course preparation materials - lvi global...course preparation materials surgery 3: live implant...
TRANSCRIPT
COURSE PREPARATION MATERIALS
Surgery 3:
Live Implant Patient: Case Planning & Implant
Placement of your choice
Important Risk Management Packet Included
LVI Global
1401 Hillshire Drive, Ste 200 Las Vegas, NV 89134
www.lviglobal.com 888.584.3237
LVI Global | [email protected] | 702.341.8510 fax
Please fax the items below to LVI Global Attention: Risk Management 702-341-8510 unless
otherwise noted.
Your travel plans should not be made until your patient has been approved by Dr. Leo Malin.
□ Student Information Form
□ Agreement For The Dentist Participant
□ Release of Liability Agreement
□ Patient Informed Consent Forms
□ Implant Patient Information and Consent Forms
□ Information Verification
□ Documentation of Work Done at Home Office
□ Medical History Form
□ Periodontal Evaluation (please state health of tissue if a probing is not available.)
□ Have an original certificate of licensure sent from your state board to:
LVI Global Attn: Risk Management
1401 Hillshire Dr. Ste 200
Las Vegas, NV 89134
□ Copy of your current liability insurance- License and Insurance must be effective through
entire course.
For case approval, you must send the following to Dr. Malin at least 4 weeks prior to the course
date at the address below:
Upper and Lower Study models
Pano or FMX
Digital Photos
Medical History
Periodontal Evaluation
Proposed Treatment Plan
Leo Malin DDS
c/o Risk Management
1401 Hillshire Dr. Ste. 200
Las Vegas, NV 89134

LVI Global | [email protected] | 702.341.8510 fax
All of us at LVI want your time here to be the best learning experience possible. It is most
important that your patient selection is to your advantage. In view of that, we must require that
your case selection comply with our guidelines. In our optimal scenario cases should exhibit the
following characteristics:
A medical history that is not compromised (cancer, diabetes, heavy smoker, etc.)
Patients must show good oral hygiene with recare within the past year.
These are general guidelines you are asked to follow. They are guidelines put in place to enable
us to follow all legal standards for this course. Any patient could have sub-clinical problems that
are not intended to be diagnosed at this time. As providers of dental care, we all must realize
that possible TMD problems are not always predictable, and changing the occlusion may cause a
hidden problem to arise. These possibilities should be addressed on the patient informed
consent form.
LVI Global | [email protected] | 702.341.8510 fax
Please read this prior to reviewing the Risk Management Documents with your patient.
It is imperative that your patient is thoroughly informed of the procedures to be performed on
them here at LVI Global. It is also imperative that your patient realizes that although you are a
licensed dentist that you will be in a training situation and applying newly learned techniques. It
is also imperative that your patient understands that they have options to the proposed
treatment for this program including no treatment at all. It should be explained to your patient
that they have the right to change their mind and refuse treatment prior to the treatment plan
being started.
Do not leave any portion of the Risk Management forms blank. Please make certain the patient
consent form is completed and explained before being signed by your patient.
As a doctor it is important that you and your patient understand that there is always some
potential harm in having any procedure performed. The more forthright you are in relaying and
explaining the possibility of adverse effects to your patient the better protected you both will
be; no matter how obscure you may perceive these effects to be.
Please note that we do require that your information is current each time you participate in a
live patient program. As of January 2008, we are now required to obtain a certification of
licensure, sometimes referred to as verification of license. This must be requested from your
state board and mailed directly to LVI Global. This is not to be confused with your certified
license as those are only sent to you and should stay at your practice. We will keep your license
on file and update it online for you for future live patient courses you attend~provided your
state has this feature available.
Please do not hesitate to contact us with any questions or concerns you may have.
888.584.3237 [email protected]

LVI Global | [email protected] | 702.341.8510 f
Please complete this form and mail or fax to:
LVI Global 1401 Hillshire Dr. Ste 200 Las Vegas, NV 89134 (888)584-3237 Fax (702)341-8510
Personal Information
First Name Preference: ______________________ Last: _____________________________ MI _______
Office Address: ______________________________________________________________________
Circle one: Designation DDS DMD Other_____________
Office Phone #: ___________________________________ Office Fax: __________________________
Home Phone #: ____________________________________Home Fax:__________________________
Mobile Phone # _______________________________________________________________________
E-Mail Address: ________________________________________________________________________
AGD #: ______________________________________________
License #: ____________________________________________________________________________
Educational Background Dental School: ____________________________________ Degree: _________________ Year: _______
Graduate Residency: ____________________________________________________________________
Do you teach? ________________________ If so, where? ______________________________________
How many years have you practiced dentistry? _______________________________________________
What procedures do you prefer doing the least and why? What is the main reason you are attending this program? What do you hope to get out of the program? What are your main concerns about cosmetic dentistry? How many of the following procedures do you do a month? Porcelain Veneers __________ Direct Resin Restorations _________ PFM’s _______ All Porcelain Crowns __________ Indirect Resin Restorations _________ Amalgam Fillings _______ Gold Inlays/Onlays __________ Non-Metallic Bridge _________ Direct Resin Veneers ______
Do You Operate:
Right Handed
Left Handed
Do You Consider Yourself:
Beginning esthetic dentist Experienced esthetic dentist
Intermediate esthetic dentist Highly experienced esthetic dentist
LVI Global | [email protected] | 702.341.8510 f
Patient’s Name
Please complete this form and mail or fax to:
LVI 1401 Hillshire Dr. Ste 200 Las Vegas, NV 89134 (888)584-3237 Fax (702)341-8510
I, ______________________________________, am a participant in a continuing dental education program, Surgery 3: Live Implant Patient: Case Planning & Implant Placement of your choice, at the Las Vegas Institute for Advanced Dental Studies on ______________20___. Pursuant to class curriculum, I willingly agree to participate in a clinical situation at or sponsored by the Las Vegas Institute for Advanced Dental Studies. I understand and agree that I will be required to conform to the institute policies and procedures during the time I spend in the clinic. I understand and agree to take direction from the clinic faculty and his/her designees. I hereby verify and confirm that _________________ is my patient of record. I also agree that I am responsible
for all the follow–up remedial care on my patient for this course.
My current liability insurance coverage is with: Name of Insurance Company _____________________________________________________
Please Print Dr.’s Name _____________________________________________________
Doctor’s Signature _____________________________________________________
Date _____________________________________________________
(______) I have requested a certification of licensure from my state board on ____________. Initial Date
LVI Global | [email protected] | 702.341.8510 f
Please complete this form and mail or fax to:
LVI 1401 Hillshire Dr. Ste 200 Las Vegas, NV 89134 (888)584-3237 Fax (702)341-8510
Release of Liability Agreement
I am participating in the LVI Course, Surgery 3: Live Implant Patient: Case Planning & Implant Placement of your choice on ______, 20__. In consideration of the opportunity to participate in this program, I hereby release the Las Vegas Institute for Advanced Dental Studies, their officers, directors, employees, and agents from any claim, damage of liability for or arising out of an injury or death which could result from my own actions or omissions or the actions or omissions of any employee or agent of the Curators of the Las Vegas Institute for Advanced Dental Studies. ___________________________________ Print Name of Dentist Participant ___________________________________ _________ Signature of Dentist Participant Date
LVI Global | [email protected] | 702.341.8510 f
Please complete this form and mail or fax to:
LVI 1401 Hillshire Dr. Ste 200 Las Vegas, NV 89134 (888)584-3237 Fax (702)341-8510
Attendee’s Full Name:__________________________________________________________ (for awards, certificates and continuing education credits)
Nick Name: ___________________________________________________________________
(if applicable, for name tags) Dental License #: _______________________________________________________________ (for continuing education credits) Attendee Signature: ___________________________________________________________
LVI Global | [email protected] | 702.341.8510 f
Please complete this form and mail to:
LVI 1401 Hillshire Dr. Ste 200 Las Vegas, NV 89134 (888)584-3237 Fax (702)341-8510
Surgery 3: Live Implant Patient: Case Planning & Implant Placement of your choice
Patient Name___________________________________________________________________________________________
Nature of Treatment to be Rendered: ____________________________________________________ including teeth #__________ Benefits of Treatment_____________________________________________________________________________________
Patient to Initial Each Line
I hereby verify and confirm that I am a patient of record of Dr. ______________________________________ (“my Doctor”). I agree and hereby consent to my Doctor performing dental work for and upon me as part of a “live patient” continuing dental education training course my Doctor will be attending at Las Vegas Institute for Advanced Dental Studies (“LVI”) in Las Vegas, Nevada. I understand the primary purpose of this continuing dental education course is to educate and train my Doctor, in a “live patient” training situation, on techniques and procedures to be performed upon me in my Doctor’s office and in the clinic at LVI. I further state that the nature and extent of the techniques, procedures, and treatment I will be receiving (my “Treatment Plan”) have been explained to me by my Doctor. My Doctor has informed me about the potential risks of using the techniques which will be applied by my Doctor as part of my Treatment Plan, and I understand my Doctor may have limited experience with such techniques he/she will be learning at LVI. I further understand that my Doctor, who will be performing such dental services for and upon me during or as part of his/her participation in a “live patient” course at LVI, will be doing so as an independent professional, and my Doctor will not be performing such services in any way as an agent or employee of LVI or any benefit of LVI or any of its employees.
My Doctor also has informed me of alternative procedures that are available to me and my options with respect to each such available alternative procedure. I am aware that one such option that is available to me is that I receive no treatment at all. Having considered the options and alternative procedures available to me, I have agreed to the specific Treatment Plan to be completed by my Doctor. I am aware that I have the absolute right to discontinue treatment at any time. I have been advised by my Doctor of the post-operative care that is necessary for me to receive after the procedure is performed at LVI, and I am aware that such post-operative care will occur at my Doctor’s office. It is my understanding that all follow-up/ remedial care will be rendered by my Doctor.
PATIENT: WITNESS: _____________________________________ __________________________________________ Signature Date Witness Date _____________________________________ _________________________________________ Printed Name Printed Name
Potential Consequences: Alternatives to treatment:
Patient Initials Patient Initials
Future need for further restorations, treatment, implant revision surgery
Long-span bridge
Potential for peri-implant or surgical site infection Removable prosthetics
Potential for fractured implant/abutment/restoration No treatment
Potential for restoration complications Other:
Inadequate bone growth or implant integration
Other:
LVI Global | [email protected] | 702.341.8510 f
Patient’s Name
DOCUMENTATION OF WORK DONE AT HOME OFFICE IN PREPARATION OF THE PATIENT AND TREATMENT PLAN
Please complete this form in its entirety. Do not leave any portion of question #3 unanswered. This should be completed from both a liability and dental standpoint. Note: (Please do not make travel plans prior to receiving approval of your case. The earlier that you get the case information in, the easier it is for you to plan.) 1. Please indicate any radiographs and/or tomograms you have taken of your patient in preparation for this course and the date taken. (please include dates) ______________________________________________________________________________ 2. Please indicate if a Smile Analysis was completed, and the date the diagnosis was determined. ______________________________________________________________________________ ****3. Please indicate the Treatment Plan including: a) treatment options that have been presented to your patient, b) option you and your patient chose, c) age and sex of your patient d) exact treatment plan to be preformed (including detail). ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________ I hereby verify and confirm that _________________ is my patient of record. I also agree that I am
responsible for all the follow–up remedial care on my patient for this course.
Participating Doctor’s Signature ______________________________________ Printed Name ______________________________________________________
LVI Global | [email protected] | 702.341.8510 fax
Dr.:_______________________________________
I have been informed and I understand the purpose and the nature of the implant
surgery procedure. I understand what is necessary to accomplish the placement of
the implant under the gum or in the bone.
My doctor has carefully examined my mouth. Alternatives to this treatment have
been explained. I have tried or considered these methods, but I desire an implant to
help secure the replaced missing teeth.
I have further been informed of the possible risks and complications involved with
surgery, drugs, and anesthesia. Such complications include pain, swelling, infection
and discoloration. Numbness of the lip, tongue, chin, cheek or teeth may occur. The
exact duration may not be determinable and may be irreversible. Also possible are
Inflammation of a vein, injury to teeth present, bone fractures, sinus penetration,
delayed healing, allergic reactions to drugs or medications used, etc.
I understand that if nothing is done, any of the following could occur: bone disease,
loss of bone, gum tissue inflammation, infection, sensitivity, looseness of teeth,
followed by necessity of extraction. Also possible are temporomandibular joint (jaw)
problems, headaches, referred pains to the back of the neck and facial muscles and
tired muscles when chewing.
My doctor has explained that there is no method to accurately predict the gum and
the bone healing capacities in each patient following the placement of the implant.
It has been explained that in some instances implants fail and must be removed, I
have been informed and understand that the practice of dentistry is not an exact
science; no guarantees or assurance as to the outcome of results of treatment or
surgery can be made.
I understand that excessive smoking, alcohol, or sugar may effect gum healing and
may limit the success of the implant. I agree to follow my doctors home care
instructions. I agree to report to my doctor for regular examinations as instructed.
I agree to the type of anesthesia, depending on the choice of the doctor. I agree not
to operate a motor vehicle or hazardous device for at least 24 hours or more until
fully recovered from the effects of the anesthesia or drugs given for my care.
LVI Global | [email protected] | 702.341.8510 fax
To my knowledge I have given an accurate report of my physical and mental health
history. I have also reported any prior allergic or unusual reactions to drugs, food,
insect bites, anesthetics, pollens, dust, blood or body diseases, gum or skin
reactions, abnormal bleeding or any other conditions related to my health.
I consent to photography, filming, recording, and x-rays of the procedure to be
performed for the advancement of implant dentistry, provided my identity is not
revealed.
I request and authorize medical/dental services for me, including implants and other
surgery. I fully understand that during, and following the contemplated procedure,
surgery, or treatment, conditions may become apparent which warrant, in the
judgment of the doctor, additional or alternative treatment pertinent to the success
of comprehensive treatment. I also approve any modification in design, materials, or
care, if it is felt this is for my best interest.
______________________________________________________________________
Signature of Patient, Parent or Guardian (If the patient is unable to sign or is a minor)
______________________________________________________________________
Witness
_____________________________________________________________________
Relationship to Patient
LVI Global | [email protected] | 702.341.8510 f
Please complete this form and mail to:
LVI 1401 Hillshire Dr. Ste 200 Las Vegas, NV 89134 (888)584-3237 Fax (702)341-8510
During certain educational courses at LVI, your photographs may be used for educational
purposes. Use of the photos, may include but not be limited to presentation in a course
teaching manual and/or presented in a power point lecture. As a patient, we request that you
sign the attached release form, prior to the use of your photographs.
I, _________________________, consent and authorize an instructor and LVI to use my name
or a photograph, photographs, video, slides-7 scans or any other image as may be necessary of
me, with or without my name, or with a fictitious name for advertising, trade, or any other
lawful purpose and I release and forever discharge either or both of them from any claim,
demands, or liability on account of such use or for the quality of the reproduction of the
photograph or photo copy provided.
Patient Signature: ____________________________________Date:______________________
Printed Name: __________________________________________________________________
Treating Doctor’s/ Instructor’s Name: _______________________________________________
Printed Name: __________________________________________________________________
Witness: ___________________________________________ Date: _______________________
Printed Name: __________________________________________________________________
LVI Global | [email protected] | 702.341.8510 fax
Diagnosis. After a careful oral examination and study of my dental condition, my dentist has advised me that I have periodontal disease. I understand that periodontal disease weakens support of my teeth by separating the gum from the teeth and possibly destroying some of the bone that supports the tooth roots. The pockets caused by this separation allow for greater accumulation of bacteria under the gum in hard to clean areas and can result in further erosion or loss of bone and gum supporting the roots of my teeth. If untreated, periodontal disease can cause me to lose my teeth and can have other adverse consequences to my health. Recommended Treatment. In order to treat this condition, my dentist has recommended that my treatment include bone regenerative/grafting surgery. I understand that a local anesthetic will be administered to me
as part of the treatment. I further understand that antibiotics and other disinfecting substances may be applied to the roots of my teeth. During this procedure, my gum will be opened to permit better access to the roots and to the eroded bone. Inflamed and infected gum tissue will be removed, and the root surfaces will be thoroughly cleaned. Bone irregularities may be reshaped. Graft material will be placed in the areas of bone loss around the teeth. Various types of graft materials may be used. These materials may include my own bone (autograft), synthetic bone substitutes (alloplast), bone obtained from animals, notably cattle and pigs (xenografts), bone obtained from tissue banks (allograft), or combinations of these product categories. Safety and sterility of all products used is on the utmost importance to your doctor and staff. Membranes or barriers may be used to cover the bone graft. My gum will be sutured back into position over the above materials, and a periodontal bandage or dressing may be placed. I further understand that unforeseen conditions may call for a modification or change from the anticipated surgical plan. These may include, but are not limited to, (1) extraction of hopeless teeth to enhance healing of adjacent teeth, (2) the removal of a hopeless root of a multi-rooted tooth so as to preserve the tooth, or (3) termination of the procedure prior to completion of all of the surgery originally outlined. Expected Benefits. The purpose of bone regenerative surgery is to reduce infection and inflammation and to restore my gum and bone to the extent possible. The surgery is intended to help me keep my teeth in the operated areas and to make my oral hygiene more effective. It should also enable professionals to better clean my teeth. The use of bone, bone graft material, or the placement of a membrane is intended to enhance bone and gum healing. Principal Risks And Complications. I understand that a small number of patients do not respond
successfully to bone regenerative procedures. This procedure may not be successful in preserving function or appearance. Because each patient’s condition is unique, long-term success may not occur. In rare cases the involved teeth may ultimately be lost. I understand that complications may result from the periodontal surgery involving bone regenerative materials, drugs, or anesthetics. These complications include, but are not limited to post-surgical infection, bleeding, swelling and pain, facial discoloration, transient but on occasion permanent numbness of the jaw, lip, tongue, teeth, chin or gum, jaw joint injuries or associated muscle spasm, transient but on occasion permanent increased tooth looseness, tooth sensitivity to hot, cold, sweet or acidic foods, shrinkage of the gum upon healing resulting in elongation of some teeth and greater spaces between some teeth, cracking or bruising of the corners of the mouth, restricted ability to open the mouth for several days or weeks, impact on speech, allergic reactions, and accidental swallowing of foreign matter. In the event that donated tissue is used for the graft, the tissue should have been tested for hepatitis, syphilis, and other infectious disease. Nevertheless, there is a remote possibility that tests will not determine the presence of diseases in a particular donor tissue. The exact duration of any complications cannot be determined, and they may be irreversible.
There is no method that will accurately predict or evaluate how my gum and bone will heal. I understand that there may be a need for a second procedure if the initial surgery does not meet pretreatment expectations. In addition, the success of bone regenerative procedures can be affected by medical conditions, dietary and nutritional problems, smoking, alcohol consumption, clenching and grinding of teeth,
LVI Global | [email protected] | 702.341.8510 fax
inadequate oral hygiene, and medications that I may be taking. To my knowledge I have reported to my dentist any prior conditions that might in any way relate to this surgical procedure. I understand that my diligence in providing the personal daily care recommended by my dentist and taking all medications as prescribed are important to the ultimate success of the procedure. Alternatives To Suggested Treatment. Alternatives to periodontal surgery with bone regenerative/grafting
surgery include: (1) No treatment – with the expectation of possible advancement of my condition which may result in premature loss of teeth, (2) extraction of a tooth or teeth involved with periodontal disease, (3) non-surgical scraping of tooth roots and lining of the gum (scaling and root planing), with or without medication, in an attempt further to reduce bacteria and tartar under the gum line. The risk of no treatment is the worsening of my condition and the premature loss of teeth. Necessary Follow-up Care and Self-Care. Existing restorative dentistry can be an important factor in the success or failure of periodontal therapy. My dentist may make recommendations for the placement of restorations, the replacement of existing restorations or their modifications, the joining of two or more of my teeth, the extraction of one or more teeth, the performance of root canal therapy, or the movement of one, several, or all of my teeth. I understand that the failure to follow such recommendations could lead to ill effects, which would become my sole responsibility. I recognize that natural teeth and their artificial replacement should be maintained daily in a clean, hygienic manner. I will need to come for appointments following my surgery so that my healing may be monitored and so that the dentist can evaluate and report on the outcome of surgery upon completion of healing. Smoking or alcohol intake may adversely affect gum healing and may limit the successful outcome of my surgery. I know that it is important (1) to abide by the specific prescriptions and instructions given by my dentist and (2) to see my dentist and hygienist for periodic examination and preventative treatment. Maintenance also may include adjustment of prosthetic appliances. No Warranty Or Guarantee. I hereby acknowledge that no guarantee, warranty or assurance has been given to me that the proposed treatment will be successful. In most cases, the treatment should provide benefit in reducing the cause of my condition and should produce healing, which will help me keep my teeth. Due to individual patient differences, however, a dentist cannot predict certainty of success. There is a risk of failure, relapse, additional treatment, or even worsening of my present condition, including the possible loss of certain teeth, despite the best of care. Publication of Records. I authorize photos, slides, x-rays or any other viewings of my care and treatment
during or after its completion to be used for the advancement of dentistry and reimbursement purposes. My identity will not be revealed to the general public, however, without my permission.
I CERTIFY THAT I HAVE READ AND FULLY UNDERSTAND THIS DOCUMENT PATIENT CONSENT
I have been fully informed of the nature of bone regenerative surgery, the procedure to be utilized, the risks and benefits of periodontal surgery, the alternative treatments available, and the necessity for the follow-up and self-care. I have had an opportunity to ask any questions I may have in connection with the treatment and to discuss my concerns with my dentist. After thorough deliberation, I hereby consent to the performance of bone regenerative surgery as presented to me during consultation and in the treatment plan presentation as described in this document. I also consent to the performance of such additional or alternative procedures as may be deemed necessary in the best judgment of my dentist. __________ ___________________ ____________________________
Date Name (Signed) Patient OR Name (Signed) Parent or Guardian (If patient is unable to sign or is a minor) __________ ___________________ ____________________________ Date Signature of Doctor Witness (Signed)
(Follow-up appointment will be needed.)
LVI Global | [email protected] | 702.341.8510 fax
I hereby authorize Dr. _______________________ and whomever he may designate as his
assistants/instructor to perform upon me the following operation and procedures:
Extraction of Teeth #’s _____________________________________
And if any unforeseen condition arises in the course of these designated operations or procedures
calling, in their judgment, for procedures in addition to or different from those now contemplated,
I further request and authorize them to do whatever they deem advisable, including extraction of
the tooth if in his judgment the tooth has a very poor prognosis.
I am informed and fully understand that inherent in any type of surgery are certain unavoidable
complications. In Oral surgery the most common of these complications include leaving a small
piece of root in the jaw if removal of the root would require extensive surgery, post-operative
bleeding, swelling or bruising, discomfort, stiff jaws, loss or loosening of dental fillings. Less
common complications can include infection, loss of or injury to adjacent teeth and soft tissues,
nerve disturbances (i.e., numbness of lip, chin and tongue), broken jaw, sinus exposure and
swallowing or inhaling of instruments, fillings or teeth into lungs.
I further consent to the administration of local anesthesia, antibiotics, analgesics or any other
drugs that may be deemed necessary in my case, and understand that there is a slight element of
risk inherent in the administration of any drug or anesthesia. This risk includes adverse drug
response (e.g., allergic reactions), heart stoppage, and inhaling of stomach contents into lungs.
I realize that it is mandatory that I give as accurate and complete medical and personal history as
possible, follow any and all instructions as directed and permit prescribed diagnostic procedures.
I further realize that in spite of the possible complications, my contemplated surgery is necessary
and is desired by me. I am aware that the practice of dentistry and surgery is not an exact science
and I acknowledge that no guarantees have been made to me concerning the results of the
operation or procedure.
Further explanation of all complications of surgery and anesthesia is available to me upon my
request from the Doctor.
__________ __________________ ____________________________
Date Name (Signed) Patient OR Name (Signed) Parent or Guardian (If patient is unable to sign or is a minor)
__________ ___________________ ____________________________
Date Signature of Doctor Witness (Signed)
MEDICAL HISTORY
Patient Name: DOB: Sex:
Height:
Weight:
Y
N
Y
N
Y
N
__ __ Abnormal Bleeding __ __ Glaucoma __ __ Stroke __ __ Alcohol Abuse __ __ Hay Fever __ __ Thyroid Problems __ __ Allergies __ __ Heart Attack __ __ Tuberculosis __ __ Anemia __ __ Heart Surgery __ __ Ulcers __ __ Angina Pectoris __ __ Hemophilia __ __ Venereal Disease __ __ Arthritis __ __ Hepatitis A __ __ Yellow Jaundice __ __ Artificial Bones __ __ Hepatitis B __ __ Do you smoke/use tobacco? __ __ Artificial Heart Valves __ __ High Blood Pressure If you are female: __ __ Asthma __ __ HIV & AIDS __ __ Are you taking birth control? __ __ Blood Transfusion __ __ Kidney Problems __ __ Are you pregnant? __ __ Cancer Chemotherapy __ __ Liver Disease __ __ Are you nursing? __ __ Colitis __ __ Low Blood Pressure __ __ If yes # of weeks:_________ __ __ Congenital Heart Defect __ __ Mitral Valve Prolapse Allergies: __ __ Cosmetic Surgery __ __ Pace Maker __ __ Aspirin __ __ Diabetes __ __ Pneumocystitis __ __ Codeine __ __ Difficulty Breathing __ __ Psychiatric Problems __ __ Dental Anesthetics __ __ Drug Abuse __ __ Radiation Therapy __ __ Erythromycin __ __ Emphysema __ __ Rheumatic Fever __ __ Jewelry __ __ Epilepsy __ __ Seizures __ __ Latex __ __ Fainting Spells __ __ Shingles __ __ Metals __ __ Fever Blisters __ __ Sickle Cell Disease __ __ Penicillin __ __ Frequent Headaches __ __ Sinus Problems __ __ Tetracycline
Other: Are you currently taking any medications (including aspirin)? If yes, please list: Is there any disease, condition or problem that you think this office should know about that is not covered above? If yes please explain: Signature:
Date:
(Parent or Guardian if under 18)
PERIODONTAL EVALUATION FORM
Please indicate on the charts below and in writing any concerns regarding the periodontal health of the patient and treatment required before and/or during the case treatment plan for this patient. Please document if the patient’s periodontal health requires no special attention.
PERIODONTAL CHARTING RECORD
Name: Medical Alert: Date: Mobility Probe 3 Probe 2 Probe 1
Date:
Date:
Date:
Buccal
Probe 1 Probe 2 Probe 3
Probe 3 Probe 2 Probe 1
BuccalLingual
Lingual
LEGENDS:
Probe 1 Probe 2 Probe 3 Mobility
LVI Global | [email protected] | 702.341.8510 fax
Registration fees are non-refundable and must be exercised within two years. LVI Global, LLC
(“LVI”) reserves the right to cancel courses 45 days prior to the scheduled date of a course or
activity. Should LVI cancel a course or activity, LVI will apply the full value of any deposits and
fees related to said course or activity to future LVI course or activities. Should LVI cancel a
course or activity, you may also have the option of having the deposits returned to you. Fees
remain non-refundable but, may be reapplied to another course or activity. LVI will not be
responsible for any other fees, costs or consequential damages associated with canceling this
LVI course or activity with the exception of non-refundable transportation or accommodation
fees booked through LVI Travel. For courses requiring a live-patient, the treating Doctor must
bring a patient of record. During courses conducted at LVI, I understand that photographs or
video may be taken of me for educational and marketing purposes. I hold harmless LVI for any
liability resulting from this production. I waive any right to inspect the finished production as
well as advertising materials in conjunction with these photographs. I understand that I may
receive marketing materials as a result of my attendance. In addition, by my signature on this
form, I authorize LVI or its partners to contact me via mail, facsimile or email.
Change/Cancellation/Postponement Policy:
- A change, cancellation or postponement of course date is not complete without your required
signature and date.
The following do not apply if moving from TBD status to date selection
- If change, cancellation, or postponement is received 60-90 days prior to registered course, 25%
of the course fee will be forfeited.
- If change, cancellation, or postponement is received within 60 days, 50% of the course fee will
be forfeited.
- If change, cancellation, or postponement is received less than 30 days prior to your registered
class, 100% of the course fee will be forfeited.
LVI Global | [email protected] | 702.341.8510 fax
This course features live-patient treatment. You must bring a patient from your practice.
Please complete the following protocol in order.
Send enclosed IMPORTANT forms 6 weeks prior to the course date to LVI. These vital
documents are the first step in getting your patient’s case approved. You may fax them to
(702) 341-8510 Attention: Risk Management.
Student Information Form
Liability Form
Patient Informed Consents
Information Verification
Implant Consent
Documentation of work done in Home Office
Medical History form
Periodontal Evaluation Form
Copy of your current license to practice dentistry with expiration date
Have an original certificate of licensure sent from your state board to:
LVI Global Attention: Risk Management 1401 Hillshire Dr. Ste 200 Las Vegas, NV 89134
Copy of your current liability insurance-must be effective through course.
Collect your patient’s case submission materials including:
Photos of the proposed implant site
A panorex, periapical, Tomograph or CT of the proposed patient (whichever you have)
A study model of the proposed patient
Patient’s medical history report that contains any information that may affect an
implant placement
A proposed treatment plan for this patient
Mail your patient’s case submission materials for approval to:
Dr. Leo Malin C/O Risk Management 1401 Hillshire Dr. Ste 200 Las Vegas, NV 89134
LVI Global | [email protected] | 702.341.8510 fax
Radiographs and Photos can be uploaded using yousendit.com
Upload instructions
Before beginning, RENAME each individual picture you are uploading
BEFORE UPLOAD so that the name of the doctor attending and the course
name is included in the filename. For example, each picture should be
“John Smith Core II 01.jpg”, “John Smith Core II 02.jpg”,etc.
Using your Web browser, go to
http://dropbox.yousendit.com/AmberHaggard619291
Type in your email
In the subject field type the course name and date and your name For
example, Core II March/April 2011 John Smith
Upload only your PROPERLY NAMED photos
If you have any issues call Programs at 702-341-7978.
Dr. Malin will review each submission for acceptance the day the materials are received.
Please do not skip this step because of a previous approval with Dr. Malin. Even though Dr.
Malin reviews a lot of cases during the Implant I, Bone Grafting, and possibly on the golf
course, he must have all of the materials regardless of previous approvals.
Once your case is approved, you must send both upper and lower impressions/models to
Aurum Ceramics for fabrication of your patients scanning appliance.
Send To: Aurum Ceramics
Attention: Grant Maier
1401 Hillshire, Suite 120
Las Vegas, NV 8913
Please use the enclosed Implant Lab Prescription
LVI Global | [email protected] | 702.341.8510 fax
IMPLANT PRESCRIPTION
(Do not send this to the lab until the case is approved by Dr. Malin)
DR. __________________________________________________
__________________________________________________
PATIENT’S NAME: _____________________________________________________
SEX: M / F AGE: ________________________
TOOTH #’S TO BE RESTORED: __________________________________________
o FABRICATE SCANNING APPLIANCE
o FABRICATE SURGICAL STENT AFTER CT SCAN IS COMPLETED (This will be done during the implant II course. Return appliance and disc)
INSTRUCTIONS:
Please include a full arch polyvinyl impression of both upper and lower, as well as bite registration.
Please note: Normal lab fees will apply
SIGNATURE: __________________________________________________________
LICENSE NO: ______________________
SEND TO: AURUM CERAMICS
Attention: Implants C/O Grant Maier 1401 Hillshire, Suite 120 Las Vegas, NV 89134
LVI Global | [email protected] | 702.341.8510 fax
Please note travel expenses are not included in your tuition. Visit the LVI Global website for the most up to date travel information.
LVI Global | [email protected] | 702.341.8510 fax
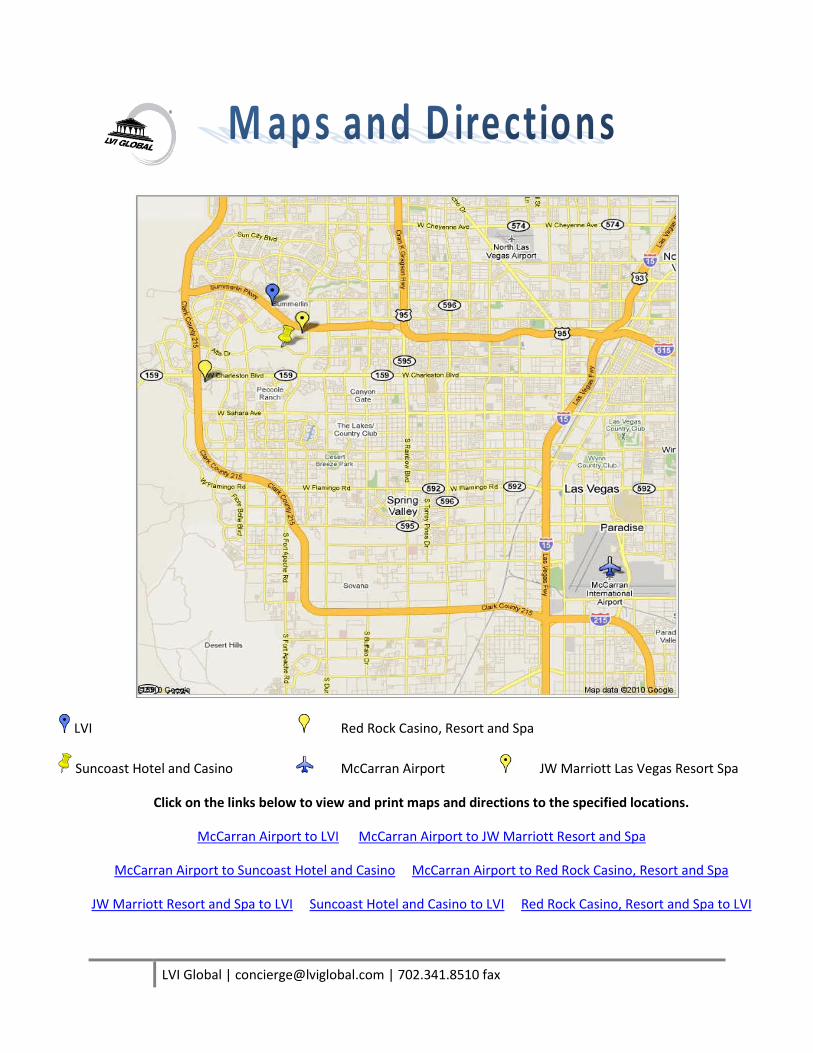
LVI Red Rock Casino, Resort and Spa
Suncoast Hotel and Casino McCarran Airport JW Marriott Las Vegas Resort Spa
Click on the links below to view and print maps and directions to the specified locations.
McCarran Airport to LVI McCarran Airport to JW Marriott Resort and Spa
McCarran Airport to Suncoast Hotel and Casino McCarran Airport to Red Rock Casino, Resort and Spa
JW Marriott Resort and Spa to LVI Suncoast Hotel and Casino to LVI Red Rock Casino, Resort and Spa to LVI
LVI Global | [email protected] | 702.341.8510 fax
What is the weather like in Las Vegas?
In the winter months temperatures range from 15-60. In spring the weather is nice with highs
between 70-80. Summer months are hot, highs up to 110, with nice warm summer nights. In
the fall it cools down with temperatures back around 70-80 degrees.
What should I wear when I come to LVI?
Business casual. We tend to keep the building cold so you might want to bring a light
sweater.
What should I wear if I am treating a patient in the clinic?
Just as you would in your office, appropriate Clinical Attire is expected at LVI. Attire should
conform to OSHA/CDC guidelines and regulations, and should include protection like closed toed
shoes for all of the team in the clinical setting.
Is food served at LVI?
A continental breakfast is served at 7:00 each morning and lunch is provided each afternoon.
Snacks are also available throughout the day.
How far is the Las Vegas Strip from LVI?
Approximately 12 miles. It could take up to 30 minutes with traffic.
Do you provide transportation to LVI?
LVI provides transportation only from the J.W. Marriott and The Red Rock Hotels. Check
with the Bell Stand for pick up times on course days.
Where do I check-in when I first arrive at LVI?
For every course you attend at LVI, you must check-in on the first day in the Hillwood Building
(the main building). However breakfast will be served in the Bistro located in the Hillshire
Building (the new building).
LVI Global | [email protected] | 702.341.8510 fax
How many CE hours can I expect to receive from this course?
After completing this program, you will receive a CE form of the appropriate AGD approved
continuing education credit hours. These credits represent the lecture and participation portion
of the course.
When will I receive my CE credits?
Your CE form will be presented along with your attendance medallion and/or letter. Please keep
a copy of this form in your office records.
Does LVI submit my CE credits for me?
We will submit your CE credits to the AGD if you provide us with your AGD number. It is your
responsibility to keep the CE form indicating your credits on file in your office and, if necessary
submit your CE hours to the appropriate organization(s) (i.e.: your state/territory, etc.).
What happens if I lose my CE letter?
Once you receive your CE form, hold on to your originals and send copies when submitting your
organizations. If your original letters are misplaced, LVI must charge a $30.00, per course,
processing fee for necessary research. Replacement CE letters can take up to 3 weeks to
receive.
Educational Objectives:
The educational objectives for this course are for the participants to be able to:
Discuss various flap designs and suturing techniques.
Utilize ridge Augmentation techniques.
Complete advanced extraction cases.
Recognize when to graft or do an immediate implant placement.
Discuss the benefits of tunnel grafting, ridge splitting with immediate implant placement, block
grafting, and bone harvesting.
Discuss the advantages of Pieazo Electric surgery.
Utilize the applications for tenting screws and titanium- reinforced membranes for hard and soft
tissue grafting.
Utilize the technique of Lateral Sinus Grafting.
Discuss potential surgical complications and management.

LVI Global | [email protected] | 702.341.8510 fax
Discuss implant denture surgical protocols.
*Funding and/or materials for this course are supported in part by Zimmer