quality education for a healthier scotland psychology equality and diversity impact assessment –...
TRANSCRIPT

Quality Education for a Healthier Scotland
Psychology
Equality and Diversity Impact Assessment – Accessing Psychological Therapies

Quality Education for a Healthier Scotland
Psychology
REFERRAL RECEIVED
BY SERVICE
INITIAL PSYCHOLOGICAL ASSESSMENT IS COMPLETE
AND TREATMENT
PLAN IS AGREED*
(THIS MAY TAKE A FEW WEEKS)
DELIVERY OF LOW INTENSITY PSYCHOLOGICAL THERAPIES/
INTERVENTIONS (HIGH VOLUME)
REFERRAL MADE FROM
GP OR OTHER SOURCE
TRIAGE BY RECEIVING SERVICE
DECISION MADE TO ACCEPT
REFERRAL OR REFER
BACK/ ONWARDS
PSYCHOLOGICAL THERAPY TREATMENT
COMMENCES AS PLANNED
PATIENT NON ATTENDANCE
E.G. DNA
PSYCHOLOGICAL THERAPY
TREATMENT IS COMPLETED AS
PLANNED
PSYCHOLOGICAL THERAPY
TREATMENT IS NOT
COMPLETED AS PLANNED E.G. PATIENT SELF DISCHARGES
TIME
Care pathway

Quality Education for a Healthier Scotland
Psychology
Barriers to accessing Psychological Therapies
Anne Joice, Programme Director – Psychological Interventions, NHS Education Scotland
Helen Walker, Education Project Manager NHS Education Scotland

Quality Education for a Healthier Scotland
PsychologyOutline
Philosophical underpinning Case identification The development of the therapeutic relationship The therapy itself Minority groups
• Gender• Age• Ethnicity• Sexual orientation• Physical health• Disability• Mental health• Socio-economic

Quality Education for a Healthier Scotland
PsychologyPhilosophical barriers
Philosophical underpinning to health and therapy Mind-body separation
Constructs of illness Perception of problems as physical or spiritual Somatisation - expecting medication? Emotions may be expressed in terms of relationships
Evidence based Healthcare Rigorous scientific approaches Evidence developed on predominantly white / western
cultures Valuing spirituality, music, intuition, art, dreams…

Quality Education for a Healthier Scotland
PsychologyCase identification as a barrier
Stages people progress through prior to seeking help – experiencing symptoms, assessing whether treatment is required, weighing up options
‘Asian’ (which includes Indian, Bangladeshi and Pakistani) people, are more likely to present to their GP with physical manifestations of their mental health problems, and do so more frequently than White people (Commander et al 1997).
GPs are less likely to detect depression and more likely to diagnose people from an Asians background with a physical disorder (Wilson & McCarthy, 1994; Williams & Hunt, 1997)
Case identification tools have been developed and validated on White populations (Husain et al, 2007).
Cultural specific instruments are being developed (Singh et al, 1974; Abas, 1996) but have not been found to have high specificity (National Collaborating Centre for Mental Health, 2009) when compared with other measures.

Quality Education for a Healthier Scotland
Psychology
Barriers to the development of the therapeutic relationship
Communication, trust and the development of a therapeutic relationship are critical to success within psychological therapies
Language and cultural barriers may hinder its development Often communication of empathy from therapist to client will
often rely on modulation of the voice, eye contact, or other subtle means that may be lost across cultures
Belief and hope in the process from both therapist and client is thought to be critical
Many cultures have explicit or implicit taboos about relationships and their confidentiality

Quality Education for a Healthier Scotland
PsychologyThe therapy itself as a barrier
Cognitive Behavioural Therapy (CBT) is based on assessing the inter-relationship between the environment and the person; focusing on thoughts, feelings, physical symptoms and behaviour ‘cognition’ is a culturally based phenomenon
some people may be uncomfortable separating their thoughts and feelings may find the concept of challenging unhelpful thoughts a difficult one to
grasp may not accept that the mind has the ‘power’ to make a difference
What is deemed to be ‘normal’ or appropriate behaviour is also a culturally mediated phenomenon.
A lack of confidence in cultural knowledge and understanding may result in some therapists lacking conviction in their ability to help people find solutions to problems that are outside their personal experience.
Transference may be based on a cultural divide

Quality Education for a Healthier Scotland
PsychologyGender
Men and women are exposed to different risks to mental health and well-being that are linked to socio-economic status, social (and reproductive roles), discrimination, violence and abuse.
The incidence and prevalence of depression and anxiety is higher among women than men (Melzer et al, 2001). - this same pattern is consistent across ethnic groups (Nazroo, 1997; Melzer et al, 2001; Melzer et al, 2004).
Men have higher levels of suicide than women (DH, 2001; WHO, 2003; Samaritans, 2003), have higher levels of substance misuse (Singleton et al, 2001; Scottish Executive, 2003) and are more likely to engage in violent behaviour (Myers, McCollam & Woodhouse, 2005).
There are crucial differences in help seeking behaviour particularly in relation to trauma - men being less likely to address this as part of a psychological therapy
Quality Education for a Healthier Scotland
Psychology
Age IAPT first wave sites have shown attrition rates decrease when home visits
are used for assessment ( 91% attendance) IAPT service outcome focus on return to work became a perverse incentive
that discriminated against Older adults It is possible that features of adult services can discriminate against older
adults e.g. referral ‘opt in’ arrangements Even when mental health problems are identified, diagnosis doesn’t
necessarily result in referral to psychological therapies. GPs often don’t refer, they don’t know what’s available and how effective it can be (Robson and Higgon 2010)
Depression is viewed as an inevitable part of ageing and thus less deserving of treatment and it’s assumed older adults aren’t interested in psychological therapies due to stigma associated with mental illness (Laidlaw 2003)
Women over 60 will is 4 times more likely than a man to fear going out at night (Palmer et al, 2003)

Quality Education for a Healthier Scotland
PsychologyEthnicity
Common barriers to mental health services include; language, stereotyping, lack of awareness of different understandings of mental illness, cultural insensitivity including toward religious or cultural beliefs, colour-blind approach, direct or indirect racism.
Consideration should be given to what mental health / illness means in different communities, and what the specific experience of stigma and discrimination is to each individual.
Reporting on the Newham IAPT demonstration site, Clarke et al. (2009) found the population consisted of 49% from Black and Minority Ethnic (BME) communities, with 13% not speaking English.
One in five of the people seen in Newham referred themselves to the service. When compared to GP referrals, self-referral patients were at least as ill and tended to have had their problems for longer

Quality Education for a Healthier Scotland
PsychologySexual orientation
Many of the risk factors are related to the experience of: economic and social discrimination; abuse, bullying, harassment and violence; and social isolation (Myers, McCollam & Woodhouse, 2005).
Factors that affect access to mental health services include; reluctance by LGBT people to disclose their sexual orientation
to health care professionals because of a fear of discrimination or negative response
the lived experience of discrimination and negative reaction following disclosure, including breaches of confidentiality

Quality Education for a Healthier Scotland
PsychologyPhysical disability
Morris (2004) reports that people with physical impairments and mental health support needs often have difficulty accessing mental health services because of their:
physical impairment difficulty using physical health services because of the inadequate
recognition of their mental health needs negative attitudes amongst staff towards mental health services.
Mann (2004)reports that cognitive impairment is an important factor in explaining treatment failure, commonly due to impaired attention, learning, memory and cognitive flexibility. There’s a strong likelihood that people are likely to drop out of 12 week CBT programmes.
People with specific perceptual or sensory disability (deaf / blind) may also have difficulty articulating responses to the therapist
Quality Education for a Healthier Scotland
PsychologyMental health problems
Rogers and Pilgrim (2003) have reported on the inequalities created by service provision which they state has three dimensions:
equity of access to services negative or stigmatising experience of mental health service
provision longer term impact for individuals.
Clinicians working in mental health can experience difficulty in accessing mental health services

Quality Education for a Healthier Scotland
PsychologySocioeconomic deprivation
Structural inequality can lead to people feeling distressed and hopeless, and to ‘unfairness being construed as in some way of their own making’ (Myers, McCollam & Woodhouse, 2005, p21) which in turn present barriers in making attempts to access services.
Travel costs to attend therapy can be off-putting

Quality Education for a Healthier Scotland
Psychology
Attrition rates in a primary care service
Jim WhiteSTEPS Primary Care Mental
Health Team

Quality Education for a Healthier Scotland
Psychology
0
5
10
15
20
25
30
35
40
1 2 3 4 5 6 7 8 9 10
Referrals by SIMD category (1 = most affluent, 10 = most deprived).

Quality Education for a Healthier Scotland
PsychologySIMD and therapy type
No differences between CBT and PCT
No SIMD differences in attendance and completion but
SIMD 10s significantly less likely to opt-in
Quality Education for a Healthier Scotland
Psychology
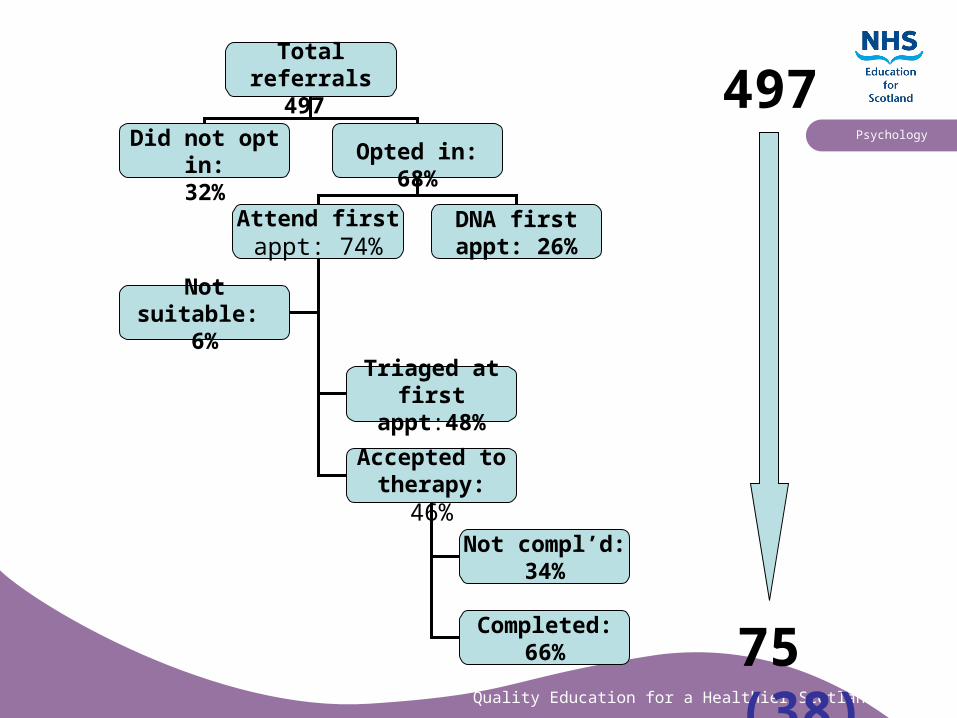
Total referrals 497
Did not opt in:32%
Opted in:68%
Attend first appt: 74%
DNA first appt: 26%
Triaged at first appt:48%
Accepted to therapy: 46%
Not compl’d:34%
Completed:66%
Not suitable: 6%
497
75 (38)

Quality Education for a Healthier Scotland
Psychology
All services are now self-referral

Quality Education for a Healthier Scotland
PsychologyNew STEPS Brochure
Therapist contactAdvice Clinic‘Call Back’
GroupsStress ControlMood MattersFirst StepsStep into ShapeConnectLifeGymDay workshops
Non-therapist contact
Healthy Reading
Steps out of Stress booklets
www.glasgowsteps.com
www.glasgowhelp.com
‘100 people’ DVD
‘Everything you always..’ DVD
STEPS sounds / podcasts
Other
Mental health info and advice
مدد لئے کے والوں بولنے اردوPartner organisations
Stay in touch with STEPS

Quality Education for a Healthier Scotland
Psychology
Call-back GP-referral National
Time to contact 8.7 hours 28 days
Attend first appt (%) 95 50
Complete treatment (%) 84 34
Quality Education for a Healthier Scotland
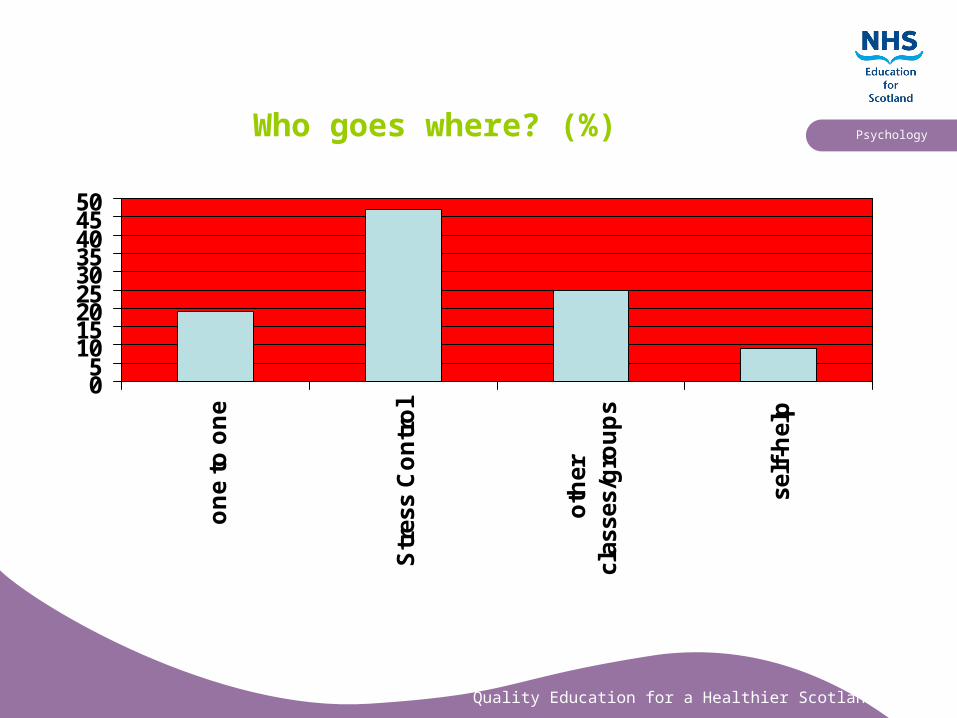
PsychologyWho goes where? (%)
05
101520253035404550
on
e to
on
e
Str
ess
Co
ntr
ol
oth
ercl
asse
s/g
rou
ps
self
-hel
p

Quality Education for a Healthier Scotland
PsychologyRecommendations….
Developing a culturally competent, gender sensitive service
Population level Service level Individual level
For more information on the legislation framework please see Equal Minds available at http://www.scotland.gov.uk/Publications/2005/11/04145113/51135