qut digital repository: · the refractive power of the whole eye, compared to that of the anterior...
TRANSCRIPT

QUT Digital Repository: http://eprints.qut.edu.au/
Read, Scott A. and Collins, Michael J. (2009) Diurnal variation of corneal shape and thickness. Optometry and Vision Science, 86(3). pp. 170-180.
© Copyright 2009 American Academy of Optometry

1
The diurnal variation of corneal shape and thickness.
Scott A Read (PhD)*
Michael J Collins (PhD)
*Corresponding Author
Contact Lens and Visual Optics Laboratory
School of Optometry
Queensland University of Technology
Room B556, O Block, Victoria Park Road, Kelvin Grove 4059
Brisbane, Queensland, Australia
Phone: 617 3864 5739, Fax: 617 3864 5665
Email: [email protected]
Number of figures: 4
Number of Tables: 2
Word count: 4822
Date: 11th September 2008

2
Abstract:
Purpose: To investigate associations between the diurnal variation in a range of
corneal parameters, including anterior and posterior corneal topography, and
regional corneal thickness.
Methods: Fifteen subjects had their corneas measured using a rotating
Scheimpflug camera (Pentacam) every 3-7 hours over a 24-hour period. Anterior
and posterior corneal axial curvature, pachymetry and anterior chamber depth
were analysed. The best fitting corneal sphero-cylinder from the axial curvature,
and the average corneal thickness for a series of different corneal regions were
calculated. Intraocular pressure and axial length were also measured at each
measurement session. Repeated measures ANOVA were used to investigate
diurnal change in these parameters. Analysis of covariance was used to
examine associations between the measured ocular parameters.
Results: Significant diurnal variation was found to occur in both the anterior and
posterior corneal curvature and in the regional corneal thickness. Flattening of
the anterior corneal best sphere was observed at the early morning
measurement (p < 0.0001). The posterior cornea also underwent a significant
steepening (p < 0.0001) and change in astigmatism 90/180° at this time. A
significant swelling of the cornea (p < 0.0001) was also found to occur

3
immediately after waking. Highly significant associations were found between
the diurnal variation in corneal thickness and the changes in corneal curvature.
Conclusions: Significant diurnal variation occurs in the regional thickness and
the shape of the anterior and posterior cornea. The largest changes in the
cornea were typically evident upon waking. The observed non-uniform regional
corneal thickness changes resulted in a steepening of the posterior cornea, and a
flattening of the anterior cornea to occur at this time.
Key words: Diurnal variation, corneal topography, posterior cornea, corneal
thickness.
4
Introduction
The cornea (in conjunction with the pre-corneal tear film) is the eye’s most
anterior optical surface, and is responsible for approximately two-thirds of the
eye’s refractive power. In recent years, advances in ophthalmic instrumentation,
has enhanced our ability to accurately, precisely and comprehensively define a
range of different corneal parameters such as anterior and posterior corneal
topography and corneal thickness. Detailed assessment of these corneal
parameters can be important for a number of different clinical and research
applications including: the diagnosis and monitoring of corneal ectatic disorders
such as keratoconus1-7 and pellucid marginal degeneration,8,9 the monitoring of
corneal dystrophies,10,11 the evaluation of corneal grafts,12-16 rigid and soft
contact lens fitting and design,17-20 the detection and monitoring of contact lens
induced corneal changes,21-26 the pre and post-operative screening of refractive
surgery candidates,27-33 and for customized refractive corrections.34-37
Knowledge of the natural diurnal variation occurring in corneal parameters is of
particular relevance to any clinical or research application requiring accurate and
precise measurements of the cornea. The cornea is typically found to be at it’s
thickest upon waking and then returns quickly to baseline within the first 2 hours
of waking.21,38-42 Measurements of the curvature,43,44 topography39,45,46 and
aberrations46 of the anterior corneal surface have also been found to undergo
significant diurnal variation. Less however, is known about the natural diurnal

5
variation that occurs in other corneal parameters such as the cornea’s regional
thickness and the shape of the posterior cornea.
The difference in refractive index between the posterior corneal surface and
aqueous humor means that the posterior cornea makes a lesser contribution to
the refractive power of the whole eye, compared to that of the anterior cornea.
However, recent research investigating the shape of the posterior cornea has
highlighted the importance of this surface, showing that the posterior cornea
contributes significantly to the astigmatism47 and spherical aberration48 of the
eye. It has also been suggested that measurement of the posterior cornea may
be important for the early detection of keratoconus,5,7,29 particularly in the
detection of early ectasia in pre- and post-operative corneal refractive surgery
patient screening.29,49
We investigated the normal variation that occurs in the cornea of young adult
subjects over a 24 hour period using an instrument capable of measuring the
anterior and posterior cornea and the regional thickness of the cornea. To
investigate the influence of variations of other ocular parameters on the observed
corneal changes, we also simultaneously measured intraocular pressure (IOP)
and ocular pulse amplitude (OPA) using dynamic contour tonometry (a
tonometric technique thought to provide IOP measures largely independent of
corneal thickness),50-53 as well as measuring the axial length of the eye.

6
Methods
Subjects and procedures
Fifteen young healthy, emmetropic adult subjects aged between 20 and 27 years
(mean age 22 years) were recruited for this study. Subjects were primarily
recruited from the students and staff of our university. Eight of the subjects were
male. All subjects were free of significant ocular or systemic disease and had no
history of ocular surgery or significant trauma. None of the subjects were contact
lens wearers. Prior to the study, each subject underwent an initial ophthalmic
examination to ensure good ocular health and to determine their refractive status.
All subjects had normal visual acuity of logMAR 0.00 or better. The subjects’
mean ± SD best sphere refraction was found to be -0.3 ± 0.4 DS (range +0.25 to
-1.13 DS), with a mean ± SD cylinder refraction of -0.2 ± 0.3 DC (range 0.00 to -
1.00 DC). No subject exhibited anisometropia of greater than 0.75 DS. Approval
from the university human research ethics committee was obtained prior to
commencement of the study and subjects gave written informed consent to
participate. All subjects were treated in accordance with the tenets of the
declaration of Helsinki.
This study took place over 5 separate days, with 2-4 subjects participating on
each day. On each day, 6 separate measurement sessions took place every 3-7
hours over a 24 hour period. At each measurement session the corneal
parameters (i.e. measures of the anterior and posterior cornea and corneal
thickness), axial length, and IOP of each subject’s right eye were measured in
7
the sitting position. The initial measurement session for all subjects took place in
the morning, at least two hours after their reported time of awaking on that day.
Following the initial measurement, subjects undertook their regular daily
activities, and returned to the research laboratory for each subsequent
measurement session. Over the course of the study, measurement sessions
occurred at the following mean times: session 1 at 09:40 (range: 08:35-11:00),
session 2 at 13:00 (12:00-14:10), session 3 at 17:30 (17:00-18:30), session 4 at
22:30 (22:00-23:20), session 5 at 06:00 (05:00-06:40) and session 6 at 09:20
(08:00-10:20). One subject was unable to attend for one of their scheduled
measurement sessions. Following session 4 (mean time 22:30), subjects went to
sleep in individual darkened rooms within the research laboratory. The next
morning, subjects were awakened and instructed to sit for 5 minutes with their
eyes closed prior to the beginning of measurement session 5, to ensure that
postural variations in IOP54,55 did not influence the results. Following session 5,
subjects remained awake until the final measurement session. At each
measurement session, the time taken to perform the entire series of
measurements on each subject was approximately 20 minutes.
Corneal parameters were measured using the Pentacam HR system (Oculus Inc,
Wetzlar Germany). The Pentacam is a non-contact instrument that utilizes a
rotating Scheimpflug camera to measure the anterior segment. Previous studies
have shown the Pentacam to have excellent repeatability for measurements of
central corneal thickness,56-59 peripheral corneal thickness,59 anterior59 and
8
posterior59,60 corneal curvature and anterior chamber depth.59,61-63 The
instrument has also been found to provide measurements of corneal thickness
from normal subjects that are in reasonable agreement with previously validated
clinical instruments.56-58 The Pentacam’s “50 picture 3D Scan” measurement
mode was used for all measures. For each measurement, the Pentacam’s
internal fixation target was adjusted so that subjects were viewing the target with
relaxed accommodation. At each measurement session a total of 5 corneal
scans were performed on each subject. The instrument also outputs a ‘quality
specification’ for each measurement which provides information about the
reliability of each 3D scan (this checks for poor alignment, excessive eye
movements, or any missing or invalid data). Any measurements flagged as
unreliable were repeated until 5 valid measures were obtained. Following image
capture, the instrument analyses these 50 cross sectional images of the anterior
eye and provides axial corneal curvature (front and back surface), elevation (front
and back corneal surface) and pachymetry maps. Anterior chamber depth (ACD)
(defined as the axial distance from the corneal endothelium to the anterior lens
surface) and central corneal thickness (CCT) at the corneal apex was also
recorded.
Axial length (defined in this case as the distance from the anterior corneal
surface to the retinal pigment epithelium along the visual axis) was measured
with the IOLMaster (Zeiss Meditec, Jena, Germany). The IOLMaster is a non-
contact instrument based upon the principles of partial coherence laser

9
interferometry (PCI)64 and has been found to provide highly precise
measurements of axial length.64-67 Prior to the study, the calibration of the
IOLMaster was checked using the instrument’s test eye. For each subject a total
of 5 measurements of axial length were taken at each measurement session and
the mean of these readings calculated. Any measurements of axial length from
the IOLMaster with a reported signal-to-noise ratio of less than 2.0 were repeated
until 5 valid readings were attained.
All IOP measures were carried out using the Pascal Dynamic contour tonometer
(DCT) (Ziemer Ophthalmic Systems, Port, Switzerland). The DCT is a contact
tonometer that works on the principle of contour matching. The instrument
outputs measures of mean IOP and ocular pulse amplitude (OPA) (defined as the
difference between the diastolic and systolic IOP) as well as a quality score
(where a score of 4 or 5 indicates an unreliable result) for each measurement.
The DCT has been found to exhibit good inter- and intra-observer repeatability,
comparable to Goldmann applanation tonometry.50 The tonometer’s calibration
was checked using the Pascal tonometer performance test kit prior to
commencement of the study. Measurements with the DCT were taken according
to manufacturer instructions, following the instillation of a drop of local anesthetic
(0.4 % oxybuprocaine hydrochloride). A total of 3 DCT measurements were
taken for each subject at each measurement session and the mean IOP and
OPA from the three measurements calculated. Any measurement displaying a
quality score of 4 or 5 was repeated until 3 valid measures were obtained. All
10
DCT measurements were taken by one clinician, experienced in the use of the
instrument.
Following the IOP measurements, a careful slit lamp examination was carried out
to ensure that no substantial epithelial disruption occurred as a result of the
contact tonometry procedure or anesthetic drops. There have been some
previous reports of transient changes in corneal thickness (lasting up to 10
minutes) following the instillation of topical anesthetic eye drops.68-70 However,
other investigators have reported that anesthetic eyedrops and contact
tonometry71 or anesthetic eye drops alone72 do not cause a significant change in
corneal thickness measures. To ensure that the corneal measurements were not
influenced by any epithelial disruption brought about by contact tonometry or
local anesthetic instillation, the tonometry was always the final measurement
performed at each session. Each measurement session was also spaced apart
by 3-7 hours. It is therefore unlikely that the contact tonometry procedure would
have substantially influenced our corneal thickness and topography results.
Data analysis
Following data collection, a range of corneal data was exported from the
Pentacam. Pachymetry, and corneal axial curvature (anterior and posterior
corneal surface), maps were all exported from the instrument for further analysis.
These maps are output from the Pentacam in a square grid format with a data

11
point spacing of 0.1 mm. These corneal data were analyzed using customized
software.
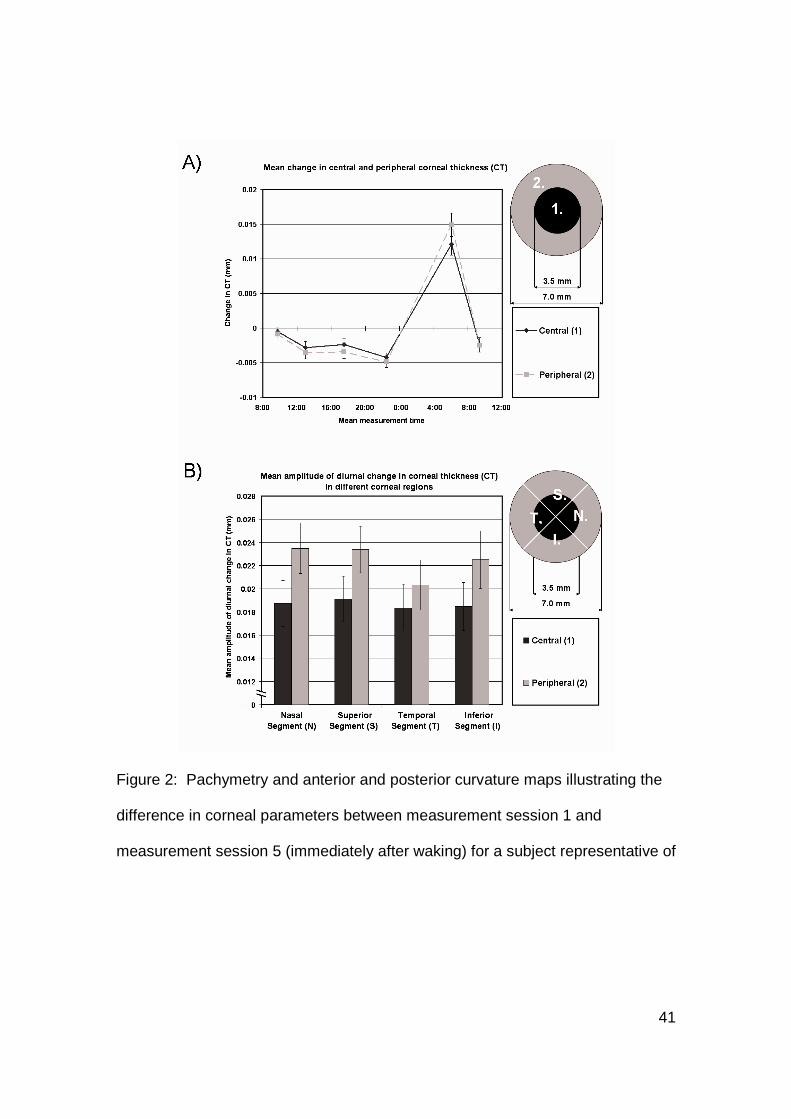
To investigate the average diurnal change in corneal thickness for our population
of subjects, data from each of the 5 pachymetry maps for each subject from each
session were analysed. The mean corneal thickness for the central 3.5 mm
diameter (i.e. Region ‘1’ in Figure 1a), and for the peripheral 3.5 mm annulus
outside of this central zone were calculated (i.e. Region ‘2’ in Figure 1a) for each
map. The average thickness of the central corneal region (region 1) and average
thickness of the peripheral corneal region (region 2) for each subject at each
measurement session was calculated. To investigate the diurnal variation in the
data from these two regions of the cornea, a repeated measures analysis of
variance (ANOVA) was carried out with two within-subject parameters: time of
measurement and corneal region (the one subject who did not have complete
sets of data from all 6 measurement sessions was not included in the ANOVAs,
since it required all subjects to have 6 complete data sets).
The corneal thickness within each of these measured regions was further
analysed to calculate the average thickness of the cornea within a 90° nasal
segment (i.e. segment ‘N’ in Figure 1b), a 90° supe rior segment (i.e. segment ‘S’
in Figure 1b), a 90° temporal segment (i.e. segment ‘T’ in Figure 1b) and a 90°
inferior segment (i.e. segment ‘I’ in Figure 1b) within both the central and
peripheral corneal regions at each session for each subject. The amplitude of

12
corneal thickness change (i.e. the difference between the maximum and
minimum corneal thickness values over the 6 measurement sessions) within
each segment for each of the corneal regions was calculated for each subject.
To investigate for significant differences between the mean amplitude of corneal
change occurring in each of the measured areas, a repeated measures ANOVA
was carried out with two within-subject factors: corneal region (i.e. central and
peripheral) and corneal segment (i.e. nasal, superior, temporal and inferior).
To investigate the average diurnal change in the anterior and posterior corneal
surfaces, each of the curvature maps were converted into axial power, assuming
a corneal refractive index of 1.376 and a refractive index of 1.336 for the
aqueous. The best fit corneal sphero-cylinder was then calculated for each of the
axial power maps for each subject at each session using the methods of Maloney
et al73 for a 3.5 mm and a 7 mm diameter for both the anterior and posterior
cornea. The best fit corneal sphero-cylinder was converted into the power
vectors M (best sphere) J0 (astigmatism 90/180°) an d J45 (astigmatism
45/135°) 74 and the average corneal power vectors calculated for each subject at
each session. The mean amplitude of change for each power vector describing
the anterior and the posterior cornea for each subject was calculated.
Each subject’s mean axial length, IOP, OPA, CCT and ACD were also calculated
for each measurement session, and group mean values calculated for each
parameter. To investigate the associations between the variations in corneal

13
curvature and the variation occurring in the other measured variables, an
analysis of covariance was carried out as described by Bland and Altman75 for
the analysis of repeated observations. The significance of the association is
determined based upon the F statistic from the analysis of covariance.
Results
A number of the measured corneal variables were found to undergo significant
diurnal variation for our population of young adult emmetropic subjects. The
largest magnitude of change in all of the measured corneal variables was
typically found to occur at measurement session 5 immediately after waking.
Corneal thickness
All subjects were found to exhibit a similar pattern of change in their corneal
thickness. A very slight decrease (thinning) from the mean corneal thickness
was observed throughout the day (between measurement sessions 1 and 4), with
a swelling of the cornea evident upon waking (measurement session 5). By
measurement session 6 (mean time 09:20) the corneal thickness had typically
returned close to its mean level. The mean ± SD corneal thickness for the
central 3.5 mm region and peripheral 3.5 to 7.0 mm annulus region was found to
be 0.540 ± 0.029 mm and 0.598 ± 0.034 mm respectively. The mean amplitude

14
of change over the 24-hour measurement period was 0.019 ± 0.008 mm and
0.022 ± 0.008 mm for the central and peripheral regions respectively. Repeated
measures ANOVA revealed a significant diurnal variation in corneal thickness
with time (p <0.0001), a significant difference between the two corneal regions (p
<0.0001) and a significant time*corneal region interaction (p<0.0001). Figure 1a
illustrates the mean change in corneal thickness in the two corneal regions over
time.
The mean amplitude of change in the nasal, superior, temporal and inferior
segments for the central and peripheral corneal regions is illustrated in Figure 1b.
Repeated measures ANOVA revealed the mean amplitude of change to be
significantly different between the central and peripheral corneal regions (p
<0.0001), while the amplitude of change in the different segments approached
significance (p=0.062). A significant interaction was found between corneal
region and corneal segment (p = 0.01). This interaction was primarily brought
about by the peripheral temporal region exhibiting significantly smaller amplitude
of thickness change compared with the superior (pair-wise comparison with
Bonferroni adjustment p = 0.003) and nasal peripheral regions (p = 0.002). We
re-analysed this pachymetry data by expressing the change in corneal thickness
as the percentage of the mean thickness in each region, and similar statistical
trends were observed.

15
In Figure 2, pachymetry maps illustrating the difference in corneal thickness
observed between the first measurement session (session 1, mean time 09:40)
and the early morning measurement session immediately after awaking (session
5, mean time 06:20), for a typical subject (subject 5) are shown.
Corneal curvature
Significant change was also found in the corneal axial curvature data. The
largest change was again typically found to be evident upon waking. Axial
curvature maps illustrating the difference between session 1 and session 5 for
both the anterior and posterior cornea surfaces from a typical subject are shown
in Figure 2. The anterior cornea was found to flatten at the early morning
measurement (with greater flattening typically observed in the central cornea)
and the posterior cornea was typically found to steepen, with some increases
also found in astigmatism (a steepening in the vertical meridian) at this time.
The best fitting corneal sphero-cylinder was found to undergo some significant
change (Table 1). The diurnal variation in the anterior corneal best sphere (M)
was highly significant (repeated measures ANOVA p <0.0001 for ‘time of
measurement’), with a mean amplitude of change of 0.36 ± 0.11 D and 0.27 ±
0.09 D for the 3.5 mm and 7.0 mm diameters. The largest changes (a flattening
of the cornea) were observed immediately after subjects awoke. The magnitude
of change for the 3.5 mm analysis diameter was significantly greater than the
magnitude of change for the 7.0 mm analysis diameter (two-tailed paired t-test p

16
<0.0001). The posterior corneal best sphere (M) was also found to undergo a
significant diurnal change (repeated measures ANOVA p <0.00001) with a
steepening of the posterior corneal curvature found upon waking. The mean
amplitude of change in the posterior corneal best sphere was 0.05 ± 0.03 D and
0.04 ± 0.02 D for the 3.5 and 7.0 mm diameters. The mean amplitude of change
in the central (3.5 mm diameter) posterior cornea was significantly greater than
the amplitude of change in the peripheral (7.0 mm diameter) posterior cornea (p
= 0.02).
The mean change in the anterior and posterior corneal best sphere (M) is
illustrated in Figure 3. It should be noted that a steepening of the anterior cornea
will lead to an increase in positive dioptric power, whereas a steepening of the
posterior cornea will lead to a decrease in positive dioptric power (due to the
refractive index difference between the cornea and the aqueous). To illustrate
this, the mean axial power best fitting sphero-cylinder was converted into axial
curvature (expressed in mm) and is also presented in Figure 3. The changes in
axial curvature (mm) give an indication of the shape changes occurring in the two
corneal surfaces, whereas the changes in axial power (D) give an indication of
the effective change in dioptric power. It is clear from Figure 3 that there is a
change in anterior and posterior axial curvature of a similar magnitude in
opposite directions (i.e. a flattening of the anterior and a steepening of the
posterior cornea). The resulting change in axial power for the anterior and

17
posterior cornea is in the same direction but is substantially smaller in the
posterior cornea due to the refractive index difference at the aqueous interface.
Anterior corneal J0 (astigmatism 90/180°) and the a nterior and posterior corneal
J45 (astigmatism 45/135°) were not found to undergo significant diurnal change
(p>0.05) (Table 1, Figure 3). The posterior corneal J0 (astigmatism 90/180°)
however, did undergo significant diurnal change (p < 0.0001). The mean
posterior corneal J0 was found to be -0.16 ± 0.05 D and -0.14 ± 0.03 D for the
3.5 mm and 7.0 mm diameters respectively with a mean amplitude of change of
0.05 ± 0.02 D and 0.03 ± 0.01 D. The amplitude of change in J0 was significantly
greater for the 3.5 mm diameter analysis (p = 0.0008). The largest change in
posterior corneal J0 was again evident upon waking, with a decrease in axial
power J0 observed. This change in axial power for posterior J0 is brought about
by a steepening of the curvature of the posterior cornea in the vertical meridian.
Associations between variables
The diurnal variation observed in IOP, OPA, CCT and ACD for our population
has been reported in detail elsewhere.76 A number of significant associations
were found between the variation in corneal power vectors and the change in
other measured variables (i.e. IOP, OPA, CCT and ACD). The results from the
analysis of covariance, the correlation coefficient (r) and it’s associated
significance (p) for each of the corneal power vectors (7 mm diameter) is
presented in Table 2.

18
The anterior corneal best sphere (M) was found to have a significant association
with the CCT (r= -0.62, p=<0.0001), indicating that a flattening of the anterior
cornea is associated with an increase in the thickness of the central cornea. The
variation in anterior corneal M was also found to be associated with the change in
ACD (r= 0.39, p= 0.003), indicative that a shallower anterior chamber was
associated with a flattening of the anterior cornea. A significant association was
also found between the changes in anterior corneal J45 (astigmatism 45/135°)
and CCT (r = 0.42, p = 0.001).
The power vectors from the posterior cornea also exhibited some significant
associations. The variation in the posterior corneal best sphere (M) was
significantly associated with the change in CCT (r = 0.73, p <0.0001), (i.e. a
steepening of the posterior cornea is associated with a thickening of the cornea).
The change in posterior corneal J0 was found to be significantly associated with
the change OPA (r = 0.40, p = 0.002), the change in CCT (r = -0.43, p = 0.006)
and with the change in ACD (r = 0.35, p = 0.01).
Discussion
We have found that small but significant diurnal changes occur in a number of
parameters describing the anterior and posterior shape and thickness of the
cornea in our population of young adult subjects. The largest magnitude

19
changes in most corneal parameters were observed to occur upon subjects’
waking, which is consistent with a number of previous studies of diurnal variation
of the cornea.38-42,45 The general pattern and magnitude of diurnal change that
we have observed in anterior corneal curvature39,45,46 and central corneal
thickness38-42 are also consistent with those of previous investigations.
Furthermore, the posterior corneal curvature was also found to undergo
significant diurnal variation. To our knowledge, this is the first study to report
upon the physiological diurnal variation that occurs in the posterior cornea. A
gradual flattening of small magnitude was observed over the course of the day
(between 9:40 and 10:30 pm), and a significant steepening and alteration in
astigmatism of the posterior cornea were evident upon waking. The strong and
highly significant correlations found between the diurnal variations in the posterior
corneal shape (both posterior corneal best sphere and astigmatism 90/180°) and
CCT are indicative that these posterior corneal changes are related to changes in
corneal hydration occurring over the diurnal period.
It is evident from Figure 3 (top right) that the magnitude of spherical shape
change found in the posterior corneal curvature (mean amplitude of change 0.05
± 0.02 mm for a 7 mm corneal diameter with a steepening upon first waking) was
approximately equal and opposite to the change found in the anterior cornea
(mean amplitude of change 0.05 ± 0.01 mm for a 7 mm corneal diameter with a
flattening upon first waking). The optical effects of these posterior corneal

20
changes though, are small (mean amplitude of change in axial power of 0.05 D),
and will not substantially impact upon the refractive power of the cornea.
In recent years, there has been interest in the shape of the posterior cornea
following laser refractive surgery27-33,77 with some evidence of a steepening of
the posterior cornea in some patients after this procedure.27,28,77 It is conceivable
that different patterns of diurnal change in the posterior cornea may be observed
in patients who have undergone laser refractive surgery (due to alterations in
corneal biomechanical properties and stromal collagen architecture as a result of
refractive surgery), and this may be a worthwhile area for future investigation.
Upon first waking, we found a flattening of the anterior corneal surface, a
steepening of the posterior corneal surface, a thickening of the cornea (of slightly
greater magnitude in the peripheral cornea) and a concomitant reduction in the
ACD.76 The pattern of corneal and anterior chamber change observed upon first
waking, are therefore indicative of corneal swelling with a backward movement of
the posterior corneal surface and a slight forward movement of the anterior
corneal surface (more so in the peripheral corneal regions). A schematic
diagram summarising the average changes that we observed in the cornea and
anterior chamber is presented in Figure 4. A backward movement of the
posterior corneal surface into the anterior chamber upon waking is consistent
with previous research into the swelling properties of the cornea.78-80

21
Our experimental findings indicate that some differences exist between the
diurnal variation occurring in the curvature of the anterior and posterior corneal
surfaces. Both spherical shape and the astigmatism of the posterior cornea were
found to vary significantly, whereas significant change was only found in the
spherical shape of the anterior cornea. Previous anatomical studies have noted
differences in the stromal collagen fibril architecture,81 the density of stromal
collagen lamellae82 and the distribution of stromal proteoglycans83 between
anterior and posterior corneal regions. The swelling properties of the anterior
and posterior stroma have also been found to differ.78,80 Differential swelling
between the anterior and posterior corneal stroma may therefore account for
some of the differences we have observed in the diurnal variation in the curvature
of the anterior and posterior corneal surfaces.
By utilizing the Pentacam instrument, we were able to observe that diurnal
variation also occurs in the regional thickness of the cornea, with greater
amplitude of diurnal change found in the peripheral cornea (on average 3.46 %
change was found in the central region compared to 3.74% change in the
peripheral corneal region). A uniform change in thickness would not alter the
axial radius of curvature of the corneal surfaces. Therefore the peripheral
thickening we observed explains the flattening of the anterior corneal radius and
steepening of the posterior corneal radius. The majority of previous studies
investigating the diurnal variation of corneal thickness have been limited to
central corneal thickness measurements,38,40-42 or central and peripheral

22
thickness with peripheral estimates based upon single points in the corneal
periphery.39 Lattimore et al84 measured the diurnal variation of the cornea’s
regional thickness using a scanning-slit device in one subject and also found that
a greater amplitude of diurnal change was evident in the peripheral cornea. The
non-uniform diurnal variation that we have observed in corneal thickness from
centre to periphery may relate to differences in the arrangement of stromal
collagen fibrils in these different corneal regions. Boote et al85 using x-ray
diffraction techniques found that whilst the diameter of stromal collagen fibrils
remained constant from centre to the periphery, the fibril spacing was greater in
the peripheral cornea. The denser packing of fibrils within the central cornea is a
possible reason for the slightly smaller amplitude of swelling noted in this region
compared to the more peripheral cornea. Previous studies of the physiological
diurnal variation of anterior corneal curvature have also found that a significant
flattening of the cornea occurs in the early morning.39,43-45 This pattern of change
in the anterior corneal curvature is consistent with the pattern of topographical
swelling that we have observed (i.e. a greater swelling in the peripheral cornea
upon first waking).
Some previous studies investigating ‘closed eye’ corneal swelling with contact
lens wear25,86-91 and open eye corneal swelling (induced by exposing the eye to
an “hypoxic” nitrogen gas atmosphere)92,93 have noted a different pattern of
regional corneal swelling, with greater swelling reported in the central cornea
compared to the periphery. The different pattern of swelling noted between our

23
current study and previous studies of closed eye swelling with contact lenses
may be indicative of the different causative mechanisms or magnitudes of
swelling involved (approximately 2-6% central corneal swelling in our current
study and 10-12% in previous contact lens studies25,86-91).
We found a number of significant associations exist between the diurnal variation
in corneal curvature and the variations in the other measured ocular variables.
The change in CCT was found to be significantly correlated with the change in
the corneal best sphere of both the anterior and posterior surface. The strong
associations found between corneal curvature of both the anterior and posterior
cornea and CCT indicate that a reasonable proportion of the diurnal variation in
the curvature of the cornea can be accounted for by changes in corneal
thickness. Interestingly, we found no significant associations between the change
in IOP and the diurnal variation of any of the measured corneal parameters.
Dynamic contour tonometry has previously been found to be able to measure
IOP independently of corneal thickness.50-53 The use of this instrument therefore
should allow any independent effects of fluctuations in the eye’s internal pressure
on the shape of the cornea to be evaluated. It therefore appears that the
changes of IOP within the physiological range found in our study (mean
amplitude of IOP change of 3.12 mmHg) were not enough to significantly
influence the measured corneal parameters.

24
In conclusion, we have found that small but significant changes occur in the
thickness of the cornea, and the shape of the anterior and posterior cornea over
a 24-hour period. This is the first study to quantify the normal physiological
diurnal variation that occurs in the posterior cornea. The posterior cornea was
found to undergo significant steepening and changes in astigmatism upon first
waking. However these changes had largely returned to normal by two to three
hours after waking. Small changes were also observed in the posterior cornea
throughout the day (a slight flattening). A significant swelling of the cornea was
evident upon waking, with the peripheral cornea exhibiting a greater magnitude of
change. Significant associations were also found between the diurnal change in
corneal thickness and the change in both the anterior and posterior corneal
curvature.
Acknowledgements:
The authors thank Inez Hsing and Andrew Tran for their assistance with data
collection and analysis procedures. We also thank Brett Davis for his assistance
with software analysis.
REFERENCES
1. Owens H, Watters GA. An evaluation of the keratoconic cornea using
computerized corneal mapping and ultrasonic measurements of corneal
thickness. Ophthal Physiol Opt 1996;16:115-23.

25
2. Schwiegerling J, Greivenkamp JE. Keratoconus detection based on
videokeratoscopic height data. Optom Vis Sci 1996;73:721-28.
3. Avitabile T, Marano F, Uva MG, Reibaldi A. Evaluation of central and
peripheral corneal thickness with ultrasound biomicroscopy in normal and
keratoconic eyes. Cornea 1997;16:639-44.
4. Pflugfelder SC, Liu Z, Feuer W, Verm A. Corneal thickness indices
discriminate between keratoconus and contact lens induced corneal thinning.
Ophthalmol 2002;109:2336-41.
5. Tanabe T, Oshika T, Tomidokoro A et al. Standardized color-coded scales for
anterior and posterior elevation maps of scanning slit corneal topography.
Ophthalmol 2002;109:1298-302.
6. Ambrosio R, Alonso RS, Luz A, Velarde LGC. Corneal-thickness spatial
profiole and corneal-volume distribution: Tomographic indices to detect
keratoconus. J Cataract Refract Surg 2006;32:1851-9.
7. Bessho K, Maeda N, Kuroda T, Fujikado T, Tano Y, Oshika T. Automated
keratoconus detection using height data of anterior and posterior corneal
surfaces. Jpn J Ophthalmol 2006;50:409-16.

26
8. Gruenauer-Kloevekorn C, Fischer U, Kloevekorn-Norgall K, Duncker GIW.
Pellucid marginal corneal degeneration: evaluation of the corneal surface and
contact lens fitting. Br J Ophthalmol 2006;90:318-23.
9. Lee BW, Jurkunas UV, Harissi-Dagher M, Poothullil AM, Tobaigy FM, Azar
DT. Ectatic disorders associated with a claw-shaped pattern on corneal
topography. Am J Ophthalmol 2007;144:154-6.
10. John GR. Videokeratographic abnormalities in a family with posterior
polymorphous dystrophy. Cornea 1998;17:380-3.
11. Ashfari NA, Pittard AB, Siddiqui A, Klintworth GK. Clinical study of Fuchs
corneal endothelial dystrophy leading to penetrating keratoplasty. A 30-year
experience. Arch Ophthalmol 2006;124:777-80.
12. Seitz B, Langenbucher A, Szentmary N, Naumann GOH. Corneal curvature
after penetrating keratoplasty before and after suture removal: A comparison
between keratoconus and Fuchs’ dystrophy. Ophthalmologica 2006;220:302-6.
13. Marcon AS, Terry MA, Kara-Jose N, Wall J, Ousley PJ, Hoar K. Influence of
final corneal thickness in visual acuity after deep lamellar endothelial
keratoplasty. Cornea 2007;26:543-5.

27
14. Vinciguerra P, Epstein D, Albe E, Spada F, Incarnato N, Orzalesi N, Rosetta
P. Corneal topography-guided penetrating keratoplasty and suture adjustment.
New approach for astigmatism control. Cornea 2007;26:675-82
15. Holz HA, Meyer JJ, Espandar L, Tabin GC, Mifflin MD, Moshirfar M. Corneal
profile analysis after Descemet stripping endothelial keratoplasty and its
relationship to postoperative hyperopic shift. J Cataract Refract Surg
2008;34:211-14.
16. Lim LS, Aung HT, Aung T, Tan DTH. Corneal imaging with anterior segment
optical coherence tomography for lamellar keratoplasty procedures. Am J
Ophthalmol 2008;145:81-90.
17. Szczotka LB. Clinical evaluation of a topographically based contact lens
fitting software. Optom Vis Sci 1997;74:14-19.
18. Reddy T, Szczotka LB, Roberts C. Peripheral corneal contour measured by
topography influences soft toric contact lens fitting success. CLAOJ
2000;26:180-5.

28
19. Szczotka LB, Roberts C, Herderick EE, Mahmoud A. Quantitative
descriptors of corneal topography that influence soft toric contact lens fitting.
Cornea 2002;21:249-55.
20. Nosch DS, Ong GL, Mavrikakis I, Morris J. The application of a
computerized videokeratography (CVK) based contact lens fitting software
programme on irregularly shaped corneal surfaces. Cont Lens Anterior Eye
2007;30:239-48.
21. Holden BA, Mertz GW, Mcnally JJ. Corneal response to contact lenses worn
under extended wear conditions. Invest Ophthalmol Vis Sci 1983;24:218-26.
22. Liu Z, Pflugfelder SC. The effects of long-term contact lens wear on corneal
thickness, curvature and surface regularity. Ophthalmology 2000;107:105-11.
23. Kaluzny JJ, Orzalkiewicz A, Czajkowski G. Changes of corneal thickness in
patients wearing frequent-replacement contact lenses. Eye Contact Lens
2003;29:23-26.
24. Schornack M. Hydrogel contact lens-induced corneal warpage. Cont Lens
Anterior Eye 2003;26:153-59.

29
25. Wang J, Fonn D, Simpson TL. Topographical thickness of the epithelium
and total cornea after hydrogel and PMMA contact lens wear with eye closure.
Invest Ophthalmol Vis Sci 2003;44:1070-74.
26. Martin R, de Juan V, Rodriguez G, Cuadrado R, Fernandez I. Measurement
of corneal swelling variations without removal of the contact lens during extended
wear. Invest Ophthalmol Vis Sci 2007;48:3043-50.
27. Baek TM, Lee KH, Kagaya F, Tomidokoro A, Amano S, Oshika T. Factors
affecting the forward shift of posterior corneal surface after laser in situ
keratomileusis. Ophthalmol 2001;108:317-20.
28. Seitz B, Torres F, Langenbucher A, Behrens A, Suarez E. Posterior corneal
curvature changes after myopic laser in situ keratomileusis. Ophthalmol
2001;108:666-73.
29. Rao SN, Raviv T, Majmudar PA, Epstein RJ. Role of Orbscan II in screening
keratoconus suspects before refractive corneal surgery. Ophthalmol
2002;109:1642-46.
30. Ambrosio R, Klyce SD, Wilson SE. Corneal topographic and pachymetric
screening of keratorefractive patients. J Refract Surg 2003;19:24-29.

30
31. Kamiya K, Miyata K, Tokunaga T, Kiuchi T, Hiraoka T, Oshika T. Structural
analysis of the cornea using scanning-slit corneal topography in eyes undergoing
excimer laser refractive surgery. Cornea 2004:23:S59-S64.
32. Varssano D, Kaiserman I, Hazarbassanov R. Topographic patterns in
refractive surgery candidates. Cornea 2004;23:602-607.
33. Ciolino JB, Belin MW. Changes in the posterior cornea after laser in situ
keratomileusis and photorefractive keratectomy. J Cataract Refract Surg 2006;
32:1426-31.
34. Alessio G, Boscia F, La Tegola MG, Sborgia C. Topography-driven
photorefractive keratectomy. Results of corneal interactive programmed
topographic ablation software. Ophthalmol 2000;107:1578-87.
35. Knorz MC and Jendritza B. Topographically-guided Laser In Situ
Keratomileusis to treat corneal irregularities. Ophthalmology 2000;107:1138-43.
36. Kanjani N, Jacob S, Agarwal A, Agarwal A, Agarwal S, Agarwal T, Doshi A,
Doshi S. Wavefront- and topography-guided ablation in myopic eyes using
Zyoptix. J Cataract Refract Surg 2004;30:398-402.
31
37. Kymionis GD, Panagopoulou SI, Aslanides IM, Plainis S, Astyrakakis N,
Pallikaris JG. Topographically supported customized ablation for the
management of decentered Laser In Situ Keratomileusis. Am J Ophthalmol
2004;137:806-11.
38. Mertz GW. Overnight swelling of the living human cornea. J Am Optom
Assoc 1980;51:211–14.
39. Kiely PM, Carney LG, Smith G. Diurnal variations of corneal topography
and thickness. Am J Optom Physiol Opt 1982;59:976–982.
40. Harper CL, Boulton ME, Bennett D, et al. Diurnal variations in human
corneal thickness. Br J Ophthalmol 1996;80:1068–72.
41. Feng Y, Varikooty J, Simpson TL. Diurnal variation of corneal and corneal
epithelial thickness measured using optical coherence tomography. Cornea
2001;20:480–83.
42. Du Toit R, Vega JA, Fonn D, et al. Diurnal variation of corneal sensitivity
and thickness. Cornea 2003;22:205–9.
43. Reynolds DR, Poynter HL. Diurnal variation in central corneal curvature.
Am J Optom Arch Am Acad Optom 1970;47:892–99.

32
44. Cronje S, Harris WF. Short-term keratometric variation in the human eye.
Optom Vis Sci 1997;74:420–24.
45. Handa T, Mukuno K, Niida T, et al. Diurnal variation of human corneal
curvature in young adults. J Refract Surg 2002;18:58–62.
46. Read SA, Collins MJ, Carney LGC. The diurnal variation of corneal
topography and aberrations. Cornea 2005;24:678–87.
47. Dubbelman M, Sicam VADP, Van der Heijde GL. The shape of the anterior
and posterior surface of the aging human cornea. Vision Res 2006;46:993-
1001.
48. Sicam VADP, Dubbelman M, van der Heijde RGL. Spherical aberration of
the anterior and posterior surfaces of the human cornea. J Opt Soc Am A
2006;23:544-49.
49. Belin MW, Khachikian SS. Keratoconus: It is hard to define, but. Am J
Ophthalmol 2007;143:500-3

33
50. Kaufmann C, Bachmann LM, Thiel MA. Comparison of dynamic contour
tonometry with goldmann applanation tonometry. Invest Ophthalmol Vis Sci
2004;45:3118-21.
51. Kanngiesser HE, Kniestedt C, Robert YCA. Dynamic contour tonometry.
Presentation of a new tonometer. J Glaucoma 2005;14:344-50.
52. Kotecha A, White ET, Shewry JM, Garway-Heath DF. The relative effects of
corneal thickness and age on Goldmann applanation tonometry and dynamic
contour tonometry. Br J Ophthalmol 2005;89:1572-75.
53. Schneider E, Grehn F. Intraocular pressure measurement – comparison of
dynamic contour tonometry and Goldmann applanation tonometry. J Glaucoma
2006;15:2-6.
54. Carlson KH, Mclaren JW, Topper JE, Brubaker RF. Effect of body position
on intraocular pressure and aqueous flow. Invest Ophthalmol Vis Sci
1987;28:1346-52.
55. Linder BJ, Trick JL, Wolf ML. Altering body position affects intraocular
pressure and visual function. Invest Ophthalmol Vis Sci 1988;29:1492-97.

34
56. Lackner B, Schmidinger G, Pieh S, Funovics MA, Skorpic C. Repeatability
and reproducibility of central corneal thickness measurement with pentacam,
orbscan and ultrasound. Optom Vis Sci 2005;82:892-99.
57. O’Donnell C, Maldona-Codina C. Agreement and repeatability of central
thickness measurement in normal corneas using ultrasound pachymetry and the
oculus pentacam. Cornea 2005;24:920-24.
58. Barkana Y, Gerber Y, Elbaz U et al. Central corneal thickness measurement
with the pentacam scheimpflug system, optical low-coherence reflectometry
pachymeter, and ultrasound pachymetry. J Cataract Refract Surg
2005;31:1729-35.
59. Shankar H, Taranath D, Santhirathelagan CT, Pesudovs K. Anterior
segment biometry with the Pentacam: Comprehensive assessment of
repeatability of automated measurements. J Cataract Refract Surg
2008;34:103-13.
60. Chen D, Lam AKC. Intrasession and intersession repeatability of the
Pentacam system on posterior corneal assessment in the normal human eye. J
Cataract Refract Surg 2007;33:448-54.
35
61. Lackner B, Schmidinger G, Skorpik C. Validity and reliability of anterior
chamber depth measurement with pentacam and orbscan. Optom Vis Sci.
2005;82:858-61.
62. Meinhardt B, Stachs O, Stave J, Beck R, Guthoff R. Evaluation of biometric
methods for measuring the anterior chamber depth in the non-contact mode.
Graefes Arch Clin Exp Ophthalmol 2006:244;559-64.
63. Rabsilber TM, Khoramnia R, Auffarth GU. Anterior chamber measurements
using Pentacam rotating Scheimpflug camera. J Cataract Refract Surg
2006;32:456-59.
64. Hitzenberger CK. Optical measurement of the axial eye length by laser
Doppler interferometry. Invest Ophthalmol Vis Sci 1991;32:616-24.
65. Lam AKC, Chan R, Pang PCK. The repeatability and accuracy of axial
length and anterior chamber depth measurements from the IOLMaster. Ophthal
Physiol Opt 2001;21:477-83.
66. Santodomingo-Rubido J, Mallen EAH, Gilmartin B and Wolffsohn. A new
non-contact optical device for ocular biometry. Br J Ophthalmol 2002;86:458-62.

36
67. Sheng H, Bottjer CA, Bullimore MA. Ocular component measurement using
the Zeiss IOLMaster. Optom Vis Sci 2004;81:27-34.
68. Herse P, Siu A. Short term effects of proparacaine on human corneal
thickness. Acta Ophthalmol 1992;70:740-44.
69. Asensio I, Rahhal SM, Alonso L, Palanc-Sanfrancisco JM, Sanchis-Gimeno
JA. Corneal thickness values before and after oxybuprocaine 0.4% eye drops.
Cornea 2003;22:527-32.
70. Nam SM, Lee HK, Kim EK, Seo KY. Comparison of corneal thickness after
the instillation of topical anesthetics. Proparacaine versus oxybuprocaine.
Cornea 2006;25:51-54.
71. Huang RYC, Lam AKC, Chan R, Young S-M. Should Orbscan pachometry
be performed before or after Goldmann applanation tonometry? Ophthal Physiol
Opt 2005;25:441-45.
72. Lam AKC, Chen D. Effect of proparacaine on central corneal thickness
values. An evaluation using noncontact specular microscopy and Pentacam.
Cornea 2007;26:55-58.
73. Maloney RK, Bogan SJ, Waring III GO. Determination of corneal image-
forming properties from corneal topography. Am J Ophthalmol 1993;115:31-41.

37
74. Thibos LN, Wheeler W, Horner D. Power vectors: An application of fourier
analysis to the description and statistical analysis of refractive error. Optom Vis
Sci 1997;74:367-75.
75. Bland JM, Altman DG. Calculating correlation coefficients with repeated
observations: Part 1 – correlation within subjects. Br Med J 1995;310:446.
76. Read SA, Collins MJ, Iskander DRI. The diurnal variation of axial length,
intraocular pressure and anterior eye biometrics. Invest Ophthalmol Vis Sci.
2008;49:2911-18.
77. Naroo SA, Charman WN. Changes in posterior corneal curvature after
photorefractive keratectomy. J Cataract Refract Surg 2000;26:872-78.
78. Kikkawa Y, Hirayama K. Uneven swelling of the corneal stroma. Invest
Ophthalmol Vis Sci 1970;9:735-41.
79. Friedman MH. A quantitative description of equilibrium and homeostatic
thickness regulation in the in vivo cornea I. The normal cornea. Biophys J.
1972;12:648-64.
38
80. Lee D, Wilson G. Non-uniform swelling properties of the corneal stroma.
Curr Eye Res 1981;8:457-61.
81. Müller LJ, Pels E, Vrensen GFJM. The specific architecture of the anterior
stroma accounts for maintenance of corneal curvature. Br J Ophthalmol 2001;
85:437-43.
82. Bergmanson JPG, Horne J, Doughty MJ, Garcia M, Gondo M. Assessment
of the number of lamellae in the central region of the normal human corneal
stroma at the resolution of the transmission electron microscope. Eye Contact
Lens 2005;31:281-87.
83. Castoro JA, Bettelheim AA, Bettelheim FA. Water gradients across bovine
cornea. Invest Ophthalmol Vis Sci 1988;29:963-68.
84. Lattimore MR, Kaupp S, Schallhorn S, Lewis R. Orbscan pachymetry.
Implications of a repeated measures and diurnal variation analysis. Ophthalmol
1999;106:977-81.
85. Boote C, Dennis S, Newton RH, Puri H, Meek KM. Collagen fibrils appear
more closely packed in the prepupillary cornea: Optical and biomechanical
implications. Invest Ophthalmol Vis Sci 2003;44:2941-48.

39
86. Bonanno JA, Polse KA. Central and peripheral corneal swelling
accompanying soft lens extended wear. Am J Optom Physiol Opt 1985;62:74-
81.
87. Bonanno JA, Polse KA, Goldman MM. Effect of soft lens power on
peripheral corneal edema. Am J Optom Physiol Opt 1986;63:520-26.
88. Erickson P, Comstock TL. An improved technique for patched eye corneal
swelling studies. Int Contact Lens Clin 1995;22:191-97.
89. Erickson P, Comstock TL, Zantos SG. Effects of hydrogel lens
transmissibility profiles on local corneal swelling during eye closure. Optom Vis
Sci 1996;73:169-77.
90. Erickson P, Comstock TL, Doughty MJ, Cullen AP. The cornea swells in the
posterior direction under hydrogel contact lenses. Ophthal Physiol Opt
1999;19:475-80.
91. Moezzi AM, Fonn D, Simpson TL, Sorbara L. Contact lens-induced corneal
swelling and surface changes measured with the Orbscan II corneal topographer.
Optom Vis Sci 2004;81:189-93.
40
92. Holden BA, McNally JJ, Mertz GW, Swarbrick HA. Topographic corneal
oedema. Acta Ophthalmol 1985;63:684–91.
93. Rom ME, Keller WB, Meyer CJ, Meisler DM, Chern KC, Lowder CY, Secis
M. Relationship between corneal edema and topography. CLAO J
1995;21:191-94.
Figures:
Figure 1: a. The mean change in corneal thickness over the 24-hour
measurement period expressed as the average difference from the mean corneal
thickness (repeated measures ANOVA, p<0.0001 for ‘measurement time’).
b. Mean amplitude of change over the 24-hour measurement period for the
different measured regions (1, 2) and segments (N-I) (repeated measures
ANOVA p <0.0001 for corneal region, and p = 0.062 for corneal segment).
Vertical error bars represent the standard error of the mean, horizontal error bars
represent the standard error in the mean time that the measurements were
taken.
41
Figure 2: Pachymetry and anterior and posterior curvature maps illustrating the
difference in corneal parameters between measurement session 1 and
measurement session 5 (immediately after waking) for a subject representative of

42
the group (Subject 5).

43
Figure 3: Change in corneal best fitting sphero-cylinder. Change in best sphere
(M) top, Astigmatism 90/180 (middle) and astigmatism 45/135 (bottom) shown for
both anterior and posterior corneal surfaces. Change in axial power (D) (left) and
change in axial curvature (mm) (right) are both presented to give an indication of
the optical and shape changes occurring in the two corneal surfaces. Vertical
error bars represent the standard error of the mean, horizontal error bars
represent the standard error in the mean time that the measurements were
taken.

44

45
Figure 4: Schematic illustration of the changes found in the cornea and anterior
chamber upon waking. The solid line represents the baseline cornea and
anterior lens surfaces (measurement session 1) and the dashed line represents
these surfaces upon first waking (measurement session 5). This shows a
backward movement of the posterior cornea, and a slight forward movement of
the anterior cornea accompanying the increase in CCT observed upon waking.
Note the diagram is not to scale and is an interpretation of the likely movement of
the relative surfaces based on our experimental data.

46
Tables:
Table 1: Mean and amplitude of diurnal variation of corneal axial power M, J0
and J45 for both the anterior and posterior cornea. Results from repeated
measures ANOVA for the change in each parameter over time also displayed.

47
Corneal
surface
Power
vector
Analysis
diameter
Mean ±
SD (D)
Mean
amplitude
of change
± SD (D)
P-Values repeated measures ANOVA
Time Region Time*
Region
Anterior
M
3.5 mm 48.35
± 1.65
0.36
± 0.11 <0.0001 <0.0001 0.19
7.0 mm 48.17
± 1.66
0.27
± 0.09
J0
3.5 mm 0.25
± 0.19
0.16
± 0.08 0.10 0.18 0.27
7.0 mm 0.28
± 0.19
0.08
± 0.04
J45
3.5 mm -0.015
±0.16
0.12
± 0.05 0.32 0.054 0.23
7.0 mm 0.018
± 0.15
0.07
± 0.03
Posterior
M
3.5 mm -6.19
± 0.26
0.05
± 0.03 <0.0001 0.003 0.75
7.0 mm -6.22
± 0.26
0.04
± 0.02
J0
3.5 mm -0.16
± 0.05
0.05
± 0.02 0.004 0.002 0.3
7.0 mm -0.14
± 0.03
0.03
± 0.01

48
J45
3.5 mm 0.017
± 0.05
0.04
± 0.01 0.75 0.06 0.75
7.0 mm 0.006
± 0.03
0.03
± 0.01
Table 2: Results from analysis of co-variance investigating association between
the change in each of the corneal power vectors for the anterior and posterior
cornea (for a 7 mm analysis diameter) and the other measured ocular
parameters. Note p-values adjusted for multiple comparisons.
Surface Power
Vector
ANCOVA
result
Ocular variable
∆ IOP ∆ OPA ∆ Axial ∆ CCT ∆ ACD

49
length
Anterior
∆ M r
(p)
-0.16
(0.86)
0.19
(0.49)
-0.08
(1.00)
-0.62
(<0.0001)
0.39
(0.003)
∆ J0 r
(p)
-0.08
(1.0)
-0.11
(1.0)
-0.22
(0.32)
0.21
(0.34)
0.08
(1.0)
∆ J45 r
(p)
0.08
(1.0)
-0.01
(1.0)
-0.12
(1.0)
0.42
(0.001)
-0.03
(1.0)
Posterior
∆ M r
(p)
-0.26
(0.12)
0.05
(1.0)
-0.03
(1.0)
0.73
(<0.0001)
0.24
(0.17)
∆ J0 r
(p)
0.23
(0.27)
0.40
(0.002)
-0.13
(1.0)
-0.43
(0.0006)
0.35
(0.01)
∆ J45 r
(p)
-0.11
(1.0)
-0.11
(1.0)
0.21
(0.34)
-0.11
(1.0)
-0.01
(1.0)