rashid hospital bariatric success story narrated by dr ali khammas md (sweden),swedish board
TRANSCRIPT
Rashid Hospital bariatric
Success story
Narrated by
Dr Ali KhammasMD (sweden),Swedish Board


SURGICAL PERSPECTIVE
Challenges in obese patients

anaesthesia
BMI and complicationComorbidities (need for mechanical vent)AirwayVascular accessBP cuffMedicationPost op pain

Surgical Tracheostomy


Radiology




In the OT




In the ward


Nursing

BENCHMARK ?
Challenges in bariatric surgery
An institutional experience with laparoscopic gastric bypass complications seen in the first year compared with open gastric bypass complications during the same period.
See C, Carter PL, Elliott D, Mullenix P, Eggebroten W, Porter C, Watts D.
General Surgery Service, Madigan Army Medical Center, Tacoma, WA 98431-5000, USA.
Abstract
BACKGROUND:Complication rates for laparoscopic bariatric surgery remain in evolution.
METHODS: Single institution review of the initial year's experience with laparoscopic gastric bypass compared with open gastric bypass complications for the same period.
RESULTS: There were 20 laparoscopic and 52 open gastric bypass procedures. Five
laparoscopic patients had major complications. There were 4 anastomotic leaks. Nine open bypass patients had major complications, with 2 leaks. Leak rate was 20% for the laparoscopic group and 4% for the open group. All leaks in both groups led to substantial morbidity. There were two deaths, one in each group. The laparoscopic death was from postleak sepsis.
CONCLUSIONS: Gastric bypass, whether done open or laparoscopically, has significant surgical risk. Complication profiles differed between the two groups. Anastomotic leaks were significantly more frequent in the laparoscopic group, probably related to the learning curve. There is a continued need for open surgery in many bariatric patients

Leveling the learning curve for laparoscopic bariatric surgery. Lublin M, Lyass S, Lahmann B, Cunneen SA, Khalili TM, Elashoff JD, Phillips EH.
Department of Surgery, Cedars-Sinai Medical Center, Los Angeles, CA 90048, USA.
Abstract
BACKGROUND: The learning curve for laparoscopic bariatric surgery is associated with increased morbidity and mortality.
METHODS: The study included the first 100 patients undergoing laparoscopic Roux-en-Y gastric bypass (LGB) by a designated surgical team. Surgeon A operated as primary surgeon, with surgeon B assisting (Stage 1). Surgeon B learned LGB in stages: exposure and jejunojejunostomy (stage 2), gastric pouch (stage 3), gastrojejunostomy (stage 4), and sequence all steps (stage 5).
RESULTS: Surgeon A achieved confidence with LGB after 20 cases and surgeon B after 25
cases (stage 2), 18 cases (stage 3), 21 cases (stage 4), and 16 cases (stage 5). Complications (8%) included small bowel obstruction (three); pulmonary embolus (two), and leak, stomal stenosis, and gastrogastric fistula (one each). There was a decreasing trend for operative duration, length of stay, and complications across the five stages (p < 0.05).

Single-stage laparoscopic sleeve gastrectomy: safety and efficacy in the super-obese. Lemanu DP, Srinivasa S, Singh PP, MacCormick AD, Ulmer S, Morrow J, Hill AG, Babor R, Rahman H.
Department of Surgery, South Auckland Clinical School, Middlemore Hospital, University of Auckland, Private Bag 93311, Otahuhu, Auckland, New Zealand. [email protected]
Abstract
BACKGROUND: Laparoscopic sleeve gastrectomy (LSG) is increasingly used as a single-stage bariatric procedure. However, its safety and efficacy in super-obese patients (body mass index [BMI] > 50 kg/m(2)) is less well defined. This series reports on 400 consecutive patients who underwent LSG at our institution, to evaluate safety and efficacy in the super-obese.
MATERIALS AND METHODS: We performed a retrospective review of prospectively collected data on
400 consecutive patients who underwent LSG at our institution. We analyzed baseline demographic data, median length of hospital stay, complications, length of follow-up, weight loss, and comorbidity resolution. We graded complications according to the Clavien-Dindo classification system. We classified patients as super-obese and non-super-obese and compared outcomes between groups. We used the two-tailed t-test and Fisher's exact test as necessary.
RESULTS: There were 400 patients, 291 of whom were female (73%). The mean age was 44 y (standard deviation [SD] ± 9 y). The mean preoperative weight and BMI were 140 kg (SD ± 31 kg) and 49 kg/m(2)
(SD ± 9 kg/m(2)), respectively. There were 67 complications (16%) in total. The major complication rate was 7.2%, with one recorded death. The median length of hospital stay was 3 d, and the mean follow-up period was 1 y. A total of 170 patients (43%) were super-obese, with a mean preoperative BMI of 56 kg/m(2) (SD ± 5 kg/m(2)). The mean absolute weight loss (59 versus 36.7 kg; P < 0.01) and percentage excess weight loss (58.9% versus 45.9%; P < 0.01) was significantly higher in the super-obese. The mean postoperative BMI for super-obese patients was 38.9 kg/m(2). There was no difference between groups in the incidence of major complications (8.2% versus 6.5%; P = 0.56).
Early results after laparoscopic Roux-en-Y gastric bypass: effect of the learning curve. Andrew CG, Hanna W, Look D, McLean AP, Christou NV.
Source
Department of Surgery, University of Manitoba, St. Boniface General Hospital, Winnipeg. [email protected]
Abstract
INTRODUCTION: This study was performed to evaluate the safety and short-term efficacy of laparoscopic Roux-en-Y gastric bypass (LRYGB) for morbid obesity and to describe the relation between learning curve and short-term outcomes.METHODS:
We collected a prospective database on the first 201 consecutive patients who underwent
LRYGB by a single university-based, experienced bariatric surgeon over 24 months. We divided patients into 3 consecutive groups of 67 patients for analysis (Group 1, Group 2 and Group 3).
RESULTS: The mean patient age was 37 (standard deviation [SD] 9) years; mean body mass index (BMI) was 49.2 (SD 8.3) kg/m2. BMI was similar in Groups 1 and 2 (mean 47.1, SD 5.9 and mean 48.7, SD 8.9 kg/m2) but increased in Group 3 (mean 52, SD 9.7 kg/m2, p < 0.01). Operative time decreased from 145 (SD 30) minutes in Group 1 to 114 (SD 24) minutes in Group 2 (p < 0.01) and was maintained at 119 (SD 23) minutes in Group 3. Early and late
complication rates were 14.9% and 12.4%, respectively. Leak rates decreased from 6.0% in the first group to 1.5% in Groups 2 and 3, but they did not reach statistical
significance. Anastomotic stricture rates decreased from 11.9% in Group 1 to 3.0% in Group 2 (p < 0.01). Overall excess weight loss for the entire series was 31.5% (SD 11.9%), 54.5% (SD 14.1%), 77.1% (SD 18.5%) and 82.1% (SD 17.5%) at 3, 6, 12 and 18 months, respectively.

Laparoscopic Roux-en-Y gastric bypass: initial 2-year experience. Suter M, Giusti V, Héraief E, Zysset F, Calmes JM.
Department of Surgery, Centre Hospitalier Universitaire Vaudois, 1011 Lausanne, Switzerland. [email protected]
BACKGROUND: Roux-en-Y gastric bypass (RYGBP)-essentially a restrictive bariatric procedure-is currently considered the gold standard for the surgical treatment of morbid obesity. Open surgery in obese patients is associated with a high risk of cardiopulmonary complications, wound infection, and late incisional hernia. Laparoscopic surgery has been shown to reduce perioperative morbidity and to improve postoperative recovery for various procedures. Herein we present our results with laparoscopic RYGBP after an initial 2-year experience.
METHODS: A prospective database was created in our department beginning without the first laparoscopic bariatric procedure. To provide a complete follow-up of 6 months, the results of all patients operated on between June 1999 and August 2001 were reviewed. Early surgical results, weight loss, correction of comorbidities, and improvement of quality of life were evaluated.
RESULTS: A total of 107 patients were included. There were 82 women and 25 men, with a mean age of 39.7 years (range, 19-58). RYGBP was a primary procedure in 80 cases (49 morbidly obese and 31 superobese patients) and a reoperation after failure or complication of another bariatric operation in 27 cases. Mean duration of surgery was 168 min for morbidly obese patients, 196 min for surperobese patients, and 205 min for reoperated patients (p <0.01). Conversion to open surgery was necessary in two cases. A total of 22 patients (20.5%) developed
complication. Nine of them (8.4%) required reoperation for leak (five cases, or 4.6%), bowel occlusion (three cases, or 2.8%), or subphrenic abscess (one case, or 0.9%).
mortality was 0.9%. Major morbidity decreased over time (first two-thirds, 12.5%, last third, 2.7%). major morbidity decreased over time (first two-thirds, 12.5%; last third, 2.7%). Excess weight loss of -50% was achieved in >80% of the patients, corresponding to a loss of 15 body mass index (BMI) units in morbidly obese patients and 20 BMI units in superobese patients. In the vast majority of patients, comorbidities improved or disappeared over time and quality of life improved.

Impact of surgeon experience and buttress material on postoperative complications after laparoscopic sleeve gastrectomy. Daskalakis M, Berdan Y, Theodoridou S, Weigand G, Weiner RA.
Center for Minimal-Invasive Surgery, Department of General and Bariatric Surgery, Krankenhaus Sachsenhausen, Frankfurt am Main, Germany.
Abstract
BACKGROUND: Sleeve gastrectomy is gaining popularity whether as a primary, staged or revisional
operation. The aim of this study is to evaluate the perioperative safety and the learning curve for laparoscopic sleeve gastrectomy (LSG).
METHODS: We performed a retrospective review of the prospectively collected data for all patients who underwent LSG for the treatment of morbid obesity at our institution from January 2003 to December 2008.
RESULTS: Data from 230 consecutive patients [male 47%, female 53%; mean age 44.0 ± 10.0 years, mean preoperative body mass index (BMI) 56.7 ± 11.5 kg/m(2)], who were operated upon by three surgeons with different degrees of bariatric experience, were analyzed. There was no 30-day
mortality, but there were two cases of late mortality (0.87%). Early complications were noted in 23 cases (10.0%), including 10 cases of leak (4.3%) and 10 cases of hemorrhage (4.3%). In 17 cases (7.4%) reoperations were performed. The rates of overall and major complications did not differ among surgeons or between early and late period of experience for the three surgeons; this trend held true individually and in subgroups. Overall, over the course of the learning curve, a significant decrease in operative time was noted. The only factor that was independently associated with complications was use of buttress material; the likelihood of complications was found to be 72% lower in patients in whom buttress material was used.

Does experience preclude leaks in laparoscopic gastric bypass? Gonzalez R, Haines K, Gallagher SF, Murr MM.
Interdisciplinary Obesity Treatment Group, Department of Surgery, University of South Florida College of Medicine, c/o Tampa General Hospital, P.O. Box 1289, Tampa, FL 33601, USA.
BACKGROUND: Improved outcomes of laparoscopic Roux-en-Y gastric bypass (LRYGB) have been demonstrated once pratice has moved beyond the learning curve. However, there is no evidence that experience has a favorable impact on the incidence of leaks. This study evaluated the incidence of staple-line leaks as experience accrued in a university-based bariatric surgery program
RESULTS: Staple-line leaks developed in 9 (4.5%) of the first 200 patients undergoing LRYGB. Among the 200 patients were 190 women (95%). The median age of the patients was 48 years (ranges, 24-62 years), and their body mass index was 43 kg/m(2) (ranges, 32-59 kg/m(2)). As surgeons' experience increased over time, there was a significant increase in the weight of patients and the percentage of patients with previous abdominal operations. There also was a significant decrease in conversion rates and operative times. Leaks occurred in six patients at the cardiojejunostomy (3%), in two patients jejunojejunostomy (1%), and in one patient at the excluded stomach (0.5%). Of the 50 leaks that occurred in each quartile, there were in the 3 in the 1st quartile, 1 in the 2nd quartile, 2 in the 3rd quartile, 3 in the 4th quartile. The differences were not significant. There was no correlation between the number of LRYGBs, and the occurrence of a leak (p = 0.59 confidence interval -0.13-0.22).

Results of 281 consecutive total laparoscopic Roux-en-Y gastric bypasses to treat morbid obesity. DeMaria EJ, Sugerman HJ, Kellum JM, Meador JG, Wolfe LG.
Department of Surgery and the Center for Minimally Invasive Surgery, Medical College of Virginia Campus of Virginia Commonwealth University, Richmond, Virginia 23298, USA. [email protected]
OBJECTIVE: To determine the safety and efficacy of laparoscopic Roux-en-Y gastric bypass for the treatment of morbid obesity.
METHODS: The authors attempted total laparoscopic Roux-en-Y gastric bypass in 281 consecutive patients. Procedures included 175 proximal bypasses, 12 long-limb bypasses, and 9 revisional procedures from previous bariatric operations. The gastrojejunostomy and jejunojejunostomy were primarily constructed using linear stapling techniques.
RESULTS: Eight patients required conversion to an open procedure (2.8%). The mean age of the patients was 41.6 years (range 15-71) and 87% were female. The mean preoperative body mass index was 48.1 kg/m2. The operative time decreased significantly from 234 +/- 77 minutes in the first quartile to 162 +/- 42 minutes in the most recent quartile. Postoperative length of stay averaged 4 days (range 2-91), with 75% of patients discharged within 3 days. The median hospital stay was 2 days. No patient died after surgery. Complications included three (1.5%) major wound infections (each followed a reoperation for a complication or open conversion),
incisional hernia in 5 patients (1.8%), and anastomotic leak with peritonitis in 14 patients (5.1%). Three gastrojejunal leaks were managed without surgery, four by laparoscopic repair/drainage, and three by open repair/drainage. Only three patients had anastomotic leaks in the most recent 164 procedures (1.8%) since the routine use of a two-layer anastomotic technique. Data at 1 year after surgery were available in 69 of 96 (72%) patients (excludes revisions). Weight loss at one year was 70 +/- 5% of excess weight. Most comorbid conditions resolved by 1 year after surgery; notably, 88% of patients with diabetes no longer required medications.
Intraoperative endoscopy and leaks after laparoscopic Roux-en-Y gastric bypass. Alaedeen D, Madan AK, Ro CY, Khan KA, Martinez JM, Tichansky DS.
Division of Laparoendoscopic and Bariatric Surgery, University of Miami, Miami, Florida 33136, USA.
Abstract
Postoperative leaks after laparoscopic Roux-en-Y gastric bypass (LRYGB) are a source of morbidity and mortality. Any intervention that would decrease leak rates after LRYGB would be useful. This investigation tested the hypothesis that postoperative leak rates are lower after LRYGB with the routine use of intraoperative endoscopy (EN). Consecutive patients who
underwent LRYGB were included. Intraoperative leak testing with air and methylene blue through an orogastric tube (OG) was used in the first 200 patients. Intraoperative endoscopy was used after the first 200 patients. There were 400 patients in this study. Preoperative demographics did not differ between groups. The intraoperative leak rate of the EN group was double the OG group (8 vs 4%; P = not significant), although the difference was not statistically significant. The OG group had a postoperative leak rate of 4 per cent with a mortality rate of 1 per cent. The EN group had a postoperative leak rate of 0.5 per cent with a mortality rate of 0 per cent. The difference in leak rates was statistically significant (P < 0.04). Despite the issues of learning curve, EN demonstrates more intraoperative leaks than OG, indicating EN may be a more sensitive test than OG. Routine use of EN is associated with less postoperative leaks after LRYGB.

Laparoscopic Roux-en-Y gastric bypass: results and learning curve of a high-volume academic program. Shikora SA, Kim JJ, Tarnoff ME, Raskin E, Shore R.
Division of Bariatric Surgery, Department of Surgery, Tufts-New England Medical Center, Boston, MA, USA.
Abstract
HYPOTHESIS: Laparoscopic Roux-en-Y gastric bypass is a complex procedure performed on a high-risk patient population. Good results can be attained with experience and volume.
DESIGN: Retrospective study.
SETTING: Tertiary care academic hospital.
PATIENTS: Seven hundred fifty consecutive morbidly obese patients undergoing surgery from March 1998 to April 2004.
RESULTS:
The patient population was 85% women and had a mean body mass index of 47 kg/m2 (range,
32-86 kg/m2). The overall complication rate was 15% and the mortality was 0.3%. For the first 100 cases, the overall complication rate was 26% with a mortality of 1%. This complication rate decreased to approximately 13% and was stable for the next 650
patients. The incidence of major complications has also decreased since the first 100 cases. Leak decreased from 3% to 1.1%. Small-bowel obstruction decreased from 5% to 1.1%. Overall mean operating time was 138 minutes (range, 65-310 minutes). It decreased from 212 minutes for the first 100 cases to 132 minutes for the next 650 and 105 minutes (range, 65-200 minutes) for the last 100 cases.
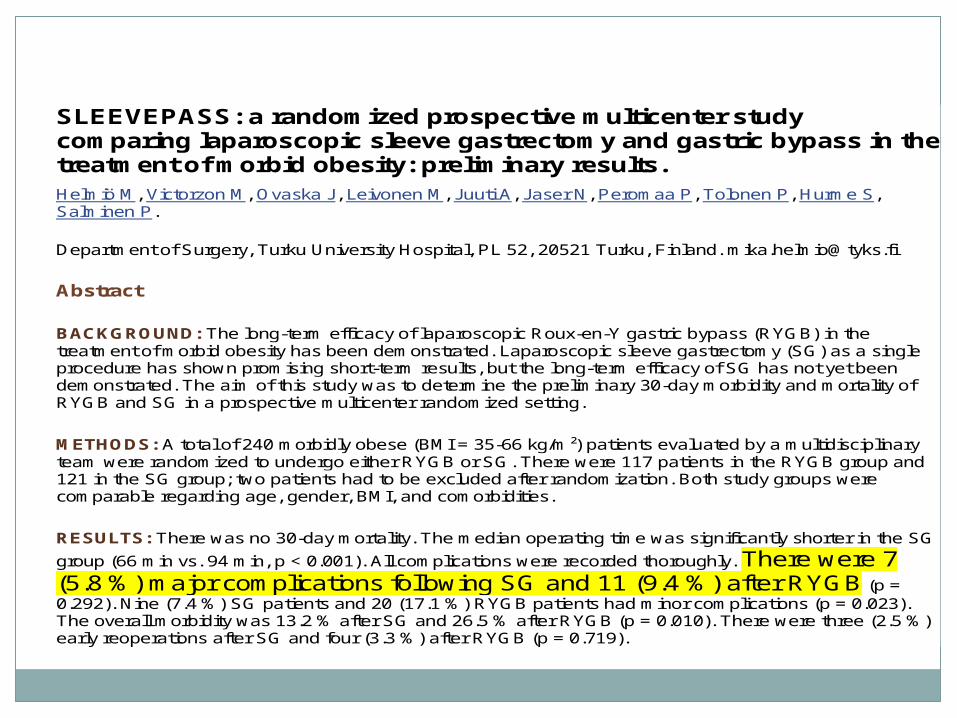
SLEEVEPASS: a randomized prospective multicenter study comparing laparoscopic sleeve gastrectomy and gastric bypass in the treatment of morbid obesity: preliminary results. Helmiö M, Victorzon M, Ovaska J, Leivonen M, Juuti A, Jaser N, Peromaa P, Tolonen P, Hurme S, Salminen P.
Department of Surgery, Turku University Hospital, PL 52, 20521 Turku, Finland. [email protected]
Abstract
BACKGROUND: The long-term efficacy of laparoscopic Roux-en-Y gastric bypass (RYGB) in the treatment of morbid obesity has been demonstrated. Laparoscopic sleeve gastrectomy (SG) as a single procedure has shown promising short-term results, but the long-term efficacy of SG has not yet been demonstrated. The aim of this study was to determine the preliminary 30-day morbidity and mortality of RYGB and SG in a prospective multicenter randomized setting.
METHODS: A total of 240 morbidly obese (BMI = 35-66 kg/m²) patients evaluated by a multidisciplinary team were randomized to undergo either RYGB or SG. There were 117 patients in the RYGB group and 121 in the SG group; two patients had to be excluded after randomization. Both study groups were comparable regarding age, gender, BMI, and comorbidities.
RESULTS: There was no 30-day mortality. The median operating time was significantly shorter in the SG
group (66 min vs. 94 min, p < 0.001). All complications were recorded thoroughly. There were 7 (5.8 %) major complications following SG and 11 (9.4 %) after RYGB (p = 0.292). Nine (7.4 %) SG patients and 20 (17.1 %) RYGB patients had minor complications (p = 0.023). The overall morbidity was 13.2 % after SG and 26.5 % after RYGB (p = 0.010). There were three (2.5 %) early reoperations after SG and four (3.3 %) after RYGB (p = 0.719).

2007
THE IDEA


الطبيعي الحل

المثالي الحل

33 CASES
2009

Drawback
SurgeonAnaesthesiaFollow up

New strategy
Multi disciplinary approachAnesthesiaDieticianPsyckologistPlastic surgeonPhysicianGuideline.

32 CASES
2010

65 CASES
2011

140 CASES
2012

2013
33 cases
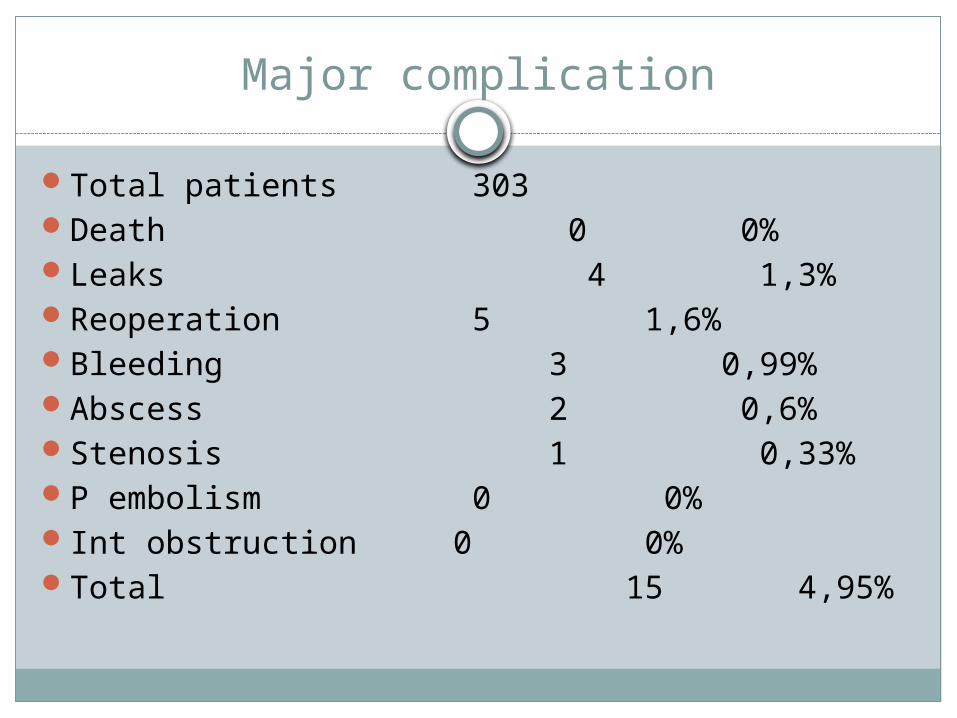
Major complication
Total patients 303Death 0 0%Leaks 4 1,3% Reoperation 5 1,6%Bleeding 3 0,99%Abscess 2 0,6%Stenosis 1 0,33%P embolism 0 0%Int obstruction 0 0%Total 15 4,95%

subanalyisis
Perioperative outcomes of revisional laparoscopic gastric bypass after failed adjustable gastric banding and after vertical banded gastroplasty: experience with 107 cases and subgroup analysis. Apers JA, Wens C, van Vlodrop V, Michiels M, Ceulemans R, van Daele G, Jacobs I.
Department of Digestive Surgery, Heilig Hart Ziekenhuis, Mol, Belgium, [email protected].
Abstract
BACKGROUND: A growing number of revision procedures are to be expected in bariatric surgery after failed restrictive procedures such as failed adjustable gastric banding (AGB) or vertical banded gastroplasty (VBG). Conversion to revisional laparoscopic Roux-en-Y gastric bypass (ReLRYGBP) has been advocated as the procedure of choice.
METHODS: The results of ReLRYGBP were reviewed in a retrospective chart review. A subgroup analysis compared perioperative results after VBG and after AGB. A second subgroup analysis compared perioperative results of ReLRYGBP immediately after AGB removal and after a delay as a two-step procedure.
RESULTS: Between 2003 and 2009, ReLRYGBP was performed for 107 patients. Of these 107 operations, 21 were performed after failed VBG and 86 after failed AGB. The mean body mass index (BMI) was 42 kg/m(2). The causes of failure were mainly insufficient weight loss or reflux disease-related symptoms. During a median follow-up period of 44 months, there was no mortality, and morbidity was 34
%, including late complications. Major early complications occurred in 11 % of the cases (n = 12). Conversions and major early complications occurred significantly more frequently after VBG than after AGB (p < 0.05). In 59 % of the cases (n = 50), ReLRYGBP was performed as a single-stage procedure immediately after removal of AGB and in 41 % of the cases (n = 36) as a delayed two-step procedure. The outcomes did not differ significantly (p > 0.5).

Outcomes of revisional procedures for insufficient weight loss or weight regain after Roux-en-Y gastric bypass. Himpens J, Coromina L, Verbrugghe A, Cadière GB.
The European School of Laparoscopy, St Blasius General Hospital, Dendermonde, Belgium. [email protected]
BACKGROUND: The Roux-en-Y gastric bypass (RYGB) performed laparoscopically (LRYGB) is the most frequently performed bariatric procedure in Belgium. However, late results in terms of weight loss or weight regain are inconsistent and may warrant a second procedure. This retrospective study analyzes the laparoscopic options for revisional surgery after LRYGB.
METHODS: Between January 1, 2001 and December 31, 2009, 70 patients underwent a new laparoscopic procedure for poor weight loss or weight regain after LRYGB. The revisional procedure was performed a median of 2.6 years after the initial bypass operation. Fifty-eight patients were available for follow-up (82.9 %); 19 underwent distalization; and 39 a new restrictive procedure.
RESULTS:
The mean mass index (BMI) before the revisional procedure was 39.1 + 11.3 kg/m(2) (30.8-51.8), down from 42.7 + 19.7 kg/m(2) (33.0-56.6) initially, which corresponded to a percentage of excess weight loss (EWL) of 12.4 + 9.3 % (-1.0-29.1). After the corrective procedure, with a follow-up of approximately 4 years, mean BMI was 29.6 + 12.4 kg/m(2) (18.0-45.5), for a significant additional percentage of EWL of 53.7 + 9.8 % (2.0-65.8). The overall complication rate was 20.7 %, and the reoperation rate was 7.3 %.
The overall leak rate was 12.1 %. Patients suffering from leaks could
consistently be treated conservatively or by stent placement. Two patients needed reconversion after distal bypass. The satisfaction index was good in just over 50 % of the patients
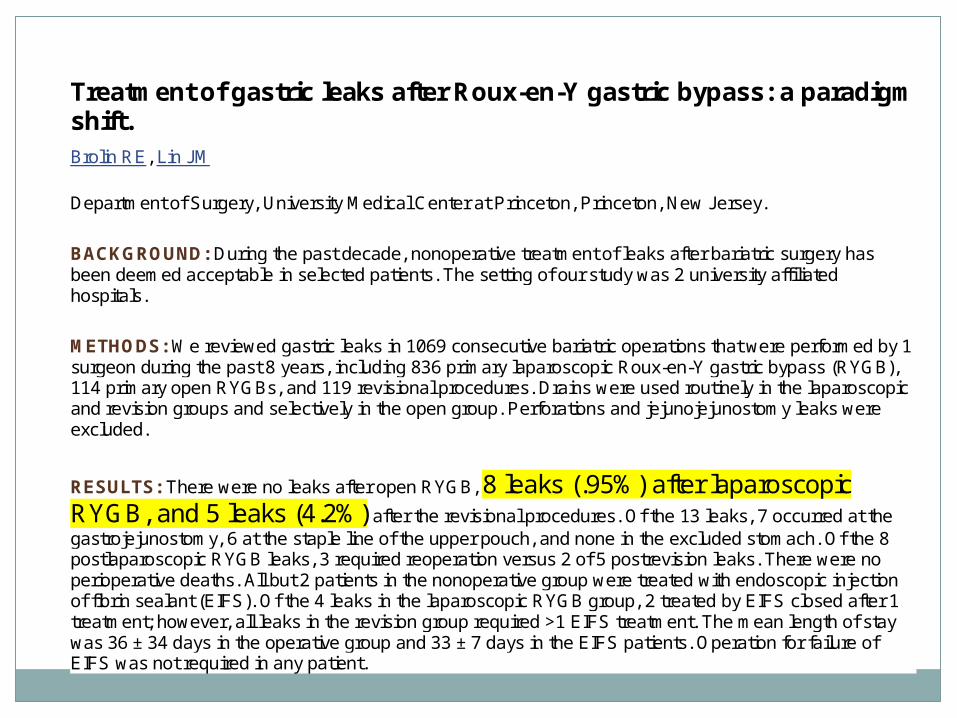
Treatment of gastric leaks after Roux-en-Y gastric bypass: a paradigm shift. Brolin RE, Lin JM
Department of Surgery, University Medical Center at Princeton, Princeton, New Jersey.
BACKGROUND: During the past decade, nonoperative treatment of leaks after bariatric surgery has been deemed acceptable in selected patients. The setting of our study was 2 university affiliated hospitals.
METHODS: We reviewed gastric leaks in 1069 consecutive bariatric operations that were performed by 1 surgeon during the past 8 years, including 836 primary laparoscopic Roux-en-Y gastric bypass (RYGB), 114 primary open RYGBs, and 119 revisional procedures. Drains were used routinely in the laparoscopic and revision groups and selectively in the open group. Perforations and jejunojejunostomy leaks were excluded.
RESULTS: There were no leaks after open RYGB, 8 leaks (.95%) after laparoscopic RYGB, and 5 leaks (4.2%) after the revisional procedures. Of the 13 leaks, 7 occurred at the gastrojejunostomy, 6 at the staple line of the upper pouch, and none in the excluded stomach. Of the 8 postlaparoscopic RYGB leaks, 3 required reoperation versus 2 of 5 postrevision leaks. There were no perioperative deaths. All but 2 patients in the nonoperative group were treated with endoscopic injection of fibrin sealant (EIFS). Of the 4 leaks in the laparoscopic RYGB group, 2 treated by EIFS closed after 1 treatment; however, all leaks in the revision group required >1 EIFS treatment. The mean length of stay was 36 ± 34 days in the operative group and 33 ± 7 days in the EIFS patients. Operation for failure of EIFS was not required in any patient.
Major cases
9 CASES BMI> 7020 REVISIONAL SURGERIES18 CASES BMI>60103 SUPER OBESE.

Major complication
Total patients 303 -20=283Death 0 0% 0%Leaks 4 1,3% -3=1
0,35%Reoperation 5 1,6% -3=2 0,7%Bleeding 3 0,99% 3
1%Abscess 2 0,6% -1=1
0,35%Stenosis 1 0,33% 1
0,35%P embolism 0 0%Int obstruction 0 0%Total 15 4,95% 8 2,8%

Contributors to success
TEAM WORK.NAGGING ANAESTHESIAADHERENCE TO POLICYMULTI DISCIPLINARY APPROACH
