quantitative effects of functional bundle branch block in patients with atrioventricular reentrant...
TRANSCRIPT

Quantitative Effects of Functional BundleBranch Block in Patients With
Atrioventricular Reentrant TachycardiaYanfei Yang, MD, Jie Cheng, MD, PhD, Kathy Glatter, MD, Parvin Dorostkar, MD,
Gunnard W. Modin, PhD, and Melvin M. Scheinman, MD
Changes in the retrograde conduction time (ventricu-loatrial [VA]) interval during functional bundle branchblock (BBB) have been used to separate septal from freewall accessory pathways (APs), but different values ofthe VA interval prolongation (DVA) have been describedin different reports. A total of 95 patients with singlenondecremental APs who developed BBB during atrio-ventricular reentrant tachycardia were studied. Freewall APs were found in 60 patients, and 35 had septalAPs. For patients with free wall APs, complete and in-complete BBB ipsilateral to the atrial insertion site of APswere observed in 39 of 60 patients (65%) and 31 of 60patients (52%), respectively. For patients who had bothcomplete (QRS >120 ms) and incomplete (QRS <120ms) BBB during atrioventricular reentrant tachycardia,DVA for patients with complete BBB was significantlygreater than in those with incomplete BBB, 59 6 19 msversus 30 6 11 ms, p <0.001. For patients with septalAPs and complete and incomplete BBB during tachycar-
dia, the mean DVA for those with complete BBB was31 6 20 ms and was significantly longer than in patientswith incomplete BBB (14 6 6 ms), p <0.001. There wasno significant difference in DVA between those with freewall APs and incomplete BBB compared with those withseptal APs and complete BBB. The criteria of QRS >120ms associated with DVA >40 ms served to best separatefree wall from septal APs with a sensitivity of 88% anda specificity of 89%. Left anterior fascicular block wasassociated with marked lengthening of DVA for thosewith left free wall APs, whereas a left posterior fascicularblock pattern resulted in a marked increase in the DVAfor patients with posteroseptal APs. In the absence offascicular block patterns, a DVA >40 ms providesstrong evidence of a free wall AP, with a sensitivity of95% and a specificity of 100%. The left posterior fascicleappears to provide predominant innervation of the pos-terior septum. Q2000 by Excerpta Medica, Inc.
(Am J Cardiol 2000;85:826–831)
Precise accessory pathway (AP) localization is crit-ical for successful ablation of APs. The observa-
tion of bundle branch block (BBB) during ortho-dromic atrioventricular reentrant tachycardia (AVRT)has been shown to be helpful for distinguishing APsites.1–5 In prior studies, differences in retrograde con-duction time (ventriculoatrial [DVA]) as a criteria forseparating free wall from septal pathways were found.The ablation procedure allows for relatively precisedetermination of the AP insertion site and was used asour gold standard. The purpose of our study wastwofold: (1) to assess the degree to which quantitativechanges in functional bundle branch conduction timeaffectedDVA in patients with free wall APs, and (2)to determine whetherDVA for those with septal APshelped determine the successful atrial ablation site.
METHODSPatient selection: We retrospectively studied 229
consecutive patients with AVRT due to a single APwho underwent electrophysiologic study and radiofre-
quency ablation between February 1993 and July1998, and 112 patients were found to have either leftBBB or right BBB pattern during AVRT. Seventeenpatients with decremental pathways were excluded.Thus, a total of 95 patients (55 men and 40 women,aged 336 17 years; range 4 to 73) were included inthe study. Forty-two patients had left free wall, 18patients right free wall, 23 posteroseptal, 7 anterosep-tal, and 5 patients with midseptal pathways.
Electrophysiologic studies: The details of our inva-sive studies have previously been reported.6 Func-tional BBB was induced by either (1) atrial extra-stimuli induced from either the high right atrium orcoronary sinus, (2) ventricular extrastimuli from theright ventricular apex, (3) initiation of burst pacingduring sinus rhythm, or (4) initiation of burst pacingduring orthodromic AVRT. The first 3 pacing proto-cols were used for all studies, whereas burst pacingduring AVRT was used only in selected patients asclinically indicated.
Bundle branch reentry was at times induced byprogrammed ventricular stimulation during tachycar-dia. In our study 2 patients with bundle branch reentrywere incorporated into the left BBB group.7,8
After completion of mapping, ablation was di-rected at the atrial insertion sites of right and left freewall pathways. Left free wall pathways were ap-proached using a transseptal approach. Septal APswere always initially approached from the right atrium
From the Cardiovascular Research Institute and Section of CardiacElectrophysiology, University of California San Francisco, San Fran-cisco, California; and New York Health Sciences Center, Syracuse,New York. Manuscript received September 13, 1999; revised manu-script received November 1, 1999, and accepted November 2.
Address for reprints: Melvin M. Scheinman, MD, Cardiac Electro-physiology, University of California San Francisco, 500 ParnassusAvenue, MU East 4S, Box 1354, San Francisco, California 94143-1354. E-Mail: [email protected].
826 ©2000 by Excerpta Medica, Inc. All rights reserved. 0002-9149/00/$–see front matterThe American Journal of Cardiology Vol. 85 April 1, 2000 PII S0002-9149(99)00875-9
and, if unsuccessful, patients then underwent transsep-tal catheterization of the left atrium.
Definitions of terms: The location of APs was de-fined as reported by Fitzpatrick et al.9
The BBB contour was defined by the morphologicchanges according to accepted electrocardiographiccriteria.10 Complete and incomplete BBB was definedby the QRS interval$120 ms and,120 ms, respec-tively. Left anterior fascicular block during tachycar-dia was defined as sudden left-axis deviation of#230°, and left posterior fascicular block (LPFB) wasdefined as sudden right-axis deviation of$190°.11
Measurements: The QRS duration was always mea-sured from the simultaneously recorded 12-lead elec-trocardiogram (Cardiolab System by Prucka Engineer-ing Inc., Houston, Texas). The VA interval duringorthodromic AVRT was measured from the earliestbeginning of the QRS complex in the 12-lead surfaceelectrocardiogram to the onset of local atrial activa-tion.2,4,5,7,12
In all, 20 patients underwent blinded measurementof both the QRS and VA intervals. The SD of eithermeasurement was6 1 ms (range 0 to 4).13,14
Statistical analysis: All data are expressed asmean 6 SD. For patients who had incomplete orcomplete BBB only, a 2-way analysis of variance wasused to analyze QRS duration andDVA. For patientswho had incomplete and complete BBB, a repeated-measures analysis of variance with a grouping factorwas used to analyze QRS duration andDVA. Cate-gorical data were analyzed with a Fisher’s exact test.A p value, 0.05 was considered statistically signif-icant.
RESULTSFree wall APs and complete BBB: Functional com-
plete BBB ipsilateral to the site of the AP was ob-served in 39 of 60 patients (65%), of whom 24 had leftand 15 right free wall pathways. The results are listedin Table I. Two patients with right free wall AP hadDVA intervals ,40 ms. In the first patient, the base-line QRS complex during sinus rhythm and duringtachycardia showed an incomplete right BBB pattern.Thus, it was not unexpected that with the developmentof complete right BBB, theDVA was ,40 ms (37
ms). The second patient with a con-cealed right free wall AP had a dom-inant R wave in V1 associated with ashort HV interval (25 to 30 ms) dur-ing both sinus rhythm and duringorthodromic AVRT. During AVRTand complete right BBB, theDVAincreased by only 22 ms. After abla-tion of the right free wall pathway,the HV interval remained short andthe QRS was unchanged despiteoverdrive pacing or programmedpremature atrial stimulation. We in-terpreted this finding as reflective ofa left His-fascicular tract,15 whichwas not involved in the tachycardiacircuit. If we exclude the latter 2
patients, then all patients with complete ipsilateralBBB patterns and free wall pathways hadDVA $40ms. Hence, interpretation of theDVA during AVRTwith functional BBB ipsilateral to the site of thepathway must be interpreted in terms of QRS durationas well as the baseline QRS configuration.
Free wall APs and incomplete BBB: In patients witha free wall AP, incomplete BBB was observed duringAVRT in 31 of 60 (52%) (Table I). This analysisincluded 1 patient with incomplete left BBB and leftanterior fascicular block associated with a left lateralAP whoseDVA interval was 55 ms. A QRS durationonly slightly ,120 ms could be associated withDVA,40 ms (Figure 1).
Septal APs: POSTEROSEPTAL APs:In all 15 patientswith posteroseptal APs, functional complete left BBBwas associated with aDVA ,40 ms, except 4 patients(as shown in the right upper quadrant of Figure 1).Three of these 4 patients with complete left BBB hadan associated LPFB pattern and had marked changesin DVA (63, 91, and 97 ms, respectively; Figure 2).For 20 patients with posteroseptal APs, induction ofcomplete right BBB during AVRT failed to prolongthe VA interval, except for 2 patients who developeda right BBB and associated posterior hemiblock pat-tern and showed aDVA of 15 and 31 ms, respectively(Figure 3). These data suggest significant innervationof the posterior septal space by branches of the leftposterior fascicle. Incomplete left BBB was observedin 9 patients with posteroseptal APs and was associ-ated withDVA #25 ms (Table I).
ANTEROSEPTAL APs:In the 7 patients with antero-septal APs, complete and incomplete right BBB, re-spectively, occurred in 6 patients during AVRT (TableI). In patients with anteroseptal APs, prolongation ofthe VA interval of ,40 ms was observed with thedevelopment of right BBB in all but 2 patients. In 1 ofthese patients, complete right BBB during AVRT re-sulted in aDVA of 41 ms (Figure 4). The stronganterior forces observed for this patient suggested thepresence of associated right midseptal block. Anotherpatient with anteroseptal AP actually had a decrease inDVA during tachycardia associated with a left BBBpattern. This observation has been reported previous-ly.16,17
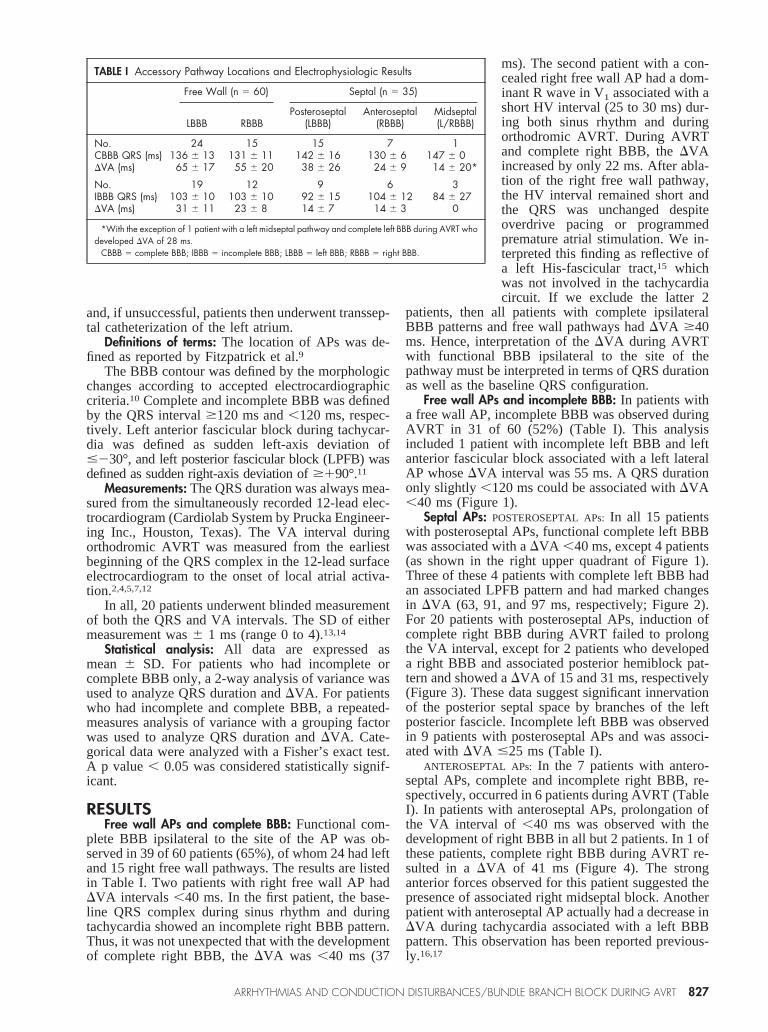
TABLE I Accessory Pathway Locations and Electrophysiologic Results
Free Wall (n 5 60) Septal (n 5 35)
LBBB RBBBPosteroseptal
(LBBB)Anteroseptal
(RBBB)Midseptal(L/RBBB)
No. 24 15 15 7 1CBBB QRS (ms) 136 6 13 131 6 11 142 6 16 130 6 6 147 6 0DVA (ms) 65 6 17 55 6 20 38 6 26 24 6 9 14 6 20*
No. 19 12 9 6 3IBBB QRS (ms) 103 6 10 103 6 10 92 6 15 104 6 12 84 6 27DVA (ms) 31 6 11 23 6 8 14 6 7 14 6 3 0
*With the exception of 1 patient with a left midseptal pathway and complete left BBB during AVRT whodeveloped DVA of 28 ms.
CBBB 5 complete BBB; IBBB 5 incomplete BBB; LBBB 5 left BBB; RBBB 5 right BBB.
ARRHYTHMIAS AND CONDUCTION DISTURBANCES/BUNDLE BRANCH BLOCK DURING AVRT 827
MIDSEPTAL APs: Either right (3 patients) or left (3patients) BBB was observed in 5 patients with mid-septal APs. Four of these patients with a right mid-septal pathway had no significant change inDVAduring AVRT with development of either BBB pat-tern. However, 1 patient with a left midseptal pathwayhad an increase inDVA of 28 ms with development ofcomplete left BBB. To our knowledge, this is the firstreport of the effects of left BBB onDVA for a patientwith a left midseptal pathway.
Comparison of patients with both complete and in-complete BBB: The change in VA interval duringtachycardia associated with both normal, incomplete,and complete BBB could be assessed (in the samepatient) for 35 patients. For these patients with freewall pathways (left, 13; right, 9), there was a statisti-cally significant increase in the meanDVA for thosewith complete BBB (596 19 ms) compared withthose with incomplete BBB (306 11 ms; p,0.001).The same comparison could be performed in 13 pa-tients with septal AP who had periods of incompleteand complete BBB. In these patients (anteroseptal APwith right BBB [n 5 5]; posteroseptal AP with leftBBB, n 5 8), theDVA (31 6 20 ms) for completeBBB was significantly greater than it was for incom-plete BBB (146 6 ms; p,0.001).
For patients with complete and incomplete BBB
during AVRT, we analyzed whetherDVA could bepredicted fromDQRS by use of linear regressionanalysis. There was a statistically significant linearincrease in change inDVA for those with free wallAPs (p,0.0001, r5 0.80) comparing incomplete andcomplete BBB, but no significant linear correlationwas found in those with septal APs (r5 0.07). Asimilar result was found (p,0.002, r5 0.65 for freewall pathways; p,0.4, r5 0.25 for septal pathways)when we compared the changes in VA interval andQRS duration from normal QRS to complete BBB.
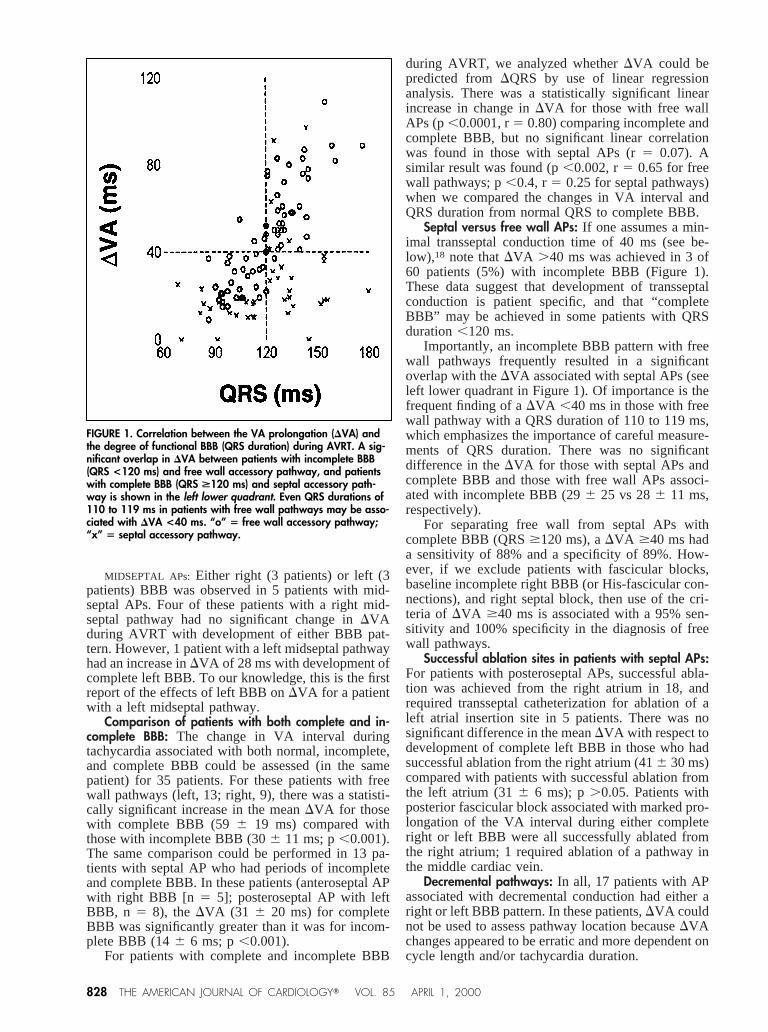
Septal versus free wall APs: If one assumes a min-imal transseptal conduction time of 40 ms (see be-low),18 note thatDVA .40 ms was achieved in 3 of60 patients (5%) with incomplete BBB (Figure 1).These data suggest that development of transseptalconduction is patient specific, and that “completeBBB” may be achieved in some patients with QRSduration,120 ms.
Importantly, an incomplete BBB pattern with freewall pathways frequently resulted in a significantoverlap with theDVA associated with septal APs (seeleft lower quadrant in Figure 1). Of importance is thefrequent finding of aDVA ,40 ms in those with freewall pathway with a QRS duration of 110 to 119 ms,which emphasizes the importance of careful measure-ments of QRS duration. There was no significantdifference in theDVA for those with septal APs andcomplete BBB and those with free wall APs associ-ated with incomplete BBB (296 25 vs 286 11 ms,respectively).
For separating free wall from septal APs withcomplete BBB (QRS$120 ms), aDVA $40 ms hada sensitivity of 88% and a specificity of 89%. How-ever, if we exclude patients with fascicular blocks,baseline incomplete right BBB (or His-fascicular con-nections), and right septal block, then use of the cri-teria of DVA $40 ms is associated with a 95% sen-sitivity and 100% specificity in the diagnosis of freewall pathways.
Successful ablation sites in patients with septal APs:For patients with posteroseptal APs, successful abla-tion was achieved from the right atrium in 18, andrequired transseptal catheterization for ablation of aleft atrial insertion site in 5 patients. There was nosignificant difference in the meanDVA with respect todevelopment of complete left BBB in those who hadsuccessful ablation from the right atrium (416 30 ms)compared with patients with successful ablation fromthe left atrium (316 6 ms); p.0.05. Patients withposterior fascicular block associated with marked pro-longation of the VA interval during either completeright or left BBB were all successfully ablated fromthe right atrium; 1 required ablation of a pathway inthe middle cardiac vein.
Decremental pathways: In all, 17 patients with APassociated with decremental conduction had either aright or left BBB pattern. In these patients,DVA couldnot be used to assess pathway location becauseDVAchanges appeared to be erratic and more dependent oncycle length and/or tachycardia duration.
FIGURE 1. Correlation between the VA prolongation (DVA) andthe degree of functional BBB (QRS duration) during AVRT. A sig-nificant overlap in DVA between patients with incomplete BBB(QRS <120 ms) and free wall accessory pathway, and patientswith complete BBB (QRS >120 ms) and septal accessory path-way is shown in the left lower quadrant. Even QRS durations of110 to 119 ms in patients with free wall pathways may be asso-ciated with DVA <40 ms. “o” 5 free wall accessory pathway;“x” 5 septal accessory pathway.
828 THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 85 APRIL 1, 2000
DISCUSSIONFree wall APs: Our findings confirmed the observa-
tion of some previous studies, but several caveats bearemphasis. First, a typical pattern of either right or leftBBB during AVRT associated with a QRS duration,120 ms may fail to reach or exceed 40 ms in patientswith free wall pathways. This finding may explain thedifference inDVA as a criteria for separating free wallpathways from septal pathways among previous stud-ies, because those studies usually used a limited num-ber of surface leads and did not specifically detail
QRS duration.2–5,7 In our study, all patients with evi-dence of complete BBB associated with QRS duration$120 ms hadDVA $40 ms when BBB was ipsilateralto the site of the AP, except for those 2 exceptionswith right free wall pathways. In contrast, severalpatients (3 of 60, 5%) with incomplete BBB had aDVA $40 ms, with a QRS duration in the range of104 to 119 ms. If we excluded patients with leftanterior fascicular block, we found that a QRS dura-tion as short as 113 ms could be associated withDVA$40 ms. If we assume that the minimal transseptal
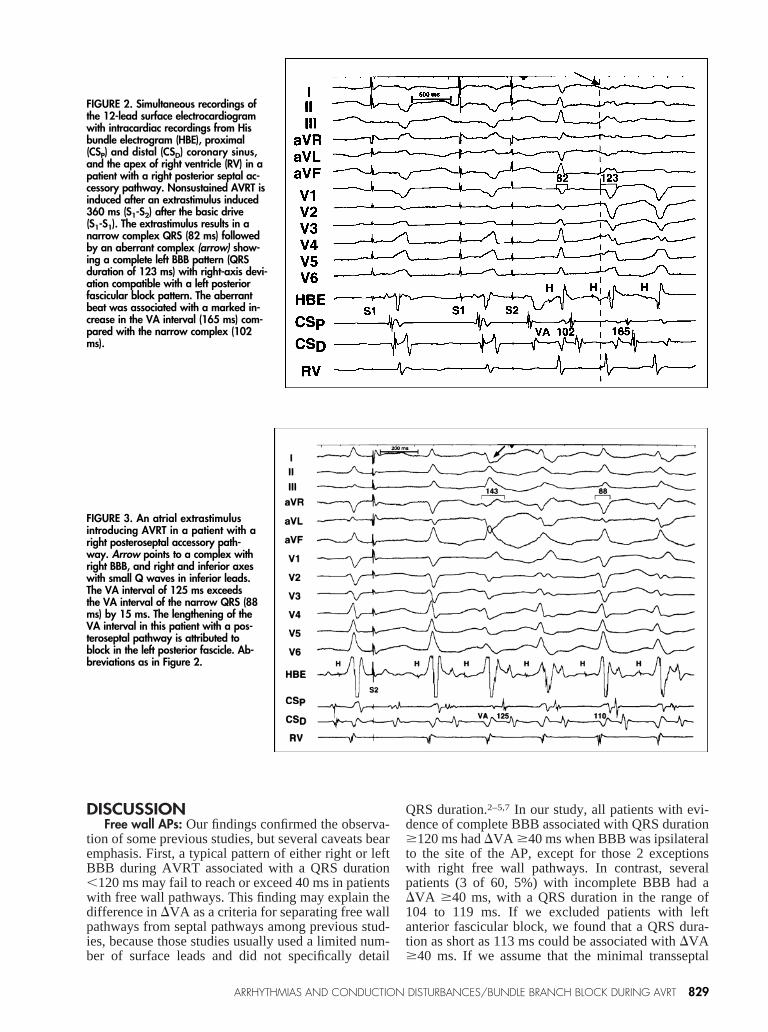
FIGURE 3. An atrial extrastimulusintroducing AVRT in a patient with aright posteroseptal accessory path-way. Arrow points to a complex withright BBB, and right and inferior axeswith small Q waves in inferior leads.The VA interval of 125 ms exceedsthe VA interval of the narrow QRS (88ms) by 15 ms. The lengthening of theVA interval in this patient with a pos-teroseptal pathway is attributed toblock in the left posterior fascicle. Ab-breviations as in Figure 2.
FIGURE 2. Simultaneous recordings ofthe 12-lead surface electrocardiogramwith intracardiac recordings from Hisbundle electrogram (HBE), proximal(CSP) and distal (CSD) coronary sinus,and the apex of right ventricle (RV) in apatient with a right posterior septal ac-cessory pathway. Nonsustained AVRT isinduced after an extrastimulus induced360 ms (S1-S2) after the basic drive(S1-S1). The extrastimulus results in anarrow complex QRS (82 ms) followedby an aberrant complex (arrow) show-ing a complete left BBB pattern (QRSduration of 123 ms) with right-axis devi-ation compatible with a left posteriorfascicular block pattern. The aberrantbeat was associated with a marked in-crease in the VA interval (165 ms) com-pared with the narrow complex (102ms).
ARRHYTHMIAS AND CONDUCTION DISTURBANCES/BUNDLE BRANCH BLOCK DURING AVRT 829
conduction time is approximately 40 ms,18 our datawould suggest that the QRS duration denoting trans-septal conduction is patient specific.
Septal APs: We found that theDVA during AVRTin 35 patients with septal AP and complete BBBexceeded 40 ms in 5 patients. A ready explanation waspossible in 3 patients with posteroseptal APs who,during AVRT or bundle branch reentry, had a com-plete left BBB associated with an LPFB pattern. An-other patient with a posteroseptal AP had aDVA of 45ms, with development of a complete left BBB duringtachycardia. In addition, 2 patients with a posterosep-tal AP associated with complete right BBB and LPFBpatterns during tachycardia had aDVA of 15 and 31ms, respectively. These data suggest that in patientswith posteroseptal APs, important innervation of theposteroseptal space is provided by the left posteriorfascicles. Importantly, successful ablation of the path-way was achieved from the right side in all patientswith LPFB and posteroseptal pathways.
Comparison with previous studies: Kerr et al3 foundthat the cutoffDVA associated with BBB ipsilateral tothe site of the free wall pathway was$35 ms, whereasthose with septal pathways had aDVA of #25 ms.However, 3 patients with intermediate values wereexcluded. More recently, Jazayeri et al7 found thatpatients with left free wall AP had aDVA .45 ms,whereas those with posteroseptal AP hadDVA inter-vals, 25 ms. In another study from the same group,it was shown that a pattern of left anterior fascicularblock alone or with left BBB resulted in pronouncedchanges in theDVA interval in patients with AVRTsupported by a left lateral AP. In contrast, patientswith AVRT using a posteroseptal AP had no change inthe VA conduction time with an LPFB pattern.11 Thedifference between these findings and our own obser-vations is not apparent.
Study limitations: Our study suffers from the stan-dard problem relating to retrospective studies. Tech-niques used for eliciting tachycardia induction from
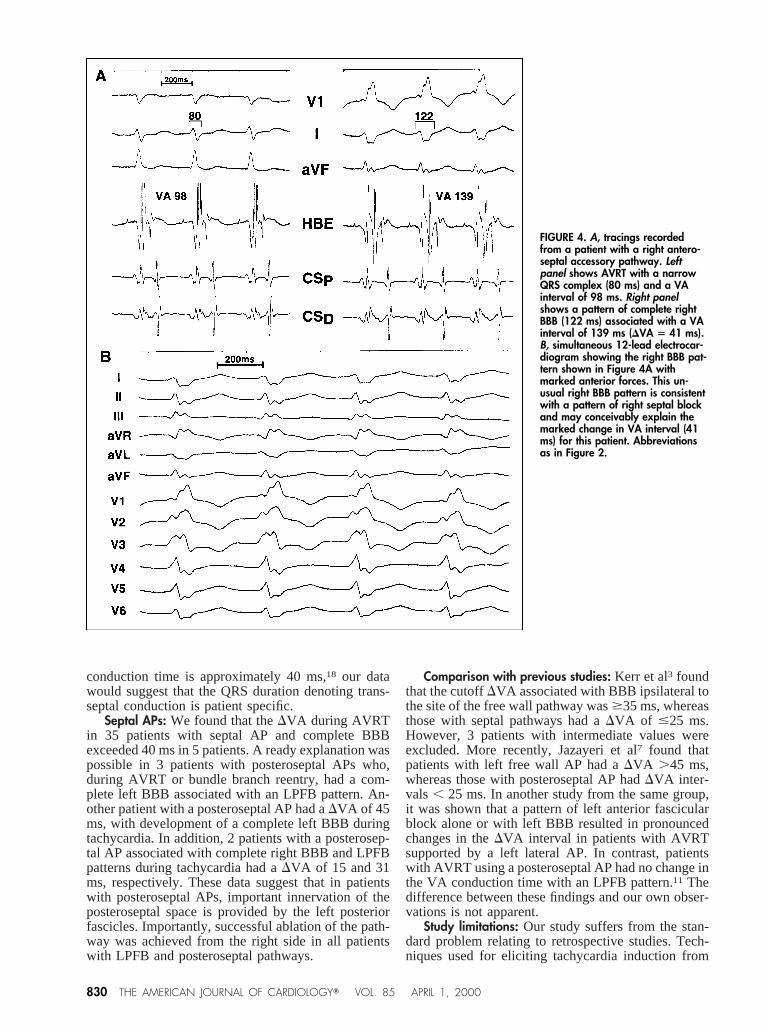
FIGURE 4. A, tracings recordedfrom a patient with a right antero-septal accessory pathway. Leftpanel shows AVRT with a narrowQRS complex (80 ms) and a VAinterval of 98 ms. Right panelshows a pattern of complete rightBBB (122 ms) associated with a VAinterval of 139 ms (DVA 5 41 ms).B, simultaneous 12-lead electrocar-diogram showing the right BBB pat-tern shown in Figure 4A withmarked anterior forces. This un-usual right BBB pattern is consistentwith a pattern of right septal blockand may conceivably explain themarked change in VA interval (41ms) for this patient. Abbreviationsas in Figure 2.
830 THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 85 APRIL 1, 2000

both the atrium and ventricle were used and frequentlyresulted in induction of BBB, but patients did not haveidentical pacing protocols. In addition, because APmay course obliquely (i.e., from the septum to the freewall), the atrial insertion site may not correspond tothe ventricular insertion site, and lead to an erroneousdiagnosis of a septal pathway.
Clinical implications: Despite the retrospective na-ture of the study, the following points bear emphasis.Our data would suggest that minimizing overlap be-tween septal and free wall APs depends on (1) care-fully measuring QRS duration by using all 12 leads ofthe surface electrocardiogram, (2) achieving aDVA$40 ms associated with QRS duration.120 ms, and(3) excluding the presence of associated fascicularblock.
1. Coumel P, Attuel P. Reciprocating tachycardia in overt and latent preexcita-tion: influence of functional bundle branch block on the rate of the tachycardia.Eur J Cardiol 1974;:423–436.2. Pritchett ELC, Tonkin AM, Dugan FA, Wallace AG, Gallagher JJ. Ventriculo-atrial conduction time during reciprocating tachycardia with intermittent bundle-branch block in Wolff-Parkinson-White syndrome.Br Heart J1976;38:1058–64.3. Kerr CR, Gallagher JJ, German LD. Changes in ventriculoatrial intervals withbundle branch block aberration during reciprocating tachycardia in patients withaccessory atrioventricular pathways.Circulation 1982;66:196–201.4. Weiss J, Brugada P, Roy D, Bar FWHM, Wellens HJJ. Localization of theaccessory pathways in the Wolff-Parkinson-White syndrome from the ventriculo-atrial conduction time of right ventricular apical extrasystoles.PACE 1983;6:260–267.5. Lehmann MH, Denker S, Mahmud R, Tchou P, Dongas J, Akhtar M. Elec-trophysiologic mechanisms of functional bundle branch block at onset of inducedorthodromic tachycardia in the Wolff-Parkinson-White syndrome.J Clin Invest1985;76:1566–1574.
6. Scheinman MM, Wang YS, Van Hare GF, Lesh MD. Electrocardiographic andelectrophysiologic characteristics of anterior, midseptal and right anterior freewall accessory pathways.J Am Coll Cardiol1992;20:1220–1229.7. Jazayeri MR, Tchou P, Caceres J, McKinnie J, Avitall B, Gilbert C, Werner P,Akhtar M. Ventriculoatrial conduction time during bundle branch reentrant beatinitiating orthodromic tachycardia: a simple and reliable method for localizationof accessory pathways.J Cardiovasc Electrophysiol1990;1:121–131.8. Gonzalez-Zuelgaray J, Sheikh S, Akhtar M, Jazayeri MR. Functional bundlebranch block as a delayed manifestation of retrograde concealment in the His-Purkinje system.J Cardiovasc Electrophysiol1996;7:248–258.9. Fitzpatrick AP, Gonzales RP, Lesh MD, Modin GW, Lee RJ, Scheinman MM.New algorithm for the localization of accessory atrioventricular connectionsusing a baseline electrocardiogram.J Am Coll Cardiol1994;23:107–116.10. Willems JL, Robles de Medina EO, Bernard R, Coumel P, Fisch C, KriklerD, Mazur NA, Meijler FL, Mogensen L, Moret P, et al. Criteria for intraventric-ular conduction disturbances and pre-excitation.J Am Coll Cardiol1985;5:1261–1275.11. Jazayeri MR, Caceres J, Tchou P, Mahmud R, Denker S, Akhtar M. Elec-trophysiologic characteristics of sudden QRS axis deviation during orthodromictachycardia.J Clin Invest1989;83:952–959.12. Benditt DG, Pritchett ELC, Smith WM, Gallagher JJ. Ventriculoatrial inter-vals: Diagnostic use in paroxysmal supraventricular tachycardia.Ann Intern Med1979;91:161–166.13. Cronbach LJ, Gleser GC, Nanda H, Rajaratnam N. The Dependability ofBehavioral Measurements: Theory of Generalizability for Scores and Profiles.New York: Wiley, 1972.14. Dixon WJ. BMDP statistical software manual. Berkeley, CA: University ofCalifornia Press, 1988.15. Sallee D III, Van Hare GF. Preexcitation secondary to fasciculoventricularpathways in children: a report of three cases.J Cardiovasc Electrophysiol1999;10:36–42.16. Baerman JM, Bauernfeind RA, Swiryn S. Shortening of ventriculoatrialintervals with left bundle branch block during orthodromic reciprocating tachy-cardia in three patients with a right-sided accessory atrioventricular pathway.J Am Coll Cardiol1989;13:215–219.17. Wellens HJJ, Durrer D. The role of an accessory atrioventricular pathway inreciprocal tachycardia: observations in patients with and without the Wolff-Parkinson-White syndrome.Circulation 1975;52:58–72.18. Venerose RS, Seidenstein M, Stuckey JH, Hoffman BF. Activation ofsubendocardial Purkinje fibers and muscle fibers of the left septal surface beforeand after left bundle branch block.Am Heart J1962;63:346–361.
ARRHYTHMIAS AND CONDUCTION DISTURBANCES/BUNDLE BRANCH BLOCK DURING AVRT 831