r j crossno, md 1 - texas & new mexico hospice...
TRANSCRIPT

Non-Pain Symptom Management March 2012
R J Crossno, MD 1
TXNMHO / TAPM Annual Convention
March 28 2015
• Ronald J Crossno, MD FAAHPM
Chief Medical Officer, Kindred at Home
(formerly Gentiva)
• Disclosures
No relevant financial disclosures
Off-Label indication is entered on slides as “OL”
• Identify common non-pain symptoms
encountered in the hospice setting, including
dyspnea, nausea, anxiety, and fatigue
• Describe the choice of appropriate therapeutic
interventions to address these symptoms
Non-Pain Symptom Management March 2012
R J Crossno, MD 2
• 70-yo female living at home
• Diagnoses
• COPD, CAD, CHF, PVD
• Continued tobacco use
• Functional
• PPS 50% / cognitively intact (with oxygen on)
• Structural
• Dyspnea with any exertion & sometimes at rest rated up to 7 on the Borg scale
• Occasional angina; 2+ pedal edema; BMI = 17; SaO2 = 84% on room air
• Current COPD meds / txs include
• Oxygen @ 2L/m, prn
• Duoneb® treatments every 4h as needed
• Xopenex® neb twice daily
• Advair® 1 inh twice daily
• Serevent® 1 inh twice daily
• Spiriva® 1 inh twice daily
• Combivent® MDI 2 puffs twice daily
• Singulair® daily
• What are your thoughts about these?
• Current cardiac meds
• Digoxin 0.25mg daily
• Lisinopril (Prinivil®) 40mg daily
• Carvedilol (Coreg®)12.5mg twice daily
• Aspirin 325mg twice daily
• Valsartan ER (Diovan®) 160mg daily
• Isosorbide mononitrate (Imdur®) 60mg daily
• Furosemide (Lasix®) 80mg daily
• What are your thoughts about these?

Non-Pain Symptom Management March 2012
R J Crossno, MD 3
• Central & peripheral chemoreceptors
• Some report severe dyspnea despite normal ABGs
• Some patients with severely abnormal ABGs are not burdened by breathlessness
• Mechanical receptors in chest wall & respiratory muscles • Sense airflow obstruction and low lung volumes
• Vagal receptors in the airways & lungs • Sense airflow obstruction and low lung volumes
• Extra-thoracic receptors on the face & in the CNS
• Persistent dyspnea despite maximal medical
management of the underlying disease
• Breathlessness is defined by the patient
• Symptom distress is defined by the patient
• Independent of underlying etiology
• Therapies are general (global), not disease-specific
Abernethy AP, et al BMJ 2003;327(7414):523-528

Non-Pain Symptom Management March 2012
R J Crossno, MD 4
• Focus on identifying and addressing underlying
cause if possible
• Focus on
• What dyspnea means to the resident in relationship to their
underlying illness
• Its effect on activities of daily living
• Concerns regarding possible treatment modalities, such as
opioids or oxygen.
• Focus on psychological and spiritual distress
TOTAL
DYSPNEA Psychological Social
Spiritual
Physical
• Improved sensation of breathlessness
• Based on 9 crossover trials mainly in COPD patients.
• Central and peripheral action
• Relief not related to respiratory rate
• No significant change in O2 sats
• Survival time is unrelated to opioid administration
• Low doses are proven safe
• Higher dose opioids may ↑ mortality risk
• Nebulized opioids are no better than placebo
• No ethical or professional barriers J Pain Symptom Manage 1999;17(4):256-65.
BMJ 2003;327(7414):523-8.
BMJ 2014;348:g445.

Non-Pain Symptom Management March 2012
R J Crossno, MD 5
• Not really effective
• Recent Cochrane review encompassing 200 individuals with advanced cancer or COPD
• no beneficial effect on the relief of dyspnea in patients
• slight, nonsignificant trend toward benefit
• Do ↑ mortality rates!
•Consider as a second-line or third-line treatment for refractory dyspnea associated with anxiety
BMJ 2014;348:g445.
• Potent symbol of medical care
• Expensive
• Fan may do just as well
• RCT of O2 vs room air
• Randomized, double-blind, multicenter trial
• Non-hypoxic residents with life-limiting illness
• Oxygen delivery compared with room air by NC
• No additional symptomatic benefit for relief of refractory
dyspnea
Lancet 2010;376(9743):784–93.
• Fan
• Breathlessness Clinics
• Psychosocial support to alleviate anxiety/distress
• Positioning and pursed lip breathing
• Relaxation techniques
• (e.g. massage, guided imagery)
• Discuss symptom management with family to alleviate
concerns
• (e.g., opioids at low doses do not hasten death)

Non-Pain Symptom Management March 2012
R J Crossno, MD 6
From Dyspnea Review for the Palliative Care Professional: Treatment Goals and Therapeutic Options, J Pall Med, 15(1), 106-114.
• Her medications were reviewed
• Non-beneficial medications were discontinued
• Duplicative medications were eliminated / consolidated
• Meds for symptoms started upon hospice admission
• Morphine 5mg q 4h prn dyspnea was started and titrated as needed
• Oxygen started at 1.5L/m continuously
• Nitroglycerin 0.4mg SL q 5m prn angina, max 3/h
• APAP 650mg every 4h prn minor/musculoskeletal pain
• Non-pharmacologic measures
• Fan in room
• Hospice aides to help with ADLs
• SCC and SW to help assess/counsel regarding anxiety-inducing concerns
• Optimize disease-directed treatments
• Opioids are the mainstay of dyspnea management when other,
definitive treatments are no longer effective
• Oxygen may help for dyspnea associated with hypoxemia
• Non-pharmacologic techniques are always worth trying
• Goals of care must be considered
• Never assume that interventions are always benign
• Sometimes our treatments may hasten death
• Try to anticipate what has a reasonable likelihood of
happening, such as a respiratory crisis with severe pulmonary
disease
• Ensure there is a plan in place to manage such crises

Non-Pain Symptom Management March 2012
R J Crossno, MD 7
• 31-yo M financial consultant
• Diagnoses
• HIV-AIDS, Visceral Kaposi’s sarcoma, wasting syndrome
• Function
• PPS = 40% / FAST = 4
• Structural
• BMI = 17
• c/o pain, currently controlled with oxycodone
• c/o nausea, uncontrolled with meds; last BM 2 days ago with
normal bowel sounds
• Has been unable to take HAART meds due to the
gastrointestinal upset
• Current “GI” meds include
• Promethazine 25mg every 4h prn
• Prochlorperazine 10mg every 6h prn
• Ondansetron 8mg every 4h prn
• Other meds
• Oxycodone ER 80mg every 12h
• Oxycodone conc. 10mg every 2h prn BTP
• Lorazepam 1mg 3x daily and every 4h prn
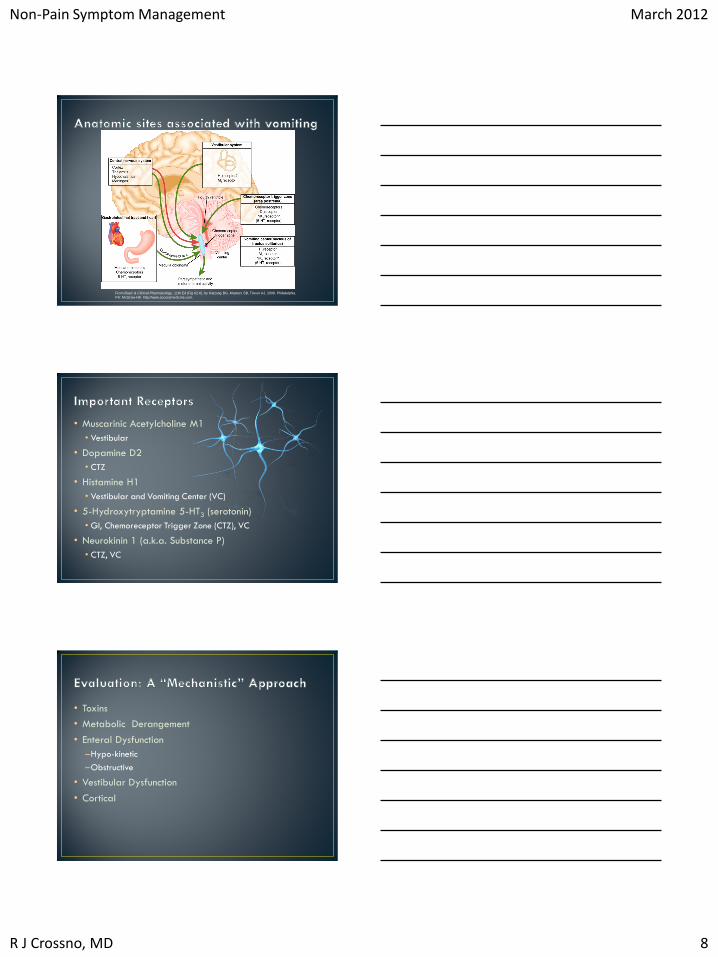
• Key Anatomic Sites
• Important Receptors
• Evaluation
• Management
Non-Pain Symptom Management March 2012
R J Crossno, MD 8
From Basic & Clinical Pharmacology, 11th Ed (Fig 62-6), by Katzung BG, Masters SB, Trevor AJ, 2008, Philadelphia,
PA: McGraw-Hill. http://www.accessmedicine.com.
• Muscarinic Acetylcholine M1
• Vestibular
• Dopamine D2
• CTZ
• Histamine H1
• Vestibular and Vomiting Center (VC)
• 5-Hydroxytryptamine 5-HT3 (serotonin)
• GI, Chemoreceptor Trigger Zone (CTZ), VC
• Neurokinin 1 (a.k.a. Substance P)
• CTZ, VC
• Toxins
• Metabolic Derangement
• Enteral Dysfunction
–Hypo-kinetic
–Obstructive
• Vestibular Dysfunction
• Cortical

Non-Pain Symptom Management March 2012
R J Crossno, MD 9
• Toxins
–Drugs
–Other Exposures
• Metabolic Derangement
–Uremia
–Hepatic Dysfunction
–Hypercalcemia
• Enteric Dysfunction
–Bowel Pattern, Pain
–Change in symptoms with vomiting
–Constipation!
• Vestibular Dysfunction
–Vertigo
• Cortical
–Anxiety
–Focal symptoms, headache etc.
• Vitals and Volume Status
• Abdominal Exam
–Distention
–Hyper or Hypo-active bowel sounds
–Abnormal Masses, Ascites etc.
–Tenderness
• Neurologic Exam
• Rectal Exam (!!!)

Non-Pain Symptom Management March 2012
R J Crossno, MD 10
• Renal Function
• Liver Function Tests
• Calcium
• Obstruction Series
• MRI or CT of Brain
*Appropriate to Goals and Patient’s Condition
Etiology Management
Vestibular H1 or M1 blockade
CNS Disease Corticosteroids
Constipation Stimulant laxative
Impaired GI motility Prokinetic agent
Anxiety Anxiolytics
Post-chemo 5-HT3 or NK-1 blockade
General D2 blockade
• Vestibular (H1 or M1 Blockade)
• MeclizineOL 25 to 50 mg PO TID
• Scopolamine via Patch, IV or SC
• CNS Disease
• Dexamethasone 8 to 16 mg PO, IV, SC
• Constipation
• Senna 2 tabs PO one to three times/day
• Methylnaltrexone 8 to 12 mg SC QOD for refractory cases
• Impaired GI motility (Prokinetic Agents)
• Metoclopramide 10 mg PO/IV AC TID + HS

Non-Pain Symptom Management March 2012
R J Crossno, MD 11
•Anxiety (Anxiolytics)
• LorazepamOL 0.5 to 2 mg PO/IV Q 4-6 hours
• Post Chemo (5-HT3 and NK1)
• Ondansetron - variable dosing (4 to 32 mg)
• Granisetron 1 mg PO Q 12 hours
• Aprepitant 125mg day 1, then 80 mg day 2, 3
•General (D2 Blockade)
• HaloperidolOL 0.5 to 1 mg PO, IV, SC
• Prochlorperazine 5 to 10 mg PO QID or 25 mg PR BID
• Frequent, small feedings
• Remove foods with unpleasant smells or visual
appearance
• Serve meals in pleasant, comfortable surroundings
• Consider “alternative” therapies
• Guided imagery has the most data showing efficacy
• He is admitted to hospice
• Exam fails to reveal acute findings other than some
constipation and general nausea
• Routine meds are started to help manage nausea
• Senna 2 po BID
• Haloperidol 1mg po BID
• Ondansetron is continued for prn usage
• These medications plus guided imagery are effective
for nausea management

Non-Pain Symptom Management March 2012
R J Crossno, MD 12
• Always rule-out impaction as a cause for nausea
• Be familiar with etiologies of nausea and use of
various medications to cover different neuroreceptors
involved in mediating nausea
• Combining meds that block other involved receptors may be
needed
• Nonpharmacologic treatments may be helpful
• Topical gels for nausea are no more effective than
placebo
• There are virtually no detectable blood levels of these drugs
when administered topically
• 65-yo F former housekeeper living with her daughter
• Diagnosis
• ASHD, CHF
• Ongoing tobacco use
• Drinks 2 glasses of wine daily
• Functional
• PPS 50% / cognitively intact
• Structural
• BMI 35; NYHA IV
• At hospice admission, she c/o anxiety “all the time”
• Besides being on appropriate cardiac meds, she is
taking
• Morphine for refractory pain is effective
• Lorazepam (Ativan®) 0.5mg TID routinely for anxiety
• What else do you need to know?
• What would you consider suggesting for management?

Non-Pain Symptom Management March 2012
R J Crossno, MD 13
• Most common anxiety-related diagnoses
• Generalized Anxiety Disorder (GAD)
• Anxiety Secondary to a Medical Condition
• Medications that can cause or exacerbate anxiety
• Caffeine
• Steroids
• Nicotine
• Antidepressants, antipsychotics, stimulants
• Phenylephrine (Sudafed)
• Synthroid over-replacement
• Symptoms are common and distressing
• Significant anxiety symptoms 25-70%
• Subsyndromal PTSD 20-80%
• Often presents with somatic symptoms
• Tension or restlessness
• Jitteriness or autonomic hyperactivity
• Hypervigilance
• Insomnia
• Distractibility
• Worry, apprehension, rumination
• Shortness of breath
• Need to evaluate carefully for medical causes such as pain and
dyspnea
• Often looks like GAD but can include panic attacks
• Actual underlying anxiety disorder
• Fear of death and the dying process
• Spiritual or existential concerns
• Chronic coping or personality style
• Medication side effects (akathisia from anti-emetics)
• Undertreated symptoms (pain, dyspnea, sepsis)
• Withdrawal states (sedatives, opioids)
• Delirium
• Anticipatory response to repeated aversive treatment (chemo)

Non-Pain Symptom Management March 2012
R J Crossno, MD 14
• Explore fears/concerns in non-judgmental fashion
• Listen, acknowledge, normalize, remain available
• Reassurance not usually effective
• Can make highly anxious pts more anxious
• Supportive-expressive therapy
• Aims to reduce symptoms & maintain coping (not cure)
• Consider psychiatric referral
• Music Therapy
• Relaxation/ Guided Imagery/ Hypnosis
• Mindfulness Based Stress Reduction (MBSR)
• Psychotherapy
• Cognitive behavioral therapy
• Interpersonal therapy (IPT) grief work
Antidepressants if life expectancy >8 weeks • SSRI’s
• Sertraline (Zoloft®) 25-200 mg qd
• CitalopramOL (Celexa®) 10-40 mg qd
• Escitalopram (Lexapro®) 5-20mg qd
• MirtazapineOL (Remeron®) • Also helps with sleep and appetite
• Antidepressants to avoid • Paroxetine (Paxil®): anti-cholinergic and withdrawal
• Venlafaxine (Effexor®): withdrawal
• Bupropion (Wellbutrin®): seizure risk
• Start low and go slow to avoid increasing anxiety
Non-Pain Symptom Management March 2012
R J Crossno, MD 15
• Benzodiazepines: drugs of choice at EOL • Lorazepam (Ativan®) 0.5-2 mg q4-6hrs prn
• Alprazolam (Xanax®) 0.25-0.5 mg q4-6hrs prn
• Clonazepam (Klonopin®) for long-acting coverage
• Can cause sedation, confusion, tolerance, abuse, disinhibition, gait instability, falls, and increased risk of death
• TrazodoneOL • Sedating but can be given in low doses during the day
(12.5-50 mg q4hrs prn)
• Buspirone (BuSpar®)
• Should be scheduled, takes at least 4-6 weeks to see an effect
(7.5-10 mg BID-TID)
Consider antipsychotics •More sedating • ChlorpromazineOL (Thorazine) 12.5-50 mg q4hrs prn
• OlanzapineOL (Zyprexa) 2.5-5 mg q 4hrs prn
• QuetiapineOL (Seroquel) 12.5-50 mg q4hrs prn
• Less sedating • HaloperidolOL (Haldol) 0.5-2 mg q4hrs prn
• RisperidoneOL (Risperdal) 0.25-1 mg q4hrs prn
• Already on a benzodiazepine
• Sertraline 50mg daily is prescribed
• Encourage moderation of alcohol & tobacco intake
• Educate about
• Interactions between benzodiazepines and alcohol
• Adverse effects of alcohol and tobacco on anxiety
• Involve rest of IDG to offer possible non-pharmacological interventions
• Over the next 3 weeks, anxiety levels greatly improve
Non-Pain Symptom Management March 2012
R J Crossno, MD 16
• Anxiety is a distressing symptom
• Benzodiazepines remains the drug of choice in EOL
care
• But management involves more than just benzodiazepines
• SSRIs are very effective in managing anxiety if sufficient time
for them to work
• Always consider
• Other modifiable causes of anxiety
• Offering non-pharmacological management
• 61 yo F librarian
• Diagnoses
• Breast cancer – originally dx 8 yr ago
• Recurrent now with multiple bone mets
• Functional
• PPS 60% / cognitively intact
• Structural
• Several bone mets with pain better now, controlled with opioids and recent radiation therapy
• BMI 24, working 2 ½-days a week
• Oncologist referred to hospice
• One month after hospice admission, the patient begins to complain of increasing fatigue
• She wants to know what she can do for this
• She’s been reading about various things on the internet
• What do you recommend to her

Non-Pain Symptom Management March 2012
R J Crossno, MD 17
• Most common symptom in palliative care patients with
cancer or other serious and/or life-threatening illness
• Definition
• Cancer-related fatigue is an
unusual, persistent, subjective
sense of tiredness related to
cancer or cancer treatment,
despite adequate rest, that
interferes with usual functioning
NCCN Guidelines
• Multiple scales for research use
• None in common practical use except linear analog
scale
• Cut off for clinically significant fatigue
• No clearly defined demarcation
• Most suggest > 4 or 5 on a 1-10 scale

Non-Pain Symptom Management March 2012
R J Crossno, MD 18
• Considered a multidimensional syndrome, often with
multiple contributors, including
• Severity of psychological Sx’s (e.g. anxiety / depression)
• Pain
• Sleep disturbances
• Dyspnea
• Anorexia
• Anemia
• Opioid use
• Various neuromodulators (cytokine dysregulation, HPA
dysregulation, autonomic failure, drug interactions)
• Anemia – transfusions and erythropoetic agents
• Deconditioning – exercise
• Depression – antidepressants
• Infections – antibiotics
• Dehydration – fluids
• Hypoxemia – oxygen therapy
• Insomnia – sleep hygiene
• Pain – pain management (e.g. opioids)
• Metabolic / endocrine disorders – correct problem
• CorticosteroidsOL
• Megestrol acetateOL
• ThalidomideOL
• MethylphenidateOL
• ModafinilOL
• MelatoninOL
• L-carnitineOL
• Counseling
• Physical and occupational therapy
Non-Pain Symptom Management March 2012
R J Crossno, MD 19
• Optimal dose and duration: unknown
• Mechanism: multiple proposed, but unknown
• Duration of benefit: unknown
• Still recommended as first-line if no contraindications
• Suggested dose: dexamethasone 8mg/d x 2 weeks
• Opioid-induced sedation
• Level 1 evidence for use in this
• Depression
• Hypoactive delirium
• Fatigue
• Some evidence for benefit and some showing no benefit
• Dose unclear, but suggest starting methylphenidate 5mg
morning, then add 5mg mid-day
• Also – no benefit with paroxetine or donepezil
• Evidence in literature for efficacy in managing CRF:
• Cognitive behavioral therapy
• Education
• Stress management groups
• Coping strategies training
• Availability may be limited for hospice patients with
advanced disease
• Counseling of family to better understand what is
happening also shown to have benefit

Non-Pain Symptom Management March 2012
R J Crossno, MD 20
• She and her family are educated regarding Cancer Related
Fatigue (CRF)
• She is started dexamethasone 8mg q am
• Sleep hygiene techniques are reviewed
• Zolpidem 5mg at bedtime, if unable to fall asleep within 20 minutes, is
made available if needed
• She declines other psychological interventions at this time
• Fatigue is a very common symptoms
• May cause distress for our patients
• Education remains a mainstay of management
• Pharmacologic interventions have limited efficacy, but
end up often being tried
• Know the facts regarding pharmacologic efficacy