realising the value stakeholder event -workshop: how does the system support
TRANSCRIPT
How does the system support communities/individuals and
how could it do it better?15th July 2015

One of the great strengths of this country is that we have an NHS that – at its best - is ‘of the people, by the people and for the people’. Yet sometimes the health service has been prone to operating a ‘factory’ model of care and repair, with limited engagement with the wider community, a shortsighted approach to partnerships, and under-developed advocacy and action on the broader influencers of health and wellbeing. As a result we have not fully harnessed the renewable energy represented by patients and communities’
NHS Five Year Forward View
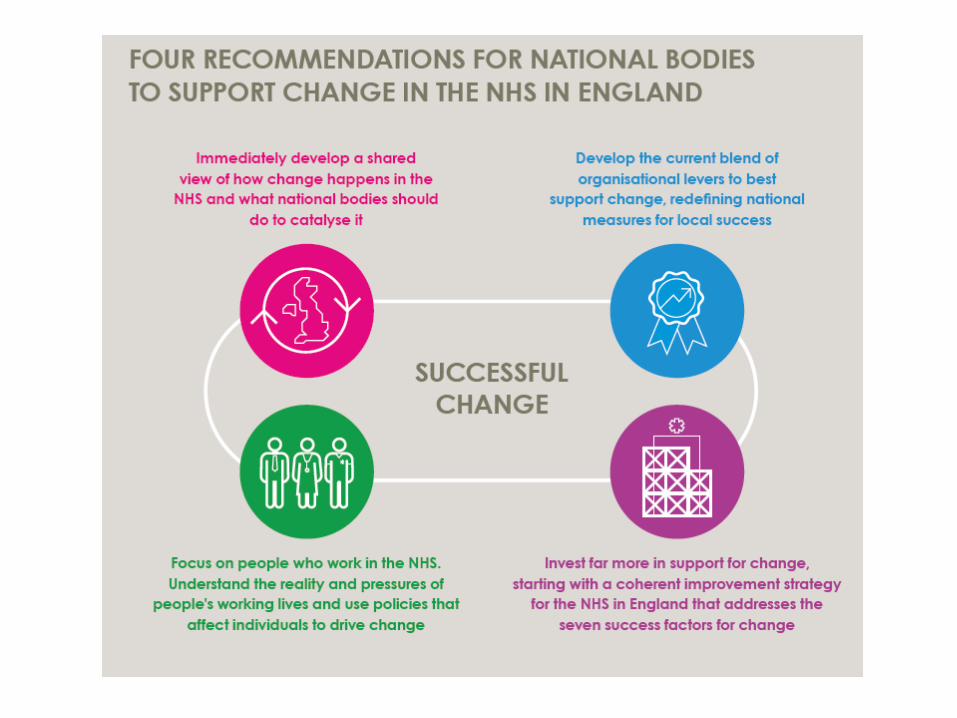
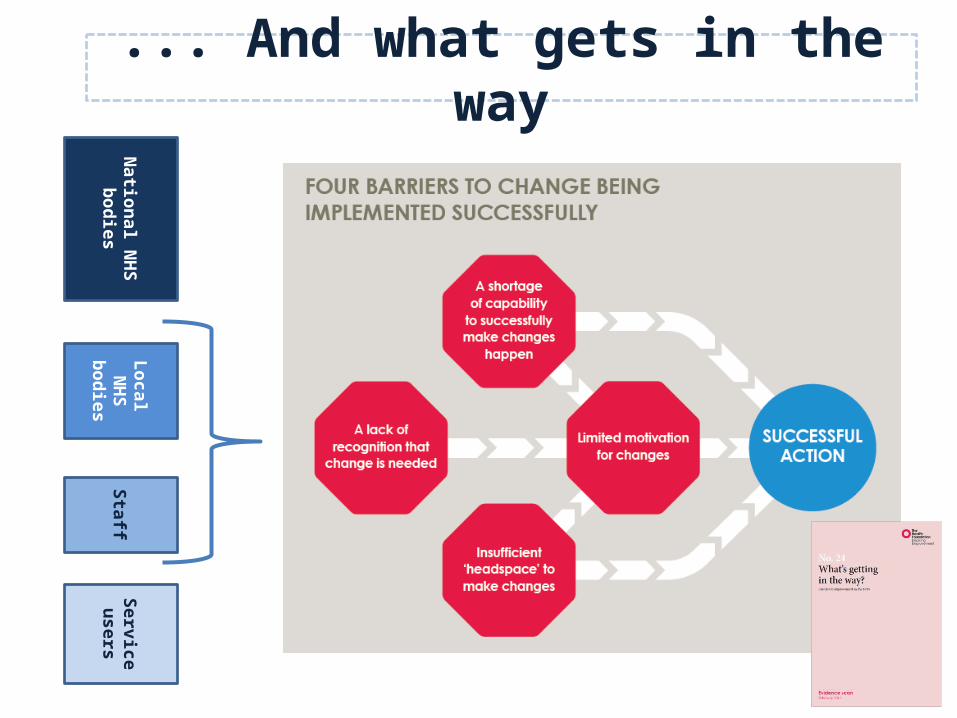
Levers and driversThe levers and drivers national bodies put in place can have a significant impact – either to support change to happen locally or to hinder/create barriers to change.
By understanding the enablers and barriers to local change that commissioners and providers face; combined with what we know from the evidence on what works; as well as our expertise in this area, we can then recommend the most impactful approaches for national bodies to take to help deliver the Five Year Forward View vision of truly person centred care delivered at scale.
National N
HS
bodiesLocal N
HS
bodiesStaff
Service users
Focus of Constructive Comfort
What is the optimum role for national policy, politics and the
‘system’ of NHS national bodies to support significant change (both
incremental and transformational) to ‘realise the value’?
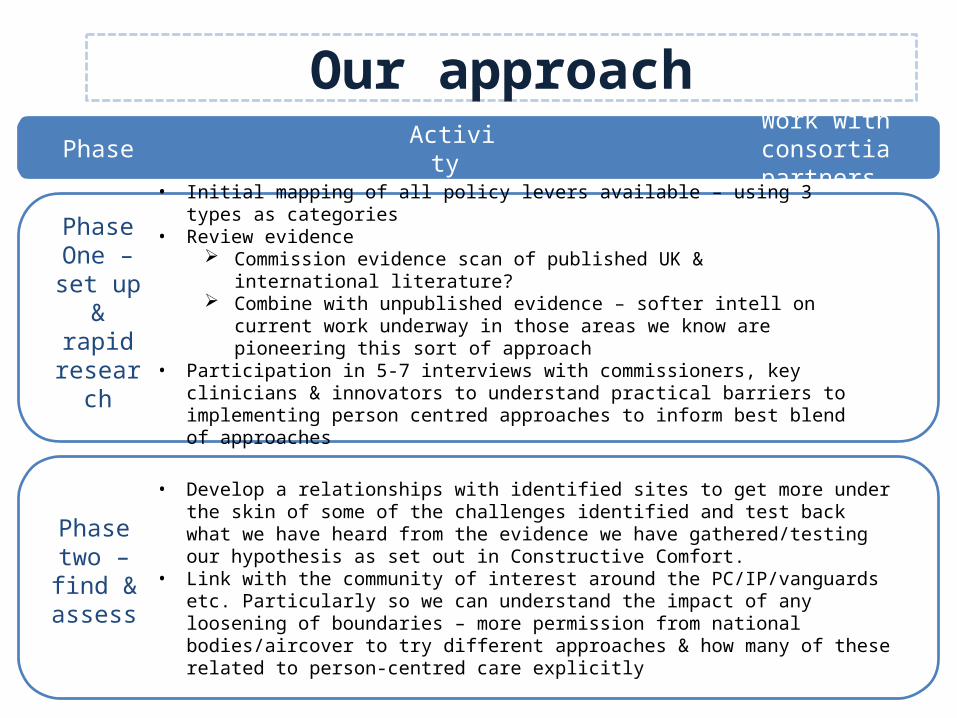
Our approach
Phase One – set
up & rapid
research
Phase two – find & assess
• Initial mapping of all policy levers available – using 3 types as categories• Review evidence
Commission evidence scan of published UK & international literature? Combine with unpublished evidence – softer intell on current work underway in
those areas we know are pioneering this sort of approach• Participation in 5-7 interviews with commissioners, key clinicians & innovators to
understand practical barriers to implementing person centred approaches to inform best blend of approaches
• Develop a relationships with identified sites to get more under the skin of some of the challenges identified and test back what we have heard from the evidence we have gathered/testing our hypothesis as set out in Constructive Comfort.
• Link with the community of interest around the PC/IP/vanguards etc. Particularly so we can understand the impact of any loosening of boundaries – more permission from national bodies/aircover to try different approaches & how many of these related to person-centred care explicitly
Phase Activity Work with consortia partners
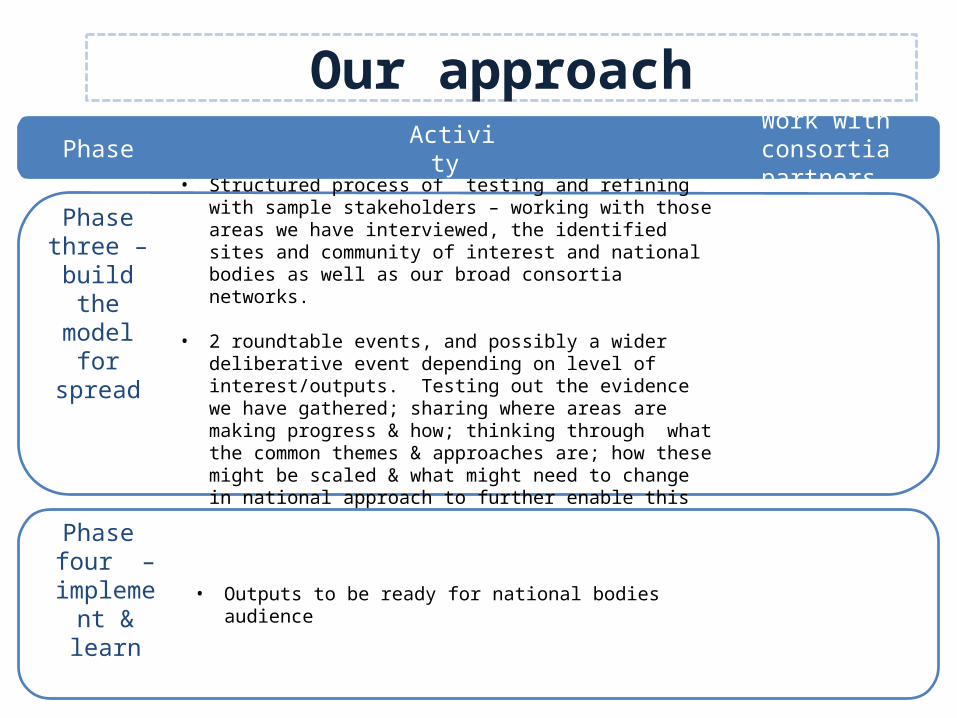
Our approach
Phase three – build the model for
spread
• Structured process of testing and refining with sample stakeholders – working with those areas we have interviewed, the identified sites and community of interest and national bodies as well as our broad consortia networks.
• 2 roundtable events, and possibly a wider deliberative event depending on level of interest/outputs. Testing out the evidence we have gathered; sharing where areas are making progress & how; thinking through what the common themes & approaches are; how these might be scaled & what might need to change in national approach to further enable this work to grow & flourish.
Phase four –
implement & learn
Phase Activity Work with consortia partners
• Outputs to be ready for national bodies audience

What will success look like?If we have been successful NHS England and other national bodies have a detailed understanding of:- the enablers and barriers that commissioners and providers encounter
when trying to implement such approaches;
- the evidence base around what levers and incentives do and do not work in seeking to effect change in person-centred care
how they might use the wide range of levers that national players have available to them & the best blend of approaches at their disposal to help tackle those barriers and enable/encourage people to take an active role in their own health and care and to engage better with their communities.
- and how you would most effectively measure impact.
What are the barriers to empowering patients and engaging communities?
Why does the obstacle exist?
Who is responsible for the obstacle?
Thinking about system levers and drivers …

What would support active and engaging communities?
Who is responsible for making this happen?
Thinking about system levers and drivers …

Constructive Comfort
National N
HS
bodiesLocal N
HS
bodiesStaff
Service users
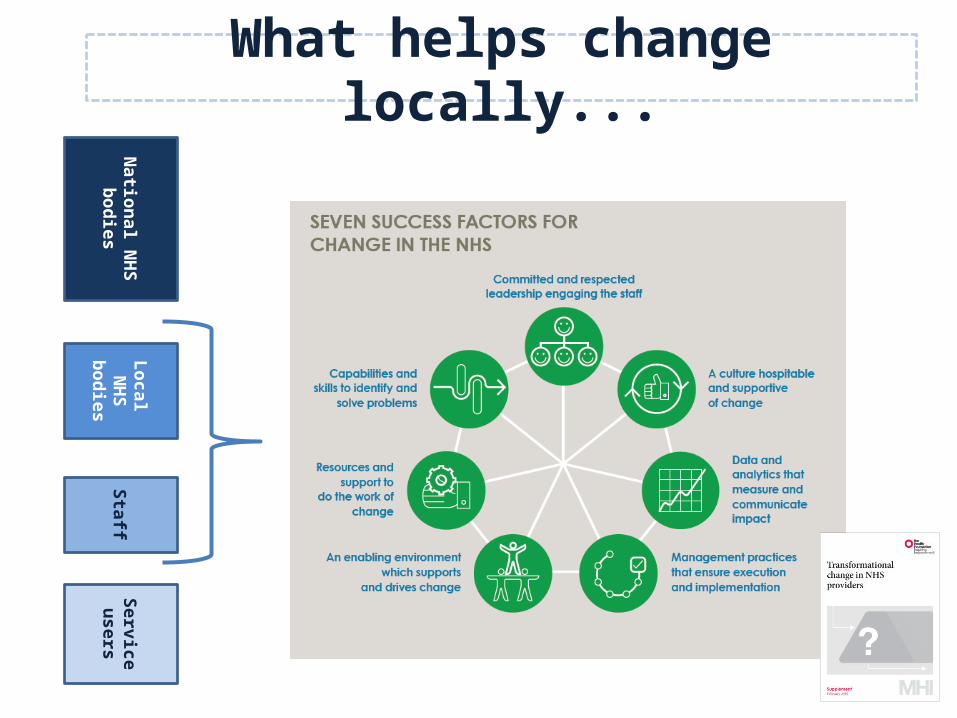
What helps change locally...
National N
HS
bodiesLocal N
HS
bodiesStaff
Service users
... And what gets in the way
National N
HS
bodiesLocal N
HS
bodiesStaff
Service users
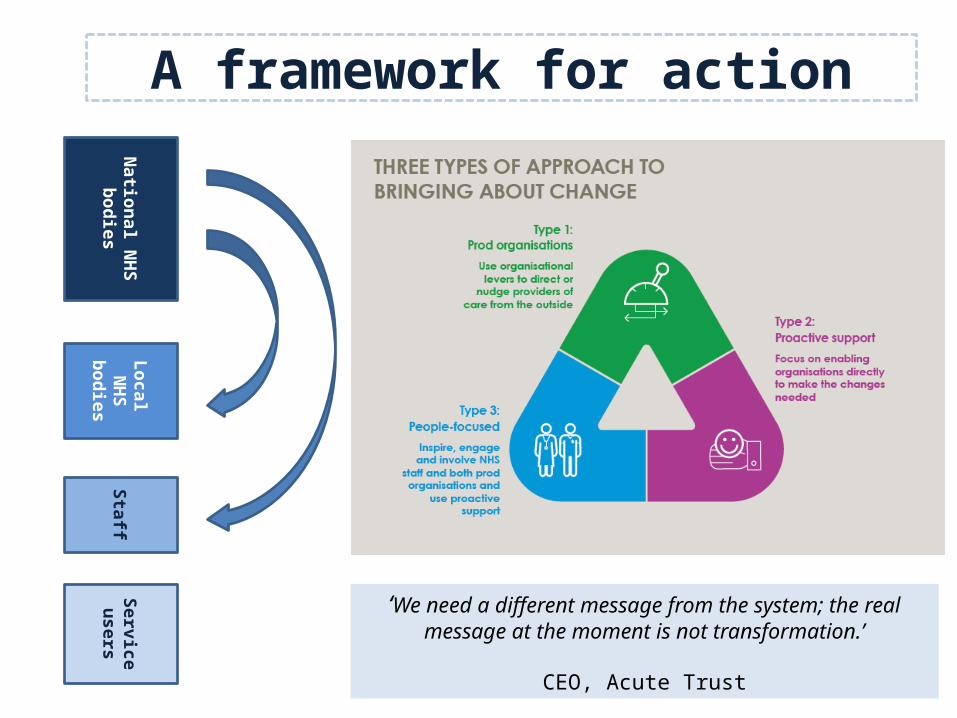
A framework for action
‘We need a different message from the system; the real message at the moment is not transformation.’
CEO, Acute Trust
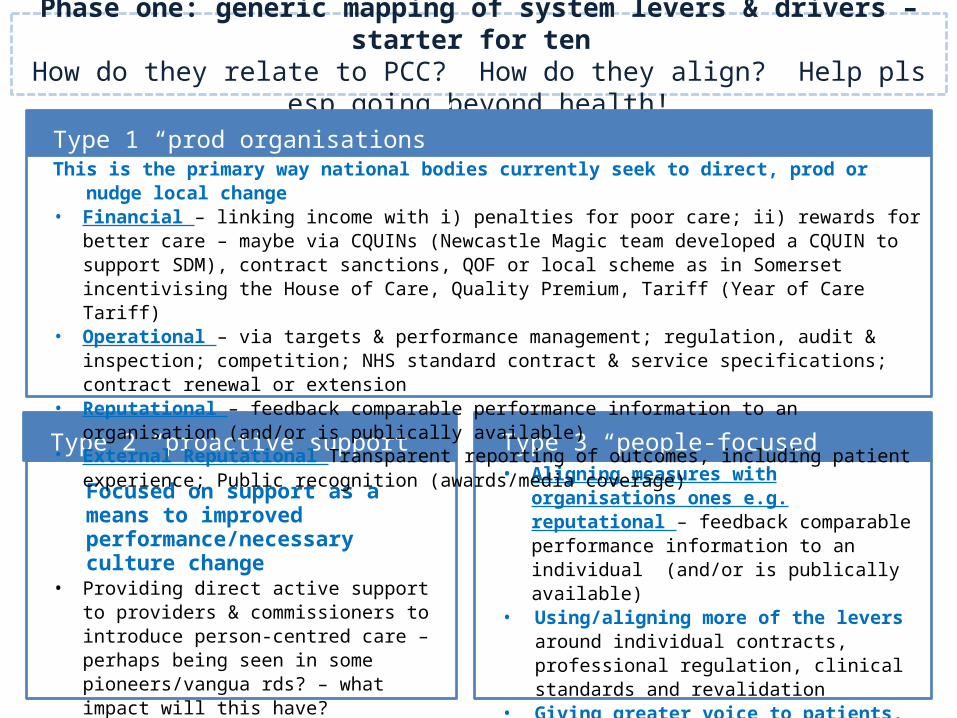
Focused on support as a means to improved performance/necessary culture change
• Providing direct active support to providers & commissioners to introduce person-centred care – perhaps being seen in some pioneers/vangua rds? – what impact will this have?
• Aligning measures with organisations ones e.g. reputational – feedback comparable performance information to an individual (and/or is publically available)
• Using/aligning more of the levers around individual contracts, professional regulation, clinical standards and revalidation
• Giving greater voice to patients, carers and families
• Perception of peers & opinion leaders
Phase one: generic mapping of system levers & drivers – starter for ten How do they relate to PCC? How do they align? Help pls esp going beyond health!
Type 1 “prod organisations”
Type 2 “proactive support” Type 3 “people-focused”
This is the primary way national bodies currently seek to direct, prod or nudge local change• Financial – linking income with i) penalties for poor care; ii) rewards for better care – maybe via CQUINs
(Newcastle Magic team developed a CQUIN to support SDM), contract sanctions, QOF or local scheme as in Somerset incentivising the House of Care, Quality Premium, Tariff (Year of Care Tariff)
• Operational – via targets & performance management; regulation, audit & inspection; competition; NHS standard contract & service specifications; contract renewal or extension
• Reputational – feedback comparable performance information to an organisation (and/or is publically available)
• External Reputational Transparent reporting of outcomes, including patient experience; Public recognition (awards/media coverage)