rehabilitation nursing role within interdisciplinary ... · rehabilitation nursing role within...
TRANSCRIPT

Rehabilitation nursing role withininterdisciplinary teamwork: the
perspectives from nurses,patients, therapists
and doctors
Jenny Liu

Introduction: • Patients requiring rehabilitation often have multiple or
complex physical, emotional and psychosocial problems. None of the professional disciplines within the healthcare team have expertise in all of these areas. While numerous works have been completed regarding the rehabilitation nursing role within the international context, there was insufficient literature discussing the rehabilitation nursing role within interdisciplinary teamwork (IDT) and the nurses’ interaction with other team members, especially from other disciplines’ and patients’ perspectives.

Research Objectives:• 1) To explore and determine the perceptions of the
rehabilitation nursing role at an inpatient rehabilitation service from the patients’, nurses’, therapists’ and doctors’ perspectives.
• 2) To identify areas of potential overlap between rehabilitation nurses and other team members within the inpatient rehabilitation service.
• 3) To identify opportunities for potential development of the rehabilitation nursing role within interdisciplinary teamwork at an inpatient rehabilitation service.

Research Design: • General Inductive Methodology of qualitative
research, which derived from grounded theory, was utilised in this study.
• Semi-structured interviews were conducted with 15 participants, which included five nurses, five patients, three therapists and two doctors.
• The general inductive analysis approach was used to analyse the data.
Method• The Study setting: inpatient rehabilitation service-Rehab
Plus, Auckland, New Zealand• Research design: • Methodology: General Inductive Methodology of
qualitative research• Semi-structured interview• Sampling, Study Population and Sample size:• Purposeful sampling, recruitment, There were five nurses,
three allied health staff, five patients and two doctors from Rehab Plus were selected and interviewed.
• a flowchart summarising the process of conducting the qualitative study.


Findings:
• Seven themes were identified and developed from the study findings: 1) the rehabilitation nursing role; 2) attitude; 3) environment; 4) communication; 5) interdisciplinary teamwork; 6) patient’s goals and patient-centred care7) service efficiency.

Seven themes identified from the current research
Rehabilitation Nursing Role
Section 5.2
Rehabilitation Nursing
AttitudeSection 5.3
EnvironmentSection 5.4
CommunicationSection 5.5
Interdisciplinary TeamworkSection 5.6
Patient goals and Patient-centred Care
Section 5.7
Service EfficiencySection 5.8

Research Findings• The research defined the rehabilitation nursing role
from the aspects of medical nursing, rehabilitation nursing and nurses within the team.
• With the rehabilitation teamwork model, the team members from different disciplines allowed and accepted the role blurring and role overlap during interdisciplinary teamwork.

Demographic characteristics of rehabilitation nurses
Nurse 1 Nurse 2 Nurse 3 Nurse 4 Nurse 5
Gender Male Female Female Female Female
Age group 30-39 60+ 40-49 50-59 40-49
Ethnicity NZ Maori NZ European Other
European
Malaysian NZ European
Country trained New Zealand New Zealand United Kingdom England New Zealand
Qualifications RN EN RN RN RN
Post Graduate (PG)
study
PG
Certificate in
Education
PG diploma in
rehab (Otago)
PG Certificate in
rehab (Otago)
Clinical
study days and case
study
One PG rehab
paper
Years of qualification
14 19 29 30 20
Years of rehab
experience 12 19 9 10 12
Level on PDRPRN 3 EN 4 RN 4 RN 4 RN 4

Demographic characteristics of patientsPatient 1 Patient 2 Patient 3 Patient 4 Patient 5
Gender Female Male Male Female Female
Age group 50-59 60-65 60-65 50-59 40-49
Ethnicity NZ European Maori &
European
Samoan Other European NZ European
Diagnosis Pathological
Fracture Right
Femur; gamma
nail fixation;
Metastatic
breast Cancer
Ischemic
Stroke- R)
MCA
subcortical
Diabetic sepsis
R) foot
R) BKA
On
haemodialysis
Avascular
Necrosis of R)
hip;
R) THJR;
Rheumatoid
Arthritis (RA)
colitis; Peritonitis;
R) hemicolectomy;
Deconditioning
Refeeding
syndrome, from
TPN to NG feeding+
oral
Chronic wound
Colostomy bag
Main Reason
for rehab
Fracture Stroke Amputation R) THJR
RA
De-conditioning
LOS when
interviewed
3 weeks 6 weeks 4 weeks 6 weeks 3 weeks

Demographic characteristics of Allied Health staff
AH 1 AH 2 AH 3
Gender Female Female Female
Ago groups 30-39 20-29 20-29
Ethnicity Germany NZ European NZ European
Country trained Germany New Zealand New Zealand
Qualification
(Disciplines)
SLT PT OT
Post graduate
study
Masters degree N/A N/A
Years of qualification 7 6 5
Years of rehab
experience
3 3 < 1

Demographic characteristics of doctors
Doctor 1 Doctor 2
Gender Male Female
Age group 50-59 30-39
Ethnicity Arabic Asian
Country trained Egypt, UK, New Zealand New Zealand
Qualifications MB. BCh., MSc., FAFRM
(RACP)
MB. BCh
Position at Rehab + Consultant in Rehabilitation
medicine
Rehabilitation registrar
Years of qualification 35 6
Years of rehab experience 14 1

Themes, codes arising from analysis of interviews with participantsTHEMES CODES
Theme 1 the rehabilitation
nursing role
Traditional nursing, “basic nursing”, “pure nursing”, “nursing nursing”; Holistic nursing care
Rehab nursing
Working within the team
Theme 2 Attitude Positive attitude to patients’ care
Positive attitude to nursing role
Some challenge or negative attitude
Theme 3 Environment Environment geographically
Rehab milieu: the environment created and maintained by staff, warm safe, supportive environment
Theme 4 Communication Communication between team members, patients and family
The methods of communication
The work environment and facilitation of communication
Room for improvement
Theme 5 Interdisciplinary
teamwork
Patient’s holistic care needs an interdisciplinary team
How the IDT works
The interaction between team members
Theme 6 Patients’ Goals
and patient-
centred care
Goal setting: patient’s goals, patient’s wants
Patient-centred care: ICF model, holistic care
IDT work together towards patient’s goals
Theme 7 Service efficiency Excellent service and nursing care, good feedback

The rehabilitation nursing role - medical nursing
Medical
and
holistic nursing:
Nurses’
perspectives
Medical nursing: monitor medical conditions, meet patients’ medical needs;
observations, medications; nursing assessment, manage clinical issues, pick up
any medical issues and report to doctors. Manage IV trolley, emergency trolley
and medical related equipment and environment.
Physical care: hygiene, skin care, prevention of further breakdown, ensure nutrition intake,
toileting issues, bowel management, incontinent issues; pain management, wound
management, diabetes care, assist mobility
Emotional support: get family involved, support patient and family, refer to psychologist
and doctors for emotional support
Patients’ perspectives Physical care: Hygiene, showering, toileting, pain, medication, make bed, assist with
mobility, get out of bed, put in the bed, nutrition, wound care, skin care, dress
Emotional: nurse is the first person to ask, frontline, be there, listen to the patients,
empathise with patients, overall wellbeing, primacy of nurse-patient relationship
AH’s perspectives “Nursing” nursing: wound care, stump dressing, medication, pressure sores, skin care,
showers, toileting, nutrition.
Doctors perspectives Pure nursing: monitor and assess patient’s medical aspects and report to doctors and the
rest of team, meet patient morbidities and rehab needs, support and assist doctors job

the rehabilitation nursing - rehab nursingRehab
nursing
Nurses
perspectives
Functional rehab: from doing for patients to educating and supervising patients to do for themselves,
self medication, do as much as they can do
Rehabilitation specific nursing work: Find out patients’ goals and work towards their goals,
attending patients’ meetings, facilitate weekend leaves, safe discharges.
Empower and enable patients: motivate patients, empower and enable them to regain their
independence; Education, teaching and training patients and family, and giving back control of their
lives.
Patients’
perspectives
Work together with patients: following instruction from PT, OT, encouraging and prompting self-
care, support, positive reinforcement, infection control, create a warm and safe environment
Confused with rehab nursing role: serve the meals, cleaning messy tables, Some nursing roles could
be done by HCA, nurse aid, then nurses have more time for nursing care or patients care.
AHs’
perspectives
See self more in a training role, not just helping or doing for patients, they support the rehab process,
help and train patients to be independent, rehab shower, rehab breakfast. Education around smoking
cessation, sit down with patients, teach self medicating.
Doctors’
perspectives
Play important role in the rehab environment. Contribute to the whole rehab process, follow
instructions from PT/OT, walk patients, daily functional goals, educate patients and families, supervise
medication, mobility and transfers, smoking cessation, inflection control, sexuality

The rehabilitation nursing role - work within the IDTWork
within the
IDT
Nurses’
perspectives
Facilitator: get patients ready for therapies; work with or assist doctor’s job; follow
instructions from therapists
Senior nurse role: management level, bed management, manage referrals, new
admissions, training staff, health promotion, continue education with IDT, coordinating,
manage staff, manage clinical issues
Role blurring or role confusing
Patients’ perspec Nurses work with therapists; follow instruction from therapists
AHs’ perspectives Engage goal setting, nurse do all sorts of things, they train, teach patients to use
walking aids, education re prevention of strokes, smoking cessation, key working issues,
discharge planning
Engage teamwork: interdisciplinary working in the team, role blurring, do a little bit of
other disciplines’ jobs, to be OT/SLT/PT’s eyes after hours
Blurring of roles: Nursing staff undertake roles that are traditionally outside of the
scope of nursing, enhanced potential to evolve from IDT to transdisciplinary model
(especially regarding equipment use)
Doctors
perspectives
Working as a team: Key workers give nurses power to coordinate patients’ rehab
programmes, link between the core team and families, coordinate and meet patients’
needs, finalise the discharge report, outcome measures-FIM, form relationship support
patients and family, support other team members job

Theme 2: attitudeNurse’s perception: Positive attitude regarding nursing role
Positive attitude regarding patients’ care
Some challenges from negative or difficult patients
Patients’ attitude Rehab nurses are positive and interested in patients
Patients are proud of themselves making progress; they appreciate nursing
care and positive reinforcement received
Doctors perception Very friendly, rehab orientated nursing team
Nurses were too shy or at second position; need to be more visible; need to
be upfront and acknowledge the value of the contribution of nursing
Therapists’ perception Nurse’s caring nature with patients.
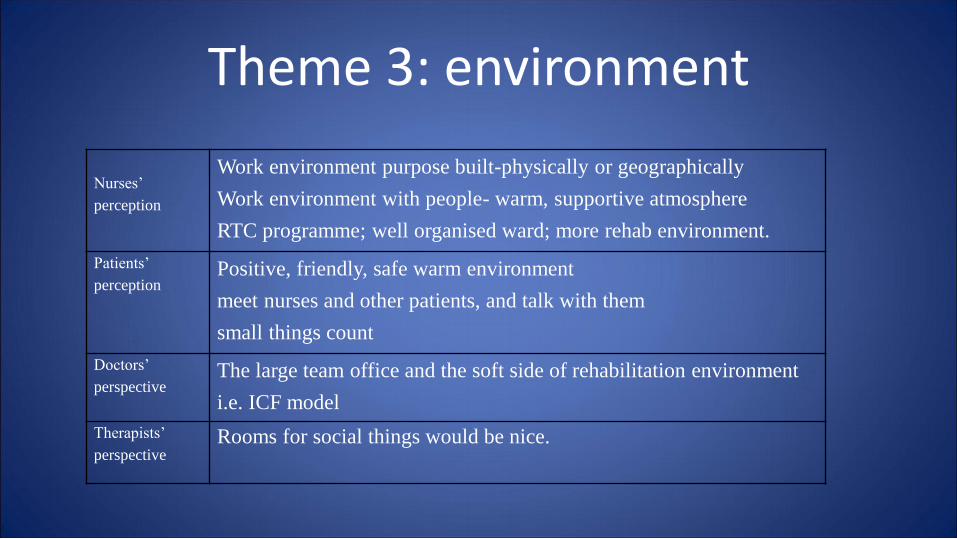
Theme 3: environment
Nurses’
perception
Work environment purpose built-physically or geographically
Work environment with people- warm, supportive atmosphere
RTC programme; well organised ward; more rehab environment.
Patients’
perceptionPositive, friendly, safe warm environment
meet nurses and other patients, and talk with them
small things count
Doctors’
perspectiveThe large team office and the soft side of rehabilitation environment
i.e. ICF model
Therapists’
perspectiveRooms for social things would be nice.

Theme 4: CommunicationNurses’
perception:
Open to each other; communicate with each other; be respectful and honest; communicate
with family; family involved meetings; family may assist patients once discharged home
With the big office open and all the therapists in the same office, enhance the
communication between team members.
Patients’
perception:
Nurses are the first people to ask about everything; communication within teams very good,
you don’t have to explain to nurses, they already know from handover or reading the notes;
Some communication gaps: staff name badges too small, need to introduce self more than
once; need to know patient’s specific rehab needs
AHs’
perspectiv
e
Nursing vs patient: nurses sit down with patients talking about medication; seeking help
from SLT with looking at medication.
between IDT; big office; ICF model; relationships between teams; joint sessions; quick
catch up on top of regular meetings/nurses’ input in patient meetings
Doctors’
perception
quite good; two way communication; direct and lateral communication between all core
team members every day; able to communicate if any problems; large team office; meet
frequently; working in close proximity facilitates process

Theme 5: interdisciplinary teamworkNurses’
perceptionPatients’ holistic care requires that the IDT works together; it works extremely well for
patients’ benefit
facilitate the goal-setting process
Staff feel supported from IDT and enjoy working together as a team towards patients’
goals.
Patients’ perception: Patients recognise most of core team members; they all do specific jobs; Nurses are the
first people to ask about everything.
Doctors’ perception: Big office and regular meetings facilitate good communication between team members,
respect. Nurses need to be more proactive and to be part of the IDT, play more prominent
and obvious role in a more assertive way
PT/nurse Interaction: PT recognise nurses’ rehab role; integrate rehab into daily life functions;
work together and share knowledge with nurses in certain areas
SLT’s role interaction with
nurse role:Cognition, memory, education, key working stuff, discharge planning. SLT workers
collaborate with nurses to solve problems, teach people communication strategies,
comfortable using the white board and are able to swallow safely. People are happy to
share their roles

Interdisciplinary teamwork (Cont…)
Nurse support SLT: Nurses are present 24hours , observe patients when they are fatigued, any problems
such as swallowing report to SLT; Nurses need ask SLT help for communication
impaired patients
SLT/ PT Seating, problems with eating and drinking.
OT /IDT: PTs, OTs,
SLTs,Nurses, Social
workers
OT/PT: working on general mobility and upper limb issues, patients’ independence
around home.
OT/SW: the level of home help; D/C planning of accommodation.
OT/SLT: cognitive therapy tasks, any cognitive issues or communication problems,
functional rehab.
OT/Nurses: working on facilitating patients’ independence of personal care. If there
were more joint AH/ nurse sessions then teamwork would be improved.

Interactions or role overlap within IDT membersDisciplines Interaction or role overlap
Nurses/doctors
(medical or rehab
related tasks)
Medical aspects of care, observation and monitoring patients’ condition and report to doctors;
follow doctors’ orders re medication or medical related tasks. pain, wound, bowels, continence
management, diabetes care, rehab related tasks
Nurses/ SLT
(working together
with patients with
communication,
swallowing,
cognition, memory
problems)
Work together with patient’s communication, swallowing, cognition, memory, key working tasks
and discharge planning.
Educate patients regarding fall risks, medication, smoking cessation etc. , enable them to
participate in rehab programme
Nurses are present 24hours; SLTs need nurses’ observation regarding patients’ problems such as
swallowing when they are fatigued. Nurses need help from SLTs for communication impaired
patients.
Nurses/OT
(working closely on
facilitating patients’
independence of
personal cares)
Rehab shower, rehab breakfast, toileting, and education about procedures. Joint sessions
introduced, so OTs/nurses work together rather than nurses just take directions from OT.
Nurses run their everyday tasks on a daily basis and make good observations and know patients
more. They are OTs’ eyes after hours and highlight patient’s needs to OTs.

Interactions or role overlap within IDT members (Cont…)Nurses/PT
(Working
together on
patient’s mobility,
equipment,
wound healing,
medication,
diabetes foot
cares etc.)
Mobility: patients’ transfers, stairs, manual handling skills.
Equipment i.e. Roho cushions, orthotics, splints, hoists
Medication, pain killers, BP medications
Wound healing, especially amputee stump wounds, pressure sores etc.
Diabetes patients, the sensations test and diabetes foot care etc.
As patients may be different between gym and day, nurses can feedback to PTs for any
issues after hours.
SLT/OT The function activities involve the level of communication, A lot of overlap between SLTs
and OTs with the cognitive therapy tasks, and to help patients return to their previous
function.
PT/OT OTs and PTs often work together because they both work on patients’ general mobility and
independence around the home. They also cross over regarding the upper limb tasks.
SLT/PT They work together regarding patients’ seating, patients’ eating and drinking stuff.

Theme 6: patients’ goals and patient-centred care
Nurses’
perspectives
The whole idea is based on the patients. The patients are the centre of the core team. The
ICF model facilitates patients’ individualised and holistic care.
goal setting is a major part, family is important with the patient rehab journey, especially
with weekend leave and safe discharge.
Goal setting: make sure it’s patient’s goals and wants, not health professionals’ goals and
wants. Core team helps patients to set up realistic goals and work towards them assisting
them to achieve their goals.
Patients’
perspectives
Individualised care, tailored for patients, negotiation and partnership with patients.
Patients have core team work for them, own nurse, PT/OT/SLT/social worker.
Start road to go home, gain knowledge about my medical problem, want to be
independent at home and come back to visit.
Doctors’ perspectives
Goal setting by patients and family directs their rehab programmes; IDT focus on rehab
intervention to help patients get their goals and achieve their goals. Utilising the ICF
model, with regular meetings, core team ensure patients’ holistic care met.
AHs’ perspectives We work together towards patients’ goals; looking at what patients want to achieve and
working towards that.

Theme 7: Service efficiencyNurses’ perspectives We provide good service and nursing care to patients; have good feedback from patients and family; we
provide a lot of support to patients. Nursing staff more stable than AH staff, nurses have a stronger voice
in the IDT. RTC improves things for nurses
Lots of pressure from management, and more complex patients, multi morbidity, unstable patients,
homeless patients, funding issues, uncertain future planning, cutting costs, stressful to staff, patients and
family.
We need to promote ourselves more to gain more recognition, better communication. Nurses need do
post graduate rehabilitation papers, do more modern research; we need education and ongoing education
with staff regarding the goal setting, the IDT, the ICF model, keyworking.
Doctors’ perspectives Regular communication between team members. the allied health team and nursing team very mobile
and rotating, on-going regular in-service, presentations, on-going teaching and education, orientation of
new staff, introduce rehabilitation framework within the ICF model, FIM training; efficacy working on
shortening LOS.
Therapists’
perspectives
We have quite a high level of cares. Lots of paper work has been put in place to continue to improve our
service
New nurses introduced to cover the ward, in order to release more nurses to attend inservice training.
More joint sessions between nurses and therapists, joint social activities.
Patient’s perspectives The overall cares to the patients is very good.
Someone trained to do meals, toileting, showering (i.e. HCA) need to be employed to free nurse’s time

Conclusion: • The present study identified a new
interdisciplinary teamwork model, where the nurses step in to work closely with patients and families and to be an integral conduit between the patient/family and other members of the IDT.

the interdisciplinary team model portrayed by literature
PATIENTand
FAMILY
Physiotherapist
Occupational Therapist
Dietician
Doctor
Psychologist
Pharmacist
Social Worker
Speech-language therapist
Nurse

Nurses step in to take more responsibilities within interdisciplinary teamwork
PATIENTand
FAMILY
Physiotherapist
Occupational Therapist
Dietician
Doctor
Psychologist
Pharmacist
Social Worker
Speech-language therapist
Nurse
Nurse

the new interdisciplinary teamwork model at Rehab Plus
PATIENTand
FAMILY
Physiotherapist
Occupational Therapist
Dietician
Doctor
Psychologist
Pharmacist
Social Worker
Speech-language therapist
Nurse

• At Rehab Plus, Nurses are more actively involved in patients’ rehabilitation processes and coordinated the patients’ care by connecting and coordinating the interdisciplinary team members’ work, as well as doing some other disciplines’ jobs to optimise patients’ care within existing service constraints.

Conclusion and implications
This research has explored the rehabilitation nursing role within interdisciplinary teamwork from nurses’, patients’, therapists’ and doctors’ perspectives in a specialist rehabilitation centre in Auckland.
Following analysis using the GIM process, seven main themes were identified from the data. The research findings explored the research questions by defining the rehabilitation nursing role from medical nursing, rehabilitation nursing and nurses within the team.
The results of the present study suggested that within the rehabilitation teamwork model,
the team members from different disciplines accepted and enjoyed the role blurring and
role overlap during the interdisciplinary teamwork.

ImplicationsRehabilitation nurses working within the interdisciplinary team allowed and accepted role
blurring and role overlap with other team members.
This research identified a new interdisciplinary teamwork model within the unit where the
nurses step in to work closely with patients and families, and be the eyes and hands of other
disciplines after hours.
The rehabilitation nurses are the essence and soul of the IDT. They are the communication centre
and the connection centre, They coordinate patients’ care by connecting and coordinating the IDT members’ jobs, as well as they cross the professional boundaries and do a little bit of other disciplines’ jobs to meet patients’ needs. They create and maintain a warm home like and rehabilitative environment for patients and team members..
With their 24 hour presence, nursing staff pick up any issues or any care gaps between other professionals and automatically fill the gap and fix the problems. they are the glue to hold the
team together and patch up if any gaps occur. They are the pivot of the IDT family.

Implications (Cont…)
The patients are the priority and are treated as the core of the core team. It is vital for the team members to work together like a family, to have a shared vision and respect each other and work together to maximise the benefits of recovery and assist patients to achieve their goals.

Implication from the studyThe results indicated that during rehabilitation practice, health professionals’ attitudes towards rehabilitation and patients are very important. The work environment included the physical environment (such as the interdisciplinary team office facilitates the team members’ communication), and the work environment which included the interdependence and relationship with other team members and patients. A healthy work environment will promote healthier employees, which includes improving employee attitudes, enhancing a generally satisfying place to work and increasing productivity.

Implication from the study• Ongoing education and further study were highlighted from the current
research. The nursing staff need to promote themselves more and gain more recognition and a stronger voice within the team. The new staff need to be orientated to the ICF model, the interdisciplinary rehabilitation team framework and post graduate study. Another implication from the study could be more joint sessions between team members and some joint social events to facilitate staff closer relationships between the staff and to establish a strong team member relationship to facilitate teamwork.
• The nurses’ multi-faceted roles implied that some nursing roles, such as assisting patients with toileting, and hygiene and skin care could be done by someone trained to be able to do basic physical and hygiene care to free the nursing staff to do more skilled jobs. This approach indicated a cost effective way to provide high quality nursing care.

LimitationsThe present research was a small study and only involved one rehabilitation centre in New Zealand. Since all the participants were recruited from the same setting with a small sample of nurses, patients, AH staff and doctors over a particular period, it is challenging to apply the findings to other areas.
Limitation from the research methodology: This research setting is the researcher’s workplace, it may raise some potential issues of researcher credibility of the research findings. However, the research process transparency was maintained by communicating and disseminating the research proposal amongst staff and managers, and involving them in the selection of participants. Returning transcripts to the interviewees was another action taken for reflexivity.
The current research did not involve social workers, psychologists, dieticians and rehab assitant, who were also important team members in that rehabilitation centre.

References