recoverin as a paraneoplastic antigen in lung cancer: the occurrence of anti-recoverin...
TRANSCRIPT
Lung Cancer (2004) 44, 193—198
Recoverin as a paraneoplastic antigen inlung cancer: the occurrence of anti-recoverinautoantibodies in sera and recoverin in tumors
Alexandr V. Bazhina, Marina S. Savchenkoa, Olga N. Shifrinab,Sofia A. Demourab,c, Svetlana Yu. Chikinab, Gabriele Jaquesd,Eugenia A. Koganc, Alexandr G. Chuchalinb, Pavel P. Philippova,*
a Laboratory of Biomedicine, Department of Cell Signalling, A.N. Belozersky Institute ofPhysico-Chemical Biology, M.V. Lomonosov Moscow State University, 119992 Moscow, Russiab Pulmonology Research Institute, 105077 Moscow, Russiac Chair of Pathoanatomy, I.M. Setchenov Moscow Medical Academy, 119881 Moscow, Russiad Klinik für Hämatologie, Onkologie und Immunologie, Klinikum der Philipps-Universität,35033 Marburg, Germany
Received 28 April 2003 ; received in revised form 29 September 2003; accepted 2 October 2003
KEYWORDSRecoverin;Non-small cell lungcarcinoma;Small cell lungcarcinoma;Cancer-associatedretinopathy;Paraneoplastic antigen;Paraneoplasticneurological syndrome;Autoimmunity
Summary Using immunoblotting with recombinant recoverin as an antigen, we haveexamined 279 serum samples from individuals with small cell lung carcinoma (SCLC, 99patients), non-small cell lung carcinoma (NSCLC, 44 patients), and non-malignant pul-monary disorders (86 patients) as well as sera from 50 healthy donors. Autoantibodiesagainst recoverin (anti-Rc) were detected in sera from 15 patients with SCLC (15% ofcases) and from 9 patients with NSCLC (about 20% of cases). Only two anti-Rc positivecases were detected in patients with non-malignant pulmonary disorders, while nosuch cases were found in healthy individuals. Immunohistochemical investigation ofparaffin sections of 44 SCLC and 40 NSCLC tumors revealed recoverin-positive reac-tion in 30 SCLC (68%) and 34 NSCLC (85%) sections. Despite the high specificity (98%),the low sensitivity (less than 20%) does not allow serum anti-Rc to be considered asa valuable marker of lung cancer. However, taking into account the high occurrenceof aberrant expression of recoverin in lung tumors, this PNA could be considered as apotential target for immunotherapy of lung cancer.© 2003 Elsevier Ireland Ltd. All rights reserved.
Abbreviations: anti-Rc, autoantibodies against recoverin; CAR,cancer-associated retinopathy; NSCLC, non-small lung cancer;PNA, paraneoplastic antigen; PNS, paraneoplastic neurologicalsyndrome; SCLC, small cell lung carcinoma
∗ Corresponding author. Tel.: +7-095-939-50-17;fax: +7-095-939-09-78.
E-mail address: [email protected] (P.P. Philippov).
1. Introduction
In 1987, Thirkill et al. [1] detected autoantibodiesagainst a retinal protein with an apparent molecu-lar weight of 26 K in sera from patients with smallcell lung carcinoma (SCLC) and the concurrent neu-rological syndrome, cancer-associated retinopathy(CAR). This protein, named ‘‘CAR-antigen’’, wasthen recognized [2] to be identical to recoverin
0169-5002/$ – see front matter © 2003 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.lungcan.2003.10.006

194 A.V. Bazhin et al.
[3—5]. In health, recoverin serves as a Ca2+-depen-dent modulator of rhodopsin phosphorylation inphotoreceptors cells [6—8]. However, being a para-neoplastic antigen (PNA), it can also be expressedin tumors localized outside the nervous system.The aberrant expression of recoverin in malig-nant cells is believed to trigger the host immuneresponse, resulting in the development of parane-oplastic retina degeneration or the CAR-syndrome[9—11].Autoantibodies against recoverin (anti-Rc) most
often occur in patients with SCLC [1,2,12—16].Also, two anti-Rc-positive cases have been de-scribed in patients with non-small cell lung car-cinoma (NSCLC) [17,18] and a few other cancers[19—21]. The CAR-syndrome, similar to other para-neoplastic neurological syndromes (PNSs), is knownto be a very rare event [9,11]. However, underly-ing autoantibodies apparently might occur morefrequently, as anti-Rc can be found in sera from pa-tients with lung cancer who had no CAR-syndrome[16,18]. Statistics on the occurrence of anti-Rc insera from patients with cancers have so far beenabsent. The same is true for that on recoverin ex-pression in tumor tissues. In this study, we haveinvestigated patients with SCLC and NSCLC to es-timate the occurrences of (i) anti-Rc in their sera,using immunoblotting with recombinant recoverinas an antigen, and (ii) recoverin expression in paraf-fin sections of their tumor, using the immunohis-tochemical method with polyclonal (monospecific)antibodies against recoverin.
2. Materials and methods
2.1. Sera and tumor tissues
Sera prepared from whole blood of patients withlung cancers were collected in the Pulmonology Re-search Institute, Moscow (Russia) during 1998—2001and in the Department of Internal Medicine, Divi-sion of Hematology/Oncology, Philipps-University,Marburg (Germany) during 1982—1986. Patients,men (m) and women (w), with lung cancers wereinvestigated before treatment (the number of thepatients is shown in brackets): SCLC patients from32 to 88 years old (79m and 20w) and NSCLC pa-tients from 51 to 75 years old (37m and 7w). Serafrom 86 patients (men and women) with differ-ent non-malignant disorders and 50 healthy indi-viduals (men and women) were collected in thePulmonology Research Institute. The lung cancerdiagnosis was established by physical examina-tion, plain chest radiography, computer tomog-raphy, bronchoscopy with biopsy and subsequent
histological and cytological analyses. The physi-cal examination and case histories of the patientsrevealed that none of the patients with cancers,including anti-Rc-positive individuals, manifestedthe CAR-syndrome.Lung cancer tissues were collected from clinics
in Moscow during 1998—2001. Forty-four samplesof SCLC (classical type) and 40 those of NSCLC (29squamous cell carcinomas and 11 adenocarcinomas)were used for the investigation.
2.2. Recoverin
Recombinant myristoylated recoverin was obtainedaccording to [22] and was used as an antigen inWestern blot analysis (see below) and for thepreparation of polyclonal (monospecific) antibodiesagainst recoverin [3,4].
2.3. Western blotting
Western blot analysis was performed, with rock-ing at room temperature, after SDS-PAGE [23] ofrecombinant myristoylated recoverin (2�g pertrack) in 12% gel. The gel slabs were electrotrans-ferred to Hybond-C Extra nitrocellulose membranes(AmershamBioscience) in Tris—glycine—methanolbuffer, pH 8.3. Then non-specific sites were satu-rated by incubation with 10% delipidated dry milkfor 1.5 h and then membranes were incubatedfor 12 h with: (i) serum from SCLC patients, (ii)serum from healthy individuals, (iii) serum frompatients with non-malignant diseases (initial di-lution of the serum was 1:20 in all cases) or (iv)rabbit polyclonal (monospecific) anti-recoverin an-tibodies (1�g/ml) as a positive control. All theincubations were performed in 20mM Tris—HCl (pH7.4) containing 500mM NaCl, 0.05% Tween-20 and1mM CaCl2 (buffer A). Blots were rinsed threetimes (each for 10min) with buffer A, incubatedfor 1.5 h with sheep anti-human IgG peroxidaseconjugate (AmershamBioscience) at the dilutionof 1:1000 with buffer A, rinsed again with 50mMTris—HCl (pH 7.6) and finally incubated with 10mM3,3′-diaminobenzidine (as a substrate) in 0.01%hydrogen peroxide; in some case immunoreactivebands were visualised by the enhanced chemilumi-nescence system (AmershamBioscience) accordingto the method described by the manufacturer.
2.4. Immunohistochemical staining
Tissue samples were fixed in 4% formaldehydeand embedded in paraffin. For the immunohisto-chemical study, the deparaffinized tissue sectionswere incubated with polyclonal (monospecific)
Recoverin as a paraneoplastic antigen in lung cancer 195
antibodies against recombinant recoverin (5�g/ml)as the first antibody. Immunoperoxidase stainingwas applied to the specimens by the streptavidin—biotin—peroxidase-complex. A scoring system wasexploited to analyze the level of recoverin ex-pression in tumor cells; the following designa-tions were used to show the percentage (p) ofrecoverin-positive cells in the sections: ‘‘0’’, re-coverin was absent; ‘‘2’’, ‘‘4’’, and ‘‘6’’ corre-sponded p < 20%, 20% < p < 50%, and p > 50%,respectively. Bovine retina sections were used as apositive control of the reaction. The tumor cells inSCLC sections were positively stained with mono-clonal antibodies to chromogranin (Dako) in the di-lution of 1:200 and to pancytokeratin (Immunotech)in the dilution of 1:100, suggesting neuroendocrinecharacteristics (data not shown).
2.5. Statistical analysis
Comparison between the groups of the investigatedindividuals was made by the χ2-test; a P-valueof <0.05 was considered as significant. Sensitiv-ity and specificity were calculated using the fol-lowing equations: sensitivity = 100 × number oftrue-positive/(number of true-positive + numberof false negative); specificity = 100 × number oftrue-negative/(number of true-negative + numberof false positive).
3. Results
3.1. Serial analyses of SCLC and NSCLC serafor the presence of anti-Rc
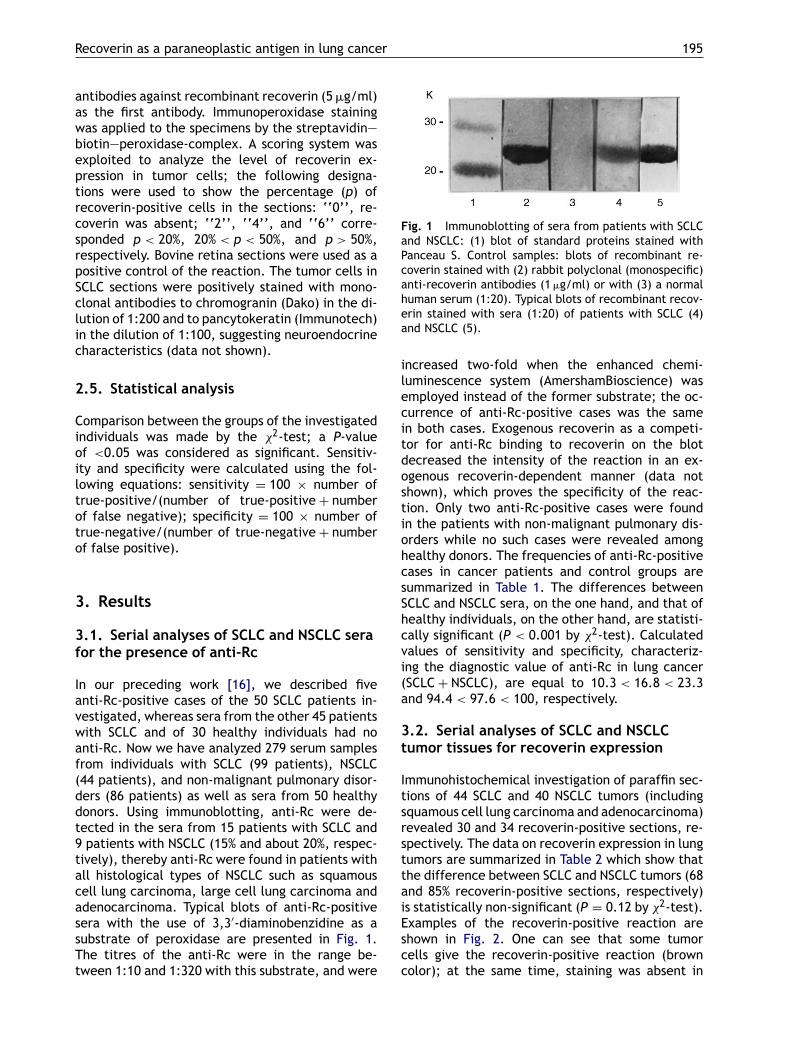
In our preceding work [16], we described fiveanti-Rc-positive cases of the 50 SCLC patients in-vestigated, whereas sera from the other 45 patientswith SCLC and of 30 healthy individuals had noanti-Rc. Now we have analyzed 279 serum samplesfrom individuals with SCLC (99 patients), NSCLC(44 patients), and non-malignant pulmonary disor-ders (86 patients) as well as sera from 50 healthydonors. Using immunoblotting, anti-Rc were de-tected in the sera from 15 patients with SCLC and9 patients with NSCLC (15% and about 20%, respec-tively), thereby anti-Rc were found in patients withall histological types of NSCLC such as squamouscell lung carcinoma, large cell lung carcinoma andadenocarcinoma. Typical blots of anti-Rc-positivesera with the use of 3,3′-diaminobenzidine as asubstrate of peroxidase are presented in Fig. 1.The titres of the anti-Rc were in the range be-tween 1:10 and 1:320 with this substrate, and were
Fig. 1 Immunoblotting of sera from patients with SCLCand NSCLC: (1) blot of standard proteins stained withPanceau S. Control samples: blots of recombinant re-coverin stained with (2) rabbit polyclonal (monospecific)anti-recoverin antibodies (1�g/ml) or with (3) a normalhuman serum (1:20). Typical blots of recombinant recov-erin stained with sera (1:20) of patients with SCLC (4)and NSCLC (5).
increased two-fold when the enhanced chemi-luminescence system (AmershamBioscience) wasemployed instead of the former substrate; the oc-currence of anti-Rc-positive cases was the samein both cases. Exogenous recoverin as a competi-tor for anti-Rc binding to recoverin on the blotdecreased the intensity of the reaction in an ex-ogenous recoverin-dependent manner (data notshown), which proves the specificity of the reac-tion. Only two anti-Rc-positive cases were foundin the patients with non-malignant pulmonary dis-orders while no such cases were revealed amonghealthy donors. The frequencies of anti-Rc-positivecases in cancer patients and control groups aresummarized in Table 1. The differences betweenSCLC and NSCLC sera, on the one hand, and that ofhealthy individuals, on the other hand, are statisti-cally significant (P < 0.001 by χ2-test). Calculatedvalues of sensitivity and specificity, characteriz-ing the diagnostic value of anti-Rc in lung cancer(SCLC + NSCLC), are equal to 10.3 < 16.8 < 23.3and 94.4 < 97.6 < 100, respectively.
3.2. Serial analyses of SCLC and NSCLCtumor tissues for recoverin expression
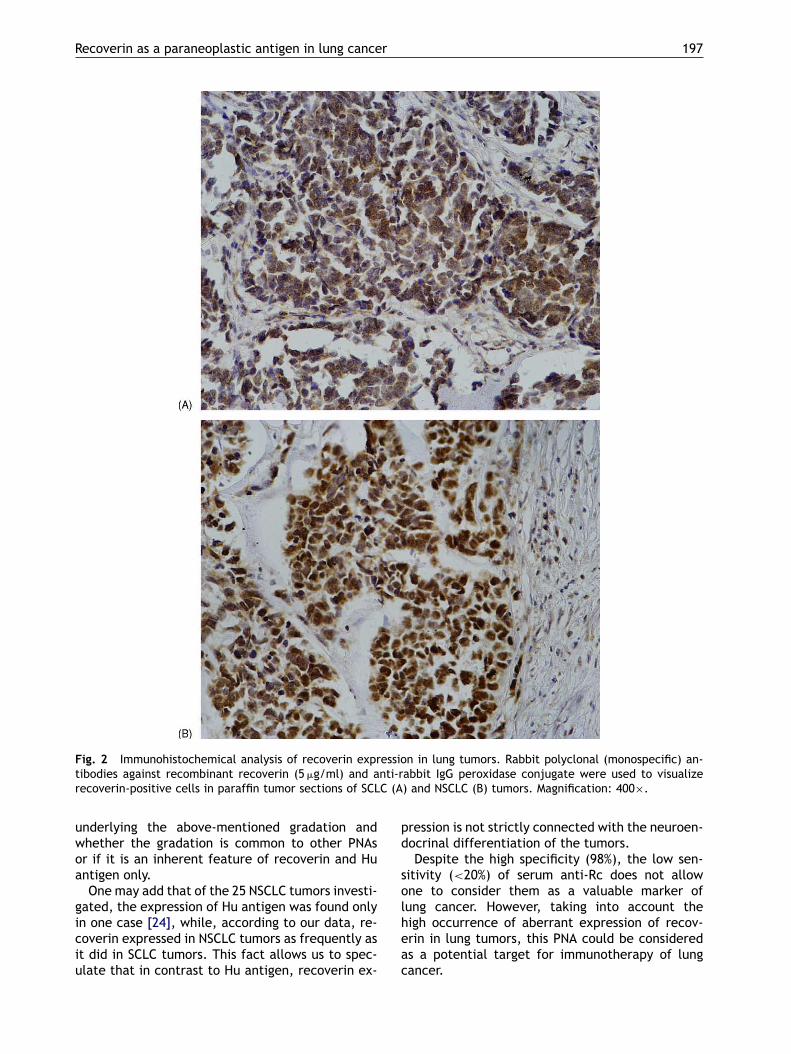
Immunohistochemical investigation of paraffin sec-tions of 44 SCLC and 40 NSCLC tumors (includingsquamous cell lung carcinoma and adenocarcinoma)revealed 30 and 34 recoverin-positive sections, re-spectively. The data on recoverin expression in lungtumors are summarized in Table 2 which show thatthe difference between SCLC and NSCLC tumors (68and 85% recoverin-positive sections, respectively)is statistically non-significant (P = 0.12 by χ2-test).Examples of the recoverin-positive reaction areshown in Fig. 2. One can see that some tumorcells give the recoverin-positive reaction (browncolor); at the same time, staining was absent in
196 A.V. Bazhin et al.
Table 1 Occurrences of anti-Rc in sera from patients with lung cancer and non-malignant pulmonary diseases(NMPDs) and from healthy individuals
Amount Occurrence of anti-Rc (%)
Serum samples(in total)
Anti-Rc-positiveserum samples
SCLC 99 15 7.5 < 15.2 < 22.7a
NSCLC 44 9 7.4 < 20.5 < 33.5a
SCLC + NSCLC 143 24 10.3 < 16.8 < 23.3a
NMPDs 86 2 −0.8 < 2.3 < 5.5b
Healthy 50 0 −1 < 0 < 1b
NMPDs + healthy 136 2 −0.5 < 1.4 < 3.4b
a Normal distribution.b Binominal distribution.
zones of stromal cells in the same sections. Itshould be stressed that the recoverin-positive re-action did not appear when anti-recoverin antibod-ies were omitted or preadsorbed with recoverin(data not shown), i.e. the staining actually reflectscross-reaction between recoverin present in thesections and added anti-recoverin antibodies.To conclude this Section, it may be noted
that (i) different levels of recoverin expressionwere detected in SCLC (scores 0—6) and NSCLC(scores 0—2) tumors; (ii) among NSCLC tumors,low-differentiated tumors demonstrated higherlevels of recoverin expression (scores 2—4) in com-parison with high-differentiated ones (scores 0—2),and (iii) NSCLC patients with anti-Rc in their serahad a higher level of recoverin expression (scores4—6) in the tumors than those who had no serumanti-Rc (scores 2—4).
4. Discussion
The aberrant expression of PNAs in malignanttumors localized outside the nervous system is
Table 2 Occurrence of recoverin expression in lung tumors
Type of lung cancer Amount Occurrence of recoverinexpression (%)
Tumours(in total)
Recoverin-positivetumors
SCLC 44 30 54.4 < 68 < 81.9a
NSCLC 40 34 73.9 < 85 < 96.0a
Including squamous-cell lung carcinoma 29 25 73.7 < 86 < 98.8a
Including adenocarcinoma 11 9 48.2 < 82 < 97.7b
SCLC + NSCLC 88 64 63.4 < 73 < 82.0a
a Normal distribution.b Binominal distribution.
believed to trigger the production of autoanti-bodies by the immune system. The autoantibodiesin turn specifically interact with correspondingepitops in neurons, which initiates the degenera-tion of the neurons and the development of PNSsin some patients with the tumors [9—11]. In thisstudy, we analyzed serial samples of tumor tissuesand sera from 143 patients with lung cancer, andfound out that (i) 68 and 85% of SCLC and NSCLCtumors are recoverin-positive and (ii) 15 and 20% ofSCLC and NSCLC sera are anti-Rc-positive, respec-tively. None of 143 patients with lung cancer hasa loss of vision, i.e. the CAR-syndrome occurrencecan be evaluated at <1%. Hence, the occurrenceof recoverin expression in lung tumors > that ofanti-Rc-positive sera � that of the CAR-syndrome.Similar gradation also exists for another PNA, Huantigen, which is one of the well-studied PNAs.This antigen was shown to be expressed in 100%SCLC tumors [24], serum autoantibodies againstthis antigen were detected in about 20% SCLC pa-tients [24], and the occurrence of the correspond-ing SCLC-associated PNS is of the order of 1% [9].However, it is still unclear what are the causes
Recoverin as a paraneoplastic antigen in lung cancer 197
Fig. 2 Immunohistochemical analysis of recoverin expression in lung tumors. Rabbit polyclonal (monospecific) an-tibodies against recombinant recoverin (5�g/ml) and anti-rabbit IgG peroxidase conjugate were used to visualizerecoverin-positive cells in paraffin tumor sections of SCLC (A) and NSCLC (B) tumors. Magnification: 400×.
underlying the above-mentioned gradation andwhether the gradation is common to other PNAsor if it is an inherent feature of recoverin and Huantigen only.One may add that of the 25 NSCLC tumors investi-
gated, the expression of Hu antigen was found onlyin one case [24], while, according to our data, re-coverin expressed in NSCLC tumors as frequently asit did in SCLC tumors. This fact allows us to spec-ulate that in contrast to Hu antigen, recoverin ex-
pression is not strictly connected with the neuroen-docrinal differentiation of the tumors.Despite the high specificity (98%), the low sen-
sitivity (<20%) of serum anti-Rc does not allowone to consider them as a valuable marker oflung cancer. However, taking into account thehigh occurrence of aberrant expression of recov-erin in lung tumors, this PNA could be consideredas a potential target for immunotherapy of lungcancer.

198 A.V. Bazhin et al.
Acknowledgements
We are indebted to Prof. K. Rawson-Jones (Fac-ulty of Foreign Languages, M.V. Lomonosov MoscowState University), Richard Lozier and E.V. Braginafor helping us in preparation of this article, and toDr. E.E. Skorikova and I.P. Vorojeikina for their as-sistance. This work was supported in part by grantsfrom the Ludwig Institute for Cancer Research andthe Russian Foundation for Basic Research, No.03-04-49181 (to P.P.P.), and by a fellowship fromMarburg University, Germany (to A.V.B.).
References
[1] Thirkill CE, Roth AM, Keltner JL. Cancer-associatedretinopathy. Arch Ophtalmol 1987;105:372—5.
[2] Polans AS, Buczylko J, Crabb J, Palczewcki K. A photore-ceptor calcium binding protein is recognized by autoan-tibodies obtained from patients with cancer-associatedretinopathy. J Cell Biol 1991;112:981—9.
[3] Dizhoor AM, Nekrasova ER, Philippov PP. New 26 kDa pro-tein specific for photoreceptor cells, capable of bindingto immobilized delipidated rhodopsin. Biokhimia (Moscow)1991;56:225—8.
[4] Dizhoor AM, Ray S, Kumar S, et al. Recoverin: a calciumsensitive activator of retinal rod guanylate cyclase. Science1991;251:915—8.
[5] Lambrecht HG, Koch KW. A 26 kd calcium binding proteinfrom bovine rod outer segments as modulator of photore-ceptor guanylate cyclase. EMBO J 1991;10:793—8.
[6] Gorodovikova EN, Gimelbrant AA, Senin II, Philippov PP. Re-coverin mediates the calcium effect upon rhodopsin phos-phorylation and cGMP hydrolysis in bovine retina rod cells.FEBS Lett 1994;349:187—90.
[7] Gorodovikova EN, Senin II, Philippov PP. Calcium-sensitivecontrol of rhodopsin phosphorylation in the reconstitutedsystem consisting of photoreceptor membranes, rhodopsinkinase and recoverin. FEBS Lett 1994;353:171—2.
[8] Kawamura S, Hisatomi O, Kayada S, Tokunaga F, Kuo CH.Recoverin has S-modulin activity in frog rods. J Biol Chem1993;268:14579—82.
[9] Dropcho EJ. Remote neurologic manifestations of cancer.Neurol Clin 2002;20:85—122.
[10] Musunuru K, Darnell RB. Paraneoplastic neurologic diseaseantigens: RNA-binding proteins and signaling proteins in
neuronal degeneration. Ann Rev Neurosci 2001;24:239—62.
[11] Posner JB, Dalmau JO. Paraneoplasic syndromes of thenervous system. Clin Chem Lab Med 2000;38:117—22.
[12] Thirkill CE, Keltner JL, Tyler NK, Roth AM. Antibody reac-tions with retina and cancer-associated antigens in 10 pa-tients with cancer-associated retinopathy. Arch Ophtalmol1993;111:931—7.
[13] Polans AS, Witkowska D, Haley TL, et al. Recoverin,a photoreceptor-specific calcium-binding protein, is ex-pressed by the tumor of a patient with cancer-associatedretinopathy. Proc Natl Acad Sci USA 1995;92:9176—80.
[14] Matsubara S, Yamaji Y, Fujita T, et al. Cancer-associatedretinopathy syndrome: a case of small cell lung can-cer expressing recoverin immunoreactivity. Lung Cancer1996;14:265—71.
[15] Thirkill CE. Lung cancer-induced blindness. Lung Cancer1996;14:253—64.
[16] Bazhin AV, Shifrina ON, Savchenko MS, et al. Low titreautoantibodies against recoverin in sera of patients withsmall cell lung cancer but without a loss of vision. LungCancer 2001;34:99—104.
[17] Salgia R, Hedges TR, Rizk M. Cancer-associated retinopa-thy in a patient with non-small cell lung carcinoma. LungCancer 1998;22:149—52.
[18] Savchenko MS, Bazhin AV, Shifrina ON, et al. Antirecoverinautoantibodies in the patient with non-small lung cancerbut without cancer-associated retinopathy. Lung Cancer2003;41:363—7.
[19] Eltabbakh GH, Hoogereland DL. Paraneoplastic retinopa-thy associated with uterine sarcoma. Gynecol Oncol1995;58:120—3.
[20] Adamus G, Amundson D, MacKay PG. Long-term per-sistence of anti-recoverin antibodies in endometrialcancer-associated retinopathy. Arch Ophthalmol 1998;116:251—3.
[21] Katsuta H, Okada M, Nakauchi T. Cancer-associatedretinopathy associated with invasive thymoma. Am J Oph-talmology 2002;134:383—9.
[22] Senin II, Zargarov AA, Alekseev AM. N-Myristoylation of re-coverin enhabces its efficiency as an inhibitor of rhodopsinkinase. FEBS Lett 1995;376:87—90.
[23] Laemmli UK. Cleavage of structural proteins during theassembly of the head of bacteriophage T4. Nature1970;227:680—8.
[24] Dalmau J, Furneaux HM, Cordon-Cardo C, Posner J. Theexpression of the Hu (paraneoplastic encephalomyeli-tis/sensory neuronopathy) antigen in human normal andtumor tissues. Am J Patol 1992;141:881—6.