reactivation planning: playbook
TRANSCRIPT
Reactivation Planning: Playbook Surgery and Interventional/Procedural PlatformsMay 5, 2020
Presented to: Insert relevant presenter information Calibri 16pt
Presented on: Month day, Year
Presented by: Insert relevant presenter information here
• Ensure safety for all patients and NM team members.
• Maintain readiness for a COVID-19 resurgence.
• Equip clinical and operational leaders to determine the local sequence, pace and approach for reactivating care based on facility, staff, supply, testing and PPE availability.
• Continue to focus on wellness as we acknowledge and respect physician and employee experiences relative to COVID-19.
• Identify lessons learned and emerging best practices, technologies and tools.
Reactivation Guiding Principles
2
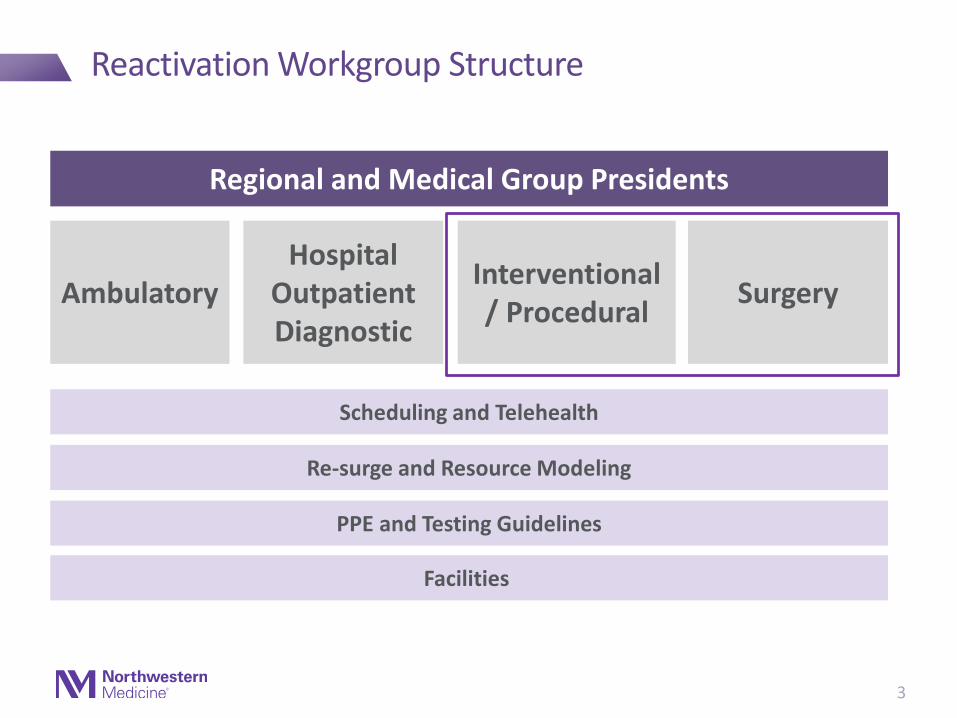
Reactivation Workgroup Structure
3
AmbulatoryHospital
Outpatient Diagnostic
Scheduling and Telehealth
Interventional / Procedural
Surgery
Regional and Medical Group Presidents
Re-surge and Resource Modeling
PPE and Testing Guidelines
Facilities
Regulatory Requirements
• IDPH Guidelines for Elective Surgeries and Procedures April 24, 2020
Minimum threshold requirements to resume elective inpatient procedures (IDPH 4/24/2020*) • Hospital availability of adult med/surg beds exceeds 20% of operating capacity for adult med/surg beds
• Hospital availability of ICU beds exceeds 20% of operating capacity for ICU beds
• Hospital ventilator capacity exceeds 20% of total ventilators
Subject to change in the event of the following circumstances:• Rapid resurgence or a second wave of COVID-19
• Decrease in statewide hospital COVID-19 testing levels
IDPH Minimum Thresholds (IDPH Section C)
*These thresholds do not apply to pediatric procedures 4

Regulatory Requirements
Case Setting and Prioritization
• Each facility should convene and charge a Surgical Review Committee (SRC), composed of surgery, anesthesiology and nursing personnel, to provide defined, transparent and responsive oversight of the prioritization of elective inpatient cases.
• This committee can lead the development and implementation of guidelines that are fair, transparent and equitable for the hospital or system in consideration of rapidly evolving local and regional issues.
• The SRC should rely heavily on elective case triage guidelines for surgical care that have been developed by professional societies.• The SRC should review regularly a list of previously postponed and canceled cases, prioritizing based on clinical considerations and
taking into account the resources and staff necessary for each procedure.
PreoperativeTesting for COVID-19
• Facilities must test each patient within 72 hours of a scheduled procedure with a preoperative COVID-19 RT-PCR test and ensure COVID-19 negative status.
• Patients must self-quarantine until the day of surgery after being tested. • A temperature check must also be completed on the day of arrival at the facility with results of less than 100.4 degrees prior to
proceeding with an elective procedure. • When clinically acceptable, providers should consider using telemedicine for preoperative visits. • In such cases, face-to-face components of the exam can happen after the result of the preoperative COVID-19 test result is known to
be negative.
Protective Equipment
Facilities may resume procedures only if there is adequate personal protective equipment with respect to the number and type of procedures that will be performed, and enough to ensure adequate supply if COVID-19 activity increases in the community within the next 14 days.
Infection Control
• Facility cleaning policies in all areas along the continuum of operative care must follow established infection control procedures.• When possible, facilities should establish non-COVID care zones for screening, temperature checks and preoperative waiting areas. • Facilities should also minimize time in waiting areas, space chairs at least 6 feet apart, and maintain low patient volumes. Visitors
should generally be prohibited; if they are necessary for an aspect of patient care or as a support for a patient with a disability, they should be pre-screened in the same way as patients (as described above).
• Facilities must have the ability to routinely screen all staff and others who will work in the facility (physicians, nurses, housekeeping, delivery and other people who would enter the patient area) with COVID-19 RT-PCR testing.
SupportServices
Other areas of the facility that support perioperative services must be ready to commence operations with uniformly heightened infection control practices, including sterile processing, the clinical laboratory and diagnostic imaging.
IDPH Guidelines for Elective Surgeries and Procedures April 24, 2020
5

Surgical/Procedural Review Committee
6
IDPH requires that each hospital have an SRC to guide prioritization of reactivation
Form
C
om
mit
tee Surgery participants:
• Department of Surgery chairs, Inpatient medical directors, Surgical Services vice president, hospital presidents
Procedural Areas participants:• Medical director, chief(s), Operations director
Surgery Participants:Procedural Participants:
Iden
tify
Vo
lum
e Review canceled and not rescheduled cases for March 15 through present:• COVID-19 Access Scheduling Dashboard (OR tabs)• Covid 19 Appointment Cancel Reschedule Details Report• COVID-19 OR Cancels and Reschedules Details Report• Epic Workbench Report: COVID Canceled/Rescheduled Appointments
[Scheduling > Reports > Follow Up > COVID canceled/Rescheduled]
Administrator who will compile cases that need to
be rescheduled and distribute to surgeons:
Pri
ori
tize
Vo
lum
e Categorize cases based on risk to the patient:• A: Emergency• B: Need to move forward with procedure/surgery
• B1: Most urgent, can no longer be postponed• B2: Less urgent, can wait a little longer
• C: Elective and can wait until adequate resources are available
How this information will be tracked/updated:

Reactivation Planning Committee
7
Form
Co
mm
itte
e Core Participants: • Inpatient medical directors, Operations director, Surgical
Services vice president, hospital presidentsSupporting Services Representatives: • MD and RN labor pool, anesthesia, diagnostic testing, lab and
blood bank, pharmacy, scheduling, facilities, equipment and IT, EVS and transport, pre-op clinic
Core Participants: Supporting Services Representatives:
Ou
tlin
eP
roce
ss
Review planning questions and recommendations.
Outline scheduling, pre-procedure covid testing, and day of procedure processes and workflows.
See supporting planning documents on Slide 8 and 9.
Ass
ess
Res
ou
rces
Document resources needed for pre, intra and post procedure phases.
Create a capacity restoration plan based on available resources.See supporting planning documents on Slides 8, 10-13.
Mo
nit
or
and
Act
ivat
e Outline monitoring process. See supporting planning document on Slide 14.
Define dashboard metrics.Current capacity and resources Future modeling capacity and resources
Create go-live checklist. See supporting planning documents on Slide 8.
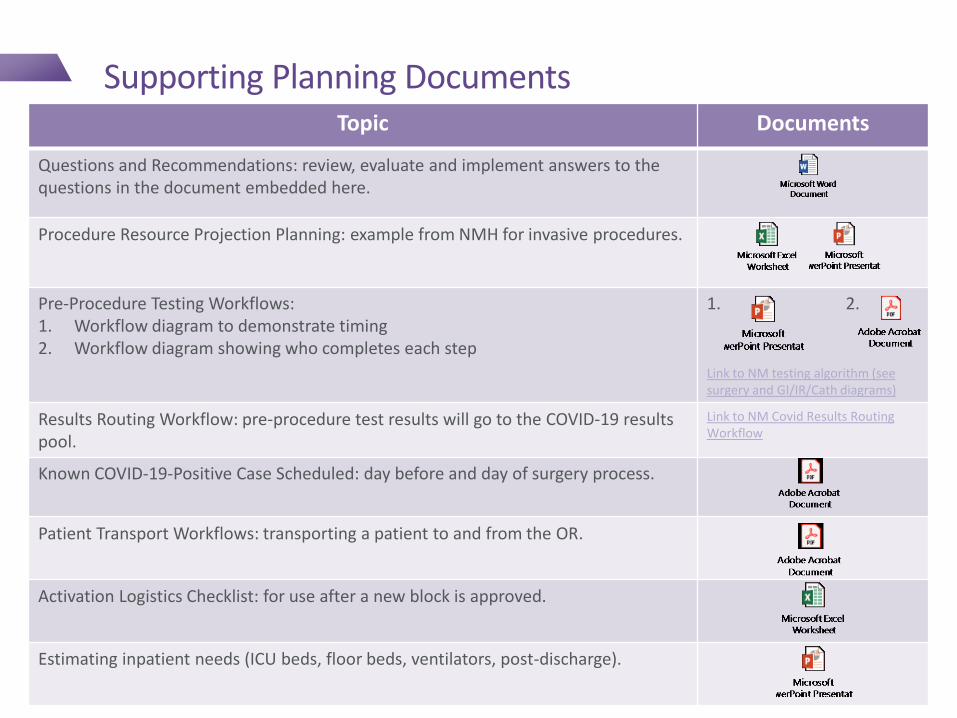
Supporting Planning DocumentsTopic Documents
Questions and Recommendations: review, evaluate and implement answers to the questions in the document embedded here.
Procedure Resource Projection Planning: example from NMH for invasive procedures.
Pre-Procedure Testing Workflows: 1. Workflow diagram to demonstrate timing2. Workflow diagram showing who completes each step
1. 2.
Link to NM testing algorithm (see surgery and GI/IR/Cath diagrams)
Results Routing Workflow: pre-procedure test results will go to the COVID-19 results pool.
Link to NM Covid Results Routing Workflow
Known COVID-19-Positive Case Scheduled: day before and day of surgery process.
Patient Transport Workflows: transporting a patient to and from the OR.
Activation Logistics Checklist: for use after a new block is approved.
Estimating inpatient needs (ICU beds, floor beds, ventilators, post-discharge).

SAMPLE Pre-Procedure Workflow IDPH Guidelines: • Facilities must test each patient within 72 hours of a scheduled procedure with a preoperative COVID-19 RT-PCR test and ensure COVID-19 negative status. • Patients must self-quarantine until the day of surgery after being tested. • A temperature check must also be completed on the day of arrival at the facility with results of less than 100.4 degrees prior to proceeding with an elective procedure. • When clinically acceptable, providers should consider using telemedicine for preoperative visits. • In such cases, face-to-face components of the exam can happen after the result of the preoperative COVID-19 test result is known to be negative
Scheduling Testing Phase Pre-Procedural Phase
Surgeon’s Office • Coordinates procedure dates with patient and communicates the need for COVID testing 48 hours prior to the procedure
• For testing, the patient should report with identification to:
• Lavin Pavilion 259 E. Erie• Cars enter the testing site from eastbound Erie
Street• Open 7 days a week 7 am-3 pm • Sends case request to Central Scheduling
• Specimen resulted.• Surgeon reviews chart by 9 am the day prior to procedure and contacts
patients with positive or indeterminate results. If changes to the surgical schedule need to be made, this must be completed by 11 am.
• If NEGATIVE: No need to contact the patient and proceed with procedure as planned.
• If POSITIVE and case can be postponed, patient should be rescheduled. If case cannot be postponed, complete procedure in full PPE and COVID designated room.
• If INDETERMINATE/INHIBITED, patient will require same-day, repeat testing, the morning of surgery. Follow same-day testing protocol.
Central Scheduling • Schedules both surgical and NORA cases• Flags all patient charts, except those with local
anesthesia type, with the pre-procedure COVID testing flag
• Patient is then added to COVID Hotline triage pool
Schedule closes at 11 am for next day cases.
Patient
COVID Ordering and Results Teams
COVID triage nurse places future COVID order panel on patient, removes flag which removes from work queue
Specimen is resulted and the COVID Results Team contacts the patient with the results and next steps the day prior to surgery.
COVID Test Site Registration
Checks in patient and releases order
COVID Drive-Through Team
Specimen collected, Pre-Op sticker added to indicate priority
Pre-Op Nursing Calls patient with time of surgery starting at 2 pm the day prior to procedure. PUI screening questions will be asked at this time.
9
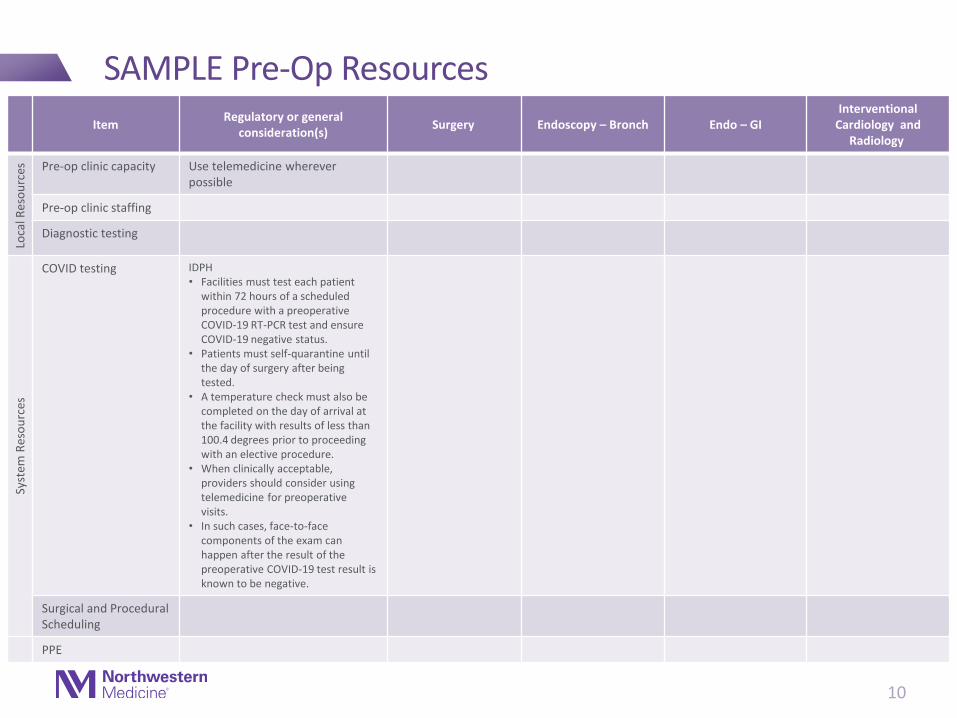
SAMPLE Pre-Op Resources
10
ItemRegulatory or general
consideration(s)Surgery Endoscopy – Bronch Endo – GI
Interventional Cardiology and
Radiology
Loca
l Res
ou
rces Pre-op clinic capacity Use telemedicine wherever
possible
Pre-op clinic staffing
Diagnostic testing
Syst
em R
eso
urc
es
COVID testing IDPH• Facilities must test each patient
within 72 hours of a scheduled procedure with a preoperative COVID-19 RT-PCR test and ensure COVID-19 negative status.
• Patients must self-quarantine until the day of surgery after being tested.
• A temperature check must also be completed on the day of arrival at the facility with results of less than 100.4 degrees prior to proceeding with an elective procedure.
• When clinically acceptable, providers should consider using telemedicine for preoperative visits.
• In such cases, face-to-face components of the exam can happen after the result of the preoperative COVID-19 test result is known to be negative.
Surgical and ProceduralScheduling
PPE

SAMPLE Procedural Resources
ItemRegulatory or general
consideration(s)Surgery Endoscopy – Bronch Endo – GI
Interventional Cardiology and
Radiology
Loca
l Res
ou
rces
Pre-op/Pre-proceduralspaces
OR or procedural room capacity
SS/Procedure RN staffing
Anesthesia staffing (including NORA)
Vent needs IDPH: Hospital ventilator capacity exceeds 20% of total ventilators
PACU/Procedure recovery set up
PACU/Procedure recovery staffing
Central supply
EVS
Patient transport
Pharmacy – Staff
Pharmacy – Meds
Lab – Blood products
PPE
11
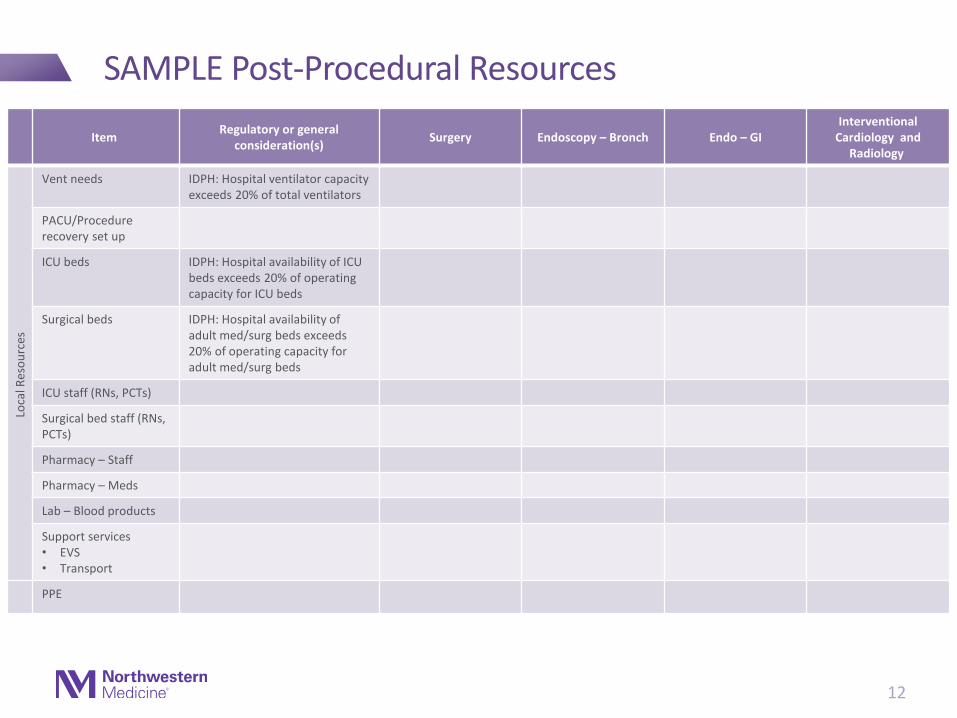
SAMPLE Post-Procedural Resources
12
ItemRegulatory or general
consideration(s)Surgery Endoscopy – Bronch Endo – GI
Interventional Cardiology and
Radiology
Loca
l Res
ou
rces
Vent needs IDPH: Hospital ventilator capacity exceeds 20% of total ventilators
PACU/Procedure recovery set up
ICU beds IDPH: Hospital availability of ICU beds exceeds 20% of operating capacity for ICU beds
Surgical beds IDPH: Hospital availability of adult med/surg beds exceeds 20% of operating capacity for adult med/surg beds
ICU staff (RNs, PCTs)
Surgical bed staff (RNs, PCTs)
Pharmacy – Staff
Pharmacy – Meds
Lab – Blood products
Support services • EVS• Transport
PPE

ResourceNeeds
15% Block 30% Block 50% Block 65% Block 80% Block 100% Block >100% Block
Associated Category 50% Cat B 100% Cat B 100% Cat BCat B backlog
100% Cat B30% Cat C
(ambulatory)
100% Cat B60% Cat C
(ambulatory)
100% Cat B100% Cat C
(include inpt)
100% Cat B100% Cat C
Cat C Backlog
# daily cases | # ORs 25 | 10 OR 45 | 18 OR (only Fein)
70 | 28 OR (only Fein)
90 | 40(add Prent, Lavin)
130| 52(add Prent, Lavin)
150 | 57(add Prent, Lavin)
TBD(add Prent, Lavin
Surgical Beds* 47 74 82 82 82 197 TBD
ICU Beds (exc. G9)* 54 66 71 71 71 85 TBD
Vent Needs* 21 33 35 35 35 55 TBD
SS RN Staffing [how many are needed from labor pool]
Pre-Op: 7PACU: 15
Pre-op: 13PACU: 20
F Pre-op: 13 PACU:20L:11, P: 11
F Pre-op:13 F PACU:20L:11, P: 13
F Pre-op:13F PACU:20L:11, P: 15
TBD
Anest. Staffing (including NORA)
Attending: 10CRNA/Res: 24
Attending: 14CRNA/Res: 34
Attending: 19CRNA/Res: 45
Attending: 25CRNA/Res: 58
Attending: 32CRNA/Res: 72
Attending: 39CRNA/Res: 72
TBD
Pre-Op Clinic APP: 11, RN: 2MA: 1-2, Spt: 2
APP: 11, RN: 3MA: 2, Spt: 2
APP: 11, RN: 3MA: 3, Spt: 4
APP: 11, RN: 4MA: 4, Spt: 4
APP: 11, RN: 5MA: 5, Spt: 4
APP: 11, RN: 6MA: 5, Spt: 4
TBD
Support Services (EVS, Transport)
TBD
Block Schedule
COVID Testing 25 per day 45 per day 70 per day 90 per day 130 per day 150 per day TBD
Pharmacy (staff and anesthetic meds)
TBD
PPE Wipes:
Face Shields:Surgical Masks:
N95:
5 per day5 per day230 per day200 per day
9 per day9 per day414 per day360 per day
14 per day14 per day644 per day560 per day
18 per day18 per day828 per day720 per day
26 per day26 per day1196 per day1040 per day
30 per day30 per day1380 per day1200 per day
TBD
SAMPLE: Capacity Restoration Planning
Syst
emLo
cal
Current State (3/31)
Target Go-Live: (5/4)
*Calculations based actual census:• 100%: 1/1/20 – 2/29/20• 30%: 3/23/20 – 3/30/20• 15%: 3/31/20 – 4/15/20
Available for surgical services use based on other demand (COVID census etc.)
Not yet available for surgical services use based on other demand

Monday Tuesday Wednesday Thursday Friday
Assess trends over past week.
Each respective chief and PM to evaluate what to begin plans for two weeks out.
Meet with respective planningteams to review resource needs available
Activation leads meet to confirm proposal:1) What units available for
non-COVID2) Additional surgical/
procedural/ambulatory volume proposed
3) Staff re-allocation plans
Meet with respective planningteams to confirmlocal resource availability –confirm questions for system
System presidents meet and discuss – address local questions, confirm plan for week following
SAMPLE: Monitoring Schedule
14
Minimum Two Weeks of Prep Before Activation
Monday Tuesday Wednesday Thursday Friday
Assess trends over past week
Confirm plan to move forward in IC
Initiate scheduling of pts and staff
Meet with respective planning teams to prep logistics for next phase
Meet with respective planning teams to prep logistics for next phase
Wee
k 1
Wee
k 2

Appendix
15
Background
• During the COVID-19 pandemic, surgeries and procedures (collectively referred to as “procedures”) for life-threatening conditions or those with a potential to cause permanent disability have been and continue to be allowed.
• Due to the COVID-19 pandemic, hospitals and Ambulatory Surgical Treatment Centers (ASTCs) have deferred nonessential procedures to conserve resources for the care of COVID-19 patients.
• Some procedures that could reasonably be delayed for a time have now been postponed to the extent that potential harm could result from further delay.
• It is important to be flexible and allow facilities to provide care for patients needing non-emergent, non-COVID-19 healthcare.
IDPH Guidance on Elective Surgeries and Procedures April 24, 2020
16

IDPH Definitions
Definition
Elective OutpatientProcedures
• An elective procedure in which the likely and expected course for the patient undergoing the procedure is that the patient will enter and leave the facility on the same day that the procedure is to be performed.
• Procedures may be performed at ASTCs or at hospitals
• Clinical decision-making on whether a case is suitable for outpatient procedure should take into account a classification such as the Elective Surgery Acuity Scale (ESAS).
• For a facility to perform outpatient procedures, all criteria listed IDPH section D must be satisfied.
Elective InpatientProcedures
An elective procedure in which the patient being considered for that procedure is likely to remain in the hospital for more than 23 hours, starting from the time of registration and ending at the time of departure.
For a hospital to perform inpatient procedures, all criteria listed on the next two slides must be met (IDPH sections C and D).
Guidelines April 24, 2020
17

SAMPLE IDPH Facility Dashboard as of 5/11/2020 for Category C Procedures > 23-hour LOS
IDPH Requirement
Description Hospital Status
Case Setting and Prioritization
• Each facility should convene and charge a Surgical Review Committee (SRC), composed of surgery, anesthesiology, and nursing personnel, to provide defined, transparent, and responsive oversight of the prioritization of elective inpatient cases.
• The SRC should review regularly a list of previously postponed and canceled cases, prioritizing based on clinical considerations and taking into account the resources and staff necessary for each procedure.
PreoperativeTesting for COVID-19
• Facilities must test each patient within 72 hours of a scheduled procedure with a preoperative COVID-19 RT-PCR test and ensure COVID-19 negative status.
• Patients must self-quarantine until the day of surgery after being tested. • A temperature check must also be completed on the day of arrival at the facility with results of less than 100.4
degrees prior to proceeding with an elective procedure. • When clinically acceptable, providers should consider using telemedicine for preoperative visits. • In such cases, face-to-face components of the exam can happen after the result of the preoperative COVID-19
test result is known to be negative.
Protective Equipment
Facilities may resume procedures only if there is adequate personal protective equipment with respect to the number and type of procedures that will be performed, and enough to ensure adequate supply if COVID-19 activity increases in the community within the next 14 days.
Infection Control
• Facility cleaning policies in all areas along the continuum of operative care must follow established infection control procedures.
• When possible, facilities should establish non-COVID care zones for screening, temperature checks, and preoperative waiting areas.
• Facilities should also minimize time in waiting areas, space chairs at least 6 feet apart, and maintain low patient volumes. Visitors should generally be prohibited; if they are necessary for an aspect of patient care or as a support for a patient with a disability, they should be pre-screened in the same way as patients (as described above).
• Facilities must have the ability to routinely screen all staff and others who will work in the facility (physicians, nurses, housekeeping, delivery and other people who would enter the patient area) with COVID-19 RT-PCR testing.
SupportServices
Other areas of the facility that support perioperative services must be ready to commence operations with uniformly heightened infection control practices, including sterile processing, the clinical laboratory and diagnostic imaging. 18
ICU Beds (Utilization threshold 80%) M/S Beds (Utilization threshold 80%) Ventilators (Tier 1 Utilization Threshold 80%)

NM owns and operates multiple outpatient surgery assets. However, only NM Surgery Center in Warrenville bills as an ASC.
NM’s Existing Outpatient Surgery Assets
Owned Sites Billing Licensing
1 NM Lavin Pavilion HOPD HOPD – Multispecialty
2 Delnor Surgical Services 345(Formerly Tri-Cities ASC)
HOPD HOPD – Multispecialty
3 NM Grayslake ASC HOPD ASC – Multispecialty (Gen Surg, OB/Gyne, Ophth, Ortho, ENT, Plastic, Podiatry, Urology)
3 NM GrayslakeEndoscopy Center
HOPD ASC – Limited Specialty (GI)
4 NM Surgery Center, Warrenville (NMSC)
ASC ASC – Limited Specialty (Ortho, Pain Mgt)
Joint Venture Sites Billing Licensing
5 The Center for Surgery,Naperville
ASC ASC – Multispecialty (Neuro, OB/Gyne, Ophth, Ortho, ENT, Pain Mgt., Plastic, Podiatry, Urology)
6 Midland Surgical Center, Sycamore
ASC ASC – Multispecialty (Neuro, OB/Gyne, Ophth, Ortho, ENT, Pain Mgt, Plastic, Podiatry, Urology)
7 Algonquin Road Surgery Center LLC
ASC ASC – Multispecialty (Neuro, OB/GYN, Opth, Oral, Ortho, ENT, Pain Mgt., Plastic, Podiatry)
1
2
4
3
7
6
5
NM Hospital
Legend
Owned Site
JV Site
Central Region
Northwest Region
North Region
South Region
West Region

Covid Testing in Procedural Areas
• Wednesday morning, April 29, 2020, NM began using Abbott ID Now to test same-day OB and surgery/procedural patients who are being collected on the clinical unit immediately prior to their procedure.
• Patients are currently being tested on the Cepheid platform with a ~2 hour turnaround time from receipt. Abbott ID Now has a shorter turnaround time of ~ 30 minutes from receipt.
• Collection for the Abbott ID Now is a dry NP swab placed in an empty tube, as opposed to an NP swab placed in viral transport medium (VTM). Dry NP swab collection improves accuracy on the Abbott platform.
Specimens should be double-bagged when sending through the pneumatic tube system.
Any questions about new collection methods should be directed to your site’s lab leaders.
20
Last Updated 4/29/20

SAMPLE Inpatient COVID Testing Workflow
21

SAMPLE Drive-Through Testing Workflow
22

Regulatory/Facility Readiness
• NM is an “Essential Business” under the Illinois Stay-at-Home Order, thereby permitting employees to return to work.
• As an Essential Business, NM has complied with and will continue to comply with the physical distancing requirements set forth in the order and as modified by the governor and IDPH.
• Designate 6-feet distances for employees and patients queueing to maintain appropriate distance.
• Have hand sanitizer and sanitizing products readily available.
• Post online information regarding whether a facility is open and how best to reach the facility and continue services by phone or remotely.
• Provide face coverings to all employees who are unable to maintain 6 feet of physical distancing (per modified order)
• Follow new requirements to maximize physical distancing and prioritize the well-being of employees, including occupancy limits (per modified order)
• In addition, NM will follow applicable guidance from OSHA, CDC, CMS, FDA and other relevant governmental agencies
23
Guiding Principles

Facility Readiness
Scope Owners
Space Modifications to Accommodate Physical Distancing • Reconfiguration of waiting spaces to space seats 6'-0" apart with consideration given to
caregivers and patient complement• Removal of magazines and educational pamphlets, decommission coffee/water stations• Ensure staff are able to maintain social distancing recommendations in work spaces• Evaluation of installation of plexiglas dividers at check in/check out and reception locations • Establish appropriate queueing demarcations
Carol Feiner, Julia Louie, Jill Gewargis
Cleaning Protocols• Evaluation of updated recommendations to include potential increased frequency and
additional touch points • Increased availability and installation of hand sanitizer and disinfectant wipes for staff and
patient/visitor use
Carol Feiner, Colleen Schmiege, Chris Silkaitis, Cindy Barnard, EVS Leadership
Building Entry/Public Spaces• Employee/visitor screening protocols and operations • Guidelines for modifications of building entries and public seating to accommodate physical
distancing
Carol Feiner, Amy Russer, Jeff Good
Signage• Development of signage package for easy and consistent implementation and distribution
across all clinics and public spaces, including physical distancing clings, queueing directions and hygiene best practices
Carol Feiner, Jill Gewargis, Victoria Pulse, Heather Cunningham
Regulatory • Review and confirmation that Clinical Reactivation plan complies with current regulatory
requirements
Danae Prousis
24
Clinical Guidelines Work Plan
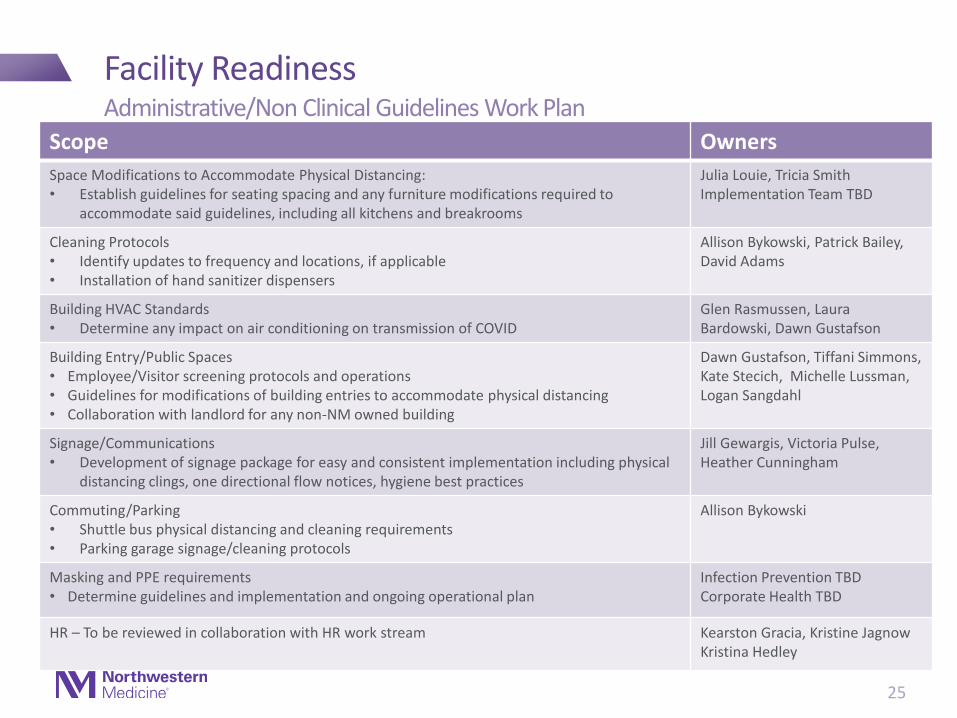
Facility Readiness
Scope Owners
Space Modifications to Accommodate Physical Distancing: • Establish guidelines for seating spacing and any furniture modifications required to
accommodate said guidelines, including all kitchens and breakrooms
Julia Louie, Tricia Smith Implementation Team TBD
Cleaning Protocols• Identify updates to frequency and locations, if applicable • Installation of hand sanitizer dispensers
Allison Bykowski, Patrick Bailey, David Adams
Building HVAC Standards• Determine any impact on air conditioning on transmission of COVID
Glen Rasmussen, Laura Bardowski, Dawn Gustafson
Building Entry/Public Spaces• Employee/Visitor screening protocols and operations • Guidelines for modifications of building entries to accommodate physical distancing• Collaboration with landlord for any non-NM owned building
Dawn Gustafson, Tiffani Simmons, Kate Stecich, Michelle Lussman, Logan Sangdahl
Signage/Communications• Development of signage package for easy and consistent implementation including physical
distancing clings, one directional flow notices, hygiene best practices
Jill Gewargis, Victoria Pulse, Heather Cunningham
Commuting/Parking• Shuttle bus physical distancing and cleaning requirements• Parking garage signage/cleaning protocols
Allison Bykowski
Masking and PPE requirements• Determine guidelines and implementation and ongoing operational plan
Infection Prevention TBD Corporate Health TBD
HR – To be reviewed in collaboration with HR work stream Kearston Gracia, Kristine JagnowKristina Hedley
25
Administrative/Non Clinical Guidelines Work Plan

Facility Readiness Playbook
26
Illustrative Excerpt (Clinical Guidelines)# Category Tactic Owner Notes
Waiting Area
1 □ Space seats 6'-0" apart; place some seats close for caregiver and patient to
sit adjacent; continue to provide a variety of seating (standard chairs and
bariatric or love seat) depending on patient type and complement
Construction/ Practice Management
2 □ Identify alternate waiting spaces (e.g. exam rooms) in the event of overflow Practice Management
3 □ Determine seating needs, options with increase in patient traffic Practice Management
4 □ Post approved signage Property Ops
5 □ Review options for partitions to allow for more seating (Phase 2) Construction
6 □ Provide wipes within the waiting room for patients to use on surfaces Property Operations/ EVS/ Supply Chain
7 □ Install "sanitation" station at appropriate locations within reasonable
distance of each clinic
Property Ops/Supply Chain
8 □ Provide additional garbage cans within the waiting space Property Ops
9 □ Remove magazines, newspapers, etc Practice Management/Volunteers
10 □ Remove educational items available for patients to take; determine if/how
to distribute
Practice Management
11 □ Remove coat hangers Construction
12 □ Decommission any self-serve refreshment stations Property Ops
13 □ Decommission phone charging stations, except in OR and ED waiting areas Property Ops
14 □ Remove remote controls Practice Management
15 □ Implement revised cleaning protocols Housekeeping/ EVS
16 □ Publish frequency of cleaning by space/area Housekeeping/ EVS
17 □ Confirm the fabrics used vinyls and solution dyed on chairs Construction
Social Distancing
Personal Sanitation
Shared Spaces/Items
Cleaning

Patient Communication Guidelines: Arrival and Appointments
• Inform patient about thermal screening, masking and minimal touch.
• Specific update about the No Visitor policy, including exemptions.
• Validation that anxiety and stress are appropriate responses to any medical appointment/procedure and these emotions may be elevated as they visit NM during the pandemic.
• Patients should arrive with a fully charged phone and/or should plan to bring a charger if they anticipate spending several hours at NM.
• Patients should arrive with questions for their provider already written down. This will help:
1) improve time efficiency in face to face visits and
2) compensate for patient's anxiety/stress which can lead to forgetting importantquestions, and
3) compensate for family who would be asking the questions.
• Patients should come prepared to take notes and should be reminded to read any printouts they receive at discharge, which may contain detailed information about treatment recommendations and future appointments.
• If patients would otherwise be accompanied by someone, they are encouraged to have that person on the phone for the entire visit, as an extra set of ears. That person should already be on the line before the provider enters the clinic room. Reminder to patients: many smart phones and tabletsallow for more than one person to be on the line at once. Patients can still have their support system with them. Those individualsshould be informed in advance of the timing and should write down questions in advance, if they plan to ask any.
• Patients with longer procedures/infusionsshould consider downloading music, a TV show, a podcast, game apps, or bring a magazine or other distraction.
• Patients should be given instructions about how to anticipate interpreter needs.
• Patients will benefit from other tips such as: familiarize yourself with a campus map before you enter campus and know your exact location PRIOR to entering the building.
• Provide some directionabout elevators (use a pen, your elbow, etc.), revolving doors, bathroom doors (eg., bring a wipe or tissue to use on doors, carry sanitizer if you have, etc) or whatever is recommended.
• Remind patients to wipe down phones and earpieces after their appointment.
• Remind them about what to expect re physical distancing, PPE, thermal scans at entrance, etc.
• Patients will also benefit from a reminderabout the frequency and quality of the sanitation on campus, as well as a reminder that the patient will not be exposed to the COVID units.
27
Source: Kim Feingold, PhD
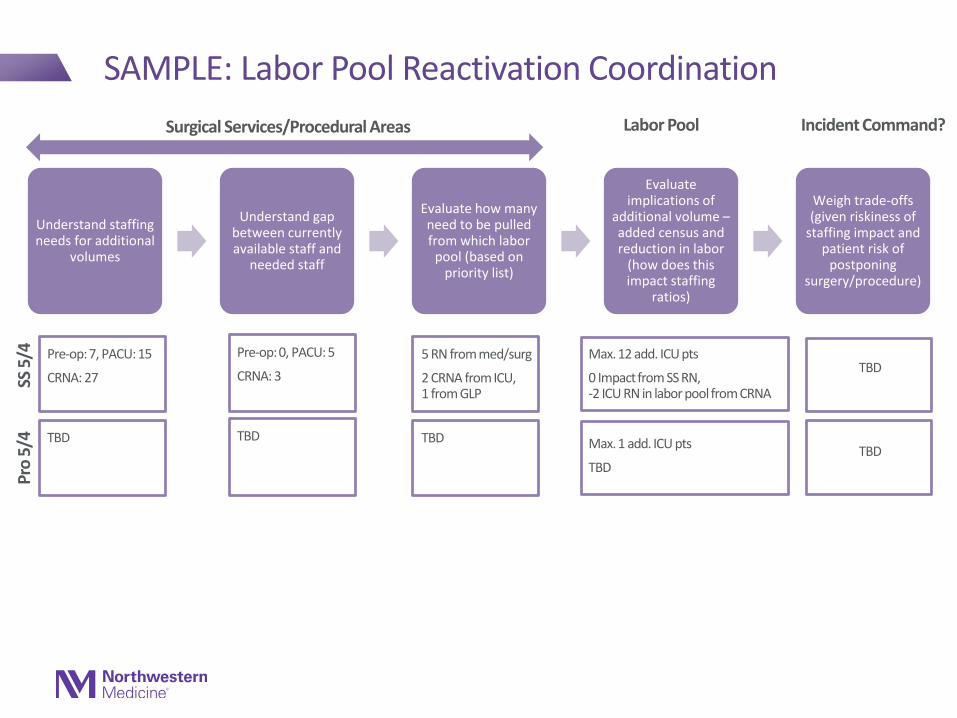
Understand staffing needs for additional
volumes
Understand gap between currently available staff and
needed staff
Evaluate how many need to be pulled from which labor
pool (based on priority list)
Evaluate implications of
additional volume –added census and reduction in labor
(how does this impact staffing
ratios)
Weigh trade-offs (given riskiness of
staffing impact and patient risk of
postponing surgery/procedure)
SAMPLE: Labor Pool Reactivation Coordination
Surgical Services/Procedural Areas Labor Pool Incident Command?
Pre-op: 7, PACU: 15
CRNA: 27
Pre-op: 0, PACU: 5
CRNA: 3
5 RN from med/surg
2 CRNA from ICU, 1 from GLP
Max. 12 add. ICU pts
0 Impact from SS RN, -2 ICU RN in labor pool from CRNA
TBD
SS 5
/4
TBD TBD TBD Max. 1 add. ICU pts
TBDTBD
Pro
5/4