rapport_task reallocation and cost prices_def_eng-gb
TRANSCRIPT

Task Reallocation & Cost Prices A research of obstacles concerning substitution
25-6-2014
Author Drs. A.J. (Arjan) Kouwen Co-author Drs. G.T.W.J (Geert) v.d. Brink

1
Executive summary In June 2013, the Radboud University Medical Center started the research ‘task reallocation and cost prices’ as
commissioned by the Ministry of Health, Welfare and Sport (VWS). The purpose was twofold: first, to map the
relationship between task reallocation practice and cost pricing of Diagnosis-Treatment Combination Care products
(DBC Care products) and secondly , as a corollary, inventory the ensuing obstacles for the deployment of nursing
specialists and phy sician assistants.
The research A practice-based research was carried out collecting both qualitative and quantitative data. 108 interv iews were taken
with nursing specialists, phy sician assistants, medical specialists and managers in the 4 participating hospitals. It
concerned 3 specialised clinical hospitals and 1 academic hospital. In addition, cost price data at procedure level were
collected to establish the relation between the task reallocation practice and cost accounting. A total of 32 nursing
specialists and 19 phy sician assistants were involved in the research who are employed in 15 different specialisms.
Research results A toolbox was developed for the analy sis, to clarify the task reallocation share in the cost prices. It was noted that both
nursing specialists ( NS) and phy sician assistants (PA) were deployed in a very varied manner. This variance is not so
much explained by the number of y ears since graduation but rather by the own professional development, self -
confidence, the acquired specialism and the trust of the medical specialist in the quality of care supplied by the NS
and/or PA.
Both groups carry out a lot of tasks that are not registered or that fall outside the scope of registered procedures (57%).
The physician assistant performs more reallocated tasks and is deployed more generally on the grounds of the broader
knowledge base (in the capacity of ward doctor). The nursing specialist is more often deployed within a specialism in
an integrated care plan, rather providing additional care. A lot additional care is characterized by providing
information to patients and meeting the inc reasing information need of scientific professional associations.
Research conclusions This research shows that the deploy ment of PA and NS in the applied procedure filing sy stem and cost price
methodologies is only clear to a very limited extent. This makes it virtually impossible to produce reliable business
cases for the effectiveness of that deployment.
Moreover, it has been established that the financial sy stem1 and national legislation in hospitals create obstacles for
task reallocation. The main ones being: the face to face criterion for registration of the first consultation, the lack of
transparency in the cost price and procedures sy stem and the fact that the NS/PA cannot open DBCs autonomously.
Finally, through a sensitiv ity analy sis, it was found that the effects of task reallocation are marginally noticeable in the
cost price methodologies currently applied.
Comprehensive pricing 2015 will eliminate a number of obstacles. At the same time, this will create a new obstacle as
it gives rise to uncertainty on funding within the hospitals. Sentiments on remuneration proceeds and government
measures may have a negative effect on the enthusiasm about task reallocation.
Despite all these obstacles, NS en PA are deployed frequently. When asked for the mot ivation for this deployment, the most often heard argument is: the quality of (integrated) care.
Research recommendations The research team stated the following recommendations based on the conclusions:
1 This concerns rules on the funding of medical specialist care and more specifically rules concerning registration and invoici ng of
healthcare activities.

2
1. Improve the provision of information within the hospital and the parties involved with respect to task
reallocation so that the effects become clear. This would stimulate the deployment of NS and PA;
2. Ensure the differentiation of procedures so that the (internal) registration sy stem shows the (financial) e ffect
of that deploy ment;
3. Offer good support for the effectiveness analysis concerning task reallocation - the toolbox may be used for
that purpose;
4. Carry out further studies of the ‘other activ ities' and also involve medical specialist activ ities so that a
comprehensive (and comparable) picture emerges of non-registered activ ities;
5. Work out a number of business cases to further develop and validate the toolbox;
6. The effects of task reallocation need to be re-measured after the implementation of ‘comprehensive pricing’ in
2015.
Appendix 1 translates these recommendations in terms of party or occupational group/profession.

3
Contents Task Reallocation & Cost Prices ................................................................................................................... 0
Executive summary ......................................................................................................................................... 1
Introduction ..................................................................................................................................................... 5
Introduction ..................................................................................................................................................... 5
1. Research design ...........................................................................................................................................6
1.1 Research questions .................................................................................................................................... 6
1.2 Research concept ...................................................................................................................................... 6
1.3 Participating hospitals............................................................................................................................... 7
1.4 Time frame ............................................................................................................................................... 7
1.5 Project structure and accountability ........................................................................................................... 8
2. Terminology and context ...........................................................................................................................9
2.1 Terminology ............................................................................................................................................. 9
2.2 The development of the professions of physician assistant and nursing specialist ........................................ 10
2.3 Legislation and regulations ......................................................................................................................12
2.4 Finance in healthcare...............................................................................................................................16
3. The research population .......................................................................................................................... 19
3.1 General characteristics .............................................................................................................................19
3.2 Characteristics sample survey.................................................................................................................. 20
3.3 Characteristics per specialism.................................................................................................................. 20
3.4 Summary characteristics ..........................................................................................................................21
4. The task reallocation toolbox ................................................................................................................. 22
4.1 Formation data ....................................................................................................................................... 22
4.2 Allocation of duties ................................................................................................................................. 22
4.3 Schedules............................................................................................................................................... 24
4.4 Cost prices ............................................................................................................................................. 24
4.5 Validation .............................................................................................................................................. 28
5. Research results ....................................................................................................................................... 28
5.1 The formative deploy ment of physician assistants and nursing specialists ................................................... 28
5.2 Allocation of tasks................................................................................................................................... 30
5.3 Motivations for the deploy ment of physician assistant or nursing specialist ................................................ 33
5.4 Registration of procedures....................................................................................................................... 34
5.5 Cost pricing in relation to task reallocation ............................................................................................... 34
6. Obstacles to task reallocation..................................................................................................................37
6.1 Perceived obstacles from interviews ......................................................................................................... 37
6.2 Obstacles observed in the research........................................................................................................... 38

4
7. Discussion (research reservations)........................................................................................................ 39
8. Conclusions and recommendations ...................................................................................................... 40
Detail Conclusions........................................................................................................................................ 42
Definitions ......................................................................................................................................................47
Reference list................................................................................................................................................. 48
Appendix 1. Summary reserved procedures ............................................................................................. 50
Appendix 2: Recommendations summarized per consultative group.................................................... 0

5
Introduction
Since the nineties, various parties in healthcare have advocated a structural task reallocation between the occupational
groups. One of the aims was maintaining the accessibility of healthcare. In 2002, the Council for Public Health and
Care (RVZ) in its report ‘Task reallocation in healthcare’ advised the minister on the manner in which the obstacles for
such a reallocation might be cleared. In the following years, study programmes were developed and the legal
regulations concerning accountability and autonomously carry ing out medical procedures for both occupational
groups were adjusted (Indiv idual Healthcare Professions Act - BIG Act). A following area of attention is the funding of
the phy sician assistants and nursing specialists. In its published advice of 2012, the Dutch Healthcare Authority (NZa)
stated the legal obstacles concerning task reallocation and a number of these obstacles will be eliminated with the
introduction of comprehensive pricing in 2015.
This has led to the research at hand, in which in a practice -based manner the v isibility of task reallocation in cost
prices is mapped as well as the obstacles to task reallocation.
6
1. Research design
This chapter successively discusses the research questions (§1.1), the research concept (§1.2), the examined hospitals
(§1 .3), the process steps (§1.4), the time frame (§1.5) and the project structure of the research (§1 .6).
1.1 Research questions Since 2012, the physician assistant and the nursing specialist may autonomously indicate and carry out a number of
reserved procedures in the area of medical specialist care2 within predetermined preconditions. Minister Schippers of
Health, Welfare and Sport (VWS) wants to stimulate a more effective organization of healthcare in this manner3. The
basic idea in this effort is that the medical specialist4 transfers certain procedures and treatments to non-medical
professionals (such as the NP and PA) so that he or she is able to concentrate on the diagnostics and treatment of more
complex healthcare issues. This raises the question how the deployment of the NS and/or PA will become clear in cost
prices and the other way round, to which extent does this insight (or the lack thereof) influence deploy ment. This
results in the following two research questions of this practice -oriented research:
1. In which manner is the deployment of the physician assistant and nursing specialist accounted for in the cost
prices of DBC Care products?
2. What are the obstacles with respect to task reallocation in the current financial and accounting regulatory
framework?
1.2 Research concept Primary starting point is the way in which task reallocation is implemented in practice and how this is refl ected in the
cost price profiles. This makes for a practice-oriented research, i.e. a multiple case study. The research steps are
indicated in figure 1 on the following page.
Through a preliminary study (phase 1) and a further fine-tuning thereof (phase 2), the validity of the cost price profiles
and cost price registration was determined with a limited number of hospitals.
Based on this preliminary study, the decision was taken to choose the base year 2012 as this was the first year in which
cost price date (mandatory ) had to be supplied. Moreover, at the time of drawing up this report, the cost price data on
2013 were not yet available with the hospitals involved.
Consequently, data collection was effected (phase 3). In first instance, a number of specia lisms were examined to
provide a first picture of the cost price information. Based on the inclusion criteria applied, next all graduated nursing
specialists in the departments Anaesthesiology, Surgery, Cardiology , General Internal Medicine, Pneumatology ,
Neurosurgery and Urology were included in the research. These were included because of the scope (number of
procedures) and the nature (surgical, observational and where this concerns internal services, therefore
anaesthesiology ). The aim was to create a range of various kinds of specialisms and this way obtain a cross-section of a
hospital. Initially, fewer specialisms were selected but in other hospitals we also examined other (additional)
departments in order to be able to compare as many hospitals as possible. Exclusion criteria:
1. All specialisms where NP/PA were trained 2. All specialisms where no NP/PA are deployed by hospitals, with the exception of two departments. These two
departments were questioned on possible obstacles of deployment.
2 Bulletin of Acts and Decrees, year of publication 2011, no. 658 and 659
3 E.I. Schippers, Preliminary Letter to the chairman of the 2
nd chamber no. 437, 29_689 Review healthcare system, 22 April 2013.
4 A medical specialist is a physician who, after a six-year university base study, has specialised in a
organ (system) or a part or field thereof.

7
On behalf of the analysis (phase 4), a toolbox was developed to map and validate the task reallocation. The toolbox
provides insight into the extent to which the reallocation is effected in practice and the way this is entered into the
financial sy stems.
Figure 1. Research steps and corresponding research questions
In phase five, the medical specialist, phy sician assistant, nursing specialist, manager and controller of various
departments were interviewed. The interviews with these different parties in the task real location practice and
registration methodology provide a cross-section that is of importance to the final conclusion. The interv iews provided
insight into the following aspects:
- Which activ ities are carried out by a PA/NP (task reallocation practice)?
- What is the level of task reallocation in relation to the medical specialist (task reallocation practice)?
- How are these activities (procedures) registered (registration methodology)?
- How are these activities expressed in the cost price of DBC Care products (registration methodology ) ?
Through desk research and data analy sis on the diagnoses concerned and the corresponding cost prices (cost drivers)
of DBC Care products it has become clear which aspects are actually included in the cost price profiles. The availability
of correct data strongly varied per department and per hospital. This is why each hospital was indiv idually assessed to
determine whether the information was complete or needed to be complemented.
1.3 Participating hospitals The research focussed on specialised clinical hospitals in the southern part of the Netherlands that apply a comparable
deployment profile of phy sician assistants or nursing specialists. In the end, four hospitals were involved in the
research: Radboud University Medical Center Nijmegen, Canisius Wilhelmina Hospital Nijmegen, St. Antonius
Hospital Nieuwegein and St. Elisabeth Hospital Tilburg.
The project team signed a confidentiality statement with these four hospitals as a lot of sensitive information was used
for the analy sis. In practice, this means that the research team no longer possesses any data at the time that this report
is published. In a possible follow-up research, these data may be acquired from the participating hospitals until May
2019 at the latest date.
1.4 Time frame A tight time schedule was drawn up for the research; the start was in June 2013 and completion of the report was scheduled for June 2014.

8
Figure 2. Time frame (planning)
1.5 Project structure and accountability The project was carried out by a project team supervised by a steering group. The approach and interim results were
reported to a specially for this purpose established steering group and to a consultative group composed of parties
involved at national level (government, industry and professional associations).
The project team consisted of the following persons:
- Mr. T.A.C. (Thijs) Sondag MSc. (up to an inc. February 2014) - Ms Y.P. (Yvonne) van Vugt MSc. - Ms K.J. (Karlijn) Verhagen MSc. (as per February 2014)
- Ms P.J.M. (Petra) Kleven MSc - Mr. drs. A.J. (Arjan) Kouwen (Project leader).
During the research, the project leader reported every two weeks to the steering group consisting of the three following persons:
- Mr. drs. G. van den Brink (commissioner, Principal Care Academy , Radboudumc) - Mr. drs. F. Lataster (Assistant Manager Service company , Radboudumc)
- Mr. Ir. E. Booden (Manager PVI, Radboudumc) The project leader regularly provided feedback to the consultative group especially set up for this purpose. The consultative group consisted of the following persons:
- Mr. drs. T.P. Hoogeveen (Ministry of Health, Welfare and Sport)
- Ms drs. L. van der Velde (Netherlands Association of Hospitals) - Mr. drs. T. Urlings (Dutch Healthcare Authority )
- Mr. dr. G.W. Salemink (Association of Dutch Health I nsurers) - Ms O. Frauenfelder (Nursing & Care Staff Netherlands) - Mr. F. de Roo MPA (Dutch Association Physician Assistants)
- Ms drs. B.J.G.M. Meulenbroek (Dutch Federation of University Medical Centers) - Ms drs. B.W.H. van de Lagemaat (Association of Medical Specialists)

9
2. Terminology and context
In this chapter, the conceptual framework (terminology ) and the context in which the research took place, will be
discussed in detail. After a further explanation of the central terms applied in the research (§2.1 ), the context of the
research will be outlined. To this end, the development of the professions of nursing specialist and physician assistant
will first be discussed (§2.2). Consequently, the laws and regulations relevant to task reallocation and registration
methodology will be elaborated (§2.3). §2.4 will outline the financial economic context.
2.1 Terminology A large number of different terms are used in the debate on task reallocation. E.g. the terms ‘profession’, ‘position’,
‘task’, ‘substitution’ and ‘job differentiation’ are of importance. The following definitions originate from the framework
of the Council for Public Health and Care (RVZ)5 applied in discussions on national level.
Profession, position and task
A profession is defined as: a complex of interrelated (core) tasks, jointly accepted theoretical and ethical premises and
professional methodologies, the nature and interrelationship of which depend on the actual work situation. A position
is described as the complex of work tasks to be carried out by a single person. The term contains the demands posed
(by a business) to the work capacity (of an employee). A task is an activity formulated according to certain rules, which
is a meaningful, logical and necessary component of carry ing out work a imed at a specific aim. With a categorization of
positions, this is determined by the organization in which the professional is employed as well as how the range of
tasks is composed.
These definitions of the terms implies that professionals with the same vocational training and professional
background may be employ ed in various positions. In a general hospital, a phy sician may fulfil positions both in direct
patient care and on the Board.
Job differentiation
Job differentiation is the breakdown of tasks, giving rise to new positions. The term is also used to indicate the spread
of positions within an organization.
Substitution
Substitution entails shifting tasks between occupational groups/professions. A distinction is made between vertical
and horizontal substitution. In vertical substitution, tasks are transferred to professionals with a lower (education)
level, in horizontal substitution to professionals with an equal (education) level.
Task reallocation
Professions or occupational groups are the main focus of task reallocation and not positions. Task reallocation is,
therefore, defined as a way to redistribute tasks between professions in a structural manner. With reference to this, the
Council defines task reallocation as: ‘the structural task reallocation between various professions’. This also means a
reallocation of tasks including responsibilities between various professions.
The distinction between professions and positions is important, because of the structural character, as indicated by the Council for Public Health and Care (RVZ). With terms such as ‘substitution’ or job differentiation’ it is not clear whether the transfer of tasks is structural or occasional. For positions change all the time. Task reallocation may furthermore be categorized according to the ty pe of organisational process. There are four ty pes:
5 Council for Public Health and Care, Task Reallocation in Healthcare, Zoetermeer 2002

10
1. Supplementation An extension of the tasks or skills of existing professionals (e.g.: the assistant/practice nurse carries out specific preventive tasks);
2. Substitution: The execution of a procedure/act by one type of professional is taken over by another type of professional (e.g.: taking over tasks of the GP by a nursing specialist or phy sician assistant);
3. Innovation: A new type of professional is introduced (e.g.: a physician assistant or nursing specialist).
Delegation
Delegation does not entail any reallocation of tasks. Certain tasks are delegated from a ‘higher qualified’ to a ‘lower qualified’ professional (e.g.: practice assistant stitches minor wounds). The Indiv idual Healthcare Professions Act (BIG) provides a clear guide for the definition of delegation. The doctor may delegate tasks to all lower -qualified professionals. In comparison with task reallocation, task delegation does not concern a structural redistribution of tasks that do not belong to the area of expertise of the person to who those tasks are delegated. This does not require direct superv ision, nor the intervention by a physician and there is no shift in responsibility.
Additional care
Within this research, we use the term ‘additional care’ for new tasks, therefore tasks that were not transferred. In this
respect, we distinguish between ‘care-related’ and ‘non-care-related’ tasks. for example psychosocial care and
administrative/logistic tasks.
Secondary care
This research focuses on the deployment of the NP/PA in hospitals. A possible deployment in primary care therefore
falls outside the scope of this research.
Our use of the term ‘secondary care’ does not take into account any possible boundary shifts between primary and
secondary care that are taking place at this time (transfer, relocation and/or liaison).
2.2 The development of the professions of physician assistant and nursing specialist Both professions, physician assistant (PA) and nurse practitioner (NP), have experienced a considerable development
in recent years. Table 1 summarizes the developments, as well as the intentions of the Minister of Health, Welfare and
Sport (in italics).
Table 1 . Chronological developments in the professional field
2001 First Nurse Practitioner graduates
2001 Start of experiments with deployment of physician assistants
2002 Task reallocation advice by Council for Public Health and Care (RvZ)
2004 First physician assistant graduates
2007 Professional profiles physician assistants (NAPA)
2009 Title ‘nurse practitioner’ replaced by nursing specialist (NL)
2009 Legally recognized title ‘nursing specialist’ (section. 14)
2012 Experiment section BIG Act in force
2012 Implementation test task reallocation NZa
2015 Independently open DBC, terminate F2F, comprehensive prices
2017 End of experiment The first nursing specialists (NS) and physician assistants (PA) graduated in 2001 and 2004 respectively. Both
professions were primarily introduced to enable task reallocation of medical specialists. In 2002, task reallocation was
the subject of a study in a broader context by the Council for Public Health and Care. This has led to legal recognition
of the title nursing specialist in 2009. In 2012, the experiment section came into force allowing NS and PA to
autonomously indicate and carry out a number of reserved procedures. As of that time, they are also subject to
(medical) disciplinary law.
The experiment formally ends in 2017 and the intention is to finalize the amendme nt to the Individual Healthcare
Professions Act (BIG).
An important result of the developments described is the increase in the number of employed physician assistants and
nursing specialists. Figure 3 shows that there has been a significant growth of the number of nursing specialists since
2006. The increase in the number of physician assistants started a little later, i.e. there is a significant growth in 2007.

11
This is based on research from 2012, carried out by Prismant commissioned by the Dutch Capacity Organ (Het
Capaciteitsorgaan)67 and this research concerned the actually employed nursing specialists and phy sician assistants.
Figure 3. The context, no. of PA/NS employed in their profession
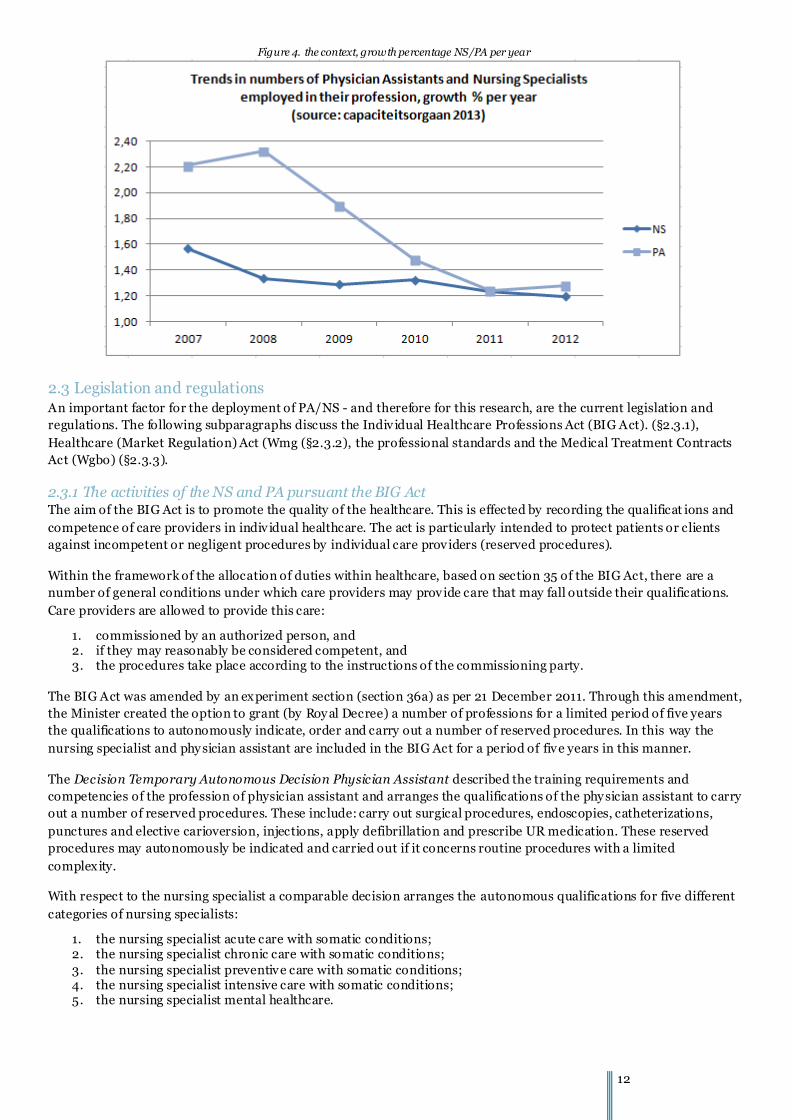
In 2012 we can still see an average growth of 20% in the numbers of nursing specialists and physician assistants in the
sector. This increase is illustrated in figure 4. It is remarkable that the nursing specialist shows a stronger increase than the physician assistant. Figure 5. Indicates the growth percentage per year; the number of physician assistants and nursing specialists increased by 20% per year in 2011.
6 Van der Velde, F., Van der Windt, W., Alumni of the Master’s degree programme Advanced Nursing Practice,
Capaciteitsorgaan, Utrecht, March 2013. 7 Van der Velde, F., Van der Windt, W., Alumni of the Master’s degree programme Physician Assistant, Capaciteitsorgaan,
Utrecht, March 2013.
12
Figure 4. the context, growth percentage NS/PA per year
2.3 Legislation and regulations An important factor for the deployment of PA/NS - and therefore for this research, are the current legislation and
regulations. The following subparagraphs discuss the Indiv idual Healthcare Professions Act (BIG Act). (§2.3.1),
Healthcare (Market Regulation) Act (Wmg (§2.3.2), the professional standards and the Medical Treatment Contracts
Act (Wgbo) (§2.3.3).
2.3.1 The activities of the NS and PA pursuant the BIG Act The aim of the BIG Act is to promote the quality of the healthcare. This is effected by recording the qualificat ions and
competence of care providers in indiv idual healthcare. The act is particularly intended to protect patients or clients
against incompetent or negligent procedures by individual care providers (reserved procedures).
Within the framework of the allocation of duties within healthcare, based on section 35 of the BIG Act, there are a
number of general conditions under which care providers may provide care that may fall outside their qualifications.
Care providers are allowed to provide this care:
1. commissioned by an authorized person, and 2. if they may reasonably be considered competent, and 3. the procedures take place according to the instructions of the commissioning party.
The BIG Act was amended by an experiment section (section 36a) as per 21 December 2011. Through this amendment,
the Minister created the option to grant (by Roy al Decree) a number of professions for a limited period of five years
the qualifications to autonomously indicate, order and carry out a number of reserved procedures. In this way the
nursing specialist and phy sician assistant are included in the BIG Act for a period of five years in this manner.
The Decision Temporary Autonomous Decision Physician Assistant described the training requirements and
competencies of the profession of physician assistant and arranges the qualifications of the phy sician assistant to carry
out a number of reserved procedures. These include: carry out surgical procedures, endoscopies, catheterizations,
punctures and elective carioversion, injections, apply defibrillation and prescribe UR medication. These reserved
procedures may autonomously be indicated and carried out if it concerns routine procedures with a limited
complexity.
With respect to the nursing specialist a comparable decision arranges the autonomous qualifications for five different
categories of nursing specialists:
1. the nursing specialist acute care with somatic conditions; 2. the nursing specialist chronic care with somatic conditions;
3. the nursing specialist preventive care with somatic conditions; 4. the nursing specialist intensive care with somatic conditions; 5. the nursing specialist mental healthcare.

13
The qualifications to perform reserved procedures of a nursing specialist intensive care are the widest (equal to those
of the physician assistant). The qualifications of the nursing specialist preventive care with somatic conditions have
the highest level of restrictions. This concerns qualifications to give injections and to prescribe UR medication.
For both the nursing specialists and the phy sician assistants, these reserved procedures may be indicated and carried
out if it concerns routine procedures with a limited complexity and if the NS/PA is competent. Moreover it applies to
both professions that the scope of the diagnostics with respect to the reserved (and regular) procedures is limited to
the subarea in which the phy sician assistant and the nursing specialist is trained. Appendix 1 provides a summary of
these qualifications.
The experiment arrangement in the BIG Act described, means in practice that nursing specialists and physician
assistants are qualified to indicate and perform reserved procedures autonomously as per 31 December 2011. The act
grants this qualification subject to a number of conditions. It has to concern proce dures:
- that are allocated to the NS/PA on the grounds of the law (appendix 1); - that lie within the area of expertise;
- with a limited complexity; - that are carried out in a routine manner; - with foreseeable risks; - for which the NS or PA is considered competent.
Which procedures in an actual situation fall under the new qualifications, is not literally laid down in the act . The
Guide Implementation Task Reallocation8 drawn up by the professional associations KNMG, V&VN and the Dutch
Association Physician Assistants (NAPA) is a useful tool to further shape the new qualifications of an NS and PA
pursuant the legal requirements.
As each department decides on the details of the deployment of the NS/PA independently, this research opted for a
quality inventory per department and to assess this separately per casus (department and/or specialism). The research
focuses on the procedures carried out by the NS/PA concerned. And especially on procedures autonomously carried
out and the registration thereof.
2.3.2 The Wmg and billable performance for nursing specialists and physician assistants The Healthcare (Market Regulation) Act (Wmg)9 is the basis for the regulation of performance and tariffs. Professions
that are added to the BIG Act, such as the NS and PA, therefore are also subject to the Wmg and such under the
performance and pricing regulation of the Dutch Healthcare Authority (NZa).
A relevant development within the Wmg in secondary care is the recent performance -based funding1 0. As from 1
January 2012, the new product structure DOT 1 1 is also introduced and performance-based funding is applicable until
2014 in combination with the transition model. As from 2008, the income of independent medical specialists is based
on full performance-based funding, subject to the proviso that remuneration turnover is subject to a temporary ceiling
until 2015. The ceiling does not apply to medical specialists in salaried employment; their remuneration is laid down
in the salary they receive and therefore falls outside the scope of pay per performance. As the situations researched
both have independent and medical specialists in salaried employment, it was important to include this distinction by
explicitly asking for the partnership situation in the research questions.
Tariffs for DBC Care products consist of a cost and remuneration part. The remuneration part is the maximum amount
per care product that may be invoiced as compensation for the serv ices of a medical specialist. The cost component is
8 KNMG, V&VN en NAPA, Implementation Task Reallocation Guide, 2012
9 http://wetten.overheid.nl/BWBR0020078/
10 NZa, CI_11_28c, Introduction performance-based funding medical specialist care
11 DOT: DBC Care products towards Transparency

14
the maximum amount per care product that may be invoiced as compensation for institution costs such as staffing and
material costs. These include the wage costs for the PA and NS. Through a mutual allocation clause a number of
partnerships compensate the hospital for a part of the wage costs of the PA/NS. In task reallocation, costs will shift
from the remuneration part to the cost component, however, by the distinction between the cost component and
remuneration part, this shift from remuneration to the cost component is not possible (see Chapter 6 for obstacles).
This of importance as task reallocation may be felt in the cost component, but may also have an effect in the
remuneration part, which is not v isible.
Register, derive and charge
The physician ensures the correct characterization of the care and among others determines the ty pe of DBC care and
the diagnosis. A care process records the complex of performances of the health facility and medical specialist ensuing
from the demand for care, but is in itself not a chargeable performance. A care process may consist of one or more sub
processes. A sub process is a specific period within the care process of a patient that is closed at a pre-determined time
based on fixed closure rules in the registration methodology. In combination with a diagnosis, a sub process may be
deduced to a DBC Care product or a product loss (non-chargeable product)
This methodology in which the care is registered based on procedures, means that within this research next to
categorization of the care products also the registered procedures and concerned care performance need to be
inventoried.
In its current policy rules, the NZa determines that the gatekeeper specialist concerned is responsible for
categorization of the care and the registration thereof1 2. All care activities take place under the responsibility of the
gatekeeper specialist (ultimately responsible medical specialist) and must therefore be linked to a care process of a
gatekeeper specialism to be chargeable. This makes it impossible for the NS/PA to open an initial sub process and this
way formally initiate a treatment. The NZa intends to make this possible in 2015.
Below, we will shortly explain the three main care activ ities and the corresponding applicable criteria for registration.
Outpatients' departm ent visit and face to face criterion
In the policy rules concerning the first outpatients' department visit, an outpatients' department visit not being a
first outpatients' department visit that leads to opening a new DBC Care product and with a repeated outpatients'
department visit in a current DBC Care product13 with the outpatients' department visits (care activity codes 190007,
190011, 190012, 190008 and 190013 respectively ) is stated that there must be:
- a face to face contact1 4 between patient and gatekeeper specialist (specialist or assistant physician)
and - “help by or through the hospital" in which the location (outpatients' department, external outpatients'
department, nursing home) has been agreed in the negotiations between the healthcare insurer a nd the
healthcare provider. Care activities that may not be designated as outpatients' department visit are: medical checkups, internal
consultations (peers), co-treatment of clinical patients, taking over clinical patients and intake interv iew for a (clinical)
admission.
Inter-colleague consultation (190050) and multidisciplinary consultation (190010)
A relevant other activ ities is the registration of Multidisciplinary inter-colleague consultation (190005) and
Multidisciplinary consultation (190010)1 5. These may be registered as soon as there is a meeting between minimally
12 the Dutch Healthcare Authority, policy rule BR/CU-2104, section 8.22, 8.25 and 8.26
13 The Dutch Healthcare Authority, policy rule BR/CU-2104, section 11.5.1.
14 As an exception hereto, a screen to screen visual contact between patient and gatekeeper specialist may be recorded
15 The Dutch Healthcare Authority, policy rule BR/CU-2104, section 11.14, 11.16 and 11.19 respectively

15
three medical specialists who systematically discuss and document the diagnostics and the treatment plan of a single
patient. Preliminary research shows that PA and NS participate in these forms of consultations. Multidisciplinary
(inter-colleague) consultation (MDO) may be registered in the case of a consultation or outpatients' department v isit
in which the patient is seen by minimally two gatekeeper specialists (specialist or assistant physician of various AGB
specialisms) and when this consultation or outpatients' department v isit is part of the DBC Care product of the
ultimately responsible medical specialist. For both consultation forms holds good that only a medical specialist may
register these1 6.
Co-treatment
Another relevant procedure concerns the activ ity co-treatment (190017) 1 7 . This is the case when a gatekeeper
specialism during a clinical admission, has a patient treated by another gatekeeper specialist on behalf of the own
request for care. This care activity may be recorded per face to face contact between patient and gatekeeper specialist
(specialist or assistant physician) within the framework of co -treatment. At the request of other departments, NS/PA
often perform a form of preventive co-treatment.
2.3.3. Other factors: professional standards and the WGBO Except for legislation and regulations concerning care safety and funding, there are other factors that may influence
the further roll-out of task reallocation.
A first factor concerns the standard of medical specialist occupational groups. These standards are applied by insurers
in procurement processes and may play a part in the deployment of the NS/PA. Despite the fact that these standards
are drawn up from a quality perspective, they are considered a requirement to maintain quality. Just as guidelines and
quality standards, they are no mandatory requirements but concern scientifically founded, widely supported
recommendations that care providers should meet to provide high-quality care. It may be that these recommendations
are not applicable in individual cases. The application of the quality standards in practice is the responsibility of the
attending physician and not meeting the quality standards may have consequences for the registration of the physician
in question, and therefore for the (non-)provision of the concerned care by the hospital itself. The standards do not
deal with the deployment of NS and/or PA, or only to a certain extent, but in practice they may act as guiding principle
for the deployment of the occupational groups/professions that are included.
We have inventoried guidelines for diagnostics and treatment of the researched departments. This shows that advice
to involve an NS/PA in the care process is limited. Despite the fact that many activ ities may also be performed by an
NS or PA, such as care coordination tasks or specific information, the NS/PA is hardly mentioned in these standards.
Examples of quality standards in which the deploy ment of an NS is advised, are those for oncology and urology 1 8.
A second, possibly not restrictive but stimulating factor for task reallocation is the Medical Treatment Agreement Act
(WGBO). A medical treatment agreement is a form of an engagement agreement (title 7 .7 Dutch Civ il Code). This act
among others arranges the right of inspection of the own medical file. The WGBO also contains an information duty
and consent requirement. The care provider is under the obligation to inform patients reasonably and to ask for
permission for a treatment (in the event of children from the parent or guardian). The patient is under the obligation
to inform the healthcare provider correctly and as completely as possible. A care provider must act in life-threatening
situations. However, this does not imply that the patient can demand care of his provider; in certain cases the care can
be refused. The duty of disclosure is important within the framework of this research. This duty concerns:
- The nature and objective of the treatment
- The risks and consequences of the treatment - Possibly any other treatment options
16The NZa intends to make it possible in 2015 that the NS/PA may register day care and the MDO.
17 The Dutch Healthcare Authority, policy rule BR/CU-2104, section 11.14, 11.16 and 11.19 respectively
18Dutch Association for Urology, Quality Standards , April 2013

16
- The prospects of the health condition of the patient
Each non-acute medical treatment requires the oral or written permission of the patie nt. Without this consent, the
care provider cannot start or continue a treatment. If the patient or care provider so wishes, the care provider will document in the file the procedures for which the patient has given his/her permission. With non -invasive procedures, the permission may be considered as granted.
This means that this obligation may influence task reallocation as the medical specialist is required to supply this information. This information may also be provided by a nursing specialist or phy sic ian assistant.
2.4 Finance in healthcare Healthcare finance has seen an important change since 2012. These reforms were meant to lead to a system of
performance-based funding. Since that time, hospitals are compensated based on the provided care performance. In
addition, in that same year, the so-called DOT methodology1 9, an envisaged simplification of the DBC Care products
was introduced. Based on an agreement between the Minister of VWS with the Association of Medical Specialists and
the Netherlands Association of Hospitals, from 2012 to 2014, the NZa also put up a turnover ceiling per institute for
the remuneration of the independent specialists. With the introduction of comprehensive prices in 2015, this turnover
ceiling as well as the maximum remuneration tariffs set by the NZa will be cancelled and the independent specialists
will also be included in the performance-based funding methodology. This will eliminate the distinction between the
remuneration part and the cost component.
In practice, the introduction of performance-based funding in 2012 entailed that hospitals had to make arrangements
with five (in 2012) healthcare insurers on the care to be provided, whereby the risk was div ided between healthcare
insurer and healthcare provider.
It is expected that in the coming period prices in line with market conditions will increasingly be sought after, whereby
hospitals, also stimulated by healthcare insurers, will reconcile pricing to actual costs. To be able to do so, all costs
must be included in the comprehensive cost price. The deployment of phy sician assistants and nursing specialists
should also be clear, in order to be able to reflect the effect of task reallocation in the cost price. In the following
paragraphs, the funding structure is first discussed from a more general perspective, insofar as relevant. Consequently ,
the paragraphs 2.4.1 up to and including 2.4.4 will go into cost prices.
2.4.1. Cost pricing Cost prices in hospitals have a long history. This paragraph provides a concise backgrou nd and substantiation.
History of cost pricing in hospitals
The Alteration Invoicing Structure (WDS) was introduced in 1989. In this policy rule of the Dutch Healthcare
Authority NZa, hospitals could price their production independently. Some hospitals the n calculated the cost prices of
procedures with the help of spreadsheets. In 1991, this resulted in a first inventory of these initiatives by the National
Hospital Institute (NZi, now Prismant). Later, in 1994, various cost allocation tables and cost price methods were
developed for the product categorization project. These focussed on determining a comprehensive cost price through a
cost allocation table. This model was adopted by the National Steering Committee DBC in 2013. Consequently, the
DBC cost price model was applied in 40 priority hospitals to analy ze the homogeneity of the DBCs. In that period,
hospitals also slowly shifted from their own local spreadsheets to professional cost price applications.
The current cost price methodology is very complex and time-consuming as it make use of a bottom-up approach with
procedures as cost units. Especially the rationalization of procedures and cost types, as well as allocating overhead
expenses is labour-intensive.
19 DOT: DBC Care products towards Transparency

17
The immediate cause for an entirely new phase in the development and the application of cost prices in hospitals (as
from 2015) is the observation of some hospital administrators that they have been setting cost prices for years but that
this is hardly relevant for the administration of the institute. At the same time setting realistic cost prices is becoming
increasingly important in the negotiations with healthcare insurers on sales prices. A realistic sales price should
include all underly ing costs.
Purpose of cost prices
Within the framework of performance-based funding, cost prices should enable the responsible departmental staff
member to influence the result. This leads to another concept of effectiveness. In that case, the benchmark between
hospitals will no longer be the criterion for the sales price. Effectiveness then means that the cost price of a care
product is lower than the sales price. And as such it is desirable for each hospital to realize the proper allocation of
costs with sufficient detailing and a proper reflection of the cost price per procedure.
The responsible departmental staff member would have to produce (care) under the market price of a care product. To
this end, he has to dispose of relevant control information, such as a margin analysis with an analysis of price,
occupancy and profile differences. This will add an external target to cost prices and not just an internal one. This
concerns determining NZa prices and price-fixing agreements with healthcare insurers. But it is also of importance -
and that may well be the main argument - because an increasingly demanding patient is asking for transparency
concerning prices and as such for a substantiation of these prices based on actual costs. Figure 5 summarizes the
arguments for a cost price methodology .
Figure 5 . Benefits and advantages of cost prices
This approach indicates that the transparency of registration and, on the basis of this, setting realistic cost prices is
important to realize good sales prices.
Determining cost prices
There are various methods to determine cost prices. In healthcare, in principle the so -called ‘cost centre method’ is
used.20. Costs are in first instance allocated to departments and next to so-called cost units. Examples of cost units are
procedures ‘first consultation’ or ‘follow-up consultation’. This method makes use of layout based on the nature of the
costs as recorded in the ledger accounts. The total costs of the departments are allocated to the registered cost units;
these may be procedures or the so-called care activ ities.
Through weighing factors, the total direct costs are allocated to the cost units. Setting the weighing factors may be
effected based on ratios (top down) or on the basis of the actual deployment of staff, material and equipment per
procedure (bottom up). The result is a comprehensive cost price (both direct and indirect costs) for the medical
procedure per department.
20 Drs. F.F. Asselman, Cost prices in hospitals, Houten, 2008
18
Cost pricing in outpatients' departments in principle requires registration of the first outpatients' department visit,
follow-up v isits, telephone consultations, internal inter-colleague consultations and outpatient interventions
(outpatient childbirths, cytostaticics treatments, etc.). In order to determine the weighing factor, the deploy ment of
medical specialists, assistant physicians and nursing staff is most relevant. The planned consulting time is mostly
taken as basis for this deployment.
At ward level, during admission, treatment and discharge, various activ ities are performed by nursing staff, assistant
phy sicians and the medical specialist. The standard cost price of a nursing day includes the activities of the medical
specialist, the ward doctor and nursing staff.
2.4.2 Procedures, care activities and DBC Care products The Foundation Dutch Hospital Data (DHD) is established by the Netherlands Association of Hospitals (NVZ) and the
Netherlands Federation of University Medical Centers (NFU) with the aim to manage and keep up to date collections
of hospital data, to monitor relevant databanks kept elsewhere and to promote high -quality provision of information
on hospital care. In the whole of the Netherlands, 40 hospitals are involved in the registration of procedures based on
the so-called CBV procedures21 . The CBV filing sy stem is based on daily practice and is used by some 40 hospitals and
seven university centers. It includes procedures of medical and paramedical disciplines. At the request of (care
providers from) hospitals, new procedures and further detailing may be included. Currently the CBV filing sy stem
contains over 55,000 procedures. With the help of the CBV filing sy stem more than 200 million procedures are
registered.
The procedure filing system is applied in a variety of ways, such as DBC registration, v isitation reports, management
information, production overviews, etc. Many procedures are equal to care activ ities which in turn are part of a care
product. In this respect, it is important that everybody interprets a certain procedure in the same manner and links it
in the same way to a care activ ity.
In the DOT structure, a diagnosis must be registered during the care process just as the care activities for each medical
action. At predetermined closing moments of care processes, the comprehensive available information of diagnosis
and care activities is sent to an external grouper22. The grouper derives care products on the basis of decision trees.
The care products form the basis for the invoice of the hospital to the health insurer and/or patien t. The decision trees
are based on the diagnosis and performed care activities. These combinations of diagnoses and care activities are also
called the care profile of a DBC Care product.
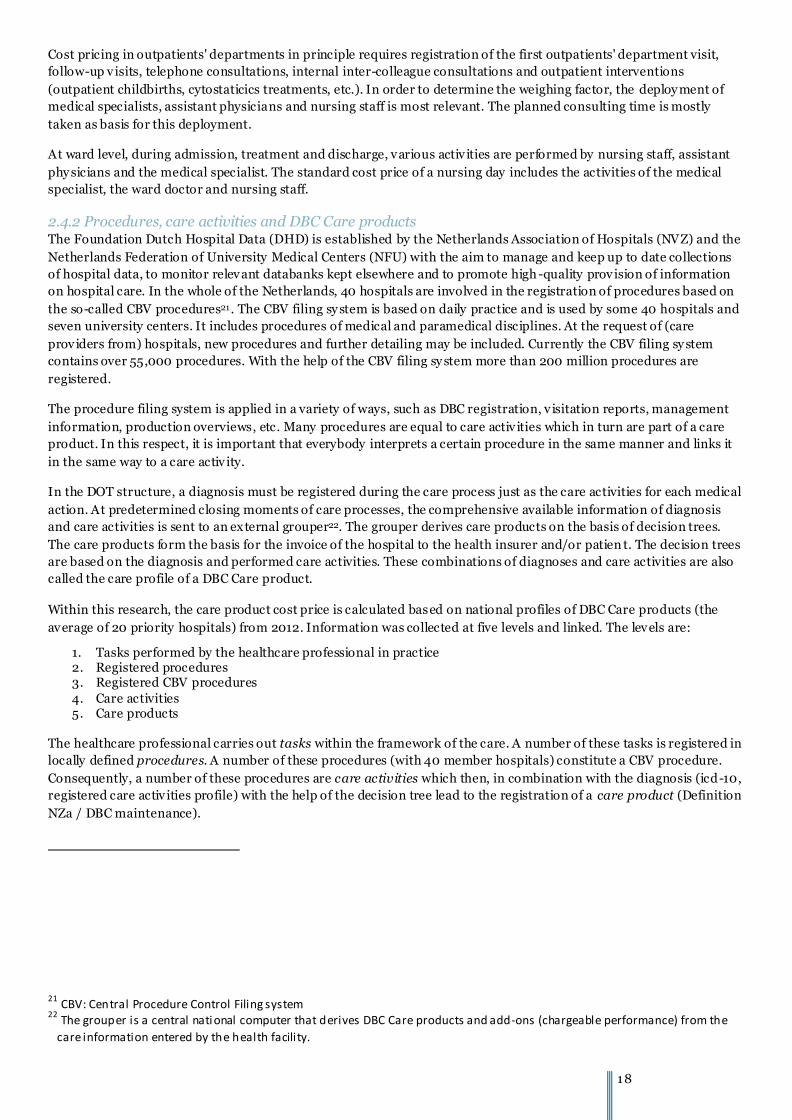
Within this research, the care product cost price is calculated based on national profiles of DBC Care products (the
average of 20 priority hospitals) from 2012. Information was collected at five levels and linked. The levels are:
1. Tasks performed by the healthcare professional in practice 2. Registered procedures 3. Registered CBV procedures
4. Care activities 5. Care products
The healthcare professional carries out tasks within the framework of the care. A number of these tasks is registered in
locally defined procedures. A number of these procedures (with 40 member hospitals) constitute a CBV procedure.
Consequently, a number of these procedures are care activities which then, in combination with the diagnosis (icd-10,
registered care activ ities profile) with the help of the decision tree lead to the registration of a care product (Definition
NZa / DBC maintenance).
21 CBV: Central Procedure Control Filing system
22 The grouper is a central national computer that derives DBC Care products and add-ons (chargeable performance) from the
care information entered by the health facility.

19
Due to the fact that the hospital may have its own registration method at local level with dummy codes etc., it may well
be that level 2 and 3, but also 3 and 4 may differ per hospital. In this research, the levels wi ll therefore be treated
separately.
3. The research population
This chapter describes the research population based on general characteristics (§3.1), characteristics sample survey
(§3.2) and characteristics per specialism (§3.3). The closing paragraph summarizes the similarities and differences
(§3.4).
3.1 General characteristics The first step was researching the general characteristics of the selected hospitals and how many physician assistants
and nursing specialists are employed. These hospitals were selected because they have a large number of PA/NS in
their serv ice and have (through partnerships) an academic background. The aim is to determine whether the hospitals
are comparable in broad outlines. Table 2 provides a summary overv iew.
Table 2: Characteristics hospitals (2012), Source: annual statements 2012
1 2 3 4
1st outpatient visits 157,450 155,213 148,755 239,180
Hospital admissions 31,363 31,563 26,556 45,521
Day treatment 53,087 48,306 29,577 51,609
Nursing days 197,104 149,986 144,809 221,196 Official beds 953 663 673 1,102
Available beds 700 - 545 848 Staffing 9,897 3,830 3,219 4,912
Care-related revenue 427m 239m 236m 399.5m
No. of medical specialists 637 210 185 274
No. of nursing specialists* 54 13 14 28
No. of physician assistants* 21 9 22 5
*Only graduates were involved in the research One hospital dev iates because of its academic character, but if we limit ourselves to care -related production, the size is
still comparable with the other hospitals. In term of outpatients' department v isits, hospital 4 is the biggest.
Hospital 1 deploy s by far the largest number of physician assistants and nursing specialists. Hospital 4 deploys
relatively more nursing specialists. If we consider the specialism in which the two occupational groups are employed,
table 3 shows that by far the largest number is employed with the surgical and diagnostic specialisms.
Table 3: Percentage of physician assistants and nursing specialists involved in the research of surgical, diagnostic and supportive
Category National Hospitals Sample survey
PA NS PA NS PA NS
Surgical 130 240 18 33 7 8
Diagnostic 135 551 32 69 24 13
Supportive 33 48 7 6 2 2
Psychiatry 0 197 0 3 0 0
Total 298 1036 57 111 33 23
% involved in research 19.5 % 10.7 % 11.1 % 2.2 %
10.5% and 19.1% of the respectively employ ed PA and NS in the selected hospitals, are involved in this research. With
the exception of the university hospital, all hospitals apply the cost perform system in the same manner. Their cost
pricing methods are therefore comparable.

20
3.2 Characteristics sample survey Within the research, we tried to interv iew the entire population NS
and PA as much as possible per hospital and per department, in
order to express views on task reallocation and cost prices. Table 4
shows the number of interviewed PA/NS in each hospital. In
addition, medical specialists, managers and controllers were also
interv iewed. A total of 108 interviews were taken for research
purposes. When we compare the number of interviewed PA/NS with
the total number of professionals per hospital, table 5 shows in brief
that on average 35% of the employed PA/NS were interviewed
(including all specialisms and departments).
Table 5: Percentage interviewed physician assistants (PA)
and nursing specialists (NS) per hospital
1 2 3 4
% interviewed PA 30.00 % 44.44 % 27.27 % 71.43 %
% interviewed NS 17.86 % 38.46 % 64.29 % 28.57 %
% of total group 21.05 % 40.91 % 41.67 % 37.14 %
Figure 6 shows a summary overv iew of the characteristics at national level, as well as other characteristics. Figure 6. Characteristics research population
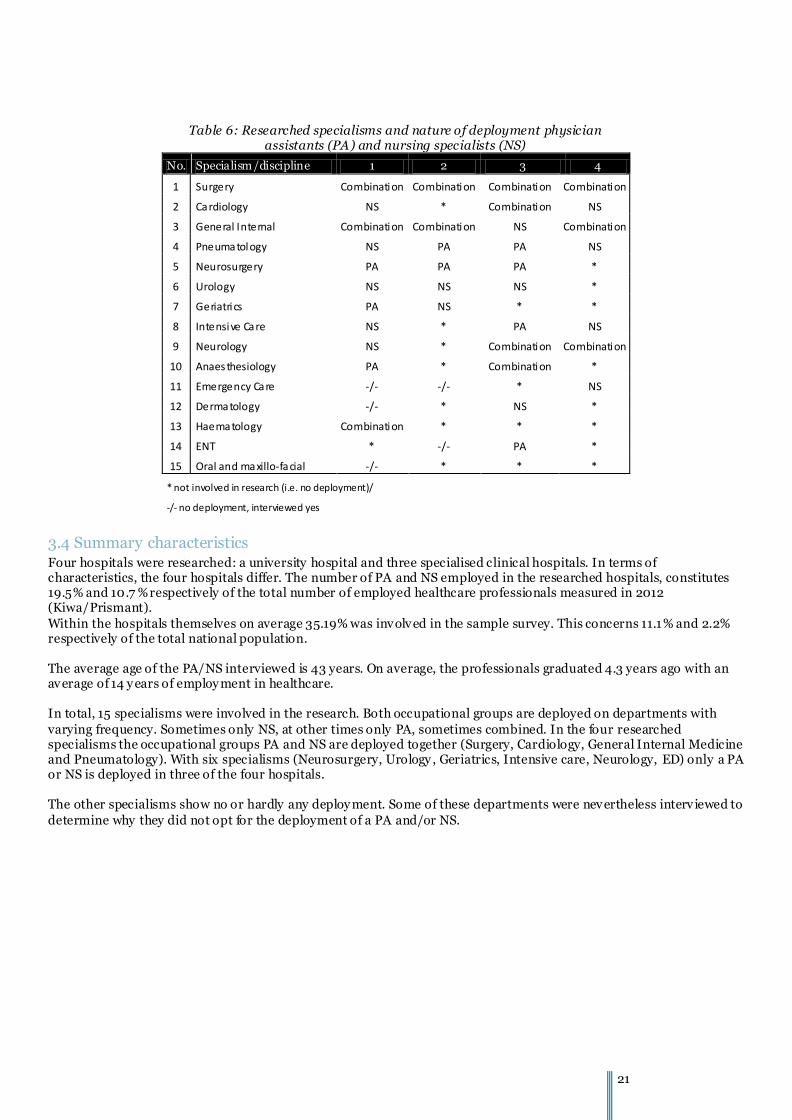
3.3 Characteristics per specialism Table 6 (next page) reflects the researched groups per specialism. This shows that in the four researched specialisms both PA and NS are deployed in the hospitals (Surgery, Cardiology, General Internal Medicine and Pneumatology). With six specialisms (Neurosurgery, Urology , Geriatrics, Intensive care, Neurology, ED) PA or NS are deployed in three of the four hospitals. The others have no or merely a limited deploy ment. Some of them have been interviewed to pinpoint any obstacles.
Table 4: Number of interviewed persons 1 2 3 4
# graduated PA 20 9 22 7
# graduated NS 56 13 14 28
# interviewed MS 10 10 10 8
# interviewed Mng 12 3 2 3
# interviewed PA 6 4 6 5
# interviewed NS 10 5 9 8
Total interviews 38 22 27 25
21
Table 6: Researched specialisms and nature of deployment physician
assistants (PA) and nursing specialists (NS)
No. Specialism/discipline 1 2 3 4
1 Surgery Combination Combination Combination Combination
2 Cardiology NS * Combination NS
3 General Internal Combination Combination NS Combination
4 Pneumatology NS PA PA NS
5 Neurosurgery PA PA PA *
6 Urology NS NS NS *
7 Geriatrics PA NS * *
8 Intensive Care NS * PA NS
9 Neurology NS * Combination Combination
10 Anaesthesiology PA * Combination *
11 Emergency Care -/- -/- * NS
12 Dermatology -/- * NS *
13 Haematology Combination * * *
14 ENT * -/- PA *
15 Oral and maxillo-facial -/- * * *
* not involved in research (i.e. no deployment)/
-/- no deployment, interviewed yes
3.4 Summary characteristics Four hospitals were researched: a university hospital and three specialised clinical hospitals. In terms of characteristics, the four hospitals differ. The number of PA and NS employed in the researched hospitals, constitutes 19.5% and 10.7 % respectively of the total number of employed healthcare professionals measured in 2012 (Kiwa/Prismant).
Within the hospitals themselves on average 35.19% was involved in the sample survey. This concerns 11.1% and 2.2% respectively of the total national population. The average age of the PA/NS interviewed is 43 years. On average, the professionals graduated 4.3 years ago with an average of 14 y ears of employ ment in healthcare. In total, 15 specialisms were involved in the research. Both occupational groups are deployed on departments with
varying frequency. Sometimes only NS, at other times only PA, sometimes combined. In the four researched specialisms the occupational groups PA and NS are deployed together (Surgery, Cardiology, General Internal Medicine and Pneumatology). With six specialisms (Neurosurgery, Urology , Geriatrics, Intensive care, Neurology, ED) only a PA or NS is deployed in three of the four hospitals. The other specialisms show no or hardly any deploy ment. Some of these departments were nevertheless interv iewed to
determine why they did not opt for the deployment of a PA and/or NS.

22
4. The task reallocation toolbox
This research tries to connect the practice of task reallocation to the underly ing cost price methodology and the
available data within the hospitals. This analyse is founded on the so -called toolbox. A method to gain insight into task
reallocation and the registration sy stems. The following description may therefore also be used by the hospitals to
show the effects of task reallocation in the cost prices. Figure 7 provides a schematic overview of the approach
Figure 7 : research approach
The approach has four main categories: formation data, allocation of duties, schedule data and cost price data. These
data are acquired from the hospital IT sy stems and the interv iews with nursing specialist/phy sician assistant, medical
specialist, manager and controller. Based on these data, the deployment and the subdiv ision according to task
reallocation, delegation or additional care is determined. This information is checked with scheduled deployment and
the cost price data. A guarantee for validated information. Discrepancies between these categories will moreover lead
to new insights, e.g. with respect to (possible) obstacles for task reallocation. During the research, the picture became
increasingly clear by further researching such discrepancies. An example is that schedule data did not match with the
hour deployment noted in the interviews. Further research provided insight into the obstacles that play a part but also
in the number of hours that presented the actual situation best based on the collected in formation.
The following paragraphs further explain the four basic steps of the model.
4.1 Formation data Based on the formation data, the deploy ment in FTE and numbers of employees may be mapped. This picture can then
be compared with the actual allocation of reallocated, delegated or additional care tasks. In determining the formation,
it is of importance to signal a trend over a number of years as the number of deployed PA/NS may forecast the level of
task reallocation. Next to conscious choices concerning task reallocation, a formation increase or decrease may also
occur through turnover. In addition, the formation medical specialists and assistant phy sicians need to be included as
this makes task reallocation financially visible.
4.2 Allocation of dut ies To reach an unambiguous and recognisable research method, it was decided to apply the following definitions on the
basis of §2.1:

23
1. T ask reallocation is aimed at a structural reallocation of tasks. This means: tasks are carried out autonomously,
the reallocated tasks are part of standard scheduling and the healthcare professional is considered to be fully
responsible for the ‘reallocated’ task.
2. Delegation is the occasional reallocation of tasks. It concerns the delegation of tasks to healthcare professionals
with a lower qualification level or even without the required expertise. In this respect, especially the temporary nature
as well as the direct involvement of the medical specialist are of importance. I.e. the task is not routinely scheduled
and the option exists of direct supervision and intervention by the medical specialist. The task is performed by order of
and under the supervision of the medical specialist.
3. Additional care means an extension of the tasks of existing professionals. In this research, we distinguish
between ‘care-related’ and ‘non-care-related’ to point out the difference between for example psycho -social care and
administrative/logistic tasks. Table 7 summarizes the operationalization of the terms.
Decision tree task reallocation
Each interview was assessed by three researchers who then gave their shared conclusion. The decision tree in Figure 8
was used. This decision tree operationalizes the legislation and regulations and the definitions appl ied on a national
level. The PA/NS interv iewed indicated in a list of procedures which ones he or she performed. Consequently, it was
determined for each procedure how many minutes the staff member was involved in this procedure, if and to what
extent the procedure was taken over from the medical specialist and whether or not the medical specialist was
involved. Based on these results, it was established which of the three types of allocation of tasks it concerned. The
statement was finally put to the medic al specialist for validation and, when possible, also to a colleague medical
specialist or an NS/PA colleague.
Figure 8: Decision tree task reallocation
Table 7: Operationalization of the terms

24
The statement of the NS and/or PA is mostly an estimate of the number of procedures and the number of minutes they
were engaged in the procedure. That estimate was consequently checked for correctness with the help of the schedule
data. This way, the research arrived at a database with detailed information concerning the procedures, with a
distinction between the registered number of procedures and the stated number of procedures.
4.2.1 The gross-net factor To determine the maximum deployability of a member of staff, the gross-net factor was used23. This factor is based on
a fulltime position of gross 1872 hours per y ear. The net deploy ability is actually lower as a result of holidays, public
holidays, absence by training courses, sickness absence and leave. In the research, a net deploy ability of 1579 hours per
year was used for general staff, based on collective agreement arrangements and a sickness absence of 4.05%. This is a
correction of 19% on gross deployability. For comparison reasons one single factor was applied to all hospitals.
4.2.2. Calculation ‘allocation of tasks’ Based on the prev ious, the total allocation of tasks was calculated as follows:
Calculation ‘allocation of tasks’ A Number of procedures * Number of minutes task reallocation (/
60) = # hour task reallocation p/y
B Number of procedures * Number of minutes task delegation (/ 60) = # hour task delegation p/y C Number of procedures * Number of minutes additional care tasks
(/ 60) = # hour additional p/y
D Total registered tasks in procedure D = A+B+C
E Net deploy ability E = FTE * (1 ,579 hours) F Other tasks F = E - D
By an inventory per healthcare professional of the number of minutes per procedure, a profile of registered procedures
arises in terms of hours per year (ratio A, B and C). This allocation of tasks leads to a total number of hours (D). When
deducting this from the gross-net factor, the ‘other tasks’ become v isible (F), the ones that are not registered.
4.3 Schedules The research also used the schedule data to check whether the data from the interviews are correct. Both the length of
time of a procedure and the number of procedures were verified.
In the first round, it was checked through the schedule code whether the data from the interv iews on the length of time
of procedures matched the planned schedule times. This is necessary because only the anaesthetics departm ent keeps
track of the realized hours as the number of hours OR time is used as basis for internal settlement.
A second check concerned the comparison between scheduled procedures and procedures that were accounted for in
the registration system. As the latter are used as basis for cost price calculation.
4.4 Cost prices This research makes the connection between the practice of task reallocation (tasks) and the ensuing registration of
procedures. These registered procedures constitute care activities which in their turn create the DBC profile of a care
product. The analysis of the cost prices took place according to the steps in Figure 9.
23 Ir. L.M. Berrevoets, Dr. HJ.J.M. Berden, Gross Net Factor as tool to make physicians’ organisation transparent, 2007.

25
Figure 9: Extensive model for the analyse of cost prices
Cost prices are founded on three basic data: costs, registered volumes of procedures and the direct and indirect tasks.
The costs are allocated to the procedures concerned based on a procedure methodology and weighing factors (or
intensities). In order to be able to calculate a cost price per procedure, the registered volume of the procedures
concerned is also required. Cost prices may be calculated at multiple levels:
1. Cost price based on total procedure file (CVB and self-defined procedures) 2. Cost price based on CBV procedures only 3. Cost price based on care activ ities 4. Cost price based on care products
These levels are indicated in the chart below. Hospitals register procedures (own or national). A number of these
procedures lead to registration of a care activity and a care activ ity is then used to derive a DBC care product. Cost
prices can be determined at each of these levels.
4.4.1 Procedures, care activities and DBC Care products The applied toolbox connects practice and financial technical system by connecting the information at four levels. The
first level is that of the inventoried tasks (interv iews). This is connected to the second level of the registered
procedures. With each procedure the scope (the number of minutes) and the nature (task reallocation, task delegation
or additional tasks) is inventoried. Next, the procedures at the third level are linked to the care activities defined at
country level so that the fourth and final level established the relation with the care product cost price. Figure 10
summarizes this.

26
Figure 10. From tasks to care products
In all cases this is based on the national (registration) rules with which hospitals have to comply .
4.4.2 From annual accounts to cost allocation The extensive model (Figure 9) is applicable in setting cost prices. Based on the annual accounts (incl. accountant
audit) the external auditor audited the total costs in the ledger. The audit is in line with the input and output of cost
perform for the member hospitals. The allocation of costs may be complex with respect the real care-related costs and
possible weighing factors that may be applied differently at department level. Figure 11 illustrates the stated audits.
Figure 11. From costs to cost price
The research did not map the allocation of costs in detail as there was always an extensive accountant audit present
(signed statement). The methodology of costing was mapped to determine whether task reallocation is reflected in the
cost prices. Hospitals often also set so-called weighing factors. Based on the interv iews, it was identified how these
weighing factors were arrived at, whether they are regularly updated an whether they lead to a v isibility task
reallocation in cost prices.
27
4.4.3 Sensitivity analysis cost prices The next step was an analysis to what extent hospitals actually express the task reallocation realized in practice in their
cost prices. In concrete terms this means that a conversion of the cost price of the procedures in which an NS/PA is
deployed to the expected cost price mutation and the effect on the DBC Care product price. It is possible to calculate
this at hospital cost level, but because of the sensitiv ity of the information, this was done at a higher level. Starting
point were a number of assumptions:
- Each hospital charges the proper costs to a procedure.
- The number of procedures listed by NS/PA is correct. When this higher than registered, the number of
registered procedures was used.
- The cost price is determined per product on the basis of the national profile. This excludes not o nly general
costs (e.g. for scientific research) but also costs for procedures that are not included in the national profile.
- The calculation is based on the assumption that a decreased deploy ment of medical specialists leads to a
reduction of costs concerning procedures.
Within these assumptions it was determined whether a cost price sufficiently expresses the measured task
reallocation. This was done according to the following calculation steps:
1. Establish the weighted average cost price per care activ ity 2. Establish the mutation cost price of the allocation of tasks based on the average salary costs including social
contributions and additional salary costs of NS/PA and medical specialist 3. Pricing care product based on (1) and (2) and the average national pr ofile24
4. Establish the total costs on the basis of (3) and volumes of a single hospital 5. Establish sensitiv ity25 of cost price calculation
Each hospital, according to its own cost price methodology, set cost prices per procedure 2012 at procedure level.
These prices were converted to a weighted average cost price per external care activ ity code, combined with the
volumes of 2012.
Consequently a new cost price per procedure was determined in which a PA/NS is deployed. The cost price per
procedure was increased by an amount per minute that the PA/NS spent on this procedure26 and was then decreased
by the average salary costs of a medical specialist.
The price per care product was next established according to the old and the new cost price. To this end, the nu mber of
times that a procedure occurs in a product according to the average national profile was multiplied by the price per
procedure.
Finally, the total costs were calculated according to the old and the new prices. This was done by multiplying the
number of times that a product is carried out per year by the price per procedure. This made it possible to compare the
old and the new cost price at procedure, care product and total cost level. Where possible, a comparison per specialism
was carried out.
24 RZ12C, average occurrence of procedures in a care profile
25 The extent to which the applied cost price methodology is sensitive to financial effects of task reallocation
26 Average salary costs PA (71,873 euro), NS (64,111 euro) and Medical Specialist (156,780 euro)

28
4.5 Validation Data collected from interviews with NS/PA were validated in three ways during the research (triangulating):
- By comparison with schedule data - By comparison with registered procedures in the ZIS - By verification of the data during the interviews with medical specialists and colleague PA/NS
The summaries of the interv iews formed the basis for these validations.
5. Research results
This chapter presents the research results v ia the toolbox components. For reasons of source protection, th e results are
not presented as traceable. §5.1. describes the formative deployment of NS/PA. §5.2 sketches the task reallocation
component in the allocation of tasks. §5.3 discusses the motivation for deploy ing NS/PA. §5.4 presents the registration
of procedures and §5.5 deals with cost pricing.
5.1 The formative deployment of physician assistants and nursing specialists All hospitals were asked to supply a formation overview per researched specialism (2010, 2011, 2012 and 2013). Two
hospitals supplied comprehensive (comparable) lists that enabled a breakdown. Due to registration reasons, the other
hospitals could only supply limited data or in an incorrect format. This implied that for these hospitals only a (limited)
analysis could be carried out with a relative picture of the formative changes in three consecutive years.
Figure 12. Graphic representation average formative deployment (FTE) in three years with two hospitals
Table 8 indicates the actual averages with indices.
Table 8. Formative deployment of two hospitals converted to FTE and index figures (2011 = 100%)
Index 2012 2013
Total formation 101.20 101.48
Increase medical specialists , incl . trainee specialist 98.51 95.40
Nursing specialists 129.12 169.34
Physician assistants 149.09 194.53
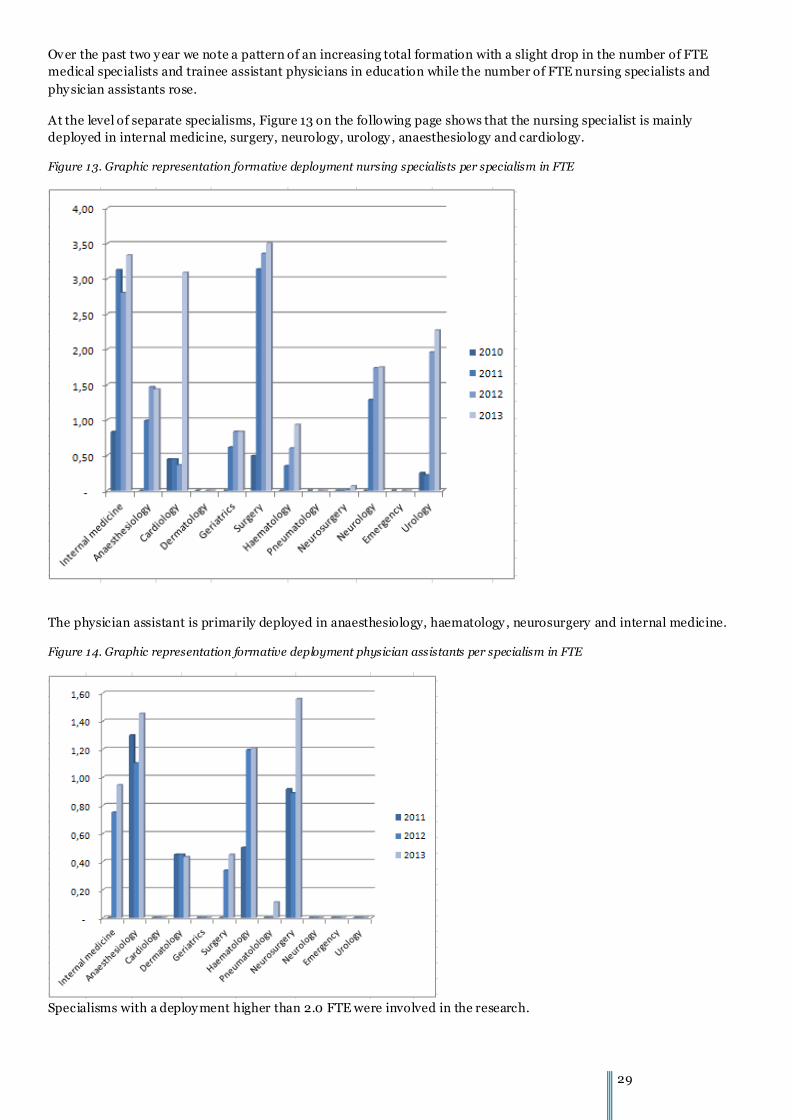
29
Over the past two y ear we note a pattern of an increasing total formation with a slight drop in the number of FTE
medical specialists and trainee assistant physicians in education while the number of FTE nursing specialists and
phy sician assistants rose.
At the level of separate specialisms, Figure 13 on the following page shows that the nursing specialist is mainly
deployed in internal medicine, surgery, neurology, urology , anaesthesiology and cardiology.
Figure 13. Graphic representation formative deployment nursing specialists per specialism in FTE
The physician assistant is primarily deployed in anaesthesiology, haematology , neurosurgery and internal medicine.
Figure 14. Graphic representation formative deployment physician assistants per specialism in FTE
Specialisms with a deploy ment higher than 2.0 FTE were involved in the research.

30
5.2 Allocation of tasks The tasks with 49 healthcare professionals were inventoried and next it
was determined which of these tasks had a relation with a procedure.
For each procedure it was then established whether it concerned task
reallocation, task delegation or additional care and whether this was
carried out autonomously. The time spent o n the procedure was also
asked, excluding the supervision time of/by the medical specialist.
Table 9 presents the average profiles in annual hours.
Figure 15 is graphic representation of this div ision in percentages.
Based on the number of employ ment hours, the maximum deployment per year was determined. The number of ‘other
hours’ (Oth-hrs) represents the remaining part of the
deployability. The categories Task Reallocation (Task reall),
Task Delegation (Task del) and Additional (Add) indicate the
number of hours that may be explained by procedures (#
procedures * # minutes). These show clear differences
between the deployment of NS and PA (see below). In
addition it was researched whether there was a relation
between the number of years after graduation and the level of
reallocation; this turned out not to be the case (P-0.56/Sign
0.701). This leads to the conclusion that there are other
factors that influence the level o f task reallocation. The
persons involved indicate that more or less tasks are taken
over from the medical specialist on the basis of trust and
personal competencies.
The first striking aspect of Figure 15 is the large number of
other tasks (Oth). This concerns on average 57 % of the net
deployable hours. A lot of interviews show that many of these
tasks are carried out above the level of specialisms in the
healthcare chain. This makes it impossible to allocate these
procedures to the NS/PA. Moreover, the PA performs more
reallocated tasks than the NS. For both groups of healthcare
professionals it may well be possible that more reallocated
tasks ‘hide’ in the other activ ities (light blue). Concerning the
deployment as ‘ward doctor’ for example, it was noted that a
lot of the tasks of the PA cannot be registered in specific procedures but are actually reallocated. Nor can a number of
those tasks be registered by the medical specialist, for that matter.
Another striking observation is that a nursing specialist carries out
more ‘additional’ care than the PA. From the interv iews it is cle ar
that this is extra time aimed at additional informing and psycho -
social counselling of patients. The additional care is also aimed at
the healthcare chain in the deploy ment as ‘case manager’. Table 10
confirms the variation in deployment.
This variation becomes even more clear at specialism level. This is represented in Figure 16 on the following page.
Table 9. Deployment profiles of both healthcare professionals in annual hours
Av. NS PA
Task reall 366.40 309.34 464.67
Task del 45.48 52.40 33.55
Add 207.22 252.75 128.79
Other 805.91 766.06 874.53
N 49.00 31.00 18.00
Figure 15. Deployment profiles of both healthcare professionals
Table 10. Average division in hours
Task reall
(Ther)
Task
del
Add
task
Other
task
Average 445.44 35.79 205.50 756.43
Standard deviation 345.34 46.15 257.53 393.91

31
Figure 16. Deployment profiles of both healthcare professionals at specialism level
This chart among others shows that the component ‘other tasks’ strongly varies per specialism. Anaesthesiology and
Geriatrics are good examples that show big differences between task reallocation and other tasks. From the variation,
it may be concluded that task reallocation is applied in a very var ied manner. This also holds good for the registration
of procedures. Further research has to point out whether the implementation of task reallocation is actually specialism
dependent.
Other tasks Based on the stated results, the content of the other tasks of NS/PA was
further examined during the interviews. Table 11 and Figure 17 represent
these tasks as indicated by NS/PA. The results were that the persons
interv iewed perform a lot of extra administration tasks. Tasks mentio ned,
are: requests for laboratory tests, requests and appointments, consultation
planning, etc. The medical specialists indicate during the interv iews that a
lot administrative tasks are indeed reallocated to the NS/PA. At the same
time they indicate that the number of administrative tasks has risen in
recent years. Inventories as a result of professional standards (e.g. DICA
inventories) are mentioned, which are particularly carried out by nursing
specialists.
Table 11. Division of other tasks
Task % stated
1. Administrative 18.69 %
2. Research 10.75 %
3. Expertise enhancement 10.28 %
4. Organisational tasks 9.35 %
5. Prescribe medication 8.88 %
6. Education 8.41 %
7. Telephone contact 7.48 %
8. Inter-colleague consultations
6.07 %

32
Two other important categories Other Tasks are carry out clinical research (and/or related) activities) and prescribe
medication without specific procedure to be registered. Figure 17 represents the division as indicated by the various
persons involved.
Figure 17. Other tasks stated by NS/PA and medical specialists
All these other tasks cannot be registered in procedures. If we distinguish between patient -based and non patient-
based tasks, it turns out that 26.22% of the task hours (432.29 hour on average) is related to patient care but that
these tasks are not (cannot) be registered in procedures. The tasks partly concern reallocated tasks, but also tasks
taken over from nursing staff. 30.3% of non-registered tasks remains, which, according to the persons interv iewed,
mainly concerns education and research. A striking difference is that physician assistants indicate that they work less
on administrative tasks than nursing specialists. This is among others explained by the fact that the physician assistant
has more ward doctor functions with less administrative activ ities. That situation also has more procedures that can be
registered.
Inter-colleague consultations and involvement
medical specialist During the interv iews both NS/PA and medical specialist
indicated that the option of inter-colleague consultations
should exist. This concerned the majority of the interv iewed
phy sician assistants (64%) and a substantial part of the
nursing specialists (36%) and medical specialists (40%). It
was also asked how long patients were discussed during
consultations before and after seeing the patent. On average
this was 6 minutes. It also became clear that an NS/PA on
average is scheduled for a longer period of time than the
medical specialist (an NS 15 minutes longer and a PA on
average 7 .5 minute longer). This is because of the provision
of information and the additional questionnaires that both
healthcare professionals have the patients complete. This
was not done by the medical specialist before; and therefore
constitutes additional tasks. The medical specialist is also
always available on call and e-mail confirmations are used.
Phy sician assistants work more autonomously in a ward or in combination with an assista nt physician resulting in a
different format of the inter-colleague consultations.
Figure 18. Necessity of inter-colleague consultations
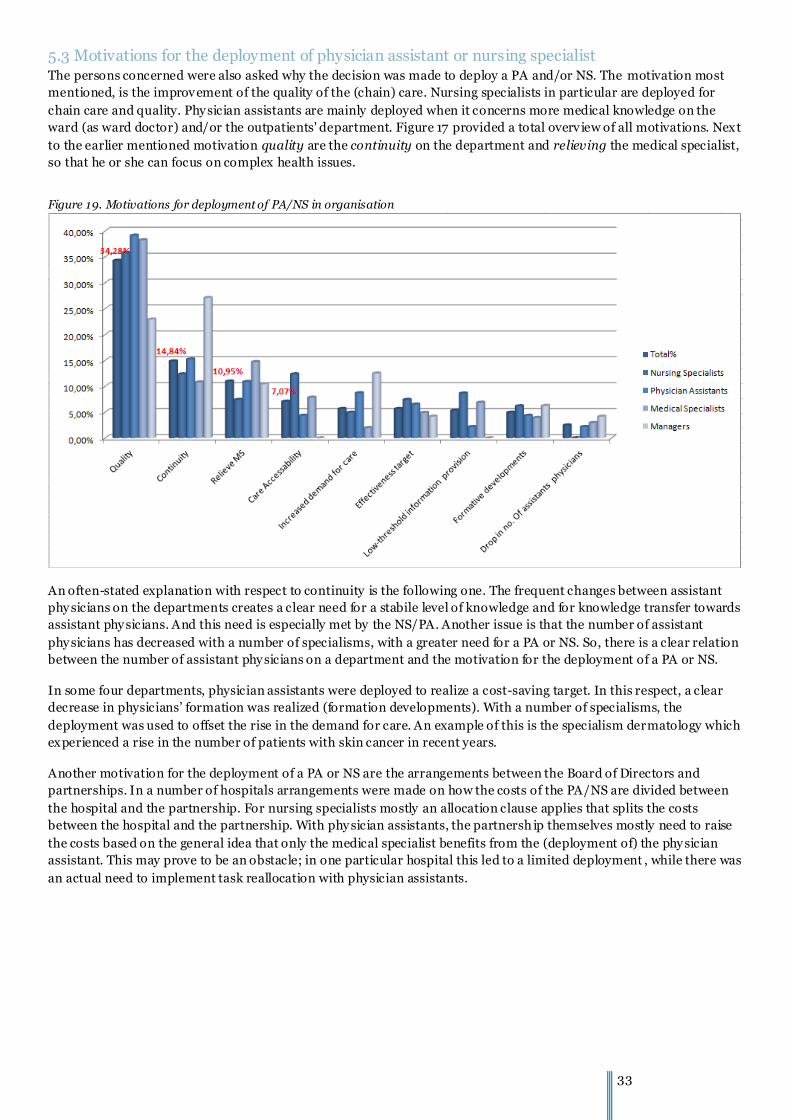
33
5.3 Motivations for the deployment of physician assistant or nursing specialist The persons concerned were also asked why the decision was made to deploy a PA and/or NS. The motivation most
mentioned, is the improvement of the quality of the (chain) care. Nursing specialists in particular are deployed for
chain care and quality. Phy sician assistants are mainly deployed when it concerns more medical knowledge on the
ward (as ward doctor) and/or the outpatients' department. Figure 17 provided a total overv iew of all motivations. Next
to the earlier mentioned motivation quality are the continuity on the department and relieving the medical specialist,
so that he or she can focus on complex health issues.
Figure 19. Motivations for deployment of PA/NS in organisation
An often-stated explanation with respect to continuity is the following one. The frequent changes between assistant
phy sicians on the departments creates a clear need for a stabile level of knowledge and for knowledge transfer towards
assistant phy sicians. And this need is especially met by the NS/PA. Another issue is that the number of assistant
phy sicians has decreased with a number of specialisms, with a greater need for a PA or NS. So, there is a clear relation
between the number of assistant phy sicians on a department and the motivation for the deployment of a PA or NS.
In some four departments, physician assistants were deployed to realize a cost-saving target. In this respect, a clear
decrease in physicians’ formation was realized (formation developments). With a number of specialisms, the
deployment was used to offset the rise in the demand for care. An example of this is the specialism dermatology which
experienced a rise in the number of patients with skin cancer in recent years.
Another motivation for the deployment of a PA or NS are the arrangements between the Board of Directors and
partnerships. In a number of hospitals arrangements were made on how the costs of the PA/NS are divided between
the hospital and the partnership. For nursing specialists mostly an allocation clause applies that splits the costs
between the hospital and the partnership. With phy sician assistants, the partnersh ip themselves mostly need to raise
the costs based on the general idea that only the medical specialist benefits from the (deployment of) the phy sician
assistant. This may prove to be an obstacle; in one particular hospital this led to a limited deployment , while there was
an actual need to implement task reallocation with physician assistants.
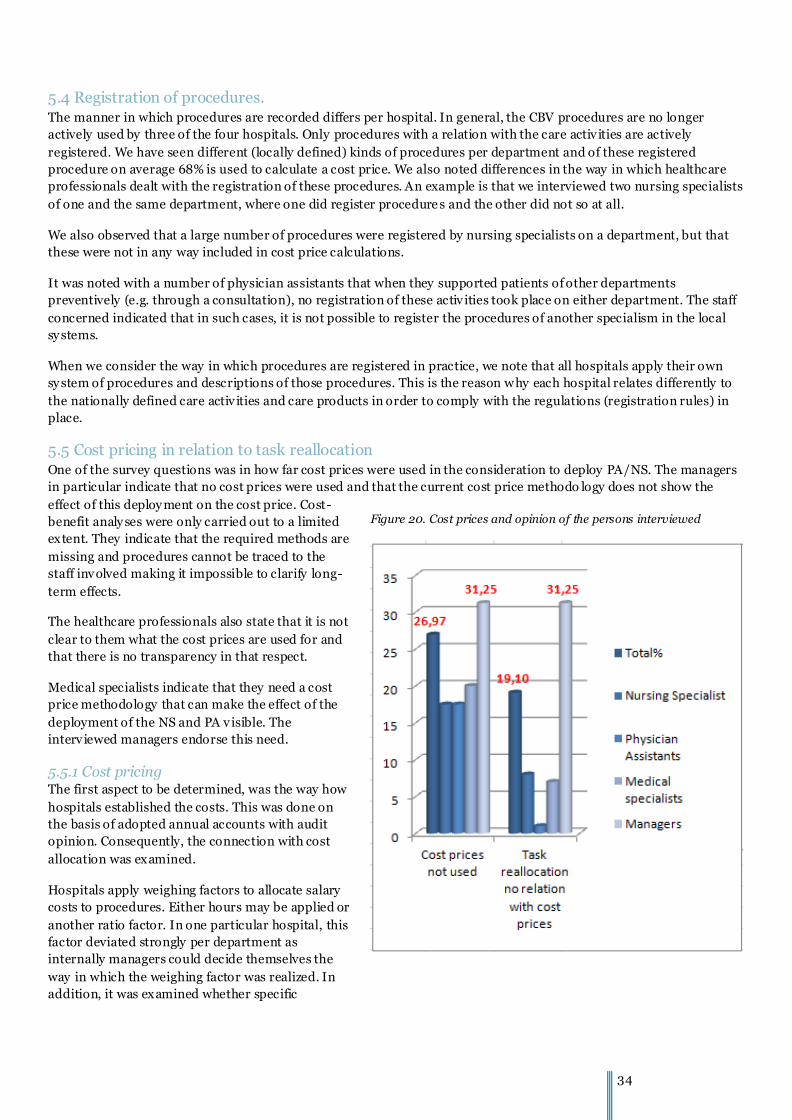
34
5.4 Registration of procedures. The manner in which procedures are recorded differs per hospital. In general, the CBV procedures are no longer
actively used by three of the four hospitals. Only procedures with a relation with the care activ ities are actively
registered. We have seen different (locally defined) kinds of procedures per department and of these registered
procedure on average 68% is used to calculate a cost price. We also noted differences in the way in which healthcare
professionals dealt with the registration of these procedures. An example is that we interviewed two nursing specialists
of one and the same department, where one did register procedure s and the other did not so at all.
We also observed that a large number of procedures were registered by nursing specialists on a department, but that
these were not in any way included in cost price calculations.
It was noted with a number of physician assistants that when they supported patients of other departments
preventively (e.g. through a consultation), no registration of these activ ities took place on either department. The staff
concerned indicated that in such cases, it is not possible to register the procedures of another specialism in the local
sy stems.
When we consider the way in which procedures are registered in practice, we note that all hospitals apply their own
sy stem of procedures and descriptions of those procedures. This is the reason why each hospital relates differently to
the nationally defined care activ ities and care products in order to comply with the regulations (registration rules) in
place.
5.5 Cost pricing in relation to task reallocation One of the survey questions was in how far cost prices were used in the consideration to deploy PA/NS. The managers
in particular indicate that no cost prices were used and that the current cost price methodo logy does not show the
effect of this deploy ment on the cost price. Cost-
benefit analy ses were only carried out to a limited
extent. They indicate that the required methods are
missing and procedures cannot be traced to the
staff involved making it impossible to clarify long-
term effects.
The healthcare professionals also state that it is not
clear to them what the cost prices are used for and
that there is no transparency in that respect.
Medical specialists indicate that they need a cost
price methodology that can make the effect of the
deployment of the NS and PA v isible. The
interv iewed managers endorse this need.
5.5.1 Cost pricing The first aspect to be determined, was the way how
hospitals established the costs. This was done on
the basis of adopted annual accounts with audit
opinion. Consequently, the connection with cost
allocation was examined.
Hospitals apply weighing factors to allocate salary
costs to procedures. Either hours may be applied or
another ratio factor. In one particular hospital, this
factor deviated strongly per department as
internally managers could decide themselves the
way in which the weighing factor was realized. In
addition, it was examined whether specific
Figure 20. Cost prices and opinion of the persons interviewed
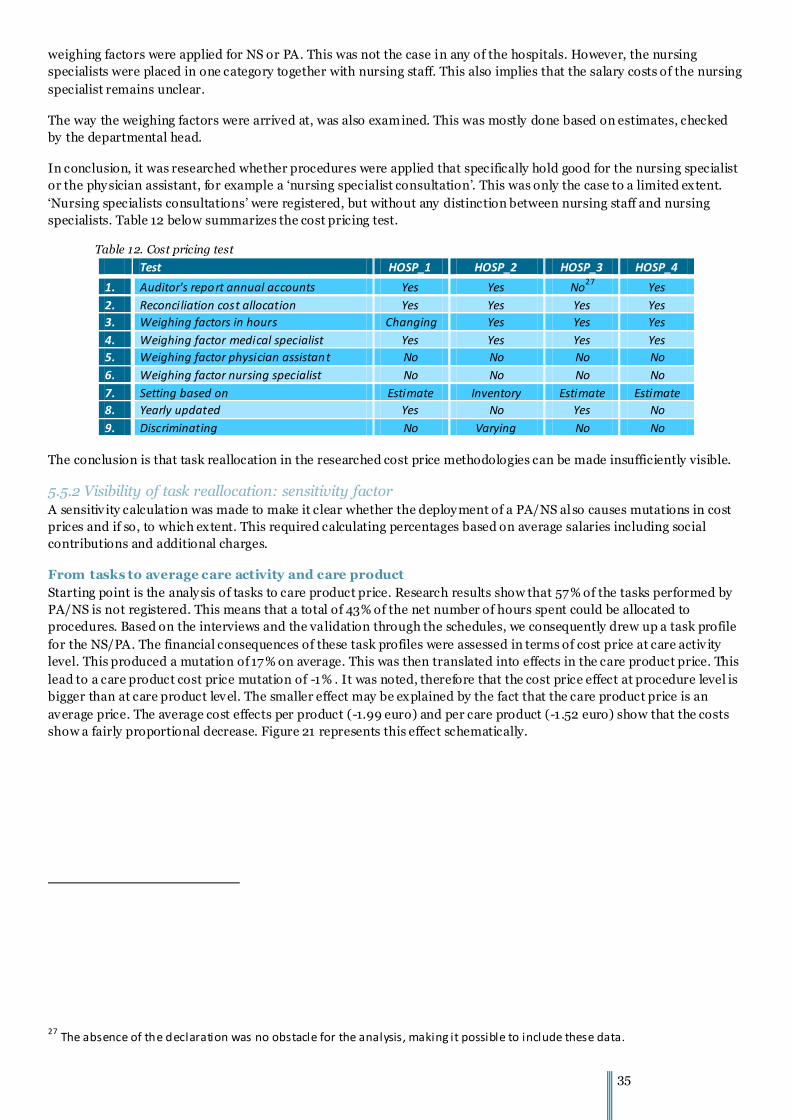
35
weighing factors were applied for NS or PA. This was not the case in any of the hospitals. However, the nursing
specialists were placed in one category together with nursing staff. This also implies that the salary costs of the nursing
specialist remains unclear.
The way the weighing factors were arrived at, was also examined. This was mostly done based on estimates, checked
by the departmental head.
In conclusion, it was researched whether procedures were applied that specifically hold good for the nursing specialist
or the phy sician assistant, for example a ‘nursing specialist consultation’. This was only the case to a limited extent.
‘Nursing specialists consultations’ were registered, but without any distinction between nursing staff and nursing
specialists. Table 12 below summarizes the cost pricing test.
Table 12. Cost pricing test
Test HOSP_1 HOSP_2 HOSP_3 HOSP_4
1. Auditor's report annual accounts Yes Yes No27
Yes
2. Reconciliation cost allocation Yes Yes Yes Yes
3. Weighing factors in hours Changing Yes Yes Yes
4. Weighing factor medical specialist Yes Yes Yes Yes
5. Weighing factor physician assistant No No No No
6. Weighing factor nursing specialist No No No No
7. Setting based on Estimate Inventory Estimate Estimate
8. Yearly updated Yes No Yes No
9. Discriminating No Varying No No
The conclusion is that task reallocation in the researched cost price methodologies can be made insufficiently visible.
5.5.2 Visibility of task reallocation: sensitivity factor A sensitiv ity calculation was made to make it clear whether the deploy ment of a PA/NS al so causes mutations in cost
prices and if so, to which extent. This required calculating percentages based on average salaries including social
contributions and additional charges.
From tasks to average care activity and care product
Starting point is the analy sis of tasks to care product price. Research results show that 57% of the tasks performed by
PA/NS is not registered. This means that a total of 43% of the net number of hours spent could be allocated to
procedures. Based on the interviews and the validation through the schedules, we consequently drew up a task profile
for the NS/PA. The financial consequences of these task profiles were assessed in terms of cost price at care activ ity
level. This produced a mutation of 17% on average. This was then translated into effects in the care product price. This
lead to a care product cost price mutation of -1% . It was noted, therefore that the cost price effect at procedure level is
bigger than at care product level. The smaller effect may be explained by the fact that the care product price is an
average price. The average cost effects per product (-1.99 euro) and per care product (-1 .52 euro) show that the costs
show a fairly proportional decrease. Figure 21 represents this effect schematically.
27 The absence of the declaration was no obstacle for the analysis, making it possible to include these data.

36
Figure 21. Effect of task reallocation in care activities and care product price
The same effect was calculated per hospital. This is shown in table 13. In all hospitals a cost price effect can be
observed, both positive and negative, depending on the exte nt of reallocation. It should be noted that the other tasks
were not included. This makes for an incomplete picture as the calculations do not include a fairly large part of the
tasks performed.
Table 13. Effect of task reallocation in care activities and care product price
A B C D
HOSP # Other task
Task reall
Task del
Add task TK_% ZA-% ZP_% Per ZA Per ZP
1 16 55.36 % 25.80
% 2.88
% 15.95
% -0.40 -31.99 -0.48 -1.25 0.06
2 7 49.34 % 40.14
% 1.35
% 9.17 % -0.51 -4.06 -0.46 -3.75 -0.31
3 11 60.15 % 20.43
% 4.73
% 14.68
% 0.03 % 5.54 % -0.27 -2.59 0.36
4 15 62.24 % 20.48
% 3.06
% 14.22
% -2.00 -35.33 -3.56 -0.37 -6.18
Av. 12 56.77 % 26.71
% 3.01
% 13.51
% -0.72 -16.46 -1.19 -1.99 -1.52
Finally, it was also noted that over 32% of the procedures no cost prices are calculated, while healthcare professionals
themselves indicate that they carry out activ ities in these procedures. The calculations were corrected for this fact.
Table 14 provides an overview per hospital.
Table 14. Number of procedures without cost price calculations
Total 1 2 3 4 Av.
Unique procedures 134 77 40 71 81
With cost price 99 64 32 25 55
Percentage 74 83 80 35 68
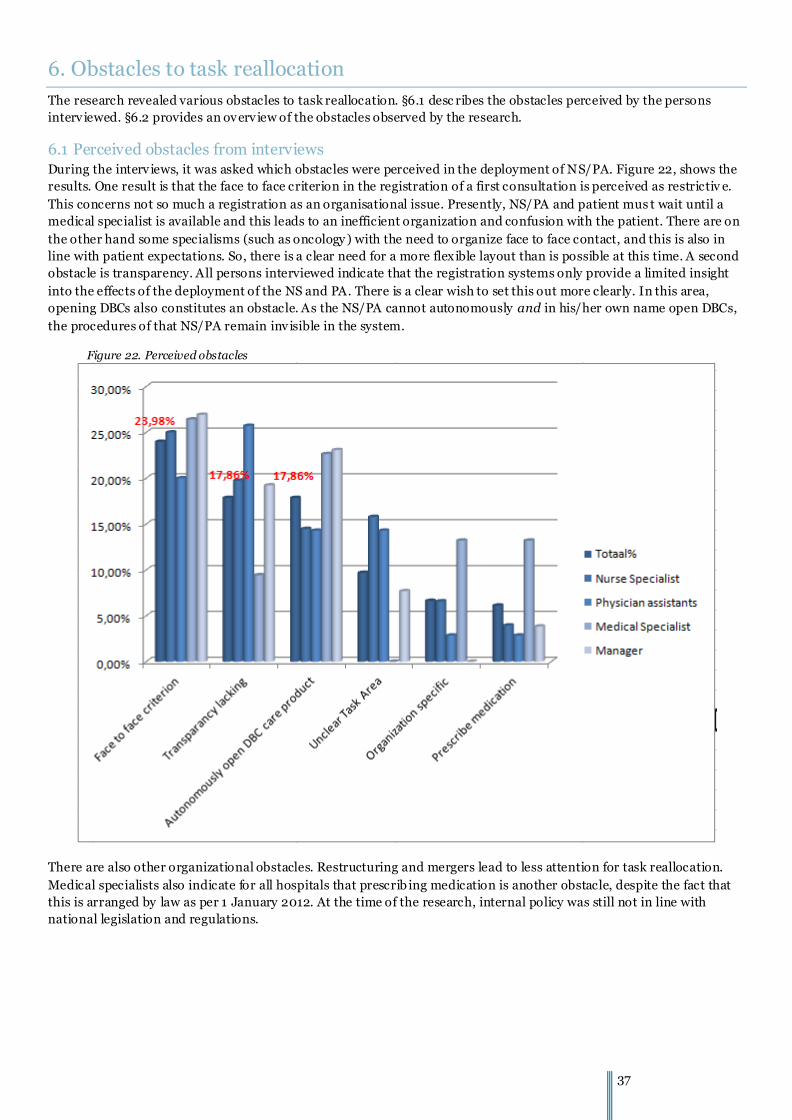
37
6. Obstacles to task reallocation
The research revealed various obstacles to task reallocation. §6.1 desc ribes the obstacles perceived by the persons
interv iewed. §6.2 provides an overv iew of the obstacles observed by the research.
6.1 Perceived obstacles from interviews During the interv iews, it was asked which obstacles were perceived in the deployment of NS/PA. Figure 22, shows the
results. One result is that the face to face criterion in the registration of a first consultation is perceived as restrictiv e.
This concerns not so much a registration as an organisational issue. Presently, NS/PA and patient mus t wait until a
medical specialist is available and this leads to an inefficient organization and confusion with the patient. There are on
the other hand some specialisms (such as oncology ) with the need to organize face to face contact, and this is also in
line with patient expectations. So, there is a clear need for a more flexible layout than is possible at this time. A second
obstacle is transparency. All persons interviewed indicate that the registration systems only provide a limited insight
into the effects of the deployment of the NS and PA. There is a clear wish to set this out more clearly. In this area,
opening DBCs also constitutes an obstacle. As the NS/PA cannot autonomously and in his/her own name open DBCs,
the procedures of that NS/PA remain inv isible in the system.
Figure 22. Perceived obstacles
There are also other organizational obstacles. Restructuring and mergers lead to less attention for task reallocation.
Medical specialists also indicate for all hospitals that prescrib ing medication is another obstacle, despite the fact that
this is arranged by law as per 1 January 2012. At the time of the research, internal policy was still not in line with
national legislation and regulations.

38
6.2 Obstacles observed in the research Within the research into registration sy stems , various obstacles were noted that confirm the statements by the
persons interviewed. Below you will find a description.
Transparency of activities
A large part of the activ ities cannot be registered as there are no procedures for those activ ities. This complicates
creating insight into the effectiveness potential of the NS/PA. This transparency is also partly missing in cost pricing,
the allocation of costs and the effect in the cost price of DOT care pro ducts.
In order arrive at a comprehensive cost price, the remuneration costs of partnerships are also required. Hospitals do
not (yet) have insight in this aspect as they are separated up to this time. This impedes a clear v iew of effectiveness.
Legislation and regulations and the professional standard
The face to face criterion, mandatory in the registration of the first consultation, constitutes an obstacle with the
majority of the specialisms. According to the interv iewed medical specialists and NS/PA, a first consultation could be
performed autonomously by an NS/PA in a large number of specialisms.
The professional standard, formulated by the scientific occupational groups, in many cases still requires the presence
of a medical specialist, despite the legal powers of the NS/PA. In addition, this standard also sets the number of
procedures a medical specialist must perform: the volume standard. In a tight labour market, such standards may
impede the further implementation of task reallocation. We do note that with an increasing number of scientific
societies, PA/NS also take part in workgroups.
Comprehensive pricing 2015 will eliminate a number of obstacles (face to face criterion, autonomously opening DBCs
and separate financing). This step, however, also creates uncertainty concerning healthcare funding, which among
others leads to more reluctance with respect to the deploy ment of NS and PA. Task reallocation is impeded by the fear
of loss of income. As soon as task reallocation is applied for purposes of income policy with respect to medical
specialists, it will become an obstacle in itself.
Arrangem ents between the Board of Directors and Partnerships
(Internal) arrangements between partnerships and the hospital constitute an important factor for the deploy ment of a
phy sician assistant. In some cases it was observed that such arrangements hamper the reallocation of tasks towards
phy sician assistant as the hospital makes no financial contribution to the deploy ment.
Inter-colleague consultations option
The availability (and therefore the option of inter-colleague consultation) of the medical specialist constitute an
important condition for the success of the NS/PA and the reallocation of tasks. The absence thereof may be regarded
as an obstacle.
6.2.1. Task reallocation advice NZa In its task reallocation advice, the NZa signals a number of obstacles to task reallocation. This particularly concerns
opening DBCs autonomously, the face to face criterion and the distinction between the cost component and the
remuneration part. Therefore, the NZa recommended the following measures to the Minister in 2012: 28
28 Dutch Healthcare Authority, Advice task reallocation in secondary somatic care and curative mental healthcare, Utrecht, 2012 .

39
- The intention to arrive at comprehensive performance and pricing in 2015, will have a positive effect on task reallocation.
- NZa recommends to extend the list of care providers that may open a care process.
- NZa also recommends to let go of the obligation of face to face contact with a gatekeeper specialist on a outpatients' department v isit and to broaden this with a face to face contact with an NS and/or PA.
7. Discussion (research reservations)
An important premise in this research is the definition of task reallocation, task delegation and additional care. The
interv iews included questions about the estimated deployment and the answers were then submitted to the medical
specialist involved. Although the estimates are quite rough, they are indicative for the practice. The estimates were
checked additionally based on the schedule data for that matter, although this does not change their indicative nature.
Because of the limited research time, we did not opt for an additional validation through time clock measurements.
A wide deployment variety was observed in practice. Nursing specialists and physician assistants within one and the
same hospital are deployed in various manners, possibly leading to a large diversity in terms of deploy ment per
hospital on national level. With independent treatment centers (ZBC) for instance in oncology, the deployment of
NS/PA may deviate from what we have noted in hospitals in this research.
Within the research population, one university medical center was researched. This is not entirely comparable with
other hospitals due to the differences in cost price calculation, culture but also with respect to the v ision on the
deployment of the PA and NS. In addition, it is our experience that medical specialists in salaried employ ment versus
those in partnerships have a different attitude towards the deployment of NS/PA. In partnerships, the business case
played a more central role; the extent of task reallocation is also determined by financial interests. The interests of the
partnership may be inconsistent with those of the occupational group NS/PA. Whatever the case, in departments with
medical specialists in salaried employment less (financial) obstacles were noted.
A related factor thereto are the arrangements between the hospitals and partnerships on the employment of NS/PA
and the mutual set-off of costs. Despite qualitative arguments in favour of the deployment, this financial argument,
may impede an optimum task reallocation. Another factor is the fear of financial measures with some specialists
(lowering the turnover ceiling) and the fact that this fear may have influenced the research outcomes.
A limited sample survey of four hospitals was opted for. On the one hand, such an in-depth survey has its advantages,
on the other hand it may limit the conclusions on a national level. A positive effect is that the differences between
hospitals are such that the research shows sufficient diversification in terms of deployment of NS/PA.
This research focuses on the financial effects of the deploy ment of the NS/PA in hospitals. The effects on the quality of
healthcare were not examined. An important question in this respect is how the pa tient feels about the deploy ment.
Particularly the extra provision of information, psycho -social counselling but also the presence of a second
occupational group next to the medical specialist may have a positive effect on the way the quality of care is perceived.

40
8. Conclusions and recommendations
Task reallocation, in this case the task reallocation between medical specialist and phy sician assistant and/or nursing
specialist, is, as we have observed, a sy mbiosis between two occupational groups. One cannot do without the other.
This makes it more than just a reallocation but more a cooperation relation.
We have come to this conclusion as the practice shows a wide variation in the way s in which physician assistants and
nursing specialists are deployed. We have not been able to note a direct relation between the scope of the reallocated
tasks and the number of years since the graduation of the healthcare professional. Apparently, there are other factors
that play a bigger part in the reallocation of tasks. It became clear from the interv iews that trust, competencies and the
development of the individual healthcare professional play an important role in the div ision tasks.
The motivation most mentioned for the deployment of a phy sician assistant and nursin g specialist is improvement of
the quality of the (chain) care, in which low-threshold care for the patient is an important outcome. This also leads to
increased effectiveness as the deploy ment enables the medical specialist to better focus on his field of expertise:
complex care issues. In many cases the interviewed medical specialists also indicated that the healthcare landscape
cannot do without physician assistants and nursing specialists.
The interv iews also revealed an increasing demand for informatio n concerning the (accessibility of) healthcare. It was
repeatedly indicated that the tasks of the medical specialist are changing. This concerns the i ncrease of administrative
tasks, quality registrations and data that needs to be supplied within the frame work of the standards of occupational
groups. Tasks that are largely reallocated to nursing specialists and physician assistants.
Furthermore, it is noted that nursing specialists are more active in chain care, in which the term ‘case manager’ often
comes up. They organize care in a low-threshold manner and make important contributions to the quality of
healthcare in specific subareas in which they are experts. Phy sician assistants are deployed from a broader medical
perspective, as ward doctor or in a combination of ward doctor, outdoor department and/or surgical interventions in
areas with relatively low complexity.
We have also observed that the inter-colleague consultations option of the medical specialist remains important and
that in the performance of the procedures a medical specialist should always be available (on call). Superv ision is
required during the introductory period. The performance requires preliminary and subsequent talks until the trust in
and the competencies of the NS/PA are such that the procedures concerned can be carried out autonomously. In the
resulting situation, the medical specialist will only be consulted with a limited number of patients and a short approval
will suffice to start a treatment for example. The supervising role o f the medical specialist cannot be registered with
the current procedure system, although this is relevant to cost pricing.
Only a very limited number of interviewed persons applied a clear -cut business case for the deployment of NS or PA,
in which the effectiveness was also included as important decision factor. Most of time it is assumed without clear
substantiation that the deployment of an NS/PA will eventually lead to effectiveness. With partnerships, the business
case is applied more prominently.
The lack of information is also evidenced by our other findings. Neither the procedure registration nor the cost price
calculation provide insight into the effects of the deploy ment of NS/PA. Therefore, we also note that the deploy ment
becomes insufficiently visible in the registration systems currently applied. This answers the first research question (In
which manner is the deployment of the physician assistant and nursing specialist accounted for in the cost prices of
DBC Care products?)
That reallocation to a high degree is possible, however, is apparent from various practical examples. These practical
examples show that medical specialists and NS/PA approach each other critically and the NS/PA eventually develop
into specialists in healthcare subareas.
(Internal) arrangements between partnerships and the hospital constitute an important factor for the deploy ment.
Partnerships and the hospital make arrangements about the way in which task reallocation is financed: by the hospital
or the partnership. In some cases it was noted that mutual arrangements between partnership and hospital impeded
the reallocation of tasks toward the physician assistant. Partnerships turned out to choose for a nursing specialist as
the hospital partly reimbursed them for the costs.
41
There is also mistrust against (the upcoming change in) the financial system that may once again lead to reductions
when the task reallocation is further implemented. Literal quotes from interviews we conducted with medical
specialists in this area:
“We are responsible for the care process and supervise and this means that we should receive a financial
remuneration.”
“We physicians are unsure about the future. Medical specialists are also aware of labour market surpluses.”
On the other hand, many medical specialists also come up with positive statements. For example:
“When my child needs to go to hospital, there is no doubt in my mind who should be at his bed; the nursing
specialist.”
“The physician assistant keeps me on my toes and he can do a number of treatments better than me.”
These quotes illustrate the two sides of task reallocation. It is important to maintain a clear distinction between those
two sides. For when task reallocation is deployed for income politics, this will influence the further deployment of NS
and PA negatively.
Our advice is the improve the provision of information concerning task reallocation and effectiveness potential. The
field (medical specialist and healthcare professionals) clearly lacks the support to make task reallocation v isible. When
we consider the cost price methodology, it is of importance to apply the right weighing factors and to make it possible
to register procedures tailored to the deployment of NS/PA.
Further development of the presented toolbox and testing the effect comprehensive funding could contribute to
making the effect of task reallocation more v isible.

42
Detail Conclusions
Task reallocation in practice C1 It is clear from practice that there is a lot of variation in the way NS/PA are deployed. The ext ent of task reallocation , task delegation and other tasks varies per healthcare professional. This variance is party explained by the nature of the
specialism, personal competencies and the trust of the medical specialist in the quality of care supplied. C2 A large part of the activ ities of the PA/NS cannot be registered as many tasks concern tasks that go beyond the specialism, are aimed at chain care and quality improvements. On average, 57% is not registered from a financial perspective with respect to their production contribution. This 57 % may be reallocated tasks that simply cannot be
registered. These tasks consist of: Patient-based tasks
1. Administrative and planning tasks (communication, GP, nursing home DICA questionnaires, etc.)
2. Non-registered telephone consultations 3. Quality / development care processes
4. Expertise promotion (training departmental nursing staff, protocols) 5. Provision of information/ patient instruction (additional accessibility by
telephone) Non patient-based
6. Education 7 . Research
8. Projects (national development directive) 9. Participation committees (hospital or national level)
Allocation of the patient-based tasks would entail a decrease of 26.22% in other tasks, which currently cannot be allocated.
C3 The nursing specialist indicates to carry out more administrative tasks than a phy sician assistant, who often takes over more tasks directly from the medical specialist. C4 Both the physician assistant and the nursing specialist are scheduled for a longer period of time for a first consultation or a follow-up consultation than a medical specialist. This is on average 7 .5 minute extra for the physician assistant
and 15 minutes for the nursing specialist. C5 In the deployment of PA and NS, medical specialists perceive a quality improvement of patient care and increased care accessibility , particularly concerning the provision of information to the patient. C6
In most cases it is matter of full substitution as there is also the superv ision and availability of the medical spec ialist involved. Usually, a slow decrease of supervision time can be observed. In the most optimum form of task reallocation, there is a short feedback (on average 6 minutes per patient), in which the medical specialist approves the start of the treatment. C7
According to most interv iewed medical specialists, the PA and NS have become indispensable in the current care landscape; they perform less complex protocolled tasks but also make an important contribution in meeting the increase in demand for care and the information needs of the patient and increasingly organize the healthcare provided. C8 There are specialisms in which task reallocation is implemented ‘easier’ and to a further extent than is the case with
other specialisms. For example, oncology and surgery processes are particularly started by the NS and/or PA in various hospitals (further analysis has to show how relative this is).

43
Task reallocation & cost prices C9 In all four hospitals, the deploy ment of the PA/NS is insufficiently reflected in cost prices. It is not possible to make (the registered procedures) production visible. One hospital applied internal ‘dummy codes’ to be able to v isualize the
consultations at the level of nursing specialists. C10 The allocation of costs varies at department level. If weighing factors are used, these are not up to date and of vary ing quality.
C11 NS/PA significantly contribute to procedures in first and follow-up consultations which, at this time, are mainly performed and registered in the name of the medical specialist. C12 Analy sis by means of the toolbox shows that the effect of task reallocation in DOT care products is reduced because the average cost price is set based on all products. Where task reallocation is v isible, structural cost saving s are realized.
C13 As a separate funding structure is applied (remuneration part and hospital part) the real effectiveness cannot be made v isible for three hospitals. Remuneration costs are not included in the cost price of procedures. C14 The registration of procedures is not unambiguous. It is not alway s clear to the NS/PA what can be registered, as a
result of which it is not transparent which activ ities are performed by the PA and/or NS. C15 Departmental heads and medical specialists state three reasons for the deploy ment of nursing specialists and phy sician assistants:
- Quality improvement in the chain care: provision of information and improved psycho -social counselling of
patients. - Continuity in departments: as an assistant phy sician is only in a department for a limited period of time, the
present expertise varies. The nursing specialist / physician assistant, on the other hand, can guarantee the continuity of service and quality.
- Reliev ing the medical specialist, so that he or she can focus on complex health issues.
C16 A physician assistant focuses on a broad range of medical procedures and can take over more tasks from the medical specialist that can be registered in procedures. As a result the detectable reallocation is larger with this group. C17
The instruments to carry out solid costs-benefit analy ses are limited.

44
Obstacles B1 A large part of the activ ities of the PA and NS cannot be registered, so that the contributions by the PA and NS cannot be made visible. This also obscures the v iew of departments what the effectiveness potential of the deploy ment is. With
some partnerships this has lead to a decreased deployment and/or the consideration not to extend this. B2 Task reallocation is only visible to a limited extent in the cost pr ices by the varying way s in which cost pricing is realized, even within the hospitals themselves. In the application of weighing factors as well, nursing specialists are placed alongside nursing staff in one and the same factor, creating insufficient diffe rentiation to make task reallocation
transparent. B3 The face to face criterion, mandatory in the registration of the first consultation, constitutes an obstacle with the majority of the specialisms. According to the medical specialist and the healthcare professionals, a large number of specialisms may well be performed by an NS/PA.
B4 In order arrive at a comprehensive price, the remuneration costs of partnerships are also required. Hospitals have no insight in the salary costs of medical specialists, the partnerships do. This may be an obstacle to map the effectiveness. B5 The professional standard, formulated by the scientific occupational groups, requires the presence of a medical specialist. In addition, there are volume standards for the number of procedures a medical specialist must perform. In
a tight labour market, these standards may impede further task reallocation. B6 (Internal) arrangements between partnerships and the hospital constitute an important factor for the deploy ment of a phy sician assistant. In some cases it was observed that such arrangements hamper the reallocation of tasks towards phy sician assistant as the hospital makes no contribution to the partnership.
B7 Task reallocation is impeded by sentiments and fears concerning expected lower income should task reallocation become v isible. As soon as task reallocation is applied for income policy purposes, it will become an obstacle in itself. B8 Supervision by and the availability of the medical specialist constitutes an important condition for the success of the
healthcare professionals and the reallocation of tasks. The absence thereof may be regarded as an obstacle. B9 Nursing specialists and phy sician assistants fail to see the importance of a good registration.

45
Recommendations A1 Ensure the differentiation of procedures so that the (internal) registration sy stem shows the (financial) effect of that
deployment; this would be possible by having care-related tasks registered through a separate procedure and care
activ ity to be able to make it transparent which effectiveness is realized with respect to a procedure performed by a
medical specialist.
A2 For hospitals is it recommended to take the following steps to improve the v isibility of task reallocation:
1. Asses the procedures and review the applied weighing factors 2. Validate the weighing factors in at least two ways (schedule / medical specialist) 3. Apply the same weighing factors for each department (to realize comparability) 4. Register a nursing specialist consultation and a physician assistant consultation and where possible extra procedures that are applicable
5. Calculate the cost prices concerned at procedure level, in which the salary costs of both groups are applied. 6. Compare the cost price of a MS c onsultation with the NS/PA consultation to gain insight into effectiveness potential. A3
Expressing the deployment of PA/NS in the cost price is only possible if the activities of the medical specialist that are related to the procedure are also included. This would produce a good balance between superv ision and autonomous deployment. A4 The face to face criterion should be eliminated with respect to the nursing specialist and phy sician assistant. In this respect, it is important that the medical specialist can still decide whether and where in the process he or she will see
the patient. A5 it should be clear to both the hospital and the partnership what the comprehensive cost price of a procedure is. These are needed to support decision-making concerning the deployment of this occupational groups by including the remuneration costs in the comprehensive price.
A6 The professional standard should be the guiding principle for the different healthcare professionals. In this respect it is important that this ties in with the daily practice and options concerning the deployment of PA and/or NS. Review these standards so that the deployment of PA/NS is not hindered by standards that do not tie in with the (daily) practice and options.
A7 The positive effect of the deployment of PA/NS should stimulate the hospital and partnership to further implement task reallocation in the future. Clear arrangements between the hospital and partnership about the remuneration of both parties is of v ital importance in this respect. For example, it can be ensured that both PA and NS have the same offset methodology. A8
Hospital and partnerships should (continue to) be able to decide themselves on the deploy ment of NS/PA. However, it must remain appealing to both parties to deploy this group. This may be done on the basis of quality considerations of from the perspective of effectiveness potential, but it must always be a clear choice by both parties. Hospitals and partnerships may stimulate the attractiveness by internally formulating this quality or effectiveness consideration in concrete policy.
A9 The inter-colleague consultations option and supervision of the NS and/or PA by the medical specialist must be included in the calculation of the cost price so that this deploy ment by the medical specialist becomes transparent. This may be realized by a weighing factor that can be applied or through a correction in the allocation of salary costs. A10 Apply the toolbox through which task reallocation may be made visible in a transparent way and a business case may
drawn up based on costs and proceeds in the broadest sense. A11

46
The effect of comprehensive prices (and all other measures) may be substantial in 2015. It is recommended to carry out a resurvey to measure the state of reallocation following these measures.
A12 More awareness should be created with both the medical specialist and NS/PA concerning the role they play in terms of financial aspects and the importance of their visibility in this.
A13 To be able to make a better comparison, the activities of the medical specialists should also be mapped. A14 Improve the provision of information with respect to task reallocation so that the effects become clear. This would
stimulate the deploy ment of NS and PA in an unambiguous manner.
A15
Carry out further studies of the ‘other activ ities' and also involve medical specialist activ ities so that a comprehensive (and comparable) picture emerges of non-registered activities. A16 Work out some three business cases to further develop and validate the toolbox so that a picture of task reallocation and its effects is created at various levels (department, specialism).
Appendix 2 provides a summary of these recommendations.

47
Definitions
Additional care Extended or added tasks from the own profession or increase in demand for care.
Gross-net factor The measurement that represents the ratio between the gross number of hours as included in the
employment contract and the net number of hours that an employee may actually be deploy ed. These constitute the
deployment hours.
CBV procedure Healthcare classification and coding system applied by some forty hospitals to record healthcare
data within the healthcare sector. The CBV filing system comprises 55,000 different procedures.
DBC care product A DBC care product is a chargeable performance derived from a sub process and care activ ities
according to decision trees set by the NZa.
Remuneration am ount The maximum amount (per care product) that may invoiced as compensation for the
services of a medical specialist. Whether or not in combination with the cost component it constitutes the tariff per
care product.
Comprehensive cost prices The (comprehensive) cost price of a product or service consists of the total costs
incurred for producing that product or providing that service.
Cost component The maximum amount per (regulated) care product that may invoiced as compensation for
institution costs. Whether or not in combination with the remuneration amount it constitutes the tariff per care
product.
Cost unit A unit to which costs are allocated.
Cost price The costs related to performing certain care activ ities or care products with allocation in accordance with
the cost price model.
Task delegation Non-structural reallocation of tasks; tasks are carried out as commissioned and under superv ision.
The responsibility remains with the delegation by the medical specialist.
Task reallocation Structural reallocation of tasks to occupational groups.
Allocation of tasks Manner in which tasks are reallocated. In this research, the term refers to the distinction
between reallocated, delegated or additional care tasks.
Care activity The building blocks of a DBC Care product and jointly the profile of a DBC care product.
Care profile A collection of care activities that belong to a care product is called the care profile of a care product.
Supervision Indiv idual learning process directed by a superv isor. This concern a form of expertise promotion aimed
at reflecting at the own way of working.

48
Reference list
M. Berg, W. Schellekens, C. Bergen, Over de kwaliteitskloof: naar een integratie van professionele en bedrijfskundige
kwaliteit. Medical Contact 2003; 58 (49): 1907 -10.
J.L.T. Blank en E. Eggink, Productiviteitstrends in de ziekenhuiszorg. Een empirisch onderzoek naar het effect van
regulering op de productiv iteitsontwikkeling tussen 1972 en 2008. IPSE Studies, Technical University/The
Netherlands Institute for Social Research(SCP), 2011.
CIBG v ia http://www.bigregister.nl W. Editors. Primary care in the driver's seat? Organizational reform in European primary care, Berkshire, England, Open University Press; 2006.
First Chamber of Parliament (2011). Wijziging van de mogelijkheid tot taakherschikking in de Wet beroepen
indiv iduele gezondheidszorg, 16 December 2013 based on http://www.eerstekamer.nl /wetsvoorstel/
32261_wijziging_van_ de_mogelijkheid_tot_Taakherschikking_ in _de_Wet_ beroepen_ indiv iduele
gezondheidszorg.
Evaluation Committee Comprehensive Funding (2012), Integrale bekostiging van zorg : Werk in uitvoering: Eindrapport van de Evaluatiecommissie Integrale Bekostiging, June 2012, The Hague. I. Heath, Skill mix in primary care. British Medical Journal 1994; 308: 993-4. 4.
G.J. Kommer, A. Wong en L.C.J. Slobbe; Determinanten van de volume groei in de zorg, Letter Report 270751021/2010, RIVM, commissioned by the Ministry of VWS, Bilthoven : National Institute for Public Health and the Environment (RIVM), (2010). L.J.R. van der Meulen, A. Beldman en A.J.J. van der Kwartel. Productiv iteitswinst in de Zorg. Who gets what, when
and how. Kiwa Prismant, 2012.
Council for Public Health and Care, Taakherschikking in de gezondheidszorg,
Zoetermeer, RVZ, 2002. B. Sibbald, M. Laurant, T. Scott, Changing task profiles. In: Saltman A, Rico A, Boerma A.C.S. Goossensen, Taakherschikking in de praktijk; anders werken in het Erasmus MC; Medisch Contact 2005; 60 (19);816-824.
G. Richardson, A. Maynard, N. Cullum, D. King, Skill mix changes: substitution or serv ice development?, Health Policy 1998; 45 (2): 119-32. Van der Velde, F., Van der Windt, W., Alumni van de Masteropleiding Advanced Nursing Practice, , Dutch Capacity
Organ (Capaciteitsorgaan) Utrecht, March 2013.
Van der Velde, F., Van der Windt, W., Alumni van de Masteropleiding Physician Assistant, Capaciteitsorgaan,
Utrecht, March 2013.
Dutch Healthcare Authority, Advies Taakherschikking in de tweedelijns somatische zorg en curatieve geestelijke
gezondheidszorg, Utrecht 2012. Dutch Healthcare Authority (NZa), Beleidsregel BR/CU 2104 Prestaties en tarieven medisch specialistische zorg, Utrecht 2013. Dutch Healthcare Authority (NZa) (2012), Toelichting op de honorariumberekening DBC-Zorgproducten 2013,
Utrecht.
Dutch Healthcare Authority (NZa), Nadere Regel NR/CU-228, Regeling medisch specialistische zorg, Utrecht 2013.
Dutch Healthcare Authority (NZa), Nadere Regel NR/CU-235, Regeling registratie en aanlevering kostprijzen
zorgproducten medisch specialistische zorg, Utrecht 2012.

49
Dutch Healthcare Authority (NZa), Verantwoordingsdocument Prestatiebekostiging Medisch Specialistische zorg,
uitwerking van de implementatie, Utrecht 2012.
Harmsen, M., Laurant M. et al (2007), Effecten van taakherschikking in de gezondheidszorg: literatuuronderzoek, Nijmegen.
Kwaliteitskoepel Medisch Specialisten (2013), Richtlijnen, 15 November 2013 based on http://www.kwaliteitskoepel.nl/kwaliteitsbibliotheek/a_z_index/. Kwaliteitskoepel Medisch Specialisten (2013), Minimale voorwaarden HHOC, 16 November based on
http://www.kwaliteitskoepel.nl/assets/structured-files/Normen/ minimale_voorwaarden_HHOC.pdf.
KPMG, V&VN en NAPA, Handreiking ‘verantwoordelijkheidsverdeling bij samenwerking in de zorg’ , 2012.
G. Ligtenberg (2012), Voorwaardelijke toelating/financiering van zorg, CVZ, April 2012, issued to the Minister of VWS, Diemen; Healthcare Insurance Board (CVZ). Ministry of VWS (2012), Naar beter betaalbare zorg: Rapport Taskforce Beheersing Zorguitgaven,
June 2012, The Hague: Ministry of Health, Welfare and Sport. Morris, Devlin, Parkin et al (2007), Economic Analysis in Health Care, John Wiley & Sons ltd. National Institute for Family Finance Information (Nibud) (2003). Normering Chirurgische behandelingen 3.0
(bariatrische chirurgie), Een onderzoek naar de kosten van kinderen in grote gezinnen. 22 May 2006 based on
http://www.nibud.nl/docs/grotgezi.pdf.
Dutch Association of Physician Assistants (2007), Beroepsprofiel voor de Phy sician Assistant . Dutch Society of Cardiology (NVvC), Volume normen cardiologie, June 2011.
Dutch Society of Radiotherapy and Oncology (NVRO), Kwaliteitsnormen Radiotherapie in Nederland versie 2.0, 30
November 2012.
Dutch Society of Obstetrica and Gy naecology (NVOG), Richtlijnen 2013, on 16 November based on http://nvog-
documenten.nl/index.php?pagina=/richtlijn/ pagina.php&fSelectNTG_ 68=80&f SelectedSub=68.
Dutch Society of Urology (NVvU), Kwaliteitsnormen, April 2013.
Platform NS and PA (2012), Phy sician assistants en verpleegkundig specialisten wettelijk op eigen benen, Nijmegen. Overheid, Wet Mededinging Gezondheidszorg, 16 December 2013 based on
http://wetten.overheid.nl/BWBR0020078/.
Council for Public Health and Care (2002), Taakherschikking in de gezondheidszorg, Zoetermeer
Schippers E.I. (2013), Herziening Zorgstelsel (29_689), Preliminary Letter no. 437 to the Chairperson of the Second Chamber of Parliament, The Hague. Staatsblad, 2011, no. 658 and 659. Foundation Oncological Cooperation (SONCOS), Standards document (2013). Multidisciplinaire normen
oncologische zorg in Nederland. Op 17 November 2013 based on http://www.soncos.org/
Nursing Professions Structure and Training Center (VBOC), Algemeen competentieprofiel en specifieke deelprofielen
verpleegkundig specialist, Work group ‘competency profile nursing specialist’, Utrecht, (2008). F.F. Asselman, Kostprijzen in ziekenhuizen, Bohn Stafleu van Loghum Houten, 2008 S. Visser, R. Westendorp, K. Cools [et al.], Kwaliteit als medicijn: Aanpak voor betere zorg en lagere kosten, Booz & Company Amsterdam, (2012).

50
Appendix 1. Summary reserved procedures


Physicians pursuant BIG
Act
NS acute care
with somatic
conditions
NS chronic care
with somatic
conditions
NS preventive
care with somatic
conditions
NS intensive care
with somatic
conditions
NS mental
healthcare
PA
. Carry out surgical procedures
. Carry out obstetric procedures
. Perform endoscopies
. Perform catheterizations
. Giv ing injections
. Perform punctures
. Anesthetization
. Perform procedures in the area of
indiv idual healthcare with the use
of radioactiv e substances or
equipment emitting ionising
radiation
. Perform electiv e cardiov ersion
. Apply defibrillation
. Apply electroconvulsion therapy
. Apply rock crushing for medical
purposes . Perform procedures with respect
to human gametes and embry os
with another aim than realizing
pregnancy in a natural way
. Prescribe UR medication
. Carry out surgical procedures
. Perform
catheterizations
. Giv e injections
. Perform punctures
. Apply defibrillation
. Prescribe UR
medication
. Carry out surgical procedures
. Perform
catheterizations
. Giv e injections
. Perform punctures
. Perform endoscopies
. Prescribe UR
medication
. Giv e injections
. Prescribe UR
medication
. Carry out surgical procedures
. Perform endoscopies
. Perform catheterizations
. Giv e injections
. Perform punctures
. Perform electiv e
cardiov ersion
. Apply defibrillation
. Prescribe UR medication
. Giv e injections
. Perform punctures
. Apply defibrillation
. Prescribe UR medication
. Carry out surgical procedures
. Perform endoscopies
. Perform catheterizations
. Giv e injections
. Perform punctures
. Perform electiv e
cardiov ersion
. Apply defibrillation
. Prescribe UR medication
Appendix 2: Recommendations summarized per consultative group

1
Hospitals
V&VN / NAPA
NVZ
Nfu
VWS
NZa
ZN
OMS
Improv e registration concerning
procedures (unambiguous
registration, rationalise procedures)
(A1 , A2)
Improv e information
prov ision concerning
financing and registration
of procedures (A14)
Improv e prov ision of information concerning procedures/ financing and cost price calculations (A10, A14)
Improv e prov ision of information concerning procedures/ financing and cost price calculations (A10, A14)
Take other effects
into account that
may impede task
reallocation
(labour market,
remuneration
changes) (A8, A5,
A11)
Enable autonomous DBC opening (A1 , A11)
Open the discussion concerning task reallocation and ask for effects of task reallocation (A12, A14)
Support partnerships
with producing
comprehensiv e prices
and the relation to
task reallocation (A12,
A14)
Register a procedure ‘nursing
specialist’ consultation and
‘phy sician assistant’ consultation to
make the effectiv eness v isible (if
possible multiple procedures) (A1 ,
A2)
Support the role and
positioning of NS/PA for
their contribution to the
hospital proceeds by
offering methods that may
sh ow their contribution
(A14)
Pr ov ide information about the toolbox that is generally applicable for hospitals and univ ersity centers (A10, A14)
Pr ov ide information about the toolbox that is generally applicable for hospitals and univ ersity centers (A10, A14)
Facilitate the
transfer to
comprehensiv e
funding by
stimulating the
use of the toolbox
(A10)
Make healthcare and sub pr ocesses of PA /NS v isible by letting PA/NS generate new care activity (A1)
Guide toolbox use
by questioning
hospitals on this
Pr ov ide insight to
both parties (A10)
Pr ov ide information
about the toolbox that
is generally applicable
for partnerships in
hospitals (A10)
Update the applied weighing factors
(and create a weighing factor that
separates PA/NS) (A5)
Pr ov ide information about
possible obstacles
concerning medical
specialist remuneration
(A14)
Facilitate further
research of the
‘other activ ities’
(A13, A15)
Create separate care
activities for PA/NS so
that cost prices can be
calculated at ZA-lev el
(A1)
Pr ofessional
standards must tie in
with task reallocation
in practice (A6)
Improv e the way in which the weighing factors are established Apply minimally 2 validations of the hourly deployment (manager, schedule) (A2, A5)
Facilitate in-
depth research
into obstacles to
further dev elop
the tool (A16)
Enable comprehensiv e
pricing (A5, A11, A12)
Apply a correction on the weighing
factor for the ‘inter-colleague
consultations by medical specialist’
and deployment medical specialist
(A3, A5, A9)
Measure effects
comprehensiv e
pricing on task
reallocation (A11)
Eliminate the face to
face criterion (A4)
Calculate the effects of the
comprehensiv e funding for the
hospital based on care activ ities and
procedures (A5, A11, A12, A14)
Make clear arrangements about
registrations outside the specialism
(NS/PA often work for more
specialisms but cannot alway s

2
register this) (A5)
Rationalize the procedure filing
sy stem where possible (A5)
Make clear arrangements on the
reimbursement of PA/NS by
partnership and hospital Ensure that
the deployment of PA /NS is
stimulated (A7, A8)
In form partnerships
about the deployment
of PA/NS Stimulate
good arrangements
between partnership
and hospital
concerning
reimbursement (A12)
Reallocated activities that are not
registered by the medical specialist
sh ould be inv entoried to get a
complete picture (A13, A15).
Determine for hospitals with partnership, long before
comprehensiv e pricing, the
comprehensiv e cost price for
procedures (hon + hosp) to make
good internal arrangements (A5)