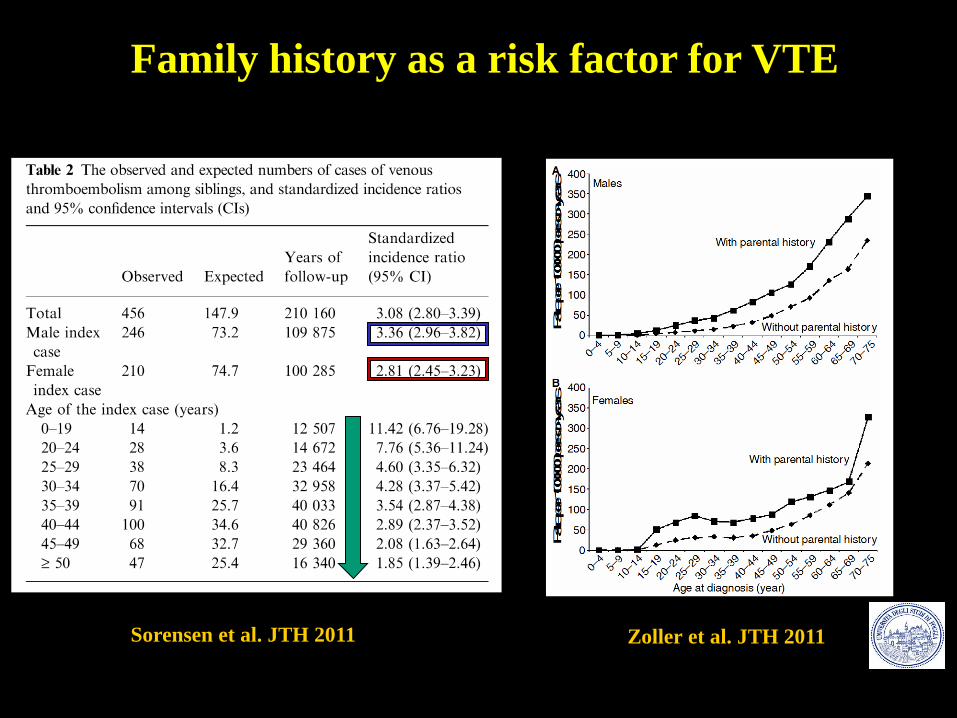
Sorensen et al. JTH 2011 Zoller et al. JTH 2011
Family history as a risk factor for VTE
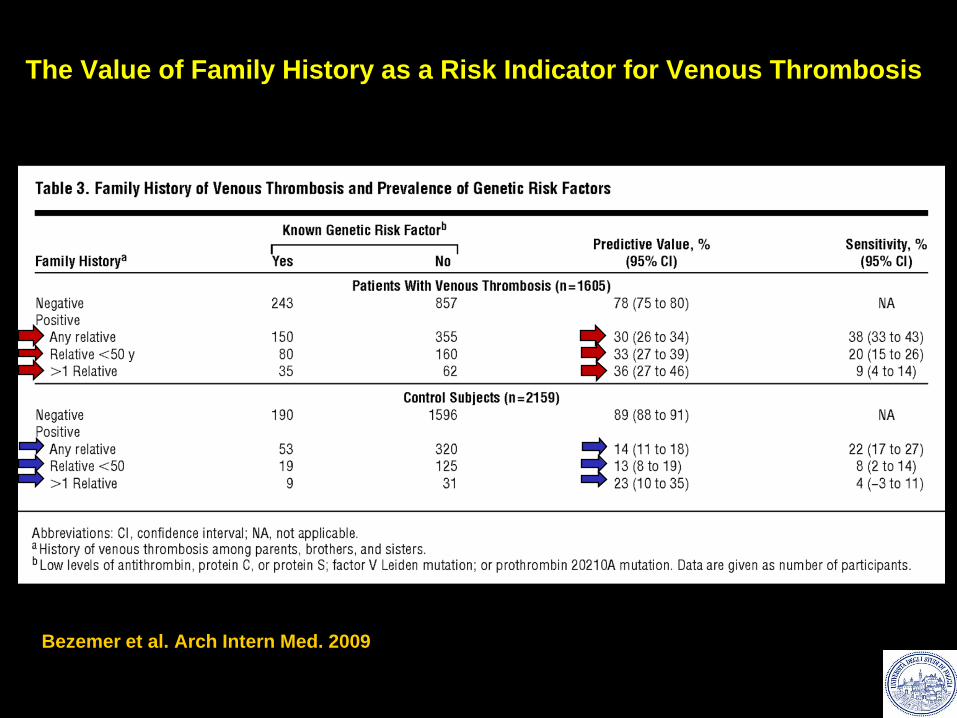
Bezemer et al. Arch Intern Med. 2009
The Value of Family History as a Risk Indicator for Venous Thrombosis
Key Points About Positive Family History
• Positive family history (1st degree relative) is VTE
risk factor (2.5-4.2 fold increased risk)
• Risk is inversely related to age when VTE occurred
• Risk is independent of presence of known genetic
thrombophilias
• Risk is due to unknown/additional risk factor
Other Inherited Risk Factors
Hyperhomocysteinemia (?)
Factor VIII (mixed)
Dysfibrinogenemias
Factor V mutations Very rare
Factor II mutations
Unique mutations
ABO
Hemoglobinopathies
Chi va studiato?
Come interpretare un test positivo/negativo?
• Asintomatico
• Asintomatico a rischio
- Tr. arteriosa
- TVP
- Gravidanza
- EP/Ter Sost
• Sintomatico
- Tr. arteriosa
- TVP
- Gravidanza
• Asintomatico
• Adulto
• Minore
• Asintomatico a rischio
- Tr. arteriosa
- TVP
- Gravidanza
- EP/Ter Sost
• Sintomatico
- Tr. arteriosa
- TVP
- Gravidanza
Quali test eseguire?
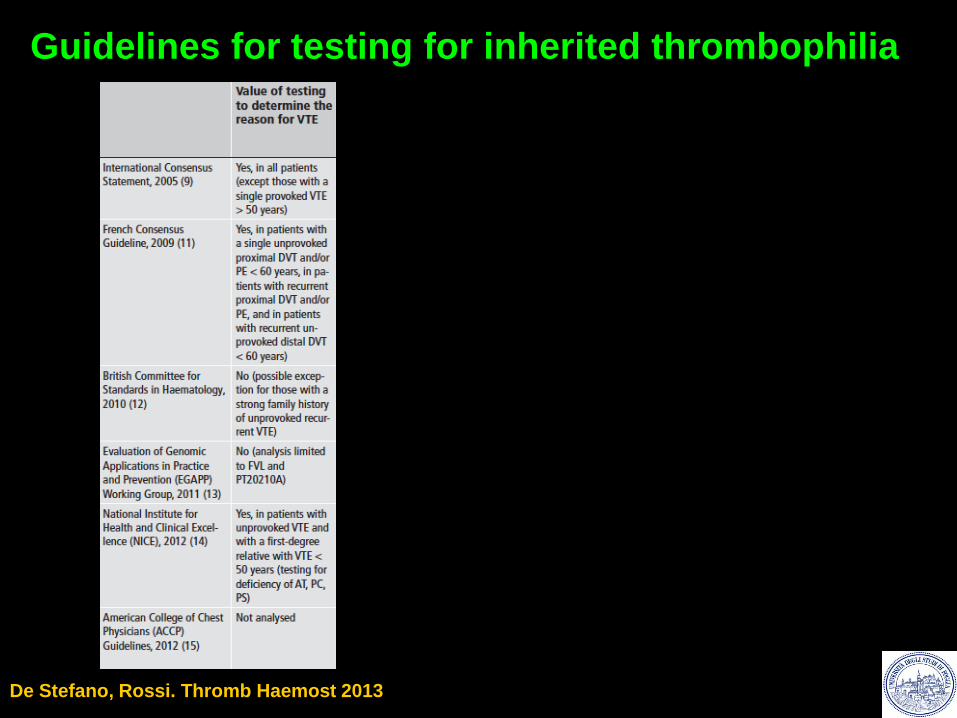
Guidelines for testing for inherited thrombophilia
De Stefano, Rossi. Thromb Haemost 2013
Individuo sano/Asintomatico
• Indiscriminate testing for heritable
thrombophilia in unselected patients presenting
with a first episode of venous thrombosis is not
indicated.
• Testing for heritable defects and, in particular,
genetic testing should be avoided in children
unless there is a strong clinical indication for it.
British Society for Haematology
Br. J. Haematol. 2001;114:512-28
Br. J. Haematol. 2010;149:209-20
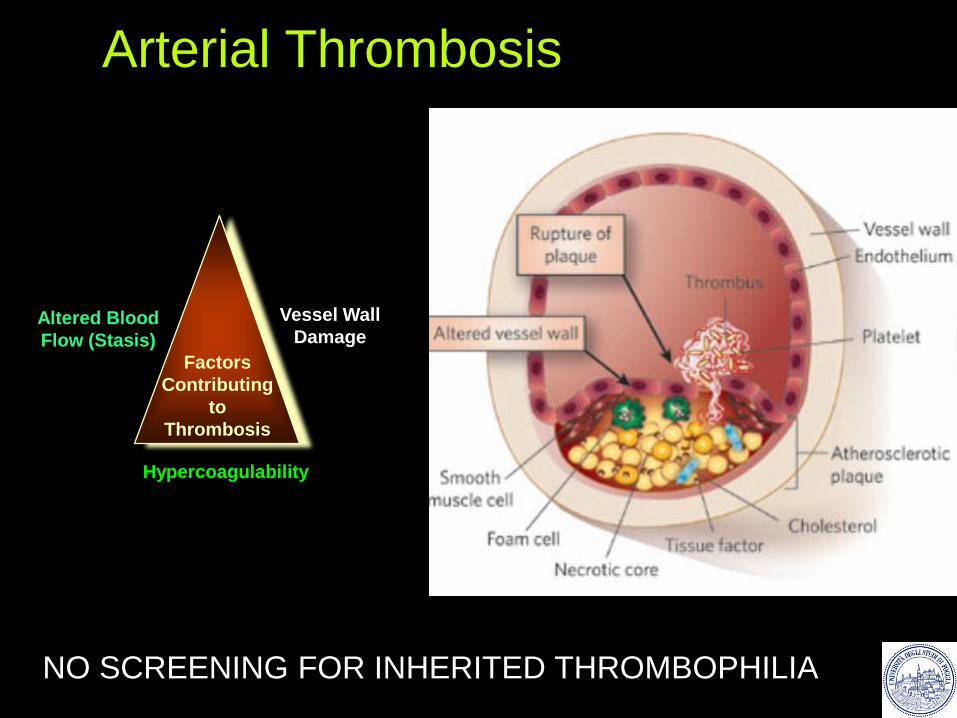
Arterial Thrombosis
Factors
Contributing
to
Thrombosis
Vessel Wall
Damage Altered Blood
Flow (Stasis)
Hypercoagulability
NO SCREENING FOR INHERITED THROMBOPHILIA
Testing for thrombophilia is unlikely
to be informative in an elderly
subject with a first venous
thromboembolism in whom the
family history is negative.
Paziente sintomatico
British Society for Haematology
Br. J. Haematol. 2001;114:512-28
• Testing is NOT recommended in unselected patients with UPPER LIMB
venous thrombosis (1B).
• Testing is NOT recommended in patients with CENTRAL VENOUS
CATHETER (CVC)-related thrombosis (1C).
• Testing for heritable thrombophilia after a first episode of cerebral vein
thrombosis (CVT) has uncertain predictive value for recurrence (C).
Decisions regarding DURATION OF ANTICOAGULANT THERAPY in
relation to the results of testing are NOT EVIDENCE-BASED.
• Testing is NOT indicated in patients with RETINAL VEIN occlusion (1B).
• Testing for heritable thrombophilia after a first episode of intra-abdominal
vein thrombosis has uncertain predictive value for recurrence (C). Br. J. Haematol. 2010;149:209-20
Paziente sintomatico
Paziente sintomatico
● a history of recurrent VTE;
● VTE before the age of 50 years;
● unprovoked VTE at any age; however, testing for protein C,
protein S, and antithrombin deficiency may be of lower
diagnostic yield in patients with a first lifetime VTE after age
50 years;
● VTE at unusual sites (eg, cerebral, mesenteric, portal,
hepatic);
● VTE patients with a positive family history of VTE; and
● VTE secondary to pregnancy, oral contraceptives, or hormone
replacement therapy.
Arch Pathol Lab Med 2002;126:1281-95
College of American Pathologists
Lo screening per trombofilia è indicato in caso di:
• Aborti ricorrenti (n=3) apparentemente inspiegati
• Morti endouterine ( n=1 >20 settimane di
gestazione)
• Preeclampsia, FGR non altrimenti spiegato
Prevenzione Del Tromboembolismo Venoso Associato Alla Gravidanza Statement condiviso tra le Società Italiana per lo Studio dell’Emostasi e
della Trombosi (SISET) e la Società Italiana di Ginecologia e Ostetricia (SIGO)
estensori del documento: E. Grandone, R. Abbate, V. De Stefano, E.M. Faioni, I. Martinelli,
G.Palareti, D. Tormene, F. Sirimarco, P. Martinelli. 2008
Trombofilia nella donna
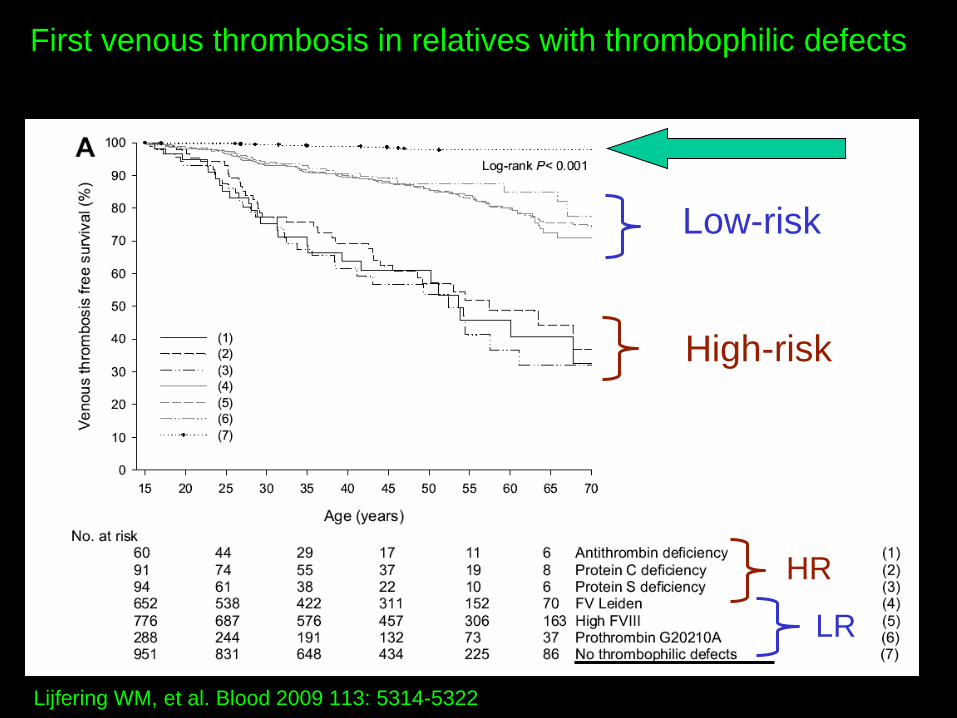
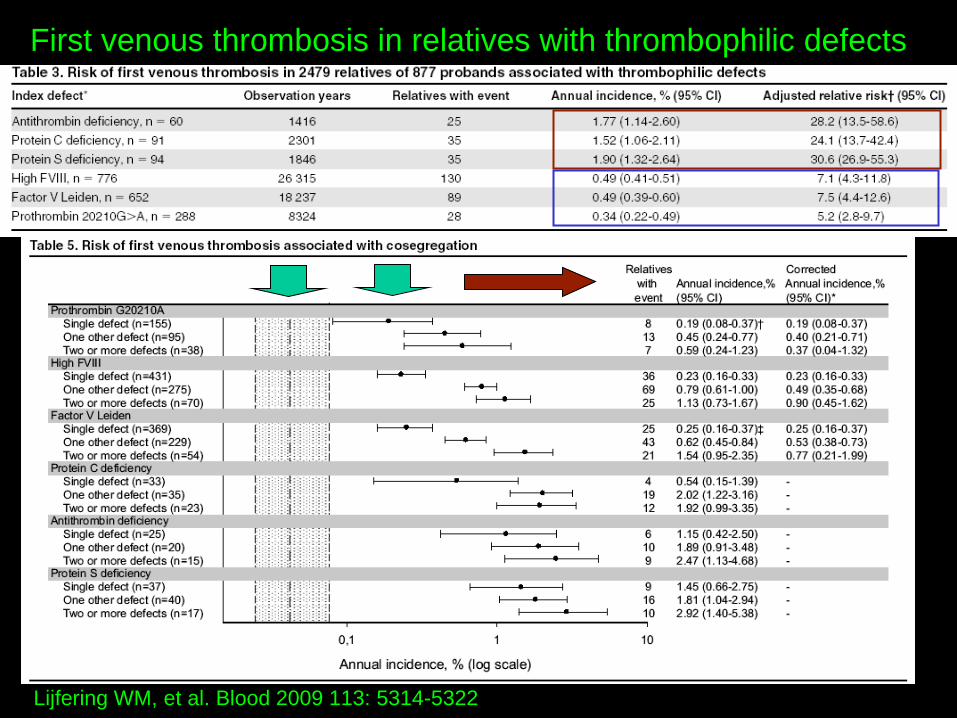
Lijfering WM, et al. Blood 2009 113: 5314-5322
First venous thrombosis in relatives with thrombophilic defects
Low-risk
LR
High-risk
HR
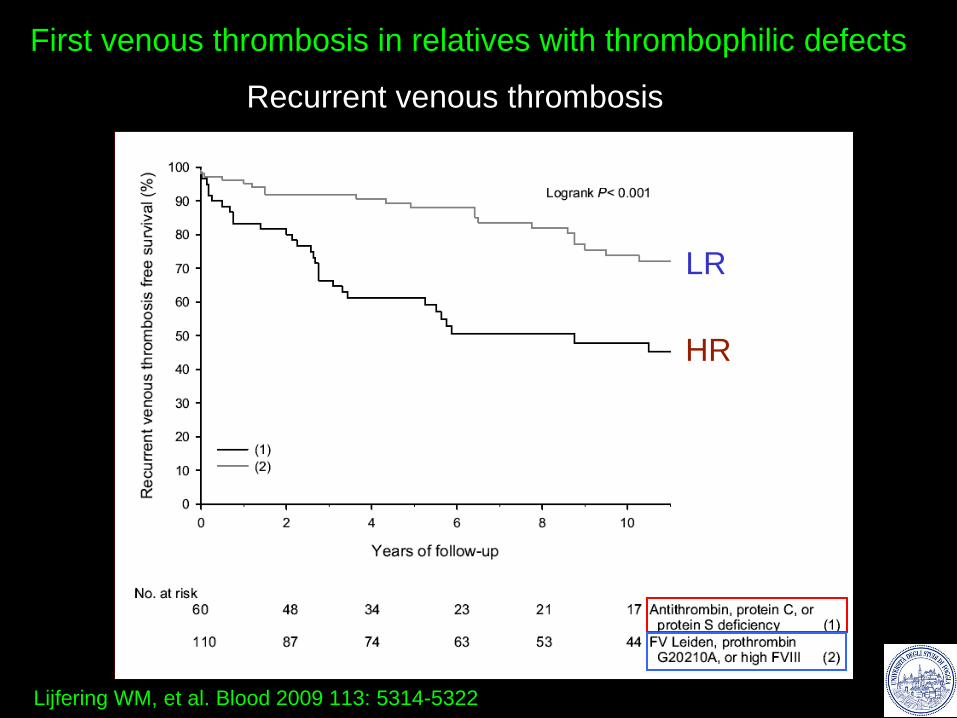
Lijfering WM, et al. Blood 2009 113: 5314-5322
First venous thrombosis in relatives with thrombophilic defects
Recurrent venous thrombosis
LR
HR
Lijfering WM, et al. Blood 2009 113: 5314-5322
First venous thrombosis in relatives with thrombophilic defects
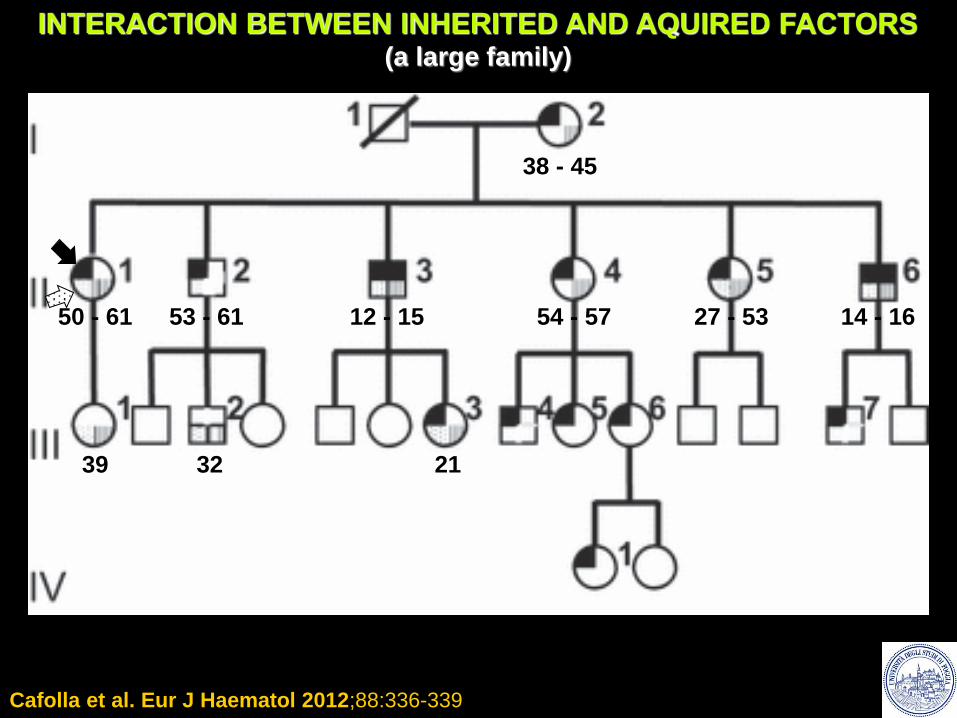
Cafolla et al. Eur J Haematol 2012;88:336-339
38 - 45
50 - 61 53 - 61 54 - 57 27 - 53 12 - 15 14 - 16
39 32 21
INTERACTION BETWEEN INHERITED AND AQUIRED FACTORS (a large family)
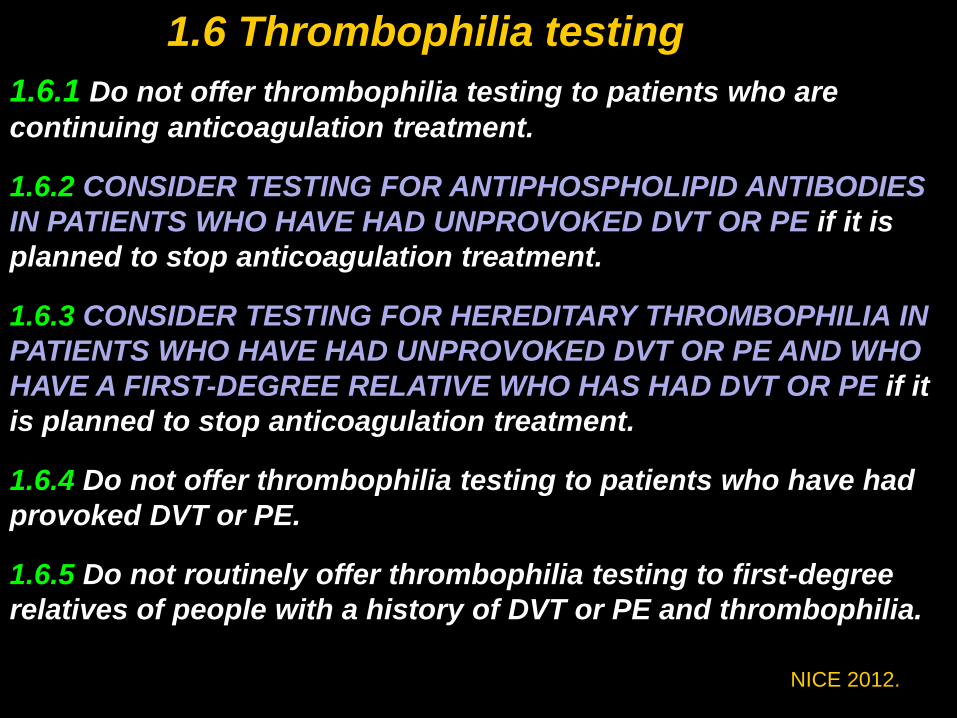
1.6.1 Do not offer thrombophilia testing to patients who are
continuing anticoagulation treatment.
1.6.2 CONSIDER TESTING FOR ANTIPHOSPHOLIPID ANTIBODIES
IN PATIENTS WHO HAVE HAD UNPROVOKED DVT OR PE if it is
planned to stop anticoagulation treatment.
1.6.3 CONSIDER TESTING FOR HEREDITARY THROMBOPHILIA IN
PATIENTS WHO HAVE HAD UNPROVOKED DVT OR PE AND WHO
HAVE A FIRST-DEGREE RELATIVE WHO HAS HAD DVT OR PE if it
is planned to stop anticoagulation treatment.
1.6.4 Do not offer thrombophilia testing to patients who have had
provoked DVT or PE.
1.6.5 Do not routinely offer thrombophilia testing to first-degree
relatives of people with a history of DVT or PE and thrombophilia.
NICE 2012.
1.6 Thrombophilia testing
Value of Genetic Thrombophilia Testing
• Testing not useful for arterial thrombosis
• Testing does not affect management of acute events
• Test results may influence decisions
– Prophylaxis during high-risk procedures
– Need to evaluate family members
– Estimate future risk for venous thrombosis (i.e.,
pregnancy complications, risk associated with oral
contraceptives, etc.)
– How long & how intensively to treat (?)
• Prevention of recurrence
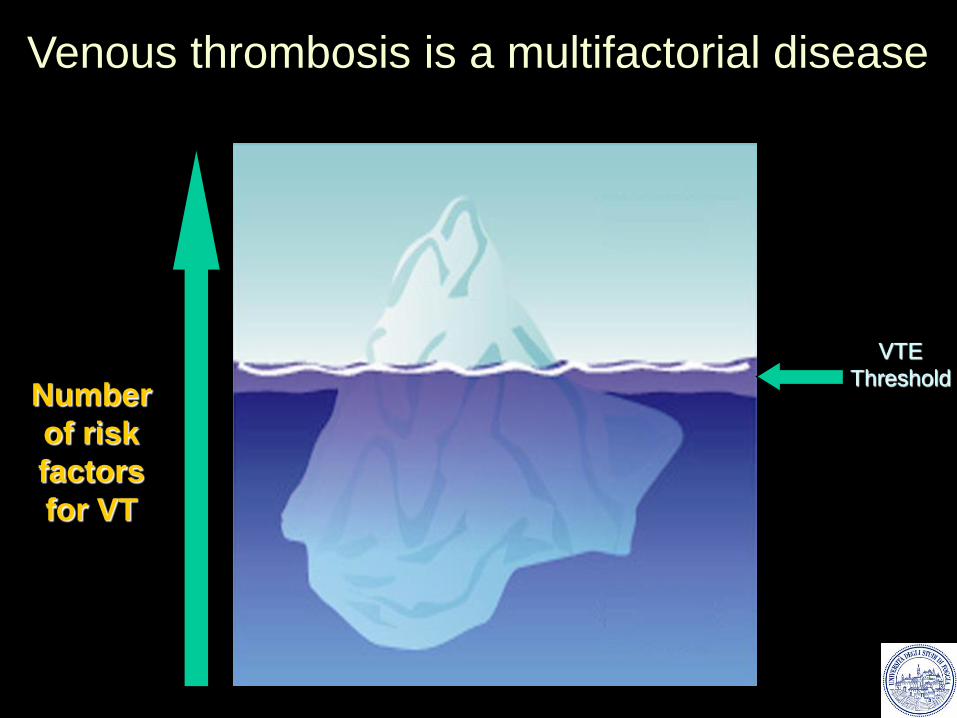
VTE
Threshold Number
of risk
factors
for VT
Venous thrombosis is a multifactorial disease
