quality, safety and patient experience strategy
TRANSCRIPT

Quality, Safety and Patient Experience Strategy
November 2015
www.castlepointandrochfordccg.nhs.uk

Quality, Safety and Patient Experience Strategy – Nov 2015
2
Document Name Quality, Safety & Patient Experience Strategy
Version V7
Author/s Name
Job Title/s
Jenny Briggs
Interim Programme Director - Transformation
Executive Lead Tricia D’Orsi
Approved by Governing Body
26.11.2015
Review Date 2.11.2018
Change Record
Date Version Changes made
18.9.15 7, still in
draft
Addition of comments from Tricia D’Orsi
17.10.2015 Version 7 Comments added TD

Quality, Safety and Patient Experience Strategy – Nov 2015
3
Contents
1. Foreword ........................................................................................................................................ 5
2. Introduction .................................................................................................................................... 6
2.1 Background and Context ..................................................................................................... 6
2.2 Defining Quality, Safety and Patient Experience............................................................. 6
2.3 Purpose of this strategy ....................................................................................................... 7
3. Our Commitment to Quality, Safety and Patient Experience ................................................ 8
3.1 Our Values............................................................................................................................. 8
3.2 Our Vision .............................................................................................................................. 8
3.3 Vision for Quality, Safety and Patient Experience........................................................... 9
4. Quality, Safety and Patient Experience through Commissioning ....................................... 11
4.1 Procurement ........................................................................................................................ 11
4.2 Incentivising and Monitoring Quality with our Providers ............................................... 11
4.3 Partnership Working .......................................................................................................... 12
4.4 Patient and Public Involvement ........................................................................................ 12
4.4.1 Commissioning Reference Group ............................................................................ 12
4.4.2 Patient Participation Groups (PPG) ......................................................................... 12
4.4.3 Governing Body .......................................................................................................... 13
5 National drivers for quality, safety and patient experience .................................................. 14
5.1 NHS Five Year Forward View .......................................................................................... 14
5.2 The NHS Outcomes Framework ...................................................................................... 14
5.3 Harm Free Care & the NHS Safety Thermometer ........................................................ 16
5.4 Summary Hospital-Level Mortality Indicators (SHMI) ................................................... 16
5.5 Care Quality Commission (CQC) – Essential Standards ............................................. 17
5.6 National Institute for Health and Care Excellence (NICE) ........................................... 17
5.7 Quality, Innovation, Productivity & Prevention (QIPP) ................................................. 18
5.8 National Reporting and Learning System (NRLS) ........................................................ 19
5.9 National Reports and Investigations ................................................................................ 19
5.10 “No Harms Event” ............................................................................................................... 20
5.11 Co-Commissioning ............................................................................................................. 20
5.12 Safeguarding adults and children .................................................................................... 20
5.13 Parity of Esteem ................................................................................................................. 21
6 Roles and Responsibilities for Quality Assurance................................................................. 22
6.1 The Role of the Clinical Commissioning Group ............................................................. 22

Quality, Safety and Patient Experience Strategy – Nov 2015
4
6.1.1 Our Role as Co-Commissioners .............................................................................. 22
6.2 Group and Team Responsibilities for Quality, Safety & Patient Experience ............ 23
6.2.1 The Governing Body .................................................................................................. 23
6.2.2 The Quality and Governance Committee ............................................................... 23
6.2.3 The Clinical Quality Review Group (CQRG) .......................................................... 23
6.2.4 The Quality Support Team ........................................................................................ 23
6.2.5 The Role of Member Practices ................................................................................. 24
6.2.6 Quality Surveillance Groups (QSGs)....................................................................... 24
6.2.7 The Commissioning Support Unit (CSU) ................................................................ 24
6.3 Individual Roles and Responsibilities .............................................................................. 25
6.3.1 The Accountable Officer ............................................................................................ 25
6.3.2 The Chief Nurse.......................................................................................................... 25
6.3.3 All CCG Staff ............................................................................................................... 25
7. Quality, Safety and Patient Experience Assurance Processes ........................................... 26
7.1 Monitoring and Assurance for Commissioned Services ............................................... 26
7.1.1 Using data to assess and improve quality, safety and patient experience ........ 27
7.1.2 Complaints and patient feedback ............................................................................ 27
7.2 Quality Monitoring for New Projects and Services ........................................................ 27
7.2.1 QIA Tool and Process................................................................................................ 28
7.3 Other Quality, Safety and Patient Experience Mechanisms ........................................ 30
7.3.1 Safeguarding adults and children ............................................................................ 30
7.3.2 Information Governance and Caldicott ................................................................... 31
7.3.3 Clinical Audit ............................................................................................................... 31
7.3.4 Medicines Management ............................................................................................ 31
7.3.5 Domestic Abuse.......................................................................................................... 32
8. Next Steps and Developments ................................................................................................. 33

Quality, Safety and Patient Experience Strategy – Nov 2015
5
1. Foreword
“Continuously improving patient safety should be at the top of the health
care agenda for the 21st century. The injunction to do no harm is the
defining principle of the clinical professions”
(Lord Darzi; High Quality Health Care for all 2008).
This Quality Strategy is to underpin the commissioning of the highest quality care services
for the people of Castle Point and Rochford.
The CCG wants the implementation of this Strategy to provide local pride in the NHS and
wants the people of Castle Point and Rochford to be confident that their healthcare services
are amongst the very best.
The CCG will strive to ensure that the high quality health care it commissions is provided on
the basis of its on-going commitment to equality of experience and outcomes, to everyone in
Castle Point and Rochford, no matter who they are or where they live.
The CCG vision “Quality Care First Time, Equitably Delivered in Response to Patients
Needs by Responsive Local Clinicians” puts quality at the centre of all that we do as an
organisation and as a result integrates the organisational functions of clinical, corporate and
financial governance.
By the integration of these functions the CCG will be able to recognise the early indications
of a failing service and give the appropriate support and take the necessary measures to
protect patients.
The purpose of the strategy is
to ensure that patients and their assessed needs are at the centre of commissioning
decisions
to ensure commissioned services are safe, clinically effective and provide a positive
experience for patients
to assure the robustness of systems and processes in place to deliver safe services
and positive experiences
to ensure that measures of quality are focused on structures, processes and most
importantly outcomes
to confirm the collaborative arrangements that will be in place with other health
commissioners and wider stakeholders
to demonstrate that the CCG has the leadership and governance arrangements in
place to meet its statutory requirements and responsibilities.
This purpose will be upheld in the CCG’s consideration of all commissioning decisions
related to all health service provision for all client groups, children, adults, older people,
people requiring mental health services and people with learning disabilities whether
receiving care in acute, community or primary care settings.

Quality, Safety and Patient Experience Strategy – Nov 2015
6
2. Introduction
2.1 Background and Context
Over the last 10 years healthcare quality, safety and patient experience have featured in a
number of high profile national inquiries and reports and these have received significant
media attention. Unfortunately many reviews have been prompted through failings in care;
however, each report provides opportunities for learning to ensure that all NHS organisations
can make improvements to quality of care and to reduce patient safety risks.
In 2013, the Prime Minister invited Professor Donald Berwick, internationally known for his
work on patient safety, to lead a review to “make zero harm a reality in our NHS.” The
review considered the breakdown of care at the Mid-Staffordshire NHS Foundation Trust
and the wider NHS quality and safety culture and landscape. In his report Professor Berwick
calls on all leaders to prioritise quality and safety in all areas of their work:
“All leaders concerned with NHS healthcare – political, regulatory, governance, executive, clinical and advocacy – should place quality of care in general, and patient safety in particular, at the top of their priorities for investment, inquiry, improvement, regular reporting, encouragement and support”
(Professor Donald Berwick, published in August 2013)
Castle Point and Rochford Clinical Commissioning Group is a group of local GPs and
clinicians who commission (buy) services for our community which is around 182,000
people. This gives us both the opportunity and responsibility to ensure that quality, safety
and patient experience is prioritised and protected as services are provided and developed
within our health and care community.
2.2 Defining Quality, Safety and Patient Experience
The Care Quality Commission, the independent regulator of health and social care in
England, assess services against five criteria which provide a helpful definition of quality,
safety and patient experience:
1. Are they safe?
2. Are they effective?
3. Are they caring?
4. Are they responsive to people’s needs?
5. Are they well-led?
We believe this wide definition extends to all aspects of care, and includes: privacy, dignity,
care and compassion, politeness, respect, safeguarding and protection of vulnerable people
as well as effective clinical treatment. Sometimes we call these areas “the basics” or
“fundamentals” in care provision, and we believe that every person deserves these whoever

Quality, Safety and Patient Experience Strategy – Nov 2015
7
they are and wherever they live. We are working with the providers of services to ensure
this will be the case.
2.3 Purpose of this strategy
The purpose of the strategy is:
To ensure that patients and their assessed needs are at the centre of our
commissioning decisions
To ensure commissioned services are safe, clinically effective and provide a positive
experience for patients
To assure the robustness of systems and processes in place to deliver safe, effective
services and positive experiences for patients
To ensure that measures of quality are focused on structures, processes and most
importantly outcomes
To confirm the collaborative arrangements that will be in place with other health and
care commissioners and wider stakeholders
To demonstrate that we have the leadership and governance arrangements in place
to meet our statutory requirements and responsibilities
This strategy sets out our commitment, vision and aims to commission the highest quality
care services for the people within Castle Point and Rochford so that people can be
confident that their health and care services are amongst the very best.
Quality, Safety and Patient Experience Strategy – Nov 2015
8
3. Our Commitment to Quality, Safety and Patient Experience
3.1 Our Values
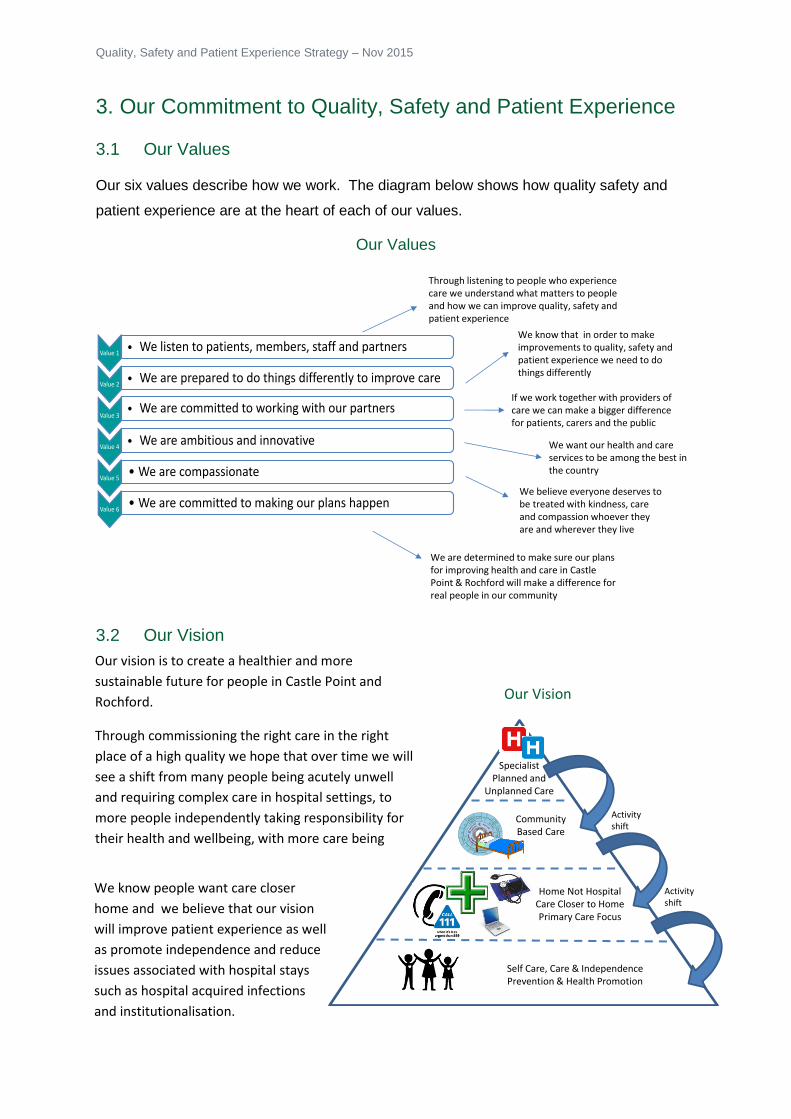
Our six values describe how we work. The diagram below shows how quality safety and
patient experience are at the heart of each of our values.
Our Values
3.2 Our Vision
Value 1• We listen to patients, members, staff and partners
Value 2• We are prepared to do things differently to improve care
Value 3• We are committed to working with our partners
Value 4• We are ambitious and innovative
Value 5• We are compassionate
Value 6• We are committed to making our plans happen
We know that in order to make improvements to quality, safety and patient experience we need to do things differently
We want our health and care services to be among the best in the country
Through listening to people who experience care we understand what matters to people and how we can improve quality, safety and patient experience
If we work together with providers of care we can make a bigger difference for patients, carers and the public
We believe everyone deserves to be treated with kindness, care and compassion whoever they are and wherever they live
We are determined to make sure our plans for improving health and care in Castle Point & Rochford will make a difference for real people in our community
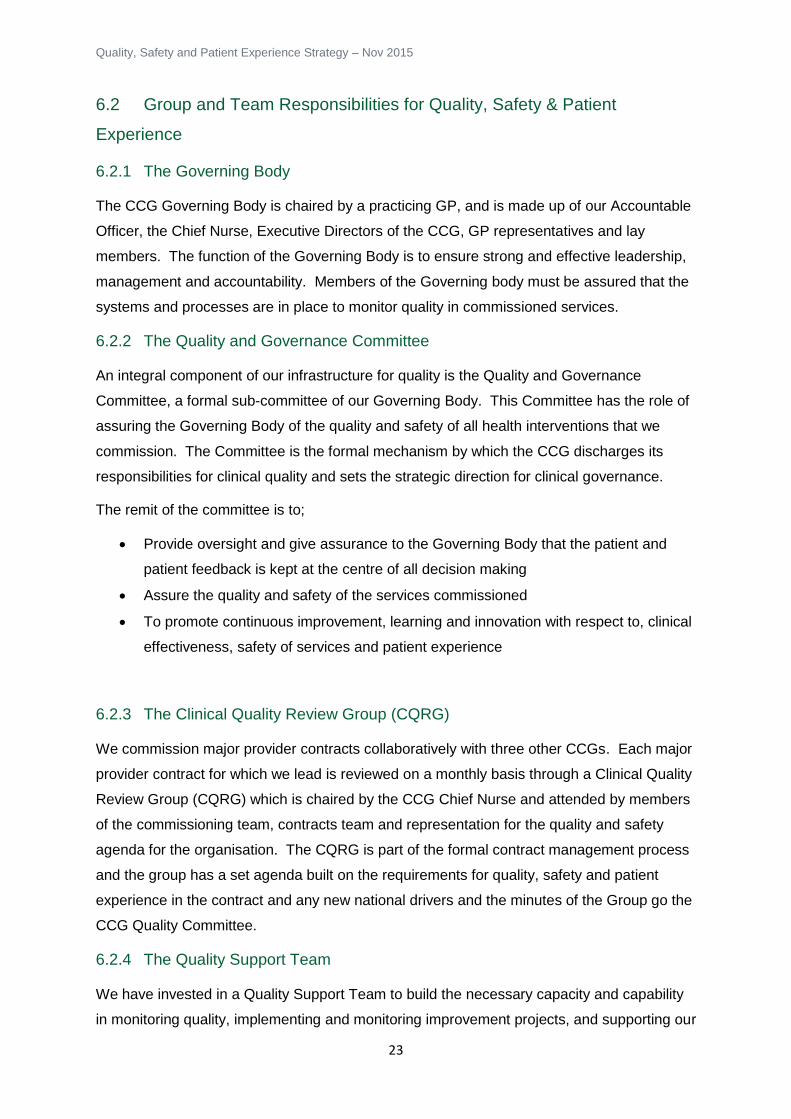
Our Vision
IntermediateCare & Discharge
Planning & Support
Self Care, Care & IndependencePrevention & Health Promotion
Home Not HospitalCare Closer to HomePrimary Care Focus
Community Based Care
Specialist Planned and
Unplanned Care
Activityshift
Activityshift
Our vision is to create a healthier and more
sustainable future for people in Castle Point and
Rochford.
Through commissioning the right care in the right
place of a high quality we hope that over time we will
see a shift from many people being acutely unwell
and requiring complex care in hospital settings, to
more people independently taking responsibility for
their health and wellbeing, with more care being
delivered in the community and closer to patients’
homes. We know people want care closer
home and we believe that our vision
will improve patient experience as well
as promote independence and reduce
issues associated with hospital stays
such as hospital acquired infections
and institutionalisation.

Quality, Safety and Patient Experience Strategy – Nov 2015
9
3.3 Vision for Quality, Safety and Patient Experience
Our vision is that health and care services within Castle Point and Rochford will be:
Effective: Meeting the needs of the person receiving care/treatment and supporting
them at their time of need
Safe: Without error, and in a way that protects people from harm, especially our
most vulnerable people
Compassionate: Offering a good experience for patients and treating them with
dignity, respect and kindness
We know nobody enjoys being unwell or injured, but we believe it is our responsibility to
commission care that gives the best possible experience for people at their time of need.
We are committed to ensuring that the services we commission fulfil our person centred
quality statements that ensure patients and carers are at the forefront of our vision.
Quality Statements
People will receive care and support in the most
appropriate environment that enables them to retain
and regain their independence
People will know what services are available to them
and will be involved and engaged In all aspects of their
care
People will be supported to manage their own health and wellbeing so that they are in
control of what, how and where care and support is
delivered
People will have a safe and positive experience of our
services
People will have timely and easy access to responsive,
integrated care and support

Quality, Safety and Patient Experience Strategy – Nov 2015
10
We aim to continuously improve care for people within Castle Point and Rochford. There
are five strategic themes we focus on, both internally and also through our relationships with
patients and the public, providers of care, regulators and with partner commissioners.
Strategic Themes for Improving Quality of Care, Patient Safety and Patient
Experience

Quality, Safety and Patient Experience Strategy – Nov 2015
11
4. Quality, Safety and Patient Experience through
Commissioning
The diagram below shows the high level tasks involved in commissioning (buying) care, and
how we make sure that quality, safety and patient experience is protected and prioritised at
each stage.
Quality, Safety and Patient Experience at each stage of the Commissioning Cycle
4.1 Procurement
We follow NHS Procurement Policy when we buy services and ensure that quality, safety
and patient experience requirements are built into contracts to enable future robust quality
monitoring. Our on-going monitoring of quality, safety and patient experiences of
commissioned services enables us to hold providers to account for performance against
those elements of the contract.
4.2 Incentivising and Monitoring Quality with our Providers
We also utilise the national Commissioning for Quality and Innovation (CQUIN) framework to
provide financial rewards (or penalties) for the achievement (or failure to achieve) quality
goals to ensure that providers of care focus their efforts on delivering high quality and safe
services that offer a positive patient experience.
Setting Strategy
Designing Services
Review & Approval
Sourcing Providers
Mobilisation
Monitoring & Evaluation
Our organisational strategy is focussed on improving health & wellbeing, preventing illness, and maintaining independence where possible. We aim to offer care closer to home, and make sure hospital care is reserved only for those who need specialist input. We believe this will offer the best care and experiences for our community.
We are working with our providers to design services that are safe, effective and will meet the needs of our population. Quality and safety and patient experience are the main focus as we discuss new services or whether changes are needed.
All new ideas and service changes undertake a Quality Impact Assessment process that benefits and risks to quality, safety and patient experience. Clinical teams are responsible for reviewing these risks and ensuring that quality, safety and patient experience will not be compromised.
We maintain strong relationships with our provider organisations and work with them to establish regular monitoring processes to ensure that patients continue to receive safe, effective care and good experiences. This includes direct patient feedback and monitoring of outcomes.
When we set up new health and care services we need to go through legal processes to select providers. Our selection process considers the quality and safety culture of the organisations we commission to ensure that our patients will receive safe, effective care and good experiences.
For some ideas we pilot (test) the service to make sure it works in the way we planned. This means we can measure the quality safety and patient experience benefits before we commit to a long contract.

Quality, Safety and Patient Experience Strategy – Nov 2015
12
4.3 Partnership Working
We are working closely with all Clinical Commissioning Groups in Greater Essex, our Local
Authorities and especially with those commissioning services for the South Essex
population. We give and receive assurances to and from each other that there are robust
systems and processes in place for managing and monitoring the quality, safety and patient
experience of services within our contracts.
Our commitment to improving quality, safety and patient experience is upheld in decision
making for health and care service provision for all client groups, children, adults, older
people, people requiring mental health services and people with learning disabilities whether
receiving care in acute, community or primary care settings. We strive to ensure that the
high quality health care we commission is provided on the basis of our on-going commitment
to equality of experience and outcomes, to everyone in Castle Point and Rochford, no matter
who they are or where they live.
4.4 Patient and Public Involvement
Our aim is that patients, carers, community representatives, community groups and the
wider public are involved in commissioning decisions at every level. We are in the process
of building a database of people living in Castle Point and Rochford who would like to be
involved or simply kept informed of any local decisions that could result in a change to the
way local health services are provided.
4.4.1 Commissioning Reference Group
Our Commissioning Reference Group is a formal advisory body. Its purpose is to support us
in ensuring that the voice of our patients, (and their carers), and public, including seldom-
heard groups, is embedded in our business, embracing the ’no decision about me without
me’ promise, and actively promoting the principles and values of the NHS Constitution.
Members of the CRG group include patient representatives from GP practices,
representatives from our local voluntary sector organisations, GPs, representatives from
both the younger and older generations of Castle Point & Rochford, CCG staff and Health
Watch Essex. The group is chaired by a lay representative.
4.4.2 Patient Participation Groups (PPG)
We have been actively encouraging Patient Participation Groups (PPG) have developed in
recent years in GP practices. These groups are an effective way for patients and GP
surgeries to work together to improve services and to promote health and improved quality
of care. Within the Castle Point and Rochford area there are a number of member practices

Quality, Safety and Patient Experience Strategy – Nov 2015
13
that have Patient Participation Groups. Information from our Commissioning Reference
Group is fed back to our GP practices to help inform patients of our plans on a wider level.
4.4.3 Governing Body
We also have lay representatives on the Governing Body so they are part of the key decision
making processes for commissioning health and care services for our population. One lay
member is the Chair of the Quality and Governance Committee.

Quality, Safety and Patient Experience Strategy – Nov 2015
14
5 National drivers for quality, safety and patient experience
There are a range of national policy drivers that influence the quality, safety and patient
experience agenda across the NHS and support us in our ambition to offer the best possible
care.
5.1 NHS Five Year Forward View
The Five Year Forward View, published in October 2014, by NHS England, sets out a
positive vision for the future based around new models of care.
“The definition of quality in health care, enshrined in law, includes three key aspects: patient
safety, clinical effectiveness and patient experience. A high quality health service exhibits all
three. However, achieving all three ultimately happens when a caring culture, professional
commitment and strong leadership are combined to serve patients, which is why the Care
Quality Commission is inspecting against these elements of quality too.
We do not always achieve these standards. For example, there is variation depending on
when patients are treated: mortality rates are 11% higher for patients admitted on Saturdays
and 16% higher on Sundays compared to a Wednesday. And there is variation in outcomes;
for instance, up to 30% variation between CCGs in the health related quality of life for people
with more than one long term condition.
We have a double opportunity: to narrow the gap between the best and the worst, whilst
raising the bar higher for everyone. To reduce variations in where patients receive care, we
will measure and publish meaningful and comparable measurements for all major pathways
of care for every provider – including community, mental and primary care – by the end of
the next Parliament. We will continue to redesign the payment system so that there are
rewards for improvements in quality. We will invest in leadership by reviewing and refocusing
the work of the NHS Leadership Academy and NHS Improving Quality. To reduce variations
in when patients receive care, we will develop a framework for how seven day services can
be implemented affordably and sustainably, recognising that different solutions will be
needed in different localities. As national bodies we can do more by measuring what
matters, requiring comprehensive transparency of performance data and ensuring this data
increasingly informs payment mechanisms and commissioning decisions.”
(Five Year Forward View, NHS England, published in October 2014)
Quality, safety and patient experience are highlighted as integral to a high quality health care
system and we are working on a range of initiatives and models of care in line with this plan,
to reduce variation in care provision, improve service provision, and to consider how to
incentivise and reward improvements to quality, safety and patient experience.
5.2 The NHS Outcomes Framework
The NHS Outcomes Framework provides a national overview of how well the NHS is
performing and is the primary accountability mechanism for improving quality throughout the

Quality, Safety and Patient Experience Strategy – Nov 2015
15
NHS. The framework was initially developed in 2010, but is updated every year. Some
indicators are shared with the Adult Social Care Outcomes Framework and/or the Public
Health Outcomes Framework. The 2015/16 framework outlines 5 domains that form key
drivers for our local priorities for commissioning and quality. These domains directly link to
quality, safety and patient experience as shown below.
NHS Outcomes Framework 2015/16
Domain Overarching indicators Improvement Areas
1. Preventing
people from
dying
prematurely
Potential years of life
lost from causes
considered amenable
to healthcare
Life expectancy at 75
Neonatal mortality and
stillbirths
Reducing premature mortality from major causes of
death
Reducing premature mortality in people with mental
illness
Reducing mortality in children
Reducing premature death in people with a learning
disability
2. Enhancing
quality of
life for
people with
long term
conditions
Health related quality
of life for people with
long term conditions
Ensuring people feel supported to manage their
condition
Improving functional ability for people with long term
conditions
Reducing time spent in hospital for people with long
term conditions
Enhancing quality of life for carers
Enhancing quality of life for people with mental illness
Enhancing quality of life for people with dementia
Improving quality of life for people with multiple long
term conditions
3. Helping
people to
recover
from
episodes of
ill health or
following
injury
Emergency
admissions for acute
conditions that should
not normally require
hospital admission
Emergency
readmissions within 30
days of discharge from
hospital
Improving outcomes from planned treatments
Preventing lower respiratory tract infections in children
from becoming serious
Improving recovery from injuries and trauma
Improving recovery from stroke
Improving recovery from fragility fractures
Helping older people to recover their independence
after illness or injury
Improving dental health
4. Ensuring
that people
have a
positive
experience
of care
Patient experience of
primary care (including
GP services, GP out of
hours services and
NHS dental services)
Patient experience of
hospital care
Friends and family test
Patient experience
categorised as poor or
worse for primary care
and/or hospital care
Improving people’s experience of outpatient care
Improving hospitals’ responsiveness to personal needs
Improving people’s experience of accident and
emergency services
Improving access to primary care services
Improving women and their families’ experience of
maternity services
Improving experience of care for people at the end of
their lives
Improving experience of healthcare for people with
mental illness
Improving children and young people’s experience of
healthcare
Improving people’s experience of integrated care

Quality, Safety and Patient Experience Strategy – Nov 2015
16
Domain Overarching indicators Improvement Areas
5. Treating
and caring
for people
in a safe
environmen
t and
protecting
them from
avoidable
harm
Deaths attributable to
problems in healthcare
Severe harm
attributable to
problems in healthcare
Reducing the incidence of avoidable harm, (e.g. VTE
related events, incidence of healthcare associated
infection, falls and pressure ulcers)
Improving safety of maternity services
Improving the culture of safety reporting
5.3 Harm Free Care & the NHS Safety Thermometer
The NHS Outcomes Framework and policy direction requires a national focus on a small
number of key outcomes that the NHS is measuring together. The NHS Safety
Thermometer is a local improvement tool for measuring, monitoring and analysing patient
harms and ‘harm free’ care. The tool measures four high-volume patient safety issues which
are also highlighted in domain 5 of the outcomes framework:
Elimination of grade 3 and 4 pressure ulcers
Falls in care
Urinary infection (in patients with a catheter), and
Treatment for venous thromboembolism
Harm free care was incentivised as a national CQUIN in 2013/14 and 2014/15 and we
continue to monitor these indicators as part of our performance monitoring with providers.
5.4 Summary Hospital-Level Mortality Indicators (SHMI)
Summary Hospital-Level Mortality Indicators report on mortality at a trust level across the
NHS in England using a standard and transparent methodology.
SHMI is the ratio between the actual number of patients who die following hospitalisation at the trust, and the number that would be expected to die, on the basis of the national average figures, given the characteristics of the patients treated there. (Hospital and Social Care Information Centre)
SHMI covers all deaths reported of patients who were admitted to non-specialist acute trusts
in England and either die in hospital or within 30 days of being discharged from hospital.
SHMI replaces the Hospitalised Standardised Mortality Ratio (HSMR) which covered deaths
that occur in a hospital setting. A high SHMI will raise questions about whether there are
underlying problems in the quality of care that a hospital is delivering to its patients and the

Quality, Safety and Patient Experience Strategy – Nov 2015
17
care they are receiving after they are discharged. This is a standing item on our Clinical
Quality Review Group with providers and any variance is closely monitored.
5.5 Care Quality Commission (CQC) – Essential Standards
The Care Quality Commission is the independent regulator of health and adult social care in
England. The CQC ensure health and social care services provide people with safe,
effective, compassionate, high-quality care and encourage care services to improve. The
CQC does this by inspecting services and publishing the results on its website to help
patients and the public make better decision about the care they receive. Registration with
the CQC is a statutory requirement of all NHS providers, Independent Healthcare providers,
Dentists and General Practitioners. The CQC Essential Standards require providers to
declare compliance against those standards and the CQC undertakes planned and
responsive inspections to monitor compliance. CQC compliance is an agenda item at our
Clinical Quality Reference Group to ensure that non-compliance is supported by a monitored
action plan.
5.6 National Institute for Health and Care Excellence (NICE)
The National Institute for Health and Care Excellence is a Non Departmental Public Body
which develops national guidance, advice and quality standards for health and social care.
NICE’s role is to improve outcomes for people using the NHS and other public health and
care services and this work takes three forms:
I. Producing evidence based guidance and advice for health, public health, and social
care practitioners. This includes:
o NICE guidelines: Preventing and managing specific conditions, improving
health and managing medicines in different settings, interventions to improve
health in communities, provision of social care to adults and children
o Technology appraisal Guidelines (TAGs): To assess the clinical and cost
effectiveness of health technologies such as new pharmaceutical and
biopharmaceutical products, but also procedures, devices and diagnostic
agents
o Medical technologies and diagnostics guidance: To ensure that the NHS is
able to adopt clinically and cost effective technologies rapidly and consistently
o Interventional procedures guidance: Recommending whether interventional
procedures are effective and safe enough for use within the NHS
II. Developing quality standards and performance metrics for those providing and
commissioning health, public health and social care services, including:

Quality, Safety and Patient Experience Strategy – Nov 2015
18
o Quality standards: A precise set of statements with accompanying metrics,
designed to drive and measure quality improvements within a particular area
of care
o Quality Outcomes Framework (QOF): An annual menu of potential indicators
for inclusion in the quality element of our contract with General Practitioners
o Clinical Commissioning Group Outcomes Indicator Set (CCGOIS): A
framework for measuring health outcomes and the quality of care (included
patient reported outcomes and patient experience) achieved by CCGs.
III. Providing a range of informational services for commissioners, practitioners and
managers across the spectrum of health and social care. This includes:
o NICE evidence: An online search facility that identifies relevant clinical, public
health and social care guidance, including access to a range of bibliographic
databases and professional journals
o Access to the British National Formulary (BNF) and British National Formulary
for Children (BNFC), including smart phone access
o Medicines and prescribing support: Advice and information on pharmaceutical
products, their scope, licensing and practical advice on developing and
maintaining local medicines formularies
Healthcare professionals are expected to take NICE guidance fully into account when
exercising their clinical judgment. The only guidelines which are mandatory are the
Technology Appraisal Guidelines (TAGs), however we ensure that NICE guidance is
considered in our commissioning decisions and implementation is monitored in
commissioned services.
5.7 Quality, Innovation, Productivity & Prevention (QIPP)
QIPP is a large transformational programme to support clinical teams and organisations to
improve the quality of caring, through productivity, prevention and innovation, to improve the
quality of care whilst delivering efficiency savings that can be reinvested into the NHS. QIPP
represents a broad, policy agenda rather than a single, definable policy, however there are a
number of national work streams within QIPP designed to support the NHS to improve care
and lower costs. These range from improving commissioning, (or purchasing), of care for
patients with long-term conditions, to improving how organisations are run, staffed and
supplied. The specific changes required to meet the agenda have been left to local
providers and commissioners to identify and implement. We are working with our local
health partners to develop integrated QIPP plans that address our local quality challenges
and make efficiency improvements. It is essential that the impact of productivity savings on
the quality of care delivered is monitored closely and the CCG has developed a Quality

Quality, Safety and Patient Experience Strategy – Nov 2015
19
Impact Assessment tool and process to review all QIPP plans and identify quality impacts
whether they are positive or negative and ensure risks are understood and mitigated
appropriately.
5.8 National Reporting and Learning System (NRLS)
Patient safety incident reporting is a vital mechanism for identifying downward trends in the
quality of care, identifying failure and facilitating learning. The National Reporting and
Learning System (NRLS) is a central database of patient safety incident reports. Since April
2010, it has been mandatory for NHS trusts in England to report all serious patient safety
incidents and the NRLS has now moved under the National Commissioning Board. Six
monthly reports are then produced that benchmark providers in terms of types of incident
and levels of harm. Since the NRLS was set up in 2003, over four million incident reports
have been submitted and information is analysed to identify hazards, risks and opportunities
to continuously improve the safety of patient care.
5.9 National Reports and Investigations
The Department of Health and health related organisations publish reports following
enquiries, inquiries, reviews and evaluations of health care provision. We review the
recommendations from these reports and assess the implications to the CCG and its
commissioned services and ensure that any recommendations and lessons learnt
implemented and embedded into local processes.
Two key reports that we are monitoring progress against are:
Transforming Care: A national response to Winterbourne View Hospital, published in
December 2012. Although two years have passed since the report was published,
the recommendations included in the report contain long term commitments to
strengthening accountability and corporate responsibility for the quality of care and
improving quality and safety, so we continue to monitor the work streams that were
established in response to this report.
The Francis Report: Outlining the Public Inquiry into the failure in NHS care at Mid
Staffordshire hospital, chaired by Sir Robert Francis QC, which was published in
2013. This report identifies warning signs that were evident at Mid Staffs hospital,
and should have alerted the wider system to the problems that led to such a
catastrophic failure in care. The key recommendations that are relevant directly to
commissioners fall into 5 themes:
1. Setting and monitoring standards
2. Learning and improvement
3. Data quality and information

Quality, Safety and Patient Experience Strategy – Nov 2015
20
4. Organisational culture
5. Patient experience
Patients First and Foremost: An initial overarching response on behalf of the health
and care system as a whole to the Mid Staffordshire NHS Public Enquiry and the
Francis Report. It details key actions to ensure that patients are the “first and
foremost” consideration of the system, and everyone who works in it. It calls for the
NHS to return to its core humanitarian values, setting out a commitment and a plan to
eradicate harm and promote excellence.
The Berwick Report: Released in August 2013, the Berwick report was a review
commissioned by the Prime Minister and carried out by Professor Don Berwick and
international expert in patient safety. The review contains ten recommendations with
the aim of making the NHS a system devoted to continual learning and
improvements in patient care, top to bottom, beginning to end. Among the
recommendations were adopting a culture of learning, ensuring adequate staffing
levels and creating a new criminal offence for recklessness.
We will continue to monitor any other high profile cases which provide on-going reminders of
the role in safeguarding the care of vulnerable people, both for adults and children.
5.10 “No Harms Event”
Across South East Essex a quarterly meeting takes place where all providers can meet to
discuss events where things have gone wrong or very right to ensure that the system can
learn and develop as a result. NHS England as well as all CCG’s are in attendance.
5.11 Co-Commissioning
We are the only CCG in Essex to have been granted fully delegated co-commissioning
responsibility for primary care. Co-commissioning offers an opportunity to raise standards of
quality within general practice services including:
Clinical effectiveness
Patient experience
Patient safety
This includes work on reducing unwarranted variation in quality and enhancing patient and
public involvement in developing services. We aim to support our member practices.
5.12 Safeguarding adults and children
Safeguarding means protecting people's health, wellbeing and human rights, and enabling
them to live free from harm, abuse and neglect. It's fundamental to high-quality health and
social care.

Quality, Safety and Patient Experience Strategy – Nov 2015
21
Safeguarding children and promoting their welfare includes:
Protecting them from maltreatment or things that are bad for their health or
development
Making sure they grow up in circumstances that allow safe and effective care.
Safeguarding adults includes:
Protecting their rights to live in safety, free from abuse and neglect.
People and organisations working together to prevent the risk of abuse or neglect,
and to stop them from happening.
Making sure people's wellbeing is promoted, taking their views, wishes, feelings and
beliefs into account.
5.13 Parity of Esteem
NHS England has established a Parity of Esteem programme as part of a “call to action” in
order to focus effort and resources on improving clinical services and health outcomes for
mental health. The emphasis is on ensuring that mental health is valued equally with
physical health. The commissioning cycle offers the ideal framework to achieve this.

Quality, Safety and Patient Experience Strategy – Nov 2015
22
6 Roles and Responsibilities for Quality Assurance
We have in place a range of groups, teams and individuals with responsibility for assuring
and providing information on quality, safety and patient experience to ensure that
interventions pursued are clearly and appropriately integrated, aligned and managed.
6.1 The Role of the Clinical Commissioning Group
The Health and social Care Act 2012 sets out the role of CCGs in regard to securing
continuous improvement in quality, safety, effectiveness and patient experience:
“Each clinical commissioning group must exercise its functions with a view to securing
continuous improvement in the quality of services provided to individuals for or in connection
with the prevention, diagnosis or treatment of illness.
In discharging its duty a clinical commissioning group must, in particular, act with a view to
securing continuous improvement in the outcomes that are achieved from the provision of
the services.
The outcomes include, in particular, outcomes which show –
(a) The effectiveness of the services,
(b) The safety of the services, and
(c) The quality of the experience undergone by patients”
(Health & Social Care Act 2012 c7 – Part 1, Section 26, 14R)
Our role in commissioning includes holding providers to account for delivery of their
contractual obligations and quality standards. We must build the right quality standards into
the contracts we place with providers, to ensure service delivery improves and that the
providers we partner with have in place systems and processes to drive continual
improvement.
6.1.1 Our Role as Co-Commissioners
The NHS Five Year Forward View set out provision for CCGs to assume greater power and
influence over the commissioning of primary care medical care. Castle Point and Rochford
CCG is one of a small number of CCGs in the country to be delegated full responsibility for
commissioning general practice services. Delegated commissioning responsibilities exclude
individual GP performance management, which NHS England retains, however the design of
GP contracts, enhanced services, local incentive schemes and decisions on discretionary
payments does now reside with the CCG.
This gives opportunities to fully embed quality, safety and patient experience into primary
care specifications as well as with our community, mental health and acute providers.
Quality, Safety and Patient Experience Strategy – Nov 2015
23
6.2 Group and Team Responsibilities for Quality, Safety & Patient
Experience
6.2.1 The Governing Body
The CCG Governing Body is chaired by a practicing GP, and is made up of our Accountable
Officer, the Chief Nurse, Executive Directors of the CCG, GP representatives and lay
members. The function of the Governing Body is to ensure strong and effective leadership,
management and accountability. Members of the Governing body must be assured that the
systems and processes are in place to monitor quality in commissioned services.
6.2.2 The Quality and Governance Committee
An integral component of our infrastructure for quality is the Quality and Governance
Committee, a formal sub-committee of our Governing Body. This Committee has the role of
assuring the Governing Body of the quality and safety of all health interventions that we
commission. The Committee is the formal mechanism by which the CCG discharges its
responsibilities for clinical quality and sets the strategic direction for clinical governance.
The remit of the committee is to;
Provide oversight and give assurance to the Governing Body that the patient and
patient feedback is kept at the centre of all decision making
Assure the quality and safety of the services commissioned
To promote continuous improvement, learning and innovation with respect to, clinical
effectiveness, safety of services and patient experience
6.2.3 The Clinical Quality Review Group (CQRG)
We commission major provider contracts collaboratively with three other CCGs. Each major
provider contract for which we lead is reviewed on a monthly basis through a Clinical Quality
Review Group (CQRG) which is chaired by the CCG Chief Nurse and attended by members
of the commissioning team, contracts team and representation for the quality and safety
agenda for the organisation. The CQRG is part of the formal contract management process
and the group has a set agenda built on the requirements for quality, safety and patient
experience in the contract and any new national drivers and the minutes of the Group go the
CCG Quality Committee.
6.2.4 The Quality Support Team
We have invested in a Quality Support Team to build the necessary capacity and capability
in monitoring quality, implementing and monitoring improvement projects, and supporting our

Quality, Safety and Patient Experience Strategy – Nov 2015
24
staff to ensure that quality, safety and patient experience are prioritised in our
commissioning and day to day business.
The Quality Support Team provides support, analysis of data and information to the CCG
Chief Nurse on all aspects of patient safety and quality, including infection control, CQUIN,
serious incidents and never events and safeguarding.
The Quality Support Team review Quality Impact Assessments for new projects to provide
challenge and feedback on mitigating actions being proposed.
6.2.5 The Role of Member Practices
We are a membership organisation, which means clinical leaders, elected to our Governing
Body by member practices agree the basic rules that make up our constitution. Member
practices are expected to become fully engaged in our work around quality improvement,
and each practice is responsible for the development of its own quality improvement plan
within the context of the primary care.
We support member practices and wider primary care to quality assure current standards,
however each practice is remains accountable for the quality of services within their own
organisation. Member practices receive monthly reports benchmarking their performance on
key quality, performance and financial measures, and practices are expected to take action
to demonstrate continuous improvement. We routinely survey and monitor patient
experiences of using member practices.
Practice patient participation groups are essential in capturing patient experiences to feed
into the early warning processes and quality review meetings with providers.
6.2.6 Quality Surveillance Groups (QSGs)
QSGs bring together commissioners, regulators and other parts of the system to share
information and intelligence on quality in order to spot the early signs of problems and to
take corrective and supportive action to prevent early problems becoming more serious
quality failures. They are supported and facilitated by the NHS England are operational in
each local area and region. The meeting is attended by the Chief Nurse and Accountable
Officer and representatives from a range of organisations including the Care Quality
Commission, Monitor, Local Authority, HealthWatch and the East of England Deanery.
6.2.7 The Commissioning Support Unit (CSU)
The North East London Commissioning Support Unit provides expert support and advice to
help clinical commissioners to deliver improved health services to local populations. The
CSU role in promoting quality assurance and improvement for us is to:

Quality, Safety and Patient Experience Strategy – Nov 2015
25
Ensure that there is a clear information on provider performance that all parties
understand
Provide support and advice on service redesign and QIPP initiatives
Support the annual and on-going contract negotiations
Coordinate contract monitoring and support the challenge on over performance,
targets, CQUINS, quality standards, QIPP, KPIs and demand management
Implementation of Super CQUIN
6.3 Individual Roles and Responsibilities
In addition to the above groups there are some individual roles within the CCG that have
responsibility for quality, safety and patient experience assurance and monitoring.
6.3.1 The Accountable Officer
The Accountable Officer (AO) holds ultimate responsibility for ensuring that the CCG is
meeting its statutory requirements for quality and safety and that there are mechanisms in
place for the CCG to recognise where there are concerns or failures in commissioned
services or in the CCGs ability to monitor the quality and safety of services. The AO reports
directly to the Governing Body.
6.3.2 The Chief Nurse
The Chief Nurse has responsibility for giving assurance to the CCG in relation to the quality
and safety of services being delivered to the local population. The Chief Nurse oversees the
processes and systems to ensure all national and local requirements to maintain and
improve quality, safety and patient experience and will be expected to report to the
Governing Body any concerns.
The Chief Nurse has responsibility for signing off all Quality Impact Assessments for new
projects, and is the Caldicott Guardian for the CCG.
6.3.3 All CCG Staff
All staff in the CCG regardless of their function will have a role to play in supporting us to
commission high quality services. This includes ensuring that their safeguarding, equality
and diversity and information governance training is up to date so they are in a position to
recognise any concerns or early warnings that they may come across as part of their day to
day business.

Quality, Safety and Patient Experience Strategy – Nov 2015
26
7. Quality, Safety and Patient Experience Assurance
Processes
We have internal quality assurance and early warning systems in place which provide
information about risks to quality, safety and patient experience of the services we
commission. A formal Quality Impact Assessment process is used to identify quality, safety
and patient experience impacts and risks associated with any new services that are
considered and/or established. This allows us to be proactive in identifying concerns early,
and take action where standards fall short, and to ensure that new projects prioritise and
protect quality, safety and patient experience.
Quality Reporting is a regular agenda item for our Governing Body, and a formal written
quality report is presented by the Chief Nurse. The Quality report provides an overview to
the Governing Body of the continued focus that we place on quality and safety of services for
our population. The Quality Report includes dashboards with month by month snapshots of
the performance monitoring for providers, information on any serious incidents that have
taken place, safeguarding issues, complaints summaries, patient experience data, National
Reporting and Learning System (NRLS) incidents and any CQC reviews/inspection updates
and key findings that have been received.
We ensure that risks are managed in line with the aims, objectives and governance
arrangements outlined in this Quality Strategy and through:
Systematic programme of implementation of our Corporate Risk Management
Strategy
Reporting, investigation, management and learning from incidents
Risk management
Identification, reporting and management of risks
Development of risk registers and monitoring of action plans to mitigate risks
Quality and Safety risks are grouped on the risk register to make more explicit to the
Governing Body the nature and scale of risks that exist in direct relation to the quality of care
we commission. The CCG will therefore clearly see any quality risks that threaten our ability
to achieve its objectives.7
7.1 Monitoring and Assurance for Commissioned Services
We monitor each major provider contract monthly at the Clinical Quality Review Group
(CQRG) described above. Commissioners also work with commissioned services to deliver

Quality, Safety and Patient Experience Strategy – Nov 2015
27
their annual ‘Quality Accounts’ to give assurance to the public and provide commentary on
the organisations commitment to governance, quality, safety and positive patient experience.
As part of contract monitoring, we also undertake a series of announced and unannounced
visits and the CCG Executive Nurses have developed a visit template to ensure consistency
of monitoring. The outcomes of these visits are discussed at the CQRGs and are reported to
the Quality and Governance committee.
7.1.1 Using data to assess and improve quality, safety and patient experience
We require performance data from all the providers we commission, and monitor this for
trends, themes and compliance with national requirements including:
Acute hospitals
Care homes
Community providers
Mental health providers
Independent hospitals
NHS 111 service
Ambulance services
Domiciliary care agencies
Support and assisted living services
We also use soft intelligence, regular and unannounced site visits and face to face dialogue
with our providers to triangulate information to inform Key Lines of Enquiry (KLOE) for
discussion at our formal meetings as part of our contract management. Any emerging or
immediate areas of concern are escalated immediately.
7.1.2 Complaints and patient feedback
We actively encourage feedback, and respect the views of patients using our commissioned
services. We are keen to learn from patient experiences, good or bad and to put in place
steps to ensure continuous improvements. The hospital providers have in place Patient
Advice Liaison teams (PALS) who are available to all the community to advise and support
patients, carers and families by providing information, and who capture learning and ideas.
7.2 Quality Monitoring for New Projects and Services
We are an innovative and ambitious CCG, with plans to develop new services and make
improvements. With all new ideas we expect that quality, safety and patient experience will
be prioritised and protected to ensure that standards remain high and risks are understood,
mitigated and managed.

Quality, Safety and Patient Experience Strategy – Nov 2015
28
We have established a robust Quality Impact Assessment process and associated tool to
assess whether quality, safety or patient experience will be impacted on by any
organisational change project. Our project management approach is shown below, QIAs are
initiated in gateway 2 and reviewed at gateways 3 and 4.
Castle Point & Rochford Project Management Approach
7.2.1 QIA Tool and Process
The QIA tool incorporates a checklist to determine what level of impact may be expected
against 47 indicators – either positive, no impact or negative impact. A full risk assessment
is undertaken against any criteria that have potential to impact negatively on quality, safety
and patient experience. The indicators are shown below:
QIA Checklist Indicators
Category Quality Indicators
Patient safety Patient safety adverse events including avoidable harm and Patient Safety Alert
Services
Medicines management and safe administration of medicines
Mortality, HSMR / SHMI
Ay infection control issues including MRSA / Cdiff
CQC visits and registration
NHSLA / CNST
Essential training

Quality, Safety and Patient Experience Strategy – Nov 2015
29
Workforce, vacancies, turnover, absence, revalidation
Safe, clean, comfortable and well maintained environment/equipment
Clinical
effectiveness
NICE guidance and Quality Standards e.g. VTE, Stroke, Dementia
Helping people recover from ill health, injury and preventing people from dying
prematurely
Other outcome guidance e.g. PROMS
Other external accreditation e.g. RCN
National clinical audit / research and development
Clinical outcomes
Breastfeeding rates
Emergency bed days
Length of stay
Emergency readmissions (30 day)
Minor injuries standards
Day case rates
Patient
experience
Patient feedback (e.g. FFT, NHS Choices, comments, compliments, concerns,
complaints, national and local surveys)
Patients, carers and public engagement
Waits for admission / treatment
Mixed sex breaches
Delayed discharge
End of life pathway
Cancelled day case operations
Waiting times for therapy services
Making every contact count
Inequalities of
care
Access to services – equality impact
Variation in care provision
Staff experience Workforce capability care and skills
Working practice
Staff satisfaction (e.g. FFT, annual staff survey / local surveys)
Mandatory training compliance
Targets &
performance
Performance
Achievement of local, regional and national targets
Promoting
wellbeing (in the
provision of care
and support)
Person’s sense of personal dignity (including treatment of the individual with respect)
Person’s physical and mental health and wellbeing
Abuse and neglect (safeguarding)
Personal control over day to day life (including over care and support and the way it is
provided)
Opportunities for participation in work, education, training or recreation
Social and economic wellbeing
Domestic, family and personal relationships
Suitability of living accommodation
Personal contribution to society including sustainability
Risk assessment is undertaken to outline:
Description of the risk or negative impact
Risk rating – including likelihood and impact according to the corporate risk register
rating

Quality, Safety and Patient Experience Strategy – Nov 2015
30
Mitigating actions and controls
Residual risk rating
Escalation and risk tracking
Metrics used to track and monitor the risk
Monitoring forum and risk owner
Risks associated with QIAs are captured in project risk logs and departmental risk logs and
are therefore subject to the corporate risk management processes. However risks identified
through the QIA process are also managed and report by the Programme Management
Office (PMO) to ensure they are tracked appropriately as projects progress through the
gateway process.
7.3 Other Quality, Safety and Patient Experience Mechanisms
7.3.1 Safeguarding adults and children
We have a clear governance process in place for safeguarding children and vulnerable
adults. The CCG works in partnership with the local Authority and the Chief Nurse is a
member of the Children and Adult Safeguarding Boards. The designate professionals for
safeguarding children and adults are within the hosted arrangements for the South Essex
CCGs and the Quality Support Team work closely with the safeguarding teams in the Local
Authority. The structure below shows the inter-dependencies across health and social care
for the management of safeguarding children and vulnerable adults. Our Chief Nurse is a
member of the Children and Adults Safeguarding Board.

Quality, Safety and Patient Experience Strategy – Nov 2015
31
Safeguarding Structure within South Essex
7.3.2 Information Governance and Caldicott
We ensure robust Information Governance arrangements through the implementation of the
requirements of the Department of Health’s Information Governance toolkit. The CCG
Senior Information Risk Owner (SIRO) is the Chief Finance Officer and the Caldicott
Guardian is the Chief Nurse. Information Governance support is through the Essex team
hosted by Basildon and Brentwood CCG..
7.3.3 Clinical Audit
Audit is an essential tool for early recognition of failing systems and processes before it
results in an incident that may cause harm. We monitor the robustness of clinical audit in
commissioned services and are actively involved in auditing patient notes through
information sharing agreements.
7.3.4 Medicines Management
The Prescribing and Medicines Management Team provides expert knowledge to help make
the best decisions around buying and prescribing high quality, cost-effective and safe drugs
and medicines. The service also ensures that the appropriate and necessary governance
around medicines use, are in place and that all legal obligations are met. This key service
helps CCGs to improve safety and quality of care around prescribing and administration of
medicines, and to manage the NHS drugs bill.

Quality, Safety and Patient Experience Strategy – Nov 2015
32
7.3.5 Domestic Abuse
We are hosting an Essex-wide programme team focussed on improving outcomes for
victims of domestic abuse and their children, reducing severe harm, and supporting victims
to feel safer in their own homes. In addition a range of initiatives are being established to
work with perpetrators to improve access to support programmes. The programme is a joint
initiative, working across a range of organisations, Essex-wide; including Essex Police,
Essex County Council, Local Housing Authorities, registered housing providers and the NHS
and is expected to reduce police call outs, health costs associated with the physical and
mental effects on victims and alternative accommodation costs for victims and perpetrators
in addition to the quality and safety benefits.
Quality, Safety and Patient Experience Strategy – Nov 2015
33
8. Next Steps and Developments
To achieve our quality ambitions we will require complete ownership within the organisation
of quality improvement on behalf of our patients. Every member of staff needs to understand
what needs to change, why it needs to change and how to make change happen. Quality is
everyone’s business and this strategy outlines the part to play of all. This process will be
informed by all aspects of the commissioning cycle, relationships with our providers and our
relationship with our local residents.
Quality is everyone’s business and everyone has a part to play.
On-going evaluation of our performance year on year against our strategic quality objectives
will be mandatory and will be led by the Quality and Governance Committee.
The CCG will continue to review National and local standards to underpin the Quality
agenda and this strategy will become the underpinning document to support the agenda.

Quality, Safety and Patient Experience Strategy – Nov 2015
34
NHS Castle Point and Rochford
Clinical Commissioning Group
12 Castle Road
Rayleigh
Essex SS6 7QF
Tel: 01268 464508
Email: [email protected]
Twitter: @CPRCCG
www.castlepointandrochfordccg.nhs.uk