reg-eaaci taskforce report
TRANSCRIPT
REG-EAACI TASKFORCE REPORT
REG SUMMIT 2016, LYON, FRANCE, 16 APRIL
SESSION: ‘INFLUENCING’ Guideline Development: the REG/EAACI Taskforce Reports
TIME: 11.45AM-12.45PM
Presenters: Nicolas Roche (Hopital de l’Hotel Dieu, Paris) &
Jon Campbell (Skaggs School of Pharmacy, Denver, Colorado)
On behalf of: Nikos Papadopoulos, Leif Bjermer, Guy Brusselle, Alison Chisholm, Jerry Krishnan, Zoe Mitchel, David Price,
Mike Thomas, Eric van Ganse, Maarten van den Berge helped by Sarah Acaster and Katy Gallop
—
Taskforce Members
Leads: Nicolas Roche & Jon Campbell
• David Price
• Mike Thomas
• Eric van Ganse
• George Christoff
• Guy Brusselle
• Jennifer Quint
• Jerry Krishnan
• Leif Bjermer
• Nikos Papadopoulos
• Maarten Van Den Berge
Background
• RCTs are not sufficient to provide holistic
evidence
• Real-life studies are subject to many sources of
biases
Where do observational studies fit in?
• (Almost) Everybody agrees on:
o Pitfalls of RCTs
o Need for real-life data
• Guideline developers are often reluctant to include real-life data
• Quality issues
• Need to help readers
• Quality assessment
o Tools required
o Remaining difficulties in quality assessment (need to help
reviewers)
o Need to improve reporting
SETTING AND DEFINING STANDARDSCREATING A LEVEL PLAYING FIELD TO HELP RAISE
(AND GUIDE ASSESSMENT OF)
THE QUALITY OF REAL-LIFE RESEARCH
ATS 2013
—
Goal
• Create a level playing field and solid foundations
for future research that will:
o Standardize the field
o Enable benchmarking
o Assist in assessing the quality of real-life data
(including their potential value to clinical
practice guidelines)
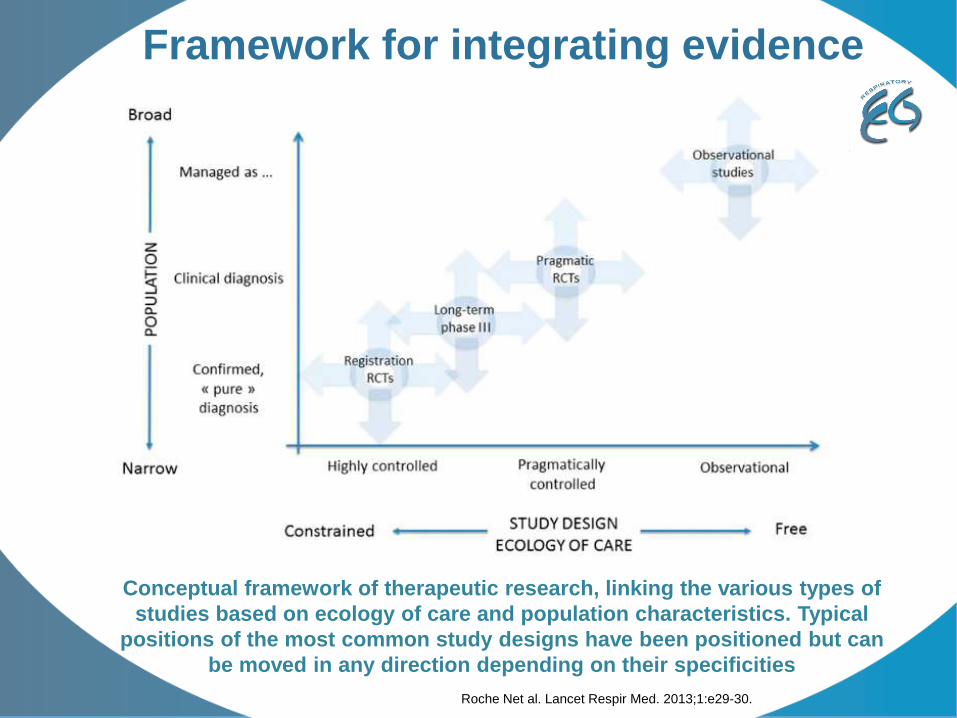
Conceptual framework of therapeutic research, linking the various types of
studies based on ecology of care and population characteristics. Typical
positions of the most common study designs have been positioned but can
be moved in any direction depending on their specificities
Roche Net al. Lancet Respir Med. 2013;1:e29-30.
Framework for integrating evidence
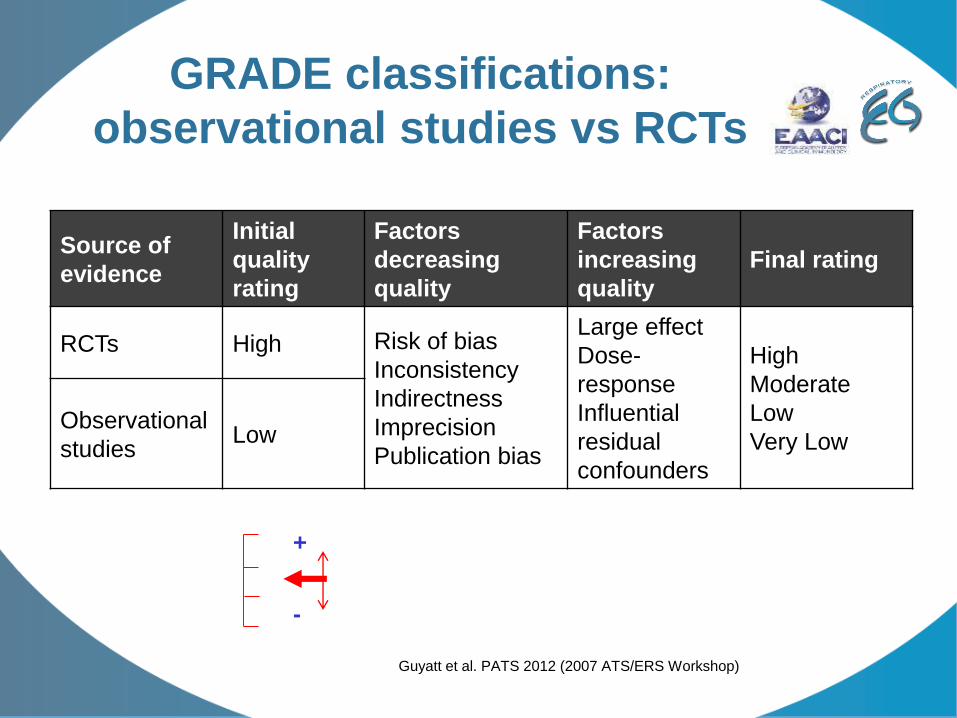
GRADE classifications:
observational studies vs RCTs
Source of
evidence
Initial
quality
rating
Factors
decreasing
quality
Factors
increasing
quality
Final rating
RCTs High Risk of bias
Inconsistency
Indirectness
Imprecision
Publication bias
Large effect
Dose-
response
Influential
residual
confounders
High
Moderate
Low
Very LowObservational
studiesLow
Guyatt et al. PATS 2012 (2007 ATS/ERS Workshop)
+
-
Stakeholders
• Researchers
• Database designers / promotors
• Guidelines developers
• Policy makers
• Reviewers (journals, projects)
• Readers
• …
Aims & Objectives
• Conduct a systematic critical review of the real-life
asthma literature published between 2004/13
o Restricted to comparative effectiveness research
• Describe the quality of currently available real-life
research in asthma
• Highlight studies worthy of possible integration into
asthma-related guidelines and policy decisions
• Recommend quality targets for the future
o And topics to address in future observational CER studies
Strategy
• Agree on / build a quality assessment tool
• Define a search strategy, perform a review of the
literature
• Apply the quality assessment tool on retrieved articles
• Synthesise, discuss and conclude on quality, and potential
influence of current comparative effectiveness
literature on future guideline and/or need for additional
studies
Taskforce Timelines
2014-2015
• Task 1: literature search to identify asthma real-life
research articles (chair: N Roche)
• Task 2: construction of a dedicated quality assessment
tool (chair : J Campbell)
2015-2016
• Task 3: quality assessment of identified asthma real-life
research articles
• Task 4: report
• Task 5: disseminate
2014-2015
Task 1 (literature search):
• Formal targeted literature search
• Poll among Taskforce members and REG members
• Limit retrieved papers to top priority (4) PICOT
questions
Task 2 (quality assessment tool):
• Combination of available tools
• Discussion and final version of the quality
assessment tool
2015-2016
Task 3 (quality assessment):
• Quality assessment of articles identified from the literature search
• Conducted by members of the Taskforce and REG-EAACI network
reviewers
• Results of quality assessment used to determine which papers could
be used to complement results of RCTs and inform guidelines.
Task 4 (dissemination):
• Results to be presented at EAACI meeting
• Publication (submission ~Q3 2016; journals: Allergy and CTA):
o A review article (detailed results of quality assessment)
o A position paper (information of guidelines)
QUALITY ASSESSMENT TOOL
DEVELOPMENT
JON CAMPBELL: Skaggs School of Pharmacy, Denver, Colorado
—
Development Phases
• Phase I: literature review
• Phase II: Initial tool creation
• Phase III: Taskforce review and pilot
• Phase IV: Larger Pilot & tool finalization/minor
modifications
• Phase V: tool finalization for use – development
of an online tool
Phase I: Literature Review
Many Study Assessment Tools Exist
• STROBE Statement: Checklist of items that should be included in reports of
observational studies
• Quality standards for real-world research: List of quality criteria for
observational database comparative studies (Roche et al)
• Report of the ISPOR Task Force on retrospective databases: A checklist for
retrospective database studies
• GRACE Checklist: Quality of observational cohort studies for decision making
support
• ENCePP Checklist: checklist for study protocols for pharmacoepidemiology
• Standards in the conduct of registry studies for patient-centered
outcomes research (PCORI): review of existing guidelines and literature to
develop methodological standards
Phase I: Literature Review
• Purpose of most existing tools:
o Primarily to provide standardization of best practice and
reporting of observational / comparative effectiveness
research studies.
• Purpose of REG-EAACI Taskforce tool:
o Decision aid to assess whether or not a study provides
evidence that could inform future guidelines (yes or no). If
yes, the tool’s criteria can aid in describing any particular
strengths or limitations of the evidence.
Phase I: Literature Review
• A synthesis of existing tools was visually
presented in tabular form.
o Overlap was assessed across tools
• Taskforce decided to focus on merging two
existing tools
o Roche and colleagues
o ISPOR task force
– ISPOR task force tool included many of the
existing tools into its development
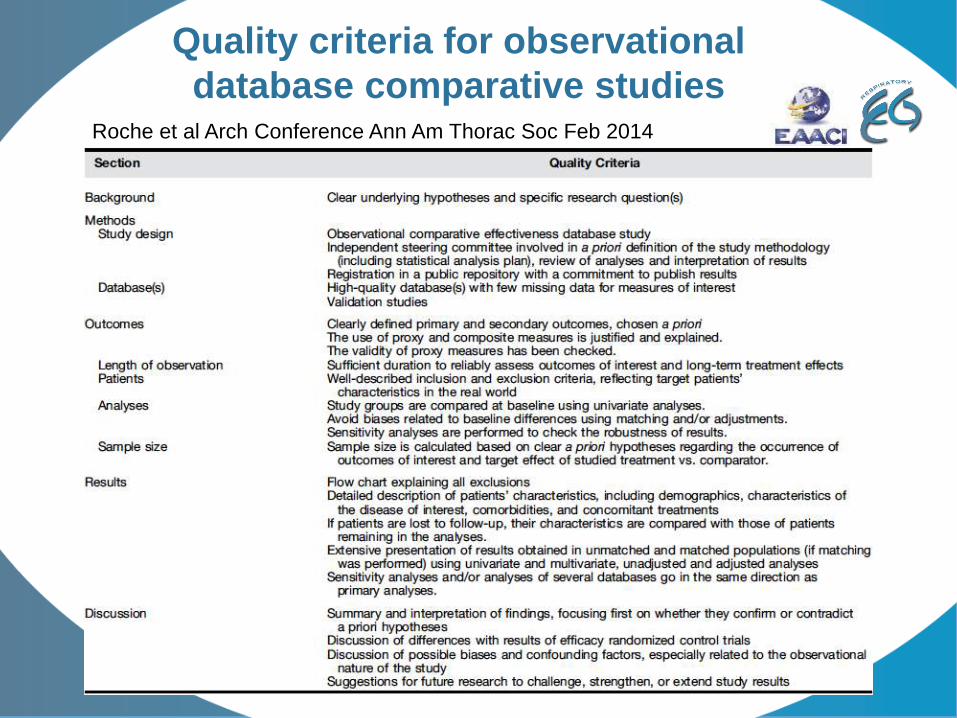
Quality criteria for observational
database comparative studiesRoche et al Arch Conference Ann Am Thorac Soc Feb 2014
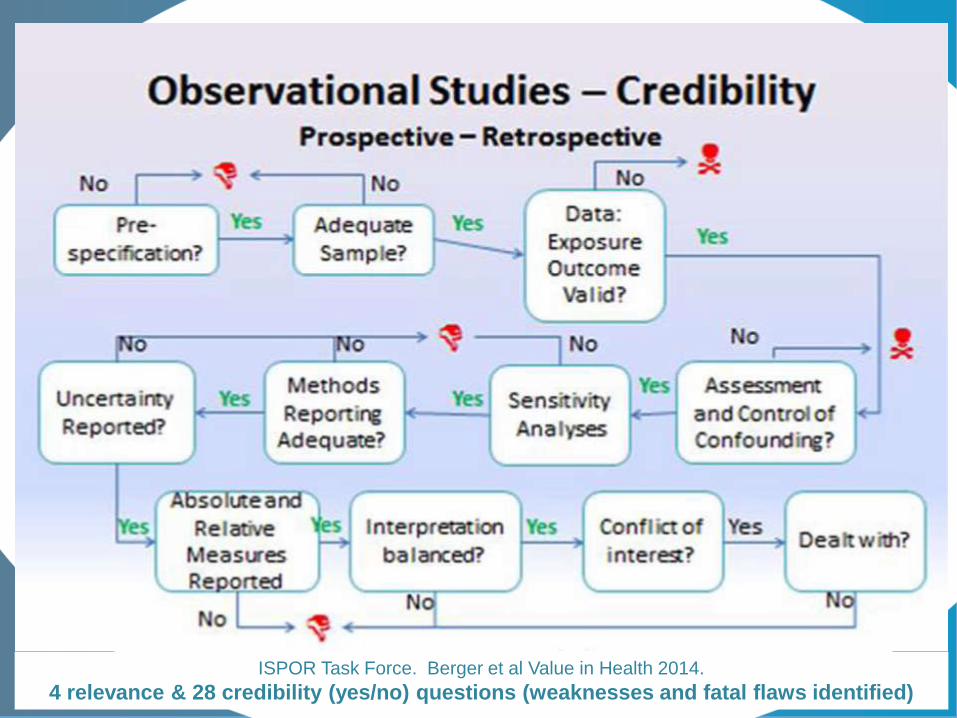
ISPOR Task Force. Berger et al Value in Health 2014.
4 relevance & 28 credibility (yes/no) questions (weaknesses and fatal flaws identified)
Phase 1: Roche (REG) and
Berger (ISPOR)
• Roche has 24 relevance and credibility questions
• ISPOR starts with 4 relevance questions and then
moves to 28 credibility questions
o Much overlap between two on domains and items
o Both are yes/no items; ISPOR has a “can’t answer”
option (NA, not reported, not enough info, not enough
training to answer).
o ISPOR has the concept of fatal flaws and weaknesses
Phase II: Initial Tool Creation
• Synthesis of pre-existing quality
recommendations to develop a first draft
Taskforce Quality Assessment Tool
• Recognition that asthma specificity is not
necessary and provides greater tool utility
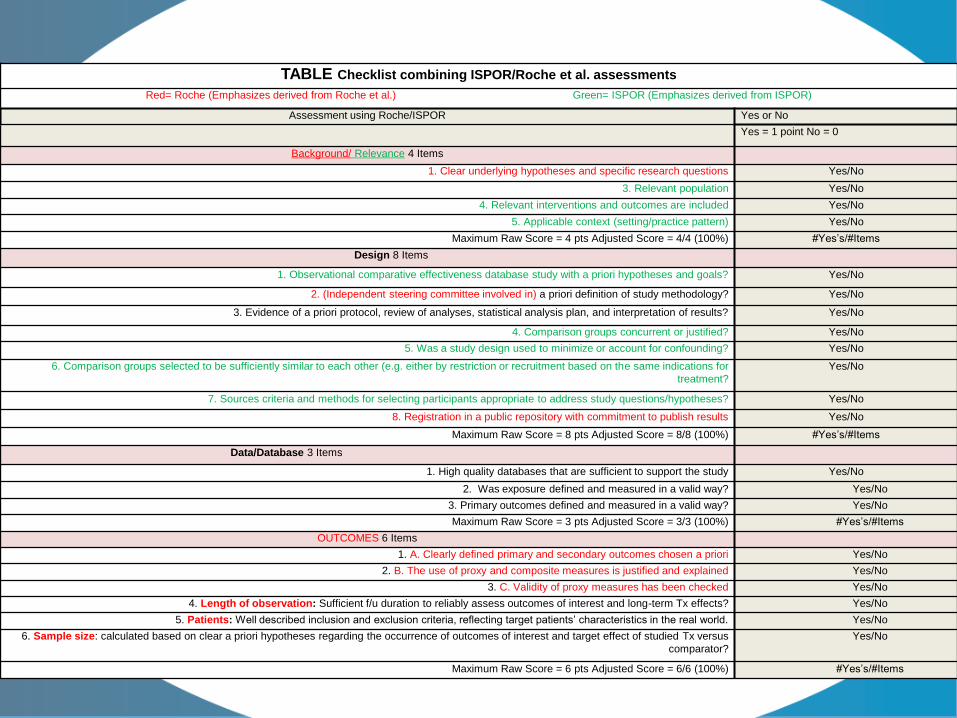
TABLE Checklist combining ISPOR/Roche et al. assessments
Red= Roche (Emphasizes derived from Roche et al.) Green= ISPOR (Emphasizes derived from ISPOR)
Assessment using Roche/ISPOR Yes or No
Yes = 1 point No = 0
Background/ Relevance 4 Items
1. Clear underlying hypotheses and specific research questions Yes/No
3. Relevant population Yes/No
4. Relevant interventions and outcomes are included Yes/No
5. Applicable context (setting/practice pattern) Yes/No
Maximum Raw Score = 4 pts Adjusted Score = 4/4 (100%) #Yes’s/#Items
Design 8 Items
1. Observational comparative effectiveness database study with a priori hypotheses and goals? Yes/No
2. (Independent steering committee involved in) a priori definition of study methodology? Yes/No
3. Evidence of a priori protocol, review of analyses, statistical analysis plan, and interpretation of results? Yes/No
4. Comparison groups concurrent or justified? Yes/No
5. Was a study design used to minimize or account for confounding? Yes/No
6. Comparison groups selected to be sufficiently similar to each other (e.g. either by restriction or recruitment based on the same indications for
treatment?
Yes/No
7. Sources criteria and methods for selecting participants appropriate to address study questions/hypotheses? Yes/No
8. Registration in a public repository with commitment to publish results Yes/No
Maximum Raw Score = 8 pts Adjusted Score = 8/8 (100%) #Yes’s/#Items
Data/Database 3 Items
1. High quality databases that are sufficient to support the study Yes/No
2. Was exposure defined and measured in a valid way? Yes/No
3. Primary outcomes defined and measured in a valid way? Yes/No
Maximum Raw Score = 3 pts Adjusted Score = 3/3 (100%) #Yes’s/#Items
OUTCOMES 6 Items
1. A. Clearly defined primary and secondary outcomes chosen a priori Yes/No
2. B. The use of proxy and composite measures is justified and explained Yes/No
3. C. Validity of proxy measures has been checked Yes/No
4. Length of observation: Sufficient f/u duration to reliably assess outcomes of interest and long-term Tx effects? Yes/No
5. Patients: Well described inclusion and exclusion criteria, reflecting target patients’ characteristics in the real world. Yes/No
6. Sample size: calculated based on clear a priori hypotheses regarding the occurrence of outcomes of interest and target effect of studied Tx versus
comparator?
Yes/No
Maximum Raw Score = 6 pts Adjusted Score = 6/6 (100%) #Yes’s/#Items
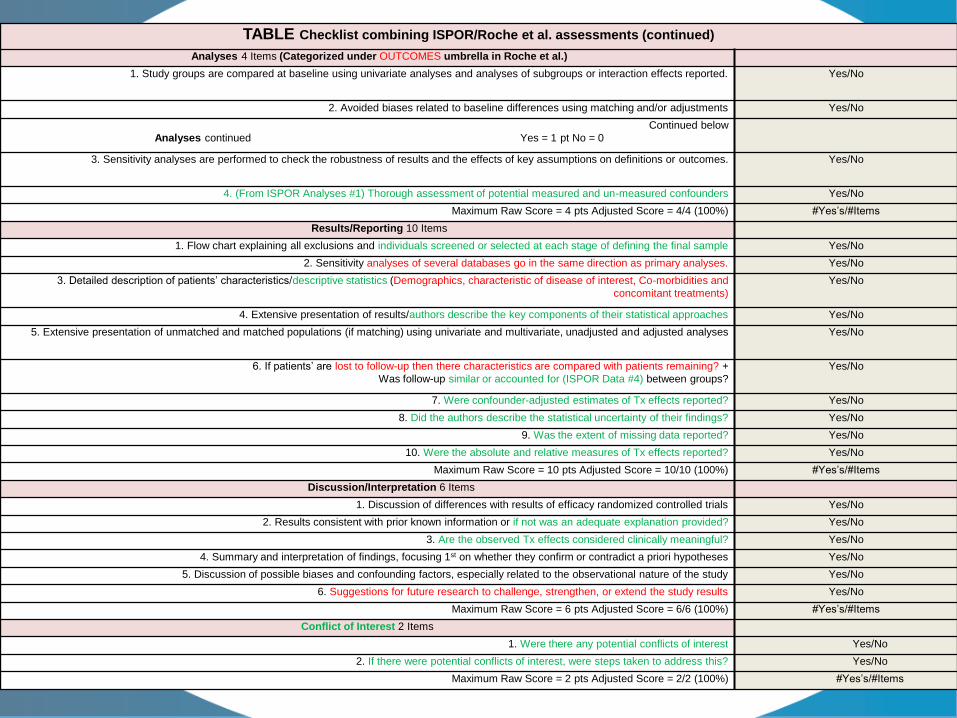
TABLE Checklist combining ISPOR/Roche et al. assessments (continued)
Analyses 4 Items (Categorized under OUTCOMES umbrella in Roche et al.)
1. Study groups are compared at baseline using univariate analyses and analyses of subgroups or interaction effects reported. Yes/No
2. Avoided biases related to baseline differences using matching and/or adjustments Yes/No
Continued below
Analyses continued Yes = 1 pt No = 0
3. Sensitivity analyses are performed to check the robustness of results and the effects of key assumptions on definitions or outcomes. Yes/No
4. (From ISPOR Analyses #1) Thorough assessment of potential measured and un-measured confounders Yes/No
Maximum Raw Score = 4 pts Adjusted Score = 4/4 (100%) #Yes’s/#Items
Results/Reporting 10 Items
1. Flow chart explaining all exclusions and individuals screened or selected at each stage of defining the final sample Yes/No
2. Sensitivity analyses of several databases go in the same direction as primary analyses. Yes/No
3. Detailed description of patients’ characteristics/descriptive statistics (Demographics, characteristic of disease of interest, Co-morbidities and
concomitant treatments)
Yes/No
4. Extensive presentation of results/authors describe the key components of their statistical approaches Yes/No
5. Extensive presentation of unmatched and matched populations (if matching) using univariate and multivariate, unadjusted and adjusted analyses Yes/No
6. If patients’ are lost to follow-up then there characteristics are compared with patients remaining? +
Was follow-up similar or accounted for (ISPOR Data #4) between groups?
Yes/No
7. Were confounder-adjusted estimates of Tx effects reported? Yes/No
8. Did the authors describe the statistical uncertainty of their findings? Yes/No
9. Was the extent of missing data reported? Yes/No
10. Were the absolute and relative measures of Tx effects reported? Yes/No
Maximum Raw Score = 10 pts Adjusted Score = 10/10 (100%) #Yes’s/#Items
Discussion/Interpretation 6 Items
1. Discussion of differences with results of efficacy randomized controlled trials Yes/No
2. Results consistent with prior known information or if not was an adequate explanation provided? Yes/No
3. Are the observed Tx effects considered clinically meaningful? Yes/No
4. Summary and interpretation of findings, focusing 1st on whether they confirm or contradict a priori hypotheses Yes/No
5. Discussion of possible biases and confounding factors, especially related to the observational nature of the study Yes/No
6. Suggestions for future research to challenge, strengthen, or extend the study results Yes/No
Maximum Raw Score = 6 pts Adjusted Score = 6/6 (100%) #Yes’s/#Items
Conflict of Interest 2 Items
1. Were there any potential conflicts of interest Yes/No
2. If there were potential conflicts of interest, were steps taken to address this? Yes/No
Maximum Raw Score = 2 pts Adjusted Score = 2/2 (100%) #Yes’s/#Items
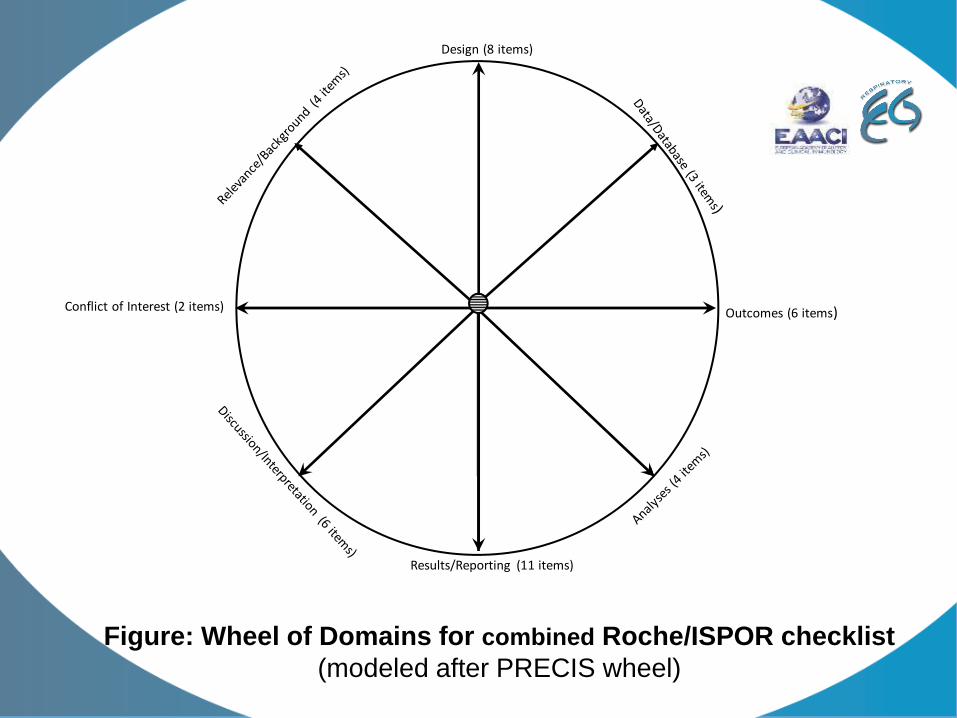
Design (8 items)
Outcomes (6 items)
Results/Reporting (11 items)
Conflict of Interest (2 items)
Figure: Wheel of Domains for combined Roche/ISPOR checklist
(modeled after PRECIS wheel)
Phase II: Initial Tool Creation
• The initial tool included:
o 13 primary quality criteria
– All primary items must be satisfied to recommend a study that
could inform future guidelines
o 14 secondary criteria
o Across 8 domains:
– Background/relevance, design, data, measures, analyses,
results/reporting, discussion/interpretation, conflict of interest
• Tool refined, based on:
o Task Force Members votes for items to keep/remove/merge
Phase III: Within taskforce pilot
• Methods:
o 6 papers distributed to 9 taskforce members
o Two reviewer groups (1 x group of 5 and 1 x group of 4)
o Each group member scored / appraised 3 papers
o Calculation of an “agreement rate” (per item & per domain – split by primary and
supporting “secondary” domains)
o Global assessment = paper of sufficient quality to inform guideline development
(Y/N) required fulfilment of all primary criteria and agreement by ALL raters
• Results:
o Overall agreement at ~50% level; agreement appeared to be random
• Action:
o Revise tool based on taskforce feedback to
– Simplify it, and
– Remove areas of potential ambiguity/subjectivity.
o Conduct an extended pilot, using a wider rater group, to see whether the tool
revisions had improved agreement rates.
Phase IV: Larger Pilot & tool
finalization/minor modifications
• Methods:
o 22 x raters involved in total
o 3 x rater groups:
– A, B, C (2 x groups of 7; 1 x group of 8)
– Members of groups A and B received 2 papers on
intervention adherence / persistence
– Members of group C received 2 papers on ICS particle
size / formulation
for quality assessment using the revised tool
o Agreement was evaluated across each field for each
rater group, separately and in total
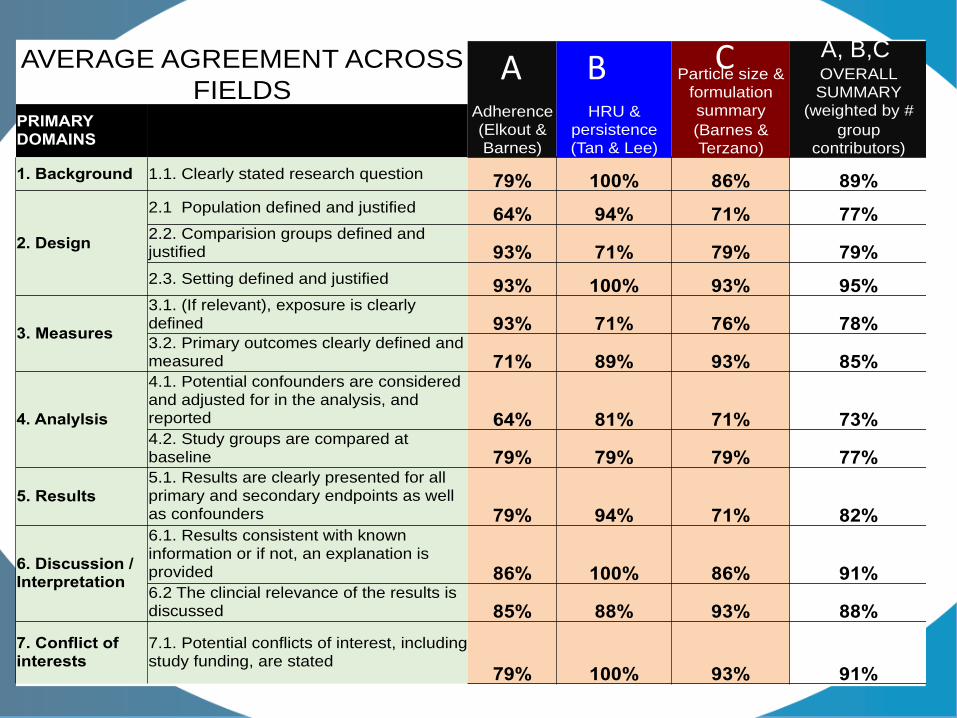
AVERAGE AGREEMENT ACROSS
FIELDS Adherence (Elkout & Barnes)
HRU & persistence (Tan & Lee)
Particle size & formulation summary
(Barnes & Terzano)
OVERALL SUMMARY
(weighted by #
group contributors)
PRIMARY DOMAINS
1. Background 1.1. Clearly stated research question 79% 100% 86% 89%
2. Design
2.1 Population defined and justified 64% 94% 71% 77% 2.2. Comparision groups defined and justified 93% 71% 79% 79%
2.3. Setting defined and justified 93% 100% 93% 95%
3. Measures
3.1. (If relevant), exposure is clearly defined 93% 71% 76% 78% 3.2. Primary outcomes clearly defined and measured 71% 89% 93% 85%
4. Analylsis
4.1. Potential confounders are considered and adjusted for in the analysis, and reported 64% 81% 71% 73% 4.2. Study groups are compared at baseline 79% 79% 79% 77%
5. Results
5.1. Results are clearly presented for all primary and secondary endpoints as well as confounders 79% 94% 71% 82%
6. Discussion / Interpretation
6.1. Results consistent with known information or if not, an explanation is provided 86% 100% 86% 91% 6.2 The clincial relevance of the results is discussed 85% 88% 93% 88%
7. Conflict of interests
7.1. Potential conflicts of interest, including study funding, are stated
79% 100% 93% 91%
A B C A, B,C
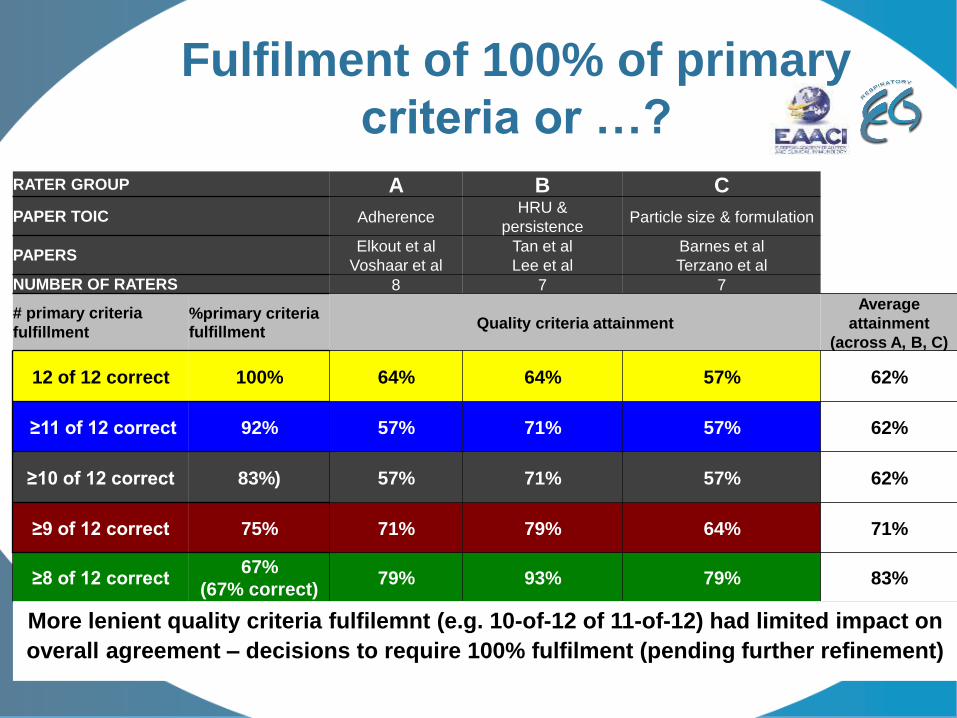
Fulfilment of 100% of primary
criteria or …?
RATER GROUP A B C
PAPER TOIC AdherenceHRU &
persistenceParticle size & formulation
PAPERSElkout et al
Voshaar et al
Tan et al
Lee et al
Barnes et al
Terzano et al
NUMBER OF RATERS 8 7 7
# primary criteria
fulfillment
%primary criteria fulfillment
Quality criteria attainment
Average
attainment
(across A, B, C)
12 of 12 correct 100% 64% 64% 57% 62%
≥11 of 12 correct 92% 57% 71% 57% 62%
≥10 of 12 correct 83%) 57% 71% 57% 62%
≥9 of 12 correct 75% 71% 79% 64% 71%
≥8 of 12 correct67%
(67% correct)79% 93% 79% 83%
More lenient quality criteria fulfilemnt (e.g. 10-of-12 of 11-of-12) had limited impact on
overall agreement – decisions to require 100% fulfilment (pending further refinement)
Phase IV: Larger Pilot & tool
finalization/minor modifications
• Remaining disagreement: Reviewer feedback suggested some of
the persisting disagreement was the result of:
o Multiple “sub-questions” within some of the appraisal criteria,
e.g. “Potential conflicts of interest, including study funding, are
stated”, which contains a question about author conflicts of
interest and also the specific study funding. Such questions lead
to greater potential for disagreement between raters.
o Poorly written papers (even though those selected for evaluation
were of above-average quality)
• Action: Each tool criteria was reviewed by the taskforce members
once more and any remaining ambiguities removed. This was
undertaken at the Amsterdam Taskforce Meeting.
Phase V: tool finalization for use,
development of an online tool
• Once the Excel version of the tool had been
approved by the taskforce, it was converted into
a Google form.
• An online tool offered:
o Smoother user/rate experience,
o Minimized opportunities for data mis-entry, AND
o Allowed automated collation into an online
spreadsheet and delivered an overview of responses
to each question.
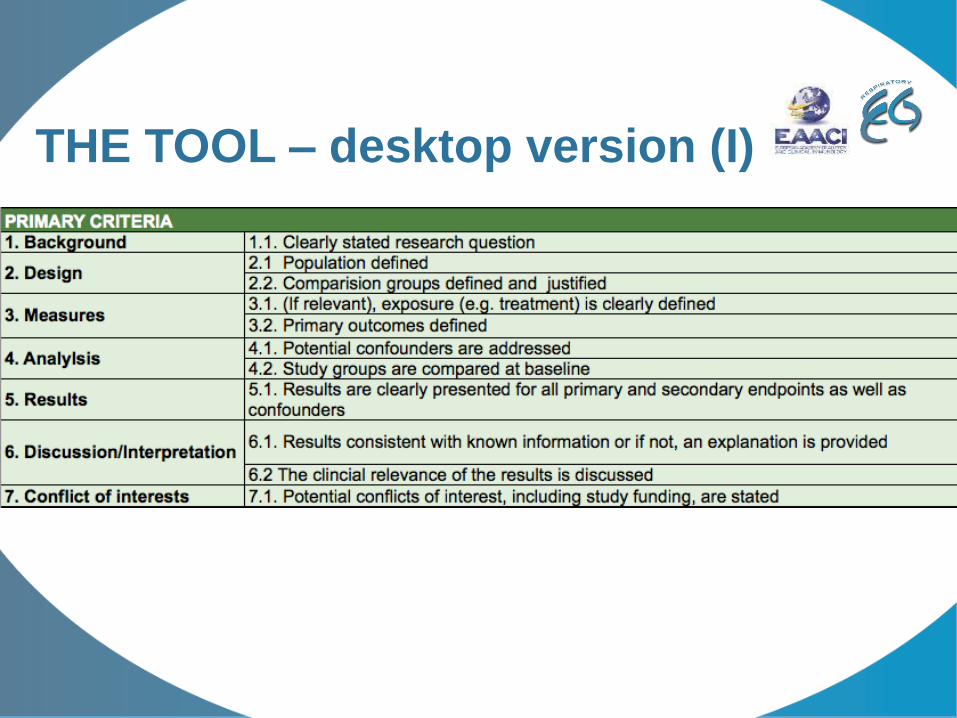
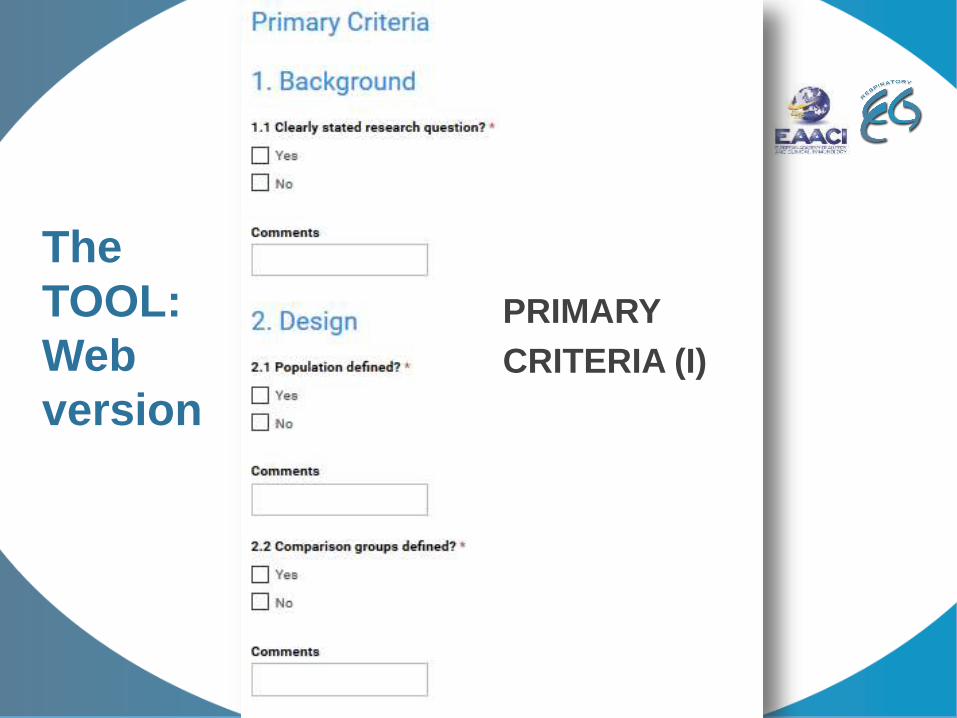
THE TOOL – desktop version (I)
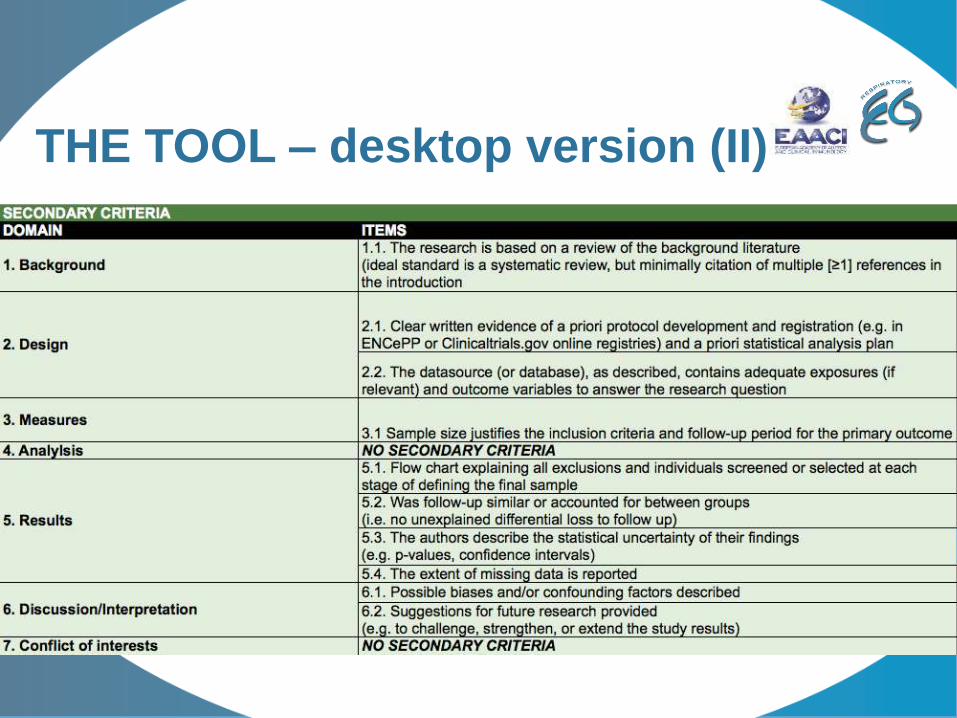
THE TOOL – desktop version (II)
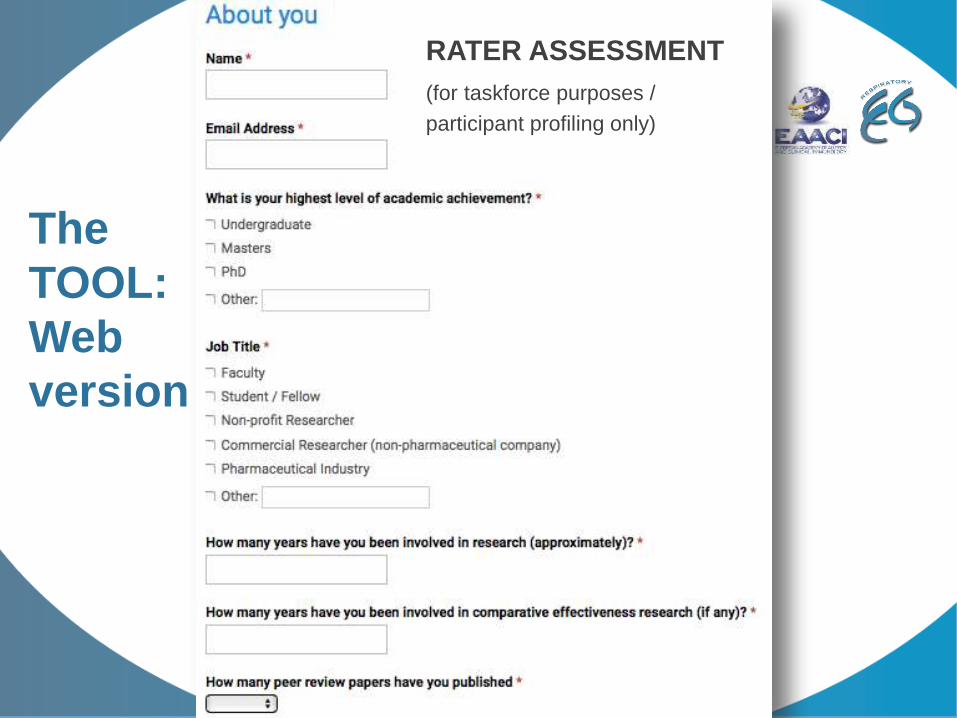
The
TOOL:
Web
version
RATER ASSESSMENT
(for taskforce purposes /
participant profiling only)
The
TOOL:
Web
version
PRIMARY
CRITERIA (I)
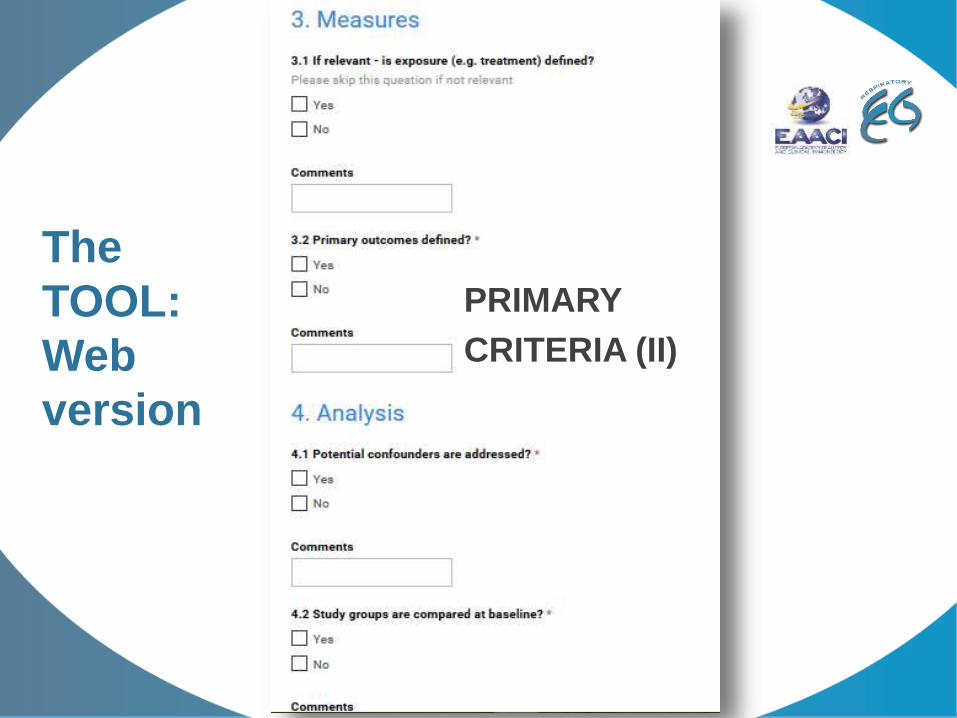
The
TOOL:
Web
version
PRIMARY
CRITERIA (II)
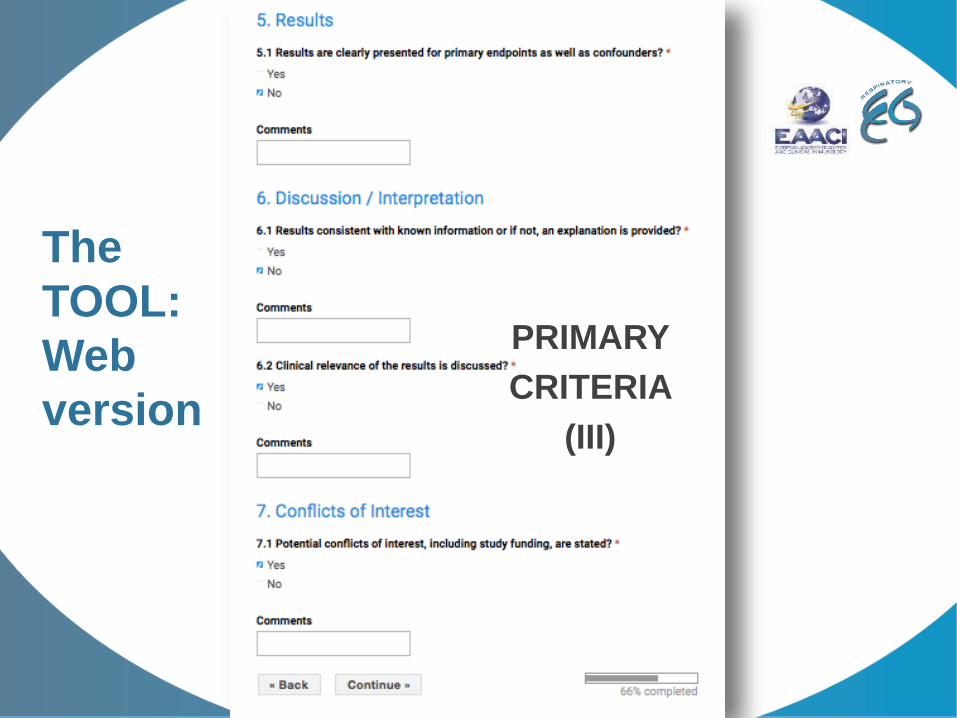
The
TOOL:
Web
version
PRIMARY
CRITERIA
(III)
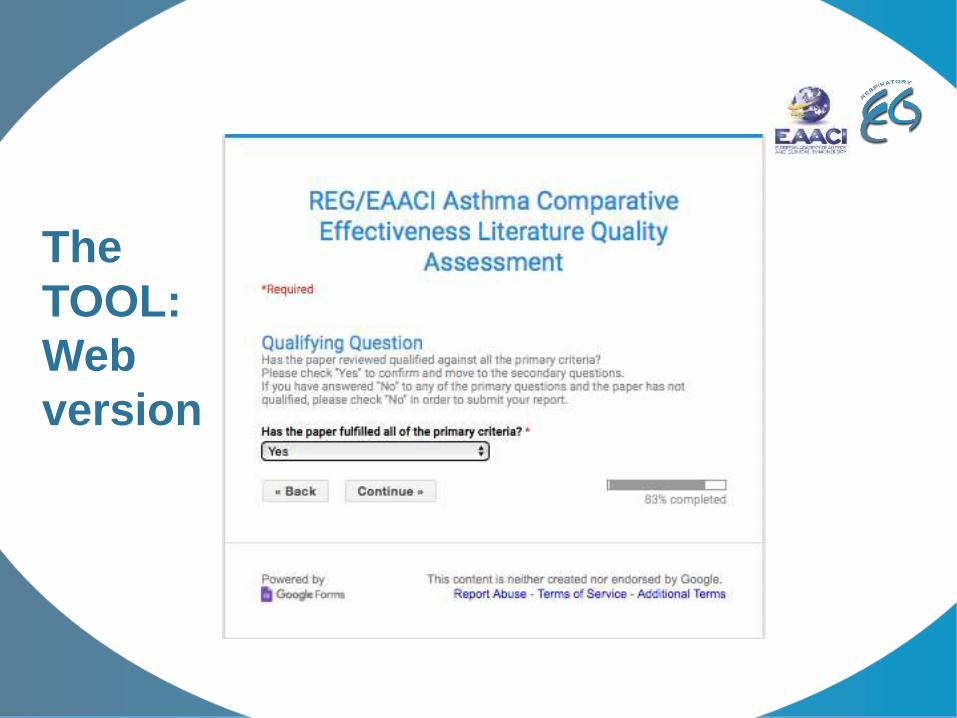
The
TOOL:
Web
version
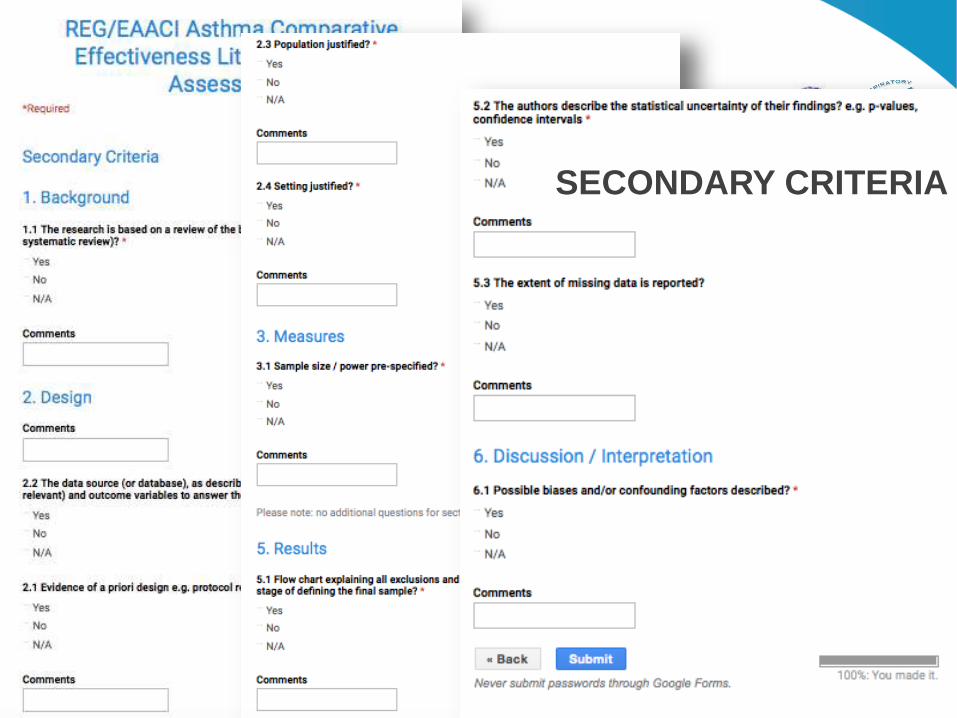
SECONDARY CRITERIA
Acknowledgements
• EAACI Task force members
• REG Staff
o Alison Chisholm
o Zoe Mitchell
• Sarah Acaster and Katy Gallop
• Robert Perry
LITERATURE REVIEW
NICOLAS ROCHE: Hopital de l’Hotel Dieu, Paris
—
PICOT questions
• TF members + informal literature search: n=21
• Preselection: n=9
o Education
o Adherence/persistence
o Smoking asthmatics
o Devices
o Molecules (ICS)
o Biotherapies (omalizumab)
o Formulations (Extra-fine)
o Strategies (ICS vs FDC…)
o Antibiotics for exacerbations (macrolides vs others)
o ACOS vs asthma vs COPD, ICS vs LABDs vs both
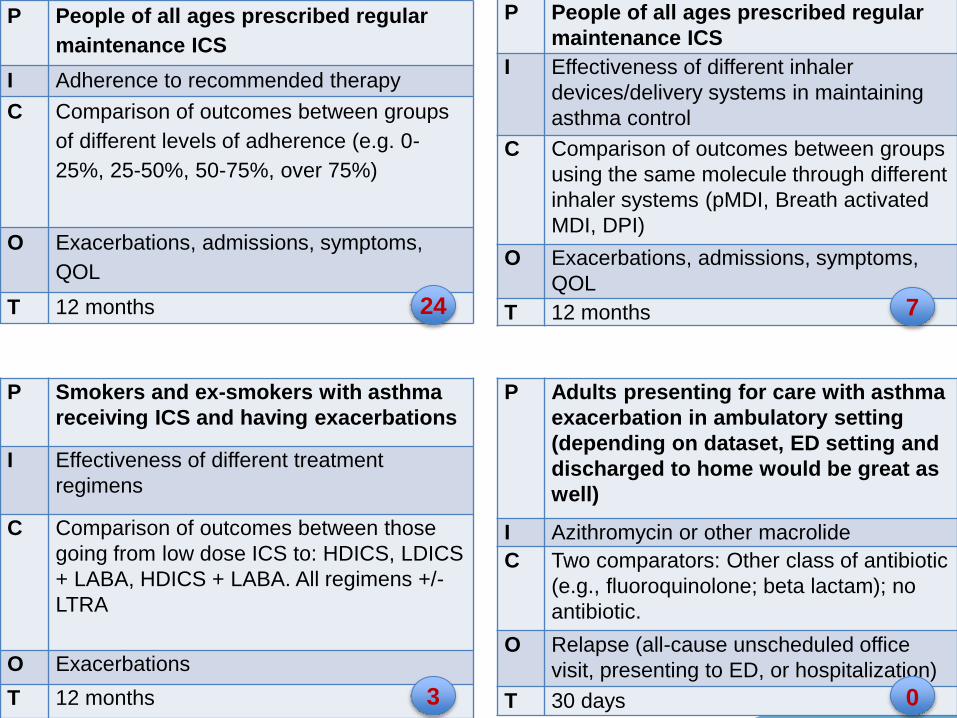
P People of all ages prescribed regular
maintenance ICS
I Adherence to recommended therapy
C Comparison of outcomes between groups
of different levels of adherence (e.g. 0-
25%, 25-50%, 50-75%, over 75%)
O Exacerbations, admissions, symptoms,
QOL
T 12 months
P People of all ages prescribed regular
maintenance ICS
I Effectiveness of different inhaler
devices/delivery systems in maintaining
asthma control
C Comparison of outcomes between groups
using the same molecule through different
inhaler systems (pMDI, Breath activated
MDI, DPI)
O Exacerbations, admissions, symptoms,
QOL
T 12 months
P Smokers and ex-smokers with asthma
receiving ICS and having exacerbations
I Effectiveness of different treatment
regimens
C Comparison of outcomes between those
going from low dose ICS to: HDICS, LDICS
+ LABA, HDICS + LABA. All regimens +/-
LTRA
O Exacerbations
T 12 months
P Adults presenting for care with asthma
exacerbation in ambulatory setting
(depending on dataset, ED setting and
discharged to home would be great as
well)
I Azithromycin or other macrolide
C Two comparators: Other class of antibiotic
(e.g., fluoroquinolone; beta lactam); no
antibiotic.
O Relapse (all-cause unscheduled office
visit, presenting to ED, or hospitalization)
T 30 days
24
0
7
3
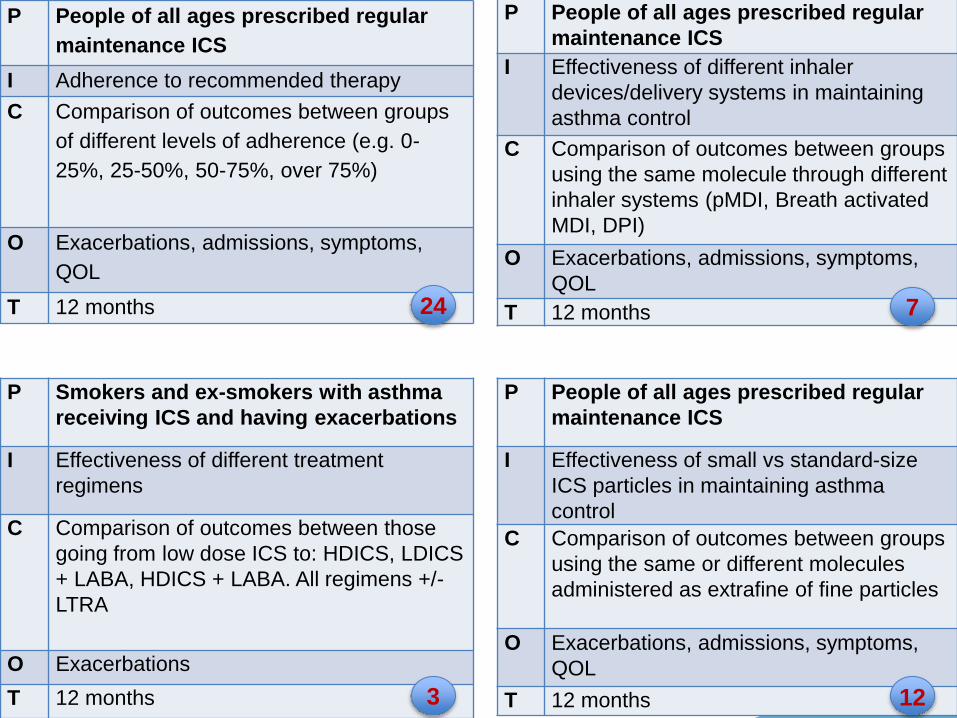
P People of all ages prescribed regular
maintenance ICS
I Adherence to recommended therapy
C Comparison of outcomes between groups
of different levels of adherence (e.g. 0-
25%, 25-50%, 50-75%, over 75%)
O Exacerbations, admissions, symptoms,
QOL
T 12 months
P People of all ages prescribed regular
maintenance ICS
I Effectiveness of different inhaler
devices/delivery systems in maintaining
asthma control
C Comparison of outcomes between groups
using the same molecule through different
inhaler systems (pMDI, Breath activated
MDI, DPI)
O Exacerbations, admissions, symptoms,
QOL
T 12 months
P Smokers and ex-smokers with asthma
receiving ICS and having exacerbations
I Effectiveness of different treatment
regimens
C Comparison of outcomes between those
going from low dose ICS to: HDICS, LDICS
+ LABA, HDICS + LABA. All regimens +/-
LTRA
O Exacerbations
T 12 months
P People of all ages prescribed regular
maintenance ICS
I Effectiveness of small vs standard-size
ICS particles in maintaining asthma
control
C Comparison of outcomes between groups
using the same or different molecules
administered as extrafine of fine particles
O Exacerbations, admissions, symptoms,
QOL
T 12 months
24
12
7
3
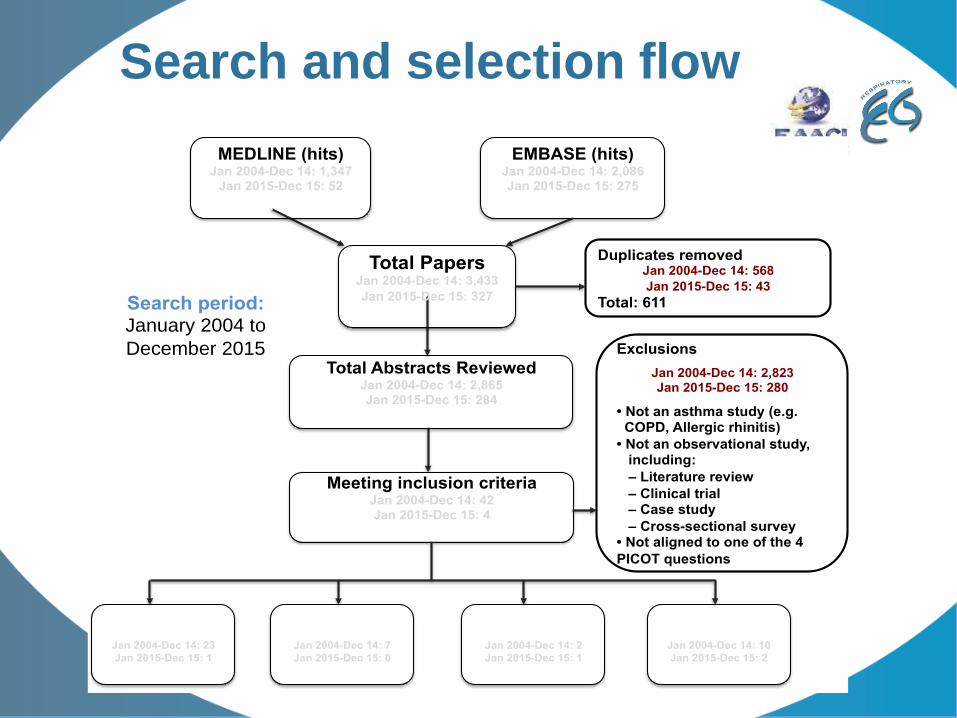
Search and selection flow
MEDLINE (hits) Jan 2004-Dec 14: 1,347
Jan 2015-Dec 15: 52
Total: 1,399
EMBASE (hits) Jan 2004-Dec 14: 2,086 Jan 2015-Dec 15: 275
Total: 2,361
Meeting inclusion criteria Jan 2004-Dec 14: 42 Jan 2015-Dec 15: 4
Total: 46
PICOT 1 ADHERENCE
Jan 2004-Dec 14: 23
Jan 2015-Dec 15: 1
24
Exclusions
Jan 2004-Dec 14: 2,823 Jan 2015-Dec 15: 280
• Not an asthma study (e.g. COPD, Allergic rhinitis)
• Not an observational study, including:
– Literature review
– Clinical trial – Case study
– Cross-sectional survey • Not aligned to one of the 4
PICOT questions
Search period: January 2004 to
December 2015
Total Papers Jan 2004-Dec 14: 3,433
Jan 2015-Dec 15: 327
Total: 3,760
Duplicates removed Jan 2004-Dec 14: 568
Jan 2015-Dec 15: 43
Total: 611
Total Abstracts Reviewed Jan 2004-Dec 14: 2,865 Jan 2015-Dec 15: 284
Total: 3,149
PICOT 2 DEVICE TYPE
Jan 2004-Dec 14: 7
Jan 2015-Dec 15: 0
7
PICOT 3 SMOKING ASTHMA
Jan 2004-Dec 14: 2
Jan 2015-Dec 15: 1
3
PICOT 4 PARTICLE SIZE
Jan 2004-Dec 14: 10
Jan 2015-Dec 15: 2
12
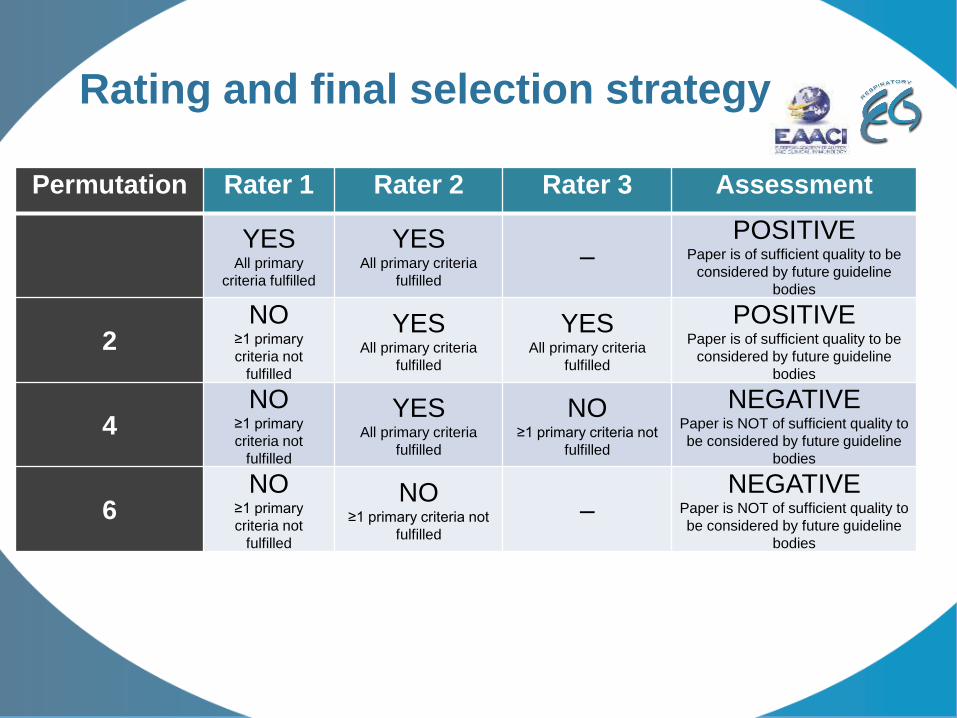
Rating and final selection strategy
Permutation Rater 1 Rater 2 Rater 3 Assessment
YESAll primary
criteria fulfilled
YESAll primary criteria
fulfilled
–POSITIVE
Paper is of sufficient quality to be
considered by future guideline
bodies
2NO
≥1 primary
criteria not
fulfilled
YESAll primary criteria
fulfilled
YESAll primary criteria
fulfilled
POSITIVEPaper is of sufficient quality to be
considered by future guideline
bodies
4NO
≥1 primary
criteria not
fulfilled
YESAll primary criteria
fulfilled
NO≥1 primary criteria not
fulfilled
NEGATIVEPaper is NOT of sufficient quality to
be considered by future guideline
bodies
6NO
≥1 primary
criteria not
fulfilled
NO≥1 primary criteria not
fulfilled
–NEGATIVE
Paper is NOT of sufficient quality to
be considered by future guideline
bodies
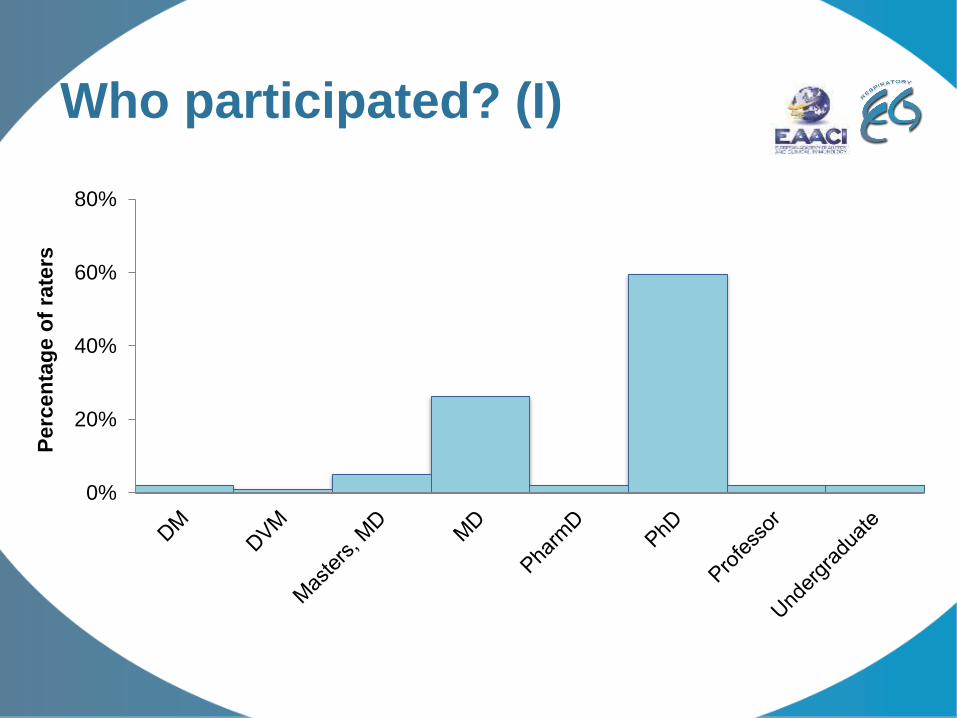
Who participated? (I)
0%
20%
40%
60%
80%
Perc
en
tag
e o
f ra
ters
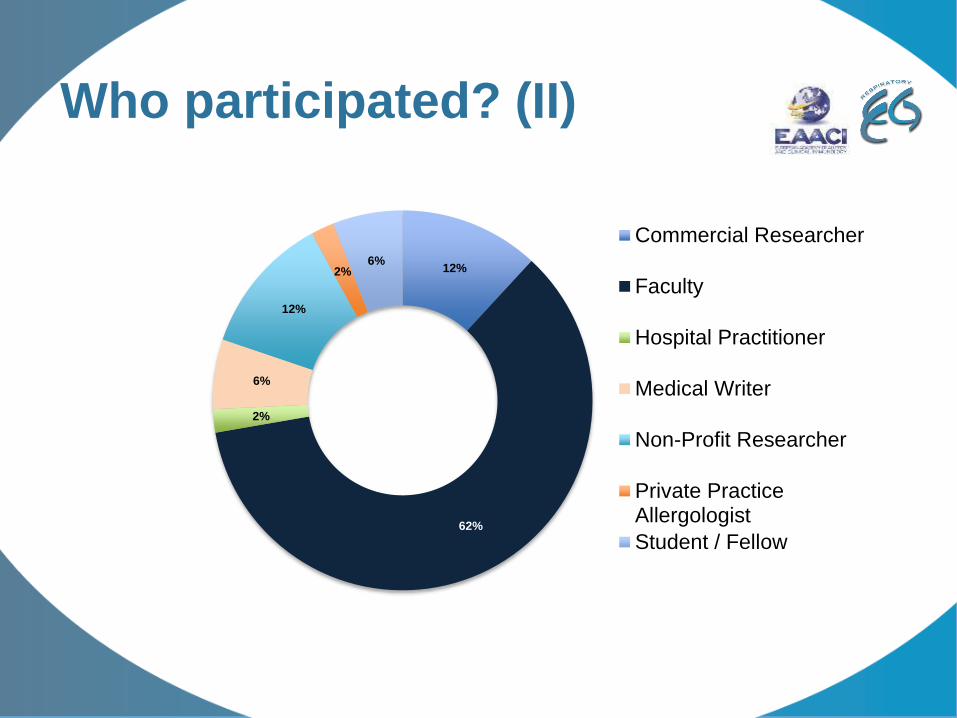
Who participated? (II)
12%
62%
2%
6%
12%
2%6%
Commercial Researcher
Faculty
Hospital Practitioner
Medical Writer
Non-Profit Researcher
Private PracticeAllergologist
Student / Fellow
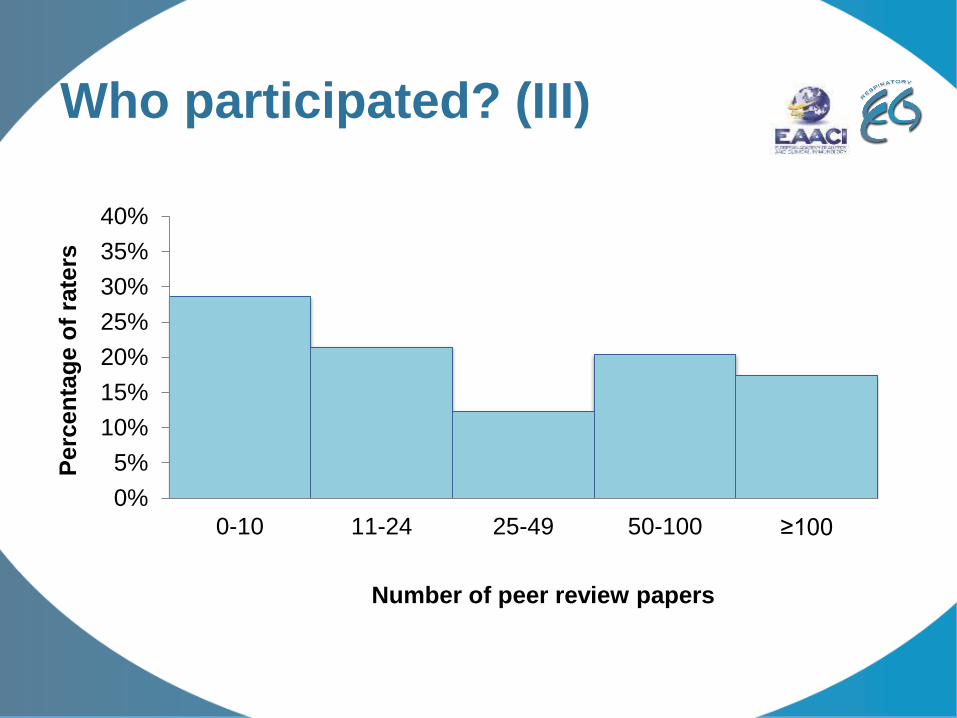
Who participated? (III)
0%
5%
10%
15%
20%
25%
30%
35%
40%
0-10 11-24 25-49 50-100 ≥100
Perc
en
tag
e o
f ra
ters
Number of peer review papers
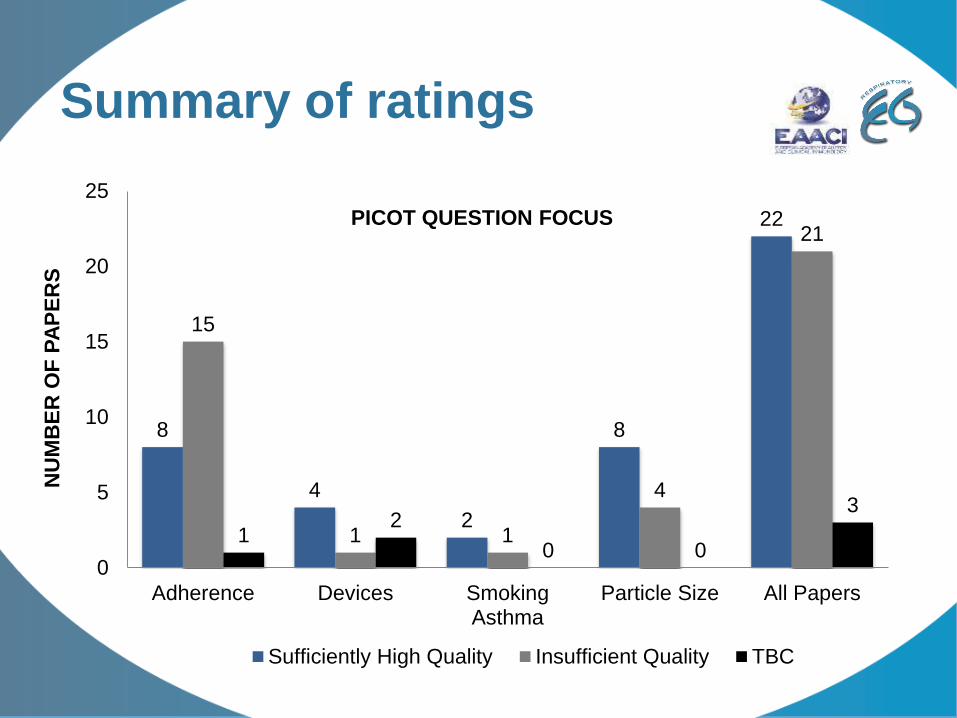
Summary of ratings
8
4
2
8
22
15
1 1
4
21
12
0 0
3
0
5
10
15
20
25
Adherence Devices SmokingAsthma
Particle Size All Papers
NU
MB
ER
OF
PA
PE
RS
PICOT QUESTION FOCUS
Sufficiently High Quality Insufficient Quality TBC
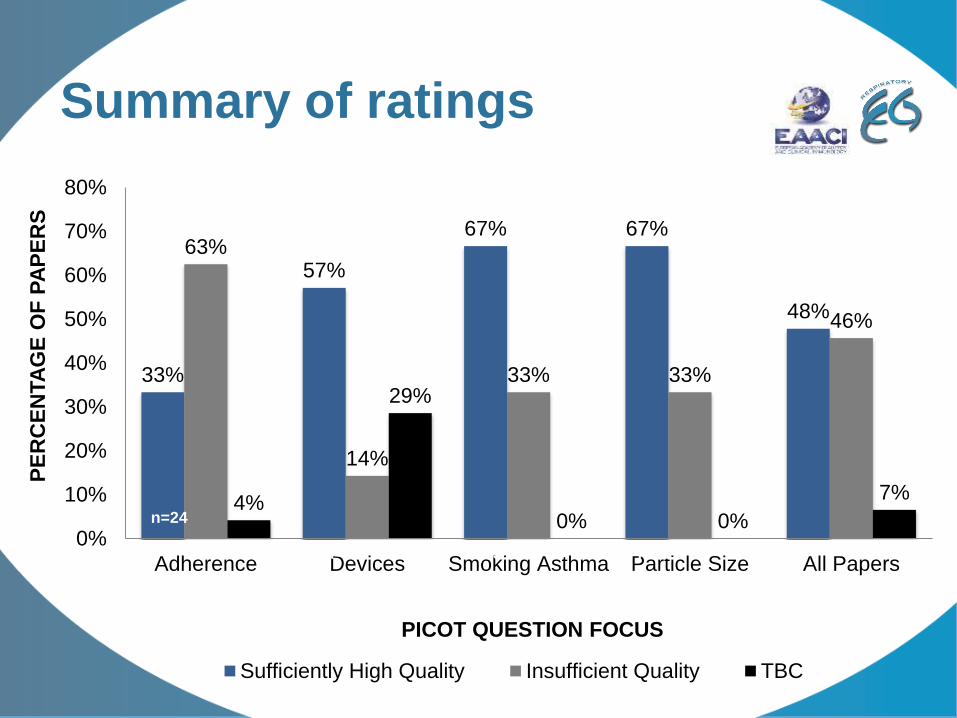
Summary of ratings
33%
57%
67% 67%
48%
63%
14%
33% 33%
46%
4%
29%
0% 0%
7%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Adherence Devices Smoking Asthma Particle Size All Papers
PE
RC
EN
TA
GE
OF
PA
PE
RS
PICOT QUESTION FOCUS
Sufficiently High Quality Insufficient Quality TBC
n=24
n=7 n=3 n=12
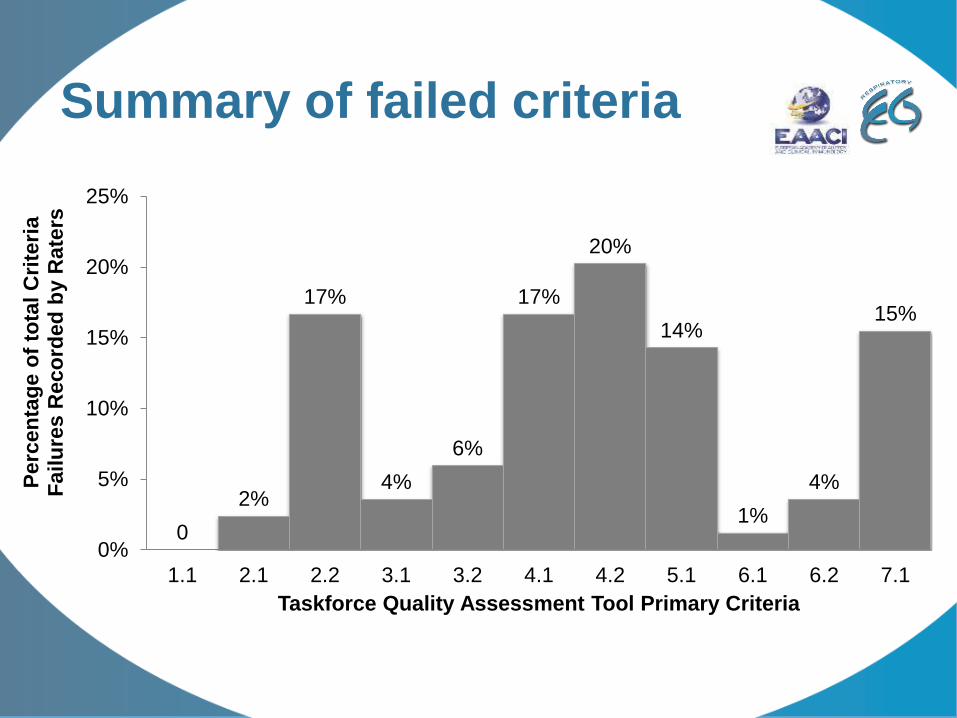
Summary of failed criteria
0
2%
17%
4%
6%
17%
20%
14%
1%
4%
15%
0%
5%
10%
15%
20%
25%
1.1 2.1 2.2 3.1 3.2 4.1 4.2 5.1 6.1 6.2 7.1
Perc
en
tag
e o
f to
tal
Cri
teri
a
Failu
res R
eco
rded
by R
ate
rs
Taskforce Quality Assessment Tool Primary Criteria
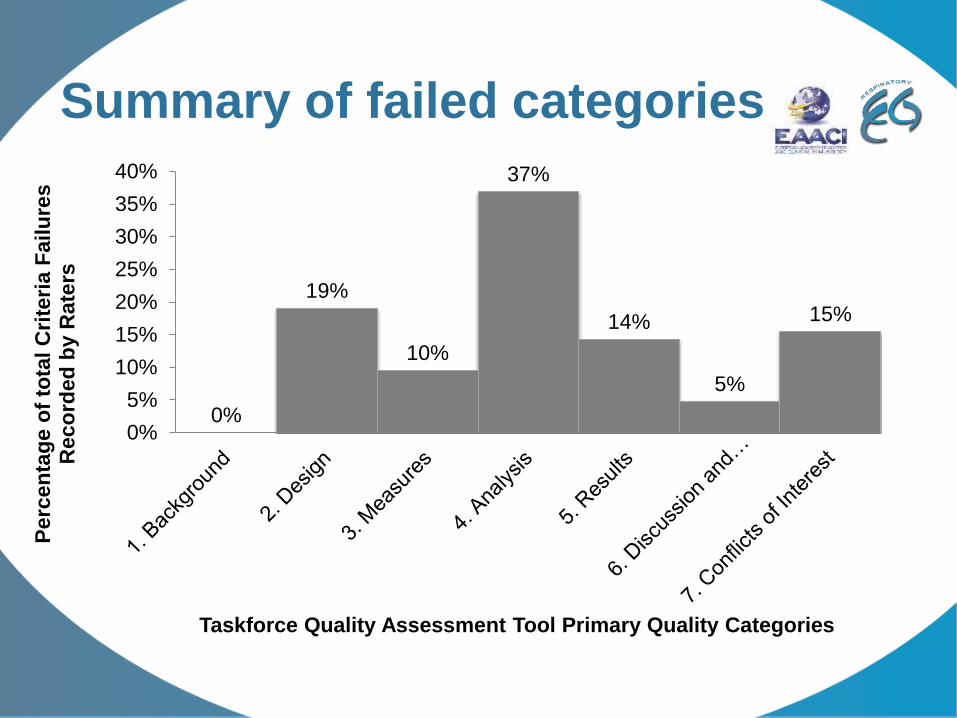
Summary of failed categories
0%
19%
10%
37%
14%
5%
15%
0%
5%
10%
15%
20%
25%
30%
35%
40%
Pe
rce
nta
ge
of
tota
l C
rite
ria
Fail
ure
s
Reco
rded
by R
ate
rs
Taskforce Quality Assessment Tool Primary Quality Categories
Reading grid
• Quality assessment
• Summary of methods
o Studied population, intervention, outcomes, setting
• Summary of results
o Magnitude of differences / robustness
• Possible remaining biases
• Final level of evidence (GRADE)
• Comparison with data from RCTs
o Explanations for differences
o Possible impact on guidelines
Key messages from papers of
sufficient quality: PICOT 1
PICOT 1: “ADHERENCE TO ICS THERAPY”
P People of all ages prescribed regular maintenance ICS
I Adherence to recommended therapy
CComparison of outcomes between groups of different levels of
adherence (e.g. 0-25%, 25-50%, 50-75%, over 75%)
O Exacerbations, admissions, symptoms, QOL
T 12 months

PICOT 1 / Adherence papers rated as being of sufficiently high quality to
inform future guideline development by Taskforce Quality Raters
1
Sadatsafavi M, Lynd LD, Marra CA, FitzGerald JM. Dispensation of long-acting β agonists with or
without inhaled corticosteroids, and risk of asthma-related hospitalisation: a population-based study.
Thorax. 2014;69(4):328-34
2
Friedman HS, Navaratnam P, McLaughlin J. Adherence and asthma control with mometasone furoate
versus fluticasone propionate in adolescents and young adults with mild asthma. J Asthma.
2010;47(9):994-1000.
3
Campbell JD, Allen-Ramey F, Sajjan SG, Maiese EM, Sullivan SD. Increasing pharmaceutical
copayments: impact on asthma medication utilization and outcomes. Am J Manag Care.
2011;17(10):703-10.
4
Tan H, Sarawate C, Singer J, Elward K, Cohen RI, Smart BA, Busk MF, Lustig J, O'Brien JD, Schatz M.
Impact of asthma controller medications on clinical, economic, and patient-reported outcomes. Mayo
Clin Proc. 2009;84(8):675-84
5
Williams LK, Pladevall M, Xi H, Peterson EL, Joseph C, Lafata JE, Ownby DR, Johnson CC.
Relationship between adherence to inhaled corticosteroids and poor outcomes among adults with
asthma. J Allergy Clin Immunol. 2004;114(6):1288-93
6
Taegtmeyer AB, Steurer-Stey C, Price DB, Wildhaber JH, Spertini F, Leuppi JD. Predictors of asthma
control in everyday clinical practice in Switzerland.
Curr Med Res Opin. 2009;25(10):2549-55
7
Laforest L, Licaj I, Devouassoux G, Chatté G, Belhassen M, Van Ganse E, Chamba G. Relative
exposure to controller therapy and asthma exacerbations: a validation study in community pharmacies.
Pharmacoepidemiol Drug Saf. 2014;23(9):958-64.
8Laforest L, Licaj I, Devouassoux G, Chatte G, Martin J, Van Ganse E. Asthma drug ratios and
exacerbations: claims data from universal health coverage systems. Eur Respir J. 2014;43(5):1378-86
9Björnsdóttir US, Sigurðardóttir ST, Jonsson JS, Jonsson M, Telg G, Thuresson M, Naya I, Gizurarson
S. Impact of changes to reimbursement of fixed combinations of inhaled corticosteroids and long-acting
β2-agonists in obstructive lung diseases: a population-based, observational study. Int J Clin Pract.
2014;68(7):812-9. Awaiting second review
Risk of asthma-related hospitalization
and maintenance treatment
• Regular treatment has to be ICS-based
o No risk difference between ICS-LABA and ICS alone
o Greater risk with LABA alone vs ICS-LABA & ICS alone
• Regular > irregular treatment or none
o Lower risk with regular treatment
o Except with LABA
• Database. Well matched
• GRADE: low → moderate
o No clinical data on severity
• Clinical impact: yes
• Similar evidence from RCTs: noSadatsafavi Thorax 2014
Adherence to ICS
• Adherence MF-DPI>FP
• SABA use MF-DPI<FP
• No difference in other clinical outcomes
• Database. Well matched
• GRADE: low → moderate
o No clinical data on severity
• Clinical impact: limited/none
• Similar evidence from RCTs: no
Freidman Thorax 2014
Impact of shifting part of drug
costs to patients• Higher copayments
o Less adherence
o More adverse asthma outcomes (outpatient and ED
visits), higher costs
• Database
• GRADE: low → moderate
o No clinical data on severity
• Clinical impact: yes
• Similar evidence from RCTs: no
Campbell Am J Manag Care 2011
ICS vs LTRA by adherence
• Monotherapy
o Adherent patients: ICS>LTRA
o Non-adherent patients: ICS<LTRA
• Combination: Best = ICS-LABA
• Database + survey
• GRADE: low → moderate
o No clinical data on severity for the database part
o Responders’ bias for the survey
• Clinical impact: yes
• Similar evidence from RCTs: partly (pragmatic)
Tan Mayo Clin Proc 2009
Adherence and asthma
exacerbations
• Low adherence increases the risk of ED visits
and oral steroid treatment
• Database, well matched
• GRADE: low → moderate
o No clinical data on severity
• Clinical impact: yes
• Similar evidence from RCTs: no
Williams JACI 2004
Adherence and asthma
control
• Lower ACQ improvement associated with low adherence
o Other predictors: age, severity
• Prospective cohort study, multivariate analysis
• GRADE: low → moderate
o Selection bias?
• Clinical impact: yes
• Similar evidence from RCTs: no
Taegtmeyer Curr Med Res Opin 2009
Adherence and asthma
outcomes
• Low adherence associated with poorer control and more
hospital contacts and oral steroid courses
• Prospective study in pharmacies , multivariate analysis,
validation of MPR data
• GRADE: low → moderate
o Selection bias & single pharmacy for each patient
• Clinical impact: yes
• Similar evidence from RCTs: no
Laforest 2014
Pharmacoepidemiol Druf Saf
Adherence and asthma
exacerbations• Low MPR increases the risk of oral steroid treatment and
hospitalization
• Database, unmatched, multivariate adjustment
• GRADE: low → moderate
o No clinical data on severity
• Clinical impact: yes
• Similar evidence from RCTs: noLaforest ERJ 2014
PICOT 1: Conclusions
• Several concordant observational studies showing an
association between low adherence and poor asthma
outcomes
o Each individually provides a moderate level of evidence
o Globally high level (concordance)?
• Adherence is influenced by copayment level
o With an impact on outcomes
• Maintenance therapy with LABA alone is dangerous
Key messages from papers
of sufficient quality:
PICOT 2
PICOT 2: “DEVICE TYPE”
P People of all ages prescribed regular maintenance ICS
I Effectiveness of different inhaler devices/delivery systems in
maintaining asthma control
CComparison of outcomes between groups using the same molecule
through different inhaler systems (pMDI, Breath activated MDI, DPI)
O Exacerbations, admissions, symptoms, QOL
T 12 months
PICOT 2 / Devices papers rated as being of sufficiently high
quality to inform future guideline development by Taskforce
Quality Raters
1
Price D, Chrystyn H, Kaplan A, Haughney J, Román-Rodríguez M, Burden A,
Chisholm A, Hillyer EV, von Ziegenweidt J, Ali M, van der Molen T. Effectiveness
of same versus mixed asthma inhaler devices: a retrospective observational
study in primary care. Allergy Asthma Immunol Res. 2012;4(4):184-91
2
Price D, Roche N, Christian Virchow J, Burden A, Ali M, Chisholm A, Lee AJ,
Hillyer EV, von Ziegenweidt J. Device type and real-world effectiveness of
asthma combination therapy: an observational study. Respir Med.
2011;105(10):1457-66. doi: 10.1016/j.rmed.2011.04.010. Epub 2011 May 25.
3
Price D, Haughney J, Sims E, Ali M, von Ziegenweidt J, Hillyer EV, Lee AJ,
Chisholm A, Barnes N. Effectiveness of inhaler types for real-world asthma
management: retrospective observational study using the GPRD. J Asthma
Allergy. 2011;4:37-47.
4
Thomas M, Price D, Chrystyn H, Lloyd A, Williams AE, von Ziegenweidt J.
Inhaled corticosteroids for asthma: impact of practice level device switching on
asthma control. BMC Pulm Med. 2009;9:1. doi: 10.1186/1471-2466-9-1.
Mixed vs single device(s)• Single device = better control and less severe
exacerbations
• Database study, adjusted analyses
• GRADE: low → moderate
o No clinical data on severity and pts knowledge/skills
• Clinical impact: yes
• Similar evidence from RCTs: no
Price Allergy Asthma Immunol Res 2012
Impact of switching
• DPI to pMDI or BAI or other DPI
• BAI to pMDI or other BAI
• Poorer outcomes following the switch
• Database study, matched & adjusted analyses
• GRADE: low → moderateo No clinical data on severity and pts knowledge/skills
• Clinical impact: possible
• Similar evidence from RCTs: no
Thomas BMC Pulm Med 2009
DPI vs pMDI for SFC
• pMDI better for several asthma outcomes
• Database study, matched
• GRADE: low → moderate
o No clinical data on severity and pts
knowledge/skills/adherence
• Clinical impact: uncertain (reinforce adherence, account
for preferences?)
• Similar evidence from RCTs: no
DPI vs pMDI & BAI for ICS
administration
• BAI and DPI better than pMDI for several asthmaoutcomes
• Database study, unmatched, adjusted
• GRADE: low → moderate
o No clinical data on severity and pts knowledge/skills/adherence
• Clinical impact: uncertain (reinforce adherence, account for preferences? Contradictory data)
• Similar evidence from RCTs: no
Price J Asthma Allergy 2011
Summary
• Using a single device might be better
• Switching without a consultation is followed by
poorer outcomes
• pMDI better for FDC?
• While BAI and DPI better for ICS?
Key messages from papers
of sufficient quality:
PICOT 3PICOT 3: “SMOKING ASTHMATICS”
P Smokers and ex-smokers with asthma receiving ICS and having
exacerbations
I Effectiveness of different treatment regimens
C Comparison of outcomes between those going from low dose ICS to:
HDICS, LDICS + LABA, HDICS + LABA. All regimens +/- LTRA
O Exacerbations
T 12 months
Impact of smoking on control
• Lower control in smokers
• Same benefit for all (current, ex, never smokers)
• Prospective cohort study, unadjusted analyses
• GRADE: low → low
o High drop-out rate,
o No adjustment nor matching
o Few clinical data available besides control
• Clinical impact: no
• Similar evidence from RCTs: no
Brusselle Respir Med 2012
Impact of smoking on control
• Better outcomes with extrafine vs standard size particles, larger differences in current and ex smokers
• Database matched study, adjusted analyses
• GRADE: low → moderateo No clinical / spirometry data
• Clinical impact: uncertain (exploratory)
• Similar evidence from RCTs: no
Roche AJRCCM 2015
Key messages from papers
of sufficient quality:
PICOT 4PICOT 4: “SMALL AIRWAYS MANAGEMENT; ICS PARTICLE SIZE”
P People of all ages prescribed regular maintenance ICS
I Effectiveness of small vs standard-size ICS particles in maintaining
asthma control
C Comparison of outcomes between groups using the same or different
molecules administered as extrafine of fine particles
O Exacerbations, admissions, symptoms, QOL
T 12 months

PICOT 2 / Smoking Asthma papers rated as being of sufficiently high quality to
inform future guideline development by Taskforce Quality Raters
1
van Aalderen WM, Grigg J, Guilbert TW, Roche N, Israel E, Martin RJ, Colice G, Postma DS, Hillyer
EV, Burden A, Thomas V, von Ziegenweidt J, Price D. Small-particle Inhaled Corticosteroid as First-
line or Step-up Controller Therapy in Childhood Asthma. J Allergy Clin Immunol Pract.
2015;3(5):721-31
2
Martin RJ, Price D, Roche N, Israel E, van Aalderen WM, Grigg J, Postma DS, Guilbert TW, Hillyer
EV, Burden A, von Ziegenweidt J, Colice G. Cost-effectiveness of initiating extrafine- or standard
size-particle inhaled corticosteroid for asthma in two health-care systems: a retrospective matched
cohort study. NPJ Prim Care Respir Med. 2014;24:14081
3
Colice G, Martin RJ, Israel E, Roche N, Barnes N, Burden A, Polos P, Dorinsky P, Hillyer EV, Lee AJ,
Chisholm A, von Ziegenweidt J, Barion F, Price D. Asthma outcomes and costs of therapy with
extrafine beclomethasone and fluticasone. J Allergy Clin Immunol. 2013;132(1):45-54
4
Price D, Thomas M, Haughney J, Lewis RA, Burden A, von Ziegenweidt J, Chisholm A, Hillyer EV,
Corrigan CJ. Real-life comparison of beclometasone dipropionate as an extrafine- or larger-particle
formulation for asthma. Respir Med. 2013;107(7):987-1000
5
Price D, Martin RJ, Barnes N, Dorinsky P, Israel E, Roche N, Chisholm A, Hillyer EV, Kemp L, Lee
AJ, von Ziegenweidt J, Colice G. Prescribing practices and asthma control with hydrofluoroalkane-
beclomethasone and fluticasone: a real-world observational study. J Allergy Clin Immunol.
2010;126(3):511-8.e1-10
6
Allegra L, Cremonesi G, Girbino G, Ingrassia E, Marsico S, Nicolini G, Terzano C; PRISMA
(PRospectIve Study on asthMA control) Study Group. Real-life prospective study on asthma control
in Italy: cross-sectional phase results. Respir Med. 2012;106(2):205-14
7
Barnes N, Price D, Colice G, Chisholm A, Dorinsky P, Hillyer EV, Burden A, Lee AJ, Martin RJ,
Roche N, von Ziegenweidt J, Israel E. Asthma control with extrafine-particle hydrofluoroalkane-
beclometasone vs. large-particle chlorofluorocarbon-beclometasone: a real-world observational
study. Clin Exp Allergy. 2011;41(11):1521-32
8
Price D, Small I, Haughney J, Ryan D, Gruffydd-Jones K, Lavorini F, Harris T, Burden A, Brockman
J, King C, Papi A. Clinical and cost effectiveness of switching asthma patients from fluticasone-
salmeterol to extra-fine particle beclometasone-formoterol: a retrospective matched observational
study of real-world patients. Prim Care Respir J. 2013;22(4):439-48
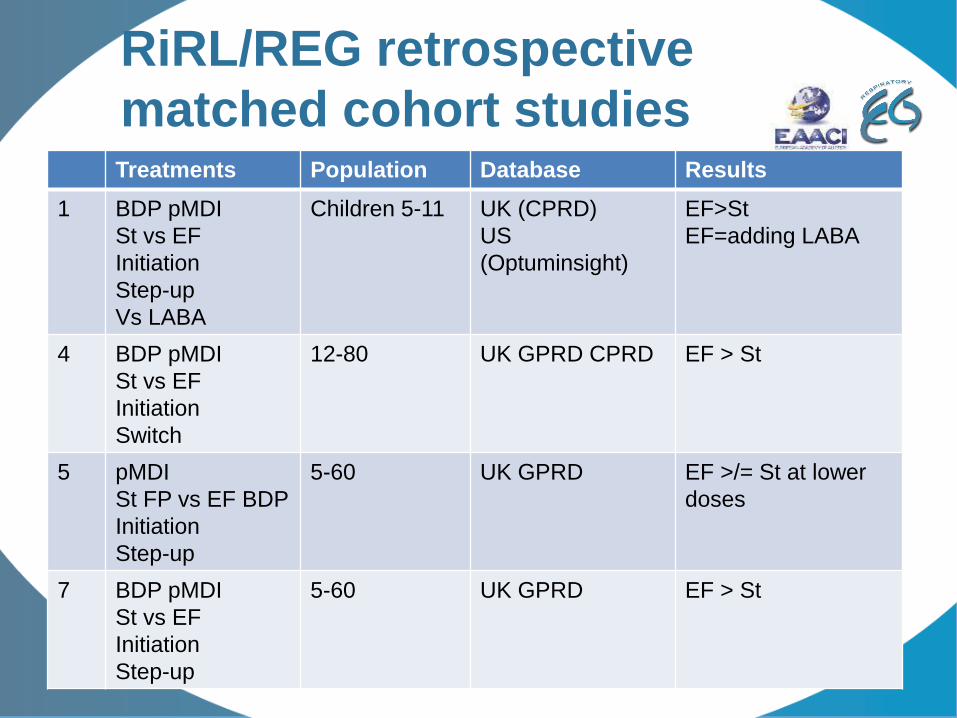
RiRL/REG retrospective
matched cohort studiesTreatments Population Database Results
1 BDP pMDI
St vs EF
Initiation
Step-up
Vs LABA
Children 5-11 UK (CPRD)
US
(Optuminsight)
EF>St
EF=adding LABA
4 BDP pMDI
St vs EF
Initiation
Switch
12-80 UK GPRD CPRD EF > St
5 pMDI
St FP vs EF BDP
Initiation
Step-up
5-60 UK GPRD EF >/= St at lower
doses
7 BDP pMDI
St vs EF
Initiation
Step-up
5-60 UK GPRD EF > St
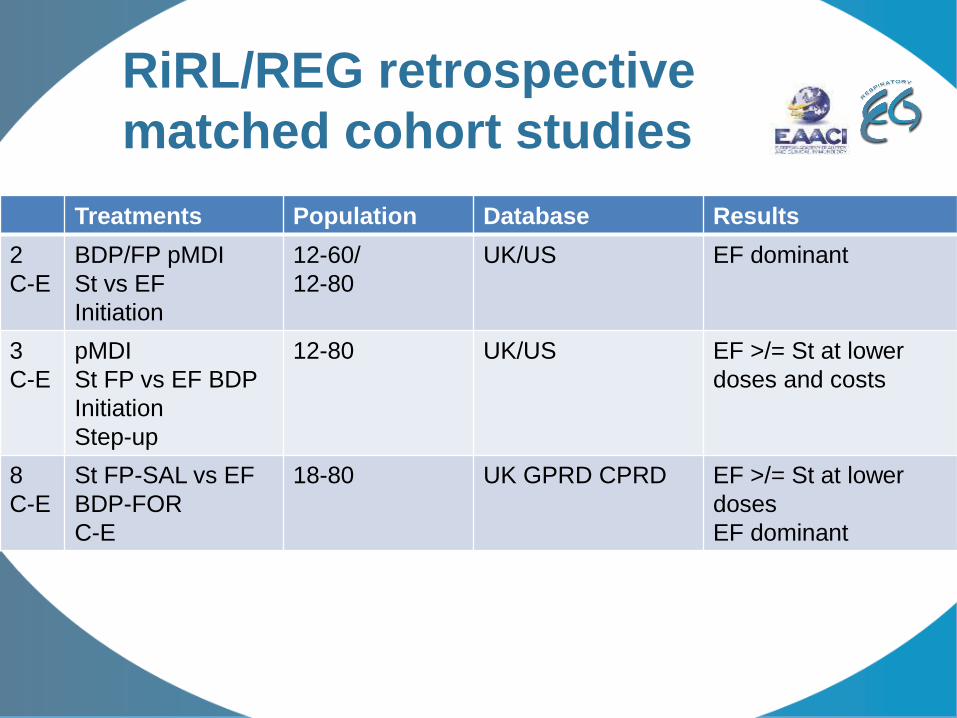
RiRL/REG retrospective
matched cohort studies
Treatments Population Database Results
2
C-E
BDP/FP pMDI
St vs EF
Initiation
12-60/
12-80
UK/US EF dominant
3
C-E
pMDI
St FP vs EF BDP
Initiation
Step-up
12-80 UK/US EF >/= St at lower
doses and costs
8
C-E
St FP-SAL vs EF
BDP-FOR
C-E
18-80 UK GPRD CPRD EF >/= St at lower
doses
EF dominant
RiRL/REG retrospective
matched cohort studies
• GRADE: low → moderate
o No clinical data on severity and pts
knowledge/skills/adherence
o Considering all studies together: high?
• Clinical impact: yes
• Similar evidence from RCTs: no
Prospective cohort study
• Unmatched, adjusted
• Comparison between treatments = secondary /
exploratory objective
• GRADE: low → low
o Selection bias
o Secondary objective
• Clinical impact: no
• Similar evidence from RCTs: no
Allegra Respir Med 2012
REG-EAACI TASKFORCE REPORT
PANEL DISCUSSION
REG SUMMIT 2016, LYON, FRANCE, 16 APRIL
SESSION: ‘INFLUENCING’ Guideline Development: the REG/EAACI Taskforce Reports
TIME: 12.45-13.45pm
Chair / Moderator: Nikos Papadopoulos
Centre for Paediatrics and Child Health, Institute of Human Development, University of Manchester,
Manchester, UK; Department of Allergy, 2nd Pediatric Clinic, University of Athens, Athens, Greece
—
• Novelty: never been done before
• Expert taskforce
• Wide range of participants:
o Countries, Societies, Guideline groups
• Focussed work
o Important evidence gaps
• Current literature
• High-threshold set for quality
• Bespoke tool
o Developed for specific purpose it was used for
o Tested for inter-rate agreement
STRENGTHS
• Narrow literature focus
• Small number of papers for some PICOT questions
• Expertise of reviewers
• Best-of-3 assessment approach?
• Assessment of reporting rather than study quality
(same thing from a guidelines’ perspective)?
WEAKNESSES
Discussion
• Considering
o the discussions around the QA tool
o the frequent difficulty in finding required information in
reviewed papers
• Integration of comparative effectiveness
research in asthma guidelines
o is at risk of remaining a subject of reluctance from
guidelines and policy makers
o until reporting markedly improves
PRACTICAL APPLICATIONS
• How the literature findings and literature quality
assessment tool can best be used in the future, e.g.:
o By guideline groups:
– To revise guidelines
– To appraise evidence
o Journal editors/reviewers:
– To assess the quality of submission
o Education:
– To train / guide new researchers
o Advocacy
– To highlight limitations in the evidence and clear areas for
improvement in the reporting of, if not the design of
observational studies in the future
Importance of the results
• The tool
• The literature appraisal
Importance by target
Target Importance
Researchers
Editorial boards
Reviewers
Guideline developers, policymakers
Others
Importance by topic
Topic Importance
PICOT 1: adherence
LABA alone dangerous
LTRA better
MF-DPI>FP
Hight copayment dangerous
PICOT 2: device
Single
Switch
pMDI vs BAI vs DPI
Importance by topic
Topic Importance
PICOT 3: smoking
Lower control in smokers
More treatment effect with EF in
smokers
PICOT 4: extrafine particles
EF>/=St
More cost-effective
POTENTIAL TO EXTEND THE WORK
• Disease areas
• Study design (pragmatic trials)
• Wider collaborations – REG/EAACI ±:
o ATS
o ± ERS
o ± others