readiness for organizational change: a longitudinal study ...€¦ · depression would reduce...
TRANSCRIPT

377
Journal of Occupational and Organizational Psychology (2002). 75, 377-392
© 2002 The British Psychological Society
www.bps.org.uk
Readiness for organizational change:A longitudinal study of workplace, psychologicaland behavioural correlates
Charles E. Cunningham'*, Christel A. Woodward^,Harry S. Shannon^, John Macintosh', Bonnie Lendrum',David Rosenbloom' and Judy Brown^'Hamilton Health Sciences and McMaster University, Hamilton, Ontario, Canada^McMaster University, Hamilton, Ontario, Canada
To examine factors influencing readiness for healthcare organizational change, 654randomly selected hospital staff completed questionnaires measuring the logisticaland occupational risks of change, ability to cope with change and to solve job-related problems, social support, measures of Karasek's (1979) active vs. passive jobconstruct (job demand x decision latitude) and readiness for organizational change.Workers in active jobs (Karasek, 1979) v/hich afforded higher decision latitude andcontrol over challenging tasks reported a higher readiness for organizational changescores. Workers with an active approach to job problem-solving with higher jobchange self-efficacy scores reported a higher readiness for change. In hierarchicalregression analyses, active jobs, an active job problem-solving style and job-changeself-efficacy contributed independently to the prediction of readiness for organiz-ational change. Time I readiness for organizational change scores and an activeapproach to job problem-solving were the best predictors of participation inredesign activities during a year-long re-engineering programme.
Healthcare organizations are undergoing unprecedented changes (Shortell, Gillies,Anderson, Erickson, & Mitchell, 1996). (Competition, funding reductions, efforts toimprove cost-efficiency, mergers and the re-engineering of work processes are placingenormous demands on healthcare organizations and their employees (Woodwardet al., 1999). Research on individual differences in readiness for organizationalchange, workplace processes that facilitate change and factors that influence theimpact of organizational change on the health and emotional well-being of employeesIs important to the success of efforts to improve the health service delivery system.
Readiness for change research suggests that a demonstrable need for change, a senseof one s ability to successfully accomplish change (self-efficacy) and an opportunity toparticipate in the change process contribute to readiness for organizational change(Armenakis, Harris, & Mossholder, 1993). Readiness for change models havebeen applied widely in the organizational and behavioural sciences. Prochaska and
^Requests for reprints should be addressed to Charles E. Cunningham, Department of Psychiatry and BehaviouralNeurosdences. Faculty of Health Sciences. McMaster University, 1200 Main Street, Homiltor], Ontario, L8N 3Z5. Canada(e-mail: [email protected]).

378 Charles E. Cunningham et al.
colleagues, for example, found that readiness for individual change proceeded throughstages (Prochaska et al., 1994; Prochaska, Redding, & Evers, 1997) beginning at theprecontemplative stage, where the need for change is not acknowledged. At thecontemplative stage, individuals consider but do not initiate change. As a preparatorystage is reached, planning for change occurs (Prochaska etal., 1994, 1997). Individualsengaged in the process of behavioural change are at the action stage, whereas thoseattempting to sustain changes are at the maintenance stage. Movement throughthese stages is governed by decisional balance, the anticipated risks of change vs. thepotential benefits of change.
This study applied an individual readiness for change model to a longitudinal studyof organizational re-engineering in healthcare settings. We developed a brief measureof individual readiness for organizational change based on Prochaska et a/.'s (1994)questionnaires and tested several assumptions of individual and organizationalreadiness for change models.
Benefits vs. risks of organizational changeReadiness for change begins with an individual's perception of the benefits of change(Prochaska et al., 1994), the risks of failing to change (Armenakis et al., 1993; Beer,1980; B. A. Spector, 1989), or the demands of externally imposed changes (Pettigrew,1987). We hypothesized, therefore, that workers' perceptions of opportunities forimprovement in staff competence, service quality, quality improvement programme ororganizational staff relationships would contribute to readiness for change scores.
Readiness for change research suggests that staff perceptions regarding the risks ofre-engineering should also influence readiness for organizational change (Prochaskaet al., 1994). Employees in healthcare organizations facing re-engineering are con-fronted with at least three types of risks. First, because organizational re-engineeringposes a threat of job change or loss, we postulated that perceptions of occupationalinsecurity would lower readiness for organizational change scores and limit partici-pation in re-engineering activities. Second, the logistical burden of re-engineeringrepresents a risk that may shift decisional balance and reduce readiness for organiz-ational change (Prochaska et al., 1997). In a healthcare work force composed largely ofwomen, the domestic responsibilities assumed by many employees might increase thelogistical demands of organizational re-engineering (Hall, 1989, 1992). Shift workmight contribute to an already difficult logistical burden. We predicted, therefore, thatchild care, household tasks, shift work and a perception of conflict between domesticand occupational responsibilities would reduce readiness for organizational changeand limit participation in re-engineering. Third, because organizational changerepresents a considerable source of stress (Eerrie, Shipley, Marmot, Stansfeld, & Smith,1995; Woodard et al., 1999), re-engineering may pose special risks lor employeesexperiencing psychological distress. We hypothesized that emotional exhaustion anddepression would reduce readiness for organizational change and participation inredesign activities.
Individual contributors to readiness for organizational changeSelf-efficacy, the perceived ability to manage change successfully, exerts a mediatingeffect on readiness for individual (Prochaska et al., 1997) and organizational change(Armenakis et al., 1993; Pond, Armenakis, & Green, 1984). Workers with confi-dence in their ability to cope with change should be more likely to contribute to

Readiness for organizational change 379
organizational redesign. In contrast, workers may resist cbanges that they believeexceed their coping capabilities (Armenakis et al., 1993; Bandum, 1982). We pre-dicted, therefore, tbat staff who were cotifidetit in their ability to cope with job changeand who adopted ati active approach to job problem-solvitig would bave a higherreadiness for cbatige scores and participate in a greater number of organizationalredesign activities.
Workplace contributors to readiness for organizational changeFinally, we a.ssumed that individual readiness for cbange would be influenced bybroader organizational factors. Jobs wbich empower (Spreitzer, 1995) employees withthe skills, attitudes and opportunities to manage change should increase work-relatedself-efficacy (Conger & Kanungo, 1988) and readiness for organizational change(Armenakis et al., 1993; Neuman, 1989). Karasek (1979) described active jobs aspsycbologically demanding positions affording bigh decision latitude. Jobs with lowdemands and low decision latitude were defined as passive (Karasek, 1979)- Activejobs increase learning opportunities and contribute to desirable stress, whicb increasesmotivation and tbe development of new bebaviour patterns (Tbeorell & Karasek,1996). Active jobs provide opportunities for enactive mastery and incremental prep-anition for larger-scale organizational cbange (Armenakis et al., 1993). Workers inactive jobs should be more confident in their ability to manage cbange (Spreitzer,1995) and better prepared to participate in organizational redesign (Armenakis et al..,1993; Beer & Walton, 1987; Neuman, 1989). Passive jobs, wliicb limit opportunities fordecision-making and control, may compound tbe anticipated occupational risks oforganizational re-engineering, lower self-efficacy and limit readiness for change. A thirdfactor, .social support (Johnson, 1991; Karasek, Triantis, & C haudhry, 1982; LaRocco,House, & French, 1980; Stansfeld, North, White, & Marmot, 1995) appears to interactwitb active jobs to predict workplace adjustment. We predicted, therefore, thathigher scores on both Karasek and Tbeorell's (1990) active vs. passive job dimensionand social support would be associated witb readiness for organizatiotial cbange andstibsequent participation in a year-long hospital re-engineering programtne.
Method
ParticipantsA sample ot 880 staff, =21% of the employees at a large Canadian teaching hospital, wasrandomly selected from tbe organization s human resources files. Participants weredrawn from a wide range of job descriptions (e.g. nurses, pbysiotherapists, housekeep-ing) at two former general hospital sites wbich eacb possessed a ntimber of units (acbildren s bospital, a cbildren's outpatient developmental and mental bealth centre,a rehabilitation hospital and a chrotiic care setting).
ProceduresBaseline surveys were sent to staff selected for tbe study after the intent to re-engineerwas amioimced, but several months before redesign planning began. Staff wereitiformed tbat the purpose of the stirvey was to understand bow workplace cbangesaffect both employees and services. Staff returned questionnaires to a universityresearch unit witb assurance tbat data would remain confidential, and tbe hospitaladmitiistnition would not have access to individual scores. Following baseline sitrveys,

380 Charles E. Cunningham et al.
an extensive programme of organizational re-engineering began. Design teams workedfor a year to achieve cost reductions and service improvements by introducing pro-gramme management, designing evidenced-based clinical pathways, redistributingtasks (multiskilling) and reducing staff. Staff were informed by regular newsletters andtown hall discussions and encouraged to pose questions, make suggestions or offerfeedback anonymously. Staff were given opportunities to participate in a wide range ofredesign activities and provided with transitional workshops and supports (e.g. resumepreparation, interview training, computer skills and career planning). At Time 2, oneyear following the completion of the first survey, the same cohort of employees wassent a second survey.
Measures
Measures of the risks ofchatigeFamily demographics. Participants completed questions regarding marital status, numberof chiitlren, time devoted to child care, care of extended family members and familyincome.
job insecurity. A 6-item 5-point (strongly disagree to strongly agree} scale (alpha=.65)measured job insecurity (Greenhalgh & Rosenhlatt. 1984).
job ir)terference. A 3-item 3-point (not at all to a great deal) scale (alpha=.64) fromthe Whitehall studies measured the adverse effects of one's job on family life (Northetal., 1993).
tAeasures of self-efficacy
jotxhange seif-efficacy. Confidence in one's ability to cope with job change, the transfer-ability of joh skills, and joh prospects were measured with a new 5-item 5-point(strongly disagree to strongly agree) seale (alpha= .71).
Active approach to job problem-soiving. This 5-item 5-point (never to almost all the time)scale, which measured an active approach to the solution of work-relatedprohlems (alpha=.75), was adapted from Israel, Schurman, and House (1986).
Aleasures of joh characteristics
job demands. A 6-point 5-item (strongly disagree to strongly agree) variation ofthe original 4-point scale (Karasek, 1985) measured psychological and physical jobdemands (alpha = .69).
Decision latitude. A 9-item 5-point (strongly disagree to strongly agree) variation of theoriginal 4-point scale (Karasek, 1985) composed of skill discretion (the breadth of skillsworkers could use) and decision-making authority measured decision latitude(alphas.60).
Active vs. passive job. Karasek's (1979) active joh construct was computed hy multiplyingdecision latitude by job-demand scores.
Social support. A 10-item 5-point (strongly disagree to strongly agree) scale(alpha=.86) composed of three supervisor support and seven colleague support

Readiness for organizational change 381
questions was adapted from Karasek's Job Content Questionnaire (four new and sixadapted questions).
Organizationlstaff relations. This 5-item 5-point (poor to excellent) scale (alpha=.79) wasadapted from the Hospital Corporation of America's staff judgments of hospitalsquestionnaire (Hays, 1994). For example, staff rated 'The way this hospital treats itsemployees'.
Service qualityQuality of patient core. A l6-item 5-point (poor to excellent or don't know) scale(alphas .93) was adapted from the Hospital Corporation of America's quality of patientcare measures (Hays, 1994). For example, staff rated the 'current quality of careprovided'.
Staff competence. This 9-item 5-point (poor to excellent or don't know) scale(alpha=.94) included items from the Hospital Corporation of America's measures(Hays, 1994). For example, staff rated the extent courtesy and respect are shownpatients by staff.
Attention to quality improvemer^t This measure was a 5-item, 5-point (poor to excellent todon't know) scale based on the Hospital Corporation of America's questionnaire(Hays, 1994) plus additional items examining staff perceptions of the hospital's com-mitment to quality improvement (alpha=.88). For example, staff rated the emphasisplaced on evidence to guide improvement of quality in eare and services'.
Psychological measuresReadiness for organizational change. A 6-item 5-point (strongly disagree to strongly agree)readiness for change scale (alpha=.63) was modelled after the measuresdeveloped by Prochaska and colleagues (1994), with questions reflecting theprecontemplative, contemplative, preparatory, action and maintenance stages of themodel (Prochaska et al., 1994). Scoring for items at the precontemplative stage (e.g.programme does not need changing) were reversed to yield a continuous scale, withhigher scores reflecting increased readiness.
Planned health and lifestyle changes. Staff checked lifestyle-change options from a list of 15Ontario Health Survey items (Ontario Ministry of Health, 1992).
Emotional exhaustion. Staff completed the 7-item 6-point (never to every day) EmotionalExhaustion seale (alpha= .91) from the Maslaeh Burnout Inventory (Maslach & Jackson,1981).
Depression. Symptoms of depression ^vere measured with a 10-item 4-point (rarely ornone of tbe time to mostly all of tbe time) scale (alpha=.78) version of the Centre forthe Epidemiological Study of Depression scale (CESD) (Radloff, 1977; Reis & Herz,1986).
Contributions to re-engineeringParticipation in re-engineering. At Time 2, one year after the start of redesign, staffrecorded which of seven possible re-engineering activities (e.g. submitting designideas, volunteering for design teams, joining design teams, participating in redesign

2.9
3.5
3.5
3.5
1.0
1.0
I.I
1.2
382 Charles £ Cunningham et al.
Table I . Mean and standard deviations for readiness for organizational change questions"
Stage of changeContent of question Mean SD
Precontemplative stageThe programme or area in which I work functions well and does not have any
aspects which need changingThere's nothing that I really need to change about the way I do my job to be
more efficientContemplative stageI've been thinking that I migbt want to help change something about the
programme or area in which I workPreparatory stageI plan to be involved in changing the programme or area in which I workAction^ tageI am working hard to help improve aspects of the programme or area in which I
work 3.7 I.IMaint^ance stageWe are trying to make sure we keep changes/improvements my programme/area
has made 3.5 .9
"Scale range I (strongly disagree) to 5 {strongly agree).
work groups, etc.) they participated in during the year following Time 1 assessments.At Time 2, staff rated their contribution to the re-engineering process on a 5-point scale(not at all to very much).
ResultsThis analysis begins by examining the workplace, psychological and domesticcorrelates of baseline readiness for org:mizational change. Hierarchical regressionequations (Tabachnik & Fidel, 1996) were computed to model the contribution ol theanticipated risks of change, job change sef-efficacy, an active approach to job-relatedproblem-solving and Karasek's (1979) model of an active job to readiness for organiz-ational change. A final regre.ssion equation examined the predictors of participation ina year-long programme of organizational re-engineering. Responses to the six items onthe readiness for organizational change measure are presented in Table 1.
Response rateOf the 65^ (74'X)) staff returning surveys, most were women (87%) mth communitycollege (44%) or university degrees (28%). Most participants were nonsupervisory(87%), nonunion (87%) staff, employed on hourly contracts (77%) with shift workrequirements (44%). A majority of participants were married or living with partners(76%) and had children in the home (71%). Although participants were employed anaverage of 35 h per week, a considerable amount of additional time was devoted tochild care (29 h) and household activities (14.7 h). Of the 834 employees eligible forparticipation at Time 2, 528 (63%) completed surveys.
Risks and benefits of organizational changeCorrelational analysis showed that domestic factors which might influence the logisti-cal burden of change, or limit participation in the redesign process, were not linked to

Readiness for organizational change 383
readiness for organizational change scores. With the exception of children under age 6in the home, whicb was related to lower participation (r=-.l6**) but not readiness(r=-.O7), gender (r=.O2, r=.O5), time devoted to child care (r=-.O3, r=-.O7),responsibility as the main family earner (r= - .08, r= - .04), household chores (r= - .08,r=-.O5), and marital status (r=.03. r=.O3) were not related to readiness for change orparticipation in redesign activities, respectively. Table 2 shows that staff with a higherreadiness for organizational change scores reported slightly more job interference withfamily life and higher emotional exhaustion scores. Shift work, which might limitparticipation in redesign activities, was associated with a slightly lower readiness fororganizational change scores (r=-.15**) and less participation in redesign activities(r=-.25**). Job insecurity (Table 2) was not linked to readiness for organizationalchange or participation in redesign activities.
The correlation analysis showed that readiness for organizational change scoreswere not linked to potential benefits of change. Staff perceptions of the quality ofpatient care (r=-.O4, r=-.O4), statT competence ir=-.O6, r=-,09), quality improve-ment programmes (r=.OO, r=-.O7), or staff-organizational relations (r=.O8, r=.O4)were not linked to readiness for organizational change or participation in redesignactivities, respectively.
Individual correlates of readiness for organizational changeAs predicted, Table 2 shows that workers with an active approach to job relatedproblem-solving and higher job-change self-eftlcacy at Time 1 reported a higher readi-ness for change scores, participated in a greater number of redesign activities duringthe following year, and reported making a greater contribution to organizationalchange.
Workplace contributors to readiness for organizational changeTable 2 shows that staff in active jobs (e.g. high decision latitude x high job demands)reported a higher readiness for organizational change scores, participated in a greaternumber of redesign activities, and felt they made a greater contribution to organiz-ational change than those in passive jobs. Although social support was only weaklyrelated to readiness for organizational change and was not related to participation inredesign activities, it was associated with lower emotional exhaustion scores.
As a measure of discriminant validity, we detemiined whether readiness for organiz-ational change was specific to the workplace or reflective of a more generalizedreadiness for personal change. Readiness for change was not linked to plans to engagein health-related personal lifestyle changes (r=.()6).
As shown in Table 2, staff with a higher readiness for organizational change scores atTime 1 participated in a greater number of redesign activities during a year-longre-engineering programme and reported making a greater contribution to organiz-ational change at Time 2.
Predicting readiness for organizational changeA hierarchical regression equation (Tabachnik & Fidell, 1996) tested the predictions ofindividual (Prochaska et al., 1994, 1997) and organizational readiness for changemodels (Armenakis et al., 1993). Prochaska s model suggests that readiness reflects abalance between the risks and benefits of change. After controlling for hospital site onstep 1, step 2 entered occupational and logistical risks of change: shift work, job

384 Charles E. Cunningham et ai
oU
re
- r — —
I I
t Io o —
* 4.ro O (N— _ O
o o 00 LTl
00
•o
r-..
1= u H ---
a. U
5 "
O Q < i/i
o
Readiness for organizational charige 385
Table 3. Sequential regression equation predicting readiness for organizational change scores
(N=62S)
Measure
Step 1: Control variableSite
Step 2: Occupational risksShift workJob interferes with familyJob insecurities
Step 3: Psychological risksEmotional exhaustionDepression
Step 4: Self-efficacyJob change self-efficacyActive job problem-solving approach
Step 5: Karsek's active jobActive vs. passive job
Multr
.12
11
.31
.48
.54
Mult r
.02
.07
.10
.23
.29
2 change
.02
.06
.02
.13
.07
Beta''
.06
- . 1 1.11.12
.03- . 1 0
.14
.26
.29
t
1.83
-3 .15* *2.36*2.81**
.60- 2 . 5 1 * *
3.20***7.03***
7 55***
"Standardized beta from final step of the regression equation.
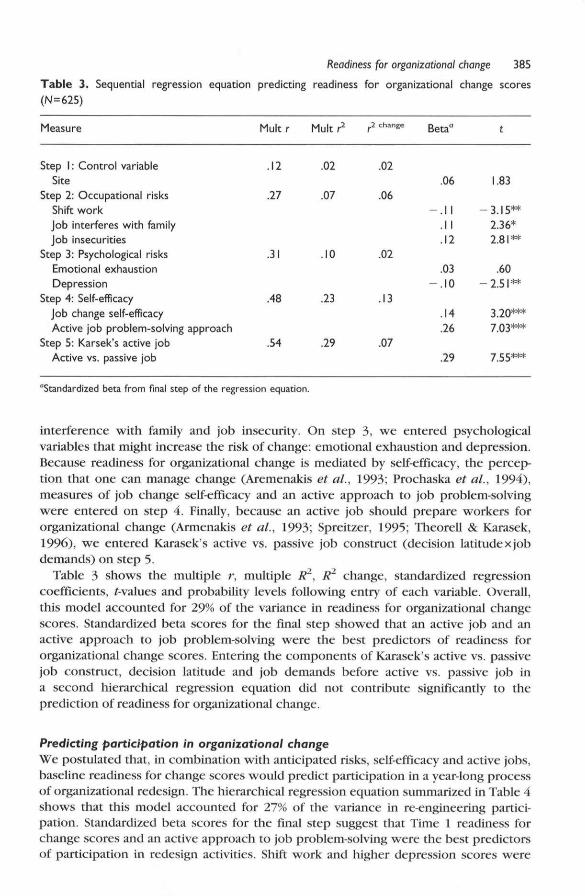
interference with family and job insecurity'. On step 3, ^ve entered psychologicalvariables that might increase the risk of change: emotional exhaustion and depression.Because readiness for organizational change is mediated by self-efficacy, the percep-tion that one can manage change (Aremenakis et al., 1993; Prochaska et al., 1994),measures of job change self-efficacy and an active approach to job problem-solvingwere entered on step 4. Finally, because an active job should prepare workers fororganizational change (Armenakis et al., 1993; Spreitzer, 1995; Theorell & Karasek,1996), we entered Karasek's active vs. passive job construct (decision latitudexjobdemands) on step 5.
Table 3 shows the multiple r, multiple R^, R^ change, standardized regressioncoefficients, f-values and probability levels following entry of each variable. Overall,this model accounted for 29% of the variance in readiness for organizational changescores. Standardized beta scores for the final step showed that an active job and anactive approach to job problem-solving were tbe best predictors of readiness fororganizational change scores. Entering the components of Karasek's active vs. passivejob construct, decision latitude and job demands before active vs. passive job ina second hierarchical regression equation did not contribute significantly to theprediction of readiness for organizational change.
Predicting participation in organizational changeWe postulated that, in combination with anticipated risks, self-efficacy and active jobs,baseline readiness for change scores would predict participation in a year-long processof organizational redesign. The hierarchical regression equation summarized in Table 4shows that this model accounted for 27% of the variance in re-engineering partici-pation. Standardized beta scores for the final step suggest that Time I readiness forchange scores and an active approach to job problem-solving were the best predictorsof participation in redesign activities. Shift work and higher depression scores were

386 Charles E. Cunningham et al.
Table 4. Hierarchical regression equation; Time I variables predicting Time 2 participation in
redesign activities (N=450)
Measure
Step 1: Control variableSite
Step 2: Occupational risksShift v^orkJob interferes with familyJob insecurity
Step 3: Psychological risksEmotional exhaustionDepression
Step 4: Self-efficacyJob change self-efficacyActive job problem-solving approach
Step 5: Karsek's active jobActive vs. passive job
Step 6: Readiness for changeTime 1 readiness for organizational change
Multr
.10
.31
.35
.47
.48
.52
Mult r
.01
.10
.12
.22
.23
.27
J change
.01
.09
.03
.10
.01
.04
Beta"
.06
- . 2 0.11.05
.08- . 11
- . 0 1
.23
.03
.24
t
1.32
_ 4^9*^M<
2.02 *
.90
1.24- 2.29*
- . 1 34.95***
.61
4.88***
"Standardized beta from final step of the regression equation.
associated with lower participation in redesign activities. Entering the compotients ofKaraseks active vs. passive job construct, decision latitude and job demands beforeactive vs. passive job in a second hierarchical regression equation did not contributesignificantly to the prediction of participation in redesign activities.
lo determine whether participation was a function of the opportunities afforded bysupervisory status, we computed the same sequential regression equation in asubsaniple of 274 nonsupervisor>' health professit)nals (Table 5). This model, again,accounted for 27% of the variance in participation in redesign activities. Significantbeta scores for the final step suggest that a higher readiness for change scores, anactive approach to job problem-solving and site were the best predictors of partici-pation in redesign activities. Shift work was, again, associated with less involvement inredesign activities.
Discussion
Organizational contributors to readiness for organizational changeReadiness for change was best predicted by combining organizational (Armenakisetal., 1993) and individual models (Prochaska etal., 1994, 1997). Work variables werethe best predictors of readiness for organizational change. Employees in active pos-itions witb more control over challenging jobs reported a higher readiness for organiz-ational change sct)res dmi were mt)re likely to participate in organizational redesign.This is consistent with research suggesting that active jobs foster personal empower-ment, improve performance, increase initiative and contribute to organizationalinnovation (Conger & Kasungo, 1988; Spreitzer, 1995; fheorell & Karasek, 1996).

Readiness for organizational change 387
Table 5. Sequential regression equation of baseline measures predicting participation in organiz-
ational re-engineering during the next year
Measure
Step I: Occupatfonal risksJob insecurity
Step 2: Logistical risksShift v/orkJob interferes with family
Step 3: Psychological risksWork stressEmotional exhaustionDepression
Step 4: Self-efficacyJob change self-efficacyJob problem-solving
Step 5: Active jobStep 6: Readiness for change
Multr
.030
.292
.353
.469
.491
.522
Multr*
.001
.085
.124
.220
.241
.272
Beta"
.060
- .184.096
- .038.052
- .112
- .016.205.307.215
t
I.I
-4.211.80
- . 7 5.83
-2 .29
- . 2 94.337.84.35
P
.272
.012
.073
.453
.408
.022
<.OOI<.OOI<.OOI<.OOI
"Standardized beta from final step of the regression equacion.
The dynamic demand-control hypothesis suggests that active jobs contribute to asense of mastery (Theorell & Karasek, 1996). In the present study, positive correlationsamong active jobs, an active approach to job problem-solving and bigber job cbangeself-efficacy are consistent with these predictions. Theorell and Karasek (1996) alsosuggested that the sense of mastery created by active jobs inhibits the perception ofstress or engenders positive stress (Theorell & Karasek, 1996). Active jobs, however,were associated with greater interference with family and higher emotional exhaustionscores. This observation questions the assumption that active jobs contribute to a stateof positive stress.
Previous studies have linked workplace social support to employee adjustmentOohnson, 1991; Karasek et al., 1982; LaRocco et al., 1980; Stansfeld et al, 1995). Inthis study, job-related interpersonal relationships made a very limited contribution tothe prediction of readiness for organizational change scores. A socially supportiveworkplace, however, was correlated with lower emotional exhaustion scores. Thesefindings suggest that supportive colleagues may play a more important role inemployee efforts to cope with the stress of organizational change (Woodward et al.,1999).
Decisional balance: Risks and benefits of changeReadiness for change models suggest that evidence of a need for change, a discrepancybetween present conditions and a targeted organizational objective, are important tothe creation of readiness for organizational change (Armenakis et al., 1993; Beer, 1980;B. A. Spector, 1989). As in many healthcare redesign initiatives (Ho, C:han, & Kidwell,1999), the need to change was imposed by funding reductions. In this study,staff judgments of the quality of the care and services provided by the organizationwere not linked to readiness for change scores. When imposed change representsoccupational, logistical and psychological risks to employees, and is not linked to a
388 Charles £, Cunningham et al.
perceived need for quality improvements, the success of these changes may becompromised (Armenakis et al., 1993; Ho et al., 1999; B. A, Spector, 1989),
Decisional balance models suggest that individuals prepare for action when theperceived benefits of change outweigli the anticipated risks of change (Prochaskaet al., 1994). Our results provide limited support for this model. Thus, shift work,which poses logistical risks to employees considering participation in organizationalredesign, was linked to a lower readiness for organization;il change scores and lessparticipation in re-engineering activities.
Most of the employees studied bere were women. The child care and householdresponsibilities which employed women assume may prolong job-related physiologicalarousal, intensify work overload and role conflict, and increase vulnerability toworkplace stress (Burke, 1993; Eckcnrode & Gore, 1990; Hall, 1989, 1992; Keita &Jones, 1990). In this study, the perception th;it work interferes with family life wasstrongly linked to emotional exliaustion and depression scores. Staff reporting a higherreadiness lor change scores and participating iii a greater number or redesign activitiesreported a slightly greater interference with their family and somewhat higheremotional exhaustion scores. Nonetheless, children in the home under age 6 wasthe only domestic responsibility measure linked to lower participation in redesignactivities.
Organizational redesign is a stressful experience for many staif (Woodw:ird et al.,1999). Nonetheless, psychological factors, which might increase the personal risks ofrapid organizational change, did not reduce readiness for change. As noted above,workers with a higher readiness for change scores reported slightly higher emotionalexhaustion scores. This is consistent with studies finding that organizational stressorsmay prompt innovation and a coping response (Bunce & West, 1994). Finally, contraryto the predictions of decisional balance models, a key work-related measure of risk, jobinsecurity, was not related to readiness for organizational change or participation inredesign activities.
Individual correlates of readiness for organizational changeSelf efficacy, the perceived ability to cope with change, is thought to be an importantcontributor to readiness (Armenakis et al., 1993; Pond et al., 1984; Prochaska et al.,1994), In this study, workers with an active approach to work problems, who weremore confident in their ability to cope with job change, reported a higher readiness fororganizational change scores at Time 1, participated in a greater number of redesignactivities during the following year, and felt that they made a greater contribution toorganizational change at Time 2, These data are consistent with studies on personalhardiness suggesting that a similar constellation of psychological characteristics isassociated with favourable responses to stressful events (Kobasa, Maddi, Fucetti, &Zola, 1985; Kobasa &Pucetti, 1983; Westman, 1990).
Measuring readiness far organizational changeIn tliis study, statf with higher readiness scores participated in more re-engineeringactivities and felt that they made a greater contribution to the organization s redesignefforts. The data support the predictive validity of this measure. The independentcontribution of readiness for change scores to the predication of participation providesiurther support for this measure's predictive validity.

Readiness for organizational change 389
The finding that readiness for organizational change scores were not related to theplanning of personal health behaviour changes supports the discriminant validity ofthis measure. Readiness for organizational change scores did not reflect a generalpropensity to personal change.
Limitations
Although a single corporate sampling frame may have limited the generalizabilityof these findings, participants were selected from different occupational groupings,inpatient and outpatient settings, and geographical locations. Participants worked inprogrammes serving children and adults with a wide range of acute and chronic healthproblems at sites with different funding bases, histories and ctiltures.
In addition, estimates of decision latitude, social support and individual readiness fororganizational change were based on employee reports. Although subject to informantbiases, perceptions of workplace eharaeteristics have been linked to more objectiveanalyses (P. Spector, Dwyer, & Jex, 1988). Moreover, physiological responses aremediated by the interaction of perceptions of workplace characteristics (e.g. jobcontrol) and more objective measures (Fox, Dwyer, & Ganster, 1993; Stansfeld et al.,1995).
Implications
This study has several implications for healthcare organizations facing change. First,active jobs that afford control over challenging tasks, conditions which optimize healthand emotional well-being (Blegen, 1993; Greenberger, Strasser, Cummings, & Dunham,1989; Karasek & Theorell, 1990; Landsbergis, 1988; Tetrick & LaRoeco, 1987; Tbeorell& Karasek, 1996), prepare workers to initiate or contribute to organizational change.
Second, encouraging an active approach to job problem-solving, building thestrategies needed to manage change suceessfully and enhancing job ehange self-effieacy (Armenakis et «/., 1993) should contribute independently to the preparatorybenefits of an active job.
Third, workers in demanding jobs reported a higher emotional exhaustion. Longi-tudinal studies suggest that organizational re-engineering increases emotional exliaus-tion (Woodward et al., 1999), wbich may adversely effect work performance (Wright& Bonett, 1997) and lower patient satisfaction (Leiter, Harvie, & Frizzell, 1998). If thestrain of rapid organizational change is not modulated, the contribtitions of employees,and the ultimate impact of redesign on patient care, may be compromised. Buildingsupportive relationships with co-workers and supervisors and limiting confiietbetween work and home life might modulate the stress of organizational change.
Stage models suggest that workers at the precontemplative or contemplative stageswould respond to different interventions to those at the preparatory or action stages(Prochaska et al., 1994, 1997). Studies linking organizational functioning to work-group readiness for ehange suggest that employees in the same work group would beat similar stages (Fox, Ellison, & Keith, 1988). The types of brief measures used heremay help identify workgroup readiness levels and design preparatory interventionsaddressing the needs of employees at different stages of the change process.
Stage models suggest a dynamic process of individual and organizational change(Prochaska et al., 1994, 1997) in which a shift in the perceived risks and benefits ofchange may prompt return to an earlier phase. This study suggests that active involve-ment in organizational ehange, reducing barriers to participation (e.g. shift work).

390 Charles E. Cunningham et al.
building problem-solving strategies and enhancing workers" perceptions of theirability to cope witb change (change sclf-efficacy) should botb enhance commitment toredesign and reduce the stress of organizational change.
Acknowledgements
This research was supported by Haniiltoti (Icalth Sciences and the Social Sciences andHumanities Research Foundation during the collection of this data. Preparation of thismanuscript was supported by a Senior Research Fellowship to the first author from the OntarioMental Health Foundation and the John C. Laidlaw Chair in Patient Centred Health Care.Deborah Fitzpatrick provided helpful comments during the preparation of the manuscript.
References
Armenakis. A, A,, Harris, S, G.. & Mossholder, K. W, (1993). Creating readiness for organizationalchange. Human Relations, 46, 681-703.
Ilandura, A, A, (i982), Selt-efficacy mechanism in human agency, American Ps}>chologist, 37,122-147,
Beer, M. (t980). Organization change and dei'elopment: A systems vieu: Santa Monica, CA:Goodyear,
lleer, M,, & Walton, A. E, (1987). Organization change and development. Annual Review ofPsychology, 38, 339-367.
Blegen. M. A. (1993), Nurses' job satisfaction: A meta-analysis of related variables. NursingResearch. 42, 36-41,
Bunce, I),, & West, M, (1994), c:hanging work environments: Intiovative coping responses tooccupational stress. Work and Stress, 8, 319-331.
Burke, R. J. (1993). Organizational-level interventions to reduee occupational stre.ssors. Workand Stress, 7, 77-87.
Conger, J. A., & Kaniingo, R. N. (1988), The empowerment process: integrating theory andpntctice. Academy of Management Review, 13, 471-482,
Eckenrode, .)., & Gore, S, (1990). Stress and coping at the boundary' of work, aiid family. InJ. Eekenrode & S. Gore (Eds,), Stress between ivork and family (pp. l-l6). New York:Plenum Press.
Ferrie.J. E., Shipley, M. J., Marmot, M. G., Stansfeld, S., & Smith, G. D. (1995), Health effects ofanticipation of job change and non-employment: Longitudinal data from the Wbitehall IIstudy, British MedicalJtnirnal. 311, 1264-1269.
Fox, M, I.,, Dwyer, I). J,. & Clanster, D. C, (1993), Effects of stressful job demands and controlon physiological and attitudinal outcomes in a hospital setting. Academy of ManagementReview, 30, 289-318.
Fox, D. G., Ellison, R, L, & Keith, K, L. (1988). Human resource management: An index and itsrelationship to readiness for change. Public Personnel Management, 17, 297-302,
Cireenberger, D, B., Strasser, S., Cummings, L. S., & Dunham, R. (1989), The impact ol personalcontrol on pertbrmance and satisfaction. Organizational Behavior and Human DecisionProcesses, 43, 29-51.
Greenhalgh, L., & Rosenblau, Z. (19H4). Job insecuritj: Toward conceptual clarity. Academy ofManagement Review. 9. 438-448,
Hall. E. M, (1989), Gender, work control, and stress: A theoretical discussion and an empiricaltest. International Journal of Health Services. 19, 72S-74S,
Hall, E. M. (1992), Double exposure: The combined impact of tbe bome and work environmentson mental strain and physical illness. International Journal of Health Services, 22, 239-260.
Hays. R, D, (1994), Short from measures of physician and employee judgements about hospitalquality./omr Commission Journal of Quality Improvement, 20, i^(^-ll.

Readiness for organizational change 391
Ho, S, J., Chan, L,, & Kidwell, R, E, Jr. (1999). The improvement of business process reengineer-ing in American and Canadian hospitals. Health Care Management Review, 24, 19-31.
Israel, B. A.. Schurman, S, J,, & House, J. A, (1986). Stress and wellness project survey. AnnArbor, MI: University of Michigan, School of Public Health,
Johnson. J, V. (1991), Collective control: strategies for survival in the workplace, InJ, V. Johnson& G, Johansson (Eds,), The psychosociat work environment: Work organization, democra-tization, and health: Essays in memory of Berbil Gardell (pp, 121-132). Amityville, NY:Baywood.
Karasek, R. A, (1979), Job demands, job decision latitude, and mental strain: Implications for jobredesign. Administration Science Quarterly, 224, 285-307,
Karasek, R. A. (1985)- Job Content Instrument Questionnaire (Mimeograph). Lowell, MA:University of Massachusetts.
Karasek, R, A,, & Theorell, T. (1990), Healthy work—Stress, productivity, and thereconstruction of working life. New York: Basic Books,
Karasek, R, A,, Triantis, K. P,, & Chaudhry, S. S, (1982), Coworker and supervisor supportas moderators of associations between task characteristics and mental strain. Journal ofOccupational Behavior, J, 181-200,
Keita, G, P., & Jones, J, M, (1990). Reducing adverse reaction to stress in the workplace,American Psychologist, 45, 1137-1141.
Kobasa, S, C, Maddi, S, R.. Pucetti, M., & Zola. M, (1985). Effectiveness of hardiness, exercise,and social support as resources against illness. Journal of Psychosomatic Research, 29,525-533,
Kobasa. S. C, & Pucetti, M, C, (1983). Personality and social resources in stress resistance.Journal ojPersonality and Social Psychology, 45, 839-850.
LaRocco, J, M., House, J. S., & French, J, R, P, (1980). Social support, occupational stress, andhcdXth. Journal of Health and Social Behavior, 21, 202-216,
Leiter, M, P., Harvie, P,, & Erizzell, C, (1998). The correspondence of patient satisfaction andnurse humout. Social Science in Medicine, 47, 1611-1617,
Landsbergis, P, A. (1988). Occupational stress among health care workers: A test of the jobdemands-control model,/oMrn«/ of Organizational Behavior, 9, 217-239.
Maslach, C. & Jackson. S, E, (1981). Measurement of experienced burnout. Journal ofOccupational Behavior, 2, 99-113,
Neuman, J. E, (1989). Why people don't participate in organizational change. Research inOrganizational Change and Development, 3, 181-212.
North. E,, Syme, S, L, Eeeney, A., Head. J.. Shipley, M, J., & Marmot, M, G, (1993). Explainingsocioeconomic differences in sickness absence: The Wliitehall II study. British MedicalJournal, .iO6, 361-366,
Ontario Ministry' of Health (1992), Ontario Health Survey 1990: Users guide Vol. Idocumentation. Toronto: Premier s Council on Health Weil-Being and Social Justice.
Pettigrev , A. (1987). Context and action in transforming the Urm. Journal of ManagementStudies, 24, 649-670,
Pond, S. G,, Armenakis, A, A., & Green, S, B. (1984), The importance of employee expectation inorganizational diagnosis. The Journal of Applied Behavioral Science, 20, 167-180,
Prochaska, J. O., Redding. C, A,, & Evers, K. (1997), The transtheoretical model of change. InK. Glanz, E. M, Lewis & B. K. Rimer (Eds), Health behewior and health education: Theory,research, and practice (pp. 60-84), San Erancisco: Jossey-Bass,
Prochaska, J. O,, Velicer, W. E,. Rossi, J. S., Goldstein, M. G,. Marcus, B, H,, RaJiowski. W,, Eiore,C, Harlow, L. L., Redding. C. A,, Rosenbloom, D.. & Rossi, S. R. (1994). Stages of change anddecisional balance for 12 problem behaviors. Health Psychology, 13. 39-46,
Radloff, L. S, (1977), The CES-D scale: A self-report depression scale for research in the generalpopuldtkm. Applied Psychological Measurement, /, 385-401,
Reis, J., & Herz. E. J. (1986). Factorial and discriminant validity of the Center for EpidemiologiealStudies Depression (CES-D) scale. Journal of Clinical Psychology, 42, 28-33.

392 Charles £. Cunningham et al.
ShorteU, S. M., Gillies, R. R., Anderson, D. A., Erickson, K. M., & MitcheU,.|. B. (1996). Remakinghealth care in America. San Francisco: Jossey-Bass.
Spector, B. A. (1989). From bogged down to fired up: Inspiring organizational change. SloanManagement Review. Summer. 29-34.
Spector, P., Dwyer, D. J., & Jex, S. M. (1988). Relation of job strcssors to affective, healthand performance outcomes: A comparison of multiple data sources. Journal of AppliedPsychology, 7J, H-19.
Spreitzer, G. M. (1995). Psychological empowerment in the workplace: Dimensions,measurement, and validation. Academy of Management Journal, 38, 1442-1465.
Stansfeld. S. A., North, F. M., Whitye, I., & Marmot, M. G. (1995). Work characteristics andpsychiatric disorder in civil servants in lonilon. Journal of Upidemiology and CommunityHealth, 49, 48-53.
Tabachnik, B. d.. & Fidell, L. S. (1996). Using multivariate statistics Cird ed.). New York:HarperCollins.
Tetrick, L. E., & URocco, J. M. (1987). Understanding, prediction, and control as moderatorsof the relationships between perceived stress, satisfaction, and psychological well-being.Jourtial of Applied Psychology, 72, 538-543.
'flieorell, T., & Karasek, R. A. (1996). Current issues relating to psychosocial job strain andcardiovascular disease research. Journal of Occupationcd Health Psychology, 1, 9-26.
Westman, M. (1990). The relationship between stress and performance: Tlie moderating effectsof hardiness. Human Pcrfonnunce. , i 141-155.
Woodward, C. A., Shannon, H. S., Cunningliam, C. E., McIntosh,J. E., Lendrum, B., Rosenbloom,D., & Brown, J. (1999). The impact of re-engineering and other cost reduction strategies onthe st:tff oi a large teaching hospital: A longitudinal study. Medical Care, A7, 547-555.
Wright, T. A., & Bonett, D. G. (1997). The contribution of burnout to work performance.Journal of Organizational Behavior, 18, 491-500.
Received 13 March 2000; revised version received 19 April 2002
