recent advances in endovascular techniques for …7baae124-f4f7-4e18-a019... · recent advances in...
TRANSCRIPT
Recent advances in endovascular techniques for management of acute nonvariceal upper gastrointestinal bleeding Romaric Loffroy Basem A. Abualsaud MingDe Lin Pramod P. Rao Abstract Over the past two decades, transcatheter arterial embolization has become the first-line therapy
for the management of upper gastrointestinal bleeding that is refractory to endoscopic
hemostasis. Advances in catheter-based techniques and newer embolic agents, as well as
recognition of the effectiveness of minimally invasive treatment options, have expanded the role
of interventional radiology in the management of hemorrhage for a variety of indications, such as
peptic ulcer bleeding, malignant disease, hemorrhagic Dieulafoy lesions and iatrogenic or trauma
bleeding. Transcatheter interventions include the following: selective embolization of the feeding
artery, sandwich coil occlusion of the gastroduodenal artery, blind or empiric embolization of the
supposed bleeding vessel based on endoscopic findings and coil pseudoaneurysm or aneurysm
embolization by three-dimensional sac packing with preservation of the parent artery.
Transcatheter embolization is a fast, safe and effective, minimally invasive alternative to surgery
when endoscopic treatment fails to control bleeding from the upper gastrointestinal tract. This
article reviews the various transcatheter endovascular techniques and devices that are used in a
variety of clinical scenarios for the management of hemorrhagic gastrointestinal emergencies.
Keywords Upper gastrointestinal bleeding; Endoscopy; Angiography; Embolization; Surgery
Introduction Upper gastrointestinal bleeding (UGIB) is defined as originating in the distal esophagus, stomach
and duodenum (proximal to the ligament of Treitz). The most common cause of nonvariceal
UGIB is peptic ulcer disease (PUD). Other less common causes include benign and malignant
tumors, ischemia, gastritis, arteriovenous malformations such as Dieulafoy lesions, Mallory-
Weiss tears, trauma and iatrogenic causes[1,2]. Effective treatment requires timely and accurate
diagnosis (location and etiology) and, unlike lower gastrointestinal bleeds, most patients have
undergone endoscopic examination and treatment prior to their referral to interventional
radiology. Of the small group of patients who fail endoscopic therapy, some are treated
surgically[3] but, increasingly, the majority are referred for embolotherapy[4]. Transcatheter
arterial embolization (TAE) has been performed for at least two decades and has been shown to
be effective at controlling hemorrhage and decreasing mortality[5-10]. Embolization techniques
have evolved with the use of microcatheters and new embolic agents. This review presents the
clinical evaluation and causative mechanisms of hemorrhagic upper gastrointestinal emergencies.
It also discusses the advances in endovascular embolization in their management, including
embolic agents, therapeutic techniques, results and limitations.
Indications Indications that require angiogram and embolization are described below. Several population-
based and prospective studies support PUD being the most common cause of acute UGIB[11].
PUD refers to either gastric or duodenal ulcers but under a broad heading of “ulcers” some
investigators also include esophageal ulcers. Approximately 50% of all cases of acute UGIB are
attributed to PUD[11].
Another recently reported trend in acute UGIB involves cyclooxygenase-2 inhibitors.
Cyclooxygenase-2 inhibitors, known for their decreased gastrointestinal toxicity, are extensively
used for both their anti-inflammatory and analgesic properties. This class of anti-inflammatory
drugs is associated with both decreased endoscopic lesions and episodes of UGIB when
compared with their nonselective nonsteroidal anti-inflammatory drug counterparts[12,13].
Population-based studies evidence suggests that the introduction of cyclooxygenase-2 inhibitors
may be associated with an overall increased nonsteroidal antiinflammatory drug use and
UGIB[14]. Gastrointestinal hemorrhage can certainly be facilitated when a patient has an
endogenous coagulopathic state or is taking anticoagulation therapy.
Classically, Mallory-Weiss tears are mucosal lacerations at the gastroesophageal junction or in
the cardia of the stomach[15]. These lesions can be associated with repeated retching or vomiting
and are another important cause of nonvariceal UGIB. It is estimated that 5% to 15% of all cases
of acute UGIB are secondary to Mallory-Weiss tears[15,16]. Most bleeding episodes caused by
MalloryWeiss tears are self-limited, requiring no endoscopic hemostasis[17]. Nevertheless, some
cases are severe enough to require blood transfusions or therapeutic interventions such as
endoscopic hemostasis, endovascular embolization or surgery.
Dieulafoy’s lesion is a rare etiology in acute UGIB. Dieulafoy’s lesions are difficult to identify
endoscopically because they often retract. Their histopathological description is a “caliber-
persistent artery” in the submucosal tissue[18]. These lesions are responsible for less than 5% of
all nonvariceal UGIB[18].
Neoplasms, both malignant and benign, are another infrequent cause of non-variceal UGIB,
contributing to less than 5% of all UGIB cases[19]. Although only a small fraction of UGIB is of
neoplastic etiology, this may be the only presenting symptom of a neoplasm, which should be
included in the differential diagnosis[19].
Other rare causes of nonvariceal UGIB should also be considered in any differential diagnosis.
Hemobilia is a rare cause of UGIB that should be considered in the setting of recent
hepatobiliary tree instrumentation, such as with endoscopic retrograde cholangiopancreatography
or laparoscopic cholecystectomy. Bile duct and hepatic artery injuries are possible complications
of these procedures, and patients can ultimately present with signs of UGIB[20]. In patients with
chronic pancreatitis who present with acute UGIB, hemosuccus pancreaticus should also be
excluded. Although it is an uncommon cause of UGIB overall, bleeding in these patients can be
secondary to a pseudoaneurysm (PA) in peripancreatic blood vessels as a complication of
pancreatic pseudocysts[21]. Finally, iatrogenic injuries secondary to biopsies or endoscopic
procedures, such as percutaneous endoscopic gastrostomy tube placement, are also rare but
documented causes of nonvariceal UGIB[22].
Anatomy The vascular supply to the stomach and duodenum is quite rich, with avid redundant supply. This
can make successful embolization more challenging; however, it decreases the incidence of
postembolization ischemia[23]. The likelihood of successful embolization reflects prior
knowledge of the location of the bleed. The left gastric artery (LGA) runs along the lesser curve
of the stomach and supplies the stomach and distal esophagus. The LGA is most often the first
branch of the celiac trunk (90%) but may arise directly from the aorta, as a lienogastric trunk or
hepatogastric trunk[24]. It anastomoses with the right gastric artery (RGA). Small distal branches
anastomose with short gastric arteries (from the splenic artery) and the left inferior phrenic
artery. The RGA most often originates from the proper, left or middle hepatic artery but may also
arise from the gastroduodenal artery (GDA) or the right hepatic artery (RHA). It is typically a
small vessel that runs in the gastrohepatic ligament and supplies the distal lesser curve of the
stomach and the pylorus. The greater curvature of the stomach is supplied by the gastroepiploic
arcade that courses along the greater curvature of the stomach and is supplied by the right
gastroepiploic artery (RGEA), the terminal branch of the GDA and the left gastroepiploic artery,
a branch of the distal splenic artery (SA). A complete arcade (rather than incomplete or weak) is
present in about 65% of patients. The duodenum is supplied by the pancreaticoduodenal arcade, supplied
by superior and inferior, posterior and anterior pancreaticoduodenal arteries, branches of the GDA and
superior mesenteric artery (SMA), respectively. The GDA arises from the common hepatic artery in a
large majority of patients but may also arise from the RHA, a replaced RHA branch of the SMA, or
directly from the celiac axis.
Diagnostic Angiography Preprocedural assessment and patient preparation Patients undergoing a transcatheter procedure for the evaluation and management of hemorrhage
are often poor surgical candidates. They are more often than not hemodynamically unstable and
often have other clinical issues, such as an electrolyte imbalance or a coagulopathy. Whenever
possible, the hemodynamic status of the patient should be stabilized by fluid resuscitation. Any
pertinent laboratory abnormalities should be corrected by the time the patient reaches the
interventional suite. The preprocedural laboratory data should include complete blood count,
renal function and coagulation parameters. Optimal laboratory parameters include a serum
creatinine < 1.5 mg/dL with an estimated glomerular filtration rate > 60, an international
normalized ratio (INR) < 1.5 and a platelet count > 50000/dL. If necessary, blood products such
as fresh frozen plasma, platelets or packed red blood cells should be transfused before the
procedure. They may also be given intra-procedurally. It is also desirable to correct any
coagulopathy before embolization because achieving hemostasis depends on technically
successful embolization as well as the patient’s ability to clot properly. Any history of prior drug
or contrast medium allergies must be documented. Any pertinent prior diagnostic cross-sectional
imaging studies should be reviewed as these may provide valuable information that may direct
and potentially affect the outcome of the intervention. Virtually all patients will also have
undergone upper endoscopy in an attempt to identify and treat the source of bleeding.
Timing of angiographic evaluation The typical candidate patient presents with the following: (1) massive bleeding (requiring
transfusion of at least 4 U of blood/24 h) or hemodynamic instability (hypotension with systolic
pressure < 100 mmHg and heart rate of 100 min or clinical shock secondary to blood loss); (2)
bleeding that has failed to respond to conservative medical therapy, including volume
replacement, antacids, H2receptor blocking agents or proton pump inhibitors; and (3) bleeding
that has failed to respond to at least one, and sometimes two, attempts at endoscopic control[25].
Endoscopy is performed before angiography. Performance of angiography before endoscopy
leads to an unacceptably high frequency of unnecessary angiography. Endoscopic diagnosis and
therapy can render angiography unnecessary. Endoscopy also helps in planning the timing and
approach of angiography. For example, inability to determine the cause of bleeding at endoscopy because
of severe bleeding should prompt urgent angiography. Even endoscopic localization of the bleeding site
without determination of the cause helps guide which artery to cannulate first at angiography[26].
Negative endoscopic information, such as excluding esophageal bleeding, is valuable to the angiographer.
On the other hand, Walsh et al[27] and Loffroy et al[25] found longer time to angiography to be
predictor of early rebleeding after TAE. They concluded that every effort should be made to perform
angiography with embolization early after bleeding onset. Thus, the ability to achieve bleeding control in
critically ill patients seems to depend chiefly on early intervention.
There is much discussion about the necessity of diagnostic studies preceding angiography.
Certainly, endoscopy has a diagnostic and therapeutic role and can completely replace the need
for angiography of the upper gastrointestinal tract in more than 90% of patients[26]. However,
most of the controversy involves the need for nuclear scintigraphy before diagnostic angiography
in the patient with lower gastrointestinal bleeding. Scintigraphy has been notoriously inaccurate
when locating lesions for surgical resection; however, scintigraphy is certainly more sensitive,
requiring reportedly 10-fold less hemorrhage than angiography to achieve a positive
study[28,29]. As an adjunct to angiography, the probability of a positive diagnostic angiogram is
increased by a preceding positive nuclear scintigraphic study. In general, the decision to proceed
directly to angiography without nuclear scintigraphy depends on the clinical situation and the
degree of hemorrhage. The clinical presentation of lower gastrointestinal bleeding may be
episodic or continual. The former ranges from minor episodes that resolve, to chronic
intermittent bleeding, to severe life-threatening hemorrhage. Angiography is warranted in the
latter group and may, with provocation, play a diagnostic role in the second. Usually, nuclear
scintigraphy is recommended before angiography in all cases of episodic bleeding. Angiography
remains the primary diagnostic imaging tool in those patients with continual active hemorrhage,
however, and delaying angiography for scintigraphy is not warranted. Intermittent lower
gastrointestinal hemorrhage deserves special attention. This difficult group of patients often
bleeds, frequently to low hemoglobin and hematocit levels, yet a site cannot be localized.
Bleeding has been successfully provoked using a variable combination of anticoagulants,
vasodilators and fibrinolytics. Wireless capsule endoscopy is now being used as a diagnostic tool
for a variety of gastrointestinal disorders including Crohn’s disease, celiac disease and obscure
gastrointestinal bleeding[30,31]. At the present time, however, it is not a practical modality to
use in acute UGIB.
Finally, the amount of bleeding may affect treatment strategy, continued active bleeding
demands for emergency angiography primarily without pre-procedural testing. Defreyne et
al[32] and Whitaker et al[33] independently indicated that the most important determinant of the
timing of angiography may be the findings of an experienced endoscopist when faced with nontractable
bleeding.
Technique of angiography In the advent of UGI bleeding, the source for hemorrhage is usually identified by endoscopy.
Therefore, angiography is most often performed only as a precursor to TAE based on the
knowledge of the vascular supply to the abnormal area. Diagnostic angiography for UGI
bleeding is straightforward and is centered on the anatomy of the celiac artery and the SMA. A
trans femoral approach is usually used and involves placement of a 5F introducer sheath in the
common femoral artery. A variety of introducers and selective catheters with a smaller caliber
can be used to cannulate the celiac artery and obtain access to the common hepatic artery. For
selective catheterization by way of the femoral route, the most widely used catheters are the
cobra, hook and shortand long-curve sidewinder with a 4F diameter. Once access is secured,
arteriogram is performed to delineate the anatomy. Localization of contrast extravasation into the
bowel lumen is considered as a direct angiographic sign of active GI bleeding. Commonly
encountered indirect angiographic signs of GI bleeding include visualization of an aneurysm, PA
or a submucosal vessel and early venous drainage of angiodysplasia. Other angiographic signs
include neovascularity, mucosal or extramucosal hyperemia, intramural pooling of contrast or
arterial wall abnormalities[34]. Selective catheterization for UGI bleeding includes the celiac and
superior mesenteric arteries. The initial artery catheterized is the one most suspected of bleeding
based on previous imaging or endoscopy, which is, of course, the celiac artery for UGI bleeding.
If no extravasation is seen, then superselective angiography is advised. Depending on endoscopic
findings that offer information on the likely location of the bleeding source, superselective
catheterization of the GDA, LGA or SA may be performed. A microcatheter is always necessary
and recommended for a distal superselective approach to the bleeding vessel so as to avoid the
spasm or occlusion caused by larger 4F or 5F catheters. Longer injection durations or use of
carbon dioxide for contrast medium can also improve sensitivity for small bleeds. In the absence
of hemodynamic instability, computed tomographic angiography is a good and reliable method
to highlight the presence of a bleed in progress and should be performed before any invasive
procedure. Arteriography after superselective cannulation may show extravasation that could
have been missed during contrast injection in the main hepatic artery. When a dual supply of the
bleeding area is suspected, both arterial sources must be embolized to assure that all of the
inflow ceases. This is typically noted in bleeding secondary to an ulcer that erodes into the GDA.
Embolization in this case must start distally to prevent persistent “backdoor” hemorrhage from
the right gastroepiploic and superior pancreaticoduodenal arteries and then proceed to the
proximal side of the erosion.
Provocative angiography We do not believe there is enough data to provide definitive guidelines to perform provocative
mesenteric angiography or pharmacoangiography. Furthermore, this technique is mainly used to
provoke lower GI bleeding, which is more challenging than UGIB. Indeed, contrary to lower GI
bleeding, almost all upper gastrointestinal bleeders have undergone endoscopy in an attempt to
identify, localize and treat the source of bleeding. Several prior studies have shown that empiric
embolization based on endoscopic findings, in the absence of contrast extravasation, can be
performed safely and successfully[25,35,36]. So the absence of angiographic extravasation is
less problematic at the level of the upper gastrointestinal tract and does not prevent from
embolizing the artery that supplies the bleeding site.
However, this technique can be applied in situations where conventional angiography is
nondiagnostic. The addition of pharmacological agents to standard angiographic protocols in
order to increase the diagnostic yield has been reported in case reports and small series.
Provocative mesenteric angiography is the use of thrombolytic, vasodilating and anticoagulation
medications to elicit active bleeding from a source that may have recently ceased hemorrhaging.
Unfortunately, the available literature on this topic is limited. This technique was first reported in
the literature in 1982[37]. Since then, our review of the literature yielded only seven small case
series and two case reports totaling 93 patients[37-45]. Koval et al[38] doubled the rate of
extravasations visualized by angiography from 32% to 65% with the introduction of
pharmacologic angiography. Malden et al[39] and Ryan et al[41] separately showed a provoked
bleeding rate of nearly 40% when previous angiograms had been normal with a minimal
complication rate. Although reasonably successful and without any reported major hemorrhagic
complications, provocative mesenteric angiography is not a commonly used examination. The
precise reasons for this are unknown but likely relate to fear of potential uncontrollable
hemorrhagic complications and lack of familiarity with this procedure by referring clinicians and
interventional radiologists. Both of these are likely a reflection of the sparse data supporting
provocative mesenteric angiography in the literature.
Basically, provocative angiography may increase the diagnostic ability when a normal
angiogram is encountered for nonvariceal UGIB. But several procedure-related factors may
affect the diagnostic yield of provocative studies; these include timing of the procedure, the type
and dosage of provocative medications and the expertise of the operators. The types of
pharmacological provocation reported in the literature have been variable[38-46]. Based on these
data, an idealized protocol could include intra-arterial tolazoline at a dose of 25 mg, intra-arterial
heparin at a dose targeted to double the patient’s baseline activated clotting time and intraarterial
urokinase in aliquots of 250000 U given over 15 min and monitored by diagnostic angiography.
Endpoints are either hemorrhage or a total of 1 000 000 U of urokinase over an interval of
approximately 1 h. However, it should be emphasized that the specific agents and their total doses in
literature are largely arbitrary. Currently, provocative angiography is rarely needed for the diagnosis of GI
bleeding and only limited reports for use in difficult and recurring nonvariceal UGIB have shown to be
beneficial[37,41]. We believe that further prospective studies are required to provide a better
understanding of optimal patient selection and optimal pharmacological provocation. Only with these
kinds of data can provocative GI bleeding studies be appropriately placed in a diagnostic algorithm for
evaluation of patients with GI hemorrhage of obscure origin.
Angiographic Interventions Over the past two decades, angiographic interventions have shifted from playing a purely
diagnostic role to being a major therapeutic option in the management of nonvariceal UGIB.
Transcatheter intervention to control GI bleeding takes two forms: the infusion of a
vasoconstricting medication and the mechanical occlusion of the arterial supply responsible for
the hemorrhage.
Intra-arterial vasopressin infusion Selective infusion of intraarterial vasoconstrictors was one of the first angiographic treatments
for GI bleeding. Vasopressin, a posterior pituitary hormone, elicits smooth muscle contraction in
the mesenteric bed, thereby decreasing the perfusion pressure to the bowel and potentially
resulting in thrombosis of the bleeding site. Vasopressin infusion is easy to perform, most often
by placing a 5F diagnostic catheter into the artery most suspected of bleeding[47]. Vasopressin is
then infused at a rate of 0.2 to 0.4 U/min until successful control of bleeding is observed on
angiography. Then, the mesenteric intraarterial infusion is continued for 12-48 h. Vasopressin
infusion has lost favor for two main reasons: necessary catheterization times can require several
days and, more importantly, the emergence of embolotherapy. For nonvariceal UGIB, the
offending arteries were easily accessible even with large and crude catheter systems and embolic
agents of the past. In addition, given the rich arterial collateral network and proximal site of
embolotherapy, ischemia was not thought to be problematic. Given that embolotherapy replaced
vasopressin infusion early in the treatment of UGIB, there is little recent data on the use of this
technique. In addition, much of the data includes treatment of variceal bleeding. A review of four
of the more recent studies consisting of 267 patients demonstrated an initial 70% to 80% success
rate. They observed approximately 20% rate of rehemorrhage with bleeding refractory to
infusion in up to 40% of patients[48-50]. Failures of vasopressin are thought to be due to the rich
collateral supply to the upper GI tract and the inability to treat potential collateral supply
pathways to the bleeding site, but this is unproven. Finally, the use of vasopressin in the
treatment of nonvariceal UGIB is empiric as there is no substantial data to support its use[51].
Transcatheter selective embolization Standard technique: Because of the high rebleeding rate with infusion therapy, other
angiographic interventions were developed to treat nonvariceal UGIB. As is true of most other
minimally invasive and image-guided interventions, embolotherapy has supplanted surgery in
most centers as the treatment of choice for endoscopy-refractory UGIB. This method is
associated with an initial bleeding control rate of 89%-98%. Clinical success rates range from
52%-98% with most reports showing success rates of 70%-80%[23,46,52,53]. The role of TAE
is to selectively reduce blood supply at the source of bleeding while maintaining enough
collateral blood flow to maintain intestinal viability. Typically, in cases of active hemorrhage
with extravasation of contrast, the bleeding vessel is identified by superselective catheterization
using a microcatheter and embolized with microcoils, particles or glue if arterial flow is not
blocked by the microcatheter (Figure 1). Superselection and embolization of short segments of
visceral arteries can be performed with newer advances in hydrophilic steerable wires,
microcatheters and embolic agents. Coaxial systems allow 2 to 3F catheters to pass through
larger primary catheters to allow access to distal arterial branches[52]. In general, bleeding in the
esophagus and fundus of the stomach is treated by embolization of the LGA (Figure 2). Bleeding
in the body and antrum of the stomach may be controlled by embolization of either the
gastroepiploic, right gastric or gastroduodenal arteries depending on the source of bleeding.
Choice of embolic agent: As is the case with microcatheters and guide wires, embolic agents
too have evolved over time. Many embolization agents have been used successfully: coils,
particulate material such as resorbable gelatin sponge, and nonresorbable polyvinyl alcohol
(PVA) or trisacryl gelatin particles. Liquids such as N-butyl 2-cyanoacrylate (NBCA) glue or
ethylene-vinyl alcohol copolymer (Onyx®, Micro Therapeutics, Inc., Irvine, CA, USA) are less
popularly used[25,46,52,54]. The choice of the best embolic agent is still debatable.
Embolotherapy in these emergency patients has to be fast, easy to perform and effective. Success
is achievable with different materials in experienced interventional radiologist’s hands. Embolic
agents have different constraints depending on the material used.
Coils alone inserted in the GDA or superselectively in the pancreaticoduodenal arteries have
been used with success by several investigators[55-59]. When used in the setting of UGIB, coils
are usually used to occlude or reduce flow into a major vessel, which can also be treated at a
more distal level with a particulate agent (usually gelatin sponge) to aid in hemostasis. The main
advantages of using coils are that they can be delivered in a very precise fashion and carry low
risk of infarction because of the preservation of the distal microvasculature. Coils and microcoils
of different size and length can be used (Figure 3). They may have thrombogenic fibers to
facilitate occlusion of the vessel and they may offer the option of detachability and retrievability.
The main drawback is that they are permanent and may preclude re-accessing the vessel in the future
should it prove necessary. Another disadvantage is that coil application is dependent upon vessel diameter
and intrinsic blood clotting. That is probably why Aina et al[35] and Loffroy et al[25] showed an
association between the use of coils alone and the incidence of bleeding recurrence, especially in patients
with coagulopathy. The advantages of use of PVA or gelatin sponge in association with coils when
choosing a strategy for this subgroup of patients cannot be over stressed.
Gelatin sponge is the main temporary embolic agent used worldwide (Figure 4). It has the
advantage that after resorption, flow will be restored weeks after embolization. Furthermore, it is
readily available, cheap and unlikely to cause ischemia. The disadvantages are that it requires
some time to prepare appropriate-sized particles and the pace of recanalization is unpredictable.
Lang[60] compared several embolic agents in a series of 57 patients. They reported that a high
rate of bleeding recurrence was observed when gelatin sponge was used alone. Similarly,
Encarnacion et al[7] achieved a low success rate (62%) in their series, which included mostly
patients embolized with gelatin sponge alone. These data confirm that the use of gelatin sponge
as the only embolic agent guarantees only short-term results and should probably be avoided.
Particles such as PVA particles and tris-acryl gelatin microspheres may be of advantage when a
flow-directed strategy is favorable, e.g. when diffuse tumor vasculariza
tion is to be excluded from the arterial supply (Figure 5). These agents have been used
successfully in treating gastrointestinal hemorrhage, usually through a microcatheter and at a site
distal to major vessels[60]. Only larger particles (> 500 µm) should be used to decrease the risk
of ischemia from normal tissue devascularization. [25,61-63]
Good results have also been reported with NBCA . Toyoda et al[63] reported that the time
required for TAE using NBCA was significantly lower than for TAE procedures that do not use
NBCA. This is important especially in cases of massive bleeding that require urgent hemostasis.
Indeed, the use of NBCA glue is particularly of interest in hemodynamically unstable patients
and in cases of underlying coagulopathy. A number of institutions have adopted selective
embolization using glue as the only embolic agent as the salvage treatment of choice in UGIB
cases. However, the use of NBCA glue requires training and considerable experience, given the
risk of bowel infarction and glue reflux into other vessels. Reflux of NBCA may also result in its
polymerization to the catheter tip (Figure 6). This bit of NBCA may then be stripped from the
catheter during catheter retraction, resulting in nontarget embolization. The use of a proper
technique, including prompt removal of the catheter after injection as well as aspiration of the
guide catheter after microcatheter removal, can significantly reduce this risk[62]. Another
drawback is the potential risk of bowel stenosis over the long-term. Lang[60] found a 25%
duodenal stenosis rate in a study of 28 patients that were followed up for at least 5 years after
embolization for bleeding duodenal ulcers, even if the link between glue embolization and duodenal
stenosis is difficult to evaluate. Onyx® seems to have great potential as a liquid embolic agent in
embolotherapy of acute arterial gastrointestinal bleeding. Lenhart et al[54] recently reported
their experience with the use of Onyx® in such a setting. Their study represents the first series to
date reporting results on arterial embolotherapy with Onyx® as an embolic agent in the
gastrointestinal tract. The success rate was high (81%) and the complication rate was almost nil.
Onyx® is a new liquid embolic agent composed of ethylene-vinyl alcohol copolymer dissolved
in dimethyl sulphoxide (DMSO), with emerging applications in neurovascular procedures,
predominantly embolization of cerebral aneurysms and arteriovenous malformations[64]. The main
advantages of Onyx® are its nonadhesive properties, high radiopacity and long solidification periods (Figure
7). These properties of Onyx® compared to acrylic glues make the embolization procedure more controllable
and predictable[65]. However, Onyx® has some disadvantageous characteristics. Firstly, DMSO can cause
severe vasospasm if injected rapidly. Secondly, DMSO is volatile and is excreted via respiration and sweat.
This has a typical smell not unlike that of diabetic ketoacidosis and may last a few days. The patient and ward
staff should be warned to expect this. Lastly, the use of Onyx® has cost implications as it is much more
expensive than alternative embolic materials and requires specific DMSO-compatible microcatheters. These
factors explain its restricted use in neuroradiology in most institutions around the world.
Finally, it is not clear if careful selection of the embolic agents according to the bleeding vessel may
play a role in a successful outcome. It would be worth comparing the different embolic agents for
arterial embolotherapy in the gastrointestinal tract in a prospective randomized multi-center trial.
However, data from the literature suggest that coils probably should not be used as the only embolic
agent but rather in association with gelatin sponge, particles or glue for the treatment of
gastroduodenal hemorrhage. Furthermore, surgical glue should probably be used more often,
especially in patients with coagulopathy, because it provides a better and faster hemostasis and does
not cause ischemia. Otherwise, the choice of embolic agent does not seem to affect clinical response
or recurrence rates.
Specific techniques of interest: The upper gastrointestinal tract contains a rich collateral blood
supply that often requires embolization of multiple arteries for successful outcomes. Careful
angiographic assessment of the collateral pathways prior to embolization is essential, especially
in patients with severe atherosclerotic occlusive disease or previous extensive upper
gastrointestinal surgery. If the bleeding is from a duodenal ulcer, the GDA needs to be
catheterized and embolized using the so-called sandwich technique: the catheter is pushed to the
origin of the RGEA and coils are introduced as the catheter is withdrawn to the proximal GDA.
Complete embolization of the GDA, which includes proximal and distal embolization and
exclusion of its two side branches, is the end point in this case (Figure 8A and B)[25,55]. A
selective superior mesenteric arteriogram is performed after embolization to ensure that no
collateral supply to the bleeding site is present. If extravasation is identified, superselective
catheterization of the inferior pancreaticoduodenal artery and the side branch responsible for the
collateral circulation is performed with the microcatheter. Embolization with microcoils of the
bleeding site is performed as distal as possible. This method can also be used at the level of the
SA for treatment of pseudoaneurysmal lesions[21]. As such, the embolization needs to take place
both distal and proximal to the lesion.
If no evidence of bleeding is found on pre-embolization arteriography, then empiric or blind
embolization is advised. Blind or empiric is defined as embolization without angiographic proof
of extravasation and is typically guided by endoscopic information regarding the location of the
bleeding vessel. Coils and gelatin sponge are then often used in such a situation (Figure 8).
Another useful maneuver in this scenario requires clips to be placed around the area of bleeding
during pre-embolization endoscopy. The clips remain in position for several hours and allow for
an educated guess of the location of the culprit vascular branch[56]. If no extravasation is seen
despite the injection of contrast, then the branches terminating to the clip are superselected using
microcatheter techniques and embolized. Arteriography at multiple projections is necessary at
this step to ensure the relation between the clip and the adjacent branches.
Blind embolization is controversial. Because massive bleeding is often intermittent, most groups
have adopted a policy to embolize on the basis of endoscopic findings even in situations where
no extravasation is seen angiographically[36]. In the independent series from Aina et al[35],
Loffroy et al[25] and Padia et al[36] there was no difference in outcome between patients who
underwent blind embolization and those who underwent embolization after a bleeding site had
been demonstrated angiographically. Other researchers have also advocated the practice of
endoscopy-directed blind embolization[57,58]. Based on the findings from the literature and our
own experience, we believe that blind embolization is appropriate. The GDA should be
embolized using the sandwich technique, in which both ends of the artery are filled with coils to
avoid retrograde bleeding from the superior mesenteric circulation. If there is suspicion that smaller
muscular branches terminating to a clip are the culprits, then those should be embolized with any of the
materials available.
PA in peripancreatic or perihepatic blood vessels as a complication of pancreatic pseudocysts or
in the setting of recent hepatobiliary tree instrumentation, respectively, may be responsible for
UGIB. Recently, TAE has generated considerable interest as the first-line therapeutic method for
PAs. The success rate is high, ranging from 62% to 100% in visceral PAs and the morbidity and
mortality rates are low[21]. Most investigators agree that coils are the most appropriate embolic
material[21,66]. However, the traditional technique for PA embolization includes isolating the
lesion by deploying coils in the parent artery, covering both sides of the PA neck to prevent
backbleeding via collaterals (sandwich technique)[21,66]. Embolization of PAs using a
combination of gelatin sponge and coils, NBCA and coils, coils alone or NBCA has also been
described[66,67]. The main drawback of these techniques is the compromised patency of the
parent vessel with potential ischemic complications. Modification of the embolization technique
can help preserve the patency of parent artery while achieving complete embolization.
Superselective arterial embolization is achieved by threeimensional coil-packing of the PA sac
using controlled, detachable microcoils placed in a concentric fashion (Figure 9). This
endovascular technique is generally used for the treatment of intracranial aneurysms[68], often
with the remodeling technique to avoid coil protrusion into the parent artery because of an
unfavorable neck-to-sac [69] ratio . When the PA neck is thin, balloon-remodeling is unnecessary.
However, this method has several potential limitations. The main technical drawback is that the
microcatheter must be placed in the PA sac. Considerable experience is required to pass through
the neck, which is typically slender in peripheral PAs. The other limitation concerns the number
of coils required for complete occlusion of the PA sac, especially those of large size, and
consequently the cost of the procedure. Compared to non-fibered coils, fibered coils have greater
occlusive power, allowing occlusion with a smaller number of coils. Controlled, detachable
fibered microcoils are now commercially available. Packing 80%-90% of the sac usually
provides complete sac exclusion while avoiding complications such as secondary rupture. Few
centers combine the use of detachable microcoils with an injection of Onyx® into the pseudo-
aneurysmal sac to reduce the amount of coils and the risk of over-packing[70]. The coil mesh has
proven to be very effective for capturing Onyx ® and facilitated complete occlusion of a
challenging lesion. However, a limitation to the selection of Onyx® for peripheral indications is
its relatively high cost compared with microcoils, as previously said. In addition, its use may add
to the complexity of embolization procedures because a balloon-assisted remodeling technique is
often necessary.
Conclusion

Nonvariceal UGIB remains a common and often serious clinical dilemma. The past two decades
have seen enormous advances in endovascular device development, including lower-profile
catheter systems and better embolic agents, and treatment of a wide variety of hemorrhagic
conditions. These all have made embolotherapy safer and more efficient and has led to its wider
acceptance. A combination of newer improved techniques, materials and embolic agents has seen
TAE replace surgery to become the gold standard for the treatment of lifethreatening UGIB
refractory to endoscopic hemostasis.
References 1. 1 Huang CS, Lichtenstein DR. Nonvariceal upper gastrointestinal bleeding.
Gastroenterol Clin North Am 2003; 32: 10�3-1078 2. 2 Rollhauser C, Fleischer DE. Nonvariceal upper gastrointestinal bleeding. Endoscopy
2004; 36: �2-�8 3. 3 Schoenberg MH. Surgical therapy for peptic ulcer and nonvariceal bleeding.
Langenbecks Arch Surg 2001; 386: 98-103 4. Defreyne L, De Schrijver I, Decruyenaere J, Van Maele G, Ceelen W, De Looze D,
Vanlangenhove P. Therapeutic decision-making in endoscopically unmanageable nonvariceal upper gastrointestinal hemorrhage. Cardiovasc Intervent Radiol 2008; 31: 897-90�
5. Rosch J, Dotter CT, Brown MJ. Selective arterial embolization. A new method for control of acute gastrointestinal bleeding. Radiology 1972; 102: 303-306
6. Funaki B. Endovascular intervention for the treatment of acute arterial gastrointestinal hemorrhage. Gastroenterol Clin North Am 2002; 31: 701-713
7. Encarnacion CE, Kadir S, Beam CA, Payne CS. Gastrointestinal bleeding: treatment with gastrointestinal arterial embolization. Radiology 1992; 183: �0�-�08
8. Lang EV, Picus D, Marx MV, Hicks ME. Massive arterial hemorrhage from the stomach and lower esophagus: impact of embolotherapy on survival. Radiology 1990; 177: 249-2�2
9. Ljungdahl M, Eriksson LG, Nyman R, Gustavsson S. Arterial embolisation in management of massive bleeding from gastric and duodenal ulcers. Eur J Surg 2002; 168: 384-390
10. Holme JB, Nielsen DT, Funch-Jensen P, Mortensen FV. Transcatheter arterial embolization in patients with bleeding duodenal ulcer: an alternative to surgery. Acta Radiol 2006; 47: 244-247
11. Laine L, Peterson WL. Bleeding peptic ulcer. N Engl J Med 1994; 331: 717-727 12. Langman MJ, Jensen DM, Watson DJ, Harper SE, Zhao PL, Quan H, Bolognese JA,
Simon TJ. Adverse upper gastrointestinal effects of rofecoxib compared with NSAIDs. JAMA 1999; 282: 1929-1933
13. Hunt RH, Harper S, Watson DJ, Yu C, Quan H, Lee M, Evans JK, Oxenius B. The gastrointestinal safety of the COX-2 selective inhibitor etoricoxib assessed by both endoscopy and analysis of upper gastrointestinal events. Am J Gastroenterol 2003; 98: 172�-1733
14. Mamdani M, Juurlink DN, Kopp A, Naglie G, Austin PC, Laupacis A. Gastrointestinal bleeding after the introduction of COX 2 inhibitors: ecological study. BMJ 2004; 328: 141�-1416
15. Llach J, Elizalde JI, Guevara MC, Pellise M, Castellot A, Gines A, Soria MT, Bordas JM, Pique JM. Endoscopic injection therapy in bleeding Mallory-Weiss syndrome: a randomized controlled trial. Gastrointest Endosc 2001; 54: 679-681
16. Huang SP, Wang HP, Lee YC, Lin CC, Yang CS, Wu MS, Lin JT. Endoscopic hemoclip placement and epinephrine injection for Mallory-Weiss syndrome with active bleeding. Gastrointest Endosc 2002; 55: 842-846
17. Morales P, Baum AE. Therapeutic Alternatives for the Mallory-Weiss Tear. Curr Treat Options Gastroenterol 2003; 6: 7�-83
18. Lee YT, Walmsley RS, Leong RW, Sung JJ. Dieulafoy’s lesion. Gastrointest Endosc 2003; 58: 236-243
19. Savides TJ, Jensen DM, Cohen J, Randall GM, Kovacs TO, Pelayo E, Cheng S, Jensen ME, Hsieh HY. Severe upper gastrointestinal tumor bleeding: endoscopic findings, treatment, and outcome. Endoscopy 1996; 28: 244-248
20. Chapman WC, Abecassis M, Jarnagin W, Mulvihill S, Strasberg SM. Bile duct injuries 12 years after the introduction of laparoscopic cholecystectomy. J Gastrointest Surg 2003; 7: 412-416
21. Loffroy R, Guiu B, Cercueil JP, Lepage C, Cheynel N, Steinmetz E, Ricolfi F, Krause D. Transcatheter arterial embolization of splenic artery aneurysms and pseudoaneurysms: shortand long-term results. Ann Vasc Surg 2008; 22: 618-626
22. Cappell MS, Abdullah M. Management of gastrointestinal bleeding induced by gastrointestinal endoscopy. Gastroenterol Clin North Am 2000; 29: 12�-167, vi-vii
23. Frisoli JK, Sze DY, Kee S. Transcatheter embolization for the treatment of upper gastrointestinal bleeding. Tech Vasc Interv Radiol 2004; 7: 136-142
24. Kadir S, Lundell C, Saeed M. Celiac, superior, and inferior mesenteric arteries. In: Kadir S, editor. Atlas of normal and variant angiography anatomy . Philadelphia: WB Saunders, 1991: 297-308
25. Loffroy R, Guiu B, D’Athis P, Mezzetta L, Gagnaire A, Jouve JL, Ortega-Deballon P , Cheynel N, Cercueil JP , Krause D. Arterial embolotherapy for endoscopically unmanageable acute gastroduodenal hemorrhage: predictors of early rebleeding. Clin Gastroenterol Hepatol 2009; 7: �1�-�23
26. Porter DH, Kim D. Angiographic intervention in upper gastrointestinal bleeding. In: Taylor MB, Gollan JL, Steer ML, Wolfe MM, editors. Gastrointestinal emergencies. Baltimore: Williams & Wilkins, 1997: 63-180
27. Walsh RM, Anain P, Geisinger M, Vogt D, Mayes J, Grundfest-Broniatowski S, Henderson JM. Role of angiography and embolization for massive gastroduodenal hemorrhage. J Gastrointest Surg 1999; 3: 61-6�; discussion 66
28. Smith R, Copely DJ, Bolen FH. 99mTc RBC scintigraphy: correlation of gastrointestinal bleeding rates with scintigraphic findings. AJR Am J Roentgenol 1987; 148: 869-874
29. Gunderman R, Leef J, Ong K, Reba R, Metz C. Scintigraphic screening prior to visceral arteriography in acute lower gastrointestinal bleeding. J Nucl Med 1998; 39: 1081-1083
30. Lo SK. Capsule endoscopy in the diagnosis and management of inflammatory bowel disease. Gastrointest Endosc Clin N Am 2004; 14: 179-193
31. Kovacs TO. Small Bowel Bleeding. Curr Treat Options Gastroenterol 200�; 8: 31-38 32. Defreyne L, Vanlangenhove P, Decruyenaere J, Van Maele G, De Vos M, Troisi R,
Pattyn P. Outcome of acute nonvariceal gastrointestinal haemorrhage after nontherapeutic arteriography compared with embolization. Eur Radiol 2003; 13: 2604-2614
33. Whitaker SC, Gregson RH. The role of angiography in the investigation of acute or chronic gastrointestinal haemorrhage. Clin Radiol 1993; 47: 382-388
34. Miller M, Smith TP. Angiographic diagnosis and endovascular management of nonvariceal gastrointestinal hemorrhage. Gastroenterol Clin North Am 200�; 34: 73�-7�23�
35. Aina R, Oliva VL, Therasse E, Perreault P, Bui BT, Dufresne MP, Soulez G. Arterial embolotherapy for upper gastrointestinal hemorrhage: outcome assessment. J Vasc Interv Radiol 2001; 12: 19�-200
36. Padia SA, Geisinger MA, Newman JS, Pierce G, Obuchowski NA, Sands MJ. Effectiveness of coil embolization in angiographically detectable versus non-detectable sources of upper gastrointestinal hemorrhage. J Vasc Interv Radiol 2009; 20: 461-466
36. Rosch J, Keller FS, Wawrukiewicz AS, Krippaehne WW, Dotter CT. Pharmacoangiography in the diagnosis of recurrent massive lower gastrointestinal bleeding. Radiology 1982; 145: 61�-619
37. Koval G, Benner KG, Ro sch J, Kozak BE. Aggressive angiographic diagnosis in acute lower gastrointestinal hemorrhage. Dig Dis Sci 1987; 32: 248-2�3
38. Malden ES, Hicks ME, Royal HD, Aliperti G, Allen BT, Picus D. Recurrent gastrointestinal bleeding: use of thrombolysis with anticoagulation in diagnosis. Radiology 1998; 207: 147-1�1
39. Bloomfeld RS, Smith TP, Schneider AM, Rockey DC. Provocative angiography in patients with gastrointestinal hemorrhage of obscure origin. Am J Gastroenterol 2000; 95: 2807-2812
40. Ryan JM, Key SM, Dumbleton SA, Smith TP. Nonlocalized lower gastrointestinal bleeding: provocative bleeding studies with intraarterial tPA, heparin, and tolazoline. J Vasc Interv Radiol 2001; 12: 1273-1277
41. Widlus DM, Salis AI. Reteplase provocative visceral arteriography. J Clin Gastroenterol 2007; 41: 830-833
42. Johnston C, Tuite D, Pritchard R, Reynolds J, McEniff N, Ryan JM. Use of provocative angiography to localize site in recurrent gastrointestinal bleeding. Cardiovasc Intervent Radiol 2007; 30: 1042-1046
43. Shetzline MA, Suhocki P, Dash R, Rockey DC. Provocative angiography in obscure gastrointestinal bleeding. South Med J 2000; 93: 120�-1208
44. Kim CY, Suhocki PV, Miller MJ, Khan M, Janus G, Smith TP. Provocative mesenteric angiography for lower gastrointestinal hemorrhage: results from a single-institution study. J Vasc Interv Radiol 2010; 21: 477-483
45. Burke SJ, Golzarian J, Weldon D, Sun S. Nonvariceal upper gastrointestinal bleeding. Eur Radiol 2007; 17: 1714-1726
46. Barr JW, Lakin RC, Ro sch J. Vasopressin and hepatic artery. Effect of selective celiac infusion of vasopressin on the hepatic artery flow. Invest Radiol 197�; 10: 200-20�
47. Sherman LM, Shenoy SS, Cerra FB. Selective intra-arterial vasopressin: clinical efficacy and complications. Ann Surg 1979; 189: 298-302
48. Clark RA, Colley DP, Eggers FM. Acute arterial gastrointestinal hemorrhage: efficacy of transcatheter control. AJR Am J Roentgenol 1981; 136: 118�-1189
49. Eckstein MR, Kelemouridis V, Athanasoulis CA, Waltman AC, Feldman L, van Breda A. Gastric bleeding: therapy with intraarterial vasopressin and transcatheter embolization. Radiology 1984; 152: 643-646
50. Stump DL, Hardin TC. The use of vasopressin in the treatment of upper gastrointestinal haemorrhage. Drugs 1990; 39: 38-3
51. Loffroy R, Rao P, Ota S, De Lin M, Kwak BK, Geschwind JF. Embolization of acute nonvariceal upper gastrointestinal hemorrhage resistant to endoscopic treatment: results and predictors of recurrent bleeding. Cardiovasc Intervent Radiol 2010; 33: 1088-1100
52. Loffroy R, Guiu B, Mezzetta L, Minello A, Michiels C, Jouve JL, Cheynel N, Rat P, Cercueil JP, Krause D. Shortand longterm results of transcatheter embolization for
massive arterial hemorrhage from gastroduodenal ulcers not controlled by endoscopic hemostasis. Can J Gastroenterol 2009; 23: 11�-120
53. Lenhart M, Paetzel C, Sackmann M, Schneider H, Jung EM, Schreyer AG, Feuerbach S, Zorger N. Superselective arterial embolisation with a liquid polyvinyl alcohol copolymer in patients with acute gastrointestinal haemorrhage. Eur Radiol 2010; 20: 1994-1999
54. Loffroy R, Guiu B, Cercueil JP, Lepage C, Latournerie M, Hillon P, Rat P, Ricolfi F, Krause D. Refractory bleeding from gastroduodenal ulcers: arterial embolization in highoperative-risk patients. J Clin Gastroenterol 2008; 42: 361-367 Eriksson LG, Sundbom M, Gustavsson S, Nyman R. Endoscopic marking with a metallic clip facilitates transcatheter arterial embolization in upper peptic ulcer bleeding. J Vasc Interv Radiol 2006; 17: 9�9-964
55. Toyoda H, Nakano S, Takeda I, Kumada T, Sugiyama K, Osada T, Kiriyama S, Suga T. Transcatheter arterial embolization for massive bleeding from duodenal ulcers not controlled by endoscopic hemostasis. Endoscopy 199�; 27: 304-307
56. De Wispelaere JF, De Ronde T, Trigaux JP, de Cannie re L, De Geeter T. Duodenal ulcer hemorrhage treated by embolization: results in 28 patients. Acta Gastroenterol Belg 2002; 65: 6-11
57. van Vugt R, Bosscha K, van Munster IP, de Jager CP, Rutten MJ. Embolization as treatment of choice for bleeding peptic ulcers in high-risk patients. Dig Surg 2009; 26: 37-42
58. Lang EK. Transcatheter embolization in management of hemorrhage from duodenal ulcer: long-term results and complications. Radiology 1992; 182: 703-707
59. Park JH, Kim HC, Chung JW, Jae HJ, Park JH. Transcatheter arterial embolization of arterial esophageal bleeding with the use of N-butyl cyanoacrylate. Korean J Radiol 2009; 10: 361-36�
60. Lee CW, Liu KL, Wang HP, Chen SJ, Tsang YM, Liu HM. Transcatheter arterial embolization of acute upper gastrointestinal tract bleeding with N-butyl-2-cyanoacrylate. J Vasc Interv Radiol 2007; 18: 209-216
63. Toyoda H, Nakano S, Kumada T, Takeda I, Sugiyama K, Osada T, Kiriyama S. Estimation of usefulness of N-butyl2-cyanoacrylate-lipiodol mixture in transcatheter arterial embolization for urgent control of life-threatening massive bleeding from gastric or duodenal ulcer. J Gastroenterol Hepatol 1996; 11: 2�2-2�8
64. Panagiotopoulos V, Gizewski E, Asgari S, Regel J, Forsting M, Wanke I. Embolization of intracranial arteriovenous malformations with ethylene-vinyl alcohol copolymer (Onyx). AJNR Am J Neuroradiol 2009; 30: 99-106
65. Loffroy R, Guiu B, Cercueil JP, Krause D. Endovascular therapeutic embolisation: an overview of occluding agents and their effects on embolised tissues. Curr Vasc Pharmacol 2009; 7: 2�0-263
66. Lau KY, Wong TP, Wong WW, Chan JK, Kan WK, Chan YF, Lee AS. Transcatheter embolisation of visceral pseudoaneurysms--technical difficulties and modification of embolisation technique. Eur J Vasc Endovasc Surg 200�; 30: 133-136
67. Tokuda T, Tanigawa N, Shomura Y, Kariya S, Kojima H, Komemushi A, Shiraishi T, Sawada S. Transcatheter embolization for peripheral pseudoaneurysms with n-butyl cyanoacrylate. Minim Invasive Ther Allied Technol 2009; 18: 361-36� 68 Lubicz B, Leclerc X, Gauvrit JY , Lejeune JP , Pruvo JP . Threedimensional packing with complex
orbit coils for the endovascular treatment of intracranial aneurysms. AJNR Am J Neuroradiol 200�; 26: 1342-1348
68. Moret J, Cognard C, Weill A, Castaings L, Rey A. [Reconstruction technic in the treatment of wide-neck intracranial aneurysms. Long-term angiographic and clinical results. Apropos of �6 cases]. J Neuroradiol 1997; 24: 30-44
69. Vanninen RL, Manninen I. Onyx, a new liquid embolic material for peripheral interventions: preliminary experience in aneurysm, pseudoaneurysm, and pulmonary arteriovenous malformation embolization. Cardiovasc Intervent Radiol 2007; 30: 196-200
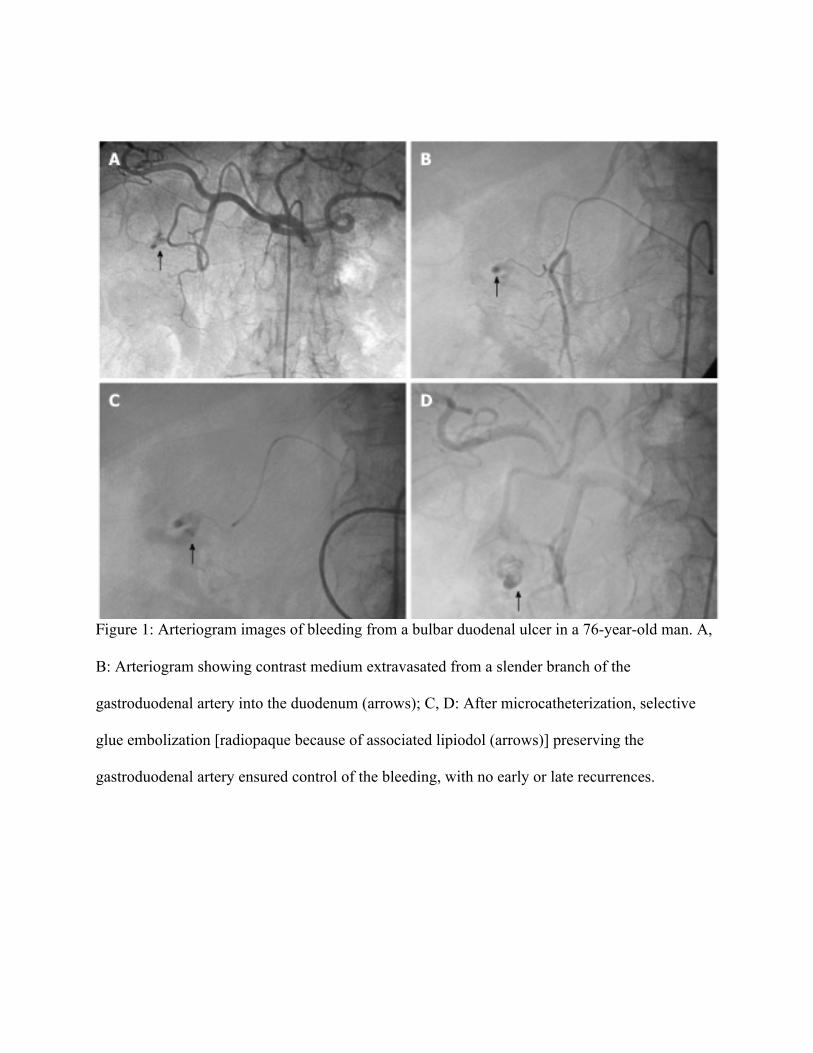
Figure 1: Arteriogram images of bleeding from a bulbar duodenal ulcer in a 76-year-old man. A,
B: Arteriogram showing contrast medium extravasated from a slender branch of the
gastroduodenal artery into the duodenum (arrows); C, D: After microcatheterization, selective
glue embolization [radiopaque because of associated lipiodol (arrows)] preserving the
gastroduodenal artery ensured control of the bleeding, with no early or late recurrences.

Figure 2: Bleeding dieulafoy lesion in an 87-year-old man. A, B: Extravasation of contrast
medium from the left gastric artery at the celiac trunk and superselective angiography indicates
continuing bleeding (arrows); C: After arterial microcatheterization, bleeding was controlled
after embolization of the left gastric artery using a Glubran/Lipidol mixture (1:3) (arrows).
Figure 3: Detachable metallic coil. This is a vessel-blocking agent which is positioned at the
target site, as opposed to released in the bloodstream.

Figure 4: Preparation of gelatin particles of various sizes by manually cutting gelatin sheets.
When the fundamental principles of embolization are scrupulously followed, absorbable agents
for temporary embolization are effective, safe and cost-effective.

Figure 5: Tris-acryl gelatin microspheres of 500-700 microns in size. Microspheres have two
major advantages: they can be calibrated to ensure accurate targeting and they do not block the
embolization catheter.

Figure 6: Glubran 2®: N-butyl 2-cyanoacrylate + metacrylosulpholane. The main advantage of
cyanoacrylate glue is the lasting nature of the vascular occlusion, compared with particles.

Figure 7: Gelling solution. The only commercially available gelling solution (Onyx®) is
composed of ethylene-vinyl-alcohol copolymer suspended in dimethyl-sulphoxide, with tantalum
to ensure visibility by fluoroscopy.
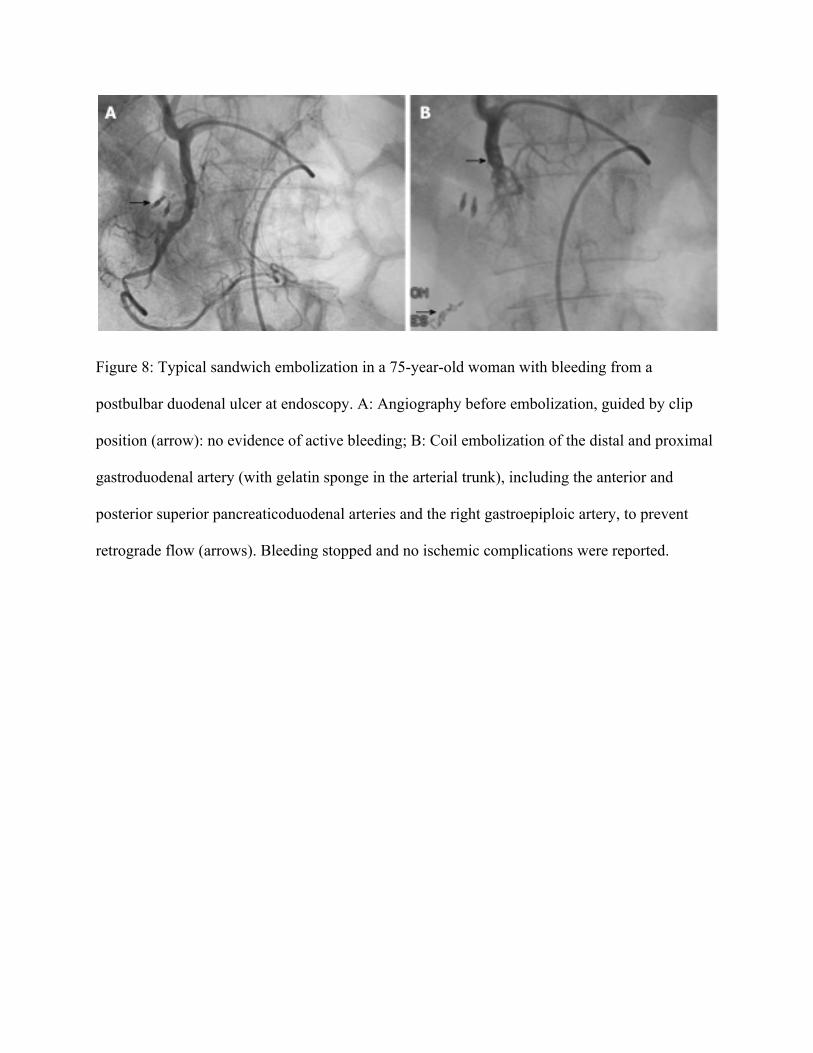
Figure 8: Typical sandwich embolization in a 75-year-old woman with bleeding from a
postbulbar duodenal ulcer at endoscopy. A: Angiography before embolization, guided by clip
position (arrow): no evidence of active bleeding; B: Coil embolization of the distal and proximal
gastroduodenal artery (with gelatin sponge in the arterial trunk), including the anterior and
posterior superior pancreaticoduodenal arteries and the right gastroepiploic artery, to prevent
retrograde flow (arrows). Bleeding stopped and no ischemic complications were reported.
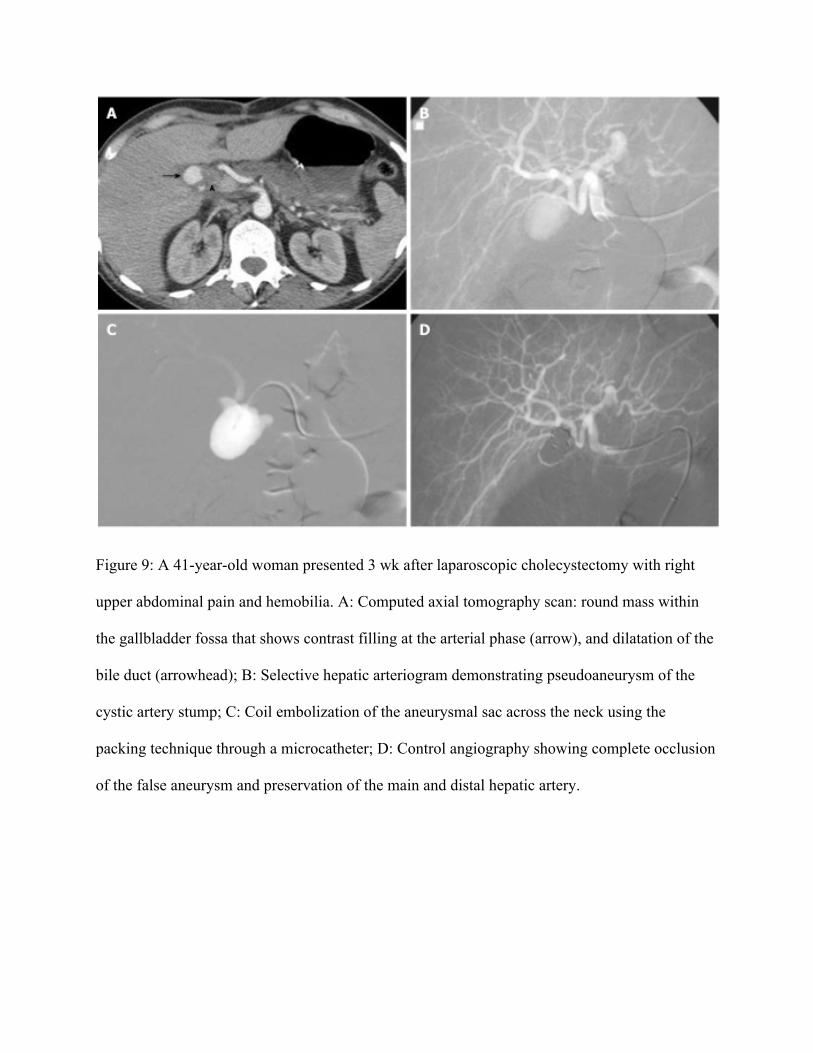
Figure 9: A 41-year-old woman presented 3 wk after laparoscopic cholecystectomy with right
upper abdominal pain and hemobilia. A: Computed axial tomography scan: round mass within
the gallbladder fossa that shows contrast filling at the arterial phase (arrow), and dilatation of the
bile duct (arrowhead); B: Selective hepatic arteriogram demonstrating pseudoaneurysm of the
cystic artery stump; C: Coil embolization of the aneurysmal sac across the neck using the
packing technique through a microcatheter; D: Control angiography showing complete occlusion
of the false aneurysm and preservation of the main and distal hepatic artery.