rehabilitation protocol for meniscus repair · rehabilitation protocol for meniscus repair this...
TRANSCRIPT

RehabilitationProtocolforMeniscusRepairThisprotocolisintendedtoguidecliniciansandpatientsthroughthepost-operativecourseforameniscusrepair.Specificinterventionshouldbebasedontheneedsoftheindividualandshouldconsiderexamfindingsandclinicaldecisionmaking.Ifyouhavequestions,contactthereferringphysician.ConsiderationsforthePost-operativeMeniscalRepairProgramManydifferentfactorsinfluencethepost-operativemeniscalrepairrehabilitationoutcomes,includingtypeandlocationofthemeniscaltearandrepair.Considertakingamoreconservativeapproachtorangeofmotion,weightbearing,andrehabprogressionwithmorecomplextears,all-insidemeniscalrepairs,andmeniscaltransplants.Itisrecommendedthatclinicianscollaboratecloselywiththereferringphysicianregardingintra-operativefindingsandsatisfactionwiththestrengthoftherepair.Post-operativeconsiderationsIfyoudevelopafever,intensecalfpain,excessivedrainagefromtheincision,uncontrolledpainoranyothersymptomsyouhaveconcernsaboutyoushouldcallyourdoctor.PHASEI:IMMEDIATEPOST-OP(0-2WEEKSAFTERSURGERY)RehabilitationGoals
• Protectrepair• Reduceswelling,minimizepain• Restorepatellarmobility• Restorefullextension• Flexion<90degrees• Minimizearthrogenicmuscleinhibition,re-establishquadcontrol,regainfullactiveextension• Patienteducation
• Keepyourkneestraightandelevatedwhensittingorlyingdown.Donotrestwithatowelplacedundertheknee
• Donotactivelybendyourknee;supportyoursurgicalsidewhenperformingtransfers(i.e.sittingtolayingdown)
• DonotpivotonyoursurgicalsideWeightBearing Walking
• Bracelocked,crutches• Partialweightbearing• Whenclimbingstairs,makesureyouareleadingwiththenon-surgicalsidewhengoingupthe
stairs,makesureyouareleadingwiththecrutchesandsurgicalsidewhengoingdownthestairsIntervention SwellingManagement
• Ice,compression,elevation(checkwithMDre:coldtherapy)• Retrogrademassage• AnklepumpsRangeofmotion/Mobility• Patellarmobilizations:superior/inferiorandmedial/lateral• Seatedassistedkneeflexionextensionandheelslideswithtowel
o ***Avoidactivekneeflexiontopreventhamstringstraintotheposteromedialjoint• Lowintensity,longdurationextensionstretches:pronehang,heelprop• Supinepassivehamstringstretch

MassachusettsGeneralHospitalSportsMedicine
2
Strengthening• Quadsets• NMEShighintensity(2500Hz,75bursts)supinekneeextended10sec/50sec,10contractions,
2x/wkduringsessions—useofclinicalstimulatorduringsession,considerhomeunitsdistributedimmediatepostop
• Straightlegraiseo **Donotperformstraightlegraiseifyouhaveakneeextensionlag
• Hipabduction• Multi-angleisometrics90and60degkneeextension
CriteriatoProgress
• KneeextensionROM0deg• KneeflexionROM90degrees• Quadcontractionwithsuperiorpatellaglideandfullactiveextension• Abletoperformstraightlegraisewithoutlag
PHASEII:INTERMEDIATEPOST-OP(3-5WEEKSAFTERSURGERY)RehabilitationGoals
• Continuetoprotectrepair• Reducepain,minimizeswelling• Maintainfullextension• Flexion<120degrees
WeightBearing Walking• Continuepartialweightbearing• ConsultwithreferringMDregardingunlockingbrace
AdditionalIntervention*ContinuewithPhaseIinterventions
Rangeofmotion/Mobility• Stationarybicycle:gentlerangeofmotiononly(seePhaseIIIforconditioning)Cardio• UpperbodyergometerStrengthening• Calfraises• Lumbopelvicstrengthening:sidelyinghipexternalrotation-clamshell,plankBalance/proprioception• Doublelimbstandingbalanceutilizingunevensurface(wobbleboard)• Jointpositionre-training
CriteriatoProgress
• Noswelling(ModifiedStrokeTest)• FlexionROM120degrees• ExtensionROMequaltocontralateralside
PHASEIII:LATEPOST-OP(6-8WEEKSAFTERSURGERY)RehabilitationGoals
• Continuetoprotectrepair• Maintainfullextension• Normalizegait• Flexionwithin10degreesofcontralateralside• Safelyprogressstrengthening• Promotepropermovementpatterns• Avoidpostexercisepain/swelling
WeightBearing • Maydiscontinueuseofbrace/crutchesafter6wksperMDandonceadequatequadcontrolisachieved
AdditionalIntervention*ContinuewithPhaseI-IIInterventions
Rangeofmotion/Mobility• Supineactivehamstringstretch• Standinggastrocstretchandsoleusstretch• Gentlestretchingallmusclegroups:pronequadstretch,standingquadstretch,kneelinghip
flexorstretch• RotationaltibialmobilizationsiflimitedROM

MassachusettsGeneralHospitalSportsMedicine
3
Cardio• Stationarybicycle,flutterkickswimming,pooljoggingStrengthening• Partialsquatexercise0-60degrees• Ballsquats,wallslides,minisquatsfrom0-60deg• Hamstringstrengthening:pronehamstringcurls• Lumbopelvicstrengthening:bridgesonphysioball,bridgeonphysioballwithroll-in,bridgeon
physioballalternating,hiphike• Gymequipment:legpressmachine,hipabductorandadductormachine,hipextensionmachine,
romanchair,seatedcalfmachine• Progressintensity(strength)andduration(endurance)ofexercisesBalance/proprioception• Singlelimbbalanceprogresstounevensurfaceincludingperturbationtraining
CriteriatoProgress
• Noswelling/painafterexercise• Normalgait• ROMequaltocontralateralside• Jointpositionsensesymmetrical(<5degreemarginoferror)
PHASEIV:TRANSITIONAL(9-12WEEKSAFTERSURGERY)RehabilitationGoals
• MaintainfullROM• Safelyprogressstrengthening• Promotepropermovementpatterns• Avoidpostexercisepain/swelling
AdditionalIntervention*ContinuewithPhaseI-IIIinterventions
Cardio• Elliptical,stairclimberStrengthening
o **Thefollowingexercisestofocusonpropercontrolwithemphasisongoodproximalstability
• Squattochair• Laterallunges• Singlelegprogression:partialweightbearingsinglelegpress,slideboardlunges:retroand
lateral,stepupsandstepupswithmarch,lateralstep-ups,stepdowns,singlelegsquats,singlelegwallslides
• KneeExercisesforadditionalexercisesanddescriptions• Gymequipment:seatedhamstringcurlmachineandhamstringcurlmachine• Romaniandeadlift
CriteriatoProgress
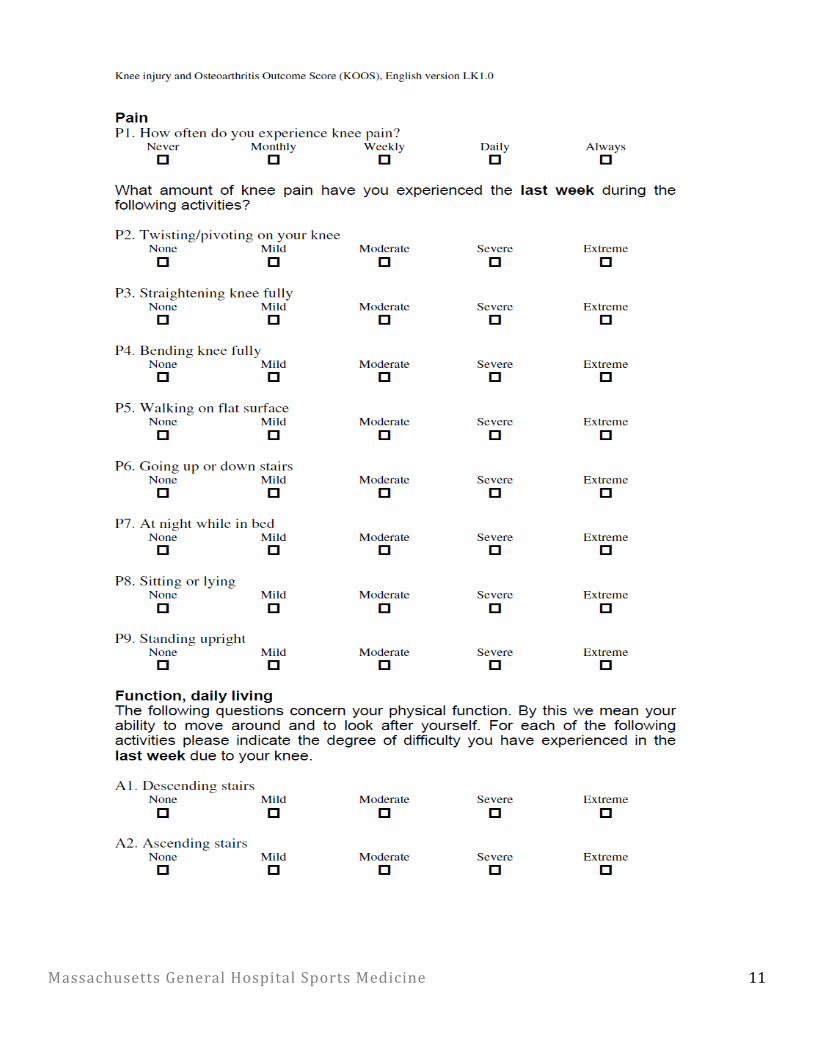
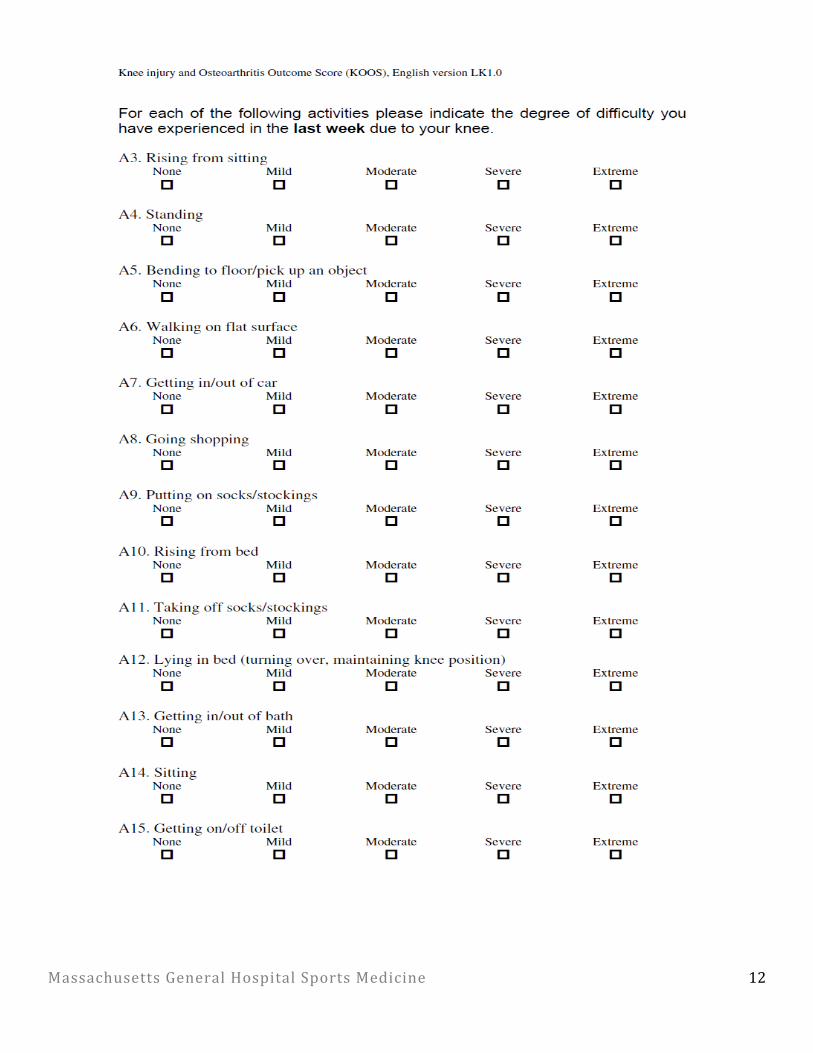
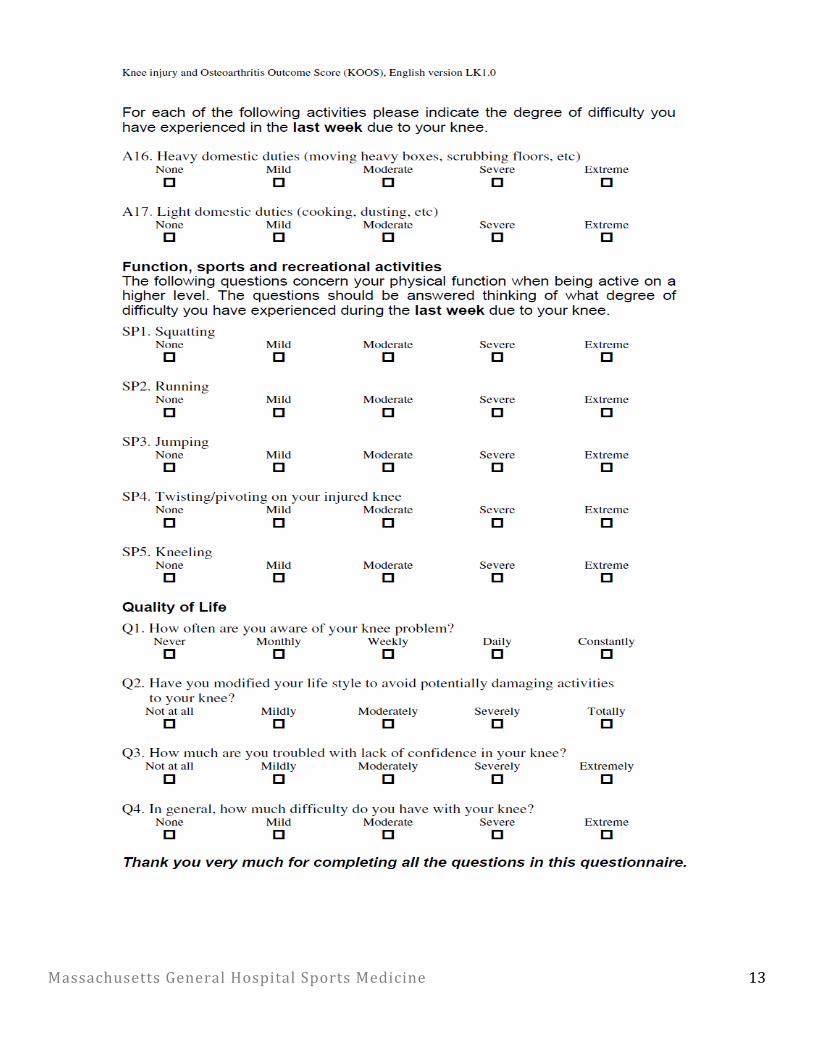
• Noepisodesofinstability• Maintainquadstrength• 10repetitionssinglelegsquatproperformthroughatleast60degkneeflexion• KOOS-sportsquestionnaire>70%• FunctionalAssessment
o Quadricepsindex>80%;HHDmeanpreferred(isokinetictestingifavailable)o Hamstring,glutmed,glutmaxindex≥80%;HHDmeanpreferred(isokinetictestingfor
HSifavailable)o Singleleghoptest≥75%comparedtocontralateralside(earliest12wks)
• Return-to-sporttestingcanbeperformedatMGHSportsPhysicalTherapy,ifnecessary
MassachusettsGeneralHospitalSportsMedicine
4
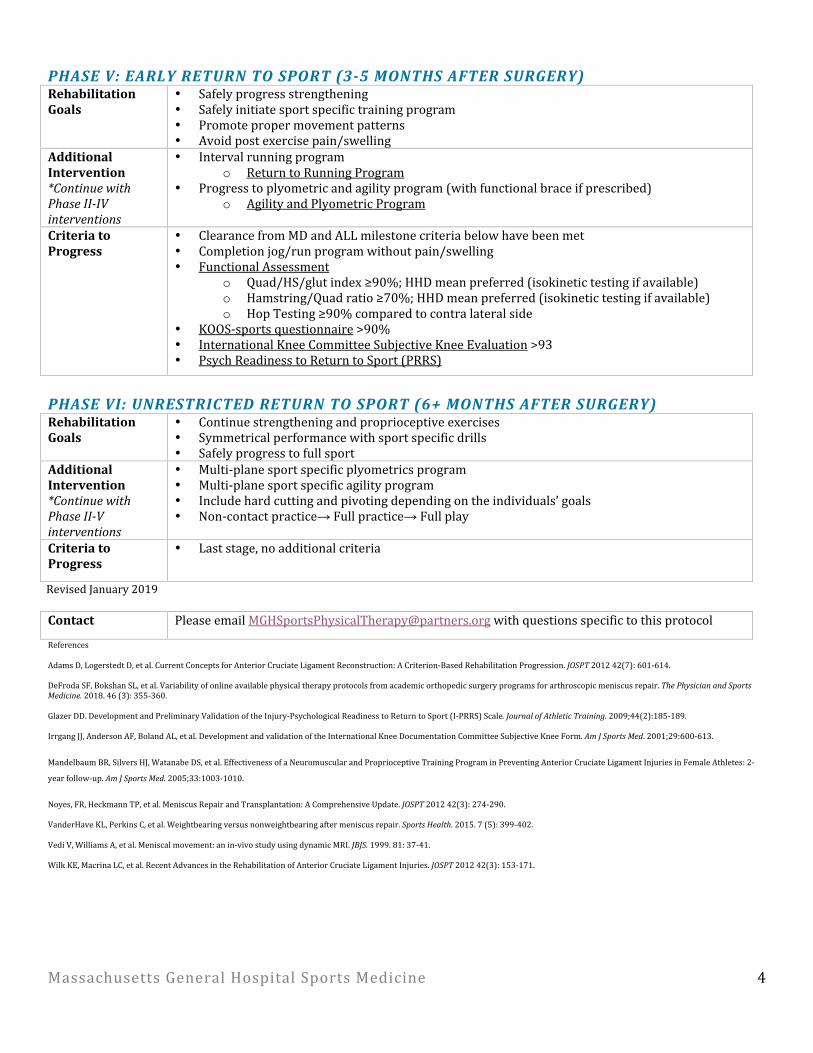
PHASEV:EARLYRETURNTOSPORT(3-5MONTHSAFTERSURGERY)RehabilitationGoals
• Safelyprogressstrengthening• Safelyinitiatesportspecifictrainingprogram• Promotepropermovementpatterns• Avoidpostexercisepain/swelling
AdditionalIntervention*ContinuewithPhaseII-IVinterventions
• Intervalrunningprogramo ReturntoRunningProgram
• Progresstoplyometricandagilityprogram(withfunctionalbraceifprescribed)o AgilityandPlyometricProgram
CriteriatoProgress
• ClearancefromMDandALLmilestonecriteriabelowhavebeenmet• Completionjog/runprogramwithoutpain/swelling• FunctionalAssessment
o Quad/HS/glutindex≥90%;HHDmeanpreferred(isokinetictestingifavailable)o Hamstring/Quadratio≥70%;HHDmeanpreferred(isokinetictestingifavailable)o HopTesting≥90%comparedtocontralateralside
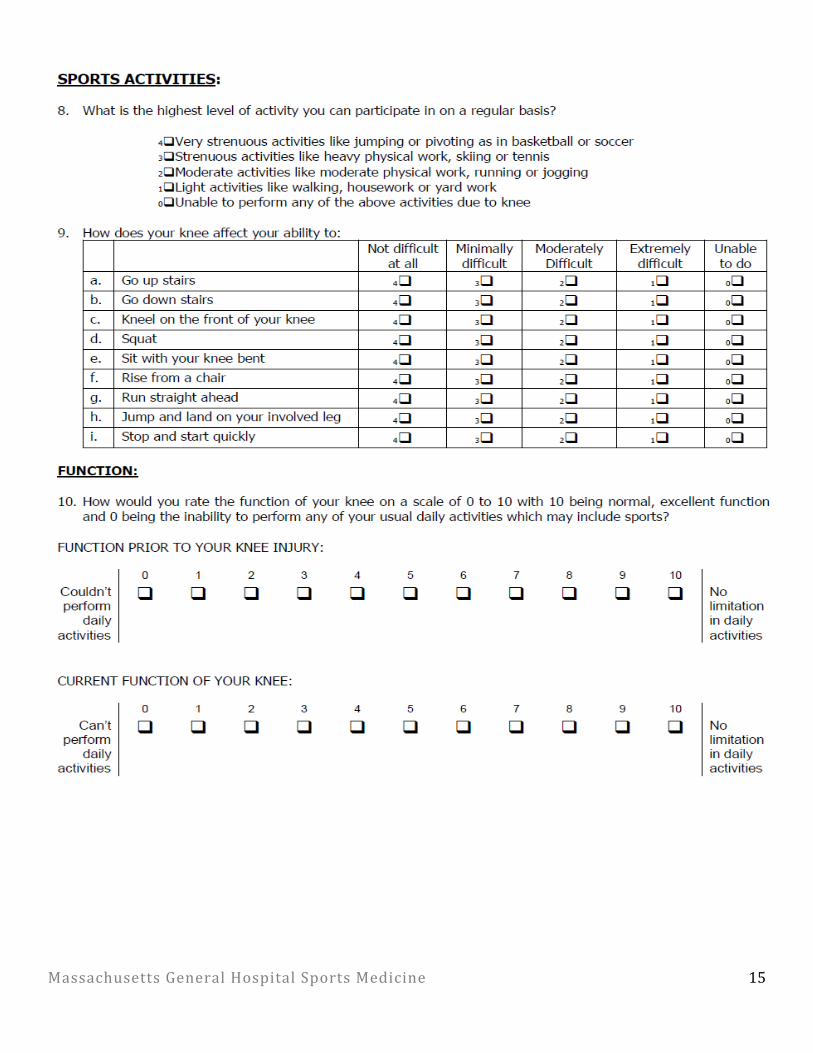
• KOOS-sportsquestionnaire>90%• InternationalKneeCommitteeSubjectiveKneeEvaluation>93• PsychReadinesstoReturntoSport(PRRS)
PHASEVI:UNRESTRICTEDRETURNTOSPORT(6+MONTHSAFTERSURGERY)RehabilitationGoals
• Continuestrengtheningandproprioceptiveexercises• Symmetricalperformancewithsportspecificdrills• Safelyprogresstofullsport
AdditionalIntervention*ContinuewithPhaseII-Vinterventions
• Multi-planesportspecificplyometricsprogram• Multi-planesportspecificagilityprogram• Includehardcuttingandpivotingdependingontheindividuals’goals• Non-contactpractice→Fullpractice→Fullplay
CriteriatoProgress
• Laststage,noadditionalcriteria
RevisedJanuary2019Contact PleaseemailMGHSportsPhysicalTherapy@partners.orgwithquestionsspecifictothisprotocol
ReferencesAdamsD,LogerstedtD,etal.CurrentConceptsforAnteriorCruciateLigamentReconstruction:ACriterion-BasedRehabilitationProgression.JOSPT201242(7):601-614.DeFrodaSF,BokshanSL,etal.Variabilityofonlineavailablephysicaltherapyprotocolsfromacademicorthopedicsurgeryprogramsforarthroscopicmeniscusrepair.ThePhysicianandSportsMedicine.2018.46(3):355-360.GlazerDD.DevelopmentandPreliminaryValidationoftheInjury-PsychologicalReadinesstoReturntoSport(I-PRRS)Scale.JournalofAthleticTraining.2009;44(2):185-189.IrrgangJJ,AndersonAF,BolandAL,etal.DevelopmentandvalidationoftheInternationalKneeDocumentationCommitteeSubjectiveKneeForm.AmJSportsMed.2001;29:600-613.
MandelbaumBR,SilversHJ,WatanabeDS,etal.EffectivenessofaNeuromuscularandProprioceptiveTrainingPrograminPreventingAnteriorCruciateLigamentInjuriesinFemaleAthletes:2-
yearfollow-up.AmJSportsMed.2005;33:1003-1010.
Noyes,FR,HeckmannTP,etal.MeniscusRepairandTransplantation:AComprehensiveUpdate.JOSPT201242(3):274-290.VanderHaveKL,PerkinsC,etal.Weightbearingversusnonweightbearingaftermeniscusrepair.SportsHealth.2015.7(5):399-402.VediV,WilliamsA,etal.Meniscalmovement:anin-vivostudyusingdynamicMRI.JBJS.1999.81:37-41.WilkKE,MacrinaLC,etal.RecentAdvancesintheRehabilitationofAnteriorCruciateLigamentInjuries.JOSPT201242(3):153-171.
MassachusettsGeneralHospitalSportsMedicine
5
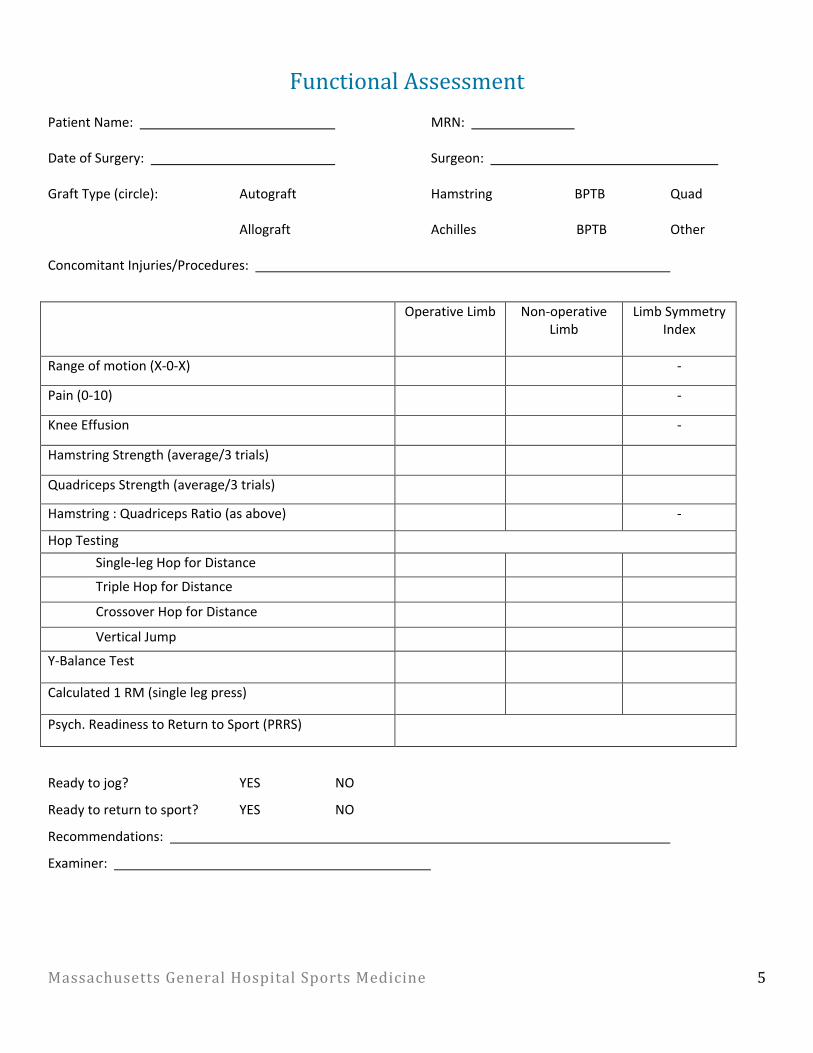
FunctionalAssessmentPatientName: MRN:
DateofSurgery: Surgeon:
GraftType(circle): Autograft Hamstring BPTB Quad
Allograft Achilles BPTB Other
ConcomitantInjuries/Procedures:
Readytojog? YES NO
Readytoreturntosport? YES NO
Recommendations:
Examiner:
OperativeLimb Non-operativeLimb
LimbSymmetryIndex
Rangeofmotion(X-0-X) -
Pain(0-10) -
KneeEffusion -
HamstringStrength(average/3trials)
QuadricepsStrength(average/3trials)
Hamstring:QuadricepsRatio(asabove) -
HopTesting
Single-legHopforDistance
TripleHopforDistance
CrossoverHopforDistance
VerticalJump
Y-BalanceTest
Calculated1RM(singlelegpress)
Psych.ReadinesstoReturntoSport(PRRS)
MassachusettsGeneralHospitalSportsMedicine
6
RangeofmotionisrecordedinX-0-Xformat:forexample,ifapatienthas6degreesofhyperextensionand135degreesofflexion,ROMwouldread:6-0-135.Ifthepatientdoesnotachievehyperextension,andislackingfullextensionby5degrees,theROMwouldsimplyread:5-135.Painisrecordedasanaveragevalueoverthepast2weeks,from0-10.0isabsolutelynopain,and10istheworstpaineverexperienced.KneeEffusionistestedusingtheModifiedStrokeTest.Anupstrokeisappliedtomedialsideofknee,followedbydownstrokeonlateralside.Thetherapistobservesformovementoffluidwitheachstroke.
- 0:nowaveproducedwithdownwardstroke- Trace:smallwaveoffluidonmedialsideofknee- 1+:largebulgeoffluidonmedialsideofkneewithdownstroke- 2+:Effusionreturnstomedialsideofkneewithoutdownstroke- 3+:inabilitytomoveeffusionfrommedialsideofknee
Quadricepsstrengthismeasuredusingahandhelddynamometer.Thepatientissecuredin60degreesofkneeflexionandtheHHDisplacedbetweenthepatient’stibiaandtheresistancearm,1inchproximaltothemidlinebetweenthemalleoli.ThepatientisinstructedtoapplyamaximalisometriceffortforcetheHHDandtheaverageof3trialsisrecordedforeachlimb.Hamstringstrengthismeasuredusingahandhelddynamometer.Thepatientissecuredin60degreesofkneeflexionandtheHHDisplacedbetweenthepatient’slowerlegandtheresistancearm,1inchproximaltothemidlinebetweenthemalleoli.ThepatientisinstructedtoapplyamaximalisometricforceagainsttheHHDandtheaverageof3trialsisrecordedforeachlimb.Hamstring:quadricepsratioiscalculatedforeachlimbbasedontheaverageof3trialsforflexionandextension,respectively.Theaverageisometrichamstringstrengthisdividedbytheaveragequadricepsstrength.Hoptestingisperformedperstandardizedtestingguidelines.Theaverageof3trialsisrecordedtothenearestcentimeterforeachlimb.

MassachusettsGeneralHospitalSportsMedicine
7
ReturntoRunningProgramThisprogramisdesignedasaguideforcliniciansandpatientsthroughaprogressivereturn-to-runprogram.Patientsshoulddemonstrate>80%ontheFunctionalAssessmentpriortoinitiatingthisprogram(afterakneeligamentormeniscusrepair).Specificrecommendationsshouldbebasedontheneedsoftheindividualandshouldconsiderclinicaldecisionmaking.Ifyouhavequestions,contactthereferringphysician. PHASEI:WARMUPWALK15MINUTES,COOLDOWNWALK10MINUTES
Day 1 2 3 4 5 6 7
Week1 W5/J1x5 W5/J1x5 W4/J2x5 W4/J2x5
Week2 W3/J3x5 W3/J3x5 W2/J4x5
Week3 W2/J4x5 W1/J5x5 W1/J5x5 ReturntoRun
Key:W=walk,J=jog**OnlyprogressifthereisnopainorswellingduringoraftertherunPHASEII:WARMUPWALK15MINUTES,COOLDOWNWALK10MINUTES
Week Sunday Monday Tuesday Wednesday Thursday Friday Saturday
1 20min 20min 20min 25min
2 25min 25min 30min
3 30min 30min 35min 35min
4 35min 40min 40min
5 40min 45min 45min 45min
6 50min 50min 50min
7 55min 55min 55min 60min
8 60min 60min
Recommendations• RunsshouldoccuronsoftersurfacesduringPhaseI• Non-impactactivityonoffdays• Goalistoincreasemileageandthenincreasepace;avoidincreasingtwovariablesatonce• 10%rule:nomorethan10%increaseinmileageperweek

MassachusettsGeneralHospitalSportsMedicine
8
AgilityandPlyometricProgramThisprogramisdesignedasaguideforcliniciansandpatientsthroughaprogressiveseriesofagilityandplyometricexercisestopromotesuccessfulreturntosportandreduceinjuryrisk.Patientsshoulddemonstrate>80%ontheFunctionalAssessmentpriortoinitiatingthisprogram.Specificinterventionshouldbebasedontheneedsoftheindividualandshouldconsiderclinicaldecisionmaking.Ifyouhavequestions,contactthereferringphysician. PHASEI:ANTERIORPROGRESSIONRehabilitationGoals
• Safelyreconditiontheknee• Providealogicalsequenceofprogressivedrillsforpre-sportsconditioning
Agility • Forwardrun• Backwardrun• Forwardleanintoarun• Forwardrunwith3-stepdeceleration• Figure8run• Circlerun• Ladder
Plyometrics • Shuttlepress:Doubleleg!alternatingleg!singlelegjumps• Doubleleg:
o Jumpsontoabox!jumpoffofabox!jumpson/offboxo Forwardjumps,forwardjumptobroadjumpo Tuckjumpso Backward/forwardhopsoverline/cone
• Singleleg(theseexercisesarechallengingandshouldbeconsideredformoreadvancedathletes):o Progressivesinglelegjumptaskso Boundingruno Scissorjumpso Backward/forwardhopsoverline/cone
CriteriatoProgress
• Noincreaseinpainorswelling• Pain-freeduringloadingactivities• Demonstratespropermovementpatterns
PHASEII:LATERALPROGRESSIONRehabilitationGoals
• Safelyreconditiontheknee• ProvidealogicalsequenceofprogressivedrillsfortheLevel1sportathlete
Agility*ContinuewithPhaseIinterventions
• Sideshuffle• Carioca• Crossoversteps• Shuttlerun• Zig-zagrun• Ladder
Plyometrics*ContinuewithPhaseIinterventions
• Doubleleg:o Lateraljumpsoverline/coneo Lateraltuckjumpsovercone
• Singleleg(theseexercisesarechallengingandshouldbeconsideredformoreadvancedathletes):o Lateraljumpsoverline/coneo Lateraljumpswithsportcord
CriteriatoProgress
• Noincreaseinpainorswelling• Pain-freeduringloadingactivities• Demonstratespropermovementpatterns
MassachusettsGeneralHospitalSportsMedicine
9
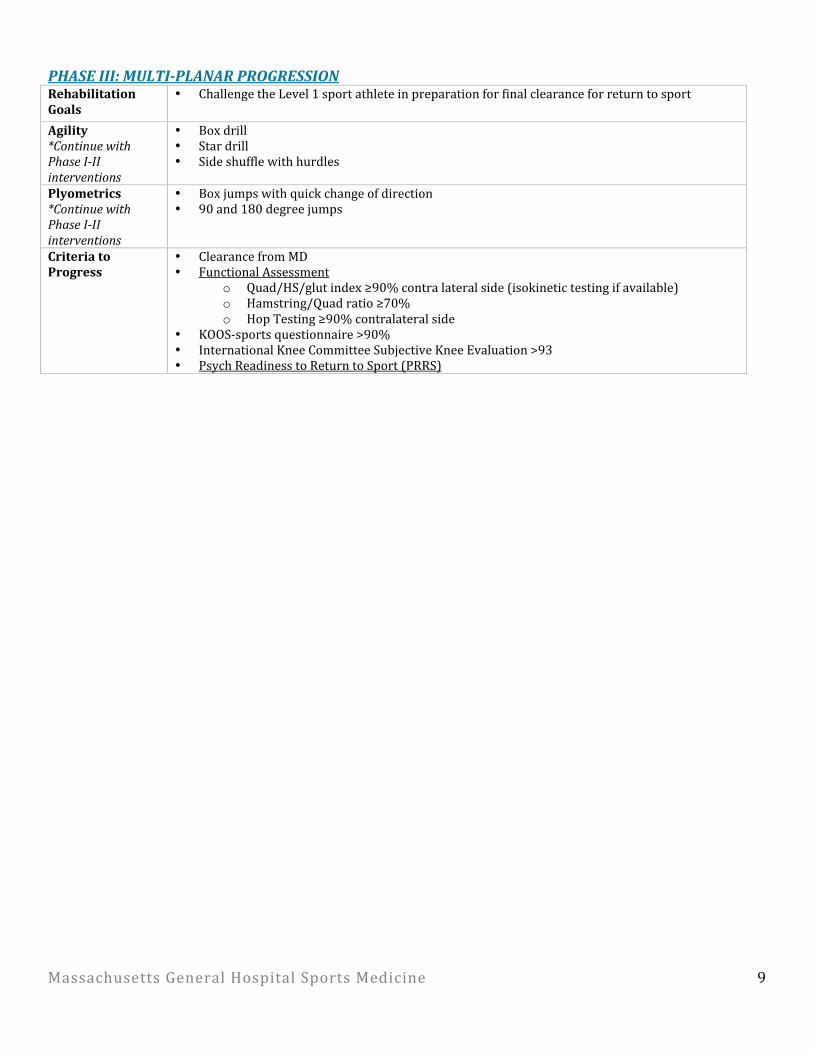
PHASEIII:MULTI-PLANARPROGRESSIONRehabilitationGoals
• ChallengetheLevel1sportathleteinpreparationforfinalclearanceforreturntosport
Agility*ContinuewithPhaseI-IIinterventions
• Boxdrill• Stardrill• Sideshufflewithhurdles
Plyometrics*ContinuewithPhaseI-IIinterventions
• Boxjumpswithquickchangeofdirection• 90and180degreejumps
CriteriatoProgress
• ClearancefromMD• FunctionalAssessment
o Quad/HS/glutindex≥90%contralateralside(isokinetictestingifavailable)o Hamstring/Quadratio≥70%o HopTesting≥90%contralateralside
• KOOS-sportsquestionnaire>90%• InternationalKneeCommitteeSubjectiveKneeEvaluation>93• PsychReadinesstoReturntoSport(PRRS)

MassachusettsGeneralHospitalSportsMedicine
10
MassachusettsGeneralHospitalSportsMedicine
11
MassachusettsGeneralHospitalSportsMedicine
12
MassachusettsGeneralHospitalSportsMedicine
13

MassachusettsGeneralHospitalSportsMedicine
14
MassachusettsGeneralHospitalSportsMedicine
15
MassachusettsGeneralHospitalSportsMedicine
16
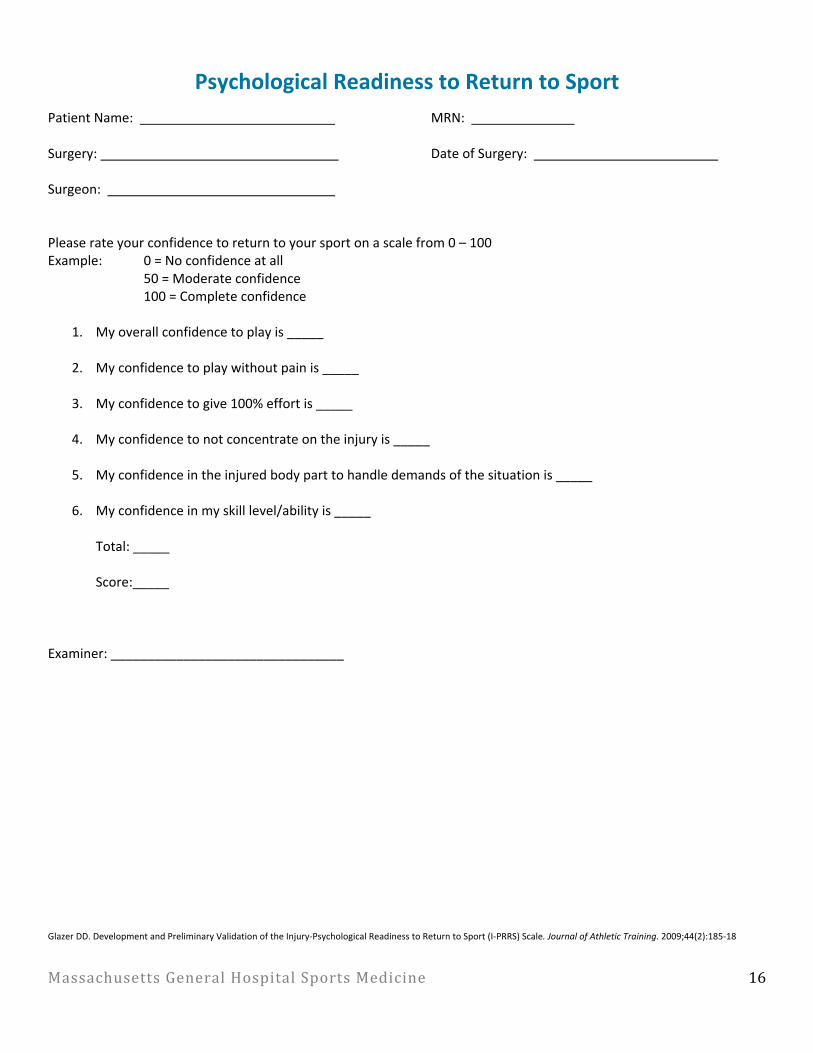
PsychologicalReadinesstoReturntoSport
PatientName: MRN:
Surgery: DateofSurgery:
Surgeon: Pleaserateyourconfidencetoreturntoyoursportonascalefrom0–100Example: 0=Noconfidenceatall 50=Moderateconfidence 100=Completeconfidence
1. Myoverallconfidencetoplayis_____
2. Myconfidencetoplaywithoutpainis_____
3. Myconfidencetogive100%effortis_____
4. Myconfidencetonotconcentrateontheinjuryis_____
5. Myconfidenceintheinjuredbodyparttohandledemandsofthesituationis_____
6. Myconfidenceinmyskilllevel/abilityis_____
Total:_____
Score:_____
Examiner:________________________________
GlazerDD.DevelopmentandPreliminaryValidationoftheInjury-PsychologicalReadinesstoReturntoSport(I-PRRS)Scale.JournalofAthleticTraining.2009;44(2):185-18