region 6 protocol update 2014 pharmacology presence regional ems
TRANSCRIPT

Region 6 Protocol Update2014 PharmacologyPresence Regional EMS

Intranasal Drug Delivery – Clinical Implications for Pre-hospital care

Educational Web site:www.intranasal.net

Topics Why use intranasal medications? Intranasal drug delivery: General
concepts Intranasal drugs indications with clinical
cases and personal insights:• Pain Control• Opiate overdose
Drug doses Resources

Why is nasal drug delivery important in prehospital care?
Efficacy, speed and ease of delivery No delivery delays (no IV) Can deliver to anyone with an exposed nose Rapid onset of action
As effective and fast as IV drugs in most situations
Safety No needle stick risk Lower risk of respiratory depression (compared to
IV)
Easier to proceed with additional care Start IV in children or agitated adult Calm the agitated patient

Understanding IN delivery: General principles
First pass metabolism
Nose brain pathway
Bioavailability / Drug absorption
Safety vs IV drugs
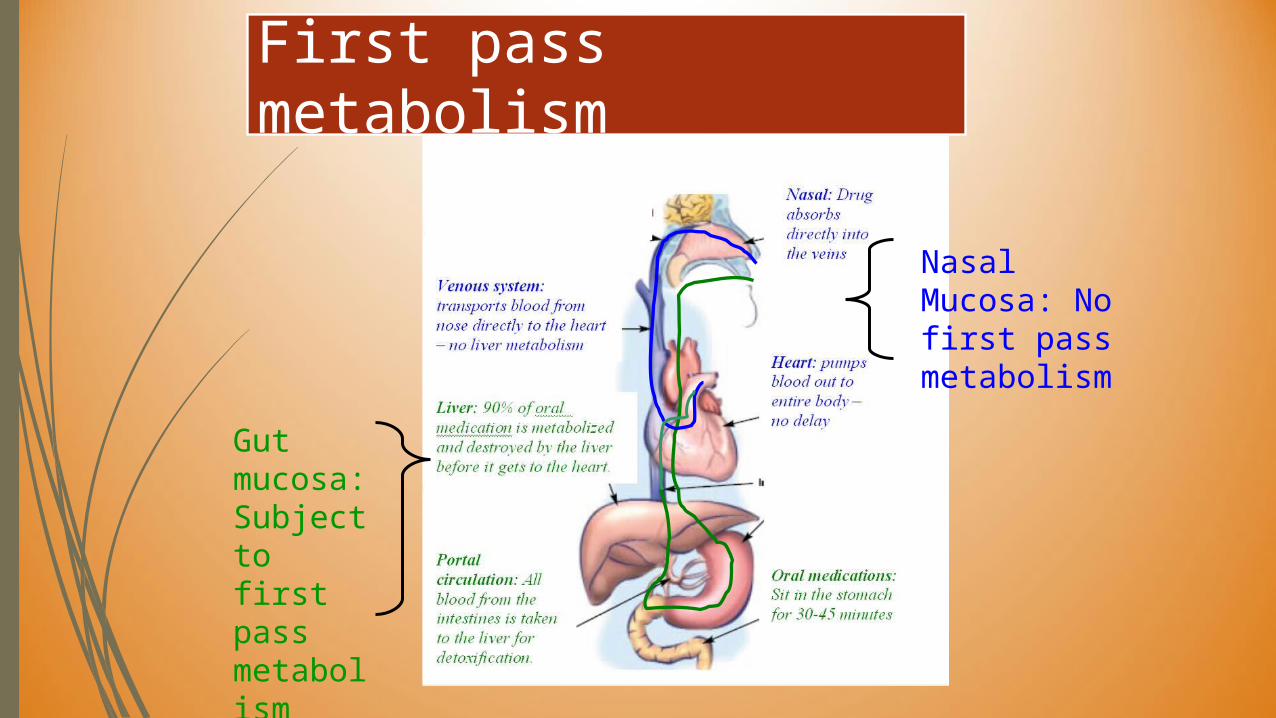
First pass metabolism
Nasal Mucosa: No first pass metabolism
Gut mucosa: Subject to first pass metabolism

Nose brain pathway
The olfactory mucosa (smelling area in nose) is in direct contact with the brain and CSF.
Medications absorbed across the olfactory mucosa directly enter the CSF.
Offers a rapid, direct route for drug delivery to the brain (skipping the blood brain barrier).
Olfactory mucosa, nerve
BrainCSF
Highly vascular nasal mucosa

Bioavailability/ Drug absorption
How much of the administered medication actually ends up in the blood stream.Examples:
IV medications are 100% bioavailable. Most oral medications are about 5%-10%
bioavailable due to destruction in the gut and liver.
Nasal medications vary depending on molecule, pH, etc
Fentanyl 80+% Naloxone 90+%

Optimizing Bioavailability of IN drugs
Minimize volume - Maximize concentration 0.2 to 0.3 ml per nostril ideal, 1 ml is maximum Most potent (highly concentrated) drug should be used
Maximize total absorptive mucosal surface area Use BOTH nostrils (doubles your absorptive surface area)
Use a delivery system that maximizes mucosal coverage and minimizes run-off.
Atomized particles across broad surface area
Beware of abnormal nasal mucosal characteristics
Mucous, blood and vasoconstrictors may reduce absorption
Suction nose or consider alternate delivery route if present
Critical Concept

Dropper vs AtomizerAbsorption
Drops = runs down to pharynx and swallowed
Atomizer = sticks to broad mucosal surface and absorbs
Usability / acceptance Drops = Minutes to give,
cooperative patient, head position required
Atomizer = seconds to deliver, better accepted

Region 6 Protocols
Intranasal medications must be administered through an atomizer

IN Administration1. Aspirate the proper volume of
medication required. Remember – use a filtered needle for aspirating from an ampule.
2. Remove the needle from the syringe and attach the MAD Nasal™ Device to the syringe.
3. Using your free hand to hold the crown of the head stable, place the tip of the atomizer snugly against the nostril aiming slightly up and outward toward the top of the ear.
4. Briskly compress the syringe plunger to deliver approximately half of the medication into the nostril.
5. Move the device over to the opposite nostril and administer the remaining medication.

What IN medications can we use in prehospital care?

Region 6 Protocol – IN MedicationsScenario Drug and Dose Protocols
Pain Control:Adult and Pediatrics
Fentanyl: 1 mcg/kg1 ml per nostrilMax dose 50 mcg;May repeat x 1 after 5 minutes at 0.5 mcg/kg
Adult and Pediatrics:• Amputation• Burns• Painful Swollen and Deformed Extremity
Opiate Overdose: Adult and Pediatrics
Naloxone: 1 mg/ml per nostril (1 ml per nostril maximum; 2 mg total dose)May repeat every 2-3 minutes to a maximum dose of 4 mg
Adult and Pediatrics:•Altered LOC•Poisoning / Overdose

Intranasal Medication Cases
Pain Control

Case: Pediatric Hand burn
A 5 year old burned her hand on the stove Clinical Needs: Pain control, Transport for wound
care Treatment: 2.0 mcg/kg of intranasal fentanyl (40
mcg – 0.8 ml of generic “IV” fentanyl) Within 3-5 minutes her pain is improved She is transported to a nearby medical facility 15 minutes later the patient easily tolerates cleansing of
the burn and dressing application.
Over a decade of prehospital and ER literature exists for burn, orthopedic trauma and visceral pain in both adults and children showing the following: Faster drug delivery (no IV start needed) so faster onset
Equivalent to IV morphine
Superior to IM morphine
Care givers are more likely to treat pediatric severe pain
Highly satisfied patients and providers
Safe
Pain control – Literature support

The Doubters: Surely IN drugs can’t be as good as an injection for pain control!
ACTUALLY – They are equivalent or better (in these settings)
Borland 2007 – IN fentanyl onset of action and quality of pain control was identical to IV morphine in patients with broken legs and arms
Borland 2008, Holdgate 2010, Crellin 2010 - time to delivery of IN opiates was half that of IV and more patients get treated
Kendal 2001 – IN opiate superior to IM opiate for pain control
Conclusions
IN opiates are just as good as IV
IN opiates are delivered in half the waiting time as IV
IN opiate are preferred by patients, providers and parents over injections
Nasal
Intravenous

Intranasal Medication Cases
Opiate Overdose

Case: Heroin Overdose
The ambulance responds to an unconscious, barely breathing patient with obvious intravenous drug needle marks on both arms – consistent with heroin overdose
After an IV is established, naloxone (Narcan) is administered and the patient is successfully resuscitated.
Unfortunately, the medic suffers a contaminated needle stick while establishing the IV.
The patient admits to being infected with both HIV and hepatitis C. He remains alert for 2 hours with no further therapy in the ED (i.e.- no need for an IV) and is discharged.

Case: Heroin Overdose
The medic now needs treatment - HIV prophylaxis
The next few months will be difficult for him: Side effects that accompany HIV medications
Personal life is in turmoil due to issues of safe sex with his spouse
Mental anguish of waiting to see if he develops HIV or hepatitis C.
He wonders why his system is not using MAD nasal to deliver naloxone on all these patients.

Opiate overdose – Literature support
Intranasal naloxone literature
Barton 02, 05; Kelly 05; Robertson 09; Kerr 09; Merlin 2010;
Doe Simkins 09; Walley 12:
IN naloxone is at least 80-90% effective at reversing opiate overdose
When compared directly it is equivalent in time of onset and in efficacy to IV or IM therapy.
IN naloxone results in less agitation upon arousal
IN naloxone is lay person approved in many places. It is safe, has saved many lives and reduces medical resource consumption

IN naloxone for opiate overdoseWhy not? Is there a downside?
High risk population for HIV, HCV, HBV Difficult IV to establish due to scarring of veins Elimination of needle eliminates needle stick risk They awaken more gently than with IV naloxone New epidemiology shows prescription drugs
(methadone, etc) are causing many deaths that naloxone at home could reverse.
Simple enough that lay public can administer and not even call ambulance

Intranasal Medications Summary
Another tool for drug delivery to supplement standard IV, IM, PO–very useful when appropriate
Supported by extensive literature Inexpensive Speeds up care in many situations Safe
Intramuscular Injections
Preferred sites: Deltoid Thigh Hip
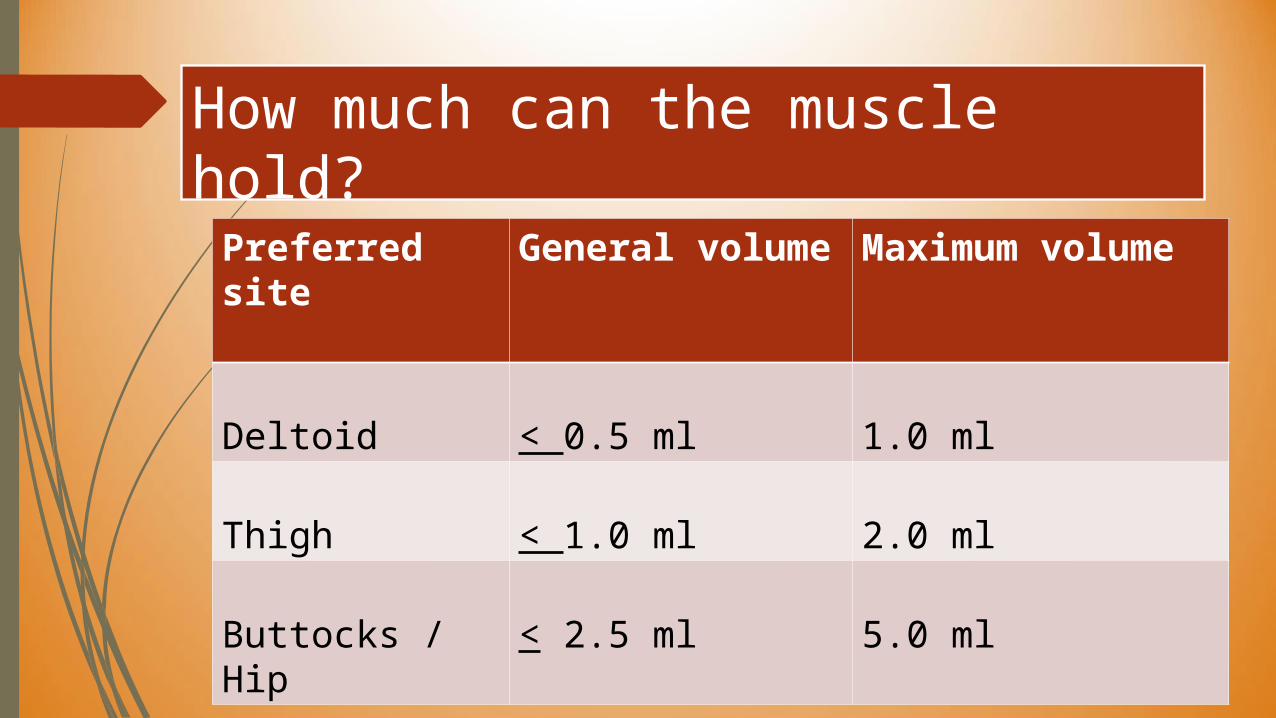
How much can the muscle hold?
Preferred site
General volume
Maximum volume
Deltoid < 0.5 ml 1.0 ml
Thigh < 1.0 ml 2.0 ml
Buttocks / Hip < 2.5 ml 5.0 ml
Amiodarone
Ventricular Ectopy Tachyarrhythmia – Stable
No longer need to mix with D5W
Dose: 150 mg IVP; may repeat q 5 – 10 minutes; maximum dose 450 mg