rotator cuff tendinopathy
TRANSCRIPT

Rotator Cuff Tendinopathy
Mr Puneet MongaConsultant Orthopaedic Shoulder Surgeon
Wrightington Hospital

Terminology
• Tendonitis / Tendinitis
• Tendinoses
• Tendinopathy

What’s the correct term to use ?
Terminology• Tendonitis / Tendinitis - Inflammation of the
tendon (rare)- Inappropriate terminology.
• Tendinoses- Degenerative condition- Tendon damage at cellular level.
• Tendinopathy - Disease of the tendon
What’s the function of the Rotator Cuff?

Function of a TendonForce Transmission from Muscle to bone


Function of the RC
• Rotation of the humerus w.r.t Scapula
• Compresses the head into the glenoid- dynamic stability
• Force coupling - Deltoid / Lattisimus / Pec Major

What’s the Aetiology of RC Tendinopathy

Causation of Rotator Cuff Tendinopathy
• Extrinsic factors
• Intrinsic factors

Acromial shapes
Bigliani, L. U.; Morrison, D. S.; and April, E. W.: The morphology of the acromion and its relationship to
rotator cuff tears. Orthop. Trans.,10: 228, 1986.10228 1986
Higher proportion of RC tears seen in Curved and Hooked Acromions
Image courtesy- Shoulderdoc.co.uk

Sub-acromial Wringer

Coronal Plane Patho-anatomy
AbductionNeutral Position
Repetitive Micro-trauma from external impingement

Sagittal - oblique Plane Pathoanatomy
Sub-Acromial volume

Subacromial Decompression
Sub-Acromial volume

Extrinsic Theory doesn’t explain it all
• RCT- Bursectomy vs Bursectomy + acromioplasty- No Difference
• Articular surface tendon damage more common
• No direct relation between acromial shape and impingement symptoms
Lewis J. Subacromial impingement syndrome: a musculoskeletal condition or a clinical illusion? Physical Therapy Reviews. 16(5):388-98. 2011

Let’s understand the normal tendon structure and healing….

Normal Tendon
Normal Cuff Tendon =
Collagen (Type I predominantly)
Elastin
Glycosaminoglycan
Proteoglycans
Water
Image Courtesy: www.ouhsc.edu

Injured tendon- Usual repair
Total Collagen decreases
Increased gene expression of Type I, VI, IX and III
Decreased Type II expression.
Repair and replacement of normal collagen
Andrew Carr, Paul Harvie Chapter; Tendon Injuries pp 101-118 Rotator Cuff Tendinopathy.In Tendon Injuries. Maffulli et al Springer, 2005.

Normal HealingRepetitive loading
Micro tears Healing
Cellular Repair

Compensated OveruseExcessive loading
Healing
Cellular Repair
So, what goes wrong in tendinopathy?

Tendinopathy
• Excessive remodelling in response to tendon damage during tendon repair
• Aberrant “quality” Collagen
“Stiffer Extracellular matrix”

Normal
Tendinopathy-Disorganised matrix
Cellular clumping
Is Tendon Structure Associated with symptoms in Chronic Achilles TEndinopathy?An update on pain mechanisms– Written by Robert-Jan de Vos, The Netherlands, Aspetar Sports Medicine Journal 2017

TendinopathyRepetitive loadingProne to
damage
Can we blame our genes ?

Role of genetics
Possible link with “ank” mutation
(This is seen in association with Progressive form of arthritis)
Gene codes for a protein which transports Pyrophosphate out of the cells…..so a defective gene leads to high concentration of PPi.
Increased Calcium deposition
Andrew Carr, Paul Harvie Chapter; Tendon Injuries pp 101-118 Rotator Cuff Tendinopathy.In Tendon Injuries. Maffulli et al Springer, 2005.

Ok, what about the tendon blood supply?

Role of blood supplyCodman’s Critical zone
Debated- perhaps decreased blood supply a result rather than a cause
“Chicken or egg”
May explain the location along with external impingement
Andrew Carr, Paul Harvie Chapter; Tendon Injuries pp 101-118 Rotator Cuff Tendinopathy.In Tendon Injuries. Maffulli et al Springer, 2005.
What’s the progression of Cuff tendinopathy ?

Unified Continuum Theory

• Why do some partial tears progress to Full
• Why do some small tears progress to large
• Why do only 4% massive tears develop Cuff tear arthritis
• Presence of Cuff tear without impingement / vice versa

Discontinuous and multifactorial modelAndrew Carr, Paul Harvie Chapter; Tendon Injuries pp 101-118 Rotator Cuff Tendinopathy.
In Tendon Injuries. Maffulli et al Springer, 2005.

Making a Diagnosis

Rotator Cuff Tendinopathy (and tears) may be asymptomatic

Using a Cluster approach recommended
• History
• Look Feel Move + Special Tests
• Investigations
Making a Diagnosis

Positive Special Test = Diagnosis!

History and physical examination provide little guidance on diagnosis of rotator cuff tears.
Jain NB, Yamaguchi K. Evid Based Med. 2014 Jun;19(3):108.

Role of Investigations
• Ultrasound - Good for soft tissues & dynamic
• Xray- Good screening tool for Bone / joint
• CT- Good for bone
• MRI- Good for soft tissues and cross sectional

Management
First line Management
• Activity Modification
• Analgesia
• Physiotherapy- Posture, motor control, stretching, strengthening, Manual therapy- 6 weeks

Physiotherapy
Principles
• Pain relief
• Maintaining Range of movement
• Progressive Strengthening

When would I expect physiotherapy to work?

Positive Predictors(1) Patient expectation of ‘complete recovery’ compared to a ‘slight improvement’ as ‘a result of physiotherapy treatment’,
(2) Lower pain severity specifically at rest,
(3) The absence of a previous major operation (shoulder surgery excluded),
(4) The absence of pain in the opposite upper quadrant and
(5) Change in pain or range of shoulder elevation with manual facilitation of the scapula during elevation of the arm.

Cortisone Injection in Cuff Tendinopathy

Is Tendinopathy inflammatory?
• No
• Biopsies- No inflammatory cells
• Degenerative changes
Sports Med. 1999 Jun;27(6):393-408.Histopathology of common tendinopathies. Update and implications for clinical management. Khan KM1, Cook JL, Bonar F,
Harcourt P, Astrom M.

1. Pragmatic reason
Neer’s Test - LA component Cross confirms the diagnosis
So, Why inject?
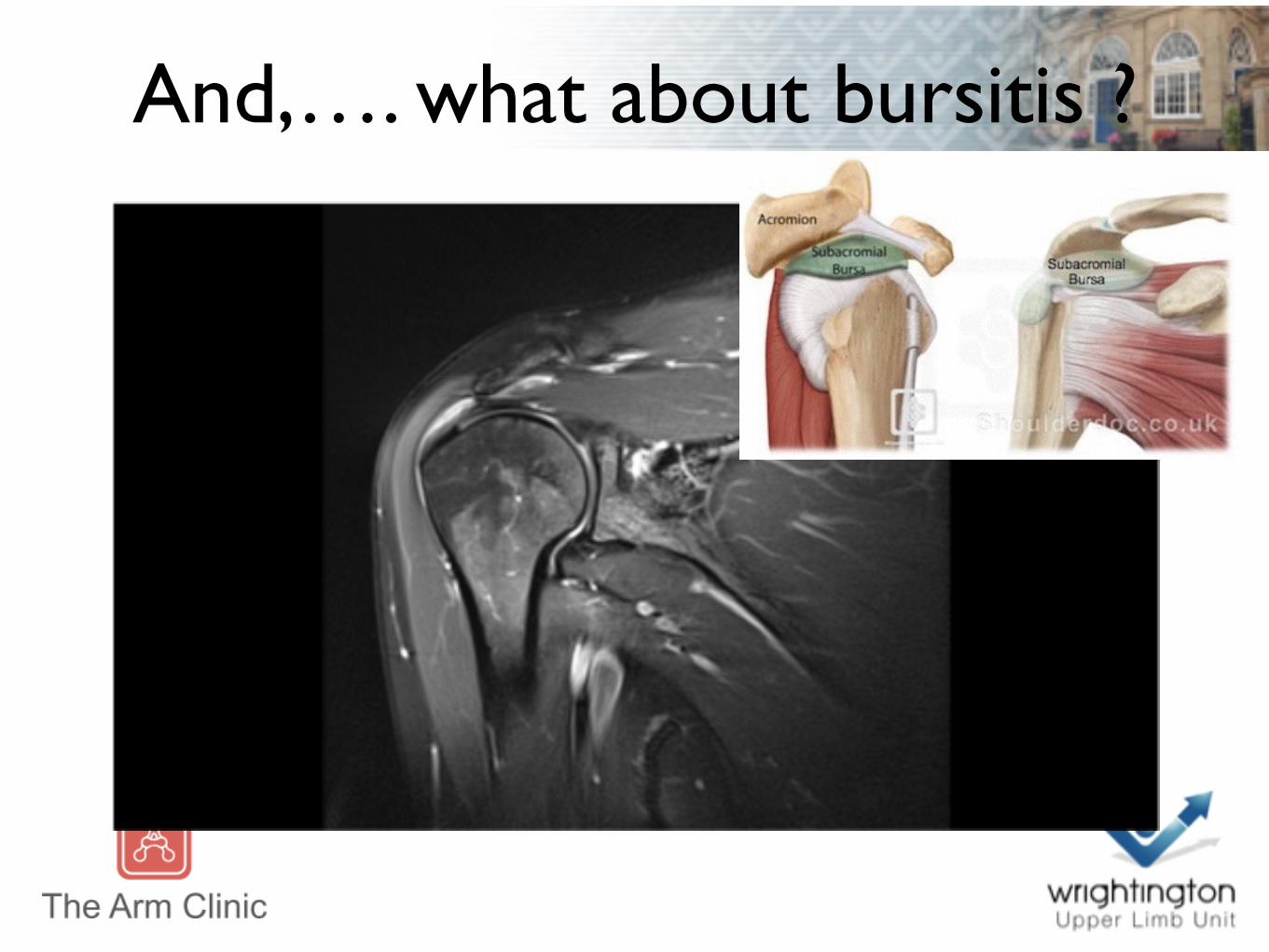
And,…. what about bursitis ?

Is Bursitis inflammatory?
• Yes
• Presence of Inflammatory mediators in Bursal biopsies
• Inflammatory mediators reduced following NSAIDs or cortisone injection
Arch Orthop Trauma Surg. 1992;111(6):336-40. Inflammation of the subacromial bursa in chronic shoulder pain. Santavirta S1, Konttinen YT, Antti-Poika I, Nordström D
J Shoulder Elbow Surg. 2005 Jan-Feb;14(1 Suppl S):84S-89S. The molecular pathophysiology of subacromial bursitis in rotator cuff disease. Blaine TA1, Kim YS, Voloshin I, Chen D, Murakami K, Chang SS, Winchester R, Lee FY, O'keefe RJ, Bigliani LU.
J Orthop Res. 2006 Aug;24(8):1756-64. Stromal cell-derived factor 1 (SDF-1, CXCL12) is increased in subacromial bursitis and downregulated by steroid and nonsteroidal anti-inflammatory agents.Kim YS1, Bigliani LU, Fujisawa M, Murakami K, Chang SS, Lee HJ, Lee FY, Blaine TA.

Current Practice
Sub-acromial Steroid Injection
Usually 1
BOA/ BESS commissioning guide

Indications for Surgery
Failure of First line treatment
Symptoms lasting more than 6 months

Notable Exception
Acute Rotator Cuff Tears
Early surgery has better outcomes
Duncan NS, Booker SJ, Gooding BW, Geoghegan J, Wallace WA, Manning PA Surgery within 6 months of an acute rotator cuff tear significantly improves
outcome. J Shoulder Elbow Surg. 2015 Dec;24(12):1876-80.

Setup• Patient Position - Beach chair / lateral
• Arm holder - traction vs mechanical
• Kit- Coblation/ shaver/ pump

Portals


Outcomes
20 year follow up 80% satisfied- 14% revision
Arthroscopy. 2015 Oct 24. pii: S0749-8063(15)00704-5. doi: 10.1016/j.arthro.2015.08.026. [Epub ahead of print]
Patients With Impingement Syndrome With and Without Rotator Cuff
Tears Do Well 20 Years After Arthroscopic Subacromial Decompression. Jaeger M1, Berndt T2, Rühmann O2, Lerch S2.

Key Points
• Both Extrinsic and Intrinsic factors play a role
• Tendinopathy is degenerative not inflammatory
• ASD when first line treatment fails
• Reliable outcomes in carefully selected patients

Comments and questions?