recent updates in pharmacy law presented by nicholas gonzales, esq. hall, render, killian, heath...
TRANSCRIPT

Recent Updates in Pharmacy Law
Presented byNicholas Gonzales, Esq.
Hall, Render, Killian, Heath & Lyman, P.C.
Indiana Pharmacists Annual ConventionFrench Lick, INSeptember 17, 20151
Indiana Pharmacists Alliance

Disclosure
• Nicholas Gonzales has no actual or potential conflict of interest in relation to this presentation.
• Hall Render is a vendor to the health care industry, providing professional legal consultation, advocacy and representation services.
• Views expressed are speaker’s views and not necessarily Hall Render’s views.
2

Recent Updates in Pharmacy Law
I. New LegislationII. Track and TraceIII. Identification of Counterfeit DrugsIV. Drug Take-Back ProgramsV. Recent Medicare GuidanceVI.Questions
3

I. New Indiana Legislation
4

S.B. 233 “Professional Licensing Matters” Effective 7/1/14
• Specifies education and training requirements for pharmacy technicians
• Certified registered nurse anesthetists may be recognized as advanced practice nurses under certain circumstances- with prescriptive authority
5

S.B. 262 ”Biosimilar Drugs” Effective 7/1/14
• Substitute an interchangeable biosimilar product for a prescribed biological product if certain conditions are met. • Requires a pharmacist to record in a certain manner the name and
manufacturer of a biologic product that the pharmacist is dispensing not later than ten days after dispensing the biologic product. • Requires the board of pharmacy to maintain a link on the board's
website to the current list of all biological products that are determined by the FDA to be interchangeable with a specific reference biological product. • Allows the Board of Pharmacy to adopt rules. • Provides that a written or electronic prescription for a biological
product must comply with the existing prescription form requirements.
6

H.B. 1218 “Drug Treatment and Reporting” Effective 3/25/14
• Insulin now a legend drug• Restricts retail sales to prescriptions by certain practitioners• Operations standards change for prior authorization concerning
home supply of opioid treatment medication from 14 days of medication to 7 days so long as conditions are met.
• Dispenser at an opioid treatment program must transmit certain information to the division within specified time frames
• Requires a provider to release certain information from a committed patient’s mental health records upon request of the court.
7

S.B. 294- “Legend Drug Investigations” Effective 7/1/15
• Prohibits a person from owning or operating a store, facility, or other place of business in Indiana where:
1. Prescriptions are accepted to be filled;2. Prescription drugs or devices are ordered, offered,
or advertised for sale, or paid for;
unless the person has a pharmacy permit. Excludes mail order and Internet based pharmacies to the extent that they are allowed to operate under state law.
8

S.B. 358 “Medications”Effective 7/1/15
• Defines "medication therapy management" (MTM)• Adds MTM to the definition of "the practice of pharmacy."• Includes APNs and PAs in the definition of "direct supervision" for
consulting with a pharmacist on certain drug regimen protocols. • Establishes the INSPECT oversight committee. • Provides the committee's approval for the board to execute a contract
with a vendor to administer the INSPECT program. • Requires approval from the chairperson of the board of pharmacy to hire
a director of the INSPECT program. • Provides that if a dispenser's pharmacy is closed the day following a
dispensing, the information required to be sent to the INSPECT program must be transmitted by the end of the next business day.
• Amends the definition of "medication assistance" in the administrative code for purposes of the rules concerning home health agencies.
9

S.B. 406 “Overdose Intervention Drugs” Effective 4/17/15
• Requires certain emergency personnel to report to the state department of health the number of times an overdose intervention medication is administered. • Allows specified health care professionals with prescriptive authority
to dispense, write a prescription, or prepare a standing order for an overdose intervention drug without examining the individual to whom it may be administered if specified conditions are met. • Allows for an individual who is a person at risk, a family member,
friend, or other individual or entity in a position to assist another individual who, there is reason to believe, is at risk of experiencing an opioid-related overdose, to obtain and administer an overdose intervention drug if certain conditions are met. • Provides for civil immunity.
10

S.B. 534 “Rules for Prescribing Controlled Substances” Effective 12/31/15
• Requires the Medical Licensing Board to adopt standards and protocols for the prescribing of controlled substances, including the use of abuse deterrent formulations. • Requires, before March 1, 2016, the following boards to adopt rules
concerning the prescribing of opioid controlled substances for pain management treatment: (1) the Medical Licensing Board, concerning physician assistants; (2) the Board of Podiatric Medicine, concerning podiatrists; (3) the State Board of Dentistry, concerning dentists; and (4) the Indiana State Board of Nursing, concerning advanced practice nurses. • Requires each board to report before December 31, 2015, to the
Legislative Council with a status report on the board's efforts to adopt the required rules. 11

S.B. 421 “Professional Licensing Matters” Effective 7/1/14
• Requires a nonresident pharmacy to submit an inspection report from the applicant’s home state
12

II. Track and Trace - Dispenser
13
Track and Trace Background
• On November 27, 2013, the Drug Supply Chain Security Act (DSCSA) was signed into law. The DSCSA outlines critical steps to build an electronic, interoperable system by November 27, 2023, which will identify and trace certain prescription drugs as they are distributed within the United States.
• This system will enhance the FDA’s ability to help protect U.S. consumers by improving detection and removal of potentially dangerous products from the pharmaceutical distribution supply chain.
http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM453225.pdf

New January 1, 2015 Requirements
• Dispensers must establish systems for verification and handling of suspect or illegitimate product.
• Dispensers must confirm that trading partners (manufacturers, repackagers, wholesale distributors, dispensers, and third-party logistics providers) are authorized, as defined by the Food, Drug & Cosmetic Act. FDA advises checking with trading partners directly to confirm they are authorized, or checking the FDA’s drug establishment registration database or the respective state authority to confirm licensure.
July 1, 2015 Requirements
Beginning 7/1/15, a Dispenser shall not accept ownership of a pharmacy product unless the previous trading partner provides the Dispenser with the:
• Transaction History• Transaction Information• Transaction Statement
The Dispenser shall be responsible for communicating the Transaction Documents to any subsequent Trading Partner unless an exception applies…

Possible Exceptions
• Distribution among hospitals or healthcare entities under common control;
• Distribution of minimal quantities for office based use; and
• The dispensing of a product to a patient pursuant to a prescription.

Recent Guidance• Prior November 1, 2015, FDA does not intent to take action
against dispensers who accept ownership of product without receiving the product tracing information.
• Prior to November 1, 2015, FDA also does not intend to take action against dispensers who do not capture and maintain the product tracing information.
• This compliance policy does not extend to transactions in which dispensers must provide the subsequent owner with product tracing information. Additionally, other product tracing requirements regarding authorized trading partners and verification related to suspect and illegitimate product (including quarantine, investigation, notification and recordkeeping) still apply and are in effect for dispensers.

III. Identification of Counterfeit Drugs
19

Identification of Suspect Product
Beginning not later than January 1, 2015, trading partners must have systems in place that enable them, upon determining that a product in their possession or control is suspect or upon receiving a request for verification from the FDA, to quarantine suspect product and promptly conduct an investigation, in coordination with other trading partners, as applicable, to determine whether a suspect product is illegitimate.

Identification of Suspect Product
Suspect product is defined as a product for which there is reason to believe it:• is potentially counterfeit, diverted, or stolen; • is potentially intentionally adulterated such that the product
would result in serious adverse health consequences or death to humans;
• is potentially the subject of a fraudulent transaction; or • appears otherwise unfit for distribution such that the product
would result in serious adverse health consequences or death to humans.

Identification of Suspect ProductSome scenarios suggested by the FDA which may indicate a high risk for a Suspect Product:• Purchasing on the Internet from an unknown source;• Purchasing from a source that a trading partner knows or has
reason to believe has transacted business involving suspect products;
• Product that is in higher demand because of its potential or perceived relationship to a public health or other emergency (e.g., antiviral drugs);
• Appearance of a package or a container used for transport (e.g., case or tote) that seems suspicious (e.g., it has a label that contains misspellings or appears different from the standard label for that product in color, font, images, or otherwise)

Identification of Suspect Product
Some FDA strategies to identify Suspect Products include:• Being alert for offers of product for sale at a very low price or
one that is “too good to be true”;• Closely examine the package and the transport container for
signs of compromise or missing or incorrect documentation;• Closely examine the label on the package, or the label on the
individual retail unit for incorrect spelling, untranslated foreign languages, or altered product information.

Notification of Illegitimate Product
In the event that a trading partner determines a Suspect Product is actually an Illegitimate Product, the trading partner must notify the FDA.

Notification of Illegitimate ProductIllegitimate product is defined as a product for which credible evidence shows that it is• counterfeit, diverted, or stolen;• intentionally adulterated such that the product would result in
serious adverse health consequences or death to humans; • is the subject of a fraudulent transaction ; or • appears otherwise unfit for distribution such that the product
would be reasonably likely to result in serious adverse health consequences or death to humans.
Notification of Illegitimate Product
The following process should be used to notify FDA: (1) Trading partners should access FDA’s Web page at
http://www.accessdata.fda.gov/scripts/cder/email/drugnotification.cfm for notifications.
(2) Trading partners should follow the instructions on the Web page for accessing Form FDA 3911.
(3) Form FDA 3911 should be submitted by using the method provided in the form or on the Web page.

IV. Drug Take-Back Programs
27

New Final Rules
• On September 9, 2014, the DEA published the final rules concerning the disposal of controlled substances ("Final Rules").
• The Final Rules implement the Secure and Responsible Drug Disposal Act of 2010 ("Act") and increase the number of ways certain people may safely and legally dispose of unwanted controlled substances.

New Methods of Drug Disposal• The Final Rules allow an "ultimate user" to voluntarily dispose
of unwanted controlled substances by depositing such unwanted controlled substances at a collection receptacle, participating in a mail-back program or a drug take-back program.
• The definition of an "ultimate user" is generally defined as a person who legally obtains and possesses a controlled substance for his/her own use or for the use of someone else in the household including any applicable animals.

New Methods of Drug Disposal• Registered manufacturers, distributors, reverse distributors,
narcotic treatment programs, hospitals/clinics with an on-site pharmacy, or retail pharmacy are eligible to register with the DEA as a Collector.
• Current DEA registrants in the above-named categories may choose to change their current DEA registration to allow them to be Collectors and receive controlled substances from end users for the purposes of destruction.

Collection Receptacles • Must meet certain design criteria;• Be permanently secured and fixed;• Placed in a location that is accessible by the general public and
within the immediate proximity of the designated area in which controlled substances are stored;
• Placed in an area where employees will have visibility of the receptacle;
• The inner liner of the receptacle must contain a tracking number and must be self-sealing; and
• Collectors are also responsible for tracking the inner liners and must meet certain recordkeeping standards.

Collection Receptacles • The Collector may only install, remove, store and transfer the
inner liner when two employees are present.• Once the inner liner is removed, it must be sent back to the
reverse distributor or the reverse distributor's location by a common or contract carrier.
• The Collector is not authorized to dispose of the controlled substances placed in such Collector's receptacle.

Mail-back Programs
• The mailer used in this program must be individually marked, pre-addressed with pre-paid postage, and must meet certain security and design requirements.
• The Collector is responsible for keeping records for each mailer, although the Collectors are not responsible for tracking mail-back packages that were disseminated but not returned.
• Each Collector with a mail-back program must have an on-site method of destruction. Collectors that use a mail-back program may choose to charge for the mailer or may give the mailer away.

Mail-back Programs
• Collectors that use a mail-back program may choose to charge for the mailer or may give the mailer away.
• The Final Rules do not address whether the Anti-Kickback Statute is implicated if a Collector provided the mailers free of charge.
• Collectors, however, must make sure they follow all applicable Federal, State and Tribal laws when participating in controlled substance disposal.

Law Enforcement Take-Back Events• These take-back events may be co-sponsored by law
enforcement and Collectors.• Law enforcement must mandate custody and control of the
collected controlled substances from the time these substances are received to the time they are securely stored, transferred or destroyed.
• There is no requirement that more than one law enforcement officer is needed to run a take-back event as long as such officer meets certain criteria.

V. Recent Part D Guidance
36

Recent Part D Reports
• June 2015 – OIG released two reports
– Ensuring the Integrity of Medicare Part DAvailable at: http://oig.hhs.gov/oei/reports/oei-03-15-00180.pdf
– Questionable Billing and Geographic Hotspots Point to Potential Fraud and Abuse in Medicare Part DAvailable at: http://oig.hhs.gov/oei/reports/oei-02-15-00190.pdf

Why is this important?
• $121 Billion
• 39 Million
• 136% Increase

Why is this important?
“OIG has made stopping Part D fraud a top priority.”
Assistant Inspector General Ann Maxwell’s testimony to Congress in July 2015
A full transcript of Ms. Maxwell’s testimony is available at: https://oig.hhs.gov/testimony/docs/2015/maxwell-0714.pdf

Spending Trends
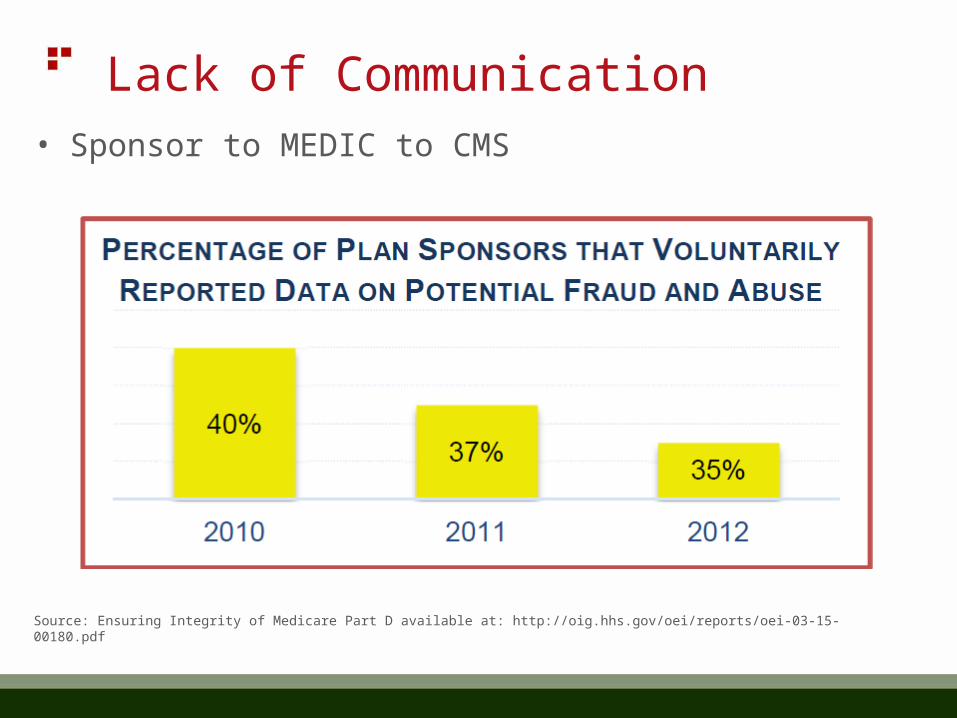
Lack of Communication• Sponsor to MEDIC to CMS
Source: Ensuring Integrity of Medicare Part D available at: http://oig.hhs.gov/oei/reports/oei-03-15-00180.pdf

Missed Opportunities
• Medicare Drug Benefit Contractor
– 2008 – 4% Proactive
– 2011 – 10% Proactive

Missed Opportunities• Plan Sponsors– Not required to report fraud and abuse– Invalid prescriber information • $1.2 billion• Invalid Prescribers (Athletic Trainers, Massage Therapist,
Dietician)– Excluded Prescribers– Schedule II Refills– Dead Beneficiaries

Questionable Billing
• Average number of prescriptions per beneficiary
• Percentage of prescriptions for commonly abused opioids
• Average number of prescribers for commonly abused opioids for beneficiaries
• Average number of drugs per beneficiary
• Percentage of beneficiaries with excessive supply of drugs

The Future
• Better use of data
• Increased communication
• Increased enforcement
Be Proactive
• Compliance Program
• Routine Self-Audits

VI. Questions
47

Denver | Detroit | Indianapolis | Louisville | Milwaukee | Philadelphia | Washington, D.C.
Nicholas A. Gonzales, Esq.Hall, Render, Killian, Heath & Lyman, P.C.111 East Kilbourn Avenue, Suite 1300Milwaukee, WI 53202(414) [email protected]
For more information on topics related to health care law, please visit
www.hallrender.com/resources. This presentation is solely for educational purposes and the matters
presented herein do not constitute legal advice with respect to your particular situation.