quality and safety measures in acute kidney disease (akd
TRANSCRIPT

Quality and Safety Measures in Acute Kidney Disease (AKD) –ADQI XXII
Jay L. Koyner MD
@jaykoyner
Section of Nephrology
Department of Medicine
University of Chicago
Disclosures
Research funding from NIH, Astute,
Bioporto, NxStage, Satellite
Healthcare
Consulting Fees from Astute
Medical, Sphingotec, Pfizer, Baxter
2

Outline
Defining AKD
Defining the Denominator
Intensity and timing of follow up care
Evidenced based follow up care for • AKI
• AKI-D
3

141 Pages Long
132 Page Appendix
64 Pages of Tables
271 Pages Long
126 ReferencesSlide from Lui Forni
2.3.4: Evaluate patients 3 months after AKI for resolution, new onset, or worsening of pre-existing CKD. (Not Graded)
If patients have CKD, manage these patients as detailed in the KDOQI CKD Guideline (Guidelines 7–15). (Not Graded)
If patients do not have CKD, consider them to be at increased risk for CKD and care for them as detailed in the KDOQI CKD Guideline 3 for patients at increased risk for CKD. (Not Graded)
KDIGO 2012 Clinical Practice Recommendations for
Post-AKI Care

6

7
Defining Acute Kidney Disease

8
Defining Acute Kidney Disease

AKD: Where Tertiary Prevention meets Primary Prevention
Kashani et al., CJASN 2019 – ADQI XXII 9

Statement #1 - In order to optimize the care of patients with AKI/AKD health care systems need to quantitate the number of patients who need and do receive follow-up care subsequent to their index AKI hospitalization.
10
11
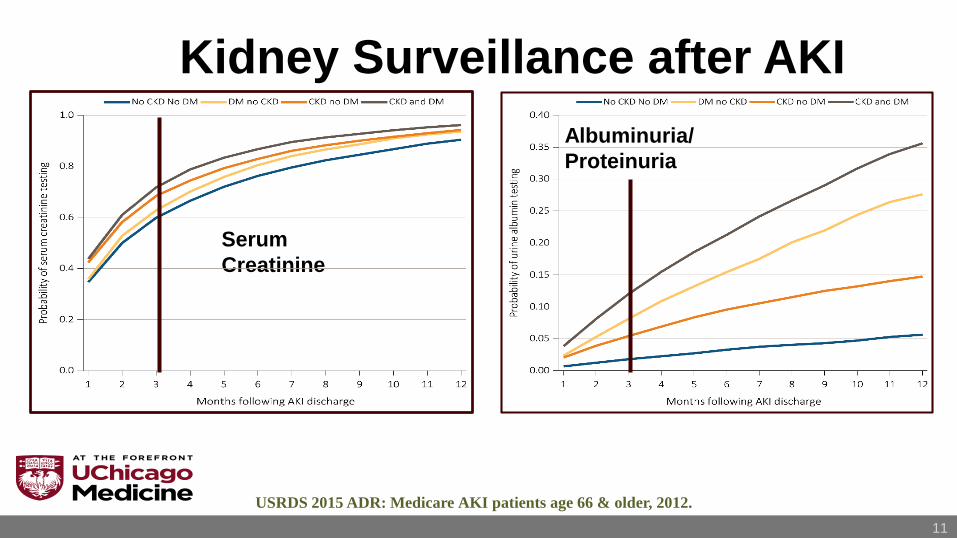
Kidney Surveillance after AKI
Serum
Creatinine
Albuminuria/
Proteinuria
USRDS 2015 ADR: Medicare AKI patients age 66 & older, 2012.

Siew et al. JASN 2012 12
Outpatient Nephrology Referral Among Patients with eGFR <60 ml/min/1.73 m2 After AKI
44% Recovered/
Improved
8.5% Referred
0.2% on RRT
11.5% Died
36% None

13
Disparity between Nephrologists' Opinions and Contemporary Practices for
Follow-up after AKI Hospitalization.
Divya J. Karsanji et al. CJASN 2017;12:1753-1761

Statement #2 - Intensity and appropriateness of follow-up depends on patient characteristics as well as severity, duration and course of AKI.
14

1 in 5 Patients with AKI Are Re-Hospitalized Within 30 Days
(N=111,778 Matched Pairs)
Silver, SA et al. Am J Med 2016; Oct (epub)
Slide Courtesy of E. Siew
HR 1.53 [95% CI: 1.50-1.57]
18% Rehospitalized
10% ER Visit
Est. cost of readmission = $40 million/yr

Relapsing AKI –Associated with Adverse outcomes
Kellum JA et al, Am J Resp Crit Care Med, 2017

Sawhney et al NDT
2018
• 7,491 patients
referred to
Nephrology in BC,
Canada
• Looking at predictors
of Kidney failure and
Death
• Prior history of AKI
increased the risk
failure and death in
those with eGFR >
30 ml/min

18

Can we utilize other physicians to care for those with AKD?

20
KAMPS Components
Kidney Function
• Kidney function measurement by serum creatinine or cystatin C; measured or
estimated GFR
• Proteinuria / albuminuria
• When available consider biomarkers, imaging and other tests as feasible and
indicated
Advocacy
• Patient and Caregiver education about AKI and CKD
• Communication with other care providers (i.e., general practitioners, dieticians,
nurses, pharmacists and social workers)
Medications
• Medication reconciliation, review and management
• Specifically discuss risk benefits of ACEI/ARB
• Review RENDS-Renal Excreted and Nephrotoxic Drugs and OTC medications
Pressure
• Ensure patient understands blood pressure goals and targets
• Discuss fluid status, ideal weight and the role of diuretics
Sick Day Protocols
• Educate patients on medications that need monitoring during
acute illnesses
Statement #3 - Post AKI - AKD Care should be evidenced based and evolve with emerging data.
21

Alan S. Go et al. CJASN doi:10.2215/CJN.12591117©2018 by American Society of Nephrology

Siew: AKI increased risk of CHF in Veterans • Observational study of 300,868
hospitalized veterans (2004-11)
• Matching Pairs
• Incident HF defined as 1 hospitalization
or >2 outpatient visits with CHF
• 1 year incidence of CHF in those with
AKI was 30.8 per 1,000 person years
vs. 24.9 (p<0.001)
• Relative Risk of CHF post AKI was 1.28
(1.23 to 1.34)
• AKI associated with increased mortality
too

Strategies to Improve OutcomesWho?
9,973 patients in Alberta, Canada, who survived for > 3 months after AKI with baseline eGFR > 45 mL/min/1.73 m2
Externally validated in 2,761 AKI survivors in Ontario
Primary outcome: sustained eGFR < 30 mL/min/1.73m2
James MT et al, JAMA, 2017

James MT et al,
JAMA, 2017

Pannu et al – Mortality and ACE/ARB Post AKI • 46,253 Hospitalized Canadian
adults with AKI – 50% increase in
SCr from preadmit values
• ACE/ARB exposure within 6 month
(n=22,193)
• Propensity score matched-pairs
• ACE/ARB exposure associated
with decreased mortality after 2
years (aHR 0.85(0.81-0.89)
• However increased risk of Renal
Hospitalization 1.28(1.12-1.46)
• No increased risk of ESRD

Strategies to Improve OutcomesHow?
Does follow-up with a nephrologist in an AKI Follow-up Clinic within 30-days after hospital discharge reduce the number of major adverse kidney events at one year?
Nephrologist Follow-up versus USual care after an acute kidney Injury hospitalizatiON (FUSION): A randomized controlled trial
Clinicaltrials.gov NCT02483039
4-site RCT, envisioned as a vanguard phase for a definitive clinical trial
Sam Silver and Ron Wald PI

Predicting CKD: With AKI Biomarkers- ASSESS-AKI…
CV Surgery
Go et al. BMC Nephrology 2010 Follow-up supported by NIH-NIDDK

29
Statement 4: Quality metrics for AKI-D and post-discharge AKD-D should be similar to quality metrics during hospitalization, and distinct from ESRD measures. In addition, there need to be specific quality metrics for the outpatient setting.



32
WATCH-ME Components
Weight Assessment
Discuss Dry Weight monitoring and permissive hypervolemia
Discuss the role for diuretics in maintaining urine output and ideal volume status
Access
Educate patients about the care of central venous catheters
Vein preservation protocols / awareness
When appropriate begin to plan and educate about the role of arteriovenous access
and other RRT modalities
Teaching
Patient and Caregiver education about dialysis requiring AKD and short- and long-term
risks and consequence
Communication with other care providers (e.g., general practitioners, dieticians, nurses,
pharmacists and social workers) about patient needs (e.g., alterations in medication
regimens in the setting of new RRT).
Clearance
Frequent assessments of underlying renal function (via pre-dialysis labs or timed
clearances)
Frequent assessments of the quality of the RRT being provided to ensure adequate
clearance
Hypotension
Patient Education and optimization of care to avoid intradialytic about hypotension
Education around blood pressure medications administration in the peri-RRT period
MEdications
Medication reconciliation, review and management
Specifically discuss risk benefits of ACEI/ARB
Review RENDS (Renal Excreted and Nephrotoxic Drugs) and over the counter
medications

Conclusions
As Nephrologists we can do a better job of following up patients after AKI / AKD
This follow up should be standardized and evidence based and should include more than just those with AKI-RRT
Future studies should inform the timing, intensity and method of AKI/ AKD follow-up.
33

Thanks Kathleen Liu
Michael Heung
Vin-Cent Wu
Lui Forni (not pictured)
ADQI Leadership Kashani, Haase, Rosner
Sam Silver and Ed Siew
34
