raltegravir - technische universität darmstadt
TRANSCRIPT

RALTEGRAVIR
P. Völker, L. von Haza, C. Wöntz & D. Zakharchuk
DaMocles June 2020

Table of contents: 1. Introduction .......................................................................................................... 2
2. Physical properties ............................................................................................. 3
3. Synthesis ................................................................................................................. 5
3.1 General synthesis ..................................................................................................... 5
4. Pharmacology ....................................................................................................... 7
4.1 Pharmacodynamics .................................................................................................. 7
Integrase: ................................................................................................................................................ 7 Mechanism of Action: ........................................................................................................................ 10
4.2 Pharmacokinetics ................................................................................................... 12
Absorption: ............................................................................................................................................ 12 Food impact: ......................................................................................................................................... 12
Gender, age and ethnic groups: ................................................................................................... 13 Young people and kids: .................................................................................................................... 13
BMI: ......................................................................................................................................................... 14 Use during pregnancy and breastfeeding: ................................................................................ 16
Safety: .................................................................................................................................................... 17 Safety in coinfected patients: hepatitis and tuberculosis: .................................................. 17 Tolerability: ........................................................................................................................................... 18
Table of figures: ...................................................................................................... 20
Sources: ...................................................................................................................... 21

2
1. Introduction
This article will give you an overview about the integrase inhibitor
Raltegravir, the antiviral agent in the medication called Isentress®.
The inhibitor targets the viral integrase, the HIV-1 enzyme that is
responsible for the integration of the viral cDNA into the host cells genome
and therefore the virus replication. In combination with other antiviral
agents Raltegravir can limit the amount of HIV virus load and at the same
time increase the number of CD4-(T)-cells, which are a type of white
blood cells that have an important share in maintaining a healthy immune
system as well as the fight against infections. Compared to other antiviral
agents that are used in a highly active antiretroviral therapy Raltegravir
has a bigger impact on multi resistant viruses.
It is the antiviral agent in the medication Isentress that is produced by
Merck & Co, used to treat the HIV infection. It was approved by the U.S.
Food and Drug Administration (FDA) in 2007 and Switzerland in 2008 as
the first integrase inhibitor. In 2008 it received the “14. PZ-
Innovationspreis”. [2]
3
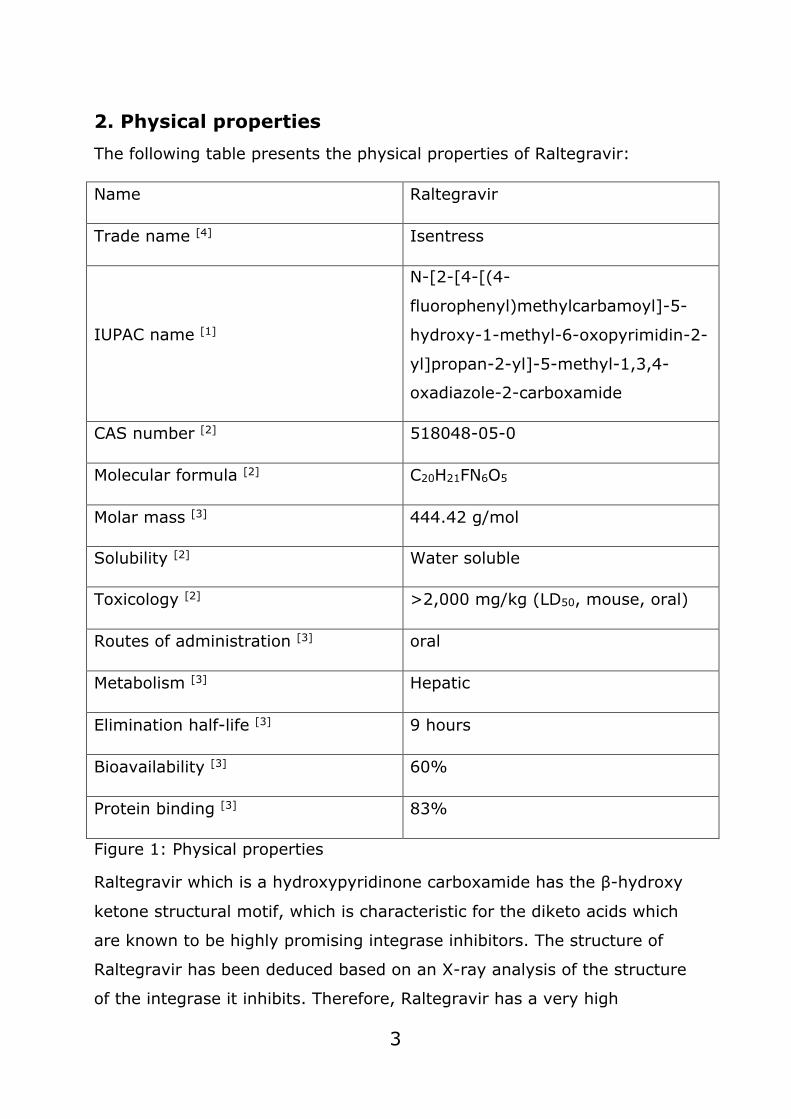
2. Physical properties The following table presents the physical properties of Raltegravir:
Name Raltegravir
Trade name [4] Isentress
IUPAC name [1]
N-[2-[4-[(4-
fluorophenyl)methylcarbamoyl]-5-
hydroxy-1-methyl-6-oxopyrimidin-2-
yl]propan-2-yl]-5-methyl-1,3,4-
oxadiazole-2-carboxamide
CAS number [2] 518048-05-0
Molecular formula [2] C20H21FN6O5
Molar mass [3] 444.42 g/mol
Solubility [2] Water soluble
Toxicology [2] >2,000 mg/kg (LD50, mouse, oral)
Routes of administration [3] oral
Metabolism [3] Hepatic
Elimination half-life [3] 9 hours
Bioavailability [3] 60%
Protein binding [3] 83%
Figure 1: Physical properties
Raltegravir which is a hydroxypyridinone carboxamide has the β-hydroxy
ketone structural motif, which is characteristic for the diketo acids which
are known to be highly promising integrase inhibitors. The structure of
Raltegravir has been deduced based on an X-ray analysis of the structure
of the integrase it inhibits. Therefore, Raltegravir has a very high

4
specificity and affinity to the viral integrase molecule. It is one of the first
pharmaceuticals this technique has ever been used on and the first
molecule of its class of drugs. This accounts for a very complex structure
and synthesis, which is shown in the following pages. [5]
The following figures show models of the structure of Raltegravir:
Figure 2: 2D-Structure of Raltegravir
Figure 3: 3D-Structure of Raltegravir

5
3. Synthesis The active compound of INSENTRESS is the potassium salt of Raltegravir.
The general synthetic route of Raltegravir Potassium is shown in the
following.
3.1 General synthesis The antiviral drug can be synthesized within few steps beginning with
Strecker reaction of acetone cyanohydrin (34.1,181) to amino nitrile
(34.1.182). Next is to convert aminonitrile into the N-Cbz
(carboxybenzyl)-protected intermediate (34.1.183) by using benzyl
chloroformate in sodium carbonate water solution. The transformation of
the obtained intermediate (34.1.183) to amidoxime (34.1.184) can be
achieved by adding hydroxylamine hydrochloride in methanol.
Figure 4: Synthesis 1
The amidoxime is then treated with dimethylacetylenedicarboxylate
(34.1.185) in chloroform. The obtained product (34.1.186) is put into
toluene and is heated at 145°C to cyclize to pyrimidine-4-
carboxylate (34.1.187).
Figure 5: Synthesis 2
The compound (34.1.187) is then benzoylated with benzoyl chloride in
pyridine. By N-methylathing the Product (34.1.188) with dimethyl sulfate
in dioxane using lithium as a base the compound (34.1.189) can be
obtained. The N-Cbz-deprotected product (34.1.190) can be achieved
due to hydrogenation.

6
Figure 6: Synthesis 3
(34.1.190) is treated with 5-methyl-1,3,4- oxadiazole-2-carbonyl chloride
(34.1.191) in the presence of triethylamine in dichloromethane. Refluxing
the product (33.1.192) with p-fluorobenzyl amine in methanol leads to
Raltegravir (34.1.178). [27]
Figure 7: Synthesis 4
The potassium salt of Raltegravir can be finally achieved by treating
Raltegravir with potassium hydroxide in ethanol at 25°C for 1.5 hours.
[28]
Figure 8: Synthesis 5
Furthermore, there are other synthesis routes providing more efficiency
for industrial manufacturing. [27]

7
4. Pharmacology
4.1 Pharmacodynamics Integrase is a HIV-1 explicit enzyme which catalyses the inclusion of a
DNA duplicate of the viral genome into the genome of host cells. The use
of Raltegravir results in the limitation of the reproduction of the virus and
thus stops further spread of the infection.
Integrase:
Integrase is an HIV-1 specific enzyme, which is one of the three enzymes
that are involved in viral replication.
It is structurally organized into three domains that are independent from
each other:
(i) the N-terminal region that carries a motif similar to a zinc finger and is
able to bind Zn2+ or other divalent metals like magnesium. This possibly
favours protein multimerization which is a necessity in the integration
process.
(ii) the main region also known as the catalytic region that contains a D,
D-35, E motif which is needed for the enzymes catalytic activity. This
region is also involved in the binding of the viral DNA extremities. These
activities require that a metallic cation cofactor like magnesium or zinc is
present to coordinate it.
(iii) the C-terminal region is able to bind to DNA without a requirement
which predetermines its involvement in ensuring the stability of the
complex with the DNA. [25]
Its main function is to catalyse the integration of viral cDNA ends (which
have been generated by reverse transcription of the viral RNA genome
before) into the host cells genome, marking the last necessary step before
the virus is able to reproduce.

8
The integration of the viral cDNA into the host genome consists of two
consecutive steps: the 3’-processing and the strand transfer.
In order to start the integration process, it is absolutely necessary to have
a complex of viral DNA and the integrase enzyme which has to be formed
beforehand. This complex formation is possible because the HIV integrase
recognizes specific sequences in the LTRs (long terminal repetition) of
viral DNA and binds to them.
At the actual beginning of the integration process the 3’processing takes
place. During this process of the integration two nucleotides are
eliminated from each 3’-end of the double helical viral DNA. Afterwards
the empty slots at the 3’-ends are filled with an OH-substituent each.
Figure 9: The two integrase catalytic reactions
9
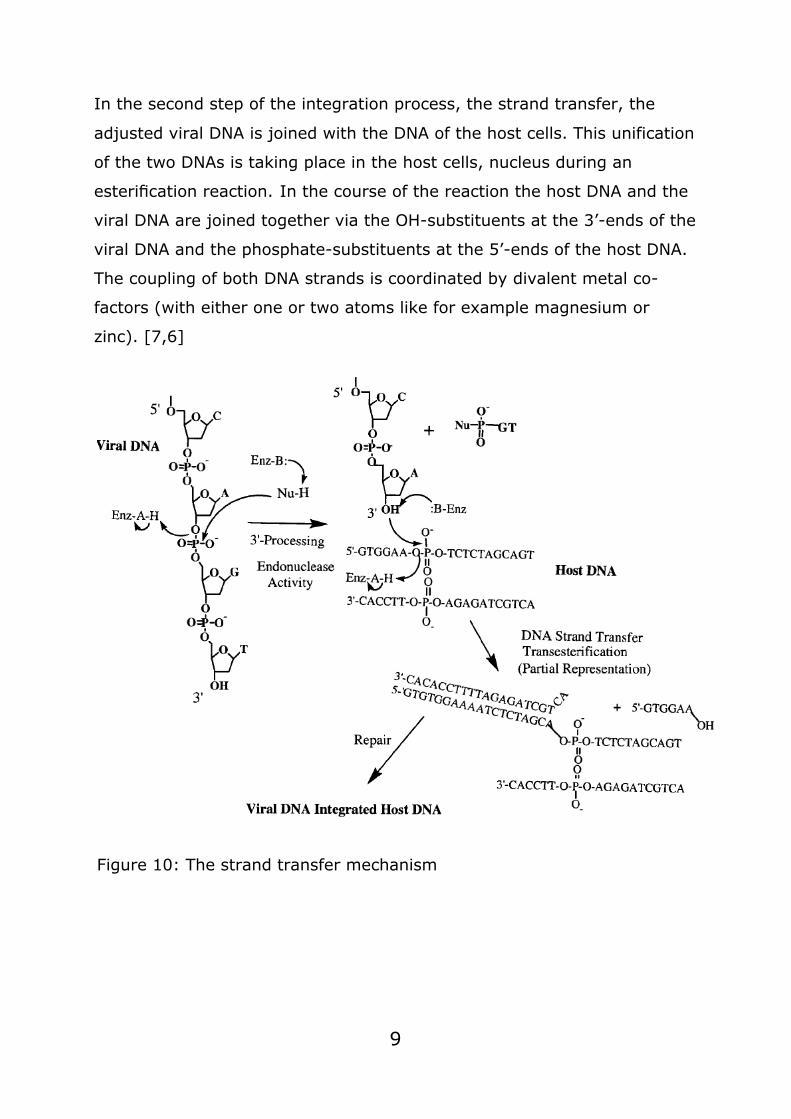
In the second step of the integration process, the strand transfer, the
adjusted viral DNA is joined with the DNA of the host cells. This unification
of the two DNAs is taking place in the host cells, nucleus during an
esterification reaction. In the course of the reaction the host DNA and the
viral DNA are joined together via the OH-substituents at the 3’-ends of the
viral DNA and the phosphate-substituents at the 5’-ends of the host DNA.
The coupling of both DNA strands is coordinated by divalent metal co-
factors (with either one or two atoms like for example magnesium or
zinc). [7,6]
Figure 10: The strand transfer mechanism

10
Mechanism of Action:
The integrase inhibitor Raltegravir that is also referred to as a strand
inhibitor because it interferes with the second step of the viral cDNA
integration reaction the strand transfer, the transfer of the viral DNA into
the host cells DNA, without having an effect on the first step of the
integration process the 3’-processing. [9]
It is able to block the transfer of a strand of viral DNA into the host cells
DNA strand by binding at the active sites of the intermediate product of
the first step of the integration reaction the PIC (pre-integration complex).
This pre-integration complex is a ternary complex made up by the HIV-1
integrase, a metallic cation cofactor (a divalent metal like magnesium or
zinc) and the viral cDNA.
The integrase inhibitor binds to the active site of the ternary complex by
chelating the divalent metallic cationic co-factors in the integrase active
site. This is interfering with the usual insertion of linear HIV-1 DNA into
the targeted host cells genome because the metallic cation co-factors that
are supposed to coordinate the second step of the integration process the
strand transfer are disabled and therefore the coupling of both DNA
strands is not taking place. [25]
11
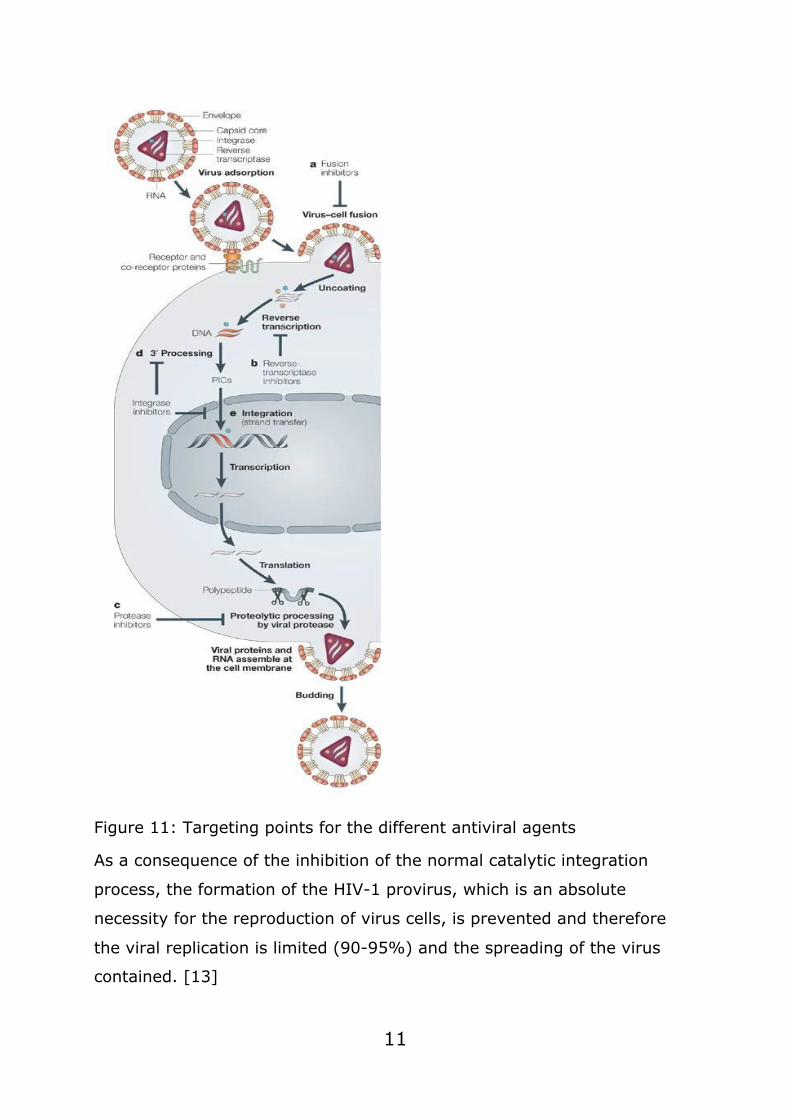
Figure 11: Targeting points for the different antiviral agents
As a consequence of the inhibition of the normal catalytic integration
process, the formation of the HIV-1 provirus, which is an absolute
necessity for the reproduction of virus cells, is prevented and therefore
the viral replication is limited (90-95%) and the spreading of the virus
contained. [13]

12
4.2 Pharmacokinetics
Absorption:
Raltegravir is quickly assimilated in the wake of taking the medication on
an empty stomach, the greatest fixation (StAX) in the blood plasma is
resolved after approximately 3 hours.
The area under the concentration - the time curve (AUC) and the STAC
value increase proportionally to the dose which can range from 100 to
1600 mg. By taking the drug 2 times a day, the equilibrium state is
reached quickly, approximately within 2 days after the start of the
treatment. The values of AUC and Cmax are speaking in favour of a
minimal accumulation of the drug.
The absolute bioavailability of Raltegravir has not been established.
Food impact:
Raltegravir can be taken regardless of mealtime. [29]
The impact of food on the pharmacokinetics of raltegravir is a little difficult
to understand. The AUC of raltegravir relative to fasting, decreased with a
low-fat meal (-46%) and it did not significantly change with a moderate-
fat meal (+13%) and increased twofold with a high-fat meal. (Raltegravir
(RAL) Dose Proportionality and Effect of Food)
In all analysed cases, food seemed to increment an intra-subject
changeability in pharmacokinetic parameters when contrasted with
fasting. It is suggested that raltegravir be taken with or without food
because of the perception that these distinctions in the introduction to
Raltegravir were not related to either decreased antiviral movement or
expanded occurrence of unfavourable occasions.
Approximately 83% of Raltegravir binds to plasma proteins in the
concentration range from 2 to 10 mmol.

13
Raltegravir effectively defeated the placental boundary in test
concentrates on rodents, however, it didn't enter the blood-cerebrum
obstruction. [29]
The terminal elimination half-life of Raltegravir is 9 h, with a shorter a-
phase half-life of ~ 1 h which determines most of the AUC. Raltegravir is
glucuronidated to Raltegravir-glucuronide by the UDP-
glucuronosyltransferase 1A1 (UGT1A1) enzyme. [30]
Following the administration of an oral dose, 51% is excreted in feces in
the form of Raltegravir; most likely, the glucuronide metabolite is
hydrolyzed by glucuronidases in the intestinal tract. A small percentage of
the dose, 32%, is excreted in the urine; only a small part, 9% of the dose,
is excreted in the urine as unchanged Raltegravir, the remaining 24% is
the glucuronide metabolite. [31]
Gender, age and ethnic groups:
Gender has no proved clinically significant effect on the pharmacokinetic
parameters of Raltegravir. In studies on patients older than 18 years of
age, no significant dependence of pharmacokinetic parameters on age was
found. Therefore, a correction of the drug dose depending is not required.
[34,35]
Young people and kids:
As indicated in the report of after-effects in sound grown-up volunteers,
the chewable tablet has a higher oral bioavailability in contrast to the pill
with film-coating, 400 mg each. Taking the chewable tablets with food
with a high fat content has no clinically noteworthy impact on the
pharmacokinetics of Raltegravir. The medication dosage for teenagers and
youngsters over 2 years of age for the treatment of HIV-1 contamination
is prescribed according to the pharmacokinetic parameters of raltegravir,
which is practically identical to that of grown-up patients taking the
medication two times per day. [29,36]
14
BMI:
Modifications in body weight can influence the sedate disposition by
changing the volume of dispersion of the medication. In a
pharmacokinetic examination, in which weight file (BMI) was treated as a
continuous variable, there was no clinically important impact of BMI on
Raltegravir pharmacokinetics. [33]
Patients with renal and hepatic insufficiency:
Renal clearance accounts for a small proportion of the elimination of
Raltegravir from the system. The pharmacokinetics of the drug was
studied on adult patients with a severe degree of renal failure as well as in
a complex pharmacokinetic analysis. [29,34]
Clinically significant discrepancy of pharmacokinetic parameters in
patients with severe renal failure compared to healthy volunteers is not
detected. Raltegravir is dispensed principally by glucuronidation in the
liver. An investigation of the pharmacokinetics of Raltegravir was
conducted on patients with a moderate hepatic inadequacy and matched
healthy control subjects. [34]
The impact of gentle hepatic inadequacy was not assessed in this
investigation, yet given the clinically unimportant outcomes for moderate
hepatic deficiency patients, an absence of clinically significant impact for
mellow inadequacy can be surmised from the data. There were no
clinically significant pharmacokinetic contrasts between patients with
moderate hepatic inadequacy and clinically unremarkable subjects. [33]
Thus, a correction of the drug dose in patients with severe kidney failure
and hepatic insufficiency is not required. [29,34]

15
Figure 12: Arithmetic mean Raltegravir plasma concentration profiles
following administration of a 400-mg single dose to subjects with hepatic
impairment, subjects with renal impairment, and corresponding matched
control subjects with normal hepatic and renal function
Patients with UDPGT polymorphism:
Polymorphisms in drug-metabolizing enzymes may have the
accompanying results: increment or lessening of the successful portion,
stretching or shortening of the length of helpful impact, ADEs, tranquilize
harmfulness and medication sedate communications.
Within this class, UGT1A1 is the specific enzyme that catalyses the
conjugation of bilirubin. On account of antiretroviral operators, various
polymorphisms have been concentrated to affirm their relationship with
hyperbilirubinemia, a condition present in a consider-capable level of
patients treated with ATV or IDV.
16
The results of these studies show that the polymorphism most closely
related with hyperbilirubinemia is UGT1A1*28, which reduces the activity
of the enzyme in individuals who are homozygotes for the rare allele.
These individuals were not excluded from the Raltegravir-development-
program, and they contributed to the robustness of the safety profile for
Raltegravir, further supporting the hypothesis that a substantial reduction
of UGT1A1 activity does not result in a clinically meaningful effect.
Recently, genetic polymorphisms of the iso-enzyme UGT2B7 have also
been studied. This enzyme has been observed to be the principal enzyme
involved in the N-glucuronidation of EFV. The exact incidence of Gilbert’s
syndrome among participants in Raltegravir clinical studies is not known.
[34,37]
Use during pregnancy and breastfeeding:
Controlled studies about the effects of the drug on pregnant women have
not been conducted, so the drug is contraindicated to use during
pregnancy.
There are no data on the intake of Raltegravir in human breast milk.
However, the intake of Raltegravir was detected when the drug was
introduced into milk in rats: when the drug was administered at a daily
dose of 600 mg/kg, the concentration of Raltegravir in milk exceeded the
plasma concentration by about 3 times.
Breastfeeding is not recommended for HIV-infected mothers in order to
avoid transmission of HIV infection to children.
If it is need to use the drug during lactation, it is recommended to stop
breastfeeding. [29]

17
Safety:
Taken together all studies suggest that Raltegravir is well tolerated with
serious drug-related adverse event (SAE) rates that were either similar or
lower than observed in the comparator arms (i.e., placebo in salvage
regimens of efavirenz in treatment-naive patients). For instance, in the
largest study of treatment-experienced patients, 2.8% of the patients on
Raltegravir + OBR reported a drug-related SAE versus 3.8% of the
patients on placebo + OBR.
There has been some concern about the development of cancer in
treatment-experienced patients on Raltegravir. Initially, a trend appeared
to be visible of an increased incidence of cancer but prolonged follow-up
of these patients did not show any differences versus placebo. Also, in
treatment-naive patients comparing Raltegravir with efavirenz, no
difference was noted. [32]
Safety in coinfected patients: hepatitis and tuberculosis:
Other than every so often expanding alanine aminotransferase (ALT) and
aspartate aminotransferase (AST), no extraordinary hepatotoxicity was
seen in clinical preliminaries. Although under-represented, hepatitis B
and/or C patients were included and had similar rates of virologic efficacy
than monoinfected in the study. [38]
Observational studies show that coinfected patients are more likely to
have baseline liver enzyme alterations and to present subsequent
increases after Raltegravir introduction, irrespective of severity and mostly
appearing early after treatment initiation. However, severe abnormalities
are globally rare and hardly warrant. [39]
The REFLATE study has demonstrated that Raltegravir 400 mg or 800 g
twice day by day can be utilized in patients co-tainted with HIV and
tuberculosis albeit still isn't totally clear which is the favoured dosing. In

18
REFLATE multiplying the portion of Raltegravir overcompensated the
impact of rifampicin acceptance. Be that as it may, the standard portion
had just little reductions in AUC0-12 and C12. [40]
Tolerability:
The resistance to the drug has not been fully studied. Despite this, there
is a study that confirms that the presence of mutations in the genes of
patients affects the tolerance and resistance to Raltegravir. According to
the study most mutations occur in genes Q148K, T97A, Y143C and Y143H.
While essential changes were uncommon, baseline secondary mutations
were more common in the two groups of patients. As with primary
mutations, more secondary mutations were found in the treatment failure
group than in the treatment success group.
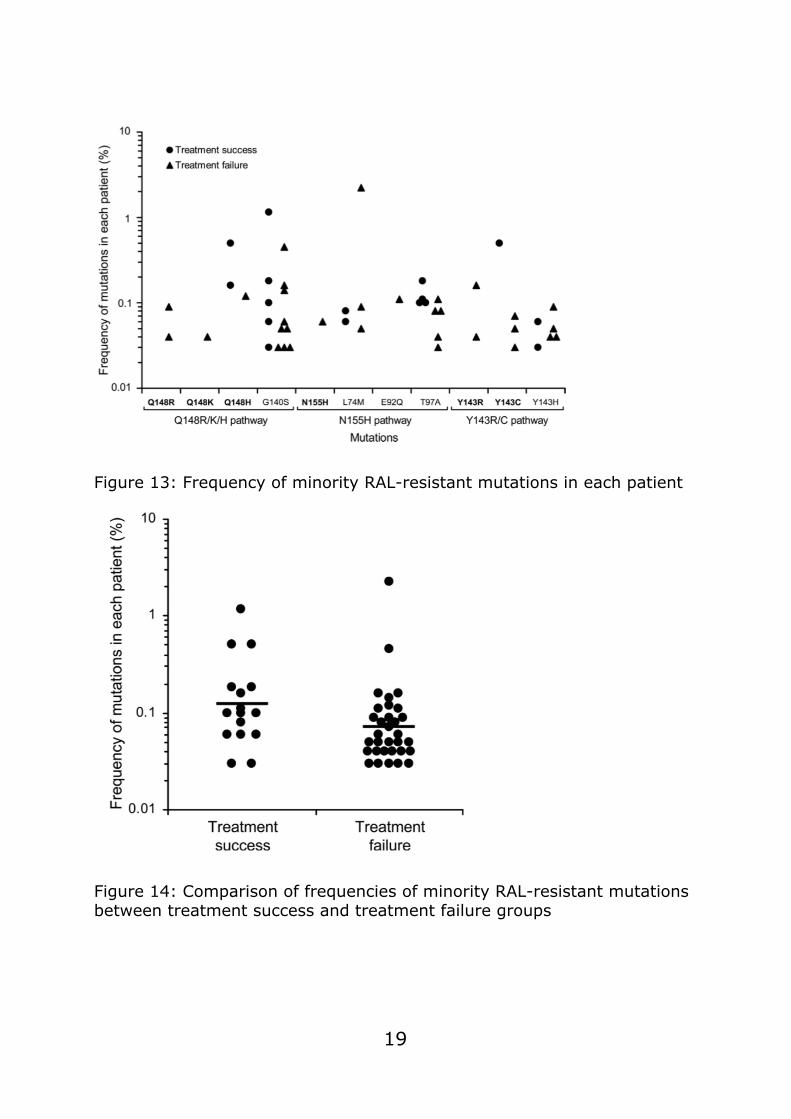
The level of each Raltegravir-safe transformation was determined by PASS
in every patient. Each symbol represents the percentage of one mutation
occurring in either treatment success (circles) or treatment failure
(triangles) patients.
All detected mutations were present at very low frequencies (<1%),
except of two secondary mutations in two patients (2.2% for L74M and
1.1% for G140S) (Fig. 14). There were no in frequencies of primary
mutations between the treatments (Fig. 15). Every single mutation was
present at extremely low frequencies (<1%). There were no significant
differences in the frequencies of minority mutations in the treatment
success groups compared to the treatment failure groups. [41]
19
Figure 13: Frequency of minority RAL-resistant mutations in each patient
Figure 14: Comparison of frequencies of minority RAL-resistant mutations between treatment success and treatment failure groups
20
Table of figures: Figure 1: Physical properties .............................................................. 3
Figure 2: 2D-Structure of Raltegravir .................................................. 4
Figure 3: 3D-Structure of Raltegravir .................................................. 4
Figure 4: Synthesis 1 ........................................................................ 5
Figure 5: Synthesis 2 ........................................................................ 5
Figure 6: Synthesis 3 ........................................................................ 6
Figure 7: Synthesis 4 ........................................................................ 6
Figure 8: Synthesis 5 ........................................................................ 6
Figure 9: The two integrase catalytic reactions ..................................... 8
Figure 10: The strand transfer mechanism ........................................... 9
Figure 11: Targeting points for the different antiviral agents ................ 11
Figure 12: Arithmetic mean Raltegravir plasma concentration profiles
following administration of a 400-mg single dose to subjects with hepatic
impairment, subjects with renal impairment, and corresponding matched
control subjects with normal hepatic and renal function ....................... 15
Figure 13: Frequency of minority RAL-resistant mutations in each patient
................................................................................................... 19
Figure 14: Comparison of frequencies of minority RAL-resistant mutations
between treatment success and treatment failure groups ..................... 19
21
Sources: [1] https://pubchem.ncbi.nlm.nih.gov/compound/Raltegravir#section=Me
SH-Entry-Terms (10.05.20)
[2] https://de.wikipedia.org/wiki/Raltegravir (10.05.20)
[3] https://en.wikipedia.org/wiki/Raltegravir (10.05.20)
[4] https://www.msd.de/fileadmin/files/fachinformationen/isentress.pdf
(10.05.20)
[5] Yong-Jin Wu, Progress in Heterocyclic Chemistry, 2012
[6] https://onlinelibrary.wiley.com/doi/epdf/10.1002/rmv.350
(10.05.2020)
[7] https://academic.oup.com/cid/article/48/7/931/326321 (11.05.2020)
[8] https://science.sciencemag.org/content/287/5453/646?casa_token=G
pWv0MyADnkAAAAA:2FwJl3xZ2t116PU1YF6bjGl0lqMf1fyzovWsgrQ8cinchn
96BD4l5NAVPGkoPavtLgh-cEaXPxNJyHE (11.05.2020)
[9] https://www.nature.com/articles/nrd1660 (08.05.2020)
[10] https://link.springer.com/article/10.2165/00003495-200868010-
00009 (10.05.2020)
[11] https://link.springer.com/article/10.2165/11204590-000000000-
00000 (14.05.2020)
[12] https://www.drugbank.ca/drugs/DB06817#BE0004855 (13.05.2020)
[13] https://pubchem.ncbi.nlm.nih.gov/compound/Raltegravir#section=Bi
ological-Half-Life (19.05.2020)
[14] www.ncbi.nlm.nih.gov/books/NBK548313 (11.05.2020)
[15] www.ema.europa.eu/en/documents/overview/isentress-epar-
medicine-overview.de.pdf (18.05.2020)
22
[16] www.nature.com/articles/nrd1660 (13.05.2020)
[17] link.springer.com/article/10.2165/00003495-200969080-00007
(11.05.2020)
[18] eurjmedres.boimedcentral.com/articles/10.1186/2047-783X-14-S3-
17 (13.05.2020)
[19] link.springer.com/article/10.1007/s40262-016-0424-1 (12.05.2020)
[20] www.mmp-online.de/heftarchiv/2013/12/integrase-inhibitoren-neue-
wege-für-die-therapie-der-hiv-1-infektion-html (12.05.2020)
[21] docplayer.org/15969678-Isentress-400-mg-filmtabletten.html
(18.05.2020)
[22] dmd.aspetjournals.org/content/35/9/1657 (17.05.2020)
[23] https://www.hivandmore.de/archiv/2008-
1/HIV1_08__FoBiBogner.pdf (18.05.2020)
[24] “Pharmacokinetics and Pharmacodynamics of Once-Daily versus
Twice-Daily Raltegravir in Treatment-Naïve HIV-Infected Patients”,
downloaded from http://aac.asm.org/ on May 3, 2020
[25] https://retrovirology.biomedcentral.com/articles/10.1186/1742-
4690-5-114 (12.05.20)
[26] Öffentlicher Beurteilungsbericht (EPAR) der europäischen
Arzneimittelagentur (EMA) zu: Isentress (11.05.20)
[27] https://www.sciencedirect.com/science/article/pii/B97801241149200
00341 - Synthesis of Best-Seller Drugs, 2016, Chapter 34, Raltegravir-
Insentress (10.05.20)
[28] https://www.thieme-connect.com/products/ejournals/pdf/10.1055/s-
0036-1591624.pdf (10.05.20)
[29] Instruction for Raltegravir: Isentress®
23
[30] Kassahun K, McIntosh I, Cui D, et al. Metabolism and disposition in
humans of raltegravir (MK-0518), an anti-AIDS drug targeting the HIV-1
integrase enzyme. Drug Metab Dispos 2007;35:1657-63
[31] Wenning LA, Petry AS, Kost JT, et al. Pharmacokinetics of raltegravir
in individuals with UGT1A1 polymorphisms. Clin Pharmacol Ther
2009;85:623-7
[32] Raltegravir: a review of its pharmacokinetics, pharmacology and
clinical studies David M Burger 864 Radboud University Nijmegen Medical
Center, Department of Pharmacy, Geert Grooteplein 10, 6525 GA
Nijmegen, the Netherlands
[33] Isentress (raltegravir) tablets [product circular]. Prescribing
information. Whitehouse Station, NJ: Merck; 2008.; Clinical Pharmacology
Profile of Raltegravir, an hiv-1 integrase strand transfer inhibitor Diana M.
Brainard, MD, Larissa A. Wenning, PhD, Julie A. Stone, PhD, John A.
Wagner, MD, PhD, and Marian Iwamoto, MD, PhD
[34] Clinical Pharmacology Profile of Raltegravir, an hiv-1 integrase strand
transfer inhibitor Diana M. Brainard, MD, Larissa A. Wenning, PhD, Julie A.
Stone, PhD, John A. Wagner, MD, PhD, and Marian Iwamoto, MD, PhD
[35] Influence of Sex/Gender and Race on Responses to Raltegravir
Combined With Tenofovir-Emtricitabine in Treatment-Naive Human
Immunodeficiency Virus-1 Infected Patients: Pooled Analyses of the
STARTMRK and QDMRK Studies Kathleen Squires,1 Linda-Gail Bekker,2
Christine Katlama,3 Yazdan Yazdanpanah,4 Yan Zhou,5 Anthony J.
Rodgers,5 Mark J. DiNubile,5 Peter A. Sklar,5 Randi Y. Leavitt,5 and Hedy
Teppler5
[36] Pharmacokinetics and 48-Week Safety and Efficacy of Raltegravir for
Oral Suspension in Human Immunodeficiency Virus Type-1-
InfectedChildren 4 Weeks to 2 Years of Age Sharon Nachman,1 Carmelita
Alvero,2 Edward P. Acosta,3 Hedy Teppler,4 Brenda Homony,4 Bobbie
Graham,5 Terence Fenton,2 Xia Xu,4 Matthew L. Rizk,4 Stephen A.
24
Spector,6 Lisa M. Frenkel,7 Carol Worrell,8Edward Handelsman,9 and
Andrew Wiznia
[37] Rotger M, Taffe P, Bleiber G et al. Gilbert syndrome and the development of antiretroviral therapy-associated
hyperbilirubinemia. J. Infect. Dis. 192(8), 1381–1386 (2005);
[38] Calza L, Danese I, Colangeli V, Vandi G, Manfredi R, Girometti N, et
al. Skeletal muscle toxicity in HIV-1-infected patients treated with a
raltegravir-containing antiretroviral therapy: a cohort study. AIDS Res
Hum Retroviruses. 2014 Dec;30(12):1162-9. doi: 10.1089/aid.2014.0113
[39] A safety evaluation of raltegravir for the treatment of HIVRosa de
Miguel, Rocio Montejano, Natalia Stella-Ascariz & Jose R Arribas
[40]Taburet A-M, Sauvageon H, Grinsztejn B, Assuied A, Veloso V, Pilotto
JH, et al. Pharmacokinetics of Raltegravir in HIV-Infected Patients on
Rifampicin-Based Antitubercular Therapy. Clin Infect Dis 2015; 61:1328–
1335.
[41]Analysis of Low-Frequency Mutations Associated with Drug Resistance
to Raltegravir before Antiretroviral Treatment� Jia Liu,1,4 Michael D.
Miller,2 Robert M. Danovich,2 Nathan Vandergrift,1 Fangping Cai,1
Charles B. Hicks,3 Daria J. Hazuda,2 and Feng Gao1* Duke Human
Vaccine Institute1 and Department of Medicine,3 Duke University Medical
Center, Durham, North Carolina 27710; Merck & Co., Inc., West Point,
Pennsylvania2; and Department of Microbiology, Peking University Health
Science Center, Beijing 100191, China4

25
Picture Sources:
Figure 1: Own work
Figure 2 & 3: Own work, using MolView
Figures 4-7:
https://www.sciencedirect.com/science/article/pii/B978012411492000034
1 - Synthesis of Best-Seller Drugs, 2016, Chapter 34, Raltegravir-
Insentress (10.05.20)
Figure 8: https://www.thieme-
connect.com/products/ejournals/pdf/10.1055/s-0036-1591624.pdf
(10.05.20)
Figure 9: https://www.nature.com/articles/nrd1660/figures/2 (12.05.20)
Figure 10: https://onlinelibrary.wiley.com/doi/epdf/10.1002/rmv.350
(12.05.20)
Figure 11: https://www.nature.com/articles/nrd1660/figures/1 (12.05.20)
Figure 12: Clinical Pharmacology Profile of Raltegravir, an hiv-1 integrase
strand transfer inhibitor Diana M. Brainard, MD, Larissa A. Wenning, PhD,
Julie A. Stone, PhD, John A. Wagner, MD, PhD, and Marian Iwamoto, MD,
PhD
Figures 13,14: Analysis of Low-Frequency Mutations Associated with Drug
Resistance to Raltegravir before Antiretroviral Treatment� Jia Liu,1,4
Michael D. Miller,2 Robert M. Danovich,2 Nathan Vandergrift,1 Fangping
Cai,1 Charles B. Hicks,3 Daria J. Hazuda,2 and Feng Gao1* Duke Human
Vaccine Institute1 and Department of Medicine,3 Duke University Medical
Center, Durham, North Carolina 27710; Merck & Co., Inc., West Point,
Pennsylvania2; and Department of Microbiology, Peking University Health
Science Center, Beijing 100191, China4s