relationship between kidney size, renal injury, and...
TRANSCRIPT

Relationship between Kidney Size, Renal Injury, and RenalImpairment Induced by Shock Wave Lithotripsy
LYNN R. WILLIS,* ANDREW P. EVAN,† BRET A. CONNORS,† PHIL BLOMGREN,†
NAOMI S. FINEBERG,‡ and JAMES E. LINGEMAN§
Departments of *Pharmacology and Toxicology,†Anatomy, and‡Medicine, School of Medicine, IndianaUniversity, and§Department of Urology, Methodist Hospital of Indiana, Inc., Indianapolis, Indiana.
Abstract.The relationship between kidney size and impairedrenal function induced by shock-wave lithotripsy (SWL) wasexamined in 6- and 10-wk-old anesthetized pigs. Each pigreceived 2000 shock waves, 24 kV, or sham SWL to the lowerpole calyx of one kidney. Bilateral GFR, renal plasma flow(RPF), and para-aminohippurate extraction was measured 1 hbefore and 1 and 4 h after SWL. The kidneys were thenremoved for morphometric analysis. Mean kidney weightswere 66.16 2.7 g (n 5 9) and 103.16 3.3 g (n 5 8) in theSWL groups, and 60.16 2.6 g (n 5 9) and 82.36 4.0 g (n 59) in the sham-SWL groups. SWL-induced lesions occupied asignificantly greater volume of the small kidneys (6.16 1.7vol % versus1.5 6 0.2 vol % in the large kidneys). RPF was
significantly reduced by SWL in small and large kidneys, butto a significantly greater extent in small kidneys. RPF was alsosignificantly reduced in the contralateral kidneys of bothgroups, but only at 1 h after SWL. SWL significantly reducedGFR to similar degrees in both kidneys of both groups, regard-less of kidney size. Para-aminohippurate extraction was like-wise reduced to similar degrees in both groups, but this effectwas evident only in the SWL-treated kidneys, and only in thepole to which the shock waves had been applied. The injuryinduced by SWL affected a larger fraction of small kidneysthan large ones, and the renal vasoconstriction induced bySWL was greatest in small kidneys.
More than 15 yr of clinical experience with shock-wave lith-otripsy (SWL) as treatment for renal calculi leaves no doubtthat high-energy shock waves can permanently damage renaltissue and, at least acutely, impair renal function (1,2). Grosshematuria consistently occurs after SWL, and magnetic reso-nance imaging reveals kidney damage after SWL in 63 to 85%of human patients (3). Histologic studies in experimental ani-mals show that shock waves injure all tissues within the focalregion (F2) of the shock waves. Vascular injury is most severein this region, with veins and small arteries showing varyingdegrees of damage. The tubular injury induced by SWL in-volves disruption of the tubular epithelium and associatedbasement membrane.
SWL also typically promotes transient impairment of GFRand renal plasma flow (RPF) in human patients (4–10) andexperimental animals (11–13). Results of longer-term studiessuggest that the impairment of renal hemodynamics may bepermanent (2), and at least one clinical report links SWL-induced renal injury to the development of irreversible acuterenal failure (14). Other reports link shock-wave-induced in-jury to the subsequent development of new-onset hypertension
(3,9,15,16) or worsened preexisting hypertension. (3,15). In-deed, elderly patients may be especially susceptible to impair-ment of renal hemodynamics and/or hypertension after SWL(17,18).
Implicit in the notion that renal hemodynamics may bepermanently impaired after SWL is the possibility that at leastsome of the tissue injury caused by the shock waves is irre-versible. Clinical doses of shock waves applied to pig kidneys,which model human kidneys in size, morphology, and function(19), severely damage renal tissue within F2. Although somehealing of the injury occurs, a substantial fraction of thedamaged tissue becomes fibrotic and nonfunctional (20). Be-cause the size of F2 is fixed for most lithotripters (F2 approx-imates a cylinder 8 cm long by 1.5 cm in diameter in theunmodified Dornier HM3 lithotripter), the lesion should en-compass a greater fraction of the functional mass of a smallkidney than of a large one. Accordingly, the resulting lesionand the extent to which renal function may be impaired shouldvary with the size of the kidney. In addition, the extent towhich SWL-induced renal injury impairs renal function mayalso be related to the extent to which renal function may havebeen compromised by preexisting renal disease or injury. Inthis context, attention has increasingly been drawn to thepossibility that risk factors may exist for SWL (2), and therehas been longstanding concern that renal impairment afterSWL may be greater in pediatric patients than in maturepatients (21,22), presumably because pediatric patients havesmaller kidneys. There has also been speculation and concernthat the seemingly higher susceptibility of older patients togreater renal impairment and incidence of hypertension (23,24)
Received August 18, 1998. Accepted February 6, 1999.Correspondence to Dr. Lynn R. Willis, Department of Pharmacology andToxicology, Indiana University School of Medicine, 635 Barnhill Drive,Indianapolis, IN 46202. Phone: 317-274-1562; Fax: 317-274-1560; E-mail:[email protected]
1046-6673/1008-1753Journal of the American Society of NephrologyCopyright © 1999 by the American Society of Nephrology
J Am Soc Nephrol 10: 1753–1762, 1999

after SWL may likewise be attributable to risk factors associ-ated with reduced functional renal mass. The present studieswere conceived with this view of risk factors for SWL in mind.The experiments tested the hypothesis that SWL-induced im-pairment of renal function is greater in small kidneys than inlarge kidneys.
Materials and MethodsAnimal Protocols
Renal Clearance Experiments. Thirty-three female farm pigswere used in the clearance studies. All pigs were obtained from thesame supplier (Hardin Farms) in the Indianapolis area. Sixteen pigswere 6 to 7 wk of age and 17 were 9 to 10 wk of age. Kidneys fromthe older pigs are similar in size to kidneys from mature adult humanbeings. The kidneys of the younger pigs contain a full complement ofnephrons but have only about two-thirds the mass of the kidneys in theolder pigs. Overall, kidney sizes in the two groups of pigs wereapproximately the same as in pediatric and adult human subjects.
On the day of each experiment, a pig was assigned either to a groupthat was to receive SWL or to a sham-control group. Each pig wasanesthetized with ketamine (15 to 20 mg/kg, intramuscularly), intu-bated, and given a mixture of isoflurane (0.8 to 1.5%) and oxygen tobreathe. Respiration was spontaneous. Catheters were placed in amarginal ear vein (Angiocath, 22-gauge, 1 inch) for infusion of fluids,in a femoral artery for monitoring BP and sampling of blood (Inter-cath, 19-gauge, 8 inches), and in both renal veins via the femoral veins(7F “Cobra,” Cook Inc.) for sampling of renal venous blood. Bothureters were cannulated with balloon catheters (7F, 65 cm, Medi-Tech) via a small midline incision immediately superior to the urinarybladder. Each catheter was visualized fluoroscopically and advancedwith the aid of a flexible guide wire to the renal hilus where theballoons were inflated. Positioning of the renal venous catheters wellinto the renal veins was verified by fluoroscopy and injections ofsmall volumes (approximately 0.5 ml) of dilute contrast medium.Body temperature was monitored throughout the experiment andmaintained at 38 to 39°C with the aid of a warming pad.
Isotonic saline was infused intravenously in amounts ranging be-tween 1 and 3% body weight during the 90 min preceding the start ofsample collection. Subsequent infusion rates were adjusted to reflectchanges in urine production.
Polyfructosan (Inutest, Henstettler, Austria) and para-aminohippu-rate (PAH) were infused intravenously in isotonic saline at 1 ml/minto establish and maintain (by continuous infusion) near-steady-stateconcentrations of each marker. Forty-five minutes into the infusion,the first of three consecutive 15-min collections of urine from eachkidney was begun. Femoral arterial and bilateral renal venous bloodsamples were drawn at the midpoint of each collection period. Afterthe third urine collection had been obtained, all infusions werestopped and the pigs were taken, still anesthetized and with allcatheters in place, to the lithotripsy suite, where they were positionedin the treatment gantry and lowered into the water bath (maintained at39°C). A small volume of contrast medium, sufficient to fill the renalpelvis, was injected retrograde into the right ureteral catheter tofacilitate the fluoroscopic placement of the lower pole calyx of theright kidney at F2. Isotonic saline was infused intravenously at ap-proximately 1 ml/min to maintain urine flow. Once placed, the tar-geted region of the kidney was subjected to SWL (2000 shocks, 24kV, unmodified Dornier HM3). The shock waves were administeredat a frequency of 2 Hz, and the electrode was replaced after each 1000shocks (replacement takes about 1 min). A fluoroscopic image wasgenerated after every 500 shocks to verify that F2 was still on target.
After all of the shocks had been administered (usually after about 18to 20 min), the pigs were returned to the laboratory where thesustaining infusion of PAH and polyfructosan was restarted and allmonitors were reconnected. Sets of three 15-min samples of urine,with midpoint arterial and renal venous blood samples, were thenobtained beginning at 1 and 4 h after SWL. At the completion of thesecollections, both kidneys were fixedin situ (see below) and removedfor morphologic analysis.
Sham treatment initially included all procedures except SWL, butwhen it was subsequently realized that data obtained from pigs thatwere not transported to the lithotripsy suite did not differ from dataobtained from pigs that were, transport, immersion, and contrastinjections were not always included in subsequent sham experiments.Time equivalent to that required for the transportation and shock-wave treatment was always included as part of this protocol.
Double Renal Vein Determination of PAH Extraction. In thecourse of fluoroscopically positioning the renal vein catheters, one ofus (B.A.C.) noticed that in some pigs the right renal vein divided intoat least two branches and that one branch appeared to drain the upperpole of that kidney while the other appeared to drain the lower pole.This anatomical feature of the renal veins of the pig is well documen-ted,a and after validating our observation, we conducted six additionalexperiments in which double renal veins were identified for the rightkidney. In those experiments, each renal vein catheter was positionedin one of those branches of the renal vein (Figure 1). No renal venousblood was collected from the left kidneys of those pigs. All othersurgical preparations, subsequent treatment with SWL, and clearancedeterminations were identical to those for the pigs described aboveexcept that renal venous blood was not obtained from the contralateralunshocked kidneys of those pigs, and PAH extractions were deter-mined only for the upper and lower poles of the shocked kidneys.
Tissue Preparation and Morphologic AnalysisAt the completion of the clearance studies, all animals were pre-
pared for vascular perfusion of both kidneys according to our previ-ously published technique (25). The kidneys were then embedded andsectioned. Computer-assisted segmentation techniques were appliedto serial sections of the kidneys, according to our recently developedprotocol, to determine the size of the lesions produced by SWL (26).Four treated kidneys from each group were analyzed in this way.
Analytical ProceduresUrine and plasma samples were analyzed for polyfructosan and
PAH according to standard methods (27,28). Clearances of each werecalculated as estimates, respectively, of GFR and RPF. The concen-tration of PAH in renal venous blood was used to calculate theextraction of PAH (EPAH) according to the equation:EPAH 5 {([PA-H]arterial 2 [PAH]renal venous)} 4 ([PAH]arterial). EPAH provides anestimate of the efficiency of renal tubular PAH secretion and is usedto calculate “true” RPF (RPF5 CPAH/EPAH). Filtration fraction (FF)was calculated asFF 5 GFR/RPF. Because of the variability encoun-tered between pigs within each group, the GFR and RPF data werefactored by kidney weight and are expressed per gram of kidneyweight.
aWrobel K-H: Das Blutgefabsystem der Niere von Sus scrofa dom. unterbesonderer Berucksichtigung des fur die menschlide Niere beschriebenenAbkurzungskrelislaufes. Inaugural Dissertation, Aus dem Veterinar-Anatomis-chen Institut der Justus Liebig, Universitat zu Gleieben, 1961.
1754 Journal of the American Society of Nephrology J Am Soc Nephrol 10: 1753–1762, 1999
Statistical AnalysesMean values were calculated for each set of three determinations
and were analyzed by repeated-measures ANOVA (RM ANOVA).Shocked and unshocked kidneys were analyzed separately. Size andtreatment were used as grouping factors, while time was treated as therepeated measure. When significant changes over time were found inthe RM ANOVA, one-way RM ANOVA and the Newman–Keuls testwere used to determine changes from baseline. The criterion forstatistical significance was set atP , 0.05. The protocol was reviewedand approved by the Institutional Animal Care and Use Committeesfor Indiana University and Methodist Hospital.
ResultsMorphologic Analysis and Quantification of Lesion
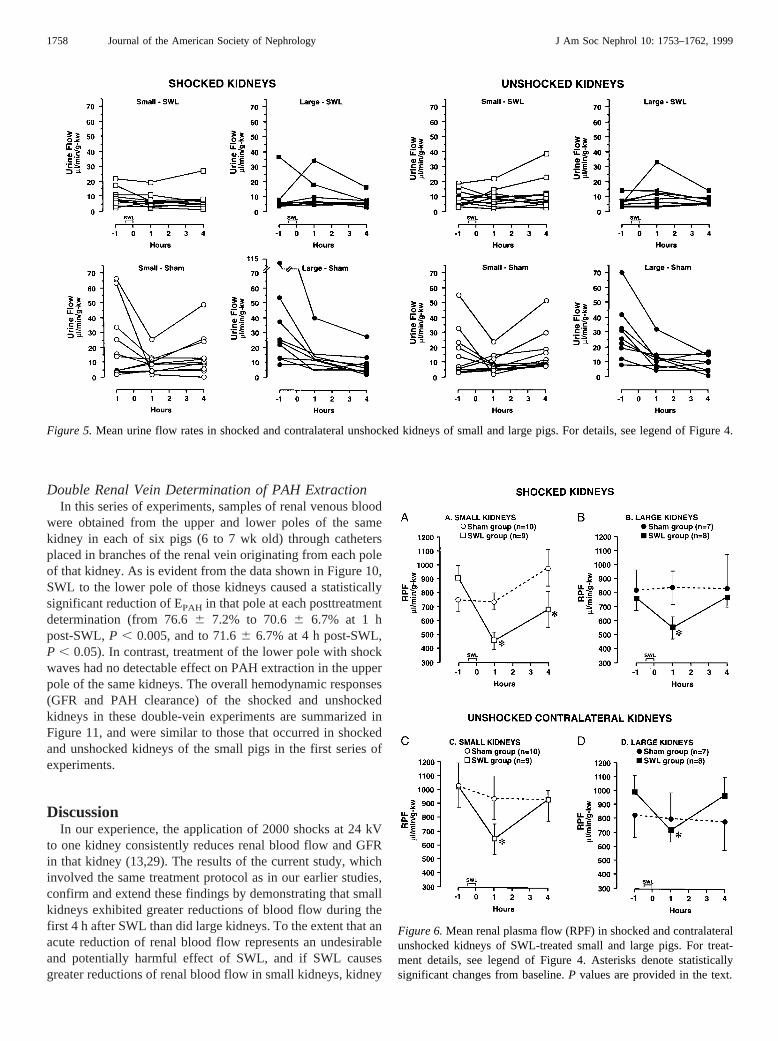
At the time of autopsy, the gross morphologic appearance ofthe SWL-treated kidneys from younger and older pigs wasstrikingly different (Figure 2). Subcapsular hematomas gener-ally encased the entire 6- to 7-wk-old kidney (both anterior andposterior surfaces), whereas the 9- to 10-wk-old kidneys hadmuch smaller sites of hemorrhage (about 1.5 cm in diameter)on either the anterior or posterior surfaces.
Examination of the treated kidneys by light microscopyrevealed multiple sites of hemorrhage within the region of thelower pole corresponding to F2 (Figure 3). Each containedruptured veins and/or arteries. Figure 3 shows a mid-coronalsection from 6- and 10-wk-old kidneys illustrating the locationand size of the SWL-induced damage. The lesions occupied6.1 6 1.7 and 1.56 0.2 volume percent, respectively, of the
younger and older kidneys. The difference between the twomeans is statistically significant (P , 0.05).
Renal Clearance ExperimentsMean body weights, kidney weights, and BP for younger
and older pigs in the SWL and sham-SWL groups are summa-rized in Table 1. Mean body weights did not differ significantlybetween the SWL and sham-SWL subgroups within either agegroup, but the younger pigs in both subgroups weighed signif-icantly less, by more than half, than their older counterparts(P . 0.001).
Kidneys in the younger, smaller pigs of both subgroupsweighed significantly less than those in the two subgroups ofolder, larger pigs, but right and left kidney weights within eachage group were not significantly different from each other.Even so, SWL-treated kidneys tended to weigh, on average,about 10% more than the contralateral untreated kidneys ineach group. This difference probably reflected the extravasa-tion and subcapsular bleeding caused by the shock waves.Since the clearance data obtained for each kidney were fac-tored by kidney weight, the weight discrepancy in shockedkidneys would be expected to underestimate the size of thechange in clearance function occurring in those kidneys afterSWL. As will be evident below, this difference has not affectedthe interpretation of these data.
Mean BP fell to similar degrees in all groups during the 6-hcourse of the experiments. As is evident from Figure 4, whichplots BP for the individual pigs in each group, BP changes
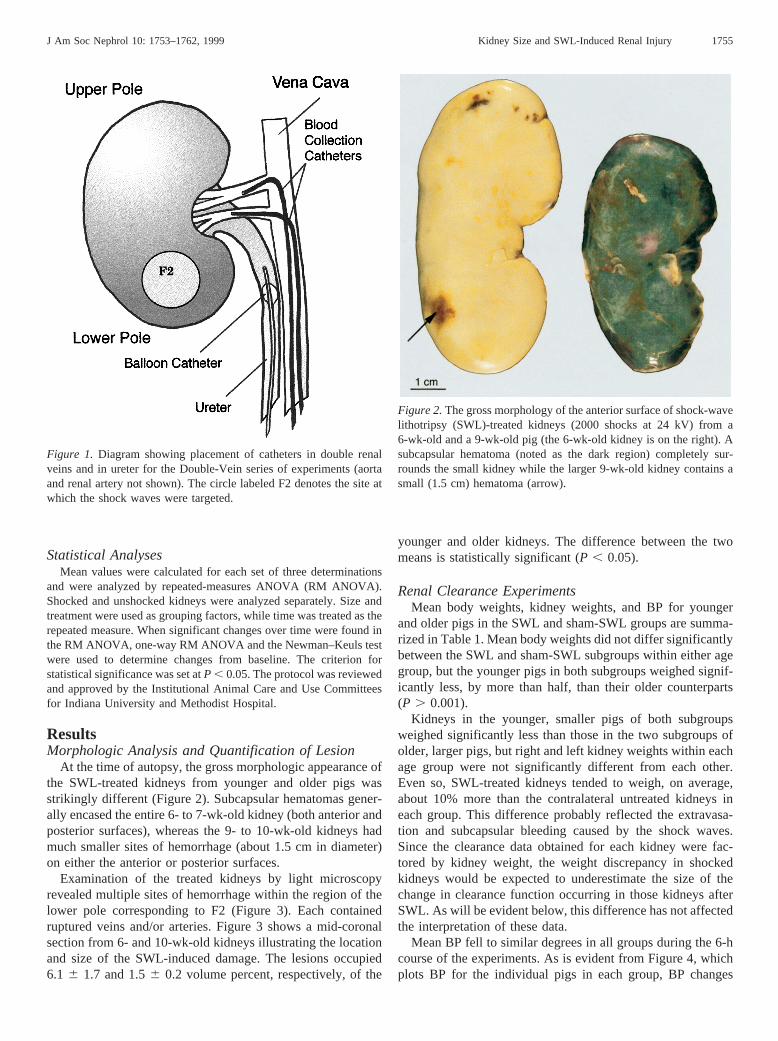
Figure 1. Diagram showing placement of catheters in double renalveins and in ureter for the Double-Vein series of experiments (aortaand renal artery not shown). The circle labeled F2 denotes the site atwhich the shock waves were targeted.
Figure 2.The gross morphology of the anterior surface of shock-wavelithotripsy (SWL)-treated kidneys (2000 shocks at 24 kV) from a6-wk-old and a 9-wk-old pig (the 6-wk-old kidney is on the right). Asubcapsular hematoma (noted as the dark region) completely sur-rounds the small kidney while the larger 9-wk-old kidney contains asmall (1.5 cm) hematoma (arrow).
J Am Soc Nephrol 10: 1753–1762, 1999 Kidney Size and SWL-Induced Renal Injury 1755

from pig to pig were generally consistent over the time courseof the experiments.
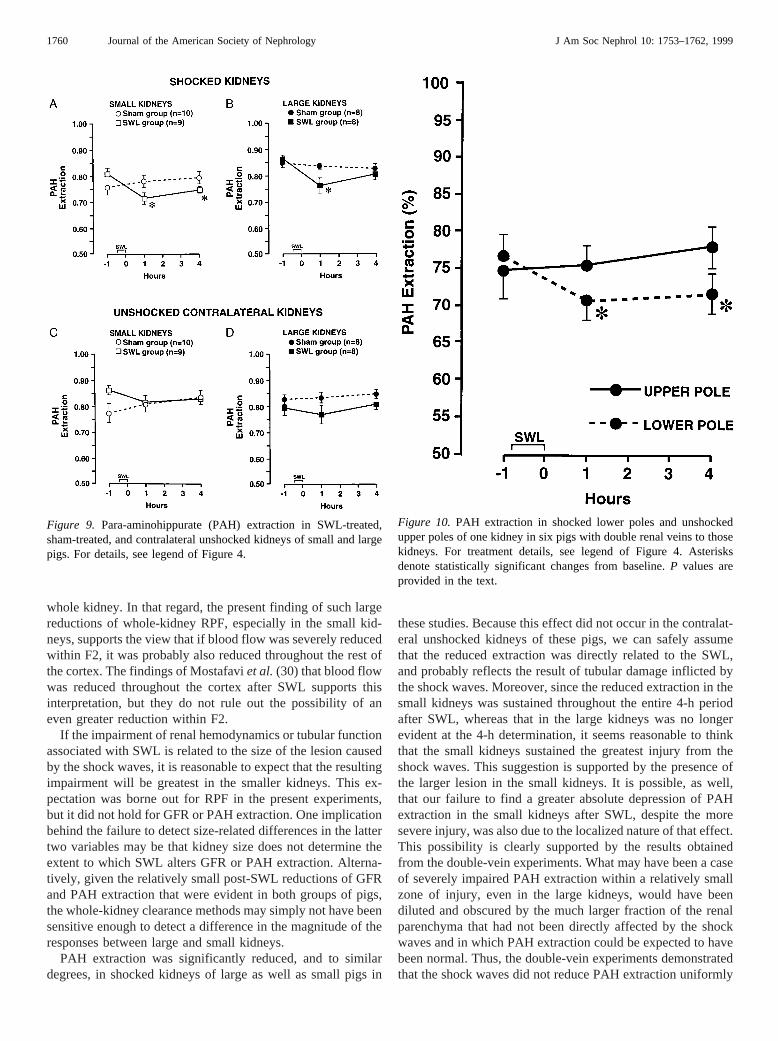
Baseline urine flow rates were, with some exceptions, com-parable in all four groups of pigs (Figure 5). No significantdifferences in baseline urine flow between or within groupswere detected. SWL caused no detectable alteration of urineflow in either group of pigs. Post-SWL urine flow rates in bothgroups of SWL-treated pigs did not differ significantly fromcorresponding values in the sham groups of pigs.
Blood was always evident in urine collected from theshocked kidneys of both SWL-treated subgroups at the 1-hpost-SWL collection, but was generally not evident, except inbarely visible amounts, during the subsequent 4-h collections.Hematuria was never observed in urine obtained from thecontralateral unshocked kidneys of either SWL-treated sub-group, nor was it evident in urine from either kidney of thesham-SWL subgroups.
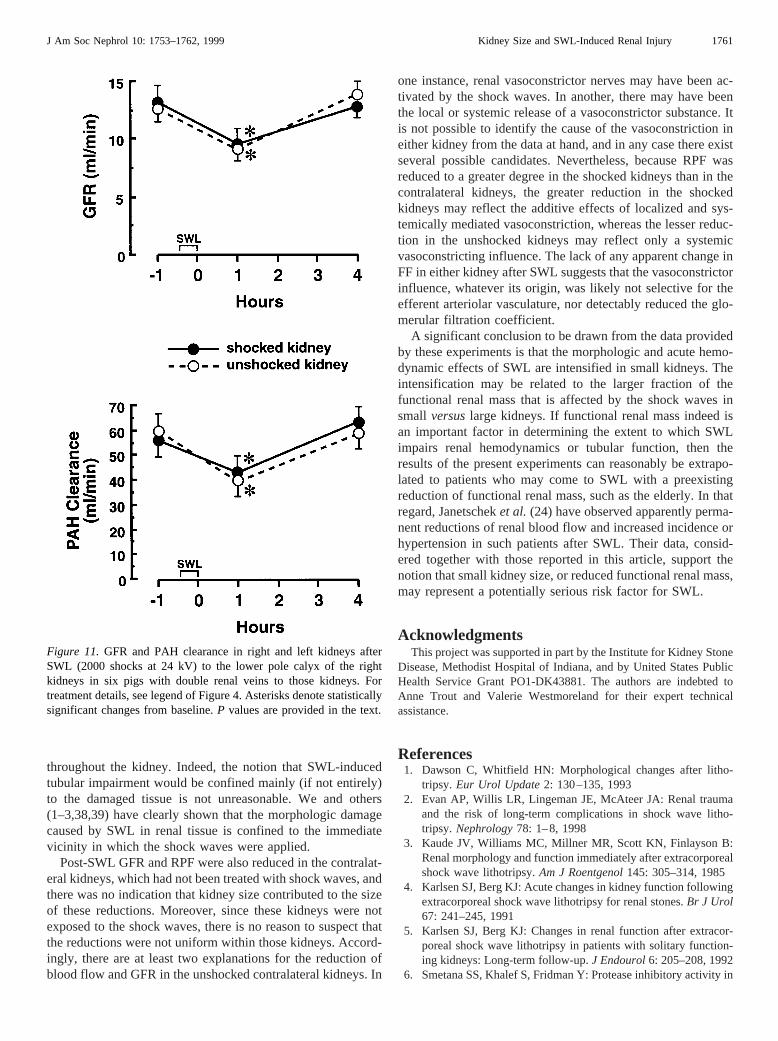
The effect of SWL and sham-SWL on RPF in shocked andunshocked kidneys of younger and older pigs is summarized inFigure 6. Expressed per gram kidney weight, baseline RPF in
both subgroups of 6- to 7-wk-old pigs did not differ signifi-cantly from baseline RPF in the corresponding subgroups ofolder pigs. A size-related difference in baseline RPF wasevident, however, when absolute values were compared be-tween older and younger pigs (baseline RPF in older pigsexceeded that in younger pigs) (data not shown).
SWL applied to the same region of right kidneys of theyounger pigs reduced RPF in those kidneys in all nine animalsstudied (Figure 6A). The mean reduction for this group wasstatistically significant at the 1-h post-SWL determination(P , 0.003), and was sustained below baseline through the 4-hperiod of observation. This response was significantly differentfrom that of the right kidneys in the sham-SWL group of youngpigs for the same period of time (P , 0.02, Figure 6A).
Mean RPF was also reduced by SWL in the shocked kidneysof the older pigs (P , 0.05, Figure 6B), but the individualresponses in those larger kidneys were more variable thanthose in the small kidneys, and, on average, RPF fell to a lesserextent than in the small kidneys. The reduction of RPF in thelarge shocked kidneys was evident only at the 1-h post-SWL
Figure 3.Digitized image (mid-coronal plane) of a 6- and 10-wk-old pig kidney after SWL (2000 shocks at 24 kV to the lower pole calyx).The large circle at the lower pole defines F2. The dark material within the circles (arrows) represents sites of intraparenchymal hemorrhage.The series of dark arrowheads lining the lower pole of the 6-wk-old kidney shows subcapsular hematomas resulting from intraparenchymalbleeding.
1756 Journal of the American Society of Nephrology J Am Soc Nephrol 10: 1753–1762, 1999

determination and had returned to baseline by the 4-h deter-mination. By comparison, RPF did not change significantlyover the course of the experiment in right kidneys of sham-treated older pigs (Figure 6B).
RPF was reduced significantly and to similar degrees in thecontralateral unshocked kidneys of both subgroups of SWL-treated pigs (P , 0.025, Figure 6C;P , 0.05, Figure 6D).
These reductions were evident only at the 1-h post-SWL de-termination, but the overall responses were significantly dif-ferent from the corresponding values in the large and smallsham-SWL pigs (P , 0.002).
The effect of SWL and sham-SWL on GFR (expressed pergram kidney weight) in large and small pigs is summarized inFigure 7. Mean baseline GFR did not differ significantlyamong any of the subgroups. Sham pigs showed no consistentchanges in GFR in either kidney over the time course of thestudy, whereas SWL reduced GFR to similar and statisticallysignificant degrees in both shocked and unshocked kidneys oflarge and small pigs at 1 h post-SWL (P , 0.001). At the 4-hpost-SWL determination, GFR had returned to or exceededbaseline values in both kidneys of large and small pigs. FF dataare summarized in Figure 8. There were no significant changesin FF in any of the subgroups of pigs.
Figure 9 summarizes the PAH extraction data for bothgroups of small and large pigs. Baseline extractions for rightand left kidneys in large and small pigs were not significantlydifferent from each other. SWL reduced EPAH to similar andstatistically significant degrees in the shocked kidneys of largeand small pigs at the 1-h post-SWL determination (29.41 62.03% in small pigs,P , 0.002,versus210.3 6 2.13% inlarge pigs,P , 0.007) (Figure 9, A and B). PAH extraction bythe small shocked kidneys remained significantly below base-line throughout the 4-h post-SWL period (P , 0.002), whereasit had returned to baseline by the 4-h determination in the largeshocked kidneys. In contrast, PAH extraction by the contralat-eral unshocked kidneys in each of the SWL-treated subgroupsshowed no significant change from baseline over the 4-h post-SWL period. No significant changes in PAH extraction wereevident in either kidney of both subgroups of sham-SWL pigs.The post-SWL pattern of PAH extraction seen in both groupsof SWL-treated kidneys was significantly different from thecorresponding patterns in each respective group of sham-con-trols (P , 0.005).
Table 1. Summary of mean body weights, kidney weights, and blood pressure in small and large, SWL-treated and controlpigsa
Group Body Weight (kg)Kidney Weight (g) Mean Blood Pressure (mmHg)
SWL-Treatedb Untreated Pre-SWL 1 h Post-SWL 4 h Post-SWL
SWLsmall pigs 15.26 0.6 72.56 2.4 65.66 2.7 72.76 4.9 68.76 3.6 53.26 2.1large pigs 32.86 2.7c 110.16 11.5c 103.16 10.5c 71.96 11.2d 70.36 9.7d 60.46 5.6d
Rightb Left Baseline 1 h Sham 4 h Sham
Shamsmall pigs 13.36 0.6 59.06 2.6 61.56 2.4 73.46 2.8 71.86 3.7 60.36 3.2large pigs 28.36 1.1c 80.96 4.0c 82.36 5.0c 84.96 5.0d 73.86 5.0d 63.56 3.9d
a Data are presented as mean6 SD. SWL, shock-wave lithotripsy.b The right kidney was always the SWL-treated kidney.c These values are significantly greater than the corresponding value for small pigs (P , 0.05).d Not statistically significant.
Figure 4. Individual mean BP measured in all pigs in the small andlarge, SWL- and sham-treated groups. SWL treatment consisted of2000 shocks at 24 kV to the lower pole calyx of right kidneys. Shamgroups received identical treatment as SWL groups except that theydid not receive SWL. Each treatment lasted approximately 20 min(see SWL designation on the x-axis).
J Am Soc Nephrol 10: 1753–1762, 1999 Kidney Size and SWL-Induced Renal Injury 1757
Double Renal Vein Determination of PAH ExtractionIn this series of experiments, samples of renal venous blood
were obtained from the upper and lower poles of the samekidney in each of six pigs (6 to 7 wk old) through cathetersplaced in branches of the renal vein originating from each poleof that kidney. As is evident from the data shown in Figure 10,SWL to the lower pole of those kidneys caused a statisticallysignificant reduction of EPAH in that pole at each posttreatmentdetermination (from 76.66 7.2% to 70.66 6.7% at 1 hpost-SWL,P , 0.005, and to 71.66 6.7% at 4 h post-SWL,P , 0.05). In contrast, treatment of the lower pole with shockwaves had no detectable effect on PAH extraction in the upperpole of the same kidneys. The overall hemodynamic responses(GFR and PAH clearance) of the shocked and unshockedkidneys in these double-vein experiments are summarized inFigure 11, and were similar to those that occurred in shockedand unshocked kidneys of the small pigs in the first series ofexperiments.
DiscussionIn our experience, the application of 2000 shocks at 24 kV
to one kidney consistently reduces renal blood flow and GFRin that kidney (13,29). The results of the current study, whichinvolved the same treatment protocol as in our earlier studies,confirm and extend these findings by demonstrating that smallkidneys exhibited greater reductions of blood flow during thefirst 4 h after SWL than did large kidneys. To the extent that anacute reduction of renal blood flow represents an undesirableand potentially harmful effect of SWL, and if SWL causesgreater reductions of renal blood flow in small kidneys, kidney
Figure 5.Mean urine flow rates in shocked and contralateral unshocked kidneys of small and large pigs. For details, see legend of Figure 4.
Figure 6.Mean renal plasma flow (RPF) in shocked and contralateralunshocked kidneys of SWL-treated small and large pigs. For treat-ment details, see legend of Figure 4. Asterisks denote statisticallysignificant changes from baseline.P values are provided in the text.
1758 Journal of the American Society of Nephrology J Am Soc Nephrol 10: 1753–1762, 1999

size appears to qualify as a risk factor for SWL-induced im-pairment of renal hemodynamics.
Mostafavi et al. (30) have recently observed substantialreductions of renal cortical blood flow in human patientsduring the first 4 h after SWL (1800 to 2200 shocks at 18 to 20kV). These observations, which were obtained under treatmentconditions similar to those used in our current and earlieranimal studies (13,31,32), corroborate, and extend to humanpatients, our findings that SWL acutely reduces renal bloodflow. Mostafavi et al. (30) also detected an SWL-inducedincrease of medullary blood flow. They attributed that increaseto a compensatory response intended to prevent potential cel-lular damage from hypoxia threatened by an overall reductionof renal blood flow (29).
Another consistent finding in our earlier studies has beenthat SWL always causes severe and localized injury to renaltissue within and near F2 (26). The injury primarily involvesvascular tissue (26), but it also affects all other types of renaltissue within and near F2. Because F2 is of relatively fixeddimensions, the tissue damage induced at F2 should comprisea greater proportion of the renal mass of a small kidney than ofa large one. The current findings support this hypothesis.
The possibility that small kidneys may be at increased risk
for adverse consequences of SWL has been of concern to somepediatric urologists for several years (22). Although pediatricSWL is generally considered safe and effective (33–35), it hasnot been known whether SWL-induced renal damage mayimpair renal growth (36,37) or otherwise adversely affect long-term renal function (37). The present findings support thetheoretical basis for these concerns by demonstrating that theacute tissue damage caused by the shock waves affects a muchlarger fraction of a smaller, and in this case, immature, kidneythan of a larger, more mature one. It remains to be determinedwhether greater initial renal injury from SWL compromisesrenal growth or long-term renal function.
The fourfold difference in fractional lesion size observedbetween small and large kidneys in these studies is substantial.Nevertheless, and kidney size aside, these lesions occupiedonly a relatively small fraction of the total functional mass ofeach kidney. Accordingly, the large average reductions of RPFin the SWL-treated kidneys of each group (50% in smallkidneys and 27% in large kidneys; Figure 6) seem out ofproportion to the size of the lesions. Moreover, it cannot bedetermined from the current results whether the renal vasocon-striction induced by SWL was generalized for the whole kid-ney or was specifically localized within or near F2. This isbecause the classic clearance method for determining RPF orGFR provides only an indication of integrated clearance for the
Figure 7. GFR in shocked and contralateral unshocked kidneys ofsmall and large pigs. For treatment details, see legend of Figure 4.Asterisks denote statistically significant changes from baseline.P values are provided in the text.
Figure 8. Filtration fraction in shocked and contralateral unshockedkidneys of small and large pigs. For treatment details, see legend ofFigure 4.
J Am Soc Nephrol 10: 1753–1762, 1999 Kidney Size and SWL-Induced Renal Injury 1759
whole kidney. In that regard, the present finding of such largereductions of whole-kidney RPF, especially in the small kid-neys, supports the view that if blood flow was severely reducedwithin F2, it was probably also reduced throughout the rest ofthe cortex. The findings of Mostafaviet al.(30) that blood flowwas reduced throughout the cortex after SWL supports thisinterpretation, but they do not rule out the possibility of aneven greater reduction within F2.
If the impairment of renal hemodynamics or tubular functionassociated with SWL is related to the size of the lesion causedby the shock waves, it is reasonable to expect that the resultingimpairment will be greatest in the smaller kidneys. This ex-pectation was borne out for RPF in the present experiments,but it did not hold for GFR or PAH extraction. One implicationbehind the failure to detect size-related differences in the lattertwo variables may be that kidney size does not determine theextent to which SWL alters GFR or PAH extraction. Alterna-tively, given the relatively small post-SWL reductions of GFRand PAH extraction that were evident in both groups of pigs,the whole-kidney clearance methods may simply not have beensensitive enough to detect a difference in the magnitude of theresponses between large and small kidneys.
PAH extraction was significantly reduced, and to similardegrees, in shocked kidneys of large as well as small pigs in
these studies. Because this effect did not occur in the contralat-eral unshocked kidneys of these pigs, we can safely assumethat the reduced extraction was directly related to the SWL,and probably reflects the result of tubular damage inflicted bythe shock waves. Moreover, since the reduced extraction in thesmall kidneys was sustained throughout the entire 4-h periodafter SWL, whereas that in the large kidneys was no longerevident at the 4-h determination, it seems reasonable to thinkthat the small kidneys sustained the greatest injury from theshock waves. This suggestion is supported by the presence ofthe larger lesion in the small kidneys. It is possible, as well,that our failure to find a greater absolute depression of PAHextraction in the small kidneys after SWL, despite the moresevere injury, was also due to the localized nature of that effect.This possibility is clearly supported by the results obtainedfrom the double-vein experiments. What may have been a caseof severely impaired PAH extraction within a relatively smallzone of injury, even in the large kidneys, would have beendiluted and obscured by the much larger fraction of the renalparenchyma that had not been directly affected by the shockwaves and in which PAH extraction could be expected to havebeen normal. Thus, the double-vein experiments demonstratedthat the shock waves did not reduce PAH extraction uniformly
Figure 9. Para-aminohippurate (PAH) extraction in SWL-treated,sham-treated, and contralateral unshocked kidneys of small and largepigs. For details, see legend of Figure 4.
Figure 10. PAH extraction in shocked lower poles and unshockedupper poles of one kidney in six pigs with double renal veins to thosekidneys. For treatment details, see legend of Figure 4. Asterisksdenote statistically significant changes from baseline.P values areprovided in the text.
1760 Journal of the American Society of Nephrology J Am Soc Nephrol 10: 1753–1762, 1999
throughout the kidney. Indeed, the notion that SWL-inducedtubular impairment would be confined mainly (if not entirely)to the damaged tissue is not unreasonable. We and others(1–3,38,39) have clearly shown that the morphologic damagecaused by SWL in renal tissue is confined to the immediatevicinity in which the shock waves were applied.
Post-SWL GFR and RPF were also reduced in the contralat-eral kidneys, which had not been treated with shock waves, andthere was no indication that kidney size contributed to the sizeof these reductions. Moreover, since these kidneys were notexposed to the shock waves, there is no reason to suspect thatthe reductions were not uniform within those kidneys. Accord-ingly, there are at least two explanations for the reduction ofblood flow and GFR in the unshocked contralateral kidneys. In
one instance, renal vasoconstrictor nerves may have been ac-tivated by the shock waves. In another, there may have beenthe local or systemic release of a vasoconstrictor substance. Itis not possible to identify the cause of the vasoconstriction ineither kidney from the data at hand, and in any case there existseveral possible candidates. Nevertheless, because RPF wasreduced to a greater degree in the shocked kidneys than in thecontralateral kidneys, the greater reduction in the shockedkidneys may reflect the additive effects of localized and sys-temically mediated vasoconstriction, whereas the lesser reduc-tion in the unshocked kidneys may reflect only a systemicvasoconstricting influence. The lack of any apparent change inFF in either kidney after SWL suggests that the vasoconstrictorinfluence, whatever its origin, was likely not selective for theefferent arteriolar vasculature, nor detectably reduced the glo-merular filtration coefficient.
A significant conclusion to be drawn from the data providedby these experiments is that the morphologic and acute hemo-dynamic effects of SWL are intensified in small kidneys. Theintensification may be related to the larger fraction of thefunctional renal mass that is affected by the shock waves insmall versuslarge kidneys. If functional renal mass indeed isan important factor in determining the extent to which SWLimpairs renal hemodynamics or tubular function, then theresults of the present experiments can reasonably be extrapo-lated to patients who may come to SWL with a preexistingreduction of functional renal mass, such as the elderly. In thatregard, Janetscheket al. (24) have observed apparently perma-nent reductions of renal blood flow and increased incidence orhypertension in such patients after SWL. Their data, consid-ered together with those reported in this article, support thenotion that small kidney size, or reduced functional renal mass,may represent a potentially serious risk factor for SWL.
AcknowledgmentsThis project was supported in part by the Institute for Kidney Stone
Disease, Methodist Hospital of Indiana, and by United States PublicHealth Service Grant PO1-DK43881. The authors are indebted toAnne Trout and Valerie Westmoreland for their expert technicalassistance.
References1. Dawson C, Whitfield HN: Morphological changes after litho-
tripsy. Eur Urol Update2: 130–135, 19932. Evan AP, Willis LR, Lingeman JE, McAteer JA: Renal trauma
and the risk of long-term complications in shock wave litho-tripsy. Nephrology78: 1–8, 1998
3. Kaude JV, Williams MC, Millner MR, Scott KN, Finlayson B:Renal morphology and function immediately after extracorporealshock wave lithotripsy.Am J Roentgenol145: 305–314, 1985
4. Karlsen SJ, Berg KJ: Acute changes in kidney function followingextracorporeal shock wave lithotripsy for renal stones.Br J Urol67: 241–245, 1991
5. Karlsen SJ, Berg KJ: Changes in renal function after extracor-poreal shock wave lithotripsy in patients with solitary function-ing kidneys: Long-term follow-up.J Endourol6: 205–208, 1992
6. Smetana SS, Khalef S, Fridman Y: Protease inhibitory activity in
Figure 11. GFR and PAH clearance in right and left kidneys afterSWL (2000 shocks at 24 kV) to the lower pole calyx of the rightkidneys in six pigs with double renal veins to those kidneys. Fortreatment details, see legend of Figure 4. Asterisks denote statisticallysignificant changes from baseline.P values are provided in the text.
J Am Soc Nephrol 10: 1753–1762, 1999 Kidney Size and SWL-Induced Renal Injury 1761
serum and urine following extracorporeal shock wave lithotripsy.Contrib Nephrol101: 194–198, 1993
7. Bomanji J, Boddy SAM, Britton KE, Nimmon CC, WhitfieldHN: Radionuclide evaluation: Pre- and post-extracorporealshock wave lithotripsy for renal calculi.J Nucl Med28: 1284–1289, 1987
8. Thomas R, Roberts J, Sloane B, Kaack B: Effect of extracorpo-real shock wave lithotripsy on renal function.J Endourol 2:141–144, 1988
9. Williams CM, Kaude JV, Newman RC, Peterson JC, ThomasWC: Extracorporeal shock-wave lithotripsy: Long-term compli-cations.Am J Roentgenol150: 311–315, 1988
10. Williams CM, Thomas WC: Permanently decreased renal bloodflow and hypertension after lithotripsy.N Engl J Med 321:1269–1270, 1989
11. Karlsen SJ, Smevik B, Stenstrom J, Berg KJ: Acute physiolog-ical changes in canine kidneys following exposure to extracor-poreal shock waves.J Urol 143: 1280–1283, 1990
12. Jaeger P, Redha F, Marquardt K, Uhlschmid G, Hauri D: Mor-phological and functional changes in canine kidneys followingextracorporeal shock-wave treatment.Urol Int 54: 48–58, 1995
13. Willis LR, Evan AP, Connors BA, Reed G, Fineberg NS, Lin-geman JE: Effects of extracorporeal shock wave lithotripsy toone kidney on bilateral glomerular filtration rate and PAH clear-ance in minipigs.J Urol 156: 1502–1506, 1996
14. Diaz-Tejeiro R, Diaz EG, Fernandez G: Irreversible acute renalfailure after extracorporeal shock-wave lithotripsy.Nephrology63: 242–243, 1993
15. Lingeman JE, Kulb TB: Hypertension following extracorporealshock wave lithotripsy [Abstract].J Urol 137: 45A, 1987
16. Ackaert KSJ, Schroder FH: Effects of extracorporeal shock wavelithotripsy (ESWL) on renal tissue.Urol Res17: 3–7, 1989
17. Knapp R, Frauscher F, Helweg G: Age-related changes in resis-tive index following extracorporeal shock wave lithotripsy.J Urol 154: 955–958, 1995
18. Peschel R, Janetschek G, Frauscher F, Hofle G, Bartsch G: DoesESWL induce hypertension in the elderly? [Abstract]J Urol 157:272, 1997
19. Evan AP, McAteer JA, Steidle CP: The mini-pig: An ideal largeanimal model for studies of renal injury in extracorporeal shockwave lithotripsy research. In:Shock Wave Lithotripsy 2, editedby Lingeman JE, Newman DM, New York, Plenum, 1989, pp35–40
20. Evan AP, Willis LR, Connors BA, McAteer JA, Lingeman JE:Renal injury by extracorporeal shock wave lithotripsy.J En-dourol 5: 25–35, 1991
21. Adams MC, Newman DM, Lingeman JE: Pediatric ESWL:Long-term results and effects on renal growth.J Endourol 3:245–254, 1989
22. Newman DE, Kaefer M: Pediatric ESWL: Suitability hinges onlong-term renal effects.Contemp Urol5: 71–76, 1992
23. Knapp R, Frauscher F, Helweg G: Blood pressure changes afterextracorporeal shock wave nephrolithotripsy: Prediction by in-trarenal resistive index.Eur Radiol6: 665–669, 1996
24. Janetschek G, Frauscher F, Knapp R, Hofle G, Peschel R, Bar-tsch G: New onset hypertension after extracorporeal shock wavelithotripsy: Age-related incidence and prediction by resistiveindex.J Urol 158: 346–351, 1997
25. Evan AP, Hay DA, Dail WG: SEM of the proximal tubule of theadult rabbit kidney.Anat Rec191: 397–413, 1978
26. Blomgren PM, Connors BA, Lingeman JE, Willis LR, Evan AP:Quantitation of shock wave lithotripsy-induced lesion in smalland large pig kidneys.Anat Rec249: 341–348, 1997
27. Smith HW, Goldring W, Chassis H: The measurement of thetubular excretory mass, effective blood flow, and filtration rate inthe normal human kidney.J Clin Invest17: 263, 1956
28. Harvey RB, Brothers AJ: Renal excretion of para-aminohippu-rate and creatinine measured by continuous in vivo sampling ofarterial and renal-vein blood.Ann NY Acad Sci102: 46–54, 1962
29. Brezis M, Rosen S: Hypoxia of the renal medulla: Its implica-tions for disease.N Engl J Med332: 647–655, 1995
30. Mostafavi MR, Chavez DR, Cannillo J, Saltzman B, PottumarthiPV: Redistribution of renal blood flow after SWL evaluated byGd-DTPA-enhanced magnetic resonance imaging.J Endourol12: 9–12, 1998
31. Willis LR, Evan AP, Connors BA, Fineberg NS, Lingeman JE:Effects of SWL on glomerular filtration rate and renal plasmaflow in uninephrectomized minipigs.J Endourol 11: 27–32,1997
32. Willis LR, Evan AP, Connors BA, Lingeman JE: Dose–responserelationship between shock wave voltage and renal tubular im-pairment [Abstract].J Urol 157: 85, 1997
33. Myers D, Mobley TB, Jenkins JM, Grine WB, Jordan WR:Pediatric low energy lithotripsy with the Lithostar.J Endourol153: 453–457, 1995
34. Van Horn AC, Hollander JB, Kass EJ: First and second gener-ation lithotripsy in children: Results, comparison and follow-up.J Urol 153: 1969–1971, 1995
35. Goel MC, Baserge NS, Babu RVR, Sinha S, Kapoor R: Pediatrickidney: Functional outcome after extracorporeal shock wavelithotripsy. J Urol 155: 2044–2046, 1996
36. Frick J, Sarica K, Kohle R, Kunit G: Long-term follow-up afterextracorporeal shock wave lithotripsy in children.Eur Urol 19:225–229, 1991
37. Lifshitz DA, Lingeman JE, Zafar FS, Hollensbe, DW, NyhuisAW, Evan AP: Alterations in predicted growth rates of pediatrickidneys treated with extracorporeal shock wave lithotripsy.J Endourol12: 469–475, 1998
38. Delius M, Jordan M, Eizenhoefer H, Marlinghaus E, Heine G,Liebich H-G, Brendel W: Biological effects of shock waves:Kidney haemorrhage by shock waves in dogs—Administra-tion rate dependence.Ultrasound Med Biol14: 689 – 694,1988
39. Roessler W, Steinbach P, Nicolai H, Hofstaedter F, Wieland WF:Effects of high-energy shock waves on the viable human kidney.Urol Res21: 273–277, 1993
This article can be accessed in its entirety on the Internet athttp://www.lww.com/JASN along with related UpToDate topics.
1762 Journal of the American Society of Nephrology J Am Soc Nephrol 10: 1753–1762, 1999