recent advances in the treatment of alzheimer's disease
TRANSCRIPT

Dr. Mohit KulmiPostgraduate resident
Department of Pharmacology
SAMC & PGI, Indore

RECENT ADVANCES IN THE PHARMACOTHERAPY OF ALZHEIMER’S DISEASE

INTRODUCTION & BRIEF HISTORY

“Alzheimer’s disease (AD) is the commonest progressive, dementing neuro-degenerative disease in the elderly characterised by memory loss, language difficulty and confusion..

▪Alois Alzheimer, a German physician, is credited with being the first to describe AD.
▪In 1906, Dr. Alzheimer observed a patient, Auguste Deter, in a local asylum who exhibited strange behaviours. He followed her care and noted her memory loss, language difficulty and confusion.
▪ After her death at the age of 51, he examined her brain tissue. The slides showed what are now known as plaques and tangles.
▪ In 1911, Doctors were using Dr. Alzheimer’s research to base diagnosis.
▪ In the 1960’s British pathologists determined that AD was not a rare disease of the young but rather what had been termed “senility.”
▪ In the 1990’s researchers identified that the beta amyloid protein was a factor in AD.

EPIDEMIOLOGY ▪ MC cause of dementia, > 65yr.
▪ Risk at the age of 80 years is around 15 to 20%.
▪ About 7.7 million new cases of dementia each year. A new case detected in every 4 seconds somewhere in world.

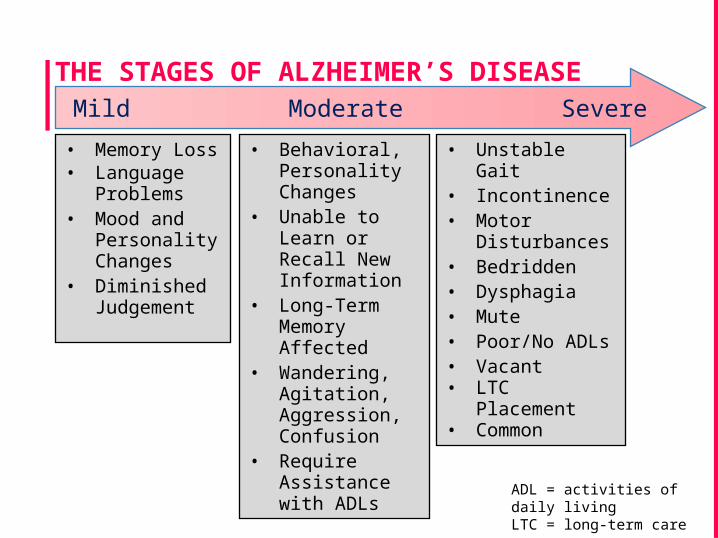
THE STAGES OF ALZHEIMER’S DISEASEMild Moderate Severe
• Memory Loss• Language
Problems• Mood and
Personality Changes
• Diminished Judgement
• Behavioral, Personality Changes
• Unable to Learn or Recall New Information
• Long-Term Memory Affected
• Wandering, Agitation, Aggression, Confusion
• Require Assistance with ADLs
• Unstable Gait• Incontinence• Motor
Disturbances• Bedridden• Dysphagia• Mute• Poor/No ADLs• Vacant• LTC Placement
• Common
ADL = activities of daily living LTC = long-term care
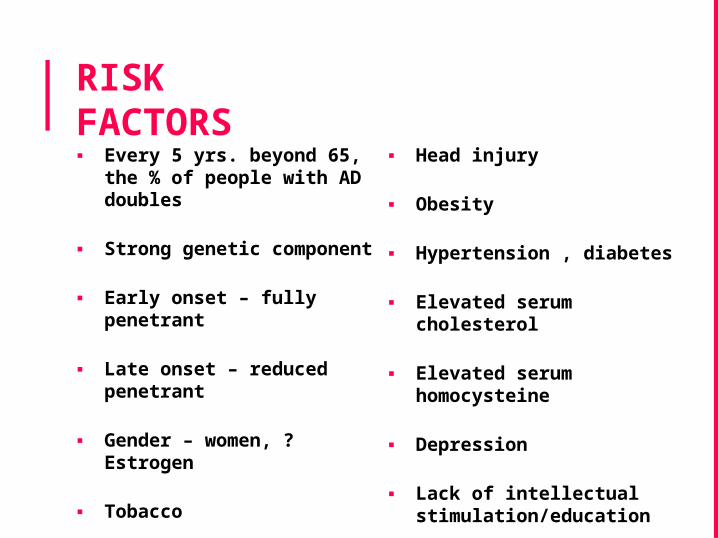
RISK FACTORS▪ Every 5 yrs. beyond 65,
the % of people with AD doubles
▪ Strong genetic component
▪ Early onset – fully penetrant
▪ Late onset – reduced penetrant
▪ Gender – women, ? Estrogen
▪ Tobacco
▪ Head injury
▪ Obesity
▪ Hypertension , diabetes
▪ Elevated serum cholesterol
▪ Elevated serum homocysteine
▪ Depression
▪ Lack of intellectual stimulation/education

PROTECTIVE FACTORS▪ Physical activity
▪ Caffeine consumption
▪ Antioxidants – VITAMIN C, E, B6 and B12
▪ Folate
▪ Omega 3 fatty acid intake
▪ Speaking > 2 languages

PATHOGENESIS AND PATHOPHYSIOLOGYAD is characterized by generalized cerebral cortical atrophy, neuronal loss, widespread cortical neuritic plaques and neurofibrillary tangles.Following mechanisms have been attributed for the development of Alzheimer’s dementia:▪ Amyloid cascade theory▪ Cholinergic hypothesis▪ Excitotoxicity▪ Genetic factors
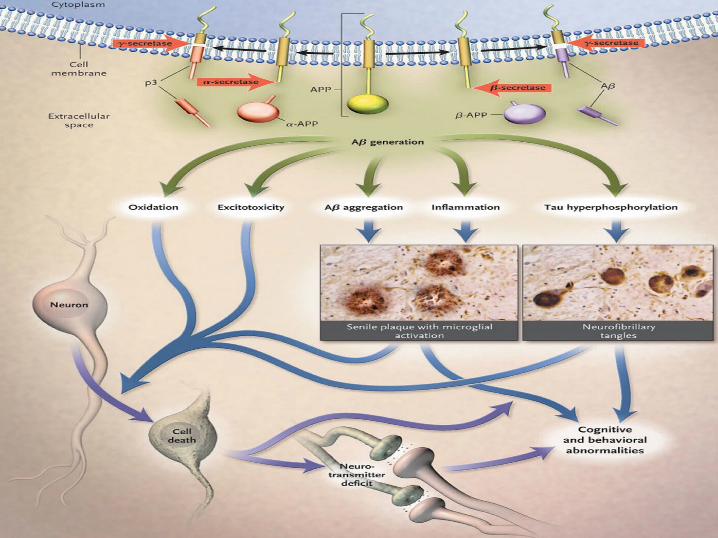
AMYLOID CASCADE THEORY▪ Alzheimer’s disease begins with the abnormal
build-up of an amyloid protein in the brain from APP (amyloid precursor protein).
▪ APP is normally found in the cell membranes of neurons and normally metabolised by a protease enzyme α-secretase.
▪ In AD, the metabolism of APP is altered by two other enzymes β and γ-secretase and is called β amyloid (Aβ).

▪ Amyloid-β is originated by the alternative cleavage of the amyloid precursor protein (APP) into smaller peptides (Aβ1-40 and Aβ1-42) by enzymes β and γ-secretase.
▪ Aβ1-42 is more prone to form insoluble aggregates (and therefore more toxic) than Aβ1-40.
▪ Once Aβ is formed, it accumulates into insoluble sheets (called β-pleated sheets).

▪ Ageing, seems to affect the balance between production and clearance of toxic Aβ peptides.
▪ These deposits are neurotoxic and activate inflammatory reaction resulting in the formation of senile or neuritic plaque.
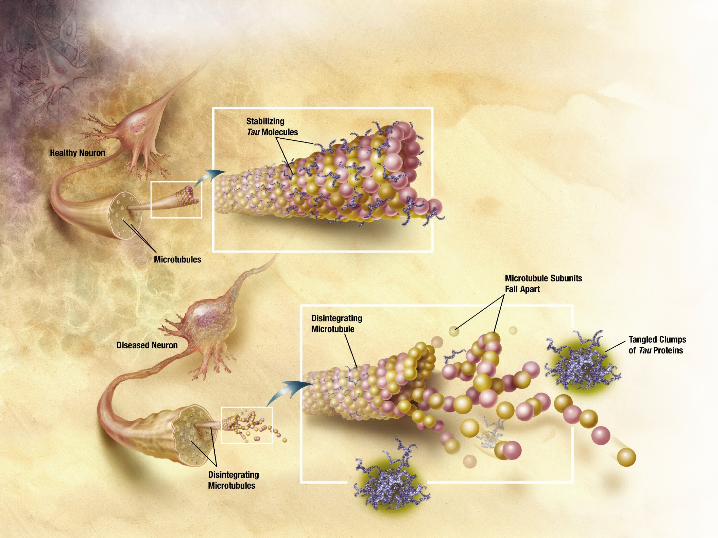
▪ This is accompanied by hyperphosphorylation of tau protein, supporting the microtubules.

▪ Hyperphosphorylated Tau aggregates into oligomers to form NFTs.
▪ Several protein kinases are involved in this process, namely glycogen synthase kinase-3 beta (GSK3β).
▪ GSK-3β, the most important Tau kinase in neurons, is overactive in AD

• Amyloid precursor protein (APP) is a membrane protein
• Sits in the membrane and extends outward.
• It is thought to be important for neuronal growth, survival, and repair
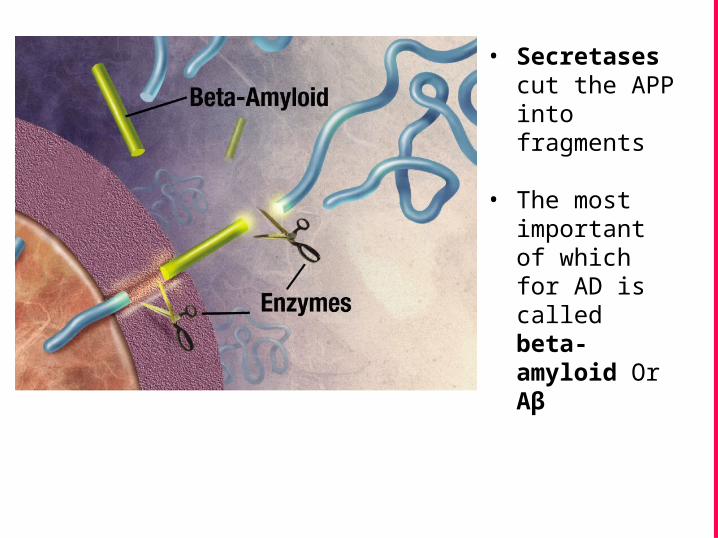
• Secretases cut the APP into fragments
• The most important of which for AD is called beta-amyloid Or Aβ

▪ Beta-amyloid is “sticky”
▪ The fragments cling together along with other material outside of the cell
▪ Forms thePlaques seen in the AD brain
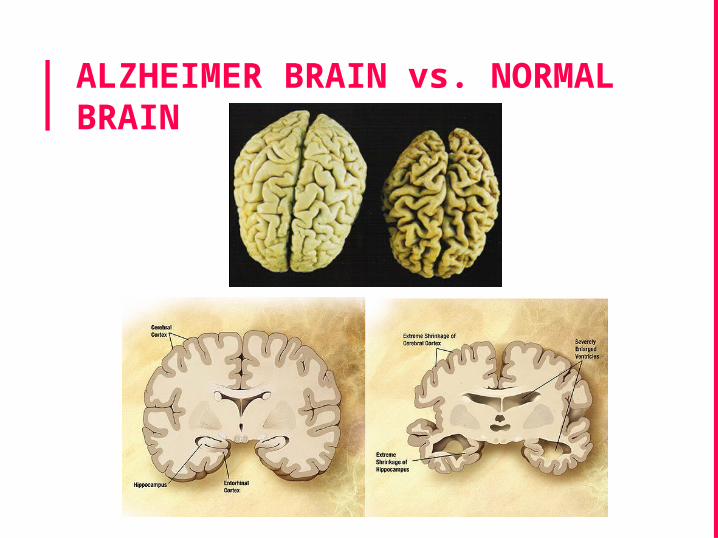
ALZHEIMER BRAIN vs. NORMAL BRAIN

CHOLINERGIC HYPOTHESIS▪ Levels of acetylcholine, noradrenaline,
serotonin, γ-aminobutyric acid (GABA), glutamate, somatostatin, neuropeptide Y, and substance P have all been documented to be reduced in the brains of AD patients.
▪ Reductions in acetylcholine and choline acetyltransferase are the most profound.
▪ Neuronal loss in the basal forebrain, which is the major region from which cholinergic projections originate.

EXCITOTOXICITY
▪ Excessive release of glutamate into the synapses.
▪ Excessive influx of calcium into the cells leading to cell death called excitotoxicity.
▪ Also lead to excessive production of Aβ and tau phosphorylation.

PHARMACOTHERAPYDRUGS FOR THE TREATMENT OF
ALZHEIMER’S

CHOLINESTERASE INHIBITORS▪ Tacrine (1993)
▪ Donepezil (1996)
▪ Rivastigmine (2000) and
▪ Galantamine (2001)

▪ Tacrine: It is the first centrally acting anti-ChE to be introduced for AD.
▪ In clinical trials tacrine produced significant improvement in memory, attention, praxis, reason and language.
▪ Frequent side effects and hepatotoxicity have restricted its use.
▪ Donepezil: This is a cerebroselective and reversible anti-AChE drug.
▪ Because of long t½ (~70 hr), donepezil is administered once daily at bed time; a distinct advantage over rivastigmine and galantamine which need twice daily dosing. Moreover, it can be used even in relatively severe case of AD.
▪ Donepezil is generally well tolerated and is not hepatotoxic.
▪ Rivastigmine: This carbamate derivative of physostigmine inhibits both AChE and BuChE.
▪ The carbamyl residue introduced by rivastigmine into AChE molecule dissociates slowly resulting in inhibition of cerebral AChE for upto 10 hours despite the 2 hr plasma t½ of the drug.
▪ Galantamine: It is a natural alkaloid which selectively inhibits cerebral AChE and has some direct agonistic action on nicotinic receptors as well.

▪ Memantine: It appears to restore the function of damaged nerve cells and reduce abnormal excitatory signals by the modulation of the NMDA receptor activity.
▪ It is indicated in moderate-to-severe AD, either to replace anti-AChEs or to supplement them.
▪ Piracetam : This cyclic GABA derivative has no GABA like activity. It selectively improves efficiency of higher telencephalic neurons.
▪ Pyritinol (Pyrithioxine) : It consists of two pyridoxine molecules joined through a disulfide bridge, but has no vit. B6 activity.
▪ It is claimed to activate cerebral metabolism by selectively increasing glucose transport across blood-brain barrier and improving regional blood flow in ischaemic brain areas.
▪ Dihydroergotoxine : It is a semisynthetic ergot alkaloid having α adrenergic blocking property; claimed to increase cerebral blood flow selectively.
▪ Citicoline: It is a compound derived from choline and cytidine, that is involved in biosynthesis of lecithin.
▪ Citicoline is believed to improve cerebral function by increasing blood flow to the brain and enhancing cerebral metabolism.
▪ Ginkgo biloba: The dried extract of this Chinese plant contains a mixture of ginkgoflavon glycosides, which have PAF antagonistic action.
▪ Since PAF has been implicated in cerebral thrombosis and infarcts, it is professed that G. biloba will prevent cerebral impairment in cerebrovascular insufficiency.

▪ Piribedil: It is a dopaminergic agonist claimed to improve memory, concentration, vigilance, giddiness and tinnitus in the elderly due to circulatory insufficiency.

RECENT ADVANCES

CLASSIFICATION
Cholinesterase inhibitor Aβ-TARGETING
STRATEGIES- β-secretase inhibitors γ-secretase
inhibitors/modulators α-secretase
activators/modulators Aβ-aggregation inhibitors M1 muscarinic agonists Aβ-degrading enzymes Apolipoprotein E (ApoE) Drugs influencing Aβ BBB
transport Immunotherapy
Drug development based on the metals hypothesis
HMG-CoA reductase inhibitors
MAO inhibitors Treatments based on tau
pathology Non-steroidal
antiinflammatory drugs (NSAIDs)
Estrogens, Nicotine, Melatonin
Cell transplantation and gene therapy
Docosahexaenoic acid (DHA), Clioquinol, Resveratrol
Vaccines

CHOLINESTERASE INHIBITOR
▪Phenserine: Phenserin treatments increased cognition and regional cerebral metabolic rate for glucose in AD patients.
▪Dimebon: A cholinesterase inhibitor and also a NMDA-antagonist, showed improved cognitive and self-service functions while diminishing the psychopathic symptoms in AD patients.
▪Huperzine A: A Chinese herb with reversibly and selectively acetylcholinesterase inhibition activity.

▪Ladostigil : A multimodal drug, combined neuroprotective effects with monoamine oxidase (MAO) -A and -B and cholinesterase inhibitory activities in a single molecule, was tested and now in Phase II clinical trial.
▪PMS777: A new cholinesterase inhibitor with anti-PAF activity is also in clinical trial
Aβ-TARGETING STRATEGIES
β-SECRETASE INHIBITORS▪ BACE (β- site APP cleaving enzyme): Lateral
ventricular injection of this inhibitor led to a significant dose- and time-dependent lowering of brain Aβ40 and Aβ42, a robust decreased sAPPβ and an increased sAPPα secretion.
▪ KMI-429: Injection of this inhibitor into the hippocampus of APP transgenic mice reduced Aβ production.
▪ GSK188909: Oral administration of this non-peptidic BACE1 inhibitor results in a significant reduction in the level of Aβ40 and Aβ42 in the brain of transgenic mice.

γ-SECRETASE INHIBITORS
▪ BMS-299897 ▪ MRK-560. ▪ LY450139 dehydrate
α-SECRETASE ACTIVATORS/MODULATORS
▪ Since α-secretase and β-secretase compete for the same substrate of APP, upregulation of α-secretase activity may decrease the amount of APP available for β-secretase, and thus decrease Aβ secretion and have therapeutic potential.

▪ Many studies had indicated that members of the adamalysin family of proteins ADAM (A Disintegrin And Metalloproteinase) mainly ADAM10, ADAM 17 and ADAM 9, fulfill some of the criteria required of α-secretase.
▪ Deprenyl: A neuroprotective agent used to slow AD progress, was shown to increase α-secretase activity by promoting ADAM10 activity.

Aβ-aggregation inhibitor▪ iAβ5p: This is the first drug was a β-sheet
breaker, which showed that intra hippocampal injection of it resulted in improved spatial memory and decreased amyloid plaque deposits.
▪ Tramiprosate: It is a compound that binds to soluble Aβ and inhibits the formation of neurotoxic aggregates that lead to amyloid plaque deposition in the brain.

M1 MUSCARINIC AGONISTSM1 muscarinic receptors play a role in an apparent linkage of three major hallmarks of AD: Aβ peptide; tau hyperphosphorylation and loss of cholinergic function.
▪ Talsaclidine: It is a functionally selective muscarinic M1 agonist that stimulates non-amyloidogenic α-secretase processing in vitro.
▪ Treatment with talsaclidine decreased CSF Aβ about 20% as compared with the baseline, suggesting its therapeutic potential.
▪ AF102B and AF267B: On clinical trial.

Aβ-DEGRADING ENZYMES▪ Neprilysin (NEP),
▪ Insulin degrading enzyme (IDE),
▪ Plasmin,
▪ Endothelin converting enzyme (ECE) 1
▪ Angiotensin-converting enzyme.
▪ Imatinib: A tyrosine kinase inhibitor, cause increase of NEP protein, mRNA levels, and activity.
▪ Valproic acid: A widely used drug in the treatment of epilepsy, was capable of up-regulating NEP expression, seen in experimental rats.
▪ Estrogen and green tea all could increase NEP activity and suggest their potential in AD treatment but there is a long way before their final clinical application.

▪ Apolipoprotein E (ApoE) promotes Aβ clearance
▪ The ApoE activates microglia and/or astrocyte to degrade Aβ. It decreased brain amyloid plaque burden and improved behaviour functions in AD transgenic mice.
▪ Bexarotene: Is a nuclear receptor modulator and ApoE activator.
APOLIPOPROTEIN E (ApoE)
Aβ BLOOD–BRAIN BARRIER TRANSPORT▪ The receptor for advanced glycation end
products (RAGE) resides in the blood vessel wall cells and transport Aβ across the blood brain barrier from systemic circulation to facilitate their accumulation in brain.
▪ In contrast to RAGE, low-density lipoprotein receptor-related protein-1 (LRP-1) mediates transport of Aβ peptide out of brain.
▪ Thus inhibition of RAGE and/or activation of LRP-1 may be a therapeutic target for AD, but there are no clinical data available at present.

IMMUNOTHERAPY
▪ Passive immunotherapy in AD patients with repeated intravenous administration of human immunoglobulin against Aβ peptide resulted in stopped cognitive decline and slight improvement in functional scores.
▪ Bapineuzumab: It shows decreased total and phosphorylated tau levels in CSF without affecting Aβ level.
▪ LY2062430 and AN1792A : On Phase I and II clinical trials.

DRUGS DEVELOPMENT BASED ON THE METALS HYPOTHESIS:▪ There is increasing evidence that metal (mainly
Cu, Zn and Fe) metabolism is involved in the major pathophysiological events of AD: APP processing and tau hyperphosphorylation.
▪ Several chelators of Zn/Cu have been shown to inhibit Aβ aggregation in vitro and in vivo.
▪ A phase II clinical trial with clioquinol, a metal-protein-attenuating compound that inhibits zinc and copper ions from binding to Aβ, led to improved cognitive function, decreased plasma Aβ42 level and zinc.

HMG-CoA REDUCTASE INHIBITORS (THE “STATINS”)▪ Clinical trial with atorvastatin provides some
clinical benefit in AD patients. Treatment with lovastatin resulted in decreased plasma Aβ level.
MONOAMINE OXIDASE INHIBITORS▪ MAO inhibitor deprenyl is an anti-Parkinson
drug used to inhibit dopamine degradation in the brain. Also as a neuroprotective agent, deprenyl has been used to slow the progress of neurodegenerative diseases such as AD for many years.
▪ Rasagiline: Another MAO-B inhibitor is a bifunctional molecule which also has acetylcholinesterase inhibition activity.

PREVENTING THE MISFOLDING OF TAU▪ Chaperones: The results from a study by
Dou and colleagues suggested that increasing the activation of molecular chaperones might prevent the misfolding of tau, which would then reduce the development of NFTs.
▪ Heat shock proteins: They have been shown to activate chaperones that prevent misfolding and even promote tau binding with microtubules.
NON-STEROIDAL ANTI-INFLAMMATORY DRUGS (NSAIDS)▪ Many epidemiological studies, have suggested
that the prolonged intake of NSAIDs may be associated with a reduced incidence of AD.
ESTROGENS▪ Merlo et al. reported that estrogen can activate
matrix metalloproteinases-2 and −9 to increase beta amyloid degradation.
NICOTINE▪ Many studies have reported the effects of
intravenous or subcutaneous nicotine administration on people with AD.
▪ Significant improvements were reported in several cognitive tasks such as free recall, visual attention and perception and in mood although not on memory.

MELATONIN ▪ In AD patients, melatonin supplementation has
been suggested to improve circadian rhythmicity, and to produce beneficial effects on memory.
CELL TRANSPLANTATION AND GENE THERAPY▪ In AD rat model, transplantation of cholinergic-
rich tissue or peripheral cholinergic neurons ameliorates abnormal behavior and cognitive function.
▪ Nerve growth factor (NGF) administration rescues neurons from injury-induced cell damage and leads to associated memory improvements and thus NGF is good for gene therapy.
DOCOSA-HEXAENOIC ACID (DHA)▪ DHA is the most abundant omega 3 fatty acid in
the brain. Data from animal models support the hypothesis that DHA maybe an effective treatment for AD by means of antiamyloid, antioxidant, and neuroprotective mechanisms.
RESVERATROL ▪ Resveratrol, a red wine polyphenol, recent
studies on red wine bioactive compounds suggest that resveratrol modulates multiple mechanisms of AD pathology.
▪ Exert its neuroprotective role through inhibition of Aβ aggregation, by scavenging oxidants and exerting anti inflammatory activities.

VACCINES▪ AN-1792: Phase I studies of AN-1792 in
humans indicated that the vaccine was well tolerated, and a portion of the patients developed amyloid antibodies.
▪ Passive immunization: By using antibodies to Aβ4-10.
▪ Intravenous immunoglobulin (IVIg): IVIg infusion may have long-term benefits for the treatment of cognitive decline in Alzheimer’s disease.


The ultimate goal for Alzheimer’s disease pharmacotherapy is not merely to ameliorate symptoms, but to alter the onset or progression of the disease.There are four drugs (donepezil, galantamine, rivastigmine, and memantine) currently approved for the treatment of Alzheimer’s disease,
CONCLUSION

CONCLUSIONThe numerous complex
and interrelated biochemical pathways underlying neurodegeneration in Alzheimer’s disease can provide numerous potential targets for therapeutic intervention.Several investigational compounds have demonstrated potential as therapeutic or preventive therapies and merit additional study.
CONCLUSIONGradual elucidation of the exact mechanisms of neurodegeneration will result in increasingly focused drug development efforts.

ThanksQuestions?