rebecca c. thurston, phd departments of psychiatry, psychology, and epidemiology university of...
TRANSCRIPT

Annoying Symptom or Harbinger of Disease? New Discoveries about Hot Flashes, Obesity, and Cardiovascular RiskRebecca C. Thurston, PhDDepartments of Psychiatry, Psychology, and EpidemiologyUniversity of Pittsburgh

Outline
Introduction to hot flashes Hot flashes and subclinical
cardiovascular disease Mechanisms Discussion/future directions

Hot Flashes Sensation of intense heat, sweating,
flushing
Hot flashes, night sweats (vasomotor symptoms)
Over 70% of women experience during menopausal transition
Can persist for decades
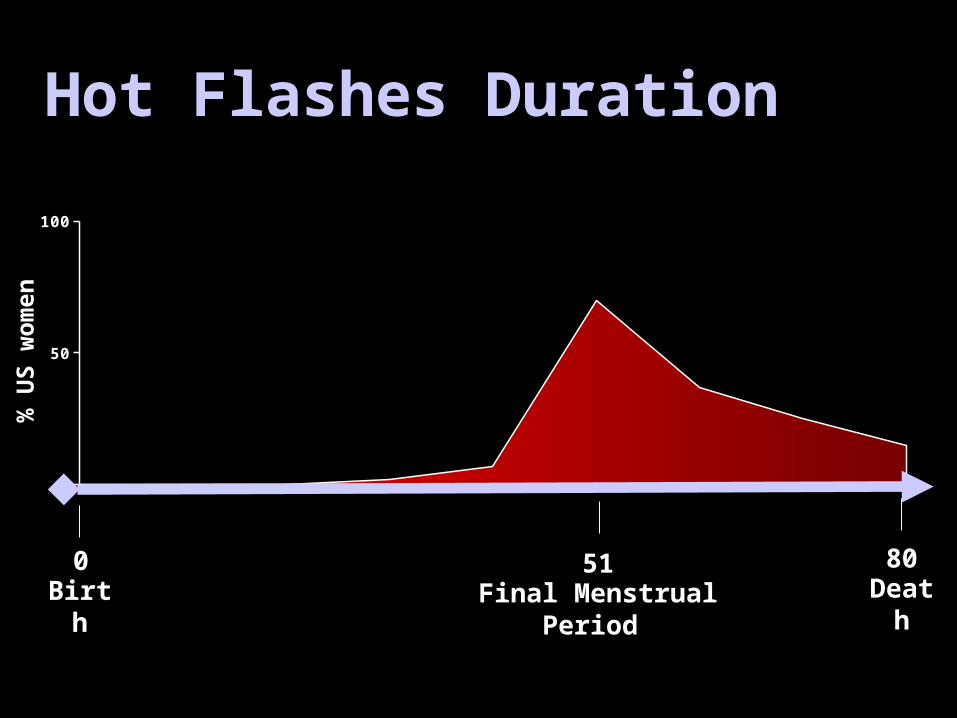
Hot Flashes Duration
0 10 20 30 40 50 60 70 800
50
100
0 8051Birth DeathFinal Menstrual Period
% U
S w
om
en

Hot Flashes Associated with pronounced
impairments quality of life:
Physical, social, emotional functioning
Sleep disruption, irritability, depressed mood, poorer cognitive function

Hot Flashes Leading cause of treatment seeking among
midlife women Findings of risk associated with hormone
therapy (HT)Most effective treatment for hot flashes
Increased interest in physiology of and nonhormonal treatments for hot flashes
Underlying physiology not well-understood

Physiology of Hot Flashes
Copyright ©2004 The Endocrine Society
Randolph, J. F. et al. J Clin Endocrinol Metab 2004;89:1555-1561
Estradiol (E2)
Follicle stimulating hormone (FSH)
Hot Flashes

Physiology of Hot Flashes
Sweating
Shivering
Thermoneutral zone
Thermoneutral zone
Tc Tc
Asymptomatic Symptomatic
Shivering
Sweating
(Freedman, 2001)

Outline
Introduction to hot flashes Hot flashes and subclinical
cardiovascular disease Mechanisms Discussion/future directions
Hot flashes long understood to have important impact on quality of life
Few medical implications?

Is a Hot Flash Just a Hot Flash? WHI & HERS: Women with hot flashes at
highest cardiovascular risk with HT use
Cardiovascular risk factors (smoking) also risk factors for hot flashes
E2 widespread cardiovascular impact
Potent vasodilator associated with hot flashes, not other types of sweating
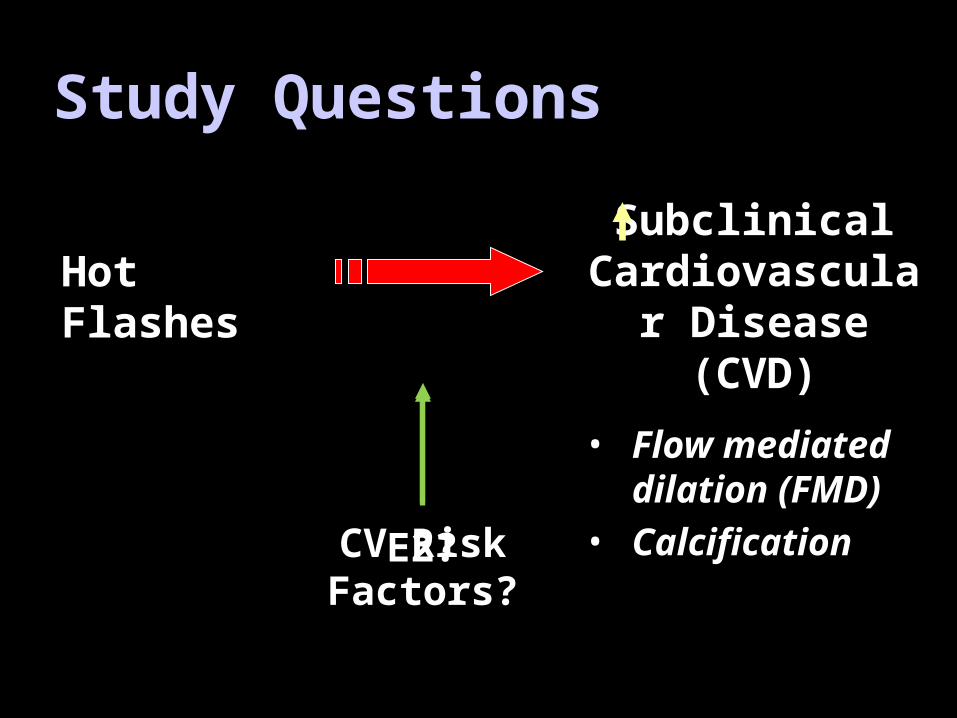
Study Questions
Hot FlashesSubclinical
Cardiovascular Disease (CVD)
• Flow mediated dilation (FMD)
• Calcification
CV Risk Factors?
E2?
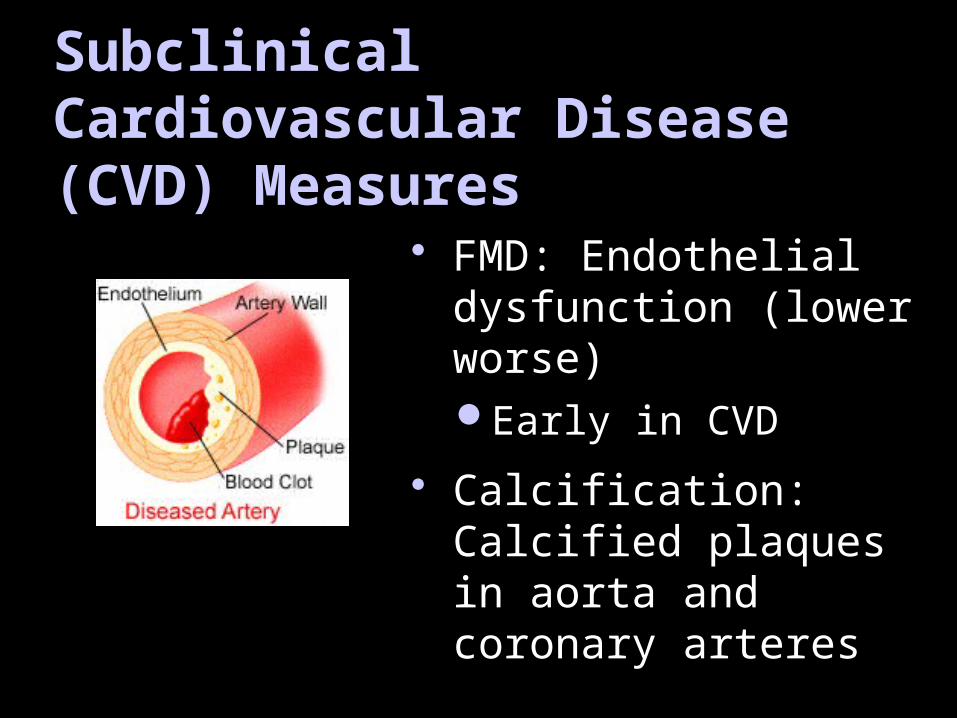
Subclinical Cardiovascular Disease (CVD) Measures
FMD: Endothelial dysfunction (lower worse)Early in CVD
Calcification: Calcified plaques in aorta and coronary arteres

Study of Women’s Health Across the Nation (SWAN)
Baseline
Yrs 4-7• FMD: Brachial
artery ultrasound• Calcification: EBT
aorta
SWAN Heart (N=557) Pittsburgh, Chicago
SWAN (N=3302)Annually:• Demographic,
Health behaviors, Affect
• Hot flashes• SBP, DBP, BMI• Blood Draw: E2,
lipids, glucose
10
B
B
B
B
2
3
4
5
6
7
8
9
1

Hot Flashes & Flow Mediated Dilation
4
6
8
10
12
None AnyHot Flashes
FM
D (
%,
M,
SD
)
B (SE) = -0.99 (0.41), p = 0.02B (SE) = -0.97 (0.44), p = 0.03B (SE) = -1.01 (0.41), p = 0.01
+ Covariates+ Covariates, E2
Age, site, race, lumen diameter, BMI, education, DBP, HT use, menopausal status, LDL, HDL, triglycerides, glucose, diabetes history, lipid med use, smoking, physical activity
Age, site, race, lumen diameter, BMI, education, DBP, HT use, HDL, LDL, triglycerides, glucose, diabetes history, lipid med use, smoking, physical activity, E2, cycle day of blood draw (Thurston et al., 2008, Circulation)
Age, site, race
*

Age, site, race, education, BMI, smoking, SBP, antidepressant use, HT, menopausal status, depressive sx, phys activity, glucose, HDL, LDL, triglycerides, diabetes hx
None Any50
60
70
80
Hot Flashes
% w
ith
Ao
rtic
Cal
cifi
cat
ion
Hot Flashes & Aortic Calcification
OR = 1.55, 1.10-2.19, p = 0.01
+ Covariates, E2OR = 1.63, 1.07-2.49, p = 0.02
+ CovariatesOR = 1.53, 1.02-2.29, p = 0.04
Age, site, race, education, BMI, smoking, SBP, antidepressant use, HT, menopausal status, depressive sx, phys activity, glucose, HDL, LDL, triglycerides, diabetes hx, cycle day, E2Age, site, race
(Thurston et al., 2008, Circulation)
*

Is a Hot Flash Just a Hot Flash?
Other subclinical CVD measures?

Intima Media Thickness (IMT)
IMT: Thickness of medial and intimal layers of carotid artery Most well-validated and
widely-used measure of subclinical CVD
Study Questions
Hot Flashes Intima media thickness (IMT)
CV Risk Factors?
E2?

Study of Women’s Health Across the Nation (SWAN)
Baseline
Baseline Yrs 4-7• IMT: Carotid artery
ultrasound
SWAN Heart (N=557) Pittsburgh, Chicago
SWAN (N=3302)Annually:• Demographic,
Health behaviors, Affect
• Hot flashes• SBP, DBP, BMI• Blood Draw: E2,
lipids, glucose
10
B
B
B
B
2
3
4
5
6
7
8
9 F
F
F
F
1
Follow up Yrs 6-9• IMT

Cross Sectional Association between Hot Flashes and IMT
age, site, race, education, BMI, smoking status, SBP, HDL, LDL, triglycerides, glucose, diabetes status/meds, CVD status/meds, HT use, menopausal statusage, site, race, education, BMI, smoking status, SBP, HDL, LDL, triglycerides, glucose, diabetes status/meds, CVD status/meds, HT use, E2, cycle day of blood draw
+E2B (SE) = 0.03 (0.01), p = 0.03B (SE) = 0.03 (0.01), p = 0.02
(Thurston et al., 2011, Menopause)
*

Association between Hot Flashes Across Visits and IMT
B (SE) = 0.03 (0.01), p = 0.03B (SE) = 0.02 (0.01), p = 0.04 +E2
age, site, race, education, BMI, smoking status, SBP, HDL, LDL, triglycerides, glucose, diabetes status/meds, CVD status/meds, HT use, menopausal statusage, site, race, education, BMI, smoking status, SBP, HDL, LDL, triglycerides, glucose, diabetes status/meds, CVD status/meds, HT use, E2, cycle day of blood draw
(Thurston et al., 2011, Menopause)
*

Relation between hot flashes and IMT by obesity status
Study Visits with Hot Flashes
None One Both0.6
0.62
0.64
0.66
0.68
0.7
0.72
0.74
0.76
NormalOverweightObeseIM
T (
mm
)
Hot flashes *BMI p<0.01

Hot Flashes and Subclinical CVD Women with hot flashes had higher
subclinical CVD (FMD, calcification, IMT) Persist controlling for CVD risk factors, E2 Most pronounced with high BMI Hot flashes mark something more? Consider role of the vasculature in hot
flashes Mechanisms?

Outline
Introduction to hot flashes Hot flashes and subclinical
cardiovascular disease Mechanisms Discussion/future directions

A Note about Measurement Epidemiologic studies use
questionnaire measures of hot flashes Crude, memory and reporting influences
Physiologic, diary measures of hot flashes Data in “real time”
More precise
Insight into reporting influences

Physiologic Measurement of Hot Flashes

Hot Flash Diary Occurrence Severity Bothersome Location on body Aura Emotions Health behaviors…

“False Positive” Hot Flash Reporting
Physiologic
Reported (Diary)
Yes No
Yes 347 208
No 394 --

Psychological Factors Associated with False Positive Hot Flashes
Low Medium High0
0.1
0.2
0.3
0.4
0.5
0.6
0.7Depressive sxState anxietyTrait anxiety
Level of Negative Affect
Fa
lse
po
sit
ive
re
po
rtin
g r
ate
(Thurston et al., 2005, Psychosom Med)
**
†
† p < 0.1* p < 0.05

Emotional Antecedents of “False Positive” Hot Flashes
0
0.5
1
1.5
2
OR
Fa
lse
Po
sit
ive
Ho
t F
las
h
Fru
stration
Sa
dn
es
s
Stre
ss
Tire
d
Ha
pp
y
Re
laxe
d
In
Co
ntro
l
*
*
* p < 0.05(Thurston et al., 2005, Psychosom Med)

A Note about Measurement
Mood and emotions can impact hot flashes
When using self-report measures only, consider the role of emotion
Best to have physiologic + diary measures (laboratory/clinical studies)

Hot Flashes and Autonomic Nervous System
Etiology of hot flashes: Role of autonomic nervous system speculatedSympathetic, parasympathetic (vagus)
Reduced parasympathetic (vagal) control of heart rate linked to elevated CVD risk
High frequency heart rate variability(HF-HRV) index of cardiac vagal control
Study Question
Hot Flashes Cardiac vagal control (HF-HRV)

PMBC FLASHES Study
• 30 peri and postmenopausal women, aged 40-60, >4 hot flashes/day, no HT, SSRI/SNRIs
• Lab procedures to induce hot flashes
• Continuous ECG (HF-HRV) and sternal skin conductance
• Hot flashes physiologically measured and self-reported
Observation30 min
Stress 5 min
Heat30 min
Cold Pressor1 min

Data Reduction & Analysis
Spectral analysis of heart rate time series Linear mixed models
Minutes during flash compared to non-flash pre and post flash periods
Covariates: Age, task, race, menopausal status, education, smoking, anxiety, BMI, diabetes, use of cardiovascular meds/HTN, physical activity

FlashPre-flash Post-flash
Hot Flash
Data Reduction & Analysis
Minute -10 Minute +10

Reduced Cardiac Vagal Control During Hot Flashes: Laboratory
* p < 0.05 vs. minute zero
Pre-Flash Period
Post-Flash Period
Flash Period
(Thurston et al. 2010, Menopause)
Flash Period

Ambulatory Study: During Daily Life• 42 peri and postmenopausal women,
aged 40-60, >4 hot flashes/day, no HT, SSRI/SNRIs, or CV medications
• Wore ambulatory monitor for 24 hourso Hot flashes o ECG o Respiration
• Hot flashes physiologically measured and self-reported

Reduced Cardiac Vagal Control During Hot Flashes: Ambulatory (24 hrs)
Pre-flash Post-flashp<0.0001 p<0.0001
Minutes surrounding hot flash
HF
-HR
V (
lnm
sec2 )
(Thurston et al., 2012,
Menopause)
Hot Flash
Autonomic nervous system and hot flashes Reduced HF-HRV during hot flashes
Laboratory and ambulatory settings
Insight into etiology of hot flashesReproductive hormonal
Thermoregulatory
Autonomic nervous system?
Mechanism linking hot flashes to CVD risk?

In SWAN, hot flashes associated with elevated subclinical CVD
Mechanisms?Autonomic nervous system (Thurston et al., 2010,
Thurston et al., 2012)
Inflammation/hemostasis (Thurston et al., 2011)
Hot Flashes and CVD risk

Other mechanisms: Inflammation/hemostasis
Inflammation/hemostasis and hot flashes?
Regulated in part by vascular endothelium
One study: IL-8 elevated among women with hot flashes (Yasui et al., 2006)
Sensitive to reproductive hormones
CV risk factors?
Study Questions
Hot Flashes
E2?
Inflammation/ hemostasis
CRP, PAI-1, Factor VIIc, TPA-antigen, fibrinogen

B
Study of Women’s Health Across the Nation (SWAN)
SWAN (N = 3302)Annually:• Demographic, Health behaviors,
Medications/Health status, Affect• Hot flashes, night sweats• SBP, DBP, BMI• Blood Draw: E2, lipids, glucose
7
6
5
4
2
3
4
5
6
7
8
9
1
3
1
B
Inflammatory/hemostatic markers:• CRP, PAI-1, and tPA-ag• Fibrinogen and FVIIc
10

0 1 3 4 5 6 75
6
7
8
9
10
None 1-5 Days 6+ Days
SWAN Visit
TP
A-a
nti
gen
(lo
g)
Hot Flashes and TPA-antigen
Hot flashes in past two weeksCovariates: education, menopausal status, alcohol, parity smoking, exercise, affect, BMI, CV meds, diabetes/insulin, steroids, pain med, antidepressants
p<0.001
(Thurston et al., 2011)

0 1 3 5 7100
105
110
115
120
125
130
135
140
None 1-5 Days 6+ Days
SWAN Visit
Fac
tor
VIIc
(lo
g)
Hot Flashes and Factor VIIc p<0.01
Hot flashes in past two weeksCovariates: education, menopausal status, alcohol, parity smoking, exercise, affect, BMI, CV meds, diabetes/insulin, steroids, pain med, antidepressants
(Thurston et al., 2011)
In SWAN, hot flashes associated with elevated subclinical CVD
Mechanisms?Autonomic nervous system (Thurston et al., 2010,
Thurston et al., 2012)
Inflammation/hemostasis (Thurston et al., 2011)
Lipids (Thurston et al., 2012)
Hot Flashes and CVD risk
What about lipids?
Well known CV risk factor
Some research suggestive of adverse lipid profile among women with hot flashes

CV risk factors?
Study Questions
Hot Flashes
E2?
Adverse lipid profile?
LDL, HDL, Triglycerides, ApoB, ApoA1
B
7
6
5
4
2
3
4
5
6
7
8
9
1
3
1
B
Lipids:• LDL, HDL, triglycerides, ApoB, ApoA1
10
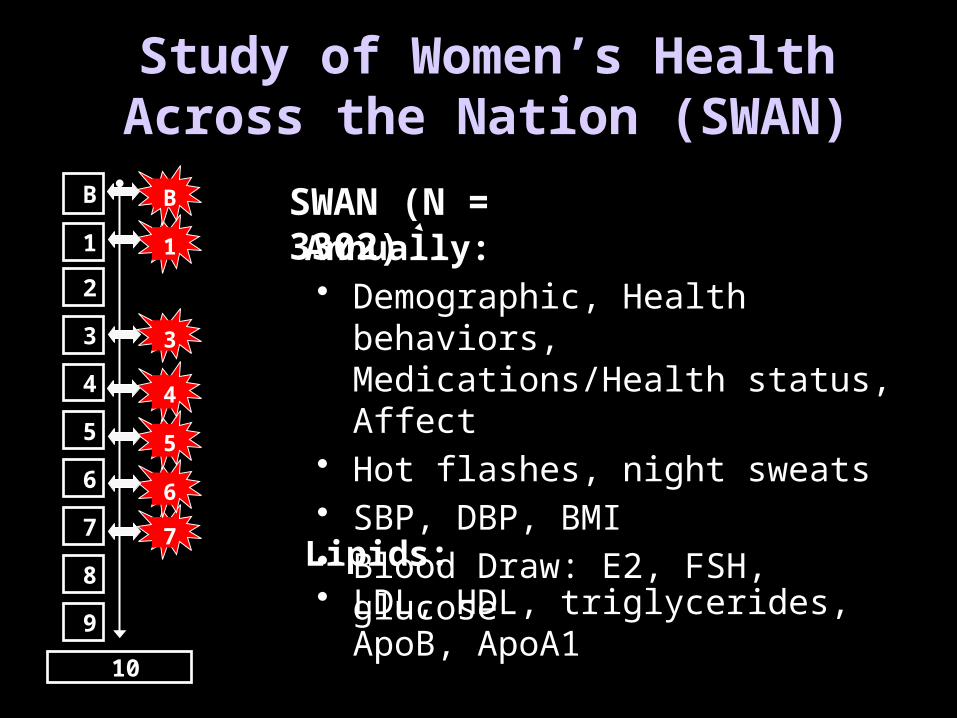
Study of Women’s Health Across the Nation (SWAN)
SWAN (N = 3302)Annually:• Demographic, Health behaviors,
Medications/Health status, Affect• Hot flashes, night sweats• SBP, DBP, BMI• Blood Draw: E2, FSH, glucose
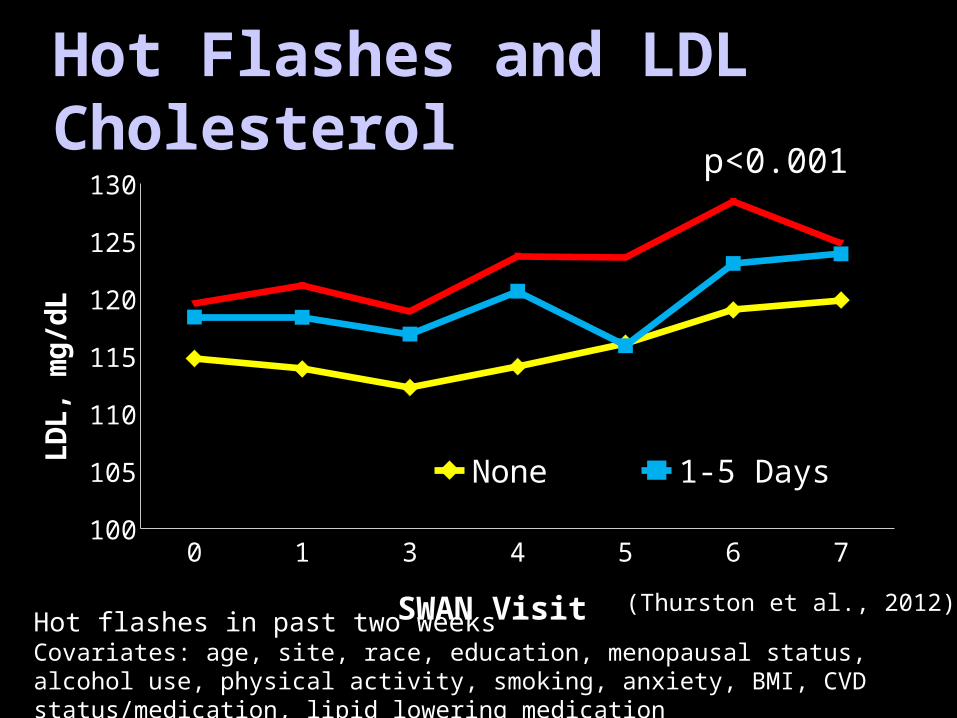
Hot Flashes and LDL Cholesterol
0 1 3 4 5 6 7100
105
110
115
120
125
130
None 1-5 Days 6+ Days
SWAN Visit
LD
L, m
g/d
L
Hot flashes in past two weeksCovariates: age, site, race, education, menopausal status, alcohol use, physical activity, smoking, anxiety, BMI, CVD status/medication, lipid lowering medication
p<0.001
(Thurston et al., 2012)

Hot Flashes and ApoB
0 1 3 4 5 6 795
100
105
110
115
120
None 1-5 Days 6+ Days
SWAN Visit
Ap
oB
, m
g/D
l
p<0.0001
Hot flashes in past two weeksCovariates: age, site, race, education, menopausal status, alcohol use, physical activity, smoking, anxiety, BMI, CVD status/medication, lipid lowering medication
(Thurston et al., 2012)

Hot Flashes and Triglycerides
0 1 3 4 5 6 780
90
100
110
120
130
140
150
160
None 1-5 Days 6+ Days
SWAN Visit
Tri
gly
ceri
des
, mg
/Dl p<0.0001
Hot flashes in past two weeksCovariates: age, site, race, education, menopausal status, alcohol use, physical activity, smoking, anxiety, BMI, CVD status/medication, lipid lowering medication
(Thurston et al., 2012)

In SWAN, hot flashes associated with elevated subclinical CVD
Mechanisms?Autonomic nervous system (Thurston et al., 2010,
Thurston et al., 2012)
Inflammation/hemostasis (Thurston et al., 2011)
Lipids (Thurston et al., 2012)
Hot Flashes and CVD risk

Outline
Introduction to hot flashes Hot flashes and subclinical
cardiovascular disease Mechanisms Discussion/future directions

Hot Flashes and CVD risk Hot flashes associated with elevated
subclinical CVDMultiple mechanisms
Subtypes of hot flashes? Synergize with other CV risk factors? Physiologic, diary measures of hot
flashes?

Next Steps: CVD Risk and Hot Flashes New study designed to address CVD risk
and hot flashes R01HL105647: N=300 with and without
hot flashes, 5 years Detailed physiologic, psychological
mechanisms Physiologic, diary hot flash measures
Implications? Better understand physiology of hot
flashes
Midlife marker of CVD risk?
Aggressive risk factor reduction among women with hot flashes?
Improve health of midlife women
SWAN has grant support from the NIH, DHHS, through the NIA,
NINR, NHLBI, ORWH (NR004061; AG012505, AG012535, AG012531, AG012539, AG012546, AG012553, AG012554, AG012495, HL065581, HL06551)
Thurston: K23AG029216University of Pittsburgh Institute
on Aging
The content of this presentation is solely the responsibility of the authors and does not
necessarily represent the official views of the NIA, NINR, ORWH or the NIH.
Karen Matthews, PhD Kim Sutton-Tyrrell, DrPH Rachel Hess, MD, MSc
Samar El Khoudary, PhD Faith Selzer, PhD
Susan Everson-Rose, PhD, MPH
Ellen Gold, PhD Imke Janssen, PhD Lynda Powell, PhD Israel Christie, PhD
Carolyn Crandall, MD, MS Barbara Sternfeld, PhD
Acknowledgements

Thank you!

Questions?