quit rates among smokers who - sinfoníarx smoking... · kennedy dt, giles jt, chang zg, small re,...
TRANSCRIPT

2
Quit rates among smokers who received pharmacist-provided pharmacotherapy and quitline
services versus those who received only quitline services.
Jill Augustine, PharmD, MPH1; Ryan Seltzer, PhD2; Martin Pelger, BSPharm, RPh3; Kevin Boesen, PharmD4; Terri
Warholak, PhD, RPh1
1 University of Arizona College of Pharmacy2University of Arizona Mel & Enid Zuckerman College of Public Health, ASHLine
3 University of Arizona College of Pharmacy Medication Management Center4SinfoníaRx

3
Supporter• [FOR APHA USE ONLY]
4
Attendance Code
[FOR APHA USE ONLY]
To obtain CPE credit for this activity, you are required to actively participate in this session. The attendance code is needed to access the evaluation and CPE form for this activity. Your CPE must be filed by April 27, 2015 at 5:00 pm EDT in order to receive credit.
5
Disclosures• Dr. Jill Augustine reports that she has stock in Pfizer,
Inc., which markets for many of the smoking cessation products.
• All other faculty declare(s) no conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and honoraria.
The American Pharmacists Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
6
• Target Audience: [FOR APHA USE ONLY]
• ACPE#: [FOR APHA USE ONLY]
• Activity Type: [FOR APHA USE ONLY]

7
Learning Objectives1. Summarize the impact of smoking cessation services on
healthcare resource cost and utilization2. Compare quit rates presented in previous literature3. Discuss the quit rates for Arizona state employees who
received pharmacotherapy smoking cessation counseling and/or telephone quit services
4. Outline key differences in the intent to treat and responder rate analyses
8
Which program had a significantly higher unadjusted quit rate for the
responder rate analysis? a. Participants receiving the combined pharmacotherapy
smoking cessation counseling plus telephone quitlineservices (Medication Management Center (MMC) participants).
b. Participants receiving telephone quitline services only (Arizona Smoker’s Helpline (ASHLine) participants).
c. There were no significant differences observed between the two groups of participants.
9
Background• Cigarette smoking is the leading cause of preventable disease and
death in the U.S. 1
– Approximately 42 million adults currently smoke cigarettes (~17.8%).1
– Annual economic costs of tobacco use exceed $289 billion.2
• Nearly 70% of ‘current’ U.S. adult cigarette smokers want to quit completely.3
– Almost 53% attempt to quit once in the past year.3
– About 43% of all adult smokers stopped smoking for >1 day. 3
• Multiple smoking cessation treatments are available including quitlineservices, nicotine replacement therapies, and prescription medications.
Objective 1

10
Background• Quitline are beneficial in helping smokers quit.4-6
– Quit rates range from 6-27%, depending on the number of calls.4
• Pharmacist-provided programs are effective in helping smokers quit.7-12
– Quit rates range from 12-28%, depending on the program type.7-12
• Combined medication-plus-counseling programs are more effective (27.6%) in treating tobacco dependence than medication (21.7%) or counseling (14.6%) used alone.5-6
Objective 2
11
Methods• Retrospective chart review• Inclusion criteria
– Received services from University of Arizona Medication Management Center (UAMMC); Arizona Smokers’ Helpline (ASHLine); or both
– Completed a follow-up phone call to determine smoking cessation– Initial enrollment prior to December 1, 2012– Completed a phone call with ASHLine
• Exclusion criteria– Participant contacted either service to request smoking cessation
information and not interested in quitting
• IRB approved project
12
InterventionsArizona Smokers’ Helpline
(ASHLine)
• Free telephone and Web-based quit service
• Any resident of Arizona may contact trained personnel
• Personnel work with smokers • Set goals• Work towards a quit date• Develop a personnel plan for
quitting
University of Arizona Medication Management
Center (MMC)• Offers pharmacotherapy
smoking cessation support• State of Arizona employees
receive information about MMC in their medical insurance packages
• Patients can• Access to pharmacotherapy
treatment options at no cost• Received scheduled
counseling by pharmacists• All patients who receive
cessation services from MMC are referred to ASHLine

13
Methods• Participants were matched on:
– Medication use– Stage of Change– Self-efficacy– Education
• Quit success (30 days smoke-free) or failure was based on participants’ self-report.

14
Methods-Data Analysis• Descriptive statistics used for baseline characteristics,
current smoking habits and matching statistics.
• Chi-square test used for unadjusted quit rates.
• Generalized linear mixed model used for adjusted quit rates.

15
Results-Baseline characteristics• 241 matched pairs
ASHLine(n=241)
MMC + ASHLine(n=241)
Age, mean (SD) 50 (13) 52 (12)
Female, n (%) 142 (59) 141 (59)
Caucasian, n(%) 188 (78) 186 (77)
Not Hispanic, n (%)* 184 (76) 206 (85)
Some College Education, n (%)* 74 (31) 100 (41)*p-value<0.001
16
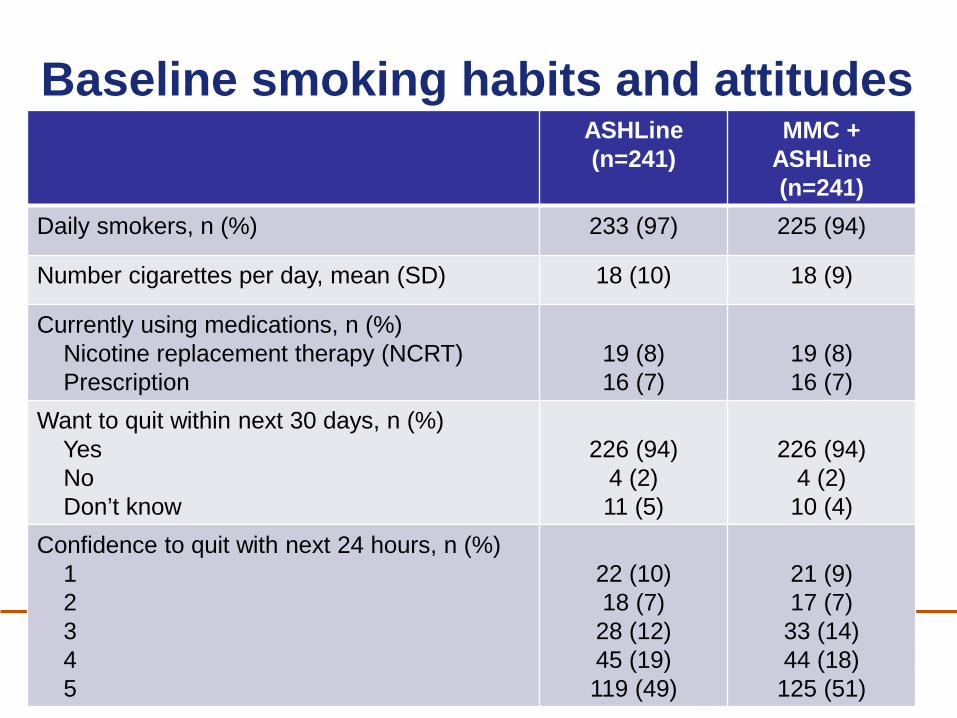
Baseline smoking habits and attitudesASHLine(n=241)
MMC + ASHLine(n=241)
Daily smokers, n (%) 233 (97) 225 (94)
Number cigarettes per day, mean (SD) 18 (10) 18 (9)
Currently using medications, n (%)Nicotine replacement therapy (NCRT)Prescription
19 (8)16 (7)
19 (8)16 (7)
Want to quit within next 30 days, n (%)YesNoDon’t know
226 (94)4 (2)11 (5)
226 (94)4 (2)10 (4)
Confidence to quit with next 24 hours, n (%)12345
22 (10)18 (7)
28 (12)45 (19)119 (49)
21 (9)17 (7)
33 (14)44 (18)
125 (51)

17
Results-Unadjusted Quit ratesIntent-to-treat analysis ASHLine
(n=241)MMC + ASHLine
(n=241)Quit, n (%) 47 (20) 43 (18)
Did Not Quit, n (%) 81 (34) 42 (17)
No response, n (%) 113 (47) 156 (65)
Quit Rate 20% 18%
Responder Rate ASHLine(n=128)
MMC + ASHLine(n=85)
Quit, n (%) 47 (37) 43 (51)
Did Not Quit, n (%) 81 (63) 42 (49)
Quit Rate* 37% 51%*p-value=0.045
§p-value=0.64
Objectives 3, 4
18
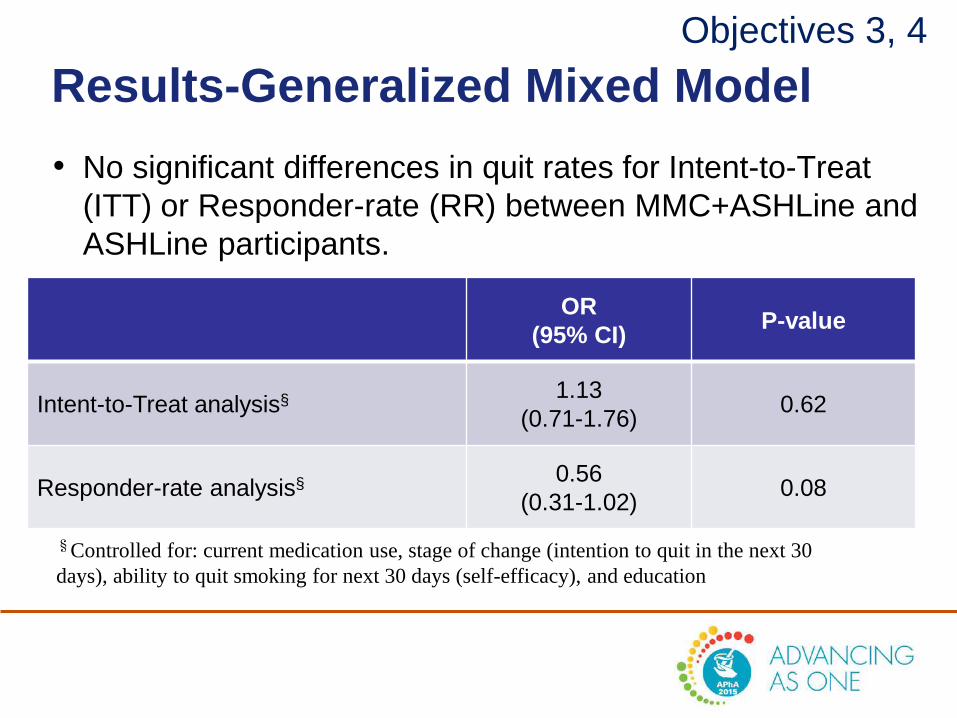
Results-Generalized Mixed Model• No significant differences in quit rates for Intent-to-Treat
(ITT) or Responder-rate (RR) between MMC+ASHLine and ASHLine participants.
OR(95% CI) P-value
Intent-to-Treat analysis§ 1.13(0.71-1.76) 0.62
Responder-rate analysis§ 0.56(0.31-1.02) 0.08
Objectives 3, 4
§Controlled for: current medication use, stage of change (intention to quit in the next 30 days), ability to quit smoking for next 30 days (self-efficacy), and education
19
Limitations• Non-randomized sample
• Baseline differences between groups
• Response bias– Self-report– Smoking stigma
• Large number of participants were lost to follow-up

20
Key Points• First study comparing quit rates between a pharmacist-
driven service and a quitline.
• Both interventions provide one-on-one support for smokers seeking help to quit.
• No significant differences observed between the groups for intent-to-treat analysis.
• Significant differences observed for responder rates for MMC+ASHLine participants (51%) versus ASHLine alone (37%).

21
References1. Centers for Disease Control and Prevention. Current Cigarette Smoking Among Adults—United States, 2005–2013..
Morbidity and Mortality Weekly Report 2014;63(47):1108–12 [accessed 2015 Jan 29].2. U.S. Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A
Report of the Surgeon General. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014 [accessed 2015 Jan 29]..
3. Centers for Disease Control and Prevention. Quitting Smoking Among Adults—United States, 2001–2010. Morbidity and Mortality Weekly Report 2011;60(44):1513–19 [accessed 2015 Jan 29].
4. Stead LF, Hartmann-Boyce J, Perera R, Lancaster T. Telephone counselling for smoking cessation. Cochrane Database Syst Rev. 2013; 8: CD002850. doi: 10.1002/14651858.CD002850.pub3.
5. Fiore MC, Jaén CR, Baker TB, et al. Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. Rockville, MD: U.S. Department of Health and Human Services. Public Health Service. May 2008.
6. An LC, Schillo BA, Kavanaugh AM, Lachter RB, Luxenberg MG, Wendling AH, Joseph AM. Increased reach and effectiveness of a statewide tobacco quitline after the addition of access to free nicotine replacement therapy. TobControl. 2006;15:286-293.
7. Sinclair HK, Bond CM, Stead LF. Community pharmacy personnel interventions for smoking cessation. Cochrane Database of Systematic Reviews 2004, Issue 1. Art. No.: CD003698. DOI: 10.1002/14651858.CD003698.pub2.
8. Kennedy DT, Giles JT, Chang ZG, Small RE, Edwards JH. Results of a smoking cessation clinic in community pharmacy practice. J Am Pharm Assoc. 2002;42(1):51–6.
9. Roth MT, Westman EC. Use of bupropion SR in a pharmacist managed outpatient smoking-cessation program. Pharmacotherapy. 2001;21(5):636–41.
10. Sinclair HK, Bond CM, Lennox AS, Silcock J, Winfield AJ, Donnan PT. Training pharmacists and pharmacy assistants in the stage-of-change model of smoking cessation: a randomized controlled trial in Scotland. Tobacco Control.1998;7(3):253–61.
11. Maguire TA, McElnay JC, Drummond A. A randomized controlled trial of a smoking cessation intervention based in community pharmacies. Addiction. 2001;96(2):325–31.
12. Mdere ND, Chindove S. Effectiveness of tobacco use cessation interventions delivered by pharmacy personnel: A systematic review. Res Soc Admin Pharm. 2014;10(1):21-44
22
Which program had a significantly higher unadjusted quit rate for the
responder rate analysis? a. Participants receiving the combined pharmacotherapy
smoking cessation counseling plus telephone quitlineservices (Medication Management Center (MMC) participants).
b. Participants receiving telephone quitline services only (Arizona Smoker’s Helpline (ASHLine) participants).
c. There were no significant differences observed between the two groups of participants.
23
Attendance Code
[FOR APHA USE ONLY]
You will need this attendance code in order to access the evaluation and CPE form for this activity. Your CPE must be filed by April 27, 2015 at 5:00 pm EDT in order to receive credit.
