"recovery focused cbt for bipolar disorder" with dr. steven jones
TRANSCRIPT

Recovery focused CBT for Bipolar Disorder
Steven JonesThis study was funded by the National Institute for Health Research (NIHR)
under its Programme Grants for Applied Research funding scheme. The views expressed are those of the author(s) and not necessarily those of the
NHS, the NIHR or the Department of Health.

Acknowledgements
• Sally Higginson• Lee Mulligan• Tony Morrison• Gina Smith• Mary Welford• John Mulligan• James Kelly • Fiona Lobban• Recovery Bipolar SURG

Background
• Traditional focus for intervention = symptom reduction/relapse prevention
• NICE recommends structured psychological interventions to help reduce relapse
• But what about other outcomes?
• Relapse is not a binary outcome
Geddes, Burgess et al. 2004; Colom, Vieta et al. 2009
Lam, Hayward et al. 2005
Case for Recovery
• Clinical vs personal recovery– Can overlap but no synonymous
• Consumers value personal recovery – Recovery ≠ symptomatic change
• Recovery reflected in government mental health policy
• But therapies do not focus on personal recovery outcomes
DOH 2001; DOH 2009 Mead and Copeland 2000
Russell and Browne 2005; Mansell, Powell et al. 2009

Case For Early Intervention• Delayed treatment associated with worse outcomes in general both functional and
symptomatic
• Later episodes – Triggered by life events previously linked to mood changes – Less likely to be mediated by cognitive processes
• Thus psychological interventions potentially more powerful when applied earlier in the illness course – CBT benefit only for those with fewer episodes ?– Earlier onset of bipolar disorder = worse clinical outcomes
Post et al 2010Drancourt et al 2012
Barnard et al 2004Jones et al 2001Scott et al 2006
Lish et al 1994Baldessarinin et al 2012
• Recent survey by Bipolar UK, Bipolar Scotland
and Royal College of Psychiatrists
• N=706
• Time to BD diagnosis 13 years
• 85% wrongly diagnosed initially – mainly depression
• 71% felt condition made worse by inappropriate treatment
• Over half of clinicians wanted tools to help screen for mania history
• So that people access the right treatments in a timely fashion
• So that people don’t receive potentially harmful interventions
• Duration of untreated bipolar disorder is associated with more mood episodes, more
• suicidality and more mood instability
Drancourt et al. 2012
RfCBT for Early Bipolar
• Intention to provide a flexible but structured intervention
• Benefits from current evidence base but matches intervention to client’s priorities
• Targets individuals early in BD course to hopefully improve trajectory
• Focus on service user valued outcome –personal recovery

RfCBT Development
• Pilot case series data
– Jones and Burrell-Hodgson, 2008
• Importance of
– flexible engagement
– consideration of meaning of diagnosis
– coping skills reviews
– role of appraisals of fluctuations in affect.
RfCBT Development
• Therapy manual development was also informed by:
– qualitative interviews about personal experiences of recovery in BD
– focus groups to consult on content, format and supporting materials
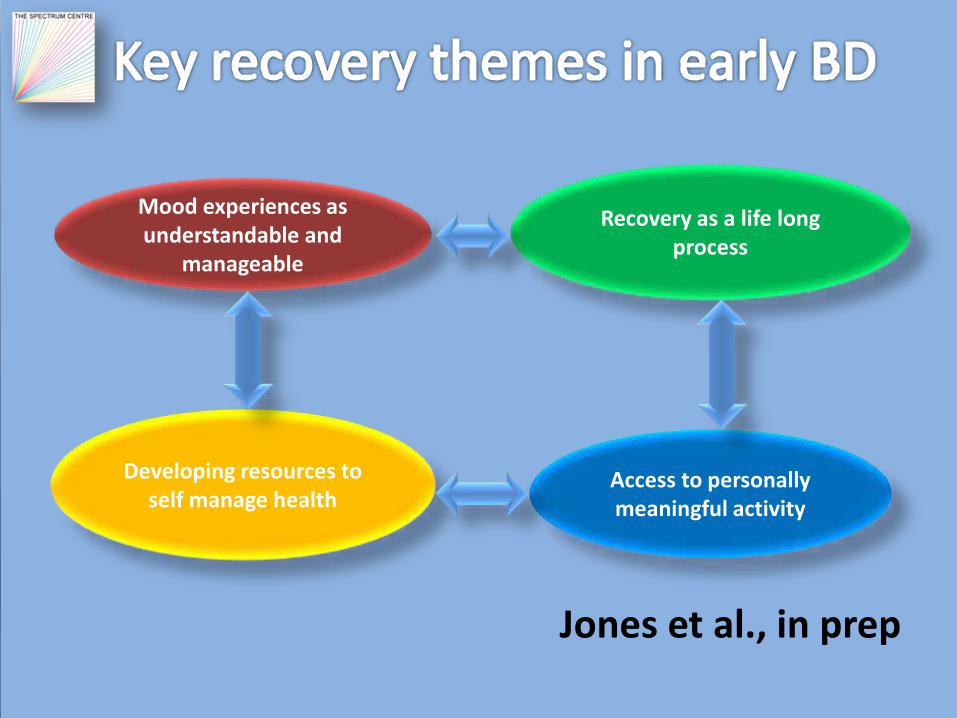
Jones et al., in prep
Mood experiences as understandable and
manageable
Recovery as a life long process
Access to personally meaningful activity
Developing resources to self manage health
Focus Group Outcome
• Importance of
– Focus on hope and opportunity
– Flexibility – timing and location
– Good quality supporting materials including recovery stories
– Documented recovery plan
– Client control of sharing with wider MH team
– Measurement of functional outcomes

RfCBT Intervention
• Delivered by mental health professionals trained to BABCP accreditation level in CBT or equivalent.
• Duration of therapy is up to 18 h over six months
• Sessions are weekly-fortnightly

RfCBT
The therapy approach differs from standard CBT for bipolar disorder in the following ways:
• Explicit focus on eliciting client focused goals rather than presuming a target of relapse prevention.
• Formulation driven idiosyncratic approach rather than applying a very similar model of bipolar experience across clients.
• Freedom to work within whatever model the client brings.
• Openness to address functioning and comorbidity issues as well as mood problems.
How to identify recovery goals
• Can be done by structured
qualitative interviews with clients
• Usually clinicians do not have time to do this
• Recent development of a quantitative measure of recovery (Bipolar Recovery Questionnaire)
• Can indicate patterns of recovery goals and also whether treatment is delivering recovery gains

Tools and Choices
• Section 1 Therapy information and appointment log
• Section 2 Useful information – Contacts, website, groups, service user poetry
• Section 3 Recovery stories
• Section 4 Understanding my experiences –Formulations, mood charts, life charts
• Section 5 Tools and Choices – Sleep diaries, EWS and coping skills, recovery plan
• Section 6 – Future thoughts and ideas – Anything else relevant inc own recovery story
Current Study
Recovery focused CBT (RfCBT) intended to
• enhance personal recovery
• reduce relapse
Participants:
Individuals <= 5 five years since onset of bipolar disorder
Meet SCID criteria for BD
Primary Outcomes
• Feasibility and acceptability
– retention of participants
– adherence to the intervention
• Personal recovery
– BRQ
• Time to relapse
– SCID Life
Secondary Outcomes
• Quality of life and social functioning
– QoL.BD
– PSP


Feasibility
• 32/33 participants in therapy received at least 6 sessions RfCBT– Mean 14.15 (s.d. 4.21)
• Recovery Fidelity Scale– Mean adherence 91% (sd 9%)
• CTS-R– Mean CTS-R (35.4 s.d. 7.9)
– Above established training threshold Keen & Freeston 2008

Recovery
Better recovery outcomes at follow-up in RfCBT gp p = 0.01
1500
1600
1700
1800
1900
2000
2100
2200
2300
2400
2500
Baseline 6 months 12 months
TAU
HAMD-RfCBT

Time to First Recurrence

Time to First Depression
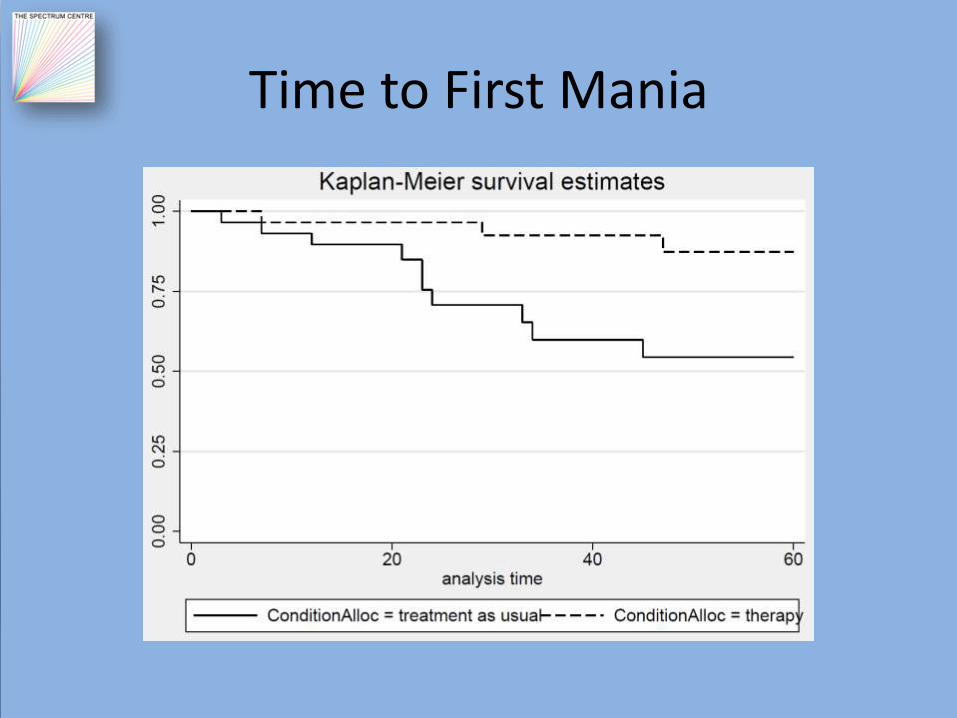
Time to First Mania

Quality of Life
Trend towards better QoL for RfBT at post therapy p =0.054
30
32
34
36
38
40
42
44
Baseline 6 months 12 months
TAU
RfCBT

Personal and Social Performance
Differences in PSP NS p = 0.151
50
55
60
65
70
75
80
85
Baseline 6 months 12 months
TAU
RfCBT
Conclusion
• RfCBT feasible in terms of – Recruitment– Retention– Engagement in therapy
• Clinical outcomes– Increase time to relapse for both poles of mood
episode– Improved recovery– Improved QoL– Impacts of mood and PSP NS
Conclusion
• Results promising for this novel therapy
• Next stage to explore in a definitive trial
– Large scale – more precise effect estimates
• Crucial to test cost-benefits of this therapy
