reducing improper payments in the medicare ffs - palmetto gba
TRANSCRIPT

Reducing Improper PaymentsReducing Improper Payments in the Medicare FFS Programin the Medicare FFS Program
Melanie Combs-Dyer, RN Deputy Director, Provider Compliance Group
Office of Financial Management
1

Roles of the Various MedicareRoles of the Various Medicare Improper Payment Review EntitiesImproper Payment Review Entities
Claim Selection Volume of Claims Purpose of Review
CERT Random Small (Approx. 50,000) To measure incidence of improper payments
MAC Targeted Variable upon number of
claims with improper payments for this provider
To prevent future improper payments
Recovery Auditors Targeted
Variable upon number of claims with improper
payments for this provider
To detect and correct past improper payments
ZPIC Targeted Variable upon number of
potentially fraudulent claims submitted by
provider
To identify potential fraud
OIG Targeted Varies on the focus of the OIG audit
To identify fraud and improper payments
2
The CERT ProcessThe CERT Process o Claims are selected randomly from all claims submitted for
payment during the reporting period
o The CERT Documentation Contractor requests medicalrecords
o Claim reviews are conducted by professional reviewers atthe CERT Review Contractor Determinations are made regarding whether the claim was paid
properly under Medicare coverage, coding, and billing rules and errorcategories are assigned
Claims determined to be paid incorrectly are scored as errors andpayments are adjusted
o Improper payment rates are calculated and reported www.cms.gov/cert
3
CERT Error CategoriesCERT Error Categories o No Documentation Errors No documentation submitted to support claim
o Insufficient Documentation Errors Documentation inadequate to determine medical necessity Required documentation elements missing (e.g., physician orders, legiblesignature)
o Medical Necessity ErrorsDocumentation adequate to show that the services/supplies billed were not medically necessary based on Medicare coverage policies
o Incorrect Coding ErrorsSubmitted documentation does not support codes billed
o Other
4
2011 CERT Findings2011 CERT Findings o Improper payment rate 8.6% ($28.8
Billion) o Downward adjustment applied for appeal
results and receipt of supporting documentation received after the reporting cutoff date Based on historical trends More accurate reflection of improper payment rate Adjustment approved by OIG
5

2011 CERT Findings2011 CERT Findings o High-error claim types: Inpatient hospital short stays (medical necessity
errors) Physician services (coding errors) DME (insufficient documentation errors)
6

CERT Historical TrendsCERT Historical Trends
Year Total Dollars Paid Adjusted Improper Payment Rate Improper Payments
2009 $285.1 10.8% $30.8B 2010 $326.4 9.1% $29.7B 2011 $336.4 8.6% $28.8B
7

OFM DemonstrationsOFM Demonstrations
o A/B Rebilling Demonstration
o Recovery Audit Program Prepayment Review Demonstration
o Prior Authorization of Power Mobility Devices (PMDs) Demonstration
Legal Authority: Under Section 402 (a)(1)(J) of the Social Security Amendments of 1967 (the Act) as amended, 42 U.S.C. §1395b-1(a)(1)(J), permits the Secretary to “develop or demonstrate improved methods for the investigation and prosecution of fraud in the provision of care or services under the health programs established by the Social Security Act.”
8

Recovery Audit Program Prepayment ReviewRecovery Audit Program Prepayment Review DemonstrationDemonstration
9
DemonstrationDemonstration Recovery Audit Program Prepayment ReviewRecovery Audit Program Prepayment Review
o Who and What Recovery Auditors will conduct prepayment review in addition to their current postpayment review work
Focus on claims with high improper payment rates Begin with reviews of short inpatient hospital stays (two days or less) Reviews may be expanded to other provider/claim types
oWhen Summer 2012 (lasting 3 years)
10

DemonstrationDemonstration Recovery Audit Program Prepayment ReviewRecovery Audit Program Prepayment Review
oWhere 7 fraud-prone states (CA, FL, IL, LA, MI, NY, and TX) + 4 states with high claims volumes for short inpatient hospital stays (MO, NC, OH, and PA) For a total of 11 states
11

DemonstrationDemonstration Recovery Audit Program Prepayment ReviewRecovery Audit Program Prepayment Review
oHow Will not replace MAC prepayment review Contractors will coordinate review areas so providers will not be reviewed by two different
contractors for the same issues Additional documentation request prepay limits same as postpayment limits Normal provider appeal rights apply Most claims will be off-limits from future post-payment reviews
oAdditional details will be released closer to implementation
12

DemonstrationDemonstration Recovery Audit Program Prepayment ReviewRecovery Audit Program Prepayment Review
o Why Allows for more reviews without increased funding. Contingency fees and administrative costs will be paid out of funds that CMS saves by denying improperly billed claims. Funds will be apportioned from amounts collected from Recovery Auditor postpayment reviews.
Focuses on error-prone claim types- inpatient hospital claims (especially short stays). Since inpatient claims are the biggest driver of the overall error rate, the error rate will decrease.
Uses current infrastructure and existing relationships between Medicare contractors and the provider community.
Reduces pay and chase syndrome by stopping improper payments before they are made.
13

Prior Authorization ofPrior Authorization of PMDsPMDs DemonstrationDemonstration
14

DemonstrationDemonstration Prior Authorization ofPrior Authorization of PMDsPMDs
o PMD have had high rates of improper payments
o This demonstration seeks to develop improved methods for the investigation and prosecution of fraud in order to protect the Medicare Trust Fund
15

DemonstrationDemonstration Prior Authorization ofPrior Authorization of PMDsPMDs
Included K0800 - K0805
All Power Operated Vehicles K0809 - K0812
All standard power wheelchairs K0813 - K0829
All Group 2 complex rehabilitative power wheelchairs K0835 - K0843
All Group 3 complex rehabilitative power wheelchairs without K0848 - K0855power options
All pediatric power wheelchairs K0890 - K0891
Miscellaneous power wheelchairs K0898
Excluded Group 3 complex rehabilitative power wheelchairs with power K0856 - K0864 options
16

DemonstrationDemonstration Prior Authorization ofPrior Authorization of PMDsPMDs
oSame Coverage Requirements as Today
oThe Prior Authorization demonstration: Does not create new documentation requirements for practitioners
and suppliers Simply requires the information be submitted earlier in the claims
process All Advanced Beneficiary Notice (ABN) procedures remain
unchanged
oCurrent requirements can be found on the DME MAC website
17

DemonstrationDemonstration Prior Authorization ofPrior Authorization of PMDsPMDs
o Where Beneficiaries residing in 7 error- and fraud-prone states: CA, IL, MI, NY,
FL, NC and TX (based beneficiary address) These 7 states: $262M of $606 M spent annually on PMDs (43%)
18
DemonstrationDemonstration Prior Authorization ofPrior Authorization of PMDsPMDs
o When Federal Register Notice during Summer 2012
announcing actual start date of demonstration
CMS expects The demonstration will apply for orders written on or after the start date. All states will start at approximately the same time Continuous Education of supplier, physicians/ practitioners and
beneficiaries
Demonstrations ends 3 years later in all 7 States
19

DemonstrationDemonstration Prior Authorization ofPrior Authorization of PMDsPMDs
oWhy Developing improved methods for the investigation and prosecution of
fraud Based on previous experience there is extensive evidence of DME fraud committed in these
states
Focuses on error-prone claim type Error rate for PMD: over 80%*
Uses private sector methodology to protect the Medicare Trust Funds Reduces pay and chase syndrome by stopping improper payments
before they are made
* According to the HHS OIG Spotlight On… Power Wheelchair (http://oig.hhs.gov/newsroom/news-releases/2011/wheelchair-medicare.asp)
20

DemonstrationDemonstration Prior Authorization ofPrior Authorization of PMDsPMDs
o CMS Adopted Changes in Response to Industry Feedback This demonstration was originally announced on
November 15, 2011 CMS published a Paperwork Reduction Act (PRA)
Package addressing both continued general medical review and the demonstration in December 2011 CMS received a number of comments about this
demonstration with the December 2011 PRA package
21
Prior Authorization ofPrior Authorization of PMDsPMDs DemonstrationDemonstration
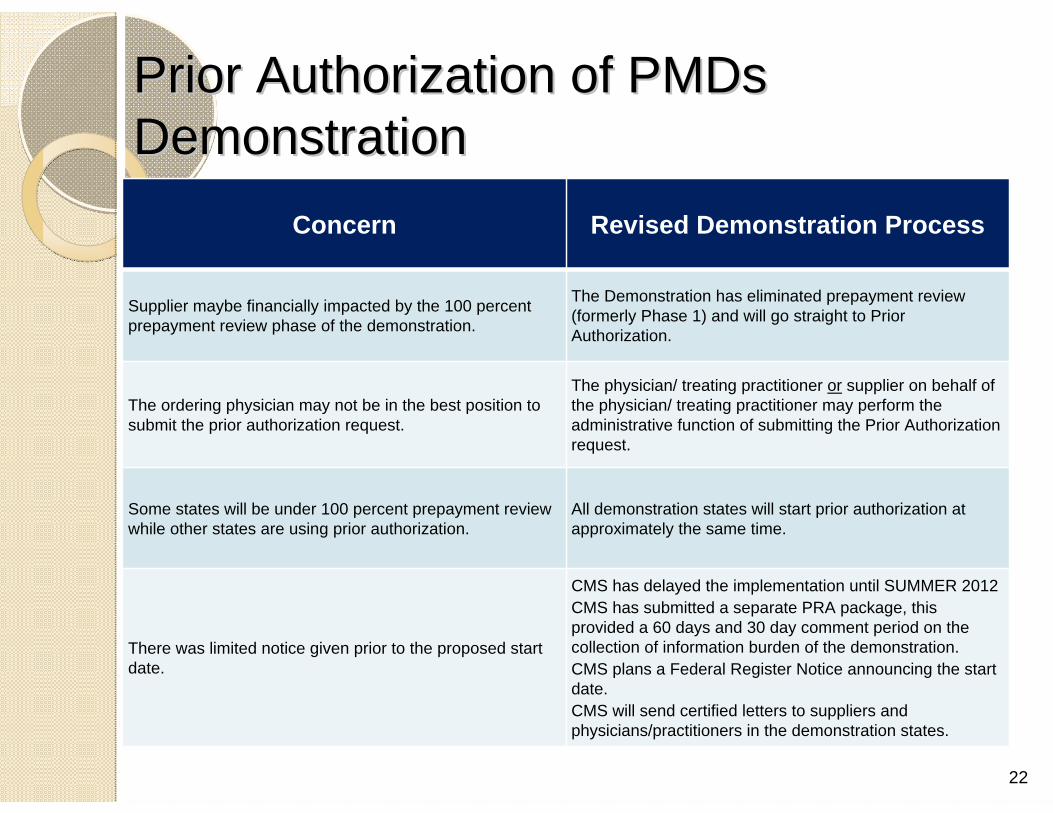
Concern Revised Demonstration Process
Supplier maybe financially impacted by the 100 percent prepayment review phase of the demonstration.
The Demonstration has eliminated prepayment review (formerly Phase 1) and will go straight to Prior Authorization.
The ordering physician may not be in the best position to submit the prior authorization request.
The physician/ treating practitioner or supplier on behalf of the physician/ treating practitioner may perform the administrative function of submitting the Prior Authorization request.
Some states will be under 100 percent prepayment review while other states are using prior authorization.
All demonstration states will start prior authorization at approximately the same time.
There was limited notice given prior to the proposed start date.
CMS has delayed the implementation until SUMMER 2012 CMS has submitted a separate PRA package, this provided a 60 days and 30 day comment period on the collection of information burden of the demonstration. CMS plans a Federal Register Notice announcing the start date. CMS will send certified letters to suppliers and physicians/practitioners in the demonstration states.
22
DemonstrationDemonstration Prior Authorization ofPrior Authorization of PMDsPMDs
o LCD requirements mandating physician/ treating practitioner origination must complete by the physician/ treating practitioner
o The supplier will still complete the detailed product description regardless of which entity is functioning as the submitter
o Ordering physician/practitioner or supplier performs the administrative function of submitting a prior authorization request to the DME MAC: Progress notes documenting the face-to-face exam 7 element order, Detailed product description Other medical documentation
23

DemonstrationDemonstration Prior Authorization ofPrior Authorization of PMDsPMDs
o Within 10 days, the DME MAC will either Affirm the prior authorization request Not affirm the prior authorization request Provide a detailed written explanation outlining which specific policy requirement(s)
was/were not met.
o The DME MAC will review request and postmark notification of a written decision within 10 days business days to: Physician/treating practitioner Beneficiary Supplier
o Submitter may re-submit (unlimited requests are allowed) DME MAC will review SUBSEQUENT requests within 20 days business days
o Suppliers should receive a Prior Authorization request decision from theDME MAC before the supplier delivers the item and submits the initial claim
24

Prior Authorization ofPrior Authorization of PMDsPMDs DemonstrationDemonstration
o In rare circumstances a 48 hour expedited review for emergencies In a situation where a practitioner indicates clearly with
rationale that the standard (routine) timeframe for a Prior Authorization Decision (10 days) could seriously jeopardize the beneficiary’s life or health, the contractor will conduct an expedited review. The expedited request must be accompanied by the required
supporting documentation for this request to be considered complete thus engaging the 48 hours for review. Inappropriate expedited requests may be downgraded to
standard requests.
25

Prior Authorization ofPrior Authorization of PMDsPMDs DemonstrationDemonstration
* Applies only to codes in the demonstration, not accessories and starts 3 months after the demonstration begins. 26
A prior authorization request is
The DME MAC decision is to
The supplier chooses to
The DME MAC will
1 Submitted Affirmative Submit a claim
Pay the claim (as long as all other requirements are met).
2 Submitted Non-affirmative A.Submit a claim
B.Fix and resubmit a PA request
Deny the claim.
3 Not submitted N/A
Submit a claim (Competitive Bid Supplier)
Sends ADR to supplier. Review the claim. If payable, pay at normal rate.
4 Not submitted N/A
Submits a claim (Non- Competitive Bid Supplier)
Sends ADR to supplier. Review the claim. If payable, pay at 75% of Medicare payment.*

DemonstrationDemonstration
Prior Authorization ofPrior Authorization of PMDsPMDs
The Face-to-Face Examination oState that the purpose of the face-to-face was to discuss the need for a PMD. oHistory of present condition and relevant past medical history, including: Symptoms that limit ambulation Diagnoses that are responsible for symptoms Medications or other treatment for symptoms Progression of ambulation difficulty over time Other diagnoses that may relate to ambulatory problems Distance patient can walk without stopping Pace of ambulation Ambulatory assistance currently used Change in condition that now requires a PMD Description of home setting and ability to perform ADLs in the home
oPhysical examination relevant to mobility needs, including: Height and weight Cardiopulmonary examination Arm and leg strength and range of motion
oNeurological examination, including: Gait Balance and coordination
Note: Not all elements listed apply to every patient. Professional discretion is necessary to determine which items are required as part of the face-to-face examination
27

DemonstrationDemonstration Prior Authorization ofPrior Authorization of PMDsPMDs
oUnacceptable Documentation of a Face-to-Face Examination (Will likely lead to a denial)
Mr. Smith is a male, age 72, with COPD, who over the last few weeks has been having more shortness of breath. He states he is unable to walk for me today because he is too tired. Therefore, he needs a PMD.
28

DemonstrationDemonstration Prior Authorization ofPrior Authorization of PMDsPMDs
oAcceptable Documentation of a Face-to-Face Examination Mr. Smith is a 72 yo male with COPD and presents today for a mobility evaluation for a PMD, worsening gradually over the past year despite compliant use of XYZ meds, nebulizers and rescue inhalers. PFT’s (attached) demonstrate the decline in lung function over the last 12 months. Now with the constant use of 2-3L NC O2 at home for the last month, he still can no longer walk to the bathroom, about 30 feet from his bed without significant SOB and overall discomfort. The kitchen is further from his bed. He says his bed/bath doorways and halls are wide enough for a scooter that will bring him to his toilet, sink and kitchen, all of which are on the same floor. VS 138/84, Ht rate 88 RR 16 at rest on 3L NC
Vision- sufficient to read newspaper with glasses on Cognition- OX3. Able to answer my questions without difficulty Ht XX Wt YY Ambulation – Sit to stand was done without difficulty. Patient attempted to ambulate 50’ in hallway, but needed to stop and rest 2 x’s before he could accomplish. HR at first stop point (about 25’) was 115 and RR was 32. Patient became slightly diaphoretic. Lung exam – Hyperresonant percussion and distant breath sounds throughout. Occ wheezes. Neuro- Hand grips of normal strength bilat. Patient able to maintain sit balance when laterally poked. Steps carefully around objects in the room. Alternative MAE equipment – Pt has attempted to use cane, walker or manual wheelchair unsuccessfully due to extreme fatigue with slight exertion described above. Assessment – Pt seems good candidate for a scooter to carry him the necessary distances in his home to use toilet/sink and kitchen facilities. Home seems…
29

DemonstrationDemonstration Prior Authorization ofPrior Authorization of PMDsPMDs
o The Valid 7-Element Order 1. Patient name 2. Description of item ordered
• “Power operated vehicle” • “Power wheelchair”, • “Power mobility device” • Or something more specific
3. Date of face-to-face examination 4. Diagnoses/conditions related to need for PMD 5. Length of need 6. Physician/practitioner signature 7. Date of physician/practitioner signature
30

DemonstrationDemonstration Prior Authorization ofPrior Authorization of PMDsPMDs
o Detailed Product Description The detailed product description must be completed by the supplier, and
reviewed and signed by the treating physician. It must contain:
Specific Healthcare Common Procedure Coding System (HCPCS) code for base and all options and accessories that will be separately billed;
Narrative description of the items or manufacturer name and model name/number;
Physician signature and date signed; and
Date stamp to document receipt date.
31
DemonstrationDemonstration
o
Prior Authorization ofPrior Authorization of PMDsPMDs
Resubmission and Appeals For non-affirmed Prior Authorization requests, unlimited
resubmissions are allowed For denied claims, all current appeal rights apply
o Beneficiary Impact The PMD benefit is not changing Beneficiaries will receive a notification of the decision
about their prior authorization request CMS encourages beneficiaries to use suppliers who
accept assignment
32

DemonstrationDemonstration Prior Authorization ofPrior Authorization of PMDsPMDs
o Physician Reimbursement Physician/Practitioner can bill G9156 after he/she submits an
initial Prior Authorization Request G-code is billed to the A/B MAC contractors with the Prior Authorization
tracking number Only one G-code may be billed per beneficiary per PMD even if the
physician/ practitioners must resubmit the request Code is not subject to co-insurance and deductible
oThis partially compensates physician/ practitioner for the additional time spent if he/she is the entity submitting a Prior Authorization request
33

Prior Authorization ofPrior Authorization of PMDsPMDs DemonstrationDemonstration
Summary Where Beneficiaries in CA, Il, MI, NY, NC,
Fl, TX
The demonstration will begin for:
Orders for PMD written Summer 2012
Submitted by Physician/ Practitioner or supplier on behalf of Physician/ Practitioner
Ends Summer 2015 (3 years after start date).
34

DemonstrationDemonstration Prior Authorization ofPrior Authorization of PMDsPMDs
For More Information Email the Prior Authorization Team [email protected]
CMS Demonstration Website go.cms.gov/PAdemo
FAQs https://questions.cms.hhs.gov/app/ho me keyword: PMD
Follow Us on Twitter @CMSGov (Look for #pmd_demonstration)
To receive Broadcast Emails Details coming soon
35

Contact informationContact information
For questions, please contact: [email protected]
For more information, please visit: http://go.cms.gov/cert-demos
36

Briefly Introducing ElectronicBriefly Introducing Electronic Submission of MedicalSubmission of Medical Documentation (Documentation (esMDesMD) to) to providersproviders
37

TodayToday’’s Paper Medical Documentation Processs Paper Medical Documentation Process
Doc’ n Request
Review ContractorLetter
Paper Medical Record
Provider
38
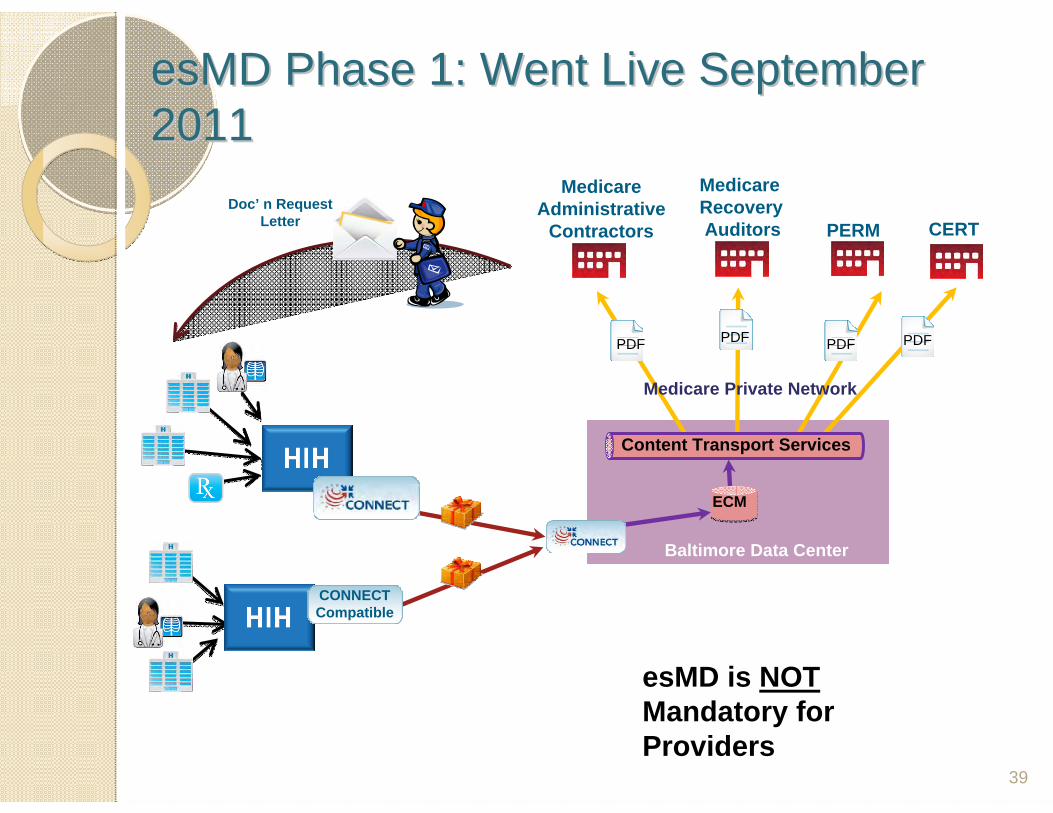
esMDesMD Phase 1: Went Live SeptemberPhase 1: Went Live September 20112011
CONNECT Compatible
Doc’ n Request Letter
Medicare Administrative
Contractors
Medicare Recovery Auditors PERM
Medicare Private Network
PDF PDF PDF
CERT
ECM
Baltimore Data Center
Content Transport Services
esMD is NOT Mandatory for Providers
39

Providers Who Want to Submit ViaProviders Who Want to Submit Via esMDesMD
STEP 1: Find out if your Review Contractors accept esMD
STEP 2: Obtain access to an esMD “gateway” (esMD gateway technology keeps the medical records safe & secure as they are moving from point A to point B)
40

Step 1: CMS Review Contractors that AcceptStep 1: CMS Review Contractors that Accept esMDesMD Approved CMS Review Contractors
Region A Medicare Recovery Auditor (DCS)
Region B Medicare Recovery Auditor (CGI)
Region C Medicare Recovery Auditor (Connolly)
Region D Medicare Recovery Auditor (HDI)
Medicare Administrative J1 (Palmetto GBA)
Medicare Administrative J3 (Noridian)
Medicare Administrative J4 (Trailblazer)
Medicare Administrative J5 (WPS)
Medicare Administrative J9 (First Coast)
Medicare Administrative J10 (Cahaba)
Medicare Administrative J11 (Palmetto)
Medicare Administrative J12 (Novitas Solutions)
Medicare Administrative J13 (NGS)
Medicare Administrative J14 (NHIC)
Medicare Administrative J15 (CGS)
DME Medicare Administrative JA (NHIC)
DME Medicare Administrative JB (NGS)
DME Medicare Administrative JC (CGS)
DME Medicare Administrative JD (NAS)
Comprehensive Error Rate Testing (CERT)
Program Error Rate Measurement (PERM)
Planning for Summer 2012
ZPIC Zone 1 (SGS)
ZPIC Zone 7 (SGS)
Medicare Administrative J8 (WPS)
Medicare Administrative JH (Novitas Solutions)
Legacy Contractor Title 18 J6 (NGS)
Medicare Administrative JF (Noridian) will be replacing J2 and J3
For updated list, visit : www.cms.gov/esMD .
41
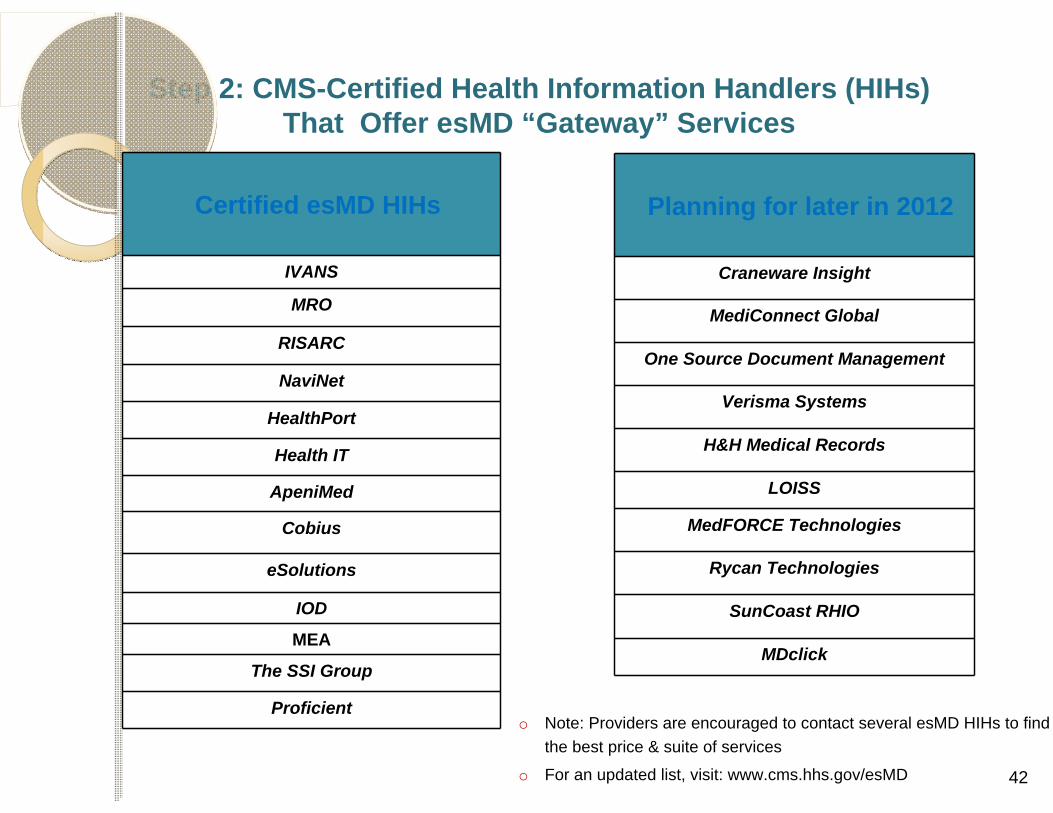
Step 2: CMS-Certified Health Information Handlers (HIHs) That Offer esMD “Gateway” Services
Certified esMD HIHs
IVANS
MRO
RISARC
NaviNet
HealthPort
Health IT
ApeniMed
Cobius
eSolutions
IOD
MEA
The SSI Group
Proficient
Planning for later in 2012
Craneware Insight
MediConnect Global
One Source Document Management
Verisma Systems
H&H Medical Records
LOISS
MedFORCE Technologies
Rycan Technologies
SunCoast RHIO
MDclick
o Note: Providers are encouraged to contact several esMD HIHs to find the best price & suite of services
o For an updated list, visit: www.cms.hhs.gov/esMD 42

InitiativeInitiative Electronic Clinical TemplateElectronic Clinical Template
o Today’s esMD system accepts medicalrecords only in pdf format
o Future: Accept medical records in “structured” format Start with Progress Notes for PMD face to face
evaluation CMS will work with ONC to form a public
workgroup to decide what the data elementsshould be First draft of data element list is posted to CMS
website
43

InitiativeInitiative Electronic Clinical TemplateElectronic Clinical Template
oDraft of data elements: go.cms.gov/eclinicaltemplate
44

Electronic Clinical TemplateElectronic Clinical Template –– First DraftFirst Draft
45

InitiativeInitiative Electronic Clinical TemplateElectronic Clinical Template
The PMD Electronic Clinical Template ODFcalls are scheduled as follows:
April 10, 2012 (2 p.m. - 3 p.m. EST)- (HELD)
June 14, 2012 (2 p.m. - 3 p.m. EST) - (HELD)
July 10, 2012 (2 p.m. - 3 p.m. EST) - (HELD)
September 25, 2012 (2 p.m. - 3 p.m. EST) - Dial in # TBD
46
QuestionsQuestions
47