rebecca sposato ms, rn. a collection unpleasant emotions stemming from a real or perceived...
TRANSCRIPT

Rebecca Sposato MS, RN
A collection unpleasant emotions stemming from a real or perceived threat/stressor ◦ Often instinctual, necessary for survival and social
order ◦ Increases when one is unable to deal with threat◦ May present as fear, dread, nervousness,
uneasiness or apprehension
May be the primary syndrome or present as a symptom of another disorder◦ Many behaviors emerge to counteract anxiety◦ Comorbid w/ depression, substance abuse etc.
Biological: genetic and neuro-chemical abnormalities
Psychodynamic: Internal and interpersonal conflict
Behavioral: learned response to a stressor
Cognitive: distorted and negative thinking
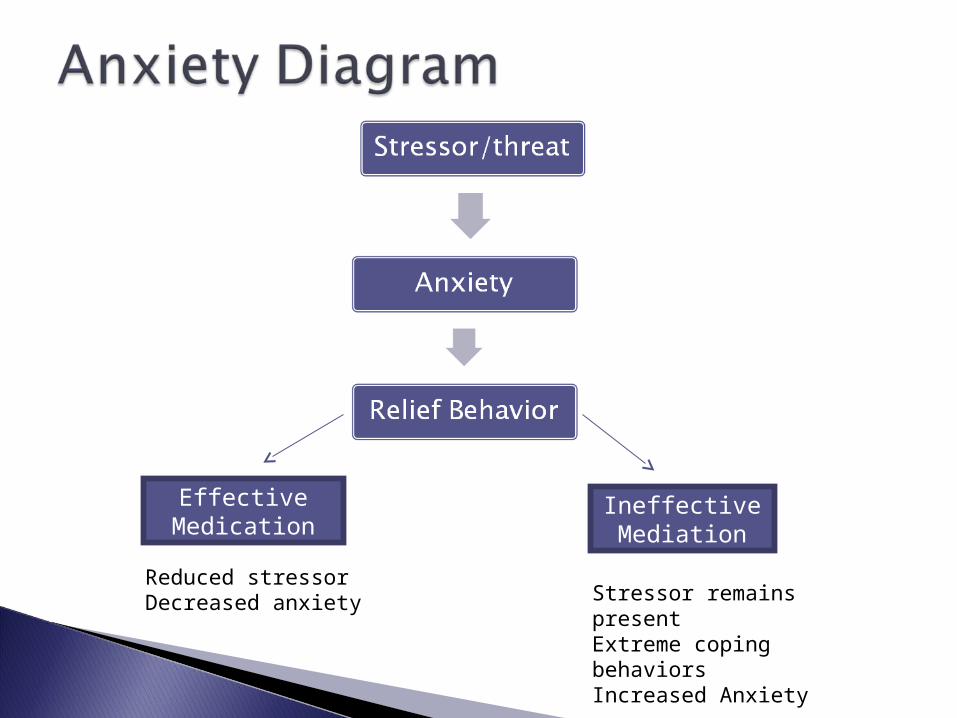
Effective Medication
Ineffective Mediation
Reduced stressor Decreased anxiety Stressor remains present
Extreme coping behaviorsIncreased Anxiety

Mild: Adaptive heightened awareness to everyday living◦ Greater focus and process additional sensory data◦ Slight physiological arousal
Moderate: No longer normal◦ impaired perceiving and processing sensory data◦ Impaired reasoning and problem-solving◦ Measurable physiological arousal

Severe: Anxiety dominates experience◦ Distorted perceiving and processing sensory data◦ Impaired memory, reasoning, problem-solving◦ Marked physiological changes
Panic: Terror dominates experience◦ Disorganized perceiving and processing sensory
data◦ Unable to purposefully interact with other persons
or environment◦ Out of control physical behavior and movements◦ Exaggerated physiological changes

Acute episode of marked anxiety and physiological changes◦ Exaggerated for perceived threat◦ Can be confused with heart attack◦ Expected (cued) – response to known trigger◦ Unexpected (uncued) – no known association
DSM-IV: Not a stand-alone disease, no numeric code, ◦ Must of 4 of the following: tachycardia,
diaphoresis, tremors, dyspnea, angina, nausea, de-realization, dizzy, fear of losing control, fear of dying, paresthesia, chills/hot flashes
Recurrent panic episodes with persistent concern lasting over 1 month and avoiding behaviors
1-2% one year prevalence in population
Variable onset and duration, typical onset between adolescence and age 30. ◦ Chronic course w/ wax-wane pattern◦ Often comorbid w/ agoraphobia
Excessive fear, with a marked physiological response, to a specific thing or situation◦ Predisposing event◦ Acute onset
6% lifetime prevalence in population◦ Often have childhood onset, ◦ 2:1 female to male◦ Subtype categories: animal, environment,
blood/injury, situation

Social phobia: exaggerated concern over being embarrassed, ridiculed or judged in the presence of others◦ Causes physical symptoms of anxiety◦ Deters normal daily, social and occupational
functioning◦ May be general or specific to public performances
or social gatherings (parties)◦ Can be acute or chronic

Persistent symptoms of anxiety not attached to specific triggers, lasting over 6 months◦ Focus of worry is out of proportion to source◦ Person may not insight into source of anxiety
5% lifetime prevalence, slightly more female
DSM-IV: a) excessive concern, b) difficult to control, c) 3 physical symptoms, d) not due to another Axis 1 condition, e) distress impairs functioning, f) the physical symptoms are not due to another condition

OCD – recurrent and time-consuming, often ritualized, behaviors causing significant impairment in daily function◦ Often an exaggerated natural behavior
(grooming, nesting, hoarding for winter)◦ Often ego-dystonic, person may or may not have
self insight into abnormality◦ 2% lifetime prevalence
Obsession – persistent and anxiety producing ideas, impulses and images that something is wrong
Compulsion – the action extending from the obsession, to temporarily fix the anxiety

A normal response to an abnormal event◦ Physiological arousal or emotionally numb,
dissociation, amnesia or flashbacks, aversion or obsession with trigger,
Triggered by an extreme life stressor/threat-◦ A recipient or witness to violence, unnatural death,
catastrophe perceived as threat to self and life Acute- Within one month of the event PTSD- Symptoms present 3 months after
event, may last years 8% lifetime prevalence
Pharmacological – benzodiazepines, Buspirone, SSRI
Milieu Therapy- supportive environment Therapy – psych, REBT, CBT, DBT,
relaxation training, ◦ Modeling- person watches another’s normal
reation◦ Systematic Desensitization- repeated increasing
exposure to trigger to grow tolerance◦ Flooding- excessive exposure to trigger to
extinguish fear Not as popular as desensitization

Symptom management and control
Promote and support adaptation and coping
Promote and support daily function
Health teaching