redesigning health services for aboriginal mothers & children
TRANSCRIPT
ConclusionThe redesign of health services for Aboriginal mothers and children in collaboration with the local Aboriginal Medical Service, GPs and the Aboriginal Community will foster culturally sensitive, appropriate, accessible and sustainable health care options for all Aboriginal families now and in the future.
These improvements will lead to better health outcomes for Aboriginal families and a reduction in longitudinal health care costs over the lifespan.
Redesigning Health Services for Aboriginal Mothers & ChildrenA partnership with CCLHD and Yerin Aboriginal Health Service Inc.
GoalAboriginal Women and children will have access to culturally safe and clinically appropriate maternal and child health care on the Central Coast irrespective of where they live.
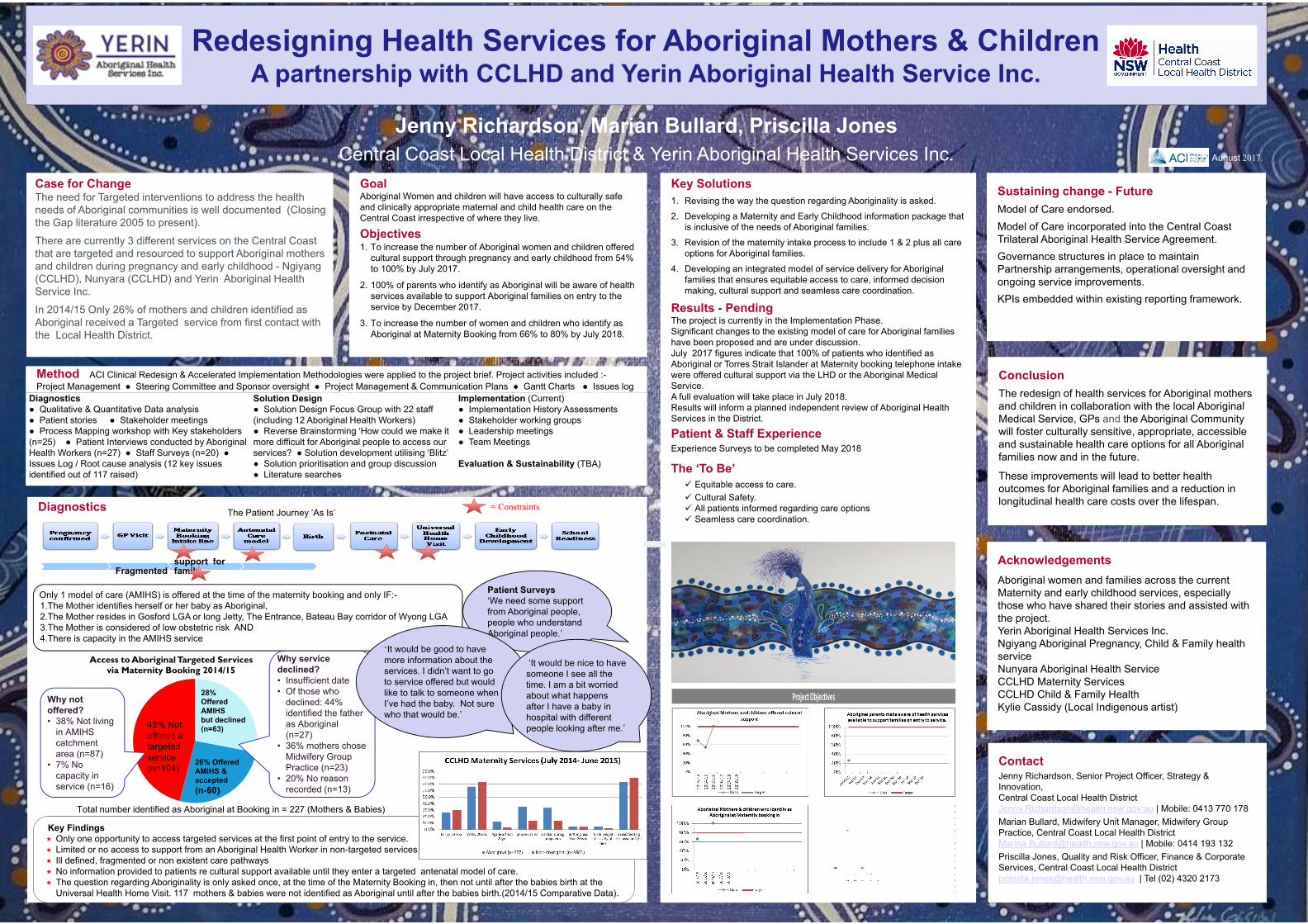
Objectives1. To increase the number of Aboriginal women and children offered
cultural support through pregnancy and early childhood from 54% to 100% by July 2017.
2. 100% of parents who identify as Aboriginal will be aware of health services available to support Aboriginal families on entry to the service by December 2017.
3. To increase the number of women and children who identify as Aboriginal at Maternity Booking from 66% to 80% by July 2018.
Sustaining change - FutureModel of Care endorsed.Model of Care incorporated into the Central Coast Trilateral Aboriginal Health Service Agreement.Governance structures in place to maintain Partnership arrangements, operational oversight and ongoing service improvements.KPIs embedded within existing reporting framework.
ContactJenny Richardson, Senior Project Officer, Strategy & Innovation,Central Coast Local Health [email protected] | Mobile: 0413 770 178Marian Bullard, Midwifery Unit Manager, Midwifery Group Practice, Central Coast Local Health [email protected] | Mobile: 0414 193 132Priscilla Jones, Quality and Risk Officer, Finance & Corporate Services, Central Coast Local Health [email protected] | Tel (02) 4320 2173
Case for ChangeThe need for Targeted interventions to address the health needs of Aboriginal communities is well documented (Closing the Gap literature 2005 to present).
There are currently 3 different services on the Central Coast that are targeted and resourced to support Aboriginal mothers and children during pregnancy and early childhood - Ngiyang (CCLHD), Nunyara (CCLHD) and Yerin Aboriginal Health Service Inc.
In 2014/15 Only 26% of mothers and children identified as Aboriginal received a Targeted service from first contact with the Local Health District.
Key Solutions1. Revising the way the question regarding Aboriginality is asked.
2. Developing a Maternity and Early Childhood information package that is inclusive of the needs of Aboriginal families.
3. Revision of the maternity intake process to include 1 & 2 plus all care options for Aboriginal families.
4. Developing an integrated model of service delivery for Aboriginal families that ensures equitable access to care, informed decision making, cultural support and seamless care coordination.
Results - PendingThe project is currently in the Implementation Phase. Significant changes to the existing model of care for Aboriginal families have been proposed and are under discussion.July 2017 figures indicate that 100% of patients who identified as Aboriginal or Torres Strait Islander at Maternity booking telephone intake were offered cultural support via the LHD or the Aboriginal Medical Service.A full evaluation will take place in July 2018. Results will inform a planned independent review of Aboriginal Health Services in the District.
Patient & Staff ExperienceExperience Surveys to be completed May 2018
The ‘To Be’ Equitable access to care. Cultural Safety. All patients informed regarding care options Seamless care coordination.
AcknowledgementsAboriginal women and families across the current Maternity and early childhood services, especially those who have shared their stories and assisted with the project.Yerin Aboriginal Health Services Inc.Ngiyang Aboriginal Pregnancy, Child & Family health serviceNunyara Aboriginal Health ServiceCCLHD Maternity ServicesCCLHD Child & Family HealthKylie Cassidy (Local Indigenous artist)
Jenny Richardson, Marian Bullard, Priscilla JonesCentral Coast Local Health District & Yerin Aboriginal Health Services Inc.
Diagnostics
Fragmentedsupport for family
Key Findings Only one opportunity to access targeted services at the first point of entry to the service. Limited or no access to support from an Aboriginal Health Worker in non-targeted services. Ill defined, fragmented or non existent care pathways No information provided to patients re cultural support available until they enter a targeted antenatal model of care. The question regarding Aboriginality is only asked once, at the time of the Maternity Booking in, then not until after the babies birth at the
Universal Health Home Visit. 117 mothers & babies were not identified as Aboriginal until after the babies birth.(2014/15 Comparative Data).
Patient Surveys‘We need some support from Aboriginal people, people who understand Aboriginal people.’
Access to Aboriginal Targeted Services via Maternity Booking 2014/15
46% Not offered a targeted service (n=104)
26% Offered AMIHS & accepted (n-60)
Why not offered? • 38% Not living
in AMIHS catchment area (n=87)
• 7% No capacity in service (n=16)
Why service declined?• Insufficient date• Of those who
declined: 44% identified the father as Aboriginal (n=27)
• 36% mothers chose Midwifery Group Practice (n=23)
• 20% No reason recorded (n=13)
28%Offered AMIHS but declined (n=63)
Total number identified as Aboriginal at Booking in = 227 (Mothers & Babies)
Only 1 model of care (AMIHS) is offered at the time of the maternity booking and only IF:-1.The Mother identifies herself or her baby as Aboriginal, 2.The Mother resides in Gosford LGA or long Jetty, The Entrance, Bateau Bay corridor of Wyong LGA 3.The Mother is considered of low obstetric risk AND 4.There is capacity in the AMIHS service
‘It would be good to have more information about the services. I didn’t want to go to service offered but would like to talk to someone when I’ve had the baby. Not sure who that would be.’
‘It would be nice to have someone I see all the time. I am a bit worried about what happens after I have a baby in hospital with different people looking after me.’
The Patient Journey ‘As Is’= Constraints
Project Objectives
August 2017.
Method ACI Clinical Redesign & Accelerated Implementation Methodologies were applied to the project brief. Project activities included :-Project Management ● Steering Committee and Sponsor oversight ● Project Management & Communication Plans ● Gantt Charts ● Issues log
Diagnostics ● Qualitative & Quantitative Data analysis● Patient stories ● Stakeholder meetings● Process Mapping workshop with Key stakeholders (n=25) ● Patient Interviews conducted by Aboriginal Health Workers (n=27) ● Staff Surveys (n=20) ●Issues Log / Root cause analysis (12 key issues identified out of 117 raised)
Solution Design● Solution Design Focus Group with 22 staff (including 12 Aboriginal Health Workers)● Reverse Brainstorming ‘How could we make it more difficult for Aboriginal people to access our services? ● Solution development utilising ‘Blitz’ ● Solution prioritisation and group discussion● Literature searches
Implementation (Current)● Implementation History Assessments● Stakeholder working groups ● Leadership meetings ● Team Meetings
Evaluation & Sustainability (TBA)