questions evidence for efficacy of can training change motor
TRANSCRIPT

Effects of training 28/5/19
Paul Hodges CCRE SPINE UQ 2019 1
Evidence for efficacy of interventions:
Can we change motor control? Does it help if we do?
Paul Hodges
Questions
• Can training change motor behaviour in people with pain?
• Can training change motor system reorganisation?
• Can training change pain?
Outcomes of treatment• Improved structure & behaviour of deep trunk
muscles (Hides et al. 2001; Tsao et al. 2008)
• Reduced activity of superficial trunk muscles (Tsao, Druit & Hodges, 2010)
• Improved proprioception(Falla, Jull & Hodges, 2007)
• Improved spine posture(Falla, Jull & Hodges, 2007)
• Improved movement (Scholtes et al, 2010)
Weeks1 2 3 40
25
30
20
10
5
0
Cro
ss-s
ectio
nal a
rea
Exercise groupControl group
15
LSD = 3.92% (p<0.05)
Restoration of cross-sectional area - multifidus
Hides et al 1997 Spine
Marker of motor adaptation⇒ Changes in control of deep
musclesTrA
OI
OE
RA
ES
0 100-100
*
Time (ms)
Hodges & Richardson, 1996 Spine
OnsetTrA
Onsetdeltoid
TrA
OI
OE
RA
ES
Deltoid
50 ms TrAOIOE
RA
Specific Training
0
0.2
0.4
0.6
0.8
0
0.4
0.8
1.2
Onset Deltoid-100 100
Flexion
Extension
Nor
mal
ized
to p
re-tr
aini
ng p
eak
1.6
PostPre
Time (ms)
**
*
*
TrA

Effects of training 28/5/19
Paul Hodges CCRE SPINE UQ 2019 2
Can training change motor system reorganisation?
Pre
PreWalking exercise
00.2 0.4 0.6 0.8 1.0
Post
Post
Pro
p. P
eak
Skilled training
Can the organisation of the motor cortex be changed with exercise?
Tsao, Galea, Hodges (2010) Eur J Pain 14:832-9
Can training change pain? Systematic reviews• Saragiotto BT, Maher CG, Yamato TP, Costa LO,
Costa LC, Ostelo RW, Macedo LG. Motor Control Exercise for Nonspecific Low Back Pain. Spine. 41(16):1284-1295, 2016 .
• Ferreira PH, Ferreira ML, Maher CG, Herbert RD, and Refshauge K. Specific stabilisation exercise for spinal and pelvic pain: a systematic review. Aust J Physiother 52: 79-88, 2006.
• Macedo LG, Maher CG, Latimer J, and McAuleyJH. Motor control exercise for persistent, nonspecific low back pain: a systematic review. Phys Ther 89: 9-25, 2009.
Effect of treatment
Acute unilateral LBP ↓ LBP recurrence
Hides et al, 2001
Spondylolisthesis pain & disability
O’Sullivan et al 1997
Pregnancy-related pelvic pain
↓ pain & disabilityStuge et al 2003
Effect of treatmentMore effective for specific LBP phenotypes
Acute unilateral LBP
↓ LBP recurrence
Hides et al, 2001
Spondylolisthesis
pain & disability
O’Sullivan et al 1997
Pregnancy-related
pelvic pain
↓ pain & disability
Stuge et al 2003
Chronic non-specific LBP
↓ pain & disability & better
early vs. graded exercise
Ferreira et al, 2007
Chronic non-specific LBP
no additional benefit
Koumantakis et al, 2005
Chronic non-specific LBP
no additional benefit
Cairns et al, 2006
Effects of training 28/5/19
Paul Hodges CCRE SPINE UQ 2019 3
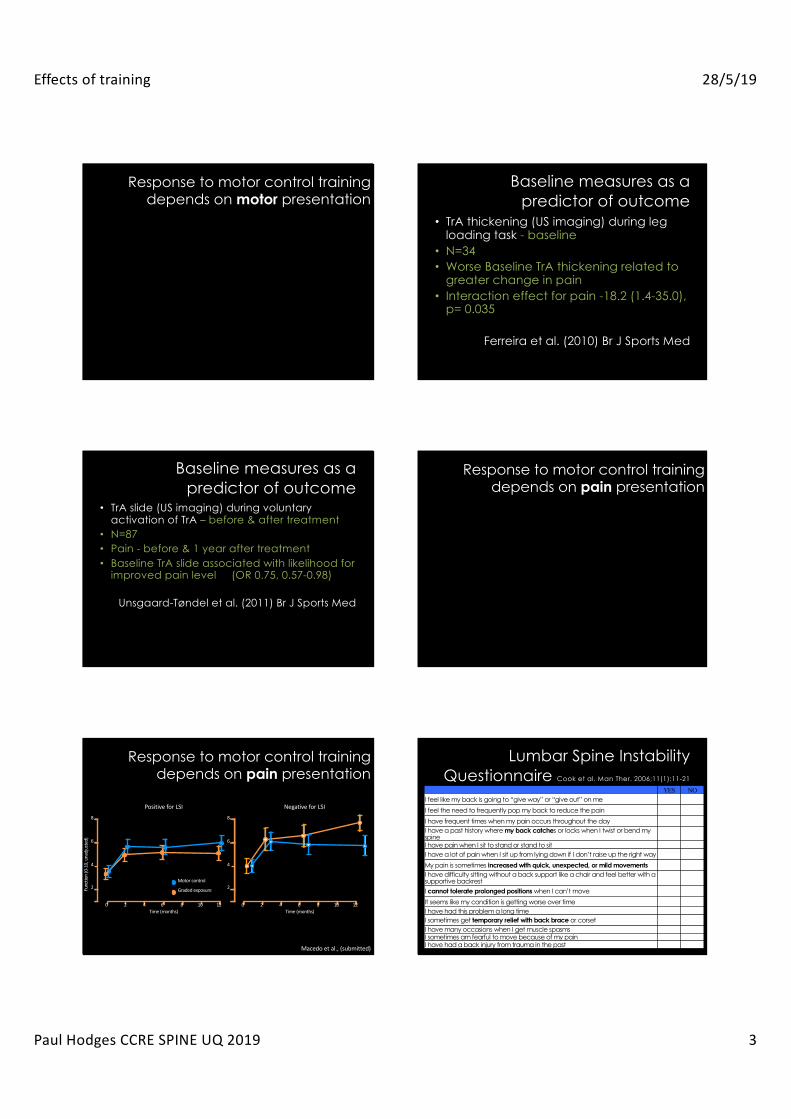
Response to motor control training depends on motor presentation
Baseline measures as a predictor of outcome
• TrA thickening (US imaging) during leg loading task - baseline
• N=34• Worse Baseline TrA thickening related to
greater change in pain• Interaction effect for pain -18.2 (1.4-35.0),
p= 0.035
Ferreira et al. (2010) Br J Sports Med
Baseline measures as a predictor of outcome
• TrA slide (US imaging) during voluntary activation of TrA – before & after treatment
• N=87• Pain - before & 1 year after treatment• Baseline TrA slide associated with likelihood for
improved pain level (OR 0.75, 0.57-0.98)
Unsgaard-Tøndel et al. (2011) Br J Sports Med
Response to motor control training depends on pain presentation
Response to motor control training depends on pain presentation
Time (months)0 2 4 8 10 12
2
4
6
8
6Time (months)
0 2 4 8 10 12
Func
tion
(0-1
0, u
nadj
uste
d)
2
4
6
8
6
Motor control
Graded exposure
Negative for LSIPositive for LSI
Macedo et al., (submitted)
Lumbar Spine Instability Questionnaire Cook et al. Man Ther. 2006;11(1):11-21
YES NOI feel like my back is going to “give way” or “give out” on me
I feel the need to frequently pop my back to reduce the pain
I have frequent times when my pain occurs throughout the dayI have a past history where my back catches or locks when I twist or bend my spineI have pain when I sit to stand or stand to sit I have a lot of pain when I sit up from lying down if I don’t raise up the right way
My pain is sometimes increased with quick, unexpected, or mild movementsI have difficulty sitting without a back support like a chair and feel better with a supportive backrestI cannot tolerate prolonged positions when I can’t move
It seems like my condition is getting worse over timeI have had this problem a long timeI sometimes get temporary relief with back brace or corsetI have many occasions when I get muscle spasmsI sometimes am fearful to move because of my painI have had a back injury from trauma in the past

Effects of training 28/5/19
Paul Hodges CCRE SPINE UQ 2019 4
Lumbar Spine Instability Questionnaire
• A measure of nociceptive pain?
Subgrouping: Evidence
0
5
10
15
20
25
30
35
Baseline 3 mo nth 12 m ont h
Oswestry Disability Index Q
M T-Ex
CB -CFT
0
2
4
6
8
Baseline 3 mo nth 12 m ont h
Pain intensity in last week
M T-Ex
CB -CFT
Vibe Fersum et al. 2013 Eur Spine J
• Subgroup – Non-specific chronic LBP (>3 months) – Provoked with postures, movement and activities
• Intervention– Classification-based cognitive functional therapy (n=62) or
manual therapy & exercise group (n=59)
* ** *
Who benefits from motor control training
• Motor control training is effective for specific subgroups (better for those with nociceptivefeatures with deficits in motor control), and when individualised to the patient
• Requires consideration of multiple domains to guide treatment– STEP 1: Is the patient appropriate for motor
control training (pain type)– STEP 2: What features of motor control require
modification
How can we make clinical decisions to guide optimal care
• Right treatment to right patient at righttime
• Hybrid method of treatment targeting
Pain mechanism based classification
• Identify mechanism of pain to guide treatment allocation
Pain neurobiology
• Not all pain is the same– Nociceptive/movement-related
• Assumed to be predominantly driven by activation of peripheral nociceptive fibres Scholz & Woolf, 2002
– Central/central sensitization• Amplification of neural signaling within the central
nervous system that elicits pain hypersensitivity – from cellular to widespread network Woolf 2011
– Neuropathic• Pain attributable to a lesion or dysfunction in the
peripheral or central nervous system Woolf, 2004
Effects of training 28/5/19
Paul Hodges CCRE SPINE UQ 2019 5
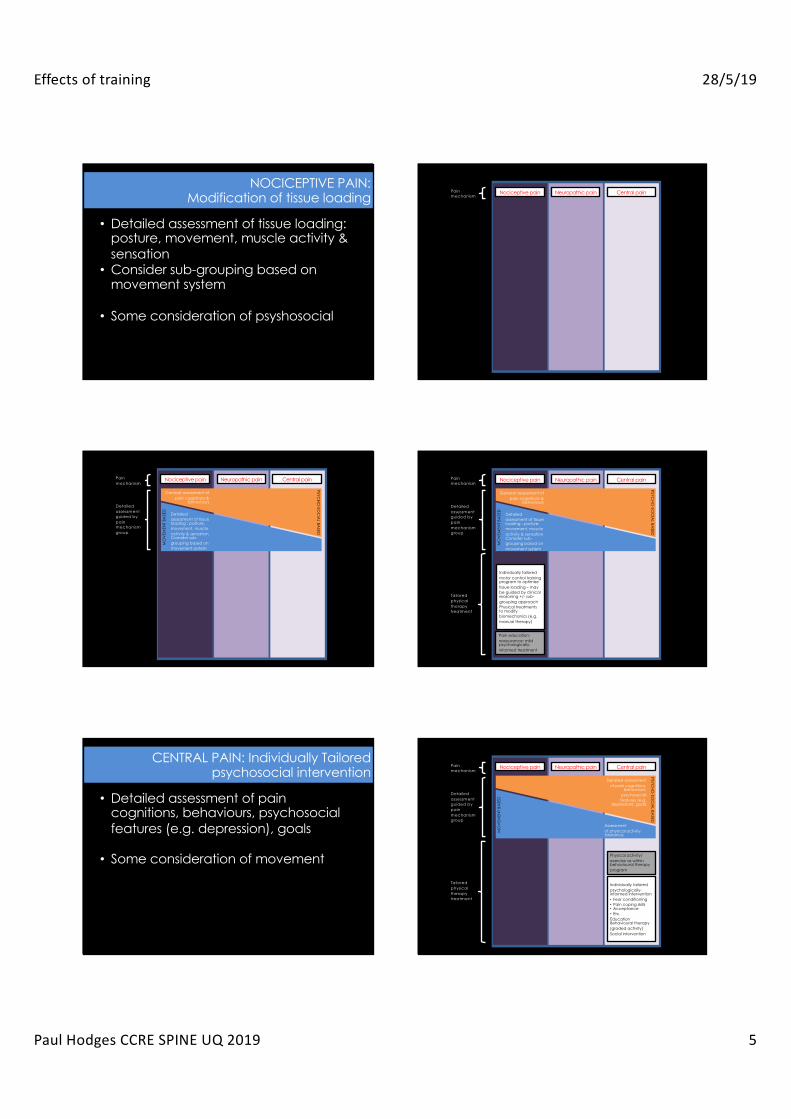
NOCICEPTIVE PAIN:Modification of tissue loading
• Detailed assessment of tissue loading: posture, movement, muscle activity & sensation
• Consider sub-grouping based on movement system
• Some consideration of psyshosocial
Nociceptive pain Central painNeuropathic painPain mechanism
Nociceptive pain Central painNeuropathic painPain mechanism
Detailed assessment guided by pain mechanism group
Detailed assessment of tissue loading : posture, movement, muscle activity & sensationConsider sub-grouping based on movement system
General assessment of pain cognitions &
behaviours
MO
VEM
ENT
BASE
D
PSYCHO
-SOC
IAL BA
SED
Nociceptive pain Central painNeuropathic painPain mechanism
Detailed assessment guided by pain mechanism group
Tailored physical therapy treatment
Individually tailored motor control training program to optimize tissue loading – may be guided by clinical reasoning +/- sub-grouping approachPhysical treatments to modify biomechanics (e.g. manual therapy)
Detailed assessment of tissue loading : posture, movement, muscle activity & sensationConsider sub-grouping based on movement system
General assessment of pain cognitions &
behaviours
Pain education; reassurance; mild psychologically-informed treatment
MO
VEM
ENT
BASE
D
PSYCH
O-SO
CIA
L BASED
CENTRAL PAIN: Individually Tailored psychosocial intervention
• Detailed assessment of pain cognitions, behaviours, psychosocial features (e.g. depression), goals
• Some consideration of movement
Nociceptive pain Central painNeuropathic pain
Individually tailored psychologically-informed intervention• Fear conditioning• Pain coping skills• Acceptance• Etc.EducationBehavioural therapy (graded activity)Social intervention
Pain mechanism
Detailed assessment guided by pain mechanism group
Tailored physical therapy treatment
Assessment of physical activity tolerance
Detailed assessment of pain cognitions,
behaviours, psychosocial features (e.g.
depression), goals
Physical activity/ exercise as within behavioural therapy program
MO
VEM
ENT
BASE
D
PSYCH
O-SO
CIA
L BASED
Effects of training 28/5/19
Paul Hodges CCRE SPINE UQ 2019 6
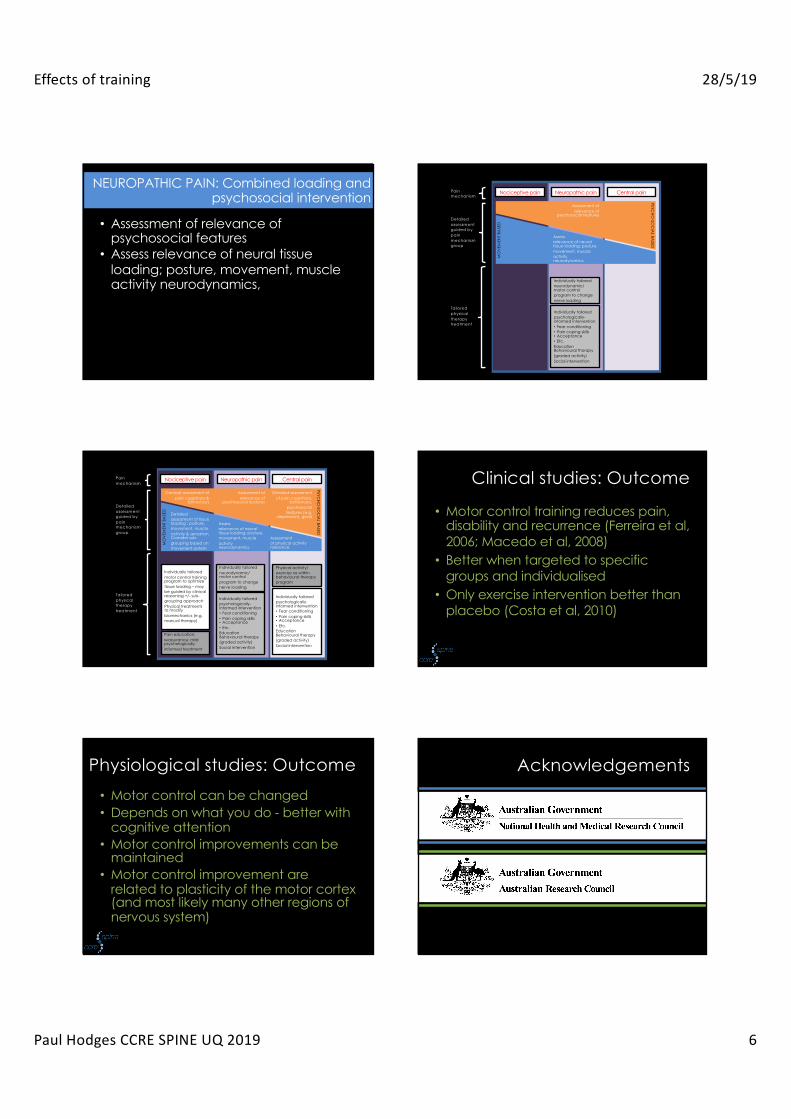
NEUROPATHIC PAIN: Combined loading and psychosocial intervention
• Assessment of relevance of psychosocial features
• Assess relevance of neural tissue loading; posture, movement, muscle activity neurodynamics,
Nociceptive pain Central painNeuropathic pain
Individually tailored neurodynamic/ motor control program to change nerve loading
Pain mechanism
Detailed assessment guided by pain mechanism group
Tailored physical therapy treatment
Assess relevance of neural tissue loading; posture, movement, muscle activityneurodynamics,
Assessment of relevance of
psychosocial features
Individually tailored psychologically-informed intervention• Fear conditioning• Pain coping skills• Acceptance• Etc.EducationBehavioural therapy (graded activity)Social intervention
MO
VEM
ENT
BASE
D
PSYCH
O-SO
CIA
L BASED
Nociceptive pain Central painNeuropathic pain
Individually tailored neurodynamic/ motor control program to change nerve loading
Individually tailored psychologically-informed intervention• Fear conditioning• Pain coping skills• Acceptance• Etc.EducationBehavioural therapy (graded activity)Social intervention
Pain mechanism
Detailed assessment guided by pain mechanism group
Tailored physical therapy treatment
Individually tailored motor control training program to optimize tissue loading – may be guided by clinical reasoning +/- sub-grouping approachPhysical treatments to modify biomechanics (e.g. manual therapy)
Detailed assessment of tissue loading : posture, movement, muscle activity & sensationConsider sub-grouping based on movement system
Assessment of physical activity tolerance
Assess relevance of neural tissue loading; posture, movement, muscle activityneurodynamics,
General assessment of pain cognitions &
behaviours
Detailed assessment of pain cognitions,
behaviours, psychosocial features (e.g.
depression), goals
Assessment of relevance of
psychosocial features
Physical activity/ exercise as within behavioural therapy program
Individually tailored psychologically-informed intervention• Fear conditioning• Pain coping skills• Acceptance• Etc.EducationBehavioural therapy (graded activity)Social intervention
Pain education; reassurance; mild psychologically-informed treatment
MO
VEM
ENT
BASE
D
PSYCHO
-SOC
IAL BA
SED
Clinical studies: Outcome
• Motor control training reduces pain, disability and recurrence (Ferreira et al, 2006; Macedo et al, 2008)
• Better when targeted to specific groups and individualised
• Only exercise intervention better than placebo (Costa et al, 2010)
Physiological studies: Outcome• Motor control can be changed• Depends on what you do - better with
cognitive attention • Motor control improvements can be
maintained• Motor control improvement are
related to plasticity of the motor cortex (and most likely many other regions of nervous system)
Acknowledgements
Effects of training 28/5/19
Paul Hodges CCRE SPINE UQ 2019 7
A/Prof'Thomas'Graven1Nielsen,'Centre'for'Sensorimotor'Interac;on,'Aalborg,'Denmark'
'Prof'Alf'Thorstensson,'Karolinska'Ins;tutet,'
Stockholm,'Sweden''
A/Prof'Jacek'Cholewicki,'Yale'University,'New'Haven,'CT,'USA'
Dr'Mary'Massery''Chicago'USA'
Dr'Paul'Cordo,'Dr'Fay'Horak,'Oregon'Health'Sciences'University,'Portland,'OR,'USA''
''
Prof'Victor'Gurfinkel,'Russian'Ins;tute'of'Informa;on'Transmission'Problems,'Moscow,'Russia''
'
Prof'Sten'Holm'&'Dr'Allison'Kaigle,'Sahlgrenska'University'Hospital,'Göteborg,'Sweden'
''
Dr'Anne'Mannion,'Schultes'Klinik,'Zurich'Switzerland''Prof'Jaap'van'Dieen,'Vrije'University,'Amsterdam,'
Netherlands''
Dr'Paulo'Ferreira,'Dr'Manuela'Ferreira,'Universidade'Federal'de'Minas'Gerais,'Belo'HorizonteBrazil'
'
Prof.'Shinn1Zong'Lin,'Tzu'Chi'University,'Taiwan'''
Prof'Lieven'Dannees,'Gent'University,'Belgium''
'''
Prof'Simon'Brumagne'&'Prof'Sabine'Verschueren,'University'of'Leuven,'Belgium'
''
A/Prof'Francois'Hug,'Nantes'University,'France'''
Prof'Jayne'Garland,'Uni.'Bri;sh'Columbia''Prof'Laurent'Bouyer,'Uni'Laval,'Quebec,'Canada''Dr'Janine'Gray,'University'of'Cape'Town,'South'Africa'
Prof'Simon'Gandevia,'Dr'Jane'Butler,'NeuRA,'Sydney''Prof'Chris'Maher,'Prof'Chris'LiYle,'Sydney'University'Dr'Siobhan'Schabrun,'Prof'Lucy'Chipchase,'Uni'Western'Sydney'Prof'Lorimer'Moseley,'Uni'South'Australia'Prof'Michele'Sterling,'Griffith'Uni,'Gold'Coast''
Program'Grant'Team'Prof'Bill'Vicenzino''Prof'Kim'Bennell'Prof'David'Hunter''
Post1docs ' ''Dr'Natalie'Collins'Dr'Welber'Marinovic'Dr'Sauro'Salomoni ''Dr'Ryan'Stafford ' ''Dr'Ruth'Sapsford' ''A/Prof'Francois'Hug'Dr'Rachel'Park''
Research'staff'Wolbert'van'den'Hoorn'Markus'Kiel'Greg'James'Mandy'Nielsen'Glenn'Russell''''
Doctoral'students'(Past)''Andrew'Briggs'Angela'Chang''Andrew'Chapman'Andrew'Claus'Sallie'Cowan''Anna'Dawson''Janine'Gray'Allison'Greig''Leanne'Hall'Nick'Karayannis''Jo'Knox'Linda1Joy'Lee'David'Macdonald'Rebecca'Mellor''Nicola'Mok''Lorimer'Moseley'Rachel'Park''Peter'Poortvliet''Ruth'Sapsford'Ryan'Stafford'Steven'Saunders''Annina'Schmid'Michelle'Smith'Natalie'Spearing'Ryan'Stafford'Narelle'Stubbs''Henry'Tsao'Donna'Urquhart'Richard'Yang'
''
'
Doctoral'students'(Present)' ' ''Kim'Allison'Rafeef'Aljuraifani'Michael'Bergin'Catharina'Bexander'Edith'Elgueta1Cancino ''Alessio'Gallina ''Jan'Gildea'Luke'Heales'David'Klyne'Liam'Maclachlan'Laura'Morrison ''Camille'Shanahan'Viana'Vuvan'Peter'Window ''
UQ'Collaborators'Prof'Gwen'Jull''A/Prof'Sandy'Brauer ''Dr'Kylie'Tucker'Dr'Andrew'Claus'Dr'Michelle'Smith'
Twitter:@paulwhodges
Thank you